

Abstract
Statement of the Problem:
To perform a successful endodontic treatment, sufficient knowledge about the number of root canals and their morphology is essential. Missed normal variations may burden this treatment.
Purpose:
This study aimed to evaluate the presence of the second canal in the roots of mandibular central and lateral incisors in an Iranian population by employing CBCT images.
Materials and Method:
This cross-sectional study recruited 180 CBCT image of mandible to evaluate the number of roots as well as the number and types of root canals. Data for each sample were collected in a data collection form set and analyzed by chi-square test using SPSS17 software.
Results:
A total of 681 permanent mandibular incisors were assessed. All samples had one root. Most of the samples (70.3%) had only one canal (type 1 Vertucci classification). The frequency of dual-canal in samples was 29.7%; the prevalence of dual-canal in mandibular lateral teeth (35%) was more than the mandibular central teeth (23.9%, p< 0.05). Following type 1 canal, type 3 (15.7%), type 5 (12.9%), type 4 (0.7%), and type 2 (0.3%) canals had the highest frequencies respectively.
Conclusion:
Based on this study, presence of a second canal in mandibular lateral teeth (35%) is more common than in mandibular central teeth (23.9 %). The most common canal type observed was type 1 (according to Vertucci classification) followed by type 3.
Keywords: Anatomy , Root canal , Incisors , Mandible , Cone beam computed tomography
Introduction
For performing a successful endodontic treatment, complete and accurate identification, clearing, and filling of the whole root canal system is crucial. To achieve this goal, clinicians should have sufficient knowledge about the number as well as the morphology of each root canal given that they might present large variations in the normal range. Since unfilled canals are assumed to be a potential cause of infection and can lead to periapical disease after treatment, their accurate detection would be indispensable.[1] One of the most important causes of failure in root canal therapy in mandibular incisors is missed second canals. This problem is recognized more often in mandibular incisors since many dentists are not able to identify this second canal.[2] In presence of a second canal, usually the lingual canal will be missed. It is reported that in most cases, two canals are interconnected in the apical third of the root; hence, it may be assumed that filling one of the canals is enough to seal the apical foramen. However, filling only one of these canals cannot ensure the success of the treatment.[2-5]
Mandibular central and lateral incisors are similar in their roots and canals morphology. These teeth have one root and one canal in most cases. Different studies reported that anatomy and morphology of mandibular incisors root canal system are not as simple as they may seem in the standard periapical radiographs. They may have some variations such as presence of second canals, lateral canals, and apical deltas.[2,4,6-7]
Various methods have been employed to investigate the morphology of the root canal system. These methods are classified into two groups of laboratory and clinical methods. The laboratory methods include decalcification,[5] dye injection,[8] conventional radiographs,[9] micro-computed tomography (Micro-CT) techniques[10] and observation of pulp chamber floor by scanning electron microscopy.[11] The clinical methods include observation during endodontic treatment (with or without magnification tools),[12] radiography[13] and investigation of previous records of patients.[14-5]
Periapical radiography is a valuable diagnostic tool to evaluate root canal morphology under clinical situations,[12] though this imaging technique may suffer from some limitations such as superimposition of surrounding structures, magnification, and distortion in the image and consequently reduced reliability.[16]
Cone beam computed tomography (CBCT) systems are specifically designed to produce three-dimensional (3D) images, with minimum superimposition of the maxillofacial structures. These Imaging system is more justified, suitable, and efficient for studying patients compared to Micro-CT scans that are only limited to in-vitro studies. At present, explicit applications of CBCT in endodontic treatments are well known and by employing this sophisticated technique, the accurate diagnostic and morphological studies of the root canal system would be possible.[16]
Some of the advantages of CBCT are low-dose radiation, short exposure time, and cost-effectiveness. However, CBCT cannot replace panoramic and conventional radiography, and is better to be used as a complementary method.[16-17] The implication of CBCT in dental root canal therapy includes identifying accessory canals in teeth with complex morphology, tuberous root canals, and diagnosis of root resorption, root fractures, and curvature of roots.[17]
This study aimed to evaluate the presence of the second canal in the roots of the mandibular central and lateral incisors in a sample of Iranian population by employing CBCT images available in the archives of a maxillofacial radiography center of Yazd Dental School.
