

Abstract
Background
Labour companionship refers to support provided to a woman during labour and childbirth, and may be provided by a partner, family member, friend, doula or healthcare professional. A Cochrane systematic review of interventions by Bohren and colleagues, concluded that having a labour companion improves outcomes for women and babies. The presence of a labour companion is therefore regarded as an important aspect of improving quality of care during labour and childbirth; however implementation of the intervention is not universal. Implementation of labour companionship may be hampered by limited understanding of factors affecting successful implementation across contexts.
Objectives
The objectives of the review were to describe and explore the perceptions and experiences of women, partners, community members, healthcare providers and administrators, and other key stakeholders regarding labour companionship; to identify factors affecting successful implementation and sustainability of labour companionship; and to explore how the findings of this review can enhance understanding of the related Cochrane systematic review of interventions.
Search methods
We searched MEDLINE, CINAHL, and POPLINE K4Health databases for eligible studies from inception to 9 September 2018. There were no language, date or geographic restrictions.
Selection criteria
We included studies that used qualitative methods for data collection and analysis; focused on women’s, partners’, family members’, doulas', providers', or other relevant stakeholders' perceptions and experiences of labour companionship; and were from any type of health facility in any setting globally.
Data collection and analysis
We used a thematic analysis approach for data extraction and synthesis, and assessed the confidence in the findings using the GRADE‐CERQual approach. We used two approaches to integrate qualitative findings with the intervention review findings. We used a logic model to theorise links between elements of the intervention and health and well‐being outcomes. We also used a matrix model to compare features of labour companionship identified as important in the qualitative evidence synthesis with the interventions included in the intervention review.
Main results
We found 51 studies (52 papers), mostly from high‐income countries and mostly describing women's perspectives. We assessed our level of confidence in each finding using the GRADE‐CERQual approach. We had high or moderate confidence in many of our findings. Where we only had low or very low confidence in a finding, we have indicated this.
Labour companions supported women in four different ways. Companions gave informational support by providing information about childbirth, bridging communication gaps between health workers and women, and facilitating non‐pharmacological pain relief. Companions were advocates, which means they spoke up in support of the woman. Companions provided practical support, including encouraging women to move around, providing massage, and holding her hand. Finally, companions gave emotional support, using praise and reassurance to help women feel in control and confident, and providing a continuous physical presence.
Women who wanted a companion present during labour and childbirth needed this person to be compassionate and trustworthy. Companionship helped women to have a positive birth experience. Women without a companion could perceive this as a negative birth experience. Women had mixed perspectives about wanting to have a male partner present (low confidence). Generally, men who were labour companions felt that their presence made a positive impact on both themselves (low confidence) and on the relationship with their partner and baby (low confidence), although some felt anxious witnessing labour pain (low confidence). Some male partners felt that they were not well integrated into the care team or decision‐making.
Doulas often met with women before birth to build rapport and manage expectations. Women could develop close bonds with their doulas (low confidence). Foreign‐born women in high‐income settings may appreciate support from community‐based doulas to receive culturally‐competent care (low confidence).
Factors affecting implementation included health workers and women not recognising the benefits of companionship, lack of space and privacy, and fearing increased risk of infection (low confidence). Changing policies to allow companionship and addressing gaps between policy and practice were thought to be important (low confidence). Some providers were resistant to or not well trained on how to use companions, and this could lead to conflict. Lay companions were often not integrated into antenatal care, which may cause frustration (low confidence).
We compared our findings from this synthesis to the companionship programmes/approaches assessed in Bohren’s review of effectiveness. We found that most of these programmes did not appear to address these key features of labour companionship.
Authors' conclusions
We have high or moderate confidence in the evidence contributing to several of these review findings. Further research, especially in low‐ and middle‐income settings and with different cadres of healthcare providers, could strengthen the evidence for low‐ or very low‐confidence findings. Ahead of implementation of labour companionship, researchers and programmers should consider factors that may affect implementation, including training content and timing for providers, women and companions; physical structure of the labour ward; specifying clear roles for companions and providers; integration of companions; and measuring the impact of companionship on women’s experiences of care. Implementation research or studies conducted on labour companionship should include a qualitative component to evaluate the process and context of implementation, in order to better interpret results and share findings across contexts.
Plain language summary
Perceptions and experiences of labour companionship
What is the aim of this synthesis?
The aim of this Cochrane qualitative evidence synthesis was to explore how women, families, and health workers experience women going through labour and childbirth with a support person ('labour companion'). A labour companion may be the woman’s partner, family member, trained supporter (doula), or nurse/midwife. We collected and analysed all relevant qualitative studies to answer this question.
This qualitative evidence synthesis links to another Cochrane Review by Bohren and colleagues from 2017 that assesses the effect of continuous support for women during childbirth. Continuous support improves health and well‐being for women and babies but factors affecting successful implementation are not well understood.
Key messages
Labour companions provide women with information, practical, and emotional support, and can speak up in support of women. Companions can help women have a positive birth experience and need to be compassionate and trustworthy. However, not all women who want a labour companion have one, especially in lower‐resource settings.
What was studied in this synthesis?
We use the term 'labour companionship' to describe support provided to women during labour and childbirth. In high‐income countries, women are often accompanied by family members or a doula. But in health facilities in low‐ and middle‐income countries, women may not be allowed to have any support person, and may go through labour and childbirth alone.
Bohren's review from 2017 shows that supporting women during childbirth has positive effects on women's experiences and on their health. We sought to understand how women, partners, and healthcare providers felt about labour companionship, and what factors might influence women's access to labour companionship.
What are the main findings?
We found 51 studies, mostly from high‐income countries and mostly describing women's perspectives. We assessed our level of confidence in each finding using the GRADE‐CERQual approach. We had high or moderate confidence in many of our findings. Where we only had low or very low confidence in a finding, we have indicated this.
Labour companions supported women in four different ways. Companions gave informational support by providing information about childbirth, bridging communication gaps between health workers and women, and facilitating non‐pharmacological pain relief. Companions were advocates, which means they spoke up in support of the woman. Companions provided practical support, including encouraging women to move around, providing massage, and holding her hand. Finally, companions gave emotional support, using praise and reassurance to help women feel in control and confident, and providing a continuous physical presence.
Women who wanted a companion present during labour and childbirth needed this person to be compassionate and trustworthy. Companionship helped women to have a positive birth experience. Women without a companion could perceive this as a negative birth experience. Women had mixed perspectives about wanting to have a male partner present (low confidence). Generally, men who were labour companions felt that their presence made a positive impact on both themselves (low confidence) and on the relationship with their partner and baby (low confidence), although some felt anxious witnessing labour pain (low confidence). Some male partners felt that they were not well integrated into the care team or decision‐making.
Doulas often met with women before birth to build rapport and manage expectations. Women could develop close bonds with their doulas (low confidence). Foreign‐born women in high‐income settings may appreciate support from community‐based doulas to receive culturally‐competent care (low confidence).
Factors affecting implementation included health workers and women not recognising the benefits of companionship, lack of space and privacy, and fearing increased risk of infection (low confidence). Changing policies to allow companionship and addressing gaps between policy and practice were thought to be important (low confidence). Some providers were resistant to or not well trained on how to use companions, and this could lead to conflict. Lay companions were often not integrated into antenatal care, which may cause frustration (low confidence).
We compared our findings from this synthesis to the companionship programmes/approaches assessed in Bohren’s review of effectiveness. We found that most of these programmes did not appear to address these key features of labour companionship.
How up‐to‐date is this synthesis?
We searched for studies published before 9 September 2018.
Summary of findings
Summary of findings for the main comparison. Summary of qualitative findings.
| Finding number | Summary of review finding | Studies contributing to the review finding | CERQual assessment (confidence in the findings) | Explanation of CERQual assessment |
| Factors affecting implementation | ||||
| Awareness‐raising among healthcare providers and women | ||||
| 1 | The benefits of labour companionship may not be recognised by providers, women, or their partners. | Abushaikha 2013; Afulani 2018; Alexander 2014; Brüggemann 2014; Coley 2016; Pafs 2016 | Moderate confidence | Due to minor concerns regarding methodological limitations, coherence, and relevance, and moderate concerns regarding adequacy |
| 2 | Labour companionship was sometimes viewed as non‐essential or less important compared to other aspects of care, and therefore deprioritised due to limited resources to spend on 'expendables'. | Akhavan 2012b; Brüggemann 2014; Lagendyk 2005; Premberg 2011 | Low confidence | Due to minor concerns regarding coherence, moderate concerns regarding methodological limitations and serious concerns regarding relevance and adequacy |
| Creating an enabling environment | ||||
| 3 | Formal changes to existing policies regarding allowing companions on the labour ward may be necessary prior to implementing labour companionship models at a facility level. | Abushaikha 2013; Kabakian‐Khasholian 2015 | Low confidence | Due to minor concerns regarding coherence, moderate concerns regarding methodological limitations and serious concerns regarding relevance and adequacy |
| 4 | In settings where companions are allowed, there can be gaps between a policy or law allowing companionship, and the actual practice of allowing all women who want companionship to have a companion present. | Brüggemann 2014; Kaye 2014 | Low confidence | Due to minor concerns regarding coherence, moderate concerns regarding methodological limitations and adequacy, and serious concerns regarding relevance |
| 5 | Providers, women and male partners highlighted physical space constraints of the labour wards as a key barrier to labour companionship as it was perceived that privacy could not be maintained and wards would become overcrowded. | Abushaikha 2013; Afulani 2018; Brüggemann 2014; Harte 2016; Kabakian‐Khasholian 2015; Qian 2001; Sapkota 2012; Shimpuku 2013 | Moderate confidence | Due to minor concerns regarding relevance and coherence, and moderate concerns regarding adequacy and methodological limitations |
| 6 | Some providers, women and male partners were concerned that the presence of a labour companion may increase the risk of transmitting infection in the labour room. | Abushaikha 2013; Brüggemann 2014; Kabakian‐Khasholian 2015; Qian 2001 | Low confidence | Due to minor concerns regarding coherence, moderate concerns regarding methodological limitations and relevance, and serious concerns regarding adequacy |
| Training, supervision, and integration with care team | ||||
| 7 | Some providers were resistant to integrate companions or doulas into maternity services, and provided several explanations for their reluctance. Providers felt that lay companions lacked purpose and boundaries, increased provider workloads, arrived unprepared, and could be in the way. | Bondas‐Salonen 1998; Brüggemann 2014; Horstman 2017; Kabakian‐Khasholian 2015; Kaye 2014; Lagendyk 2005; Torres 2013 | High confidence | Due to minor concerns regarding methodological limitations, coherence and relevance, and moderate concerns regarding adequacy |
| 8 | In most cases, male partners were not integrated into antenatal care or training sessions before birth. Where they were included in antenatal preparation, they felt that they learned comfort and support measures to assist their partners, but that these measures were often challenging to implement throughout the duration of labour and birth. | Abushaikha 2013; Bondas‐Salonen 1998; Chandler 1997; Ledenfors 2016; Sapkota 2012; Somers‐Smith 1999 | Low confidence | Due to minor concerns regarding coherence, moderate concerns regarding methodological limitations and relevance, and serious concerns regarding adequacy |
| 9 | In settings where lay companionship or doula care were available, providers were not well trained on how to integrate the companion as an active or important member of the woman’s support team. | Bondas‐Salonen 1998; Brüggemann 2014; Kabakian‐Khasholian 2015; Kaye 2014; Lagendyk 2005; Torres 2013 | Moderate confidence | Due to minor concerns regarding methodological limitations, coherence and relevance, and moderate concerns regarding adequacy |
| 10 | Some doulas felt that they were not well integrated into decision‐making or care co‐ordination by the healthcare providers, and were sometimes ignored by healthcare providers. | Berg 2006; McLeish 2018; Stevens 2011; Torres 2013 | Low confidence | Due to minor concerns regarding coherence, moderate concerns regarding methodological limitations, and serious concerns regarding relevance and adequacy |
| 11 | Most healthcare providers believed that having a lay companion support a woman throughout labour and childbirth was beneficial to the woman and worked well when companions were integrated into the model of care. However, when lay companions were not well engaged or integrated, conflict could arise as they may be perceived as an additional burden for healthcare providers to manage their presence, and provide ongoing direction and support. | Brüggemann 2014; Harte 2016; Kabakian‐Khasholian 2015; Khresheh 2010; Maher 2004; Qian 2001 | Moderate confidence | Due to minor concerns regarding coherence, and moderate concerns regarding methodological limitations, relevance, and adequacy |
| 12 | Most midwives believed that doulas played a collaborative role in supporting women during childbirth, and were assets to the team who provided more woman‐centred, needs‐led support. However, some midwives found it difficult to engage as carers with women when doulas were present, as they felt that doulas encroached on their carer role. | Akhavan 2012b; Lundgren 2010; McLeish 2018; Stevens 2011 | Low confidence | Due to minor concerns regarding coherence, moderate concerns regarding methodological limitations and adequacy, and serious concerns regarding relevance |
| 13 | Lay companions received little or no training on how to support the woman during labour and childbirth, which made them feel frustrated. | Kululanga 2012; Sapkota 2012 | Low confidence | Due to minor concerns regarding methodological considerations and coherence, and serious concerns regarding relevancy and adequacy |
| 14 | Some men felt that they were actively excluded, left out, or not involved in their female partner's care. They were unsure of where they fit in to support the woman, and felt that their presence was tolerated but not necessary. | Bäckström 2011; Chandler 1997; Kaye 2014; Kululanga 2012; Longworth 2011; Somers‐Smith 1999 | Moderate confidence | Due to minor concerns regarding coherence, and moderate concerns regarding methodological limitations, relevance and adequacy |
| Roles that companions play | ||||
| Informational support | ||||
| 15 | Women valued the non‐pharmacological pain relief measures that companions helped to facilitate, including a soothing touch (holding hands, massage and counter pressure), breathing, and relaxation techniques. | Campero 1998; Chapman 1990; Dodou 2014; de Souza 2010; Fathi 2017; Hunter 2012; Kabakian‐Khasholian 2015; Khresheh 2010; Lundgren 2010; McLeish 2018; Sapkota 2013; Sapkota 2012; Somers‐Smith 1999; Thorstensson 2008; Torres 2015 | High confidence | Due to minor concerns regarding adequacy, coherence, and relevance, and moderate concerns regarding methodological limitations |
| 16 | Doulas played an important role in providing information to women about the process of childbirth, duration of labour, and reasons for medical interventions. They bridged communication gaps between clinical staff and women, and facilitated a more actively engaged environment where women were encouraged to ask questions. | Akhavan 2012a; Akhavan 2012b; Berg 2006; Campero 1998; Darwin 2016; Gilliland 2011; Horstman 2017; LaMancuso 2016; McGarry 2016; McLeish 2018; Schroeder 2005; Torres 2013; Torres 2015 | Moderate confidence | Due to minor concerns regarding coherence and adequacy and moderate concerns regarding methodological limitations and relevance |
| 17 | Lay companions also played a role in providing informational support to women or acting as the woman's voice during labour and childbirth. This usually took the form of acting as an intermediary by relaying, repeating, or explaining information from the healthcare provider to the woman, and from the woman to the healthcare provider. | Alexander 2014; Bondas‐Salonen 1998; Khresheh 2010; Price 2007; Qian 2001; Sapkota 2012 | Moderate confidence | Due to minor concerns regarding methodological limitations, coherence and relevance, and moderate concerns regarding adequacy |
| 18 | Companions played an important role to help facilitate communication between the woman and healthcare providers, including representing the woman's interests and speaking on her behalf when she was unable to do so. They helped to relay information between the woman and healthcare provider, such as asking questions and setting boundaries. | Akhavan 2012b; Bondas‐Salonen 1998; Darwin 2016; Gentry 2010; Hardeman 2016; Horstman 2017; Hunter 2012; Khresheh 2010; Koumouitzes‐Douvia 2006; LaMancuso 2016; Lundgren 2010; McGarry 2016; McLeish 2018; Premberg 2011; Price 2007; Stevens 2011; Torres 2015 | Moderate concerns | Due to minor concerns regarding coherence and adequacy, and moderate concerns regarding methodological limitations and relevance |
| Advocacy | ||||
| 19 | Companions played a role to bear witness to the process of childbirth. They shared the childbirth experience with the woman by being with her, and were viewed as observers who could monitor, reflect, and report on what transpired throughout labour and childbirth, such as witnessing pain, the birth process, and the woman's transformation to motherhood. | Afulani 2018; Alexander 2014; Bondas‐Salonen 1998; Dodou 2014; Horstman 2017; Hunter 2012; Longworth 2011; Price 2007; Sapkota 2012 | High confidence | Due to minor concerns regarding methodological considerations, coherence, relevance and adequacy |
| Practical support | ||||
| 20 | Companions provided physical support to women throughout labour and childbirth, such as giving them a massage and holding their hand. Companions encouraged and helped women to mobilise throughout labour or to change positions, such as squatting or standing, and provided physical support to go to the bathroom or adjust clothing. | Afulani 2018; Chandler 1997; Chapman 1990; de Souza 2010; Fathi 2017; Hunter 2012; Kabakian‐Khasholian 2015; Khresheh 2010; Koumouitzes‐Douvia 2006; McLeish 2018; Premberg 2011; Price 2007; Sapkota 2012; Shimpuku 2013; Torres 2013 | High confidence | Due to minor concerns regarding coherence, relevance and adequacy, and moderate concerns regarding methodological limitations |
| 21 | Companions played an important role to assist healthcare providers to care for women by observing and identifying potential issues throughout labour and childbirth. | Akhavan 2012b; Alexander 2014; Khresheh 2010; Qian 2001; Sapkota 2012; Shimpuku 2013 | Moderate confidence | Due to minor concerns regarding coherence and relevance, and moderate concerns regarding methodological limitations and adequacy |
| 22 | Some healthcare providers and doulas felt that shortcomings in maternity services could be potentially addressed by doulas or lay companions. | Afulani 2018; Akhavan 2012b; Stevens 2011 | Very low confidence | Due to minor concerns regarding coherence, moderate concerns regarding methodological limitations, and serious concerns regarding relevance and adequacy |
| Emotional support | ||||
| 23 | Women valued that companions and doulas helped to facilitate their feeling in control during labour and gave them confidence in their abilities to give birth. | Berg 2006; Campero 1998; Chapman 1990; Darwin 2016; Dodou 2014; Fathi 2017; Gilliland 2011; Hunter 2012; Ledenfors 2016; Price 2007; Sapkota 2012 | Moderate confidence | Due to minor concerns regarding adequacy and coherence, and moderate concerns regarding methodological limitations and relevance |
| 24 | Companions often provided emotional support to women through the use of praise and reassurance. They acknowledged the women's efforts and concerns, and provided reinforcement through verbal encouragement and affirmations. | Abushaikha 2012; Alexander 2014; Bäckström 2011; Berg 2006; Bondas‐Salonen 1998; de Souza 2010; Fathi 2017; Gentry 2010; Gilliland 2011; Hardeman 2016; Harte 2016; Horstman 2017; Hunter 2012; Kabakian‐Khasholian 2015; Khresheh 2010; Koumouitzes‐Douvia 2006; Ledenfors 2016; Lundgren 2010; McGarry 2016; McLeish 2018; Premberg 2011; Price 2007; Sapkota 2012; Schroeder 2005; Somers‐Smith 1999; Thorstensson 2008; Torres 2013; Torres 2015 | High confidence | Due to very minor concerns regarding adequacy, minor concerns regarding coherence and relevance, and moderate concerns regarding methodological limitations |
| 25 | The continuous physical presence of someone caring was an important role that companions played, particularly in settings where continuous midwifery care was not available or not practiced. The continuous presence of the companion signalled to the woman the availability of support when needed, and helped to pass the time throughout labour. | Abushaikha 2012; Afulani 2018; Berg 2006; Bondas‐Salonen 1998; Campero 1998; Darwin 2016; Dodou 2014; Koumouitzes‐Douvia 2006; Lundgren 2010; McLeish 2018; Price 2007; Sapkota 2012; Somers‐Smith 1999; Stevens 2011; Thorstensson 2008; Torres 2015 | Moderate confidence | Due to minor concerns regarding coherence and adequacy, and moderate concerns regarding methodological limitations and relevance |
| Experiences of companionship | ||||
| Women’s experiences | ||||
| 26 | Women stated different preferences for their desired companion, including their husband or male partner, sister, mother, mother‐in‐law, doula, or a combination of different people. Regardless of which person they preferred, women who wanted a labour companion present during labour and childbirth expressed the need for this person to be a caring, compassionate, and trustworthy advocate. | Abushaikha 2012; Afulani 2018; Akhavan 2012a; Alexander 2014; Berg 2006; Bondas‐Salonen 1998; Campero 1998; Dodou 2014; Fathi 2017; Hunter 2012; Kabakian‐Khasholian 2015; Khresheh 2010; Lundgren 2010; Pafs 2016; Price 2007; Qian 2001; Sapkota 2012; Shimpuku 2013; Somers‐Smith 1999; Torres 2015 | High confidence | Due to very minor concerns regarding coherence, relevance and adequacy, and minor concerns regarding methodological limitations |
| 27 | Women described the desire for a happy and healthy birth for both themselves and their babies. Support provided by doulas and companions paved the way for them to have a positive birth experience, as the support facilitated them to feel safe, strong, confident and secure. | Abushaikha 2012; Abushaikha 2013; Akhavan 2012a; Alexander 2014; Berg 2006; Bondas‐Salonen 1998; Campero 1998; Darwin 2016; Dodou 2014; Gilliland 2011; Hunter 2012; Kabakian‐Khasholian 2015; Khresheh 2010; Koumouitzes‐Douvia 2006; Ledenfors 2016; Lundgren 2010; McGarry 2016; Price 2007; Sapkota 2012; Schroeder 2005; Torres 2015 | High confidence | Due to minor concerns regarding coherence, relevance, and adequacy, and moderate concerns regarding methodological limitations |
| 28 | Immigrant, refugee, and foreign‐born women resettled in high‐income countries highlighted how community‐based doulas (e.g. someone from their ethnic/religious/cultural community trained as a doula) were an important way for them to receive culturally competent care. | Akhavan 2012a; Hardeman 2016; LaMancuso 2016; Stevens 2011 | Low confidence | Due to minor concerns regarding coherence, moderate concerns regarding methodological limitations and relevance, and serious concerns due to adequacy |
| 29 | Some women were concerned that their male partners would have diminished sexual attraction to them if they witnessed the birth. Likewise, some men believed that it is taboo to see a female partner give birth because of the risk of a loss of sexual interest. | Abushaikha 2013; Afulani 2018; Kululanga 2012; Pafs 2016; Sapkota 2012 | Moderate confidence | Due to minor concerns regarding methodological limitations and coherence, moderate concerns regarding relevance, and serious concerns regarding adequacy |
| 30 | Some women felt embarrassed or shy to have a male partner as a companion present throughout labour and childbirth. | Abushaikha 2013; Afulani 2018; Alexander 2014; Sapkota 2012 | Low confidence | Due to minor concerns regarding methodological limitations and coherence, moderate concerns regarding relevance, and serious concerns regarding adequacy |
| 31 | Women who did not have a companion may view the lack of support as a form of suffering, stress and fear that made their birth experience more challenging. These women detailed experiences of poor quality of care that included mistreatment, poor communication, and neglect that made them feel vulnerable and alone. | Afulani 2018; Alexander 2014; Campero 1998; Chadwick 2014; Fathi 2017; Khresheh 2010; Pafs 2016 | Moderate confidence | Due to minor concerns regarding methodological limitations and coherence, and moderate concerns regarding relevance and adequacy |
| 32 | Some women described having their male partners present as an essential part of the birth process, which facilitated bonding between the father and the baby, the couple, and as a family. | Abushaikha 2012; Bondas‐Salonen 1998; Price 2007 | Low confidence | Due to minor concerns regarding methodological limitations and coherence, moderate concerns regarding relevance, and serious concerns regarding adequacy |
| 33 | Most women who had a doula present described doulas as motherly, sisterly, or like family, suggesting a high level of relational intimacy. | Berg 2006; Coley 2016; Hunter 2012; Koumouitzes‐Douvia 2006; McGarry 2016 | Low confidence | Due to minor concerns regarding coherence, moderate concerns regarding methodological limitations and adequacy, and serious concerns regarding relevance |
| Male partners' experiences | ||||
| 34 | Male partners had three main motivations for acting as a labour companion for their female partner: curiosity, woman’s request, and peer encouragement, and were in agreement that ultimately it should be the woman’s choice about who is allowed to be present. | Bondas‐Salonen 1998; Chapman 1990; Kululanga 2012; Longworth 2011; Pafs 2016; Sapkota 2012; Somers‐Smith 1999 | Moderate confidence | Due to minor concerns regarding methodological limitations, coherence, and relevance, and moderate concerns regarding adequacy |
| 35 | Men who acted as labour companions for their female partners felt that their presence made a positive impact on themselves as individuals. | Kululanga 2012; Sapkota 2012 | Low confidence | Due to minor concerns regarding methodological considerations and coherence, and serious concerns regarding relevancy and adequacy |
| 36 | Men who acted as labour companions for their female partners felt that their presence made a positive impact on their relationship with their female partner and the new baby. | Dodou 2014; Kululanga 2012; Sapkota 2012 | Low confidence | Due to minor concerns regarding methodological considerations and coherence, and serious concerns regarding relevancy and adequacy. |
| 37 | Men who acted as labour companions for their female partners may feel scared, anxious or helpless when witnessing their partners in pain during labour and childbirth. | Fathi 2017; Kaye 2014; Kululanga 2012; Sapkota 2012 | Low confidence | Due to minor concerns regarding methodological considerations and coherence, and serious concerns regarding relevancy and adequacy. |
| 38 | Some lay companions (both male and female) were deeply impacted by witnessing a woman's pain during labour. Observing this pain caused feelings of frustration and fear, as they felt that there was nothing that they could do to help alleviate their pain. | Abushaikha 2013; Chandler 1997; Chapman 1990; Fathi 2017; Kabakian‐Khasholian 2015; Kululanga 2012; Sapkota 2012 | Moderate confidence | Due to minor concerns regarding coherence and relevance, and moderate concerns regarding methodological limitations and adequacy |
| 39 | Some male partners felt that they were not well integrated into the care team or decision‐making. These men felt that their presence was tolerated by healthcare providers, but was not a necessary role. They relied on cues from the woman and healthcare provider for when and how to give support, but were often afraid to ask questions to avoid being labelled as difficult. | Bäckström 2011; Chandler 1997; Kaye 2014; Kululanga 2012; Longworth 2011; Somers‐Smith 1999 | Moderate confidence | Due to minor concerns regarding coherence, and moderate concerns regarding methodological limitations, relevance, and adequacy |
| Doulas’ experiences | ||||
| 40 | Doulas often met with women, and sometimes their partners, prior to the birth to establish a relationship with them. This helped to manage expectations, and mentally and physically prepare the woman and her partner for childbirth. | Akhavan 2012b; Berg 2006; Coley 2016; Darwin 2016; Koumouitzes‐Douvia 2006; Lundgren 2010; Shlafer 2015; Stevens 2011; Torres 2015 | Moderate confidence | Due to minor concerns regarding coherence and adequacy, and moderate concerns regarding methodological limitations and relevance |
| 41 | Doulas believed that one of their key responsibilities was to build rapport and mutual trust with the woman, in order to improve her birth experience. This relationship was foundational for the doulas to give effective support, and for the women to feel comfortable enough to let go. Doulas built rapport by communicating, providing practical support, comforting and relating to the woman. | Berg 2006; Coley 2016; de Souza 2010; Gilliland 2011; Hunter 2012; Koumouitzes‐Douvia 2006; McGarry 2016; Shlafer 2015; Thorstensson 2008 | Moderate confidence | Due to minor concerns regarding coherence and adequacy, and moderate concerns regarding methodological limitations and relevance |
| 42 | Doulas found that the experience of providing support to women in labour could have a positive personal impact on themselves. Some found that acting as a doula built their self‐confidence, made them feel like they were making a difference, and provided a sense of fulfilment. | Hardeman 2016; Hunter 2012; McGarry 2016; Thorstensson 2008 | Low confidence | Due to minor concerns regarding coherence, moderate concerns regarding methodological limitations, and serious concerns regarding relevance and adequacy |
Background
Women have traditionally been attended to by a companion throughout labour and childbirth, but initiatives to increase the number of women giving birth in health facilities have not necessarily respected this tradition. A Cochrane systematic review of interventions concluded that having a labour companion improves outcomes for women, yet this basic, inexpensive intervention is far from universal (Bohren 2017). There is also a global interest in improving the quality of maternal and newborn care, including to “initiate, support and sustain programs designed to improve the quality of maternal health care” (World Health Organization 2014a). This includes a strong focus on respectful care as an essential component of quality of care (World Health Organization 2018). The presence of a labour companion is therefore regarded as an important aspect of improving quality of care during labour and childbirth. In addition to influencing women’s satisfaction with care, providing labour companionship may also influence the social dynamic between the woman and the healthcare provider, including behaviours that could be classified as mistreatment during childbirth.