Materials and Method
This cross-sectional study recruited 180 randomly selected mandibular CBCT images of patients referred to a maxillofacial radiography center in Yazd between 2011 and 2015. These images were taken for other diagnostic and therapeutic purposes.
The inclusion criteria were CBCT images of mandible with at least one mandibular incisor with a closed apex, without any filling, calcification, or post-core of the root canal, and without any signs of root resorption or periapical lesions. Moreover, the quality of selected CBCT images should have been good with no motion or foreign object artifacts. CBCT images of non-Iranian patients and syndromic patient were excluded.
A total of 681 mandibular incisors (330 central incisors and 351 lateral incisors) were evaluated.
All CBCT images were obtained by Planmeca ProMax® 3D (Helsinki; Finland) unit with 0.2 mm voxel size, exposure conditions of 10 mA and 90 KVp, and the exposure time of 14 seconds. The field of view (FOV) was 100×70×50mm. In all three (axial, coronal, and sagittal) planes, 0.2 mm slice thickness was selected for more precise detection and interpretation of the root and root canal morphology.
CBCT images were studied on Romexis software (Planmeca; Helsinki; Finland) on a computer monitor (Dell Trinitron, Round Rock TX) under standard conditions (semi-dark room with constant light intensity) to view the images in the axial, sagittal, and coronal planes. The number of roots and root canals (regarding the presence or absence of the second canal) and the type of canals (using Vertucci classification)[5] for each mandibular central and lateral incisor was recorded on a check-list through detailed scrolling along the image from the pulp chamber to the apex part in the axial sections of CBCT images (Figure 1).
Figure1.
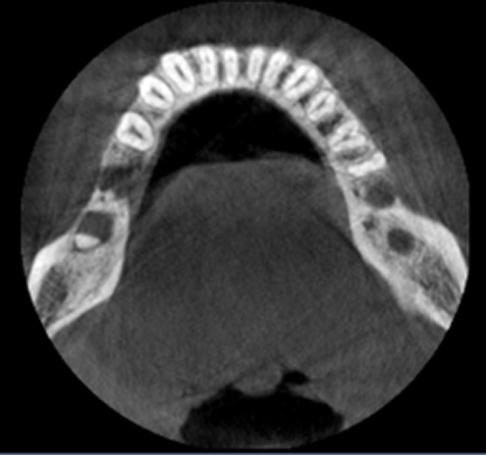
Axial plane, observing two canals in all four mandibular incisors in a patient
During the scrolling along the (axial) plane of the image, the reproduced images of two other (coronal and sagittal) planes were also evaluated. These planes were observed for accurate evaluation of root canal system and number of roots (Figure 2).
Figure2.
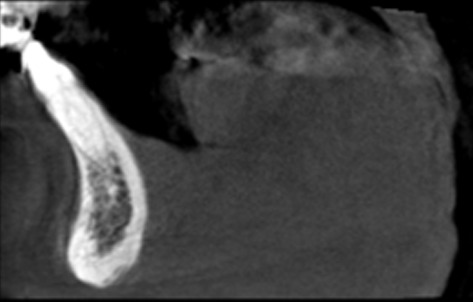
Sagittal plane, double canal in the mandibular lateral teeth
To avoid any bias; all the images were evaluated by two separate radiologist observers. Conflicting images with different opinions of observers were given to the third observer (an endodontist) for interpretation, and his opinion was debated and confirmed by a third radiologist. Final decisions were considered as diagnosis.
Results
In this study, 180 CBCT images of patients referred to a maxillofacial radiography center in Yazd (2011 -2015) were analyzed. In each image, four lateral and central mandibular incisors both sides were evaluated in terms of number of roots and root canals for detection of presence or absence of the second canal and canal type. All samples had one root. Two hundred and two (29.7%) of the examined teeth with 95% confidence interval showed second canal (Figure 3).
Figure3.