Following a technical meeting held at the World Health Organization in August 2015, it was noted that implementation of labour companionship may be hampered by a lack of understanding of the factors affecting successful implementation, especially in low‐ and middle‐income countries (LMICs). In these settings, qualitative research on labour companionship could provide more in‐depth understanding of factors influencing effective implementation, including shedding light on:
the differences in the nature, degree, acceptability and contextual operation of labour companionship provided by professional labour companions when compared to lay labour companions;
characteristics and features of labour companionship in settings where it is working well and less well, including barriers and facilitators to implementation and sustainability;
women’s perceptions and experiences of labour companionship;
partners’ or other community members’ perceptions and experiences of labour companionship; and
healthcare providers’ perceptions and experiences of labour companionship.
Description of the topic
In the Bohren 2017 intervention review, continuous support is defined as “continuous presence and support during labour and birth”. The person providing the support could have qualifications as a healthcare professional (nurse, midwife), training as a doula or childbirth educator, or be a family member, spouse/partner, friend or stranger with little or no special training in labour support” (Bohren 2017). The terminology of 'continuous support' has been used to describe this type of intervention since the first version of Bohren 2017 was published in 2003, and through six review updates.
In this qualitative evidence synthesis, we use the term 'labour companionship' to describe support provided to a woman during labour and childbirth, in order to cover the full spectrum of contexts and situations in which women may be accompanied and supported during labour. For example, in certain settings, labour companionship may not be allowed 'continuously' throughout labour and childbirth, but may be allowed 'intermittently' (e.g. during labour but not during the birth). In this qualitative evidence synthesis, the person providing labour companionship may be any of the people described in Bohren 2017, including a healthcare professional, doula, childbirth educator, family member, spouse/partner, friend or stranger. For the purposes of this synthesis, a doula refers to a “trained professional who provides continuous physical, emotional and informational support to a mother before, during and shortly after childbirth to help her achieve the healthiest, most satisfying experience possible” (DONA International, 2018). A 'lay companion' refers to a person supporting a woman throughout labour and childbirth who is not a healthcare provider, doula or other trained professional. In practice, a 'lay companion' typically refers to a woman’s partner, family member, or friend.
In many high‐income settings, a woman’s partner, family members, or friends may be encouraged to accompany her throughout her labour and childbirth. In settings where a woman has a private labour suite, she may be able to have several people supporting her through labour and childbirth. She may also be able to hire a doula to provide additional support. In contrast, health facilities in LMICs or other contexts that prioritise the medicalisation of childbirth may not allow women to have a support person present in the labour ward. In these settings, there also may not be one‐to‐one maternity care models. Thus, women may typically go through labour and childbirth without supportive care from either a lay companion or a healthcare professional.
Why is it important to do this synthesis?
The Bohren 2017 intervention review measured the effectiveness of continuous support during labour, from 26 studies involving 15,858 women in 17 different countries. Women allocated to continuous support were more likely to have a spontaneous vaginal birth (average risk ratio (RR) 1.08, 95% confidence interval (CI) 1.04 to 1.12; 21 studies, 14,369 women; low‐quality evidence); and less likely to:
report negative ratings of or feelings about their childbirth experience (average RR 0.69, 95% CI 0.59 to 0.79; 11 studies, 11,133 women; low‐quality evidence);
use any intrapartum analgesia (average RR 0.90, 95% CI 0.84 to 0.96; 15 studies, 12,433 women);
have a caesarean birth (average RR 0.75, 95% CI 0.64 to 0.88; 24 studies, 15,347 women; low‐quality evidence);
have an instrumental vaginal birth (RR 0.90, 95% CI 0.85 to 0.96; 19 studies, 14,118 women),
have regional analgesia (average RR 0.93, 95% CI 0.88 to 0.99; 9 studies, 11,444 women); and
have a baby with a low five‐minute Apgar score (RR 0.62, 95% CI 0.46 to 0.85; 14 studies, 12,615 women).
In addition, their labours were shorter (mean difference (MD) −0.69 hours, 95% CI −1.04 to −0.34; 13 studies, 5429 women; low‐quality evidence). Bohren 2017 was not able to combine data from two studies for postpartum depression included in the review due to differences in women, hospitals and care providers. There was no apparent impact on other intrapartum interventions, maternal or neonatal complications, such as admission to special care nursery (average RR 0.97, 95%CI 0.76 to 1.25; 7 studies, 8897 women; low quality evidence), and exclusive or any breastfeeding at any time point (average RR 1.05, 95% CI 0.96 to 1.16; 4 studies, 5584 women; low‐quality evidence; Bohren 2017).
While Bohren 2017 concluded that providing continuous support to women was promising to improve women’s birth experiences and clinical outcomes, implementation of this intervention remains substandard. The level of organisation and support required to restructure maternity services to allow the presence of companions is complex and requires a better understanding of the factors that may influence success and sustainability. Understanding the values, preferences, and knowledge of key stakeholders, as well as the feasibility and applicability of the intervention for diverse contexts and health systems is critical for successful implementation. Bohren 2017 was not designed to answer these types of questions; thus it has been acknowledged that a qualitative evidence synthesis could address these questions and better understand factors that may affect implementation. Synthesising the qualitative evidence can allow us to explore similarities and differences across contexts, and better understand how the structure and components of the intervention may influence health and well‐being outcomes.
A previous literature review by Kabakian‐Khasholian 2017 synthesised factors affecting implementation of continuous support from the studies included in the 2013 version of Bohren 2017 (Hodnett 2013), and supplemented with 10 qualitative studies conducted alongside the studies. We believed that in addition to the 10 qualitative studies conducted alongside the studies, that there would be meaningful qualitative evidence on labour companionship conducted outside of the context of a study. Therefore, we decided to search for qualitative studies that explored labour companionship either alongside or outside of the context of a study.
This review is one of a series of reviews that aimed to inform the World Health Organization’s (WHO) “Recommendations for intrapartum care for a positive childbirth experience” World Health Organization 2018. Labour companionship is recommended in four WHO guidelines World Health Organization 2012; World Health Organization 2014b; World Health Organization 2015; World Health Organization 2018.
Objectives
The overall objective of the review is to describe and explore the perceptions and experiences of women, their partners, community members, healthcare providers and administrators, and other key stakeholders regarding labour companionship. The review has the following objectives:
to identify women’s, partners’, community members’, healthcare providers’ and administrators’, and other key stakeholders’ perceptions and experiences regarding labour companionship in health facilities;
to identify factors affecting successful implementation and sustainability of labour companionship; and
to explore how the findings of this review can enhance understanding of the related Cochrane systematic review of interventions (Bohren 2017).
Methods
Criteria for considering studies for this synthesis
Types of studies
We included primary studies that used qualitative methods for data collection (e.g. interviews, focus group discussions, observations), and that used qualitative methods for data analysis (e.g. thematic analysis, grounded theory). We excluded primary studies that collected data using qualitative methods but did not perform a qualitative analysis (e.g. open‐ended survey questions where responses are analysed using descriptive statistics). We included mixed‐methods studies when it was possible to extract data resulting from qualitative methods. Qualitative studies did not need to be linked to effectiveness studies included in the related Cochrane Review (Bohren 2017), and did not need to be linked to an intervention.
Topic of interest
The phenomena of interest in this review are the perceptions and experiences of labour companionship during childbirth in health facilities, of women, partners, community members, healthcare providers and administrators, and other key stakeholders. This includes factors that may influence the feasibility, acceptability and sustainability of implementing a labour companionship intervention.
We included studies that focused on the perceptions and experiences of:
women, including those who have had an experience of labour companionship and those who have not;
partners or other community members who have provided labour support or could potentially provide labour support in the future;
all cadres of healthcare providers (e.g. doctors, nurses, midwives, lay health workers, doulas) who are involved in providing healthcare services to women; and
other relevant stakeholders involved in providing or organising care, including administrators and policy‐makers.
We included studies of labour companionship in any country and in any type of health facility (e.g. health clinics, hospitals, midwife‐led clinics). We were able to potentially include studies published in English, French, Spanish, Turkish, and Norwegian, based on the language abilities of the review team. Additional languages will be included in future updates of this review if we can identify appropriate translators.
Search methods for the identification of studies
Electronic searches
We searched the following electronic databases for eligible studies from inception to 9 September 2018:
MEDLINE Ovid
CINAHL EbscoHost; and
POPLINE K4Health.
We developed search strategies using guidelines developed by the Cochrane Qualitative Research Methods Group for searching for qualitative evidence (Noyes 2011; see Appendix 1 for the search strategies). We chose these databases as we anticipated that they would provide the highest yield of relevant results based on preliminary, exploratory searches. There were no language, date or geographic restrictions for the search.
Searching other sources
In addition to database searching, we searched references of all included studies and other key references, e.g. references identified in Bohren 2017. We used OpenGrey (www.opengrey.eu) to search for relevant grey literature. We contacted key researchers working in the field for additional references or unpublished materials.
Data collection, management and synthesis
Selection of studies
We exported titles and abstracts identified through the database searches to EndNote, and removed duplicates. Two independent review authors assessed each record for eligibility for inclusion according to predefined criteria. We excluded references that did not meet the inclusion criteria.
We retrieved full‐text articles for studies included after title and abstract screening. Two independent review authors assessed each full text for eligibility for inclusion according to predefined criteria. We resolved any disagreements between review authors through discussion or by involving a third review author. If necessary, we contacted study authors for more information to determine study eligibility.
Translation of languages other than English
For studies that were not published in a language that could be understood by the review authors (e.g. in languages other than English, French, Spanish, Turkish and Norwegian), the abstract was subject to initial translation through open source software (Google Translate). If this indicated inclusion, then we sought support through our research networks to translate the full text. Where this was not possible, we listed the study as awaiting classification to ensure transparency in the review process (see Characteristics of studies awaiting classification).
Data extraction
We extracted data from the included studies using an Excel form designed for this review. This form included information about the study setting, sample characteristics, objectives, guiding framework, study design, data collection and analysis methods, qualitative themes, qualitative findings, supporting quotations, conclusions, and any relevant tables, figures or images.
Management and synthesis
We used a thematic synthesis approach, as described by Thomas and Harden (Thomas 2008). Thematic synthesis is a useful approach to analyse data from qualitative evidence syntheses exploring people’s perspectives and experiences, acceptability, appropriateness, and factors influencing implementation (Thomas 2008). This is comprised of familiarisation with and immersion in the data, free line‐by‐line coding of the findings of primary studies, organisation of free codes into related themes and development of descriptive themes, and development of analytical themes and interpretations to generate further concepts, understandings and hypotheses (Thomas 2008). We used a modified SURE framework (SURE Collaboration 2011), as an a priori framework to help identify and categorise barriers and facilitators to implementing labour companionship as an intervention (Glenton 2013). The SURE framework provided us with a comprehensive list of factors that could influence the implementation of labour companionship, and helped to integrate the findings of this synthesis with the related Cochrane systematic review of interventions, Bohren 2017. The review authors selected an article that was highly relevant to the review question, and used this article as the basis for the code list, complemented by elements of the SURE framework. First, we structured the codes as 'free' codes with no established link between them. Then we tested these codes on a further three articles, to determine if and how well the concepts translated from one study to another. This further developed the codebook, and we added new codes as necessary. The review authors sought similarities and differences between the codes and grouped the codes according to a hierarchical structure. As new codes arose throughout the analysis process, we revisited studies already coded to determine if the new codes applied or not. Two review authors coded the data, and worked as a team to generate analytical themes. We coded included studies using Atlas.ti software. This facilitated the analysis as the review team developed primary document families to organise groups of studies based on common attributes. We also used it to restrict code‐based searches, to filter coding outputs and to assist in subgroup analyses. For example, primary document families included: type of participant (midwife, doctor, healthcare administrator, woman); geographical location (regional and country‐specific); country income level (high, middle, low); type of labour companion described (doula, health worker, companion of choice, family member, partner); and type of qualitative study (associated with an intervention or stand‐alone study). This allowed the review team to hypothesise what factors shape the perceptions and experiences of women, healthcare providers and administrators.
Assessment of the methodological limitations in included studies
To be eligible for inclusion in this review, studies must have used qualitative methods for data collection and data analysis. We used an adaptation of the CASP tool (www.casp‐uk.net to appraise the quality of included studies, and included the following domains: aims, methodology, design, recruitment, data collection, data analysis, reflexivity, ethical considerations, findings, and research contribution. Two independent review authors critically appraised the included studies using this form. We resolved any disagreements between review authors through discussion or by involving a third review author. Critical appraisal is a component of the assessment of confidence for each review finding; we did not use critical appraisal as a basis for exclusion.
Assessment of confidence in the synthesis findings
We used the CERQual (Confidence in the Evidence from Reviews of Qualitative research) approach to assess our confidence in the review findings (Colvin 2018; Glenton 2018; Lewin 2018a; Lewin 2018b; Munthe‐Kaas 2018; Noyes 2018). This approach, building on the GRADE approach (Schünemann 2017), and the Cochrane tool for assessing risk of bias (Higgins 2017), for Cochrane systematic reviews of interventions, is becoming the standard to assess confidence in the findings from qualitative evidence syntheses (Ames 2017; Bohren 2015a; Colvin 2013; Lewin 2015; Munabi‐Babigumira 2017; Odendaal 2015).The CERQual approach assesses the following four concepts (Lewin 2018a).
Methodological limitations of included studies: the extent to which there are concerns about the design or conduct of the primary studies that contributed evidence to an individual review finding. Confidence in a finding may be lowered by substantial methodological limitations.
Coherence of the review finding: an assessment of how clear and cogent the fit is between the data from the primary studies and the review finding that synthesises the data. 'Cogent' refers to a well‐supported or compelling fit. Variations in data across the included studies without convincing and cogent explanations may lower the confidence in a review finding.
Adequacy of the data contributing to a review finding: an overall determination of the degree of richness and quantity of data supporting a review finding. Confidence in a finding may be lowered if a finding is supported by results from only one or a few of the included studies, or when the data supporting a finding are very thin.
Relevance of the included studies to the review question: the extent to which the body of evidence from the primary studies supporting a review finding is applicable to the context (perspective or population, phenomenon of interest, setting) specified in the review question. Confidence in a finding may be lowered when contextual issues in a primary study used to support a review finding are different to the context of the review question.
The above assessments resulted in an assessment of the overall confidence in each review finding as high, moderate, low or very low. Qualitative review findings and CERQual assessments are presented in Table 1, and as a more detailed evidence profile in Appendix 2 that summarises the finding, overall confidence assessment, and rationale for assessment of each finding.
Summary of qualitative findings table
Our findings are presented in the 'Summary of qualitative findings' table. The table provides an assessment of confidence in the evidence, as well as an explanation of this assessment, based on the GRADE‐CERQual approach (Lewin 2018a; Lewin 2018b).
Linking the synthesised qualitative findings to a Cochrane intervention review
One of the objectives of this qualitative evidence synthesis was to better explain and contextualise the findings from the related Cochrane systematic review of interventions, Bohren 2017, and potentially identify hypotheses for future subgroup analyses. We conducted this qualitative evidence synthesis in parallel to the update of Bohren 2017, but we have presented the methods and results as an independent review. Integrating findings from intervention and qualitative reviews is an emerging methodological area, and there are no agreed methods for how to conduct this type of analysis. We used two methods to integrate the synthesised qualitative findings with the Cochrane intervention review: a logic model and a matrix model.
Logic model
We used methods similar to other Cochrane Reviews (see Glenton 2013), to develop a logic model to link qualitative findings for labour companionship to outcomes described in the intervention review, Bohren 2017. The aim of this logic model was not necessarily to demonstrate causal links between elements of the intervention or programme and health and well‐being outcomes. Rather, we used the logic model to depict theories and assumptions about the links, based on the evidence in both reviews and more broadly. We depicted the logic model as a logical flow from components of the labour companionship programme, to intermediate or process outcomes, and resulting in longer‐term health and well‐being outcomes identified in Bohren 2017. Two review authors (MAB and ÖT) reviewed the 'Summary of qualitative findings' table and organised these findings into logical chains of events that may lead to the outcomes reported in Bohren 2017. First, we categorised each finding from the qualitative synthesis and outcome from Bohren 2017 as either:
a component of the companionship programme (qualitative evidence synthesis);
an Intermediate or process outcome (qualitative evidence synthesis);
longer‐term health and well‐being outcomes (Bohren 2017 and qualitative evidence synthesis); or
a moderator (positive or negative), that could influence the relationship between a programme component and intermediate, process, or longer‐term outcomes (qualitative evidence synthesis).