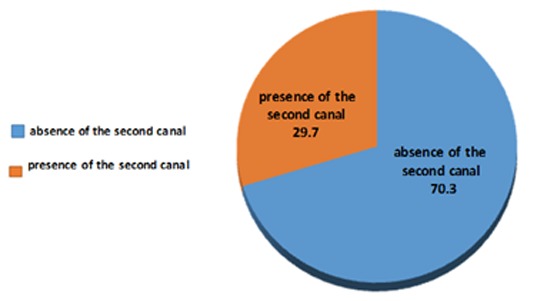
Percentage of presence or absence of the second canal in this study
The interclass correlation coefficient (ICC) of 0.986 was obtained between the first and second observers regarding the detection of the presence of the second canal, with 95% confidence interval from 0.9838 to 0.9880 and p= 0.00. The second canal was detected in ninety-four cases (27.3%) on the right side and in 108 cases (32%) on the left side (Table 1).
Table 1.
Frequency and frequency percentage of the second canal on the right and left sides
| Second canal | Absence | Presence | Total | p Value |
|---|---|---|---|---|
| Side | ||||
| Right | 250(72.7%) | 94(27.3%) | 344(100%) | 0.177 |
| Left | 229(68%) | 108(32%) | 337(100%) | |
| Total | 479(70.3%) | 202(29.7%) | 681(100%) |
Based on the chi-square test results, no significant difference was obtained between left and right sides, considering the presence or absence of the second canal. (p= 0.177) The second canal was present in seventy-nine cases of mandibular central incisors (23.9%) and 123 cases of lateral incisors (35%). (Table 2)
Table 2.
Frequency and the frequency percentage of the second canal in the central and lateral incisors
| Second canal | Absence | Presence | Total | p Value |
|---|---|---|---|---|
| Tooth type | ||||
| central | 251(76.1%) | 79(23.9%) | 330(100%) | 0.002 |
| lateral | 228(65%) | 123(35%) | 351(100%) | |
| Total | 479(70.3%) | 202(29.7%) | 681(100%) |
According to results of chi-square test, there was a significant difference between the frequency of the second canal in mandibular central and lateral incisors. (p< 0.05) The frequency and percentage of the canal type (according to Vertucci classification) is shown in Figure 4.
Figure4.
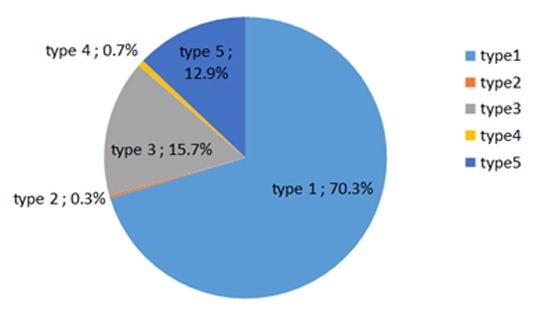
Frequency and percentage of canal types (Vertucci classification) in this study
The highest frequency and percentage in the central teeth were observed in type 1 (251 cases; 76.1%) followed by type 3 (52 cases; 15.8%). In addition, the highest frequency and percentage in the lateral teeth were observed in type 1 (228 cases; 65%) followed by type 5 (63 cases; 17.9%). (Table 3)
Table 3.
Frequency and percentage of the canal types in the central and lateral teeth
| Canal type | 1 | 2 | 3 | 4 | 5 | Total | p Value |
|---|---|---|---|---|---|---|---|
| Tooth type | |||||||
| Central | 251(76.1%) | 0 | 52(15.8%) | 2(0.6%) | 25(7.6%) | 330(100%) | 0.000 |
| Lateral | 228(65%) | 2(0.6% ) | 55(15.7%) | 3(0.9%) | 63(17.9%) | 351(100%) | |
| Total | 479(70.3%) | 2(0.3% ) | 107(15.7%) | 5(0.7%) | 88(12.9%) | 681(100%) |
According to chi-square test, there was a significant difference between the frequency and frequency percentage of canal types in mandibular central and lateral incisors. (p< 0.05) The highest frequency and percentage of the canal type on the right side was detected in type 1 (250 cases; 72.7%) and type 5 (41 cases; 11.9%). The highest frequency and percentage on the left side was seen in type 1 (229 cases; 68%) and type 3 (57 cases; 16.9%). (Table 4) Considering the results of chi-square test, there was no significant difference between the frequency (and frequency percentage) of canal types in mandibular central and lateral incisors on both sides. (p= 0.447)
Table 4.