We used an iterative process to develop the chains of events, and in some cases, we used imputation to categorise the findings and outcomes as components, outcomes, and moderators. We sometimes rephrased 'negative' qualitative findings as 'positive' findings for the programme components and intermediate or process outcomes to create a more logical flow. For example, one qualitative finding found that women and providers often were unaware of the benefits of labour companionship, but we rephrased the programme component as, “train women and providers on the benefits of companionship”. To improve transparency of this process, within the logic model, the numbers in parentheses refer to the reference number of the relevant finding from the 'Summary of qualitative findings' table.
Matrix model
We used a matrix‐model approach similar to Candy 2011 and Ames 2017. Two authors (MAB and ÖT) used a matrix‐model approach to create a comparative table that explored whether the interventions included in the related Cochrane systematic review of interventions (Bohren 2017), contained the features of labour companionship that women, partners and providers identified as important in the qualitative evidence synthesis. To create the matrix, we first reviewed the 'Summary of qualitative findings' table to identify the features of labour companionship that key stakeholders viewed as important moderators (positive or negative). We organised these features into groups and developed seven questions reflecting these issues. Each question could be answered as yes, no, not reported or not applicable, to reflect whether this feature of companionship was addressed in the intervention.
Were providers trained on the benefits of labour companionship prior to implementation?
Were women educated about the benefits of labour companionship prior to implementation?
Was the labour ward structured or restructured in a way to ensure that privacy can be maintained for all women?
Were providers trained on how to integrate companions into the care team?
Were clear roles and expectations set for companions and providers?
For studies with lay companions, was training for companions on how to support women integrated into antenatal care?
Did the woman choose her own companion?
We created a table listing the seven questions and assessed whether the studies included Bohren 2017 reflected these features.
Review author reflexivity
The perspectives of the review authors regarding subject expertise, employment, perspectives of labour companionship, and other background factors may affect the manner in which we collect, analyse and interpret the data. At the outset of this review, all review authors believed that labour companionship was valuable to improve women’s experiences of care, but that critical barriers exist to successful implementation of labour companionship, particularly in LMICs. In many contexts of childbirth in health facilities, the provision of clinical procedures and assessments is considered the pinnacle of care, and women’s experiences of care, including labour companionship and respectful care, are deprioritised. To minimise the risk that our perspectives as authors influence the analysis and interpretation, we used refutational analysis techniques, such as exploring and explaining contradictory findings between studies. We accounted for these differences, and any other issues that may have contributed to the interpretation of the review findings, by describing it in a 'Reflexivity' section when publishing the protocol and full review.
Results
Results of the search
We identified 52 papers from 51 studies published on or before 9 September 2018 that fulfilled the inclusion criteria and are included in this synthesis. Figure 1 depicts the flow of studies.
1.
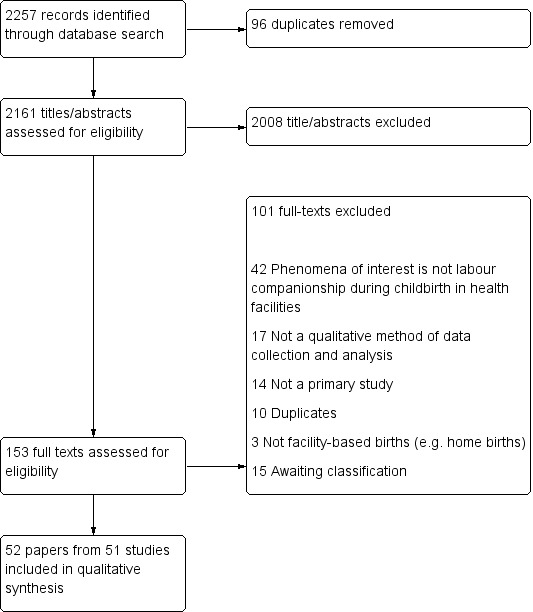
Study flow diagram
Description of studies
Study participants
Participants in the included studies included a mix of perspectives of women, healthcare providers (midwives, nurses, and doctors), male partners, and doulas (note: no studies included the perspectives of women or partners in non‐heterosexual relationships). Fifteen of the included studies were from the perspectives of women only, four were healthcare providers only, 10 were male partners only, five were doulas only, and 18 were mixed perspectives. The Characteristics of included studies outlines the type of participants and study design for each included study.
Type of labour companion and model of care
Different types of companions supported women at different times throughout pregnancy and childbirth. Twenty‐seven of the included studies had lay companions providing support to women, which was typically a male partner (18 studies: Abushaikha 2012; Abushaikha 2013; Afulani 2018; Alexander 2014; Bäckström 2011; Bondas‐Salonen 1998; Chandler 1997; Chapman 1990; Harte 2016; Kaye 2014; Kululanga 2012; Ledenfors 2016; Longworth 2011; Pafs 2016; Premberg 2011; Qian 2001; Sapkota 2012; Somers‐Smith 1999), a female companion such as a sister, mother, mother‐in‐law, or friend ( studies: Afulani 2018; Alexander 2014; Fathi 2017; Harte 2016; Kabakian‐Khasholian 2015; Khresheh 2010). Five studies specified that the lay companion was anyone who the woman chose (Brüggemann 2014) or did not specify who the lay companion was (Dodou 2014; Maher 2004; Price 2007; Shimpuku 2013). Twenty‐three of the included studies described support provided by doulas (Akhavan 2012a; Akhavan 2012b; Berg 2006; Campero 1998; Coley 2016; Darwin 2016; de Souza 2010; Gentry 2010; Gilliland 2011; Hardeman 2016; Horstman 2017; Hunter 2012; Koumouitzes‐Douvia 2006; Lagendyk 2005; LaMancuso 2016; Lundgren 2010; McGarry 2016; McLeish 2018; Schroeder 2005; Shlafer 2015; Stevens 2011; Torres 2013; Torres 2015). One included study (Thorstensson 2008), described support provided to women by female student midwives whose sole responsibility was to provide continuous support (e.g. no concurrent clinical responsibilities). Two included studies described women’s desire to have companionship from a male partner, friend or relative, and the experience of lacking this type of support (Afulani 2018; Chadwick 2014).
Thirty‐eight of the included studies described companionship provided only during labour and childbirth, for example, from admission to the health facility for labour, throughout childbirth and early postpartum periods (Abushaikha 2012; Abushaikha 2013; Afulani 2018; Akhavan 2012a; Akhavan 2012b; Alexander 2014; Bäckström 2011; Bondas‐Salonen 1998; Brüggemann 2014; Campero 1998; Chadwick 2014; Chandler 1997; Chapman 1990; Dodou 2014; de Souza 2010; Fathi 2017; Gilliland 2011; Hardeman 2016; Harte 2016; Horstman 2017; Kabakian‐Khasholian 2015; Kaye 2014; Khresheh 2010; Kululanga 2012; LaMancuso 2016; Ledenfors 2016; Longworth 2011; Lundgren 2010; Maher 2004; Pafs 2016; Premberg 2011; Price 2007; Qian 2001; Sapkota 2012; Shimpuku 2013; Shlafer 2015; Somers‐Smith 1999; Thorstensson 2008). Twelve of the included studies described an extended model of companionship with doulas, that included support during the pregnancy and/or postpartum periods (Berg 2006; Coley 2016; Darwin 2016; Gentry 2010; Hunter 2012; Lagendyk 2005; McGarry 2016; McLeish 2018; Schroeder 2005; Stevens 2011; Torres 2013; Torres 2015). One study did not specify the timing of doula support (Koumouitzes‐Douvia 2006).
Most studies did not have a description of the background or training doulas had in order to practice. Only six studies described doula training or certification programmes (Coley 2016; Lagendyk 2005; Lundgren 2010; McGarry 2016; McLeish 2018; Shlafer 2015), which varied across contexts. Doulas in a study conducted by Lundgren 2010 in Sweden met seven times for a course about birth and breastfeeding. Lagendyk 2005 described training for doulas working in both a hospital and community setting in Canada. In the hospital setting, doulas completed an unspecified certified doula training course for 14 hours and attended an unspecified number of births with a more experienced doula (Lagendyk 2005). In the community setting, doulas completed a 12‐hour training course and attended two births with an experienced volunteer (Lagendyk 2005). A study on doula support for incarcerated women by Shlafer 2015 in the USA describes that doulas were trained and certified by DONA International, as well as receiving additional training by the Department of Corrections, Human Subject Research, and 14 hours of continuing education per year. In the UK, McGarry 2016 described that doulas undertook training and mentoring through a website (www.doulatraining.org), worked alongside a mentor for six months to two years, attended a minimum of four births, and passed a formal assessment interview. Coley 2016 described a process where volunteers participated in training certified by DONA International and participated in three births in the USA. McLeish 2018 described a 90‐hour training programme for doulas that led to accredited qualification, in addition to ongoing support and supervision from a project co‐ordinator.
Setting
Five studies were conducted in five low‐income countries: Uganda (Kaye 2014), Malawi (Kululanga 2012), Rwanda (Pafs 2016), Nepal (Sapkota 2012), and Tanzania (Shimpuku 2013). Thirteen studies were conducted in 11 middle‐income countries: Syria (Abushaikha 2012; Abushaikha 2013), Ghana (Alexander 2014), Brazil (Brüggemann 2014; Dodou 2014; de Souza 2010), Mexico (Campero 1998), South Africa (Chadwick 2014), , Jordan (Khresheh 2010), Kenya (Afulani 2018), Iran (Fathi 2017), and China (Qian 2001); and one multi‐country study conducted in Syria, Egypt and Lebanon (Kabakian‐Khasholian 2015). Thirty‐three studies were conducted in six high‐income countries: Sweden (Akhavan 2012a; Akhavan 2012b; Bäckström 2011; Berg 2006; Ledenfors 2016; Lundgren 2010; Premberg 2011; Thorstensson 2008), Finland (Bondas‐Salonen 1998), Canada (Chandler 1997; Lagendyk 2005; Price 2007), USA (Chapman 1990; Coley 2016; Gentry 2010; Hardeman 2016; Horstman 2017; Hunter 2012; Koumouitzes‐Douvia 2006; LaMancuso 2016; Schroeder 2005; Shlafer 2015; Torres 2013; Torres 2015), United Kingdom (Darwin 2016; Longworth 2011; McGarry 2016; McLeish 2018; Somers‐Smith 1999), and Australia (Harte 2016; Maher 2004; Stevens 2011), and one multi‐country study conducted in the USA and Canada (Gilliland 2011). Of the 33 studies conducted in high‐income countries, 21 studies focused on doula models of companionship (Akhavan 2012a; Akhavan 2012b; Berg 2006; Coley 2016; Darwin 2016; Gentry 2010; Gilliland 2011; Hardeman 2016; Horstman 2017; Hunter 2012; Koumouitzes‐Douvia 2006; Lagendyk 2005; LaMancuso 2016; Lundgren 2010; McGarry 2016; McLeish 2018; Schroeder 2005; Shlafer 2015; Stevens 2011; Torres 2013; Torres 2015).
Seven studies were conducted in Africa (Afulani 2018; Alexander 2014; Chadwick 2014; Kaye 2014; Kululanga 2012; Pafs 2016; Shimpuku 2013); two in Asia (Qian 2001; Sapkota 2012); 14 in Europe (Akhavan 2012a; Akhavan 2012b; Bäckström 2011; Berg 2006; Bondas‐Salonen 1998; Darwin 2016; Ledenfors 2016; Longworth 2011; Lundgren 2010; McGarry 2016; McLeish 2018; Premberg 2011; Somers‐Smith 1999; Thorstensson 2008); five in the Middle East (Abushaikha 2012; Abushaikha 2013; Fathi 2017; Kabakian‐Khasholian 2015; Khresheh 2010); 17 in North America (Campero 1998; Chandler 1997; Chapman 1990; Coley 2016; Gentry 2010; Gilliland 2011; Hardeman 2016; Horstman 2017; Hunter 2012; Koumouitzes‐Douvia 2006; Lagendyk 2005; LaMancuso 2016; Price 2007; Schroeder 2005; Shlafer 2015; Torres 2013; Torres 2015); three in South America (Brüggemann 2014; Dodou 2014; de Souza 2010); and three in Oceania (Harte 2016; Maher 2004; Stevens 2011).
Thirteen studies were conducted alongside an intervention or as an evaluation of an intervention or programme (Akhavan 2012a; Akhavan 2012b; Campero 1998; Coley 2016; Darwin 2016; Gentry 2010; Kabakian‐Khasholian 2015; Khresheh 2010; Lagendyk 2005; LaMancuso 2016; McGarry 2016; Schroeder 2005; Shlafer 2015), and 39 studies were stand‐alone qualitative studies (not attached to an intervention, evaluation, or programme).
Critical appraisal of included studies
Detailed critical appraisals can be found in Appendix 3. Fifty‐one of the included studies were published in peer‐reviewed journals, which might impose word limits that are not well suited for comprehensively reporting qualitative research (one included study is a full doctoral dissertation (Chapman 1990)). Across all studies, there was generally poor reporting of recruitment strategies, researcher reflexivity, healthcare context, and data analysis methods. All studies had at a minimum a brief description about the participants, sampling, data collection and analysis methods. Most studies used interviews or focus group discussions, with only a few studies using other qualitative methods of data collection such as participant observation. Reviewer concerns regarding a lack of rich data and thick description of study methodology (depth and breadth) may be attributed to word limits set by journals.
Confidence in the findings
Out of 42 review findings, we used the CERQual approach to grade seven review findings as high confidence, 18 as moderate confidence, and 17 as low or very low confidence (Table 1). The explanation for each CERQual assessment is shown in the evidence profile in Appendix 2.
Themes and findings identified in the synthesis
From the thematic synthesis, we developed 10 overarching themes, which we organised under three domains using the following structure:
-
Factors affecting implementation
Awareness‐raising among healthcare providers and women
Creating an enabling environment
Training, supervision and integration with care team
-
Companion roles
Informational support
Advocacy
Practical support
Emotional support
-
Experiences of companionship
Women’s experiences
Male partners’ experiences
Doulas’ experiences
We explore each review finding under these themes and domains in depth in the following sections. At the end of the results section, we bring together the results of this qualitative evidence synthesis and the related Cochrane systematic review of interventions (Bohren 2017).
Findings
In the sections below, we report each review finding and provide a link to the CERQual evidence profile table supporting the assessment of confidence in that finding (Appendix 2). For each finding, we start with a short, overall summary and then present the detailed results.
Factors affecting implementation
Awareness‐raising among healthcare providers and women
Finding 1
The benefits of labour companionship may not be recognised by providers, women, or their partners (moderate confidence; Abushaikha 2013; Afulani 2018; Alexander 2014; Brüggemann 2014; Coley 2016; Pafs 2016). Some providers viewed companionship as a low priority in their setting because of the lack of clear benefit to the woman (Brüggemann 2014). Some women and male partners believed that the partner was unable to do anything to help the woman during labour (Abushaikha 2013; Alexander 2014). When potential tasks or responsibilities for the labour companion were identified (e.g. holding her hand, rubbing her back, encouraging her), it was perceived that this was the role of the clinical staff or that the woman could persevere without this support (Abushaikha 2013; Alexander 2014; Coley 2016).
Finding 2
Labour companionship was sometimes viewed as non‐essential or less important compared to other aspects of care, and therefore deprioritised due to limited resources to spend on 'expendables' (low confidence; Akhavan 2012b; Brüggemann 2014; Lagendyk 2005; Premberg 2011). For example, some health facilities required labour companions to wear hospital‐issued clothing, but clothing for labour companions may not always be available (Brüggemann 2014). Where labour companions were allowed, health facilities faced difficulties to provide adequate material resources, such as bed or chair space (Brüggemann 2014; Premberg 2011).
Creating an enabling environment
Finding 3
Formal changes to existing policies regarding allowing companions on the labour ward may be necessary prior to implementing labour companionship models at a facility level (low confidence; Abushaikha 2013; Kabakian‐Khasholian 2015). When policies are changed, healthcare providers of all levels should be aware of the new policies and how to comply with them in their practice (Abushaikha 2013). Policy changes should also be communicated to women and their families, in order to manage their expectations for the labour and childbirth (Abushaikha 2013; Kabakian‐Khasholian 2015).
Finding 4
In settings where companions are allowed, there can be gaps between a policy or law allowing companionship, and the actual practice of allowing all women who want companionship to have a companion present (low confidence; Brüggemann 2014; Kaye 2014). In Uganda and Brazil, not all women were allowed to have companions because of congested labour wards and concerns about privacy if the companion was male (Brüggemann 2014; Kaye 2014). In Brazil, by law, companionship is allowed for all women, but some healthcare providers may not allow the woman to have a companion present, for example if she does not have adequate insurance, if the companion appears unprepared, or because of a fear of being 'supervised' by the companion (Brüggemann 2014).
Finding 5
Providers, women and male partners highlighted physical space constraints of the labour wards as a key barrier to labour companionship as it was perceived that privacy could not be maintained and wards would become overcrowded (moderate confidence; Abushaikha 2013; Afulani 2018; Brüggemann 2014; Harte 2016; Kabakian‐Khasholian 2015; Qian 2001; Sapkota 2012; Shimpuku 2013). Labour wards often had open floor plans, possibly with only a curtain to separate beds (Abushaikha 2013; Brüggemann 2014; Kabakian‐Khasholian 2015; Qian 2001; Sapkota 2012; Shimpuku 2013). In some cases, women were allowed only to have a female companion, in order to protect the privacy of other women, thus restricting her choices (Afulani 2018; Brüggemann 2014).
Finding 6
Some providers, women and male partners were concerned that the presence of a labour companion may increase the risk of transmitting infection in the labour room (low confidence; Abushaikha 2013; Brüggemann 2014; Kabakian‐Khasholian 2015; Qian 2001). Although acknowledging that there was no evidence suggesting that companions increase the risk of spreading infection (Brüggemann 2014), it was believed that the presence of an additional non‐clinical person may threaten the sterility of the labour room (Brüggemann 2014; Abushaikha 2013; Kabakian‐Khasholian 2015; Qian 2001).
Training, supervision, and integration with care team
Finding 7
Some providers were resistant to integrate companions or doulas into maternity services, and provided several explanations for their reluctance.Providers felt that lay companions lacked purpose and boundaries, increased provider workloads, arrived unprepared, and could be in the way (high confidence; Bondas‐Salonen 1998; Brüggemann 2014; Horstman 2017; Kabakian‐Khasholian 2015; Kaye 2014; Lagendyk 2005; Torres 2013). Some providers were also concerned that they could be evaluated unfairly by companions who did not understand the physiology of birth and potential interventions (Brüggemann 2014). Doulas were not always perceived to be a contributing member of the team, and may be viewed hostilely as 'anti‐medical establishment' or as a threat to the role of midwives or nurses (Horstman 2017; Lagendyk 2005; Torres 2013).
Finding 8
In most cases, male partners were not integrated into antenatal care or training sessions before birth.Where male partners were included in antenatal preparation, they felt that they learned comfort and support measures to assist their partners, but that these measures were often challenging to implement throughout the duration of labour and birth (low confidence; Abushaikha 2013; Bondas‐Salonen 1998; Chandler 1997; Ledenfors 2016; Sapkota 2012; Somers‐Smith 1999). Male involvement during pregnancy also helped them to feel more engaged and able to participate in and interact with healthcare services (Abushaikha 2013; Bondas‐Salonen 1998; Sapkota 2012).
Finding 9
In settings where lay companionship or doula care were available, providers were not well trained on how to integrate the companion as an active or important member of the woman’s support team (moderate confidence; Bondas‐Salonen 1998; Brüggemann 2014; Kabakian‐Khasholian 2015; Kaye 2014; Lagendyk 2005; Torres 2013). This could lead to conflict between the provider, companion/doula and the woman, or feeling that the companion/doula was “in the way,” "evaluating" the provider, or "taking over" the role of the provider (Brüggemann 2014; Kabakian‐Khasholian 2015; Lagendyk 2005; Torres 2013). In contexts where there is a more technocratic or less woman‐centred model of maternity care, women’s needs (including companionship) may be deprioritised in lieu of institutional routines, further exacerbating a potential point of conflict (Brüggemann 2014).
Finding 10
Some doulas felt that they were not well integrated into decision‐making or care co‐ordination by the healthcare providers, and were sometimes ignored by healthcare providers. These doulas believed that healthcare providers assumed that doulas were working outside of the medical system, and were not considered to have valuable knowledge about a woman's labour progress (low confidence; Berg 2006; McLeish 2018; Stevens 2011; Torres 2013).
Finding 11
Most healthcare providers believed that having a lay companion support a woman throughout labour and childbirth was beneficial to the woman and worked well when companions were integrated into the model of care. However, when lay companions were not well engaged or integrated, conflict could arise as they may be perceived as an additional burden for healthcare providers to manage their presence, and provide ongoing direction and support (moderate confidence; Brüggemann 2014; Harte 2016; Kabakian‐Khasholian 2015; Khresheh 2010; Maher 2004; Qian 2001). Some healthcare providers feared that in the presence of a lay companion, women may be less likely to co‐operate with instructions or less tolerant to pain (Kabakian‐Khasholian 2015; Maher 2004; Qian 2001), and that conflict could arise between the woman and provider if companions interfered with the care process (Harte 2016; Maher 2004).
Finding 12
Most midwives believed that doulas played a collaborative role in supporting women during childbirth, and were assets to the team who provided more woman‐centred, needs‐led support.However, some midwives found it difficult to engage as carers with women when doulas were present, as they felt that doulas encroached on their carer role (low confidence; Akhavan 2012b; Lundgren 2010; McLeish 2018; Stevens 2011). This role conflict was also exacerbated when doulas provided medical advice, which midwives felt was inappropriate given their training (Stevens 2011).
Finding 13
Lay companions received little or no training on how to support the woman during labour and childbirth, which made them feel frustrated (low confidence; Kululanga 2012; Sapkota 2012). They wanted to be better included into antenatal care or birth preparation classes to learn specific ways to physically and emotionally support the woman (Kululanga 2012; Sapkota 2012).
Finding 14
Some men felt that they were actively excluded, left out, or not involved in their female partner's care. They were unsure of where they fit in to support the woman, and felt that their presence was tolerated but not necessary (moderate confidence; Bäckström 2011; Chandler 1997; Kaye 2014; Kululanga 2012; Longworth 2011; Somers‐Smith 1999). Male partners who felt conflicted about their role were unsure of the appropriate time to engage with healthcare providers to support the woman or to step back, which created a paradox for them (Bäckström 2011; Chandler 1997). These men suggested that antenatal preparation focusing on male engagement may help to manage their expectations about their involvement in the labour and childbirth process and encourage them to feel a part of the action (Kaye 2014).
Companion roles
Informational support
Finding 15
Women valued the non‐pharmacological pain relief measures that companions helped to facilitate, including a soothing touch (holding hands, massage and counter pressure), breathing and relaxation techniques (high confidence; Campero 1998; Chapman 1990; Dodou 2014; de Souza 2010; Fathi 2017; Hunter 2012; Kabakian‐Khasholian 2015; Khresheh 2010; Lundgren 2010; McLeish 2018; Sapkota 2012; Somers‐Smith 1999; Thorstensson 2008; Torres 2015). Companions provided information to women and helped them to adopt these coping measures. Companions also helped women to adopt alternative positions to ease pain, such as squatting, sitting on a ball and walking (Hunter 2012; Kabakian‐Khasholian 2015; Khresheh 2010; Sapkota 2012; Somers‐Smith 1999; Torres 2015). Some women also found comfort in spiritual support, when their companions read holy texts or prayed (Khresheh 2010; Maher 2004).
Finding 16
Doulas played an important role in providing information to women about the process of childbirth, duration of labour, and reasons for medical interventions. They bridged communication gaps between clinical staff and women, and facilitated a more actively engaged environment where women were encouraged to ask questions (moderate confidence; Akhavan 2012a; Akhavan 2012b; Berg 2006; Campero 1998; Darwin 2016; Gilliland 2011; Horstman 2017; LaMancuso 2016; McGarry 2016; McLeish 2018; Schroeder 2005; Torres 2013; Torres 2015). This helped women to better understand the process of childbirth, which helped to alleviate anxieties and confusion. Doulas were perceived to have a certain amount of clinical knowledge, and their informed counsel helped to normalise childbirth experiences, legitimise women's desires for more information, and encourage women to speak up for themselves. This type of informational support may be of particular importance for certain vulnerable groups of women, such as migrant/refugee women, or women with disabilities (Akhavan 2012a; Akhavan 2012b; LaMancuso 2016; McGarry 2016).
Finding 17
Lay companions also played a role in providing informational support to women or acting as the woman's voice during labour and childbirth. This usually took the form of acting as an intermediary by relaying, repeating or explaining information from the healthcare provider to the woman, and from the woman to the healthcare provider (moderate confidence; Alexander 2014; Bondas‐Salonen 1998; Khresheh 2010; Price 2007; Qian 2001; Sapkota 2012). This is in contrast to doulas, who women viewed as having reliable and helpful information of their own to share.
Finding 18
Companions played an important role to help facilitate communication between the woman and healthcare providers, including representing the woman's interests and speaking on her behalf when she was unable to do so. They helped to relay information between the woman and healthcare provider, such as asking questions and setting boundaries (moderate confidence; Akhavan 2012b; Bondas‐Salonen 1998; Darwin 2016; Gentry 2010; Hardeman 2016; Horstman 2017; Hunter 2012; Khresheh 2010; Koumouitzes‐Douvia 2006; LaMancuso 2016; Lundgren 2010; McGarry 2016; McLeish 2018; Premberg 2011; Price 2007; Stevens 2011; Torres 2015). Doulas often acted as interpreters, to translate cultural and individual preferences and expectations from the woman to the providers, as well as to translate medical terminology from the providers to the woman (Darwin 2016; Gentry 2010; LaMancuso 2016; McGarry 2016; Stevens 2011). This signal translation helped women to express themselves and be understood, while respecting their needs and wishes and providing them with confidence and security (Darwin 2016; Gentry 2010; LaMancuso 2016; McGarry 2016; Stevens 2011). Similarly, doulas may help to correct perceived imbalances of power between women and healthcare providers, empowering women to make decisions and express themselves (McLeish 2018).
Advocacy
Finding 19
Companions played a role to bear witness to the process of childbirth. They shared the childbirth experience with the woman by being with her, and were viewed as observers who could monitor, reflect, and report on what transpired throughout labour and childbirth, such as witnessing pain, the birth process, and the woman's transformation to motherhood (high confidence; Afulani 2018; Alexander 2014; Bondas‐Salonen 1998; Dodou 2014; Horstman 2017; Hunter 2012; Longworth 2011; Price 2007; Sapkota 2012).
Practical support
Finding 20
Companions provided physical support to women throughout labour and childbirth, such as giving them a massage and holding their hand. Companions encouraged and helped women to mobilisethroughout labour or to change positions, such as squatting or standing, and provided physical support to go to the bathroom or adjust clothing (high confidence; Afulani 2018; Chandler 1997; Chapman 1990; de Souza 2010; Fathi 2017; Hunter 2012; Kabakian‐Khasholian 2015; Khresheh 2010; Koumouitzes‐Douvia 2006; McLeish 2018; Premberg 2011; Price 2007; Sapkota 2012;Shimpuku 2013; Torres 2013). While women were pushing, companions helped support them in different positions, such as holding a leg or an arm, or stabilising her back.
Finding 21
Companions played an important role to assist healthcare providers to care for women by observing and identifying potential issues throughout labour and childbirth (moderate confidence; Akhavan 2012b; Alexander 2014; Khresheh 2010; Qian 2001; Sapkota 2012; Shimpuku 2013). In LMIC settings, where facilities may be short staffed, companions could help the healthcare provider by gathering medical supplies and helping with certain tasks when staff were too busy, such as changing soiled linens or fetching food and water (Alexander 2014; Khresheh 2010; Qian 2001; Sapkota 2012; Shimpuku 2013). In settings where midwives were more clinically‐orientated or overstretched, companions could take on the role of the supporter, allowing the midwives to focus on clinical aspects of care (Akhavan 2012b).
Finding 22
Some healthcare providers and doulas felt that doulas or lay companions could potentially address shortcomings in maternity services (very low confidence; Afulani 2018; Akhavan 2012b; Stevens 2011). For example, doulas could help provide culturally competent care (including interpretation), enhance continuity of care for the woman throughout labour, and enhance the provision of supportive care, such as massage (Akhavan 2012b; Lundgren 2010; Stevens 2011).
Emotional support
Finding 23
Women valued that companions and doulas helped to facilitate their feeling in control during labour and gave them confidence in their abilities to give birth (moderate confidence; Berg 2006; Campero 1998; Chapman 1990; Darwin 2016; Dodou 2014; Fathi 2017; Gilliland 2011; Hunter 2012; Ledenfors 2016; Price 2007; Sapkota 2012). Companions helped women to feel self‐confident and improved their self‐esteem when they acknowledged and reinforced their efforts, provided encouragement and directions to maintain control, and ensured that women were aware of their choices. This process helped women to feel that they played a more active and participatory role in their birth processes (Berg 2006; Campero 1998; Darwin 2016; Dodou 2014; Hunter 2012; Sapkota 2012). Women with companions also felt that they were more aware of their progression through labour, and were better able to draw connections between the passage of time, tolerance for pain, dilatation of the cervix, and their experience of birth (Campero 1998; Sapkota 2012; Berg 2006).
Finding 24
Companions often provided emotional support to women through the use of praise and reassurance. They acknowledged the women's efforts and concerns, and provided reinforcement through verbal encouragement and affirmations (high confidence; Abushaikha 2012; Alexander 2014; Bäckström 2011; Berg 2006; Bondas‐Salonen 1998; de Souza 2010; Fathi 2017; Gentry 2010; Gilliland 2011; Hardeman 2016; Harte 2016; Horstman 2017; Hunter 2012; Kabakian‐Khasholian 2015; Khresheh 2010; Koumouitzes‐Douvia 2006; Ledenfors 2016; Lundgren 2010; McGarry 2016; McLeish 2018; Premberg 2011; Price 2007; Sapkota 2012; Schroeder 2005; Somers‐Smith 1999; Thorstensson 2008; Torres 2013; Torres 2015). This increased women's ability to cope, empowered them by validating their experiences, and gave them the strength and confidence to progress through the process of labour. Many women felt that praise and reassurance created a safe and secure birth environment, by alleviating their fears and helping them to focus (Abushaikha 2012; Alexander 2014; Bondas‐Salonen 1998; Gilliland 2011; Hunter 2012; Khresheh 2010; Premberg 2011; Schroeder 2005; Somers‐Smith 1999; Thorstensson 2008). In some contexts, praise took a spiritual form, through prayer or reading of religious texts (Abushaikha 2012; Alexander 2014; Kabakian‐Khasholian 2015; Khresheh 2010).
Finding 25
The continuous physical presence of someone caring was an important role that companions played, particularly in settings where continuous midwifery care was not available or not practiced. The continuous presence of the companion signalled to the woman the availability of support when needed, and helped to pass the time throughout labour (moderate confidence; Abushaikha 2012; Afulani 2018; Berg 2006; Bondas‐Salonen 1998; Campero 1998; Darwin 2016; Dodou 2014; Koumouitzes‐Douvia 2006; Lundgren 2010; McLeish 2018; Price 2007; Sapkota 2012; Somers‐Smith 1999; Stevens 2011; Thorstensson 2008; Torres 2015). Continuous support contributed to a woman's sense of security, promoted a calm atmosphere, and built trust between the woman and companion (Berg 2006; Bondas‐Salonen 1998; Campero 1998; Darwin 2016; Lundgren 2010; Price 2007; Sapkota 2012; Stevens 2011; Thorstensson 2008; Torres 2015). This could contribute to a consistency of the childbirth experience, where a healthcare provider could come and go, or a woman could be referred to a different facility, but the companion would be there continuously.
Experiences of companionship
Women's experiences
Finding 26
Women stated different preferences for their desired companion, including their husband or male partner, sister, mother, mother‐in‐law, doula, or a combination of different people. Regardless of which person they preferred, women who wanted a labour companion present during labour and childbirth expressed the need for this person to be a caring, compassionate, and trustworthy advocate (high confidence; Abushaikha 2012; Afulani 2018; Akhavan 2012a; Alexander 2014; Berg 2006; Bondas‐Salonen 1998; Campero 1998; Dodou 2014; Fathi 2017; Hunter 2012; Kabakian‐Khasholian 2015; Khresheh 2010; Lundgren 2010; Pafs 2016; Price 2007; Qian 2001; Sapkota 2012; Shimpuku 2013; Somers‐Smith 1999; Torres 2015). These differences among women, both between and within populations, demonstrate the importance of giving women a choice of their companion.
Finding 27
Women described the desire for a happy and healthy birth for both themselves and their babies. Support provided by doulas and companions paved the way for them to have a positive birth experience, as the support facilitated them to feel safe, strong, confident and secure (high confidence; Abushaikha 2012; Abushaikha 2013; Akhavan 2012a; Alexander 2014; Berg 2006; Bondas‐Salonen 1998; Campero 1998; Darwin 2016; Dodou 2014; Gilliland 2011; Hunter 2012; Kabakian‐Khasholian 2015; Khresheh 2010; Koumouitzes‐Douvia 2006; Ledenfors 2016; Lundgren 2010; McGarry 2016; Price 2007; Sapkota 2012; Schroeder 2005; Torres 2015). Support also provided a human dimension of care, based on an individual woman's unique needs, which provided comfort and mitigated distress for the woman. Women described both having a positive birth experience because of the presence of companions, and that the presence of a companion was a positive experience (Akhavan 2012a; Berg 2006; Bondas‐Salonen 1998; Campero 1998; Darwin 2016; Dodou 2014; Hunter 2012; Khresheh 2010; Koumouitzes‐Douvia 2006; Ledenfors 2016; Lundgren 2010; Price 2007; Sapkota 2012; Schroeder 2005).
Finding 28
Immigrant, refugee, and foreign‐born women resettled in high‐income countries highlighted how community‐based doulas (e.g. someone from their ethnic/religious/cultural community trained as a doula) were an important way for them to receive culturally competent care (low confidence; Akhavan 2012a; Hardeman 2016; LaMancuso 2016; Stevens 2011). Community‐based doulas empowered women to ask questions, acted as the woman’s advocate, and ensured that their customs and traditions were respected (Akhavan 2012a; LaMancuso 2016; Stevens 2011). When women received this type of care, they felt more confident to give birth and less like 'outsiders' in their new community (Akhavan 2012a; LaMancuso 2016; Stevens 2011).
Finding 29
Some women were concerned that their male partners would have diminished sexual attraction to them if they witnessed the birth (Abushaikha 2013; Sapkota 2012).Likewise, some men believed that it is taboo to see a female partner give birth because of the risk of a loss of sexual interest (moderate confidence; Afulani 2018; Kululanga 2012; Pafs 2016). However, male partners who acted as labour companions did not mention feeling that they were less attracted to their partner after the birth.
Finding 30
Some women felt embarrassed or shy to have a male partner as a companion present throughout labour and childbirth (low confidence; Abushaikha 2013; Afulani 2018; Alexander 2014; Sapkota 2012). These women felt uncomfortable to have someone there to witness them in labour pains, which may result in grunting or crying, to see them naked during examinations, or to provide practical support such as cleaning up bodily fluids.
Finding 31
Women who did not have a companion may view the lack of support as a form of suffering, stress and fear that made their birth experience more challenging. These women detailed experience of poor quality of care that included mistreatment, poor communication, and neglect that made them feel vulnerable and alone (moderate confidence; Afulani 2018; Alexander 2014; Campero 1998; Chadwick 2014; Fathi 2017; Khresheh 2010; Pafs 2016). Some women without companions described feeling lonely and isolated throughout labour, and that their only contact with other people was during clinical examinations by providers (Campero 1998; Chadwick 2014).
Finding 32
Some women described having their male partners present as an essential part of the birth process, which facilitated bonding between the father and the baby, the couple, and as a family (low confidence; Abushaikha 2012; Bondas‐Salonen 1998; Price 2007). They described the male partner witnessing the birth as a unique and emotional experience that ultimately led to the creation of a family unit.
Finding 33
Most women who had a doula present described doulas as motherly, sisterly, or like family, suggesting a high level of relational intimacy (low confidence; Berg 2006; Coley 2016; Hunter 2012; Koumouitzes‐Douvia 2006; McGarry 2016). Some women believed that the experience of giving birth with a doula itself demanded the creation of a close bond as the doula was present solely to provide support to the woman during an intimate period (Berg 2006; Hunter 2012).
Male partners' experiences
Finding 34
Male partners had three main motivations for acting as a labour companion for their female partner: curiosity, woman’s request, and peer encouragement, and were in agreement that ultimately it should be the woman’s choice about who is allowed to be present (moderate confidence; Bondas‐Salonen 1998; Chapman 1990; Kululanga 2012; Longworth 2011; Pafs 2016; Sapkota 2012; Somers‐Smith 1999). Some men were curious about what the childbirth process entailed and wanted to be present as a learning experience (Kululanga 2012; Pafs 2016; Sapkota 2012). Other men’s female partners requested their presence to help support them, and believed that their presence was important (Bondas‐Salonen 1998; Chapman 1990; Kululanga 2012; Pafs 2016; Sapkota 2012; Somers‐Smith 1999). Some men were encouraged by their peers to act as a labour companion either explicitly through discussions, or implicitly through the belief that all male partners were acting as labour companions (Kululanga 2012; Longworth 2011; Somers‐Smith 1999). In Nepal, some men felt that cultural norms around birthing practices and the presence of men on the labour ward made some men feel uncomfortable with the idea of supporting their female partners (Sapkota 2012).
Finding 35
Men who acted as labour companions for their female partners felt that their presence made a positive impact on themselves as individuals (low confidence; Kululanga 2012; Sapkota 2012). They felt that they had a better understanding of childbirth, and recognised the importance of their presence and playing an active role in their partner's birth to act as an advocate and strengthen their partner's confidence (Kululanga 2012; Sapkota 2012). Most men felt positively about the experience, and believed that they would be better able to support their partner during future births (Kululanga 2012; Sapkota 2012).
Finding 36
Men who acted as labour companions for their female partners felt that their presence made a positive impact on their relationship with their female partner and the new baby (low confidence; Dodou 2014; Kululanga 2012; Sapkota 2012). The male partner described developing a bond/attachment with the baby from the time of birth, and bearing witness to the important event for them to become fathers (Dodou 2014; Kululanga 2012; Sapkota 2012). Men also felt that they were able to share the responsibilities of the birth with their partner, and that this experience increased their respect and love for their partners (Dodou 2014; Kululanga 2012; Sapkota 2012).
Finding 37
Men who acted as labour companions for their female partners may feel scared, anxious or helpless when witnessing their partners in pain during labour and childbirth (low confidence; Fathi 2017; Kaye 2014; Kululanga 2012; Sapkota 2012). Men were fearful for their partners' health and anxious about the amount of blood loss during the birth. Feelings of helplessness arose when men did not know how to support their partner or alleviate their partner's pain. Some women expressed concern for their male partner's well‐being, as they felt that witnessing the birth may cause him emotional distress and suffering from seeing his partner in pain (Abushaikha 2013; Sapkota 2012).
Finding 38
Some lay companions (both male and female) were deeply impacted by witnessing a woman's pain during labour (moderate confidence; Abushaikha 2013; Chandler 1997; Chapman 1990; Fathi 2017; Kabakian‐Khasholian 2015; Kululanga 2012; Sapkota 2012). Observing this pain caused feelings of frustration and fear, as they felt that there was nothing that they could do to help alleviate their pain.
Finding 39
Some male partners felt that they were not well integrated into the care team or decision‐making (moderate confidence; Bäckström 2011; Chandler 1997; Kaye 2014; Kululanga 2012; Longworth 2011; Somers‐Smith 1999). These men felt that their presence was tolerated by healthcare providers, but was not a necessary role. They relied on cues from the woman and healthcare provider for when and how to give support, but were often afraid to ask questions to avoid being labelled as difficult.
Doulas' experiences
Finding 40
Doulas often met with women, and sometimes their partners, prior to the birth to establish a relationship with them. This helped to manage expectations, and mentally and physically prepare the woman and her partner for childbirth (moderate confidence; Akhavan 2012b; Berg 2006; Coley 2016; Darwin 2016; Koumouitzes‐Douvia 2006; Lundgren 2010; Shlafer 2015; Stevens 2011; Torres 2015). These meetings often included developing a birth plan, and discussing concerns, options and procedures for labour and childbirth. Women found these meetings to be an easily accessible way to prepare for birth, that they improved the continuity of care, and were often in addition to regular antenatal care appointments or childbirth education classes.
Finding 41
Doulas believed that one of their key responsibilities was to build rapport and mutual trust with the woman, in order to improve her birth experience. This relationship was foundational for the doulas to give effective support, and for the women to feel comfortable enough to let go. Doulas built rapport by communicating, providing practical support, comforting and relating to the woman (moderate confidence; Berg 2006; Coley 2016; de Souza 2010; Gilliland 2011; Hunter 2012; Koumouitzes‐Douvia 2006; McGarry 2016; Shlafer 2015; Thorstensson 2008). These techniques were adapted for different women to suit their personalities and individual needs. For example, doulas supporting women with intellectual disabilities used more visual prompts to reinforce key learning points (McGarry 2016). This bond may be more important for women who are in labour without any other support except from a doula, for example, incarcerated women (Shlafer 2015), as the woman may view the doula as her only source of support. When they were able to establish rapport with women, doulas felt motivated and confident to provide effective support (Thorstensson 2008). However, when doulas were unable to establish a rapport with the woman, for example if the woman was in severe pain, doulas felt powerless and lost confidence in their abilities (Thorstensson 2008).
Finding 42
Doulas found that the experience of providing support to women in labour could have a positive personal impact on themselves. Some found that acting as a doula built their self‐confidence, made them feel like they were making a difference, and provided a sense of fulfilment (low confidence; Hardeman 2016; Hunter 2012; McGarry 2016; Thorstensson 2008).
Integrating the findings from this synthesis with the findings of the Cochrane intervention review, 'Continuous support for women during childbirth'
Our third objective was to explore how the findings of this review can enhance our understanding of the related Cochrane systematic review of interventions (Bohren 2017). In this qualitative synthesis, we found that only 13 out of 52 qualitative studies (25%) were conducted alongside a study or as an evaluation of an intervention or programme, and 39 were stand‐alone qualitative studies. However, Bohren 2017 and this qualitative synthesis include data from comparable populations and conceptualisations of labour companionship and continuous support. Bohren 2017 identified no studies on continuous support conducted in low‐income countries; in contrast, this synthesis identified six qualitative studies conducted in low‐income countries.
We used two methods to integrate the synthesised qualitative findings with Bohren 2017:
a logic model;
a matrix model,
Logic model
The logic model integrates the findings of the qualitative synthesis with the outcomes identified in Bohren 2017, and proposes chains of events that may lead to the outcomes measured in Bohren 2017. Figure 2 presents the logic model, and we present a narrative summary of the model below.
2.
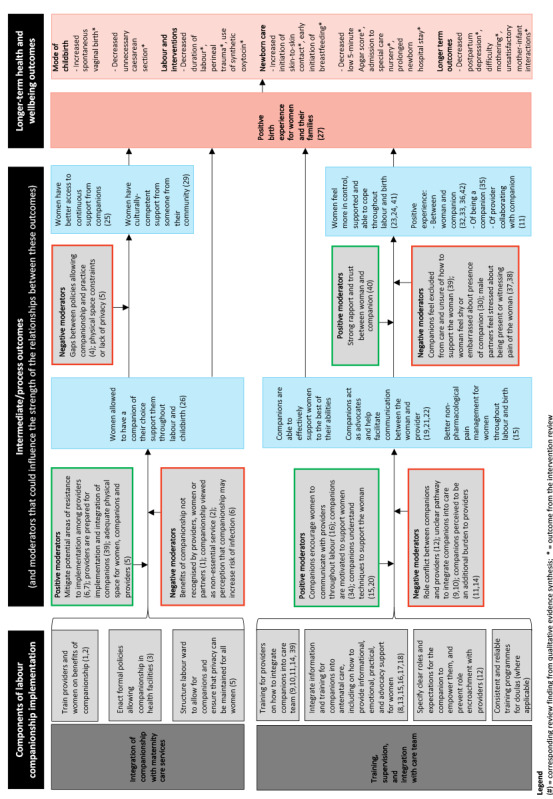
Logic model integrating findings from the qualitative synthesis with the outcomes identified in the intervention review, and proposed chain of events that may lead to the outcomes measured in the intervention review.
Integration of companionship with maternity care services
In the first chain of events, companionship is integrated into existing maternity care services. Providers are trained on the benefits of companionship, in order to reduce resistance to the intervention. Women are educated about the benefits of labour companionship, in order to normalise the presence of companions on the labour ward and prepare them for their own birth. Where necessary, formal changes are enacted at a health facility‐level or health system‐level, or both, to allow companionship. Lastly, efforts are made to structure or restructure labour wards in order to allow companionship and ensure that privacy can be maintained for all women. These programme components will create an enabling environment that allows all women who desire a companion to have a companion of her choice throughout labour and childbirth. In turn, this may lead to women having better access to continuous support and culturally‐competent care from someone in their community. Ultimately, this may lead to more positive birth experiences for women and their families, and improved health outcomes.