Frequency and percentage of the canal type in the incisors on the right and left sides
| Canal type | 1 | 2 | 3 | 4 | 5 | Total | p Value |
|---|---|---|---|---|---|---|---|
| Side | |||||||
| Right | 250(72.7% ) | 0 | 50(14.5%) | 3(0.9%) | 41(11.9%) | 344(100%) | 0.447 |
| Left | 229(68%) | 2(0.6%) | 57(16.9%) | 2(0.6%) | 47(13.9%) | 337(100%) | |
| Total | 479 (70.3%) | 2(0.3%) | 107(15.7%) | 5(0.7%) | 88 (12.9%) | 681(100%) |
Discussion
Anthropometric studies are useful to improve and establish data for each race; hence, the current cross-sectional study was conducted to assess 180 CBCT images that included 681 mandibular incisors in order to establish the number of canals and canal types in Iranians.
The inability to detect the second canal is a major cause of root canal therapy failure in mandibular incisors.[2] The incidence of the second canal in mandibular incisors has been reported between 11.5% and 45% in previous studies.[1,3,7] In this study, second canal was observed in 23.9% of central incisors, 35% of lateral incisors, and 29.7% of both mandibular incisors respectively.
Al-Qudah et al.[2] reported a second canal in 26.2% of mandibular incisors, which is similar to the result obtained by our study. With the aid of canal staining and clearing technique, evaluation of 450 extracted mandibular incisors of Jordanian population was performed in their study.
Ezoddini et al.[18] studied 68 extracted mandibular incisors in a sample of Iranian population and reported an incidence of 55.9 % for the second canal, which is not consistent with the results of our study. This difference can be attributed to the difference in sample sizes and methods employed in two studies.
Patel et al.[19] reported the use of CBCT for evaluation of canal to be as precise as modified canal staining and tooth clearing method. Considering that CBCT method is applicable in in-vivo studies, and comparing the studies that were performed with in-vitro design, this method can be more suitable and efficient for patients.[18,20-21]
In the study conducted by Amin Sobhani et al.[22] on 632 central and 614 mandibular lateral incisors, using CBCT imaging in an Iranian population, all samples had one root .They observed double canal in 27.3% of central and 29.4% of lateral incisors which is closely similar to the results obtained by our research. This similarity is rational since same study method was employed (CBCT images) and same race was studied. It should be noticed that in present study, slice thickness was set for 0.2mm, which could provide more precise and accurate results comparing to similar studies.[23-24]
In the study conducted by Geduk et al.[25] in a Turkish population, the presence of the second canal was observed in 36% of mandibular central and lateral incisors. In the present study, the frequency of second canal in mandibular lateral incisors (35%) was higher than mandibular central incisors (23.9%) (p< 0.05), which is consistent with the results of Zitong Lin et al.[4] study. They reported the double canal frequency in the mandibular lateral and central incisors to be 25.5% and 10.9%, respectively. This frequency was reported as 17.5% and 8.9% in Masatoshi et al.[7] study. These differences can be attributed to the difference in the studied races and sample sizes.
Sert et al.[20] performed a study using clearing and staining methods on the extracted mandibular permanent incisors. The result of their study revealed that presence of the second canal was 68% in mandibular central incisors and 63% in mandibular lateral incisors. The differences with the results of current study can be attributed to differences in sample size, study method, and the studied race.
Although most of the mandibular incisors have one apical foramen, supposing that treatment of only one canal would seal the apical foramen cannot always be true, since the presence of pulp tissue remnants in other canals can lead to necrosis and release of destructive compounds to periodontal tissues and consequent failure in the root canal treatment. Therefore, sufficient knowledge of root canal morphology (number and type of canals) in these teeth will be effective in treatment of their root canals.[26]
In present study, all canal types were observed in the mandibular incisors. The most common type of canal reported, based on Vertucci classification, is type 1 (70.3%), followed by type 3 (15.7%) and type 5 (12.9%).