This chain of events may be enhanced or threatened in several ways. Allowing a woman to have a companion of her choice may be improved when areas of potential resistance are addressed among providers, providers are prepared for the implementation and integration of companions, and there is adequate physical space for women, companions and providers. In contrast, allowing a woman to have a companion of her choice may be threatened if the benefits of companionship are not recognised, companionship is viewed as a non‐essential service, or there are negative perceptions about companionship. Furthermore, women’s access to continuous support and culturally‐competent care may be threatened by gaps between policies allowing companionship and actual practice, or physical‐space constraints that influence privacy.
Training, supervision and integration with care team
In the second chain of events, all key stakeholders are trained, companions are supervised, and are integrated with the care team. Providers are trained on how to integrate companions into their care team to foster inclusion. During antenatal care, companions and women are provided with information and training, including on how to provide informational, emotional, practical and advocacy support for women. At a facility‐level, clear roles and expectations are specified for companions and providers to empower them, and prevent role encroachment. Where applicable, there are consistent and reliable training programmes for doulas. These programme components streamline the integration of companions into the care team, and ensure that companions effectively support women to the best of their abilities, act as advocates, and help facilitate communication between the woman and provider. Through labour companionship, women have access to better non‐pharmacological pain management throughout labour and childbirth. In turn, this may lead to women feeling more in control, supported and able to cope throughout labour and childbirth. Furthermore, there are positive experiences between the woman and companion, of being a companion, and of providers collaborating with companions. This may lead to positive birth experiences for women and their families, and improved health outcomes.
This chain of events may be enhanced or threatened in several ways. Companions may act as better advocates when they are able to encourage women to communicate with providers throughout labour. Companions may be able to support women to the best of their abilities when they are highly motivated. When companions understand techniques to support women, women may experience better non‐pharmacological pain management. In contrast, role conflict between companions and providers, unclear pathways to integrate companions into care, and the perception that companions are an additional burden to providers may threaten the ability of companions to support women. Furthermore, strong rapport and trust between the woman and companion may lead to women feeling more in control, supported and able to cope. However, when companions are excluded from care, women are shy or embarrassed in the presence of companions, or companions are stressed, women may feel less in control, less well supported or less able to cope.
Matrix model
The matrix model (Figure 3), provides a useful summary of how the synthesised qualitative findings are reflected in the content of the interventions in the studies included in the related Cochrane systematic review of interventions (Bohren 2017). The matrix shows that most interventions included in the Bohren 2017 review did not include the key features of labour companionship that we identified in this qualitative evidence synthesis. Six interventions (22.2%) specified that providers, and seven interventions (25.9%) specified that women were trained on the benefits of labour companionship prior to implementation. Three interventions (11.1%) specified that the labour ward was structured or restructured in a way to ensure that privacy could be maintained for all women. One intervention (3.7%) specified that providers were trained on how to integrate companions into the care team. Five interventions (18.5%) specified that there were clear roles and expectations set for companions and providers. Of the nine interventions with lay companions, three (33.3%) specified that training for companions on how to support women was integrated into antenatal care. In nine interventions (33.3%) women were allowed to choose their own companion.
3.
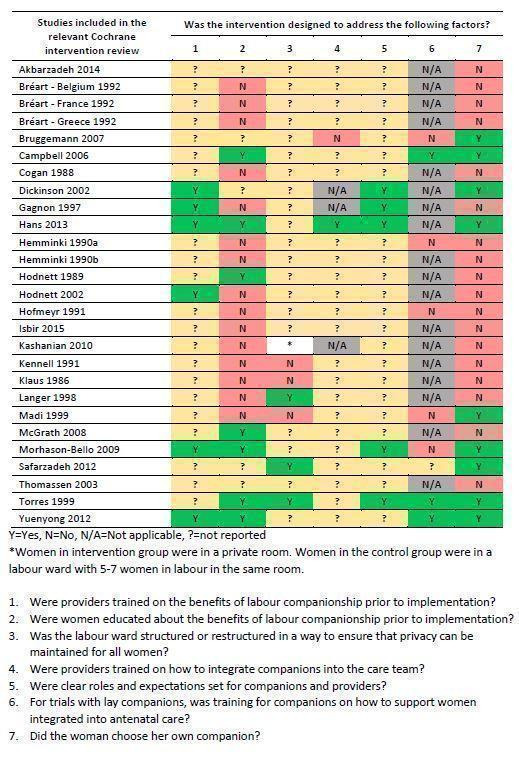
Figure 3. Matrix model applying key findings from the qualitative synthesis to studies included in the Cochrane intervention review (Bohren 2017)
No interventions in the Bohren 2017 review included all the features that we identified, and approximately half of the features across all studies in our qualitative synthesis were not reported in the interventions in Bohren 2017. We are unable to determine if the interventions did not address these features, or if authors of the intervention studies did not report them due to the limited amount of information available in the study reports, particularly for the older interventions (14 of the 27 interventions were conducted before 2000).
Using the logic and matrix models to identify hypotheses for subgroup analyses in the Cochrane intervention review, 'Continuous support for women during childbirth'
In future updates of Bohren 2017, the review authors could explore how the presence of the components identified in the logic and matrix models influence the success and implementation of continuous support programmes. In order to assess this, studies would need to report on these components. However, historically, many studies conducted on aspects related to intrapartum care do not include woman‐reported outcomes or assess women’s experiences of care. For example, of the 26 studies that provided usable outcome data to Bohren 2017, only 11 (42.3%) measured women’s negative ratings or negative feelings about the birth experience, and the definitions for this outcome were heterogeneous.
Discussion
Summary of main results
We found 52 relevant papers from 51 studies, mostly from high‐income countries. Many explored women’s perceptions of labour companionship. We assessed many findings of experiences of companionship and factors affecting implementation as high or moderate confidence; we have labelled findings that we assessed as low‐ or very low‐confidence findings.
Labour companions played four roles to support women. Firstly, companions provided informational support, by providing information about the process of childbirth, bridging communication gaps between clinical staff and women, acting as an intermediary to communicate between the clinical staff and the woman, and facilitating non‐pharmacological pain relief. Secondly, companions acted as advocates for women. Thirdly, companions provided practical support, including encouraging women to mobilise, providing massage, holding her hand. Fourthly, companions provided emotional support by helping women to feel in control and confident by using praise and reassurance, and by providing a continuous physical presence.
In general, women who wanted a companion present during labour and childbirth needed this person to be compassionate and trustworthy. Companionship helped women to have a positive birth experience, and women without a companion may view this as a negative birth experience. Women had mixed perspectives about the desire to have a male partner present (low confidence). In general, men who acted as labour companions felt that their presence made a positive impact on themselves as individuals (low confidence) and on their relationship with their partner and baby (low confidence), although some felt anxious witnessing the pain of childbirth (low confidence). Some male partners felt that they were not well integrated into the care team or decision‐making.
Doulas often met with women before the birth to build rapport and manage expectations. Women may develop close bonds with their doulas (low confidence). Foreign‐born women in high‐income settings may appreciate the support of community‐based doulas to receive culturally‐competent care (low confidence). Factors that affected implementation included that the benefits of companionship were not recognised by providers or women, viewed as a non‐essential service (low confidence), physical space constraints that threatened privacy, and fear of increased risk of infection (low confidence). Formal changes to existing policies to allow companionship (low confidence), and addressing gaps between policy and practice of allowing companionship may be important (low confidence). Some providers were resistant to integrating companions or not well trained on how to integrate companions, which may lead to conflict. Lay companions were often not integrated into antenatal care, which may cause frustration (low confidence).
The matrix model shows that most studies included in the related Cochrane systematic review of interventions (Bohren 2017), did not include the key features of labour companionship identified in the qualitative evidence synthesis.
Summary of integrating findings from this qualitative evidence synthesis with the findings of the relevant Cochrane intervention review, 'Continuous support for women during childbirth'
Our comparisons of the qualitative findings and the intervention review (Bohren 2017), through the logic model suggests that implementation of labour companionship programmes may be most successful when each of the programme components are incorporated into the design, and moderators are accounted for. Doing so may have a positive influence on the success and sustainability of a labour companionship programme.
Our comparisons of the qualitative findings and the intervention review (Bohren 2017), through the matrix model suggests that most studies included in Bohren 2017 did not include the key features of labour companionship identified in this qualitative evidence synthesis. The matrix table presented in Figure 3 may be useful to inform the development of future studies or programmes. Furthermore, this qualitative synthesis may help to explain why certain labour companionship interventions are more or less effective than others by providing insight into how the interventions were structured.
Finally, in this qualitative synthesis, 27 out of 51 studies (52.9%) had lay companions providing support to women, compared to seven out of 26 studies (26.9%) in the Bohren 2017. Future studies may consider using a lay companion to provide support, particularly in settings where doula support is not feasible and health workforce constraints preclude retired or student midwives from acting as labour companions.
Overall completeness and applicability of evidence
A majority of the included studies included the perspectives of women or male partners. Only four included studies focused on the perspectives of healthcare providers (midwives and nurses only). Given that the introduction of companionship requires a restructuring of service provision to include the presence of an additional support person, the inclusion of more provider perspectives could have added important information about factors that may influence sustainable and successful implementation. Additionally, understanding the perspectives of healthcare administrators or policy‐makers would add an important dimension of higher‐level decision‐making and contexts that may influence the implementability of the programme.
Nineteen of the 51 studies included in this qualitative synthesis were conducted in LMICs, and of these, only three studies were conducted attached to an intervention or evaluation (Campero 1998; Kabakian‐Khasholian 2015; Khresheh 2010). As researchers implement labour companionship programmes or studies in LMIC settings, it may be useful to conduct qualitative research to assess the feasibility, acceptability, values, preferences and experiences of populations in those settings (including women, partners, and healthcare providers).
Lastly, almost all of the qualitative studies used interview or focus group methods, which rely on the self‐report of the individual participants. It may also be useful to use other qualitative methods of data collection, such as participant observation of the labour ward or longer‐term ethnographic research in a healthcare setting, in order to better understand actual practices and changes over time.
Confidence in the findings
Our confidence in the qualitative findings ranges from very low to high, based on the CERQual assessments. The main reasons for downgrading for methodological limitations were poor reporting of recruitment strategies, researcher reflexivity, healthcare context, and data analysis methods. Assessing coherence generally led to improving how the review finding was written, in order to better explain and account for divergent cases. Downgrading for adequacy typically occurred when there were concerns about the richness or the quantity of the data contributing to the review finding. Downgrading for relevance typically occurred when the setting of the individual studies contributing to the review finding was only partially relevant to the review question. Typically, this was in relation to contributing studies conducted in high‐income settings in Europe or North America.
Agreements and disagreements with other studies and reviews
The findings from this qualitative synthesis have some similarities with other qualitative and mixed‐methods reviews on quality of maternity care and companionship (Beake 2018; Bohren 2015a; Kabakian‐Khasholian 2017; Munabi‐Babigumira 2017; Shakibazadeh 2018); however none of these reviews had the same focus as this synthesis.
Kabakian‐Khasholian 2017 explored factors assessing the implementation of companion of choice at birth based on the study reports included in a previous version of the Cochrane intervention review, 'Continuous support for women during childbirth' (Bohren 2017), supplemented by 10 qualitative studies. Similar to this synthesis, Kabakian‐Khasholian 2017 found that women and their families appreciated continuous support during labour and childbirth, and that key barriers to implementation included provider resistance and structural constraints. They identified an additional benefit of introducing companionship in reducing the financial costs of obstetric interventions such as epidural use and caesarean section (Kabakian‐Khasholian 2017).
Beake 2018 explored the experiences of women, labour companions and providers on the management of early labour, and found that the perceived benefit of support by a labour companion during early labour varied. Some companions were supportive and encouraged women to relax, but others were anxious and urged women to seek early admission to the health facility (Beake 2018). The mixed experience of supportive and anxious labour companions aligns with the findings from this synthesis that suggest that when companions are not well prepared or are anxious to see a woman in pain, they may not understand how to best support a woman.
Munabi‐Babigumira 2017 explored factors influencing the provision of intrapartum and postnatal care by skilled birth attendants in LMICs, and found that staff shortages and workload may jeopardise a provider's ability to express support, empathy and friendliness to women during labour and childbirth (Munabi‐Babigumira 2017). They also found that providers were sometimes unaware of recommended effective practices or non‐receptive to new practice knowledge (Munabi‐Babigumira 2017), which may influence the introduction of interventions such as labour companionship. This aligns with the findings from this synthesis in relation to the importance of training providers on the benefits of companionship, and how companions may be able to help address shortcomings in maternity services, particularly in LMICs.
Bohren 2015a and Shakibazadeh 2018 explored the mistreatment of women during childbirth and respectful maternity care. Both reviews found that women desire supportive care and the presence of a labour companion, but that many women across the world were not allowed to have a companion present throughout labour and childbirth (Bohren 2015a;Shakibazadeh 2018). The absence of a companion contributed to women’s feelings of disempowerment, fear, and loneliness throughout labour and childbirth (Bohren 2015a;Shakibazadeh 2018).
Reflexivity discussions in the included studies
Childbirth can be an intensely powerful and private experience in a woman’s life. It is relevant to consider how different aspects of study design may influence how a woman discusses and describes her birth experience. For example, studies that use healthcare providers to recruit and conduct interviews or focus groups with women may influence women’s participation (e.g. they may not perceive that they have a choice to decline to participate) and responses (e.g. they may not feel comfortable to disclose negative experiences with care (courtesy or social desirability bias)). Furthermore, the setting where an interview or focus group is conducted (e.g. facility‐based or community‐based) may also influence women’s participation and responses. Many of the studies included in this synthesis did not provide an adequate report of the recruitment strategy, the background of the interviewer, or the location of the data collection; therefore, it is difficult to assess how responses may have been influenced by these factors.
Authors' conclusions
Implications for practice
The following questions were derived from our findings, and may help programme managers, researchers, and other key stakeholders to assess whether the labour companionship interventions they are planning adequately address factors that may affect implementation, as described by women, their family members, and healthcare providers.
Were providers trained on the benefits of labour companionship prior to implementation?
Were women trained on the benefits of labour companionship prior to implementation?
Was the labour ward structured or restructured in a way to ensure that privacy can be maintained for all women?
Were providers trained on how to integrate companions into the care team?
Were clear roles and expectations set for companions and providers?
For studies with lay companions, was training for companions on how to support women integrated into antenatal care?
Did the woman choose her own companion?
Policy changes may be needed at different levels (health system, health facilities) in order to change practice to allow companionship. Furthermore, where there is limited continuity between antenatal and intrapartum care, training for companions may not be feasible during antenatal care. Therefore, training for companions will need to appropriately reflect the local context, for example, providing brief educational materials for companions about supporting women upon admission to the health facility for childbirth.
Implications for research
We developed implications for research based on the overview of studies included in this review and CERQual (Confidence in the Evidence from Reviews of Qualitative research) assessments.
Better reporting is needed in qualitative studies, particularly around sampling methods, researcher reflexivity, and data analysis. Future qualitative studies on this topic, and more broadly, should transparently report their research methods, including reflection on the researchers’ roles and how they may influence the conduct and results of the study.
More research about implementing labour companionship models in different contexts, particularly in low‐ and middle‐income countries, is needed to understand how different models may improve outcomes for women and babies. Understanding how different cadres of healthcare providers, such as midwives, nurses, obstetricians, and healthcare managers, perceive labour companionship and factors that may affect implementation would provide valuable evidence to scale‐up implementation. Implementation research or studies conducted on labour companionship should include a qualitative component to evaluate the process and context of implementation, in order to better interpret results and share findings across contexts. This aligns with the “WHO [World Health Organization] Standards for improving quality of maternal and newborn care in health facilities”, where every woman “is offered the option to experience labour and childbirth with the companion of her choice” (World Health Organization 2016).
Further research is needed to understand the most appropriate ways to engage lay companions during antenatal care, including the content of training programmes. Similarly, more research is needed to understand how labour wards in lower‐resource settings may be physically designed to allow labour companionship, while maintaining privacy and confidentiality for women.
What's new
| Date | Event | Description |
|---|---|---|
| 31 July 2019 | Amended | Plain language summary title added |
History
Protocol first published: Issue 11, 2016 Review first published: Issue 3, 2019
| Date | Event | Description |
|---|---|---|
| 8 April 2019 | Amended | Correction made to Acknowledgements and Sources of support |
| 19 March 2019 | Amended | Correction made to Contact person's e‐mail address |
| 5 October 2016 | Feedback has been incorporated | Final revision to "reflexivity" section. |
| 24 September 2016 | Feedback has been incorporated | Updated with responses to peer review comments from SD, DH and CG. |
| 19 April 2016 | Amended | Draft protocol with feedback from authors. |
Acknowledgements
This review is funded by the Department of Reproductive Health and Research, World Health Organization.
Claire Glenton and Simon Lewin of the Norwegian Satellite of Cochrane Effective Practice and Organisation of Care (EPOC), and Emma Allanson of The University of Western Australia provided guidance in developing the protocol and review. Marit Johansen of EPOC developed and ran the search strategy during the initial search and search update.
Valuable feedback was received from the editors and peer reviewers: Elizabeth Paulsen, Soo Downe, Ruth Garside, Tamar Kabakian‐Khasholian, and Anne‐Marie Bergh.
The EPOC Norwegian Satellite receives funding from the Norwegian Agency for Development Cooperation (Norad), via the Norwegian Institute of Public Health to support review authors in the production of their reviews.
This Cochrane Review is associated with the Research, Evidence and Development Initiative (READ‐It) project. READ‐It (project number 300342‐104) is funded by UK aid from the UK government; however, the views expressed do not necessarily reflect the UK government’s official policies.
Appendices
Appendix 1. Search strategies
MEDLINE Search strategy
| # | Searches |
| 1 | Perinatal Care/ |
| 2 | Obstetric Nursing/ |
| 3 | Delivery, Obstetric/ |
| 4 | Labor, Obstetric/ |
| 5 | Parturition/ |
| 6 | Home Childbirth/ |
| 7 | Natural Childbirth/ |
| 8 | or/1‐7 |
| 9 | Social Support/ |
| 10 | 8 and 9 |
| 11 | Doulas/ |
| 12 | (doula or doulas or obstetric nursing).ti,ab,kf. |
| 13 | ((childbirth? or birth? or labor or laboring or labour or labouring or intrapartum) adj6 (support* or companion* or coach*)).ti,ab,kf. |
| 14 | (((presence or present or attend* or accompan*) adj3 (family member? or friend? or spouse? or partner? or unskilled)) and (childbirth? or birth? or labor or labour)).ti,ab,kf. |
| 15 | (((presence or present or attend* or accompan*) adj3 (midwife or midwives or midwifery or nurse)) and (childbirth? or birth? or labor or labour)).ti,ab,kf. |
| 16 | or/11‐15 |
| 17 | 10 or 16 |
| 18 | limit 17 to "qualitative (best balance of sensitivity and specificity)" |
| 19 | qualitative research/ |
| 20 | 17 and 19 |
| 21 | 18 or 20 |
CINAHL, Ebsco search strategy
| # | Query |
| S29 | S27 AND S28 |
| S28 | EM 201611‐ |
| S27 | S25 AND S26 |
| S26 | Limiters ‐ Exclude MEDLINE records |
| S25 | S23 OR S24 |
| S24 | S18 AND S22 |
| S23 | S18 AND S19 |
| S22 | S20 OR S21 |
| S21 | TI qualitative OR AB qualitative |
| S20 | (MH "Qualitative Studies+") |
| S19 | Limiters ‐ Clinical Queries: Qualitative ‐ Best Balance |
| S18 | S10 OR S17 |
| S17 | S11 OR S12 OR S13 OR S14 OR S15 OR S16 |
| S16 | TI ( (presence or present or attend* or accompan*) N3 (midwife or midwives or midwifery or nurse) and (childbirth* or birth* or labor or labour) ) OR AB ( (presence or present or attend* or accompan*) N3 (midwife or midwives or midwifery or nurse) and (childbirth* or birth* or labor or labour) ) |
| S15 | TI ( ((presence or present or attend* or accompan*) N3 ("family member" or "family members" or friend* or spouse* or partner* or unskilled)) and (childbirth* or birth* or labor or labour) ) OR AB ( ((presence or present or attend* or accompan*) N3 ("family member" or "family members" or friend* or spouse* or partner* or unskilled)) and (childbirth* or birth* or labor or labour) ) |
| S14 | TI ( (childbirth* or birth* or labor or laboring or labour or labouring or intrapartum) N6 (support* or companion* or coach*) ) OR AB ( (childbirth* or birth* or labor or laboring or labour or labouring or intrapartum) N6 (support* or companion* or coach*) ) |
| S13 | TI ( doula or doulas or "obstetric nursing" ) OR AB ( doula or doulas or "obstetric nursing" ) |
| S12 | (MH "Labor Support") |
| S11 | (MH "Doulas") |
| S10 | S6 AND S9 |
| S9 | S7 OR S8 |
| S8 | (MH "Caregiver Support") |
| S7 | (MH "Support, Psychosocial") |
| S6 | S1 OR S2 OR S3 OR S4 OR S5 |
| S5 | (MH "Childbirth+") |
| S4 | (MH "Labor") |
| S3 | (MH "Delivery, Obstetric") |
| S2 | (MH "Obstetric Nursing") |
| S1 | (MH "Prenatal Care") |
POPLINE, K4Health search strategy
Keyword: CARE AND SUPPORT AND Keyword: CHILDBIRTH
OR
Keyword: KINSHIP NETWORKS AND Keyword: CHILDBIRTH
OR
All Fields: doula OR doulas OR "prenatal support" OR "childbirth support" OR "birth support" OR "labor support" OR "labour support" OR "intrapartum support" OR "childbirth companion" OR "childbirth companionship" OR "birth companion" OR "birth companionship" OR "labor companion" OR "labor companionship" OR "labour companion" OR "labour companionship" OR "support during labor" OR "support during labour" OR "support during childbirth" OR "support during birth" OR "support during delivery"
Appendix 2. Evidence profile
| Finding number | Summary of review finding | Studies contributing to the review finding | Methodological limitations | Coherence | Relevance | Adequacy | CERQual assessment (confidence in the findings) | Explanation of CERQual assessment |
| Factors affecting implementation | ||||||||
| Awareness‐raising among healthcare providers and women | ||||||||
| 1 | The benefits of labour companionship may not be recognised by providers, women, or their partners. | Abushaikha 2013; Afulani 2018; Alexander 2014; Brüggemann 2014; Coley 2016; Pafs 2016 | Minor concerns regarding methodological limitations due to issues with reflexivity, recruitment and research design | Minor concerns regarding coherence | Minor concerns regarding relevancy | Moderate concerns regarding adequacy due to 6 contributing studies with moderately thick data | Moderate confidence | Due to minor concerns regarding methodological limitations, coherence, and relevancy, and moderate concerns regarding adequacy |
| 2 | Labour companionship was sometimes viewed as non‐essential or less important compared to other aspects of care, and therefore deprioritised due to limited resources to spend on 'expendables'. | Akhavan 2012b; Brüggemann 2014; Lagendyk 2005; Premberg 2011 | Moderate concerns regarding methodological limitations due to issues regarding recruitment, reflexivity and ethical considerations | Minor concerns regarding coherence | Serious concerns regarding relevance due to evidence from limited contexts and only in middle‐ and high‐income countries | Serious concerns regarding adequacy due to 4 contributing studies with thin data | Low confidence | Due to minor concerns regarding coherence, moderate concerns regarding methodological limitations and serious concerns regarding relevance and adequacy |
| Creating an enabling environment | ||||||||
| 3 | Formal changes to existing policies regarding allowing companions on the labour ward may be necessary prior to implementing labour companionship models at a facility level. | Abushaikha 2013; Kabakian‐Khasholian 2015 | Moderate concerns regarding methodological limitations due to issues regarding research design, recruitment and reflexivity | Minor concerns regarding coherence | Serious concerns regarding relevance due to limited evidence from limited contexts (2 countries in the Middle East) | Serious concerns regarding adequacy due to 2 contributing studies with thin data | Low confidence | Due to minor concerns regarding coherence, moderate concerns regarding methodological limitations and serious concerns regarding relevance and adequacy |
| 4 | In settings where companions are allowed, there can be gaps between a policy or law allowing companionship, and the actual practice of allowing all women who want companionship to have a companion present. | Brüggemann 2014; Kaye 2014 | Moderate concerns regarding methodological limitations due to issues regarding reflexivity, recruitment and research design | Minor concerns regarding coherence | Serious concerns regarding relevance due to limited evidence from limited contexts (2 low and middle income countries) | Moderate concerns regarding adequacy due to 2 contributing studies with thick data | Low confidence | Due to minor concerns regarding coherence, moderate concerns regarding methodological limitations and adequacy, and serious concerns regarding relevance |
| 5 | Providers, women and male partners highlighted physical space constraints of the labour wards as a key barrier to labour companionship as it was perceived that privacy could not be maintained and wards would become overcrowded. | Abushaikha 2013; Afulani 2018; Brüggemann 2014; Harte 2016; Kabakian‐Khasholian 2015; Qian 2001; Sapkota 2012; Shimpuku 2013 | Moderate concerns regarding methodological limitations due to issues with reflexivity, recruitment, research design, ethical considerations, and data analysis | Minor concerns regarding coherence | Minor concerns regarding relevance, may be more relevant in LMIC settings with overcrowded wards | Moderate concerns regarding adequacy due to 8 contributing studies with reasonably thick data | Moderate confidence | Due to minor concerns regarding relevance and coherence, and moderate concerns regarding adequacy and methodological limitations |
| 6 | Some providers, women and male partners were concerned that the presence of a labour companion may increase the risk of transmitting infection in the labour room. | Abushaikha 2013; Brüggemann 2014; Kabakian‐Khasholian 2015; Qian 2001 | Moderate concerns regarding methodological considerations due to issues regarding recruitment, reflexivity, research design and analysis | Minor concerns regarding coherence | Moderate concerns regarding relevance due to limited range of contexts only in middle‐income countries | Serious concerns regarding adequacy due to 4 contributing studies with thin data | Low confidence | Due to minor concerns regarding coherence, moderate concerns regarding methodological limitations and relevance, and serious concerns regarding adequacy |
| Training, supervision, and integration with care team | ||||||||
| 7 | Some providers were resistant to integrate companions or doulas into maternity services, and provided several explanations for their reluctance. Providers felt that lay companions lacked purpose and boundaries, increased provider workloads, arrived unprepared, and could be in the way. | Bondas‐Salonen 1998; Brüggemann 2014; Horstman 2017; Kabakian‐Khasholian 2015; Kaye 2014; Lagendyk 2005; Torres 2013 | Minor concerns regarding methodological limitations, due to issues with reflexivity, recruitment strategies, and data analysis | Minor concerns regarding coherence | Very minor concerns regarding relevance | Moderate concerns regarding adequacy due to 7 contributing studies with reasonably thick data | High confidence | Due to very minor concerns regarding relevance, minor concerns regarding methodological limitations and coherence , and moderate concerns regarding adequacy |
| 8 | In most cases, male partners were not integrated into antenatal care or training sessions before birth. Where they were included in antenatal preparation, they felt that they learned comfort and support measures to assist their partners, but that these measures were often challenging to implement throughout the duration of labour and birth. | Abushaikha 2013; Bondas‐Salonen 1998; Chandler 1997; Ledenfors 2016; Sapkota 2012; Somers‐Smith 1999 | Moderate concerns regarding methodological limitations due to issues regarding recruitment, reflexivity, research design and ethical considerations | Minor concerns regarding coherence | Moderate concerns regarding relevance due to evidence from limited contexts | Serious concerns regarding adequacy due to 6 contributing studies with relatively thin data | Low confidence | Due to minor concerns regarding coherence, moderate concerns regarding methodological limitations and relevance, and serious concerns regarding adequacy |
| 9 | In settings where lay companionship or doula care were available, providers were not well trained on how to integrate the companion as an active or important member of the woman’s support team. | Bondas‐Salonen 1998; Brüggemann 2014; Kabakian‐Khasholian 2015; Kaye 2014; Lagendyk 2005; Torres 2013 | Minor concerns regarding methodological limitations due to issues with research design, reflexivity, recruitment and data analysis | Minor concerns regarding coherence | Minor concerns regarding relevancy due to evidence from a limited range of contexts | Moderate concerns regarding adequacy due to 6 contributing studies with moderately thick data | Moderate confidence | Due to minor concerns regarding methodological limitations, coherence and relevance, and moderate concerns regarding adequacy |
| 10 | Some doulas felt that they were not well integrated into decision‐making or care co‐ordination by the healthcare providers, and were sometimes ignored by healthcare providers. | Berg 2006; McLeish 2018; Stevens 2011; Torres 2013 | Moderate concerns regarding methodological limitations due to issues regarding reflexivity, recruitment, research design and ethical considerations | Minor concerns regarding coherence | Serious concerns regarding relevance due to limited evidence from limited contexts (all high‐income countries) | Serious concerns regarding adequacy due to 4 contributing studies with thin data | Low confidence | Due to minor concerns regarding coherence, moderate concerns regarding methodological limitations, and serious concerns regarding relevance and adequacy |
| 11 | Most healthcare providers believed that having a lay companion support a woman throughout labour and childbirth was beneficial to the woman and worked well when companions were integrated into the model of care. However, when lay companions were not well engaged or integrated, conflict could arise as they may be perceived as an additional burden for healthcare providers to manage their presence, and provide ongoing direction and support. | Brüggemann 2014; Harte 2016; Kabakian‐Khasholian 2015; Khresheh 2010; Maher 2004; Qian 2001 | Moderate concerns regarding methodological limitations due to issues regarding reflexivity, recruitment, ethical considerations and data analysis | Minor concerns regarding coherence | Moderate concerns regarding relevance due to evidence from limited contexts | Moderate concerns regarding adequacy due to 6 contributing studies with reasonably thick data | Moderate confidence | Due to minor concerns regarding coherence, and moderate concerns regarding methodological limitations, relevance, and adequacy |
| 12 | Most midwives believed that doulas played a collaborative role in supporting women during childbirth, and were assets to the team who provided more woman‐centred, needs‐led support. However, some midwives found it difficult to engage as carers with women when doulas were present, as they felt that doulas encroached on their carer role. | Akhavan 2012b; Lundgren 2010; McLeish 2018; Stevens 2011 | Moderate concerns regarding methodological limitations due to issues regarding reflexivity, recruitment, research design and ethical considerations | Minor concerns regarding coherence | Serious concerns regarding relevance due to limited evidence from limited contexts (all high‐income countries) | Moderate concerns regarding adequacy due to 4 contributing studies with reasonably thick data | Low confidence | Due to minor concerns regarding coherence, moderate concerns regarding methodological limitations and adequacy, and serious concerns regarding relevance |
| 13 | Lay companions received little or no training on how to support the woman during labour and childbirth, which made them feel frustrated. | Kululanga 2012; Sapkota 2012 | Minor concerns regarding methodological considerations due to issues with reflexivity and recruitment | Minor concerns regarding coherence | Serious concerns regarding relevancy due to partial evidence from a limited range of contexts and only low‐income countries | Serious concerns regarding adequacy due to 2 contributing studies with thin data | Low confidence | Due to minor concerns regarding methodological considerations and coherence, and serious concerns regarding relevancy and adequacy |
| 14 | Some men felt that they were actively excluded, left out, or not involved in their female partner's care. They were unsure of where they fit in to support the woman, and felt that their presence was tolerated but not necessary. | Bäckström 2011; Chandler 1997; Kaye 2014; Kululanga 2012; Longworth 2011; Somers‐Smith 1999 | Moderate concerns regarding methodological limitations due to issues regarding reflexivity, recruitment, research design, and ethical considerations | Minor concerns regarding coherence | Moderate concerns regarding relevance due to evidence from limited contexts (predominantly Europe, North America, and Africa) | Moderate concerns regarding adequacy due to 6 contributing studies with relatively thick data | Moderate confidence | Due to minor concerns regarding coherence, and moderate concerns regarding methodological limitations, relevance and adequacy |
| Roles that companions play | ||||||||
| Informational support | ||||||||
| 15 | Women valued the non‐pharmacological pain relief measures that companions helped to facilitate, including a soothing touch (holding hands, massage and counter pressure), breathing, and relaxation techniques. | Campero 1998; Chapman 1990; Dodou 2014; de Souza 2010; Fathi 2017; Hunter 2012; Kabakian‐Khasholian 2015; Khresheh 2010; Lundgren 2010; McLeish 2018; Sapkota 2012; Somers‐Smith 1999; Thorstensson 2008; Torres 2015 | Moderate concerns regarding methodological limitations due to issues with reflexivity, data analysis, recruitment strategy, and research design | Minor concerns regarding coherence | Minor concerns regarding relevance, although this finding was primarily found in high‐ and middle‐income settings | Minor concerns regarding adequacy due to 14 contributing studies with reasonably thick data | High confidence | Due to minor concerns regarding adequacy, coherence, and relevance, and moderate concerns regarding methodological limitations |
| 16 | Doulas played an important role in providing information to women about the process of childbirth, duration of labour, and reasons for medical interventions. They bridged communication gaps between clinical staff and women, and facilitated a more actively engaged environment where women were encouraged to ask questions. | Akhavan 2012a; Akhavan 2012b; Berg 2006; Campero 1998; Darwin 2016; Gilliland 2011; Horstman 2017; LaMancuso 2016; McGarry 2016; McLeish 2018; Schroeder 2005; Torres 2013; Torres 2015 | Moderate concerns regarding methodological limitations due to issues regarding reflexivity, recruitment, ethical considerations, data analysis and research design | Minor concerns regarding coherence | Moderate concerns regarding relevance due to limited evidence from limited contexts (predominantly high‐income countries where doula studies took place) | Minor concerns regarding adequacy due to 13 contributing studies with moderately thick data | Moderate confidence | Due to minor concerns regarding coherence and adequacy and moderate concerns regarding methodological limitations and relevance. |
| 17 | Lay companions also played a role in providing informational support to women or acting as the woman's voice during labour and childbirth. This usually took the form of acting as an intermediary by relaying, repeating, or explaining information from the healthcare provider to the woman, and from the woman to the healthcare provider. | Alexander 2014; Bondas‐Salonen 1998; Khresheh 2010; Price 2007; Qian 2001; Sapkota 2012 | Minor concerns regarding methodological limitations due to issues regarding reflexivity, recruitment, ethical considerations and data analysis | Minor concerns regarding coherence | Minor concerns regarding relevance | Moderate concerns regarding adequacy due to 6 contributing studies with moderately thin data | Moderate confidence | Due to minor concerns regarding methodological limitations, coherence and relevance, and moderate concerns regarding adequacy |
| 18 | Companions played an important role to help facilitate communication between the woman and healthcare providers, including representing the woman's interests and speaking on her behalf when she was unable to do so. They helped to relay information between the woman and healthcare provider, such as asking questions and setting boundaries. | Akhavan 2012b; Bondas‐Salonen 1998; Darwin 2016; Gentry 2010; Hardeman 2016; Horstman 2017; Hunter 2012; Khresheh 2010; Koumouitzes‐Douvia 2006; LaMancuso 2016; Lundgren 2010; McGarry 2016; McLeish 2018; Premberg 2011; Price 2007; Stevens 2011; Torres 2015 | Moderate concerns regarding methodological limitations due to issues regarding reflexivity, recruitment, research design, ethical considerations and data analysis | Minor concerns regarding coherence | Moderate concerns regarding relevance due to evidence from limited contexts (predominantly high‐income countries) | Minor concerns regarding adequacy | Moderate concerns | Due to minor concerns regarding coherence and adequacy, and moderate concerns regarding methodological limitations and relevance. |
| Advocacy | ||||||||
| 19 | Companions played a role to bear witness to the process of childbirth. They shared the childbirth experience with the woman by being with her, and were viewed as observers who could monitor, reflect, and report on what transpired throughout labour and childbirth, such as witnessing pain, the birth process, and the woman's transformation to motherhood. | Afulani 2018; Alexander 2014; Bondas‐Salonen 1998; Dodou 2014; Horstman 2017; Hunter 2012; Longworth 2011; Price 2007; Sapkota 2012 | Minor concerns regarding methodological considerations | Minor concerns regarding coherence | Minor concerns regarding relevance | Minor concerns regarding adequacy | High confidence | Due to minor concerns regarding methodological considerations, coherence, relevance and adequacy |
| Practical support | ||||||||
| 20 | Companions provided physical support to women throughout labour and childbirth, such as giving them a massage and holding their hand. Companions encouraged and helped women to mobilise throughout labour or to change positions, such as squatting or standing, and provided physical support to go to the bathroom or adjust clothing. | Afulani 2018; Chandler 1997; Chapman 1990; de Souza 2010; Fathi 2017; Hunter 2012; Kabakian‐Khasholian 2015; Khresheh 2010; Koumouitzes‐Douvia 2006; McLeish 2018; Premberg 2011; Price 2007; Sapkota 2012; Shimpuku 2013; Torres 2013 | Moderate concerns regarding methodological limitations due to issues regarding research design, reflexivity, recruitment, ethical considerations, and data analysis | Minor concerns regarding coherence | Minor concerns regarding relevance | Minor concerns regarding adequacy | High confidence | Due to minor concerns regarding coherence, relevance and adequacy, and moderate concerns regarding methodological limitations |
| 21 | Companions played an important role to assist healthcare providers to care for women by observing and identifying potential issues throughout labour and childbirth. | Akhavan 2012b; Alexander 2014; Khresheh 2010; Qian 2001; Sapkota 2012; Shimpuku 2013 | Moderate concerns regarding methodological limitations due to issues regarding research design, reflexivity, recruitment, ethical considerations and data analysis | Minor concerns regarding coherence | Minor concerns regarding relevance | Moderate concerns regarding adequacy due to 6 contributing studies with moderately thick data | Moderate confidence | Due to minor concerns regarding coherence and relevance, and moderate concerns regarding methodological limitations and adequacy |
| 22 | Some healthcare providers and doulas felt that shortcomings in maternity services could be potentially addressed by doulas or lay companions. | Afulani 2018; Akhavan 2012b; Stevens 2011 | Moderate concerns regarding methodological limitations due to issues with research design, recruitment, reflexivity and ethical considerations | Minor concerns regarding coherence | Serious concerns regarding relevance due to partial evidence from a limited range of contexts (Australia, Kenya and Sweden) | Serious concerns regarding adequacy due to 3 contributing studies with thin data | Very low confidence | Due to minor concerns regarding coherence, moderate concerns regarding methodological limitations, and serious concerns regarding relevance and adequacy |
| Emotional support | ||||||||
| 23 | Women valued that companions and doulas helped to facilitate their feeling in control during labour and gave them confidence in their abilities to give birth. | Berg 2006; Campero 1998; Chapman 1990; Darwin 2016; Dodou 2014; Fathi 2017; Gilliland 2011; Hunter 2012; Ledenfors 2016; Price 2007; Sapkota 2012 | Moderate concerns regarding methodological limitations due to issues with reflexivity, recruitment, research design and data analysis | Minor concerns regarding coherence | Moderate concerns regarding relevance due to limited evidence from Africa, Asia and low‐income countries | Minor concerns regarding adequacy due to 11 contributing studies with reasonably thick data | Moderate confidence | Due to minor concerns regarding adequacy and coherence, and moderate concerns regarding methodological limitations and relevance |
| 24 | Companions often provided emotional support to women through the use of praise and reassurance. They acknowledged the women's efforts and concerns, and provided reinforcement through verbal encouragement and affirmations. | Abushaikha 2012; Alexander 2014; Bäckström 2011; Berg 2006; Bondas‐Salonen 1998; de Souza 2010; Fathi 2017; Gentry 2010; Gilliland 2011; Hardeman 2016; Harte 2016; Horstman 2017; Hunter 2012; Kabakian‐Khasholian 2015; Khresheh 2010; Koumouitzes‐Douvia 2006; Ledenfors 2016; Lundgren 2010; McGarry 2016; McLeish 2018; Premberg 2011; Price 2007; Sapkota 2012; Schroeder 2005; Somers‐Smith 1999; Thorstensson 2008; Torres 2013; Torres 2015 | Moderate concerns regarding methodological limitations due to issues regarding reflexivity, recruitment, ethical considerations, and data analysis | Minor concerns regarding coherence | Minor concerns regarding relevance | Very minor concerns regarding adequacy | High confidence | Due to very minor concerns regarding adequacy, minor concerns regarding coherence and relevance, and moderate concerns regarding methodological limitations |
| 25 | The continuous physical presence of someone caring was an important role that companions played, particularly in settings where continuous midwifery care was not available or not practiced. The continuous presence of the companion signalled to the woman the availability of support when needed, and helped to pass the time throughout labour. | Abushaikha 2012; Afulani 2018; Berg 2006; Bondas‐Salonen 1998; Campero 1998; Darwin 2016; Dodou 2014; Koumouitzes‐Douvia 2006; Lundgren 2010; McLeish 2018; Price 2007; Sapkota 2012; Somers‐Smith 1999; Stevens 2011; Thorstensson 2008; Torres 2015 | Moderate concerns regarding methodological limitations due to issues regarding reflexivity, recruitment, ethical considerations and data analysis | Minor concerns regarding coherence | Moderate concerns regarding relevance due to evidence from limited contexts (predominantly high‐income settings in Europe and North America) | Minor concerns regarding adequacy | Moderate confidence | Due to minor concerns regarding coherence and adequacy, and moderate concerns regarding methodological limitations and relevance |
| Experiences of companionship | ||||||||
| Women’s experiences | ||||||||
| 26 | Women stated different preferences for their desired companion, including their husband or male partner, sister, mother, mother‐in‐law, doula, or a combination of different people. Regardless of which person they preferred, women who wanted a labour companion present during labour and childbirth expressed the need for this person to be a caring, compassionate, and trustworthy advocate. | Abushaikha 2012; Afulani 2018; Akhavan 2012a; Alexander 2014; Berg 2006; Bondas‐Salonen 1998; Campero 1998; Dodou 2014; Fathi 2017; Hunter 2012; Kabakian‐Khasholian 2015; Khresheh 2010; Lundgren 2010; Pafs 2016; Price 2007; Qian 2001; Sapkota 2012; Shimpuku 2013; Somers‐Smith 1999; Torres 2015 | Minor concerns regarding methodological limitations due to issues with recruitment, reflexivity, ethical considerations, and data analysis | Very minor concerns regarding coherence | Very minor concerns regarding relevance | Very minor concerns regarding adequacy | High confidence | Due to very minor concerns regarding coherence, relevance and adequacy, and minor concerns regarding methodological limitations |