In a research, Geduk et al.[25] investigated the morphology of the mandibular incisors using CBCT imaging and reported that all the mandibular incisors had one root and most of them had one canal (Type 1) (64.4%) followed by type 3 (19.4%) which is consistent with the results of our study. They reported that following type 3, the most common canals were type 2 (15.2%), type 5 (0.8%), and type 4 (0.2%), respectively. In our study, following canal type 3, the type 5 (12.9%), type 4 (0.7%), and type 2 (0.3%) were more prevalent, respectively.
Zitong Lin et al.,[4] conducted a study on the mandibular incisors using CBCT, reported that type 1 (81.8%), and type 3 (12.7%) were the most common canal types, which is consistent with the results yielded by our study. In their study, the prevalence of type 2 was the third most common type while in our study it was type 5 (12.9%).
It should be noticed that considering the higher cost CBCT image taking and also the higher dose of radiation that patients receive in this modality, prescription of this imaging technique is not recommended routinely for every root canal therapy treatment. However, our results support the notion that for post-treatment complications and re-treatment of failed treated mandibular incisors, application of CBCT for determination of possible second canal has its own advantages.
Conclusion
The frequency of second canal in mandibular lateral incisors is higher than mandibular central incisors. The most common canal type is type 1 followed by type 3 according to Vertucci classification.
Acknowledgement
The authors wish to thank the Vice Chancellor of Research of Shahid Sadoughi University of Medical Sciences. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for profit sectors.
Conflict of Interest:The authors certify no conflict of interest.
References
- 1.Pattanshetti N, Gaidhane M, Al Kandari AM. Root and canal morphology of the mesiobuccal and distal roots of permanent first molars in a Kuwait population--a clinical study. Int Endod J. 2008; 41: 755–762. doi: 10.1111/j.1365-2591.2008.01427.x. [DOI] [PubMed] [Google Scholar]
- 2.Al-Qudah AA, Awawdeh LA. Root canal morphology of mandibular incisors in a Jordanian population. Int Endod J. 2006; 39: 873–877. doi: 10.1111/j.1365-2591.2006.01159.x. [DOI] [PubMed] [Google Scholar]
- 3.Tabrizi-Zadeh M, Farazi K. Evaluation of root canal morphology of human mandibular incisors in Yazd. J Dent Med. 2003; 16: 56–60. [Google Scholar]
- 4.Lin Z, Hu Q, Wang T, Ge J, Liu S, Zhu M, et al. Use of CBCT to investigate the root canal morphology of mandibular incisors. Surg Radiol Anat. 2014; 36: 877–882. doi: 10.1007/s00276-014-1267-9. [DOI] [PubMed] [Google Scholar]
- 5.Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endodontic Topics. 2005; 10: 3–29. [Google Scholar]
- 6.Kabak YS, Abbott PV. Endodontic treatment of mandibular incisors with two root canals: report of two cases. Aust Endod J. 2007; 33: 27–31. doi: 10.1111/j.1747-4477.2007.00054.x. [DOI] [PubMed] [Google Scholar]
- 7.Miyashita M, Kasahara E, Yasuda E, Yamamoto A, Sekizawa T. Root canal system of the mandibular incisor. J Endod. 1997; 23: 479–484. doi: 10.1016/S0099-2399(97)80305-6. [DOI] [PubMed] [Google Scholar]
- 8.Yu DC, Tam A, Schilder H. Root canal anatomy illustrated by microcomputed tomography and clinical cases. Gen Dent. 2006; 54: 331–335. [PubMed] [Google Scholar]
- 9.Ingle JI, Bakland LK. Ingle’s endodontics. 6th ed. Hamilton: BC Decker; 2008. p. 603. [Google Scholar]
- 10.Torabinejad M, Walton RE, Fouad AF. Endodontics: Principles and practice. 5th ed. StLouis: Elsevier; 2015. p. 231. [Google Scholar]