| 27 | Women described the desire for a happy and healthy birth for both themselves and their babies. Support provided by doulas and companions paved the way for them to have a positive birth experience, as the support facilitated them to feel safe, strong, confident and secure. | Abushaikha 2012; Abushaikha 2013; Akhavan 2012a; Alexander 2014; Berg 2006; Bondas‐Salonen 1998; Campero 1998; Darwin 2016; Dodou 2014; Gilliland 2011; Hunter 2012; Kabakian‐Khasholian 2015; Khresheh 2010; Koumouitzes‐Douvia 2006; Ledenfors 2016; Lundgren 2010; McGarry 2016; Price 2007; Sapkota 2012; Schroeder 2005; Torres 2015 | Moderate concerns regarding methodological limitations due to issues regarding reflexivity, recruitment, research design, ethical considerations and data analysis | Minor concerns regarding coherence | Minor concerns regarding relevance | Minor concerns regarding adequacy | High confidence | Due to minor concerns regarding coherence, relevance, and adequacy, and moderate concerns regarding methodological limitations |
| 28 | Immigrant, refugee, and foreign‐born women resettled in high‐income countries highlighted how community‐based doulas (e.g. someone from their ethnic/religious/cultural community trained as a doula) were an important way for them to receive culturally competent care. | Akhavan 2012a; Hardeman 2016; LaMancuso 2016; Stevens 2011 | Moderate concerns regarding methodological limitations due to issues with research design, recruitment, reflexivity and ethical considerations | Minor concerns regarding coherence | Moderate concerns regarding relevance due to evidence from a limited range of contexts | Serious concerns regarding adequacy due to 4 contributing studies with moderately thick data | Low confidence | Due to minor concerns regarding coherence, moderate concerns regarding methodological limitations and relevance, and serious concerns due to adequacy. |
| 29 | Some women were concerned that their male partners would have diminished sexual attraction to them if they witnessed the birth. Likewise, some men believed that it is taboo to see a female partner give birth because of the risk of a loss of sexual interest. | Abushaikha 2013; Afulani 2018; Kululanga 2012; Pafs 2016; Sapkota 2012 | Minor concerns regarding methodological limitations | Minor concerns regarding coherence | Moderate concerns regarding relevance due to evidence from limited contexts predominantly in low‐ and middle‐income country settings | Serious concerns regarding adequacy due to 5 contributing studies with thin data | Moderate confidence | Due to minor concerns regarding methodological limitations and coherence, moderate concerns regarding relevance, and serious concerns regarding adequacy |
| 30 | Some women felt embarrassed or shy to have a male partner as a companion present throughout labour and childbirth. | Abushaikha 2013; Afulani 2018; Alexander 2014; Sapkota 2012 | Minor concerns regarding methodological limitations | Minor concerns regarding coherence | Moderate concerns regarding relevance due to evidence from limited contexts predominantly in LMIC settings | Serious concerns regarding adequacy due to 4 contributing studies with thin data | Low confidence | Due to minor concerns regarding methodological limitations and coherence, moderate concerns regarding relevance, and serious concerns regarding adequacy |
| 31 | Women who did not have a companion may view the lack of support as a form of suffering, stress and fear that made their birth experience more challenging. These women detailed experiences of poor quality of care that included mistreatment, poor communication, and neglect that made them feel vulnerable and alone. | Afulani 2018; Alexander 2014; Campero 1998; Chadwick 2014; Fathi 2017; Khresheh 2010; Pafs 2016 | Minor concerns regarding methodological limitations | Minor concerns regarding coherence | Moderate concerns regarding relevance due to evidence from limited contexts predominantly in LMIC settings | Minor concerns regarding adequacy due to 7 contributing studies with reasonably thick data | Moderate confidence | Due to minor concerns regarding methodological limitations, coherence, and adequacy, and moderate concerns regarding relevance |
| 32 | Some women described having their male partners present as an essential part of the birth process, which facilitated bonding between the father and the baby, the couple, and as a family. | Abushaikha 2012; Bondas‐Salonen 1998; Price 2007 | Minor concerns regarding methodological limitations | Minor concerns regarding coherence | Moderate concerns regarding relevance due to evidence from limited contexts predominantly in middle‐ and high‐income settings | Serious concerns regarding adequacy due to 3 contributing studies with thin data | Low confidence | Due to minor concerns regarding methodological limitations and coherence, moderate concerns regarding relevance, and serious concerns regarding adequacy |
| 33 | Most women who had a doula present described doulas as motherly, sisterly, or like family, suggesting a high level of relational intimacy. | Berg 2006; Coley 2016; Hunter 2012; Koumouitzes‐Douvia 2006; McGarry 2016 | Moderate concerns regarding methodological limitations due to issues regarding reflexivity, recruitment and ethical considerations | Minor concerns regarding coherence | Serious concerns regarding relevance due to evidence from limited contexts in high‐income settings only | Moderate concerns regarding adequacy due to 5 contributing studies with moderately thick data | Low confidence | Due to minor concerns regarding coherence, moderate concerns regarding methodological limitations and adequacy, and serious concerns regarding relevance |
| Male partner’s experiences | ||||||||
| 34 | Male partners had three main motivations for acting as a labour companion for their female partner: curiosity, woman’s request, and peer encouragement, and were in agreement that ultimately it should be the woman’s choice about who is allowed to be present. | Bondas‐Salonen 1998; Chapman 1990; Kululanga 2012; Longworth 2011; Pafs 2016; Sapkota 2012; Somers‐Smith 1999 | Minor concerns regarding methodological limitations | Minor concerns regarding coherence | Minor concerns regarding relevance | Moderate concerns regarding adequacy due to 5 contributing studies with relatively thin data | Moderate confidence | Due to minor concerns regarding methodological limitations, coherence, and relevance, and moderate concerns regarding adequacy |
| 35 | Men who acted as labour companions for their female partners felt that their presence made a positive impact on themselves as individuals. | Kululanga 2012; Sapkota 2012 | Minor concerns regarding methodological considerations due to issues with reflexivity and recruitment | Minor concerns regarding coherence | Serious concerns regarding relevancy due to partial evidence from a limited range of contexts and only low‐income countries | Serious concerns regarding adequacy due to 2 contributing studies with thin data | Low confidence | Due to minor concerns regarding methodological considerations and coherence, and serious concerns regarding relevancy and adequacy. |
| 36 | Men who acted as labour companions for their female partners felt that their presence made a positive impact on their relationship with their female partner and the new baby. | Dodou 2014; Kululanga 2012; Sapkota 2012 | Minor concerns regarding methodological considerations due to issues with reflexivity and recruitment | Minor concerns regarding coherence | Serious concerns regarding relevancy due to partial evidence from a limited range of contexts and only LMICs | Serious concerns regarding adequacy due to 3 contributing studies with thin data | Low confidence | Due to minor concerns regarding methodological considerations and coherence, and serious concerns regarding relevancy and adequacy. |
| 37 | Men who acted as labour companions for their female partners may feel scared, anxious or helpless when witnessing their partners in pain during labour and childbirth. | Fathi 2017; Kaye 2014; Kululanga 2012; Sapkota 2012 | Minor concerns regarding methodological considerations due to issues with reflexivity, research design and recruitment | Minor concerns regarding coherence | Serious concerns regarding relevancy due to partial evidence from a limited range of contexts and only low‐income countries | Serious concerns regarding adequacy due to 4 contributing studies with moderately thick data | Low confidence | Due to minor concerns regarding methodological considerations and coherence, and serious concerns regarding relevancy and adequacy. |
| 38 | Some lay companions (both male and female) were deeply impacted by witnessing a woman's pain during labour. Observing this pain caused feelings of frustration and fear, as they felt that there was nothing that they could do to help alleviate their pain. | Abushaikha 2013; Chandler 1997; Chapman 1990; Fathi 2017; Kabakian‐Khasholian 2015; Kululanga 2012; Sapkota 2012 | Moderate concerns regarding methodological limitations due to issues regarding reflexivity, recruitment, research design, data analysis and ethical considerations | Minor concerns regarding coherence | Minor concerns regarding relevance | Moderate concerns regarding adequacy due to 7 contributing studies with relatively thin data | Moderate confidence | Due to minor concerns regarding coherence and relevance, and moderate concerns regarding methodological limitations and adequacy |
| 39 | Some male partners felt that they were not well integrated into the care team or decision‐making. These men felt that their presence was tolerated by healthcare providers, but was not a necessary role. They relied on cues from the woman and healthcare provider for when and how to give support, but were often afraid to ask questions to avoid being labelled as difficult. | Bäckström 2011; Chandler 1997; Kaye 2014; Kululanga 2012; Longworth 2011; Somers‐Smith 1999 | Moderate concerns regarding methodological limitations due to issues regarding research design, reflexivity, recruitment, and ethical considerations | Minor concerns regarding coherence | Moderate concerns regarding relevance due to evidence from limited contexts (predominantly high‐income countries) | Moderate concerns regarding adequacy due to 6 contributing studies with relatively thick data | Moderate confidence | Due to minor concerns regarding coherence, and moderate concerns regarding methodological limitations, relevance, and adequacy. |
| Doulas’ experiences | ||||||||
| 40 | Doulas often met with women, and sometimes their partners, prior to the birth to establish a relationship with them. This helped to manage expectations, and mentally and physically prepare the woman and her partner for childbirth. | Akhavan 2012b; Berg 2006; Coley 2016; Darwin 2016; Koumouitzes‐Douvia 2006; Lundgren 2010; Shlafer 2015; Stevens 2011; Torres 2015 | Moderate concerns regarding methodological limitations due to issues regarding research design, recruitment, reflexivity, and ethical considerations | Minor concerns regarding coherence | Moderate concerns regarding relevance due to evidence from limited contexts where doula studies took place (high‐income countries) | Minor concerns regarding adequacy | Moderate confidence | Due to minor concerns regarding coherence and adequacy, and moderate concerns regarding methodological limitations and relevance |
| 41 | Doulas believed that one of their key responsibilities was to build rapport and mutual trust with the woman, in order to improve her birth experience. This relationship was foundational for the doulas to give effective support, and for the women to feel comfortable enough to let go. Doulas built rapport by communicating, providing practical support, comforting and relating to the woman. | Berg 2006; Coley 2016; de Souza 2010; Gilliland 2011; Hunter 2012; Koumouitzes‐Douvia 2006; McGarry 2016; Shlafer 2015; Thorstensson 2008 | Moderate concerns regarding methodological limitations due to issues with research design, reflexivity, recruitment, ethical considerations, and data analysis | Minor concerns regarding coherence | Moderate concerns regarding relevance due to evidence from limited contexts (predominantly high‐income settings in Europe and North America) | Minor concerns regarding adequacy | Moderate confidence | Due to minor concerns regarding coherence and adequacy, and moderate concerns regarding methodological limitations and relevance. |
| 42 | Doulas found that the experience of providing support to women in labour could have a positive personal impact on themselves. Some found that acting as a doula built their self‐confidence, made them feel like they were making a difference, and provided a sense of fulfilment. | Hardeman 2016; Hunter 2012; McGarry 2016; Thorstensson 2008 | Moderate concerns regarding methodological limitations due to issues with recruitment, reflexivity and ethical considerations | Minor concerns regarding coherence | Serious concerns regarding relevance due to limited evidence from limited contexts (all high‐income countries) | Serious concerns regarding adequacy due to 4 contributing studies with thin data | Low confidence | Due to minor concerns regarding coherence, moderate concerns regarding methodological limitations, and serious concerns regarding relevance and adequacy |
| LMICs: low‐ and middle‐income countries | ||||||||
Appendix 3. Critical appraisal of included studies
| Author/year | Is there a statement of research aims? | Is a qualitative approach justified? | Was the research design appropriate to address the aims? | Was the recruitment strategy appropriate to address the aims? | Was the role of the researcher/ reflexivity described? | Have ethical issues been considered? | Was the data analysis sufficiently clear and rigorous? | Were the findings supported by the evidence? | Overall assessment |
| Abushaikha 2012 | Yes | Yes | Partial ‐ FGDs and IDIs with women took place in the hospital shortly after birth | Unclear how participants were recruited | Partial ‐ researchers described as maternity nurse researchers but no discussion on how this might influence data collection or analysis | Yes | Yes | Yes | Moderate concerns |
| Abushaikha 2013 | Yes | Yes | Partial ‐ FGDs and IDIs with women took place in the hospital shortly after birth | Unclear how participants were recruited | Partial ‐ researchers described as maternity nurse researchers but no discussion on how this might influence data collection or analysis | Yes | Yes | Yes | Moderate concerns |
| Afulani 2018 | Yes | Yes | Yes | Yes | Partial ‐ researchers described the data collectors but no discussion on how this might influence data collection or analysis | Yes | Yes | Yes | Minor concerns |
| Akhavan 2012a | Yes | Yes | Yes | Unclear how participants were recruited | No | Partial ‐ mentions consent process but not IRB approval | Yes | Yes | Moderate concerns |
| Akhavan 2012b | Yes | Yes | Yes | Unclear how participants were recruited | No | Partial ‐ mentions consent process but not IRB approval | Yes | Yes | Moderate concerns |
| Alexander 2014 | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Minor concerns |
| Bäckström 2011 | Yes | Yes | Yes | Partial ‐ male partners recruited by midwives providing care, which may introduce bias | No | Yes | Yes | Yes | Minor concerns |
| Berg 2006 | Yes | Yes | Yes | Partial ‐ women were recruited through their doulas, which may introduce bias | No | Yes | Yes | Yes | Moderate concerns |
| Bondas‐Salonen 1998 | Yes | Yes | Yes | Unclear how participants were recruited | No | Yes | Yes | Yes | Minor concerns |
| Brüggemann 2014 | Yes | Yes | Yes | Unclear how participants were recruited | No | Yes | Yes | Yes | Minor concerns |
| Campero 1998 | Yes | Yes | Yes | Unclear how participants were recruited | No | Partial ‐ mentions consent process but not IRB approval | Yes | Yes | Minor concerns |
| Chadwick 2014 | Yes | Yes | Yes | Partial ‐ women recruited through a home visiting programme, which may introduce bias | No | Yes | Yes | Yes | Minor concerns |
| Chandler 1997 | Yes | Yes | Yes | Partial ‐ unclear how the "secondary informants" became participants | No | Yes | Yes | Partial | Moderate concerns |
| Chapman 1990 | Yes | Yes | Yes | Unclear how participants were recruited | No | Partial ‐ mentions consent process but not IRB approval | Yes | Yes | Moderate concerns |
| Coley 2016 | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Minor concerns |
| Darwin 2016 | Yes | Yes | Yes | Partial ‐ women recruited finished support services before the time of the study (2012) and may have given birth up to six years previously, may introduce bias | No | Yes | Yes | Yes | Moderate concerns |
| Dodou 2014 | Yes | Yes | Partial ‐ IDIs took place in the rooming‐in unit within 24 h after birth | Unclear how participants were recruited | No | Yes | Yes | Partial ‐ some quotations are disconnected from author interpretation | Moderate concerns |
| de Souza 2010 | Yes | Yes | Yes | Yes | No | Yes | Partial ‐ data analysis process somewhat unclear | Partial ‐ some quotations are disconnected from author interpretation | Moderate concerns |
| Gentry 2010 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Minor concerns |
| Gilliland 2011 | Yes | Yes | Yes | Partial ‐ unclear how women were recruited | No | Yes | Yes | Yes | Minor concerns |
| Hardeman 2016 | Yes | Yes | Partial ‐ triangulation of IDIs with other data collection methods or participants would have been helpful | Yes | No | Yes | Yes | Yes | Moderate concerns |
| Harte 2016 | Yes | Yes | Yes | Unclear how participants were recruited | No | Partial ‐ mentions IRB approval but unclear consent process | Yes | Yes | Moderate concerns |
| Horstman 2017 | Partial | Yes | Yes | Partial ‐ women recruited by healthcare providers | No | Unclear ‐ no mention of consent or IRB approval | Partial ‐ unclear what is new analysis and what is existing research | Yes | Serious concerns |
| Hunter 2012 | Yes | Yes | Yes | Unclear how participants were recruited | No | Partial ‐ mentions IRB approval but unclear consent process | Yes | Yes | Moderate concerns |
| Kabakian‐Khasholian 2015 | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Moderate concerns |
| Kaye 2014 | Yes | Yes | Partial ‐ men were interviewed while their partner was in labour in a high‐dependency ward | Partial ‐ men recruited whose partners were in a high‐dependency unit, but the objective was to explore all men | No | Yes | Yes | Yes | Moderate concerns |
| Khresheh 2010 | Yes | Yes | Yes | Partial ‐ large nonresponse rate and only 1 attempted contact per potential participant | No | Yes | Partial ‐ limited description of data analysis | Yes | Serious concerns |
| Koumouitzes‐Douvia 2006 | Yes | Yes | Yes | Yes | No | Unclear ‐ no mention of consent process or IRB approval | Yes | Yes | Moderate concerns |
| Kululanga 2012 | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Minor concerns |
| Lagendyk 2005 | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Minor concerns |
| LaMancuso 2016 | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Minor concerns |
| Ledenfors 2016 | Yes | Yes | Yes | Partial ‐ there were 2 recruitment methods but resulted in a small self‐selected sample which may introduce bias | No | Partial ‐ mentions consent process but not IRB approval | Yes | Yes | Moderate concerns |
| Longworth 2011 | Yes | Yes | Yes | Partial ‐ participants recruited through parentcraft classes, which may introduce bias | Yes | Partial ‐ mentions IRB approval but unclear consent process | Yes | Yes | Moderate concerns |
| Lundgren 2010 | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Minor concerns |
| Maher 2004 | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Minor concerns |
| McGarry 2016 | Not clear | Yes | Yes | Unclear how participants were recruited | No | Yes | Yes | Yes | Moderate concerns |
| McLeish 2018 | Yes | Yes | Partial ‐ triangulation of IDIs with other data collection methods or participants would have been helpful | Partial ‐ doula project coordinators identified potential participants, but unclear how they were identified (all women, or some women and some women, how were they chosen?) | Yes | Yes | Yes | Yes | Minor concerns |
| Pafs 2016 | Yes | Yes | Yes | Unclear how participants were recruited | Yes | Yes | Yes | Yes | Minor concerns |
| Premberg 2011 | Yes | Yes | Yes | No | Partial ‐ stated that researcher viewpoints were taken into consideration, but not what the viewpoints were | Partial ‐ mentions IRB approval but unclear consent process | Yes | Yes | Moderate concerns |
| Price 2007 | Yes | Yes | Yes | Partial ‐ only women with unassisted vaginal birth included but population of interest is all women | No | Yes | Yes | Yes | Minor concerns |
| Qian 2001 | Yes | Yes | Yes | Unclear how participant was recruited | No | Partial ‐ mentions IRB approval but unclear consent process | Partial ‐ limited description of data analysis | Partial ‐ limited qualitative data presented | Moderate concerns |
| Sapkota 2012 | Yes | Yes | Yes | Unclear how participants were recruited | No | Yes | Yes | Yes | Moderate concerns |
| Schroeder 2005 | Yes | Yes | Partial ‐ IDIs took place within 1 week after birth | Unclear ‐ it seems that all incarcerated pregnant women used doula services and were interviewed, but unclear how they were recruited or how information was provided | No | Partial ‐ mentions IRB approval but unclear consent process | Partial ‐ limited description of data analysis | Partial ‐ some quotations are disconnected from author interpretation | Serious concerns |
| Shimpuku 2013 | Yes | Yes | Partial ‐ IDIs took place 24 h after birth | Unclear how participants were recruited | Yes | Yes | Yes | Yes | Minor concerns |
| Shlafer 2015 | Yes | Yes | Partial ‐ IDIs only with doulas, but incarcerated women's perspectives also important to assess acceptability of doula care | Unclear how participants were recruited | No | Yes | Yes | Yes | Minor concerns |
| Somers‐Smith 1999 | Yes | Yes | Yes | Unclear how participants were recruited | No | Yes | Yes | Yes | Moderate concerns |
| Stevens 2011 | Yes | Yes | Partial ‐ very small sample size | Unclear how participants were recruited | Partial ‐ states the background of the researchers but no discussion on how this might influence data collection or analysis | Unclear | Yes | Yes | Moderate concerns |
| Thorstensson 2008 | Yes | Yes | Yes | Unclear how participants were recruited | No | Partial ‐ mentions IRB approval but unclear consent process | Yes | Yes | Moderate concerns |
| Torres 2013 | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Minor concerns |
| Torres 2015 | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Minor concerns |
| FGD: focus group discussion; IDI: in‐depth interview; IRB: Institutional Review Board | |||||||||
Appendix 4. Other related reviews
| Cochrane Reviews |
|
Bohren 2017 (systematic review of interventions) Munabi‐Babigumira 2017 (qualitative evidence synthesis) |
| Literature reviews |
|
Rosen 2004 Knape 2013 Steel 2015 Kabakian‐Khasholian 2017 Beake 2018 |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Abushaikha 2012.
| Aims | To understand the role of fathers during childbirth | |
| Setting | Syria; major urban governmental obstetrical hospital in Tartous | |
| Type of companion | Lay person ‐ male partner | |
| Notes | ‐ | |
Abushaikha 2013.
| Aims | To explore barriers to fathers’ presence during childbirth | |
| Setting | Syria; major urban governmental obstetrical hospital in Tartous | |
| Type of companion | Lay person ‐ male partner | |
| Notes | ‐ | |
Afulani 2018.
| Aims | To explore women's and providers' perceptions of birth companionship | |
| Setting | Kenya; rural | |
| Type of companion | Lay person ‐ not specified | |
| Notes | ‐ | |
Akhavan 2012a.
| Aims | To explore foreign‐born women's experiences of community‐based doula support | |
| Setting | Sweden; Våstra Götaland region | |
| Type of companion | Community‐based doula | |
| Notes | ‐ | |
Akhavan 2012b.
| Aims | To explore midwives' experiences of doula support for immigrant women | |
| Setting | Sweden; Våstra Götaland region | |
| Type of companion | Community‐based doula | |
| Notes | ‐ | |
Alexander 2014.
| Aims | Explore pregnant women's attitudes towards including a lay companion as a source of social support during labour and childbirth | |
| Setting | Ghana; rural Catholic referral hospital in Apam | |
| Type of companion | Lay person ‐ not specified | |
| Notes | ‐ | |
Berg 2006.
| Aims | To explore women’s perspectives of doula support | |
| Setting | Sweden; Gothenburg and Stockholm | |
| Type of companion | Private doulas | |
| Notes | ‐ | |
Bondas‐Salonen 1998.
| Aims | To explore women's experiences of their partners' presence during labour and childbirth | |
| Setting | Finland; urban and rural | |
| Type of companion | Lay person ‐ male partner | |
| Notes | ‐ | |
Brüggemann 2014.
| Aims | To explore nurses' reports of health service acceptability of labour companions during childbirth | |
| Setting | Brazil; Santa Cataraina obstetric centres, some of which allowed companions and other did not allow them | |
| Type of companion | Lay person ‐ companion of choice | |
| Notes | ‐ | |
Bäckström 2011.
| Aims | To describe first‐time fathers' experiences of support during labour | |
| Setting | Sweden; south‐western country hospital | |
| Type of companion | Lay companion ‐ male partner | |
| Notes | ‐ | |
Campero 1998.
| Aims | To explore women's perspectives of doula support during labour and childbirth | |
| Setting | Mexico; maternity hospital in Mexico City | |
| Type of companion | Doula | |
| Notes | ‐ | |
Chadwick 2014.
| Aims | To explore women’s negative experiences during childbirth in public healthcare settings | |
| Setting | South Africa; informal settlements in Cape Town | |
| Type of companion | No companion | |
| Notes | ‐ | |
Chandler 1997.
| Aims | To explore first‐time fathers' expectations and experiences of childbirth | |
| Setting | Canada | |
| Type of companion | Lay person ‐ male partner | |
| Notes | ‐ | |
Chapman 1990.
| Aims | To describe and explain expectant fathers' experiences during labour and birth, including the roles adopted by expectant fathers during labour and birth and conditions associated with these roles | |
| Setting | USA: San Francisco Bay Area | |
| Type of companion | Lay person ‐ male partner | |
| Notes | ‐ | |
Coley 2016.
| Aims | To explore adolescent mothers' and doula’s perspectives of a doula‐support programme | |
| Setting | USA; southeastern region | |
| Type of companion | Doula | |
| Notes | ‐ | |
Darwin 2016.
| Aims | To explore disadvantaged women’s experiences with a trained volunteer doula service | |
| Setting | UK | |
| Type of companion | Doula | |
| Notes | ‐ | |
de Souza 2010.
| Aims | To explore doulas' experiences providing support during labour and childbirth | |
| Setting | Brazil; a municipal public hospital in Recife‐Pernambuco | |
| Type of companion | Doula | |
| Notes | ‐ | |
Dodou 2014.
| Aims | To explore women’s perception of birth companions in humanised childbirth | |
| Setting | Brazil; secondary‐level public hospital in Fortaleza/CE | |
| Type of companion | Lay person ‐ not specified | |
| Notes | ‐ | |
Fathi 2017.
| Aims | To explore Iranian mothers' experiences of labour and labour support | |
| Setting | Iran; Mashhad | |
| Type of companion | Lay person ‐ female | |
| Notes | ||
Gentry 2010.
| Aims | To explore the services doulas provide for disadvantaged pregnant and parenting adolescents who received support from a community‐based doula programme | |
| Setting | USA; southeastern region | |
| Type of companion | Community‐based doula | |
| Notes | ‐ | |
Gilliland 2011.
| Aims | To examine the functions and processes of emotional support strategies used by birth doulas | |
| Setting | Canada and USA | |
| Type of companion | Doula | |
| Notes | ‐ | |
Hardeman 2016.
| Aims | To characterise the intentions and motivations of racially and ethnically diverse women who chose to become doulas and to describe their early doula careers, and the experiences that sustain their work | |
| Setting | USA; Minneapolis, Minnesota | |
| Type of companion | Doula | |
| Notes | ‐ | |
Harte 2016.
| Aims | To explore inhibiting and facilitating design factors influencing childbirth supporters’ experiences | |
| Setting | Australia; a labour and birth room in a maternity unit of a metropolitan hospital | |
| Type of companion | Lay person ‐ male partner, female family members | |
| Notes | ‐ | |
Horstman 2017.
| Aims | To understand how doulas are communicatively situated in the master narrative of childbirth | |
| Setting | USA; Midwest | |
| Type of companion | Doula | |
| Notes | ‐ | |
Hunter 2012.
| Aims | To explore women's and doulas’ perspectives of labour support | |
| Setting | USA; a birth education centre in the Midwest | |
| Type of companion | Doula | |
| Notes | ‐ | |
Kabakian‐Khasholian 2015.
| Aims | To explore the perceptions of women, female family members, and healthcare providers on their acceptance of labour companionship | |
| Setting | Beirut, Lebanon; Damascus, Syria; Mansoura, Egypt | |
| Type of companion | Lay person ‐ female family member | |
| Notes | ‐ | |
Kaye 2014.
| Aims | To understand male involvement during pregnancy and childbirth by exploring men’s perceptions, experiences and practices | |
| Setting | Uganda; high‐dependency unit in Kampala | |
| Type of companion | Lay companion ‐ male partner | |
| Notes | ‐ | |
Khresheh 2010.
| Aims | To explore women’s experiences with receiving family support during labour | |
| Setting | Jordan; Al‐Karak government hospital | |
| Type of companion | Lay person ‐ female family member | |
| Notes | ‐ | |
Koumouitzes‐Douvia 2006.
| Aims | To explore the experiences of childbearing women who received doula support during the perinatal period | |
| Setting | USA; Puget Sound area of Washington state | |
| Type of companion | Doula | |
| Notes | ‐ | |
Kululanga 2012.
| Aims | To explore father’s experiences of being present at birth | |
| Setting | Malawi; two hospitals in Blantyre | |
| Type of companion | Lay person ‐ male partner | |
| Notes | ‐ | |
Lagendyk 2005.
| Aims | To document the process and outcome of an attempt to combine and institutionalise 2 grassroots health programmes that provided trained volunteers to support women through labour and childbirth in hospital | |
| Setting | Canada; rural regional health authority | |
| Type of companion | Doula | |
| Notes | ‐ | |
LaMancuso 2016.
| Aims | To explore Karen refugee women’s, community‐based doulas’, and medical providers’ perspectives on doula support for resettled refugee women | |
| Setting | USA; Karen refugee women resettled in Buffalo, New York | |
| Type of companion | Community‐based doula | |
| Notes | ‐ | |
Ledenfors 2016.
| Aims | To explore the perspectives of first‐time fathers present at childbirth | |
| Setting | Sweden; county in south east | |
| Type of companion | Lay person ‐ male partner | |
| Notes | ‐ | |
Longworth 2011.
| Aims | To explore the role, expectations and meanings that individual fathers ascribe to their presence at birth | |
| Setting | UK; northwest England | |
| Type of companion | Lay person ‐ male partner | |
| Notes | ‐ | |
Lundgren 2010.
| Aims | To describe women’s experiences of having a doula present during childbirth | |
| Setting | Sweden; 2 maternity hospitals in Gothenburg | |
| Type of companion | Doula | |
| Notes | ‐ | |
Maher 2004.
| Aims | To explore midwives’ perspectives of support people during labour and delivery | |
| Setting | Australia; 3 urban hospitals serving diverse populations in Melbourne | |
| Type of companion | Lay person ‐ not specified | |
| Notes | ‐ | |
McGarry 2016.
| Aims | To explore women’s and doulas’ perspectives of support for women with intellectual disabilities | |
| Setting | UK; rural county in England | |
| Type of companion | Doula | |
| Notes | ‐ | |
McLeish 2018.
| Aims | To explore volunteer doulas’ and disadvantaged mothers’ understanding and experience of the community doula role during labour and birth, and how that interrelates with their understanding and experience of the midwife's role | |
| Setting | England; Bradford, Hull and Essex | |
| Type of companion | Doula | |
| Notes | ‐ | |
Pafs 2016.
| Aims | To explore fathers’ perspectives on their roles during pregnancy and childbirth | |
| Setting | Rwanda; 3 public hospitals in Kigali | |
| Type of companion | Lay person ‐ male partner | |
| Notes | ‐ | |
Premberg 2011.
| Aims | To explore first‐time fathers’ experiences of childbirth | |
| Setting | Sweden; 2 labour wards in a university hospital in Gothenburg | |
| Type of companion | Lay person ‐ male partner | |
| Notes | ‐ | |
Price 2007.
| Aims | To explore women’s experiences with support during childbirth | |
| Setting | Canada; a tertiary care birth unit in the east | |
| Type of companion | Lay person ‐ not specified | |
| Notes | ‐ | |
Qian 2001.
| Aims | To explore women’s and providers’ views on social support, hospital environment, and care during childbirth | |
| Setting | China; 3 hospitals in Shanghai (urban) and one hospital in Jiangsu province (rural) | |
| Type of companion | Lay person ‐ male partner | |
| Notes | ‐ | |
Sapkota 2012.
| Aims | To explore husbands’ experiences of providing support during childbirth | |
| Setting | Nepal; a midwife‐run birthing centre and a public maternity hospital in Kathmandu | |
| Type of companion | Lay person ‐ male partner | |
| Notes | ‐ | |
Schroeder 2005.
| Aims | To explore incarcerated women’s experiences with doula support through a doula programme for incarcerated women | |
| Setting | USA; urban jails | |
| Type of companion | Doula | |
| Notes | ‐ | |
Shimpuku 2013.
| Aims | To understand women’s perceptions about their hospital birth experience, including what they experienced during attended births, how they assessed this birthing experience, and what attracted the women to deliver in the presence of skilled birth attendants | |
| Setting | Tanzania; a rural hospital in the North Central region | |
| Type of companion | Lay person ‐ not specified | |
| Notes | ‐ | |
Shlafer 2015.
| Aims | To assess the implementation of a doula support programme for incarcerated women, specifically
|
|
| Setting | USA; state prison in the Midwest | |
| Type of companion | Doula | |
| Notes | ‐ | |
Somers‐Smith 1999.
| Aims | To explore primigravid women's expectations of support from their partners during childbirth, and to assess whether that support was provided. To assess male partners' perspectives of their role as a supporter and how they thought they fulfilled that role | |
| Setting | UK; an urban and a peri‐urban antenatal clinic in Hampshire | |
| Type of companion | Lay person ‐ male partner | |
| Notes | ‐ | |
Stevens 2011.
| Aims | To explore midwives’ and doulas’ perspectives of doula support | |
| Setting | Australia; New South Wales | |
| Type of companion | Doula | |
| Notes | ‐ | |
Thorstensson 2008.
| Aims | To explore student midwives’ experiences offering continuous support during childbirth | |
| Setting | Sweden; a labour ward in a central hospital in the southwest | |
| Type of companion | Provider ‐ student midwife | |
| Notes | ‐ | |
Torres 2013.
| Aims | To examine strategies utilised by lactation consultants and doulas to navigate the occupational boundaries of the maternity care system and investigate what impact these strategies have on their ability to create change | |
| Setting | USA | |
| Type of companion | Doula | |
| Notes | ‐ | |
Torres 2015.
| Aims | To explore the role lactation consultants and doulas play in maternity care, whether these occupations are a reflection of the outsourcing of care, and how the existence of these types of paid support may illustrate transformations in care more broadly | |
| Setting | USA; Midwest | |
| Type of companion | Doula | |
| Notes | ‐ | |
NHS: National Health Service
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Adejoh 2018 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Alcantara 2016 | Not qualitative method of data collection and analysis |
| Anono 2018 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Banda 2010 | Not qualitative method of data collection and analysis |
| Behruzi 2010 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Behruzi 2011 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Behruzi 2014 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Binfa 2016 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Bowers 2002 | Not a primary study |
| Bramadat 1993 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Brodrick 2008 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Brookes 1991 | Not qualitative method of data collection and analysis |
| Bruggemann 2005 | Not a primary study |
| Bruggemann 2008 | Not a primary study |
| Cagle 1999 | Not a primary study |
| Callister 1992 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Carter 2002 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Chalmers 1987 | Not qualitative method of data collection and analysis |
| Chalmers 1994 | Not qualitative method of data collection and analysis |
| Chamberlain 2000 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Chaturvedi 2015 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Cheung 2009 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Chi 2018 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Cipolletta 2011 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Corbett 2012 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Crissman 2013 | The phenomena of interest is not labour companionship during childbirth in facilities |
| de Melo 2013 | Not a primary study |
| Dim 2011 | Not a qualitative method of data collection and analysis. |
| DiMatteo 1993 | Not qualitative method of data collection and analysis |
| Duggan 2012 | The phenomena of interest is not labour companionship during childbirth in facilities |
| El‐Nemer 2006 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Essoka 2000 | Not qualitative method of data collection and analysis |
| Etowa 2012 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Flemming 2009 | Not a primary study |
| Gibbins 2001 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Green 2007 | Not a primary study |
| Grewal 2008 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Hallgren 1999 | The phenomena of interest is not labour companionship |
| Hatamleh 2013 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Hoga 2011 | Not a primary study |
| Howarth 2011 | Not facility‐based births (i.e. home births) |
| Ith 2013 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Johansson 2015 | Not a primary study |
| Karlstrom 2015 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Kempe 2013 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Kgokgothwane 2002 | Not qualitative method of data collection and analysis |
| Larkin 2012 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Maimbolwa 2003 | The phenomenon of interest is not labour companionship during childbirth in health facilities |
| Maluka 2018 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Mami 2013 | Not facility‐based births (i.e. home births) |
| Maputle 2018 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Martins 2008 | Not facility‐based births (i.e. home births) |
| McLemore 2017 | Not a primary study |
| Mselle 2018 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Ojelade 2017 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Papagni 2006 | Not qualitative method of data collection and analysis |
| Pascali‐Bonaro 2004 | Not a primary study |
| Pyone 2014 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Ramashwar 2008 | Not qualitative method of data collection and analysis |
| Raven 2015 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Richards 1992 | Not a primary study |
| Sapkota 2014 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Sauls 2004 | Not qualitative method of data collection and analysis |
| Shahoei 2014 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Shimpuku 2010 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Simmonds 2012 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Spiby 2016 | Not qualitative method of data collection and analysis |
| Steel 2013 | Not qualitative method of data collection and analysis |
| Steel 2015 | Not a primary study |
| Story 2012 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Tarlazzi 2015 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Theuring 2010 | Not qualitative method of data collection and analysis |
| Udofia 2012 | Not qualitative method of data collection and analysis |
| Vikstrom 2016 | The phenomena of interest is not labour companionship during childbirth in facilities |
| Yuenyong 2008 | Not a primary study |
Characteristics of studies awaiting assessment [ordered by study ID]
Bruggemann 2007.
| Notes | Portuguese‐language article |
Bruggemann 2016.
| Notes | Portuguese‐language article |
de Carvalho 2003.
| Notes | Portuguese‐language article |
de Souza 2015.
| Notes | Portuguese‐language article |
Florentino 2007.
| Notes | Portuguese‐language article |
Fu 2001.
| Notes | Chinese‐language article |
Hoga 2007.
| Notes | Portuguese‐language article |
Jamas 2013.
| Notes | Portuguese‐language article |
Nakano 2007.
| Notes | Portuguese‐language article |
Perazzini 2017.
| Notes | Portuguese‐language article |
Ribeiro 2018.
| Notes | Portuguese‐language article |
Rocha 2018.
| Notes | Portuguese‐language article |
Rossi 2016.
| Notes | Portuguese‐language article |
Santos 2009.
| Notes | Portuguese‐language article |
Vanuzzi 2017.
| Notes | Portuguese‐language article |
Differences between protocol and review
Emma Allanson was a co‐author on this review protocol. We appreciate her contributions to the conceptualisation of the protocol design.
We have modified the wording of the objectives. The objectives listed in the protocol were:
The overall objective of the review is to describe and explore the perceptions and experiences of women, partners, community members, healthcare providers and administrators, and other key stakeholders who have experience with a labour companion. The review has the following objectives:
To identify, appraise and synthesise qualitative research evidence on women’s, partners’, community members’, healthcare providers’ and administrators’, and other key stakeholders’ perceptions and experiences regarding labour companionship in health facilities
To identify barriers and facilitators to successful implementation and sustainability of labour companionship.
To explore how the findings of this review can enhance our understanding of the related intervention review (Hodnett 2013).
Contributions of authors
MAB and ÖT designed this synthesis. MAB led the review process with input and support from BB, HMK and ÖT.
Sources of support
Internal sources
No sources of support supplied
External sources
-
Department of Reproductive Health and Research, World Health Organization, Switzerland.
Other
-
Department for International Development, UK.
Project number 300342‐104
Declarations of interest
MAB also led the update of the Cochrane intervention review 'Continuous support for women during childbirth' and is an Associate Editor with Cochrane Effective Practice and Organisation of Care. BB: none HMK: none ÖT: none
Edited (no change to conclusions)
References
References to studies included in this review
Abushaikha 2012 {published data only}
- Abushaikha L, Massah R. The roles of the father during childbirth: the lived experiences of Arab Syrian parents. Health Care for Women International 2012;33(2):168‐81. [DOI] [PubMed] [Google Scholar]
Abushaikha 2013 {published data only}
- Abushaikha L, Massah R. Perceptions of barriers to paternal presence and contribution during childbirth: an exploratory study from Syria. Birth 2013;40(1):61‐6. [DOI] [PubMed] [Google Scholar]
Afulani 2018 {published data only}
- Afulani P, Kusi C, Kirumbi L, Walker D. Companionship during facility‐based childbirth: results from a mixed‐methods study with recently delivered women and providers in Kenya. BMC Pregnancy Childbirth 2018;18(1):150. [DOI] [PMC free article] [PubMed] [Google Scholar]
Akhavan 2012a {published data only}
- Akhavan S, Edge D. Foreign‐born women's experiences of community‐based doulas in Sweden—a qualitative study. Health Care for Women International 2012;33(9):833‐48. [DOI] [PubMed] [Google Scholar]
Akhavan 2012b {published data only}
- Akhavan S, Lundgren I. Midwives' experiences of doula support for immigrant women in Sweden‐‐a qualitative study. Midwifery 2012;28(1):80‐5. [DOI] [PubMed] [Google Scholar]
Alexander 2014 {published data only}
- Alexander A, Mustafa A, Emil S A, Amekah E, Engmann C, Adanu R, et al. Social support during delivery in rural central Ghana: a mixed methods study of women's preferences for and against inclusion of a lay companion in the delivery room. Journal of Biosocial Science 2014;46(5):669‐85. [DOI] [PubMed] [Google Scholar]
Bäckström 2011 {published data only}
- Bäckström C, Hertfelt Wahn E. Support during labour: first‐time fathers’ descriptions of requested and received support during the birth of their child. Midwifery 2011;27(1):67‐73. [DOI] [PubMed] [Google Scholar]
Berg 2006 {published data only}
- Berg M, Terstad A. Swedish women's experiences of doula support during childbirth. Midwifery 2006;22(4):330‐8. [DOI] [PubMed] [Google Scholar]
Bondas‐Salonen 1998 {published data only}
- Bondas‐Salonen T. How women experience the presence of their partners at the births of their babies. Qualitative Health Research 1998;8(6):784‐800. [Google Scholar]
Brüggemann 2014 {published data only}
- Brüggemann OM, Ebsen ESi, Oliveira ME, Gorayeb MK, Ebele RR. Reasons which lead the health services not to allow the presence of the birth companion: nurses' discourses. Texto & Contexto Enfermagem 2014;23(2):270‐7. [Google Scholar]
Campero 1998 {published data only}
- Campero L, Garcia C, Diaz C, Ortiz O, Reynoso S. Alone, I wouldn't have known what to do: a qualitative study on social support during labor and delivery in Mexico. Social Science and Medicine 1998;47(3):395‐403. [DOI] [PubMed] [Google Scholar]
Chadwick 2014 {published data only}
- Chadwick RJ, Cooper D, Harries J. Narratives of distress about birth in South African public maternity settings: a qualitative study. Midwifery 2014;30(7):862‐8. [DOI] [PubMed] [Google Scholar]
Chandler 1997 {published data only}
- Chandler S, Field P A. Becoming a father. First‐time fathers' experience of labor and delivery. Journal of Nurse‐Midwifery 1997;42(1):17‐24. [DOI] [PubMed] [Google Scholar]
Chapman 1990 {published data only}
- Chapman LL. Co‐laboring: maintaining and redefining the expectant fathers' role during labor and birth [DNS Dissertation]. San Francisco: University of California San Francisco, 1990. [Google Scholar]
Coley 2016 {published data only}
- Coley SL, Nichols TR. Understanding factors that influence adolescent mothers' doula use: a qualitative study. Journal of Perinatal Education 2016;25(1):46‐55. [DOI] [PMC free article] [PubMed] [Google Scholar]
Darwin 2016 {published data only}
- Darwin Z, Green J, McLeish J, Willmot H, Spiby H. Evaluation of trained volunteer doula services for disadvantaged women in five areas in England: women's experiences. Health & Social Care in the Community 2016;25:25. [DOI] [PubMed] [Google Scholar]
de Souza 2010 {published data only}
- Souza KR, Dias MD. Oral history: experience of doulas in the care of women. Acta Paulista de Enfermagem 2010;23(4):493‐9. [Google Scholar]
Dodou 2014 {published data only}
- Dodou HD, Rodrigues DP, Guerreiro EM, Cavalcante Guedes MV, Nery do Lago P, Sousa de Mesquita N. The contribution of the companion to the humanization of delivery and birth: perceptions of puerperal women. Anna Nery School Journal of Nursing / Escola Anna Nery Revista de Enfermagem 2014;18(2):262‐9. [Google Scholar]
Fathi 2017 {published data only}
- Fathi Najafi T, Latifnejad Roudsari R, Ebrahimipour H. The best encouraging persons in labor: a content analysis of Iranian mothers' experiences of labor support. PLoS One 2017;12(7):e0179702. [DOI] [PMC free article] [PubMed] [Google Scholar]
Gentry 2010 {published data only}
- Gentry QM, Nolte KM, Gonzalez A, Pearson M, Ivey S. "Going beyond the call of doula": a grounded theory analysis of the diverse roles community‐based doulas play in the lives of pregnant and parenting adolescent mothers. Journal of Perinatal Education 2010;19(4):24‐40. [DOI] [PMC free article] [PubMed] [Google Scholar]
Gilliland 2011 {published data only}
- Gilliland AL. After praise and encouragement: emotional support strategies used by birth doulas in the USA and Canada. Midwifery 2011;27(4):525‐31. [DOI] [PubMed] [Google Scholar]
Hardeman 2016 {published data only}
- Hardeman RR, Kozhimannil KB. Motivations for entering the doula profession: perspectives from women of color. Journal of Midwifery & Women's Health 2016;61(6):773‐80. [DOI] [PMC free article] [PubMed] [Google Scholar]
Harte 2016 {published data only}
- Harte JD, Sheehan A, Stewart SC, Foureur M. Childbirth supporters' experiences in a built hospital birth environment: exploring inhibiting and facilitating factors in negotiating the supporter role. HERD 2016;9(3):135‐61. [DOI] [PubMed] [Google Scholar]
Horstman 2017 {published data only}
- Horstman HK, Anderson J, Kuehl RA. Communicatively making sense of doulas within the U.S. master birth narrative: doulas as liminal characters. Health Communication 2017;32(12):1510‐9. [DOI] [PubMed] [Google Scholar]
Hunter 2012 {published data only}
- Hunter C. Intimate space within institutionalized birth: women's experiences birthing with doulas. Anthropology & Medicine 2012;19(3):315‐26. [DOI] [PubMed] [Google Scholar]
Kabakian‐Khasholian 2015 {published data only}
- Kabakian‐Khasholian T, El‐Nemer A, Bashour H. Perceptions about labor companionship at public teaching hospitals in three Arab countries. International Journal of Gynaecology & Obstetrics 2015;129(3):223‐6. [DOI] [PubMed] [Google Scholar]
Kaye 2014 {published data only}
- Kaye DK, Kakaire O, Nakimuli A, Osinde MO, Mbalinda SN, Kakande N. Male involvement during pregnancy and childbirth: men's perceptions, practices and experiences during the care for women who developed childbirth complications in Mulago Hospital, Uganda. BMC Pregnancy and Childbirth 2014;14:54. [DOI] [PMC free article] [PubMed] [Google Scholar]
Khresheh 2010 {published data only}
- Khresheh R, Barclay L. The lived experience of Jordanian women who received family support during labor. MCN. The American Journal of Maternal Child Nursing 2010;35(1):47‐51. [DOI] [PubMed] [Google Scholar]
Koumouitzes‐Douvia 2006 {published data only}
- Koumouitzes‐Douvia J, Carr CA. Women's perceptions of their doula support. Journal of Perinatal Education 2006;15(4):34‐40. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kululanga 2012 {published data only}
- Kululanga LI, Malata A, Chirwa E, Sundby J. Malawian fathers' views and experiences of attending the birth of their children: a qualitative study. BMC Pregnancy and Childbirth 2012;12:141. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lagendyk 2005 {published data only}
- Lagendyk LE, Thurston WE. A case study of volunteers providing labour and childbirth support in hospitals in Canada. Midwifery 2005;21(1):14‐22. [DOI] [PubMed] [Google Scholar]
LaMancuso 2016 {published data only}
- LaMancuso K, Goldman RE, Nothnagle M. "Can I Ask That?": perspectives on perinatal care after resettlement among Karen refugee women, medical providers, and community‐based doulas. Journal of Immigrant and Minority Health / Center for Minority Public Health 2016;18(2):428‐35. [DOI] [PubMed] [Google Scholar]
Ledenfors 2016 {published data only}
- Ledenfors A, Bertero C. First‐time fathers' experiences of normal childbirth. Midwifery 2016;40:26‐31. [DOI] [PubMed] [Google Scholar]
Longworth