- 11.Reuben J, Velmurugan N, Kandaswamy D. The evaluation of root canal morphology of the mandibular firstmolar in an Indian population using spiral computed tomography scan: an in vitro study. J Endod. 2008; 34: 212–215. doi: 10.1016/j.joen.2007.11.018. [DOI] [PubMed] [Google Scholar]
- 12.Cleghorn BM, Christie WH, Dong CC. Root and root canal morphology of the human permanentmaxillary first molar: a literature review. J Endod. 2006; 32: 813–821. doi: 10.1016/j.joen.2006.04.014. [DOI] [PubMed] [Google Scholar]
- 13.Alaçam T, Tinaz AC, Genç O, Kayaoglu G. Second mesiobuccal canal detection in maxillary first molarsusing microscopy and ultrasonics. Aust Endod J. 2008; 34: 106–109. doi: 10.1111/j.1747-4477.2007.00090.x. [DOI] [PubMed] [Google Scholar]
- 14.Vizzotto MB, Silveira PF, Arús NA, Montagner F, Gomes BP, da Silveira HE. CBCT for the assessment of second mesiobuccal (MB2) canalsin maxillary molar teeth: effect of voxel size and presence of root filling. Int Endod J. 2013; 46: 870–876. doi: 10.1111/iej.12075. [DOI] [PubMed] [Google Scholar]
- 15.Zheng QH, Wang Y, Zhou XD, Wang Q, Zheng GN, Huang DM. A cone-beam computed tomography study of maxillary first permanent molar root and canal morphology in a Chinese population. J Endod. 2010; 36: 1480–1484. doi: 10.1016/j.joen.2010.06.018. [DOI] [PubMed] [Google Scholar]
- 16.Cotton TP, Geisler TM, Holden DT, Schwartz SA, Schindler WG. Endodontic applications of cone-beam volumetric tomography. J Endod. 2007; 33: 1121–1132. doi: 10.1016/j.joen.2007.06.011. [DOI] [PubMed] [Google Scholar]
- 17.Scarfe W, Farman A. Oral Radiology—principles and interpretation. 7th ed. Philadelphia: Elsevier: 2014. pp. 199–213. [Google Scholar]
- 18.Ezoddini F, Mohammadi Z, Tabrizizadeh M. Root canal morphology of human mandibular incisors in Yazd province. Dent Res J. 2006;1: 37–39. [Google Scholar]
- 19.Patel S, Dawood A, Ford TP, Whaites E. The potential applications of cone beam computed tomography in the management of endodontic problems. Int Endod J. 2007; 40: 818–830. doi: 10.1111/j.1365-2591.2007.01299.x. [DOI] [PubMed] [Google Scholar]
- 20.Sert S, Bayirli GS. Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J Endod. 2004; 30: 391–398. doi: 10.1097/00004770-200406000-00004. [DOI] [PubMed] [Google Scholar]
- 21.Scarlatescu S, Didilescu AC, Stratul SI, Rusu D, Grigore M, Greabu M, et al. Root Canal Morphology ofMandibular Central Incisors in a South-Eastern Romanian Population: Endodontic and Periodontal Implications. Timisoara Medical Journal. 2010; 60: 280–283. [Google Scholar]
- 22.Aminsobhani M, Sadegh M, Meraji N, Razmi H, Kharazifard MJ. Evaluation of the root and canal morphology of mandibularpermanent anterior teeth in an Iranian population by cone-beam computed tomography. J Dent (Tehran) 2013; 10: 358–366. [PMC free article] [PubMed] [Google Scholar]
- 23.Kayaoglu G, Peker I, Gumusok M, Sarikir C, Kayadugun A, Ucok O. Root and canal symmetry in the mandibular anterior teeth of patients attending a dental clinic: CBCT study. Braz Oral Res. 2015; 29: 1–7. doi: 10.1590/1807-3107BOR-2015.vol29.0090. [DOI] [PubMed] [Google Scholar]
- 24.Altunsoy M, Ok E, Nur BG, Aglarci OS, Gungor E, Colak M. A cone-beam computed tomography study of the root canal morphology of anterior teeth in a Turkish population. Eur J Dent. 2014; 8: 302–306. doi: 10.4103/1305-7456.137630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Geduk G, Deniz Y, Zengin AZ, Eroglu E. Cone-beam computed tomography study of root canal morphology of permanent mandibular incisors in a Turkish sub-population. Journal of Oral and Maxillofacial Radiology. 2015; 3: 7–10. [Google Scholar]
- 26.Cunningham SJ, Hunt NP. Quality of life and its importance in orthodontics. J Orthod. 2001; 28: 152–158. doi: 10.1093/ortho/28.2.152. [DOI] [PubMed] [Google Scholar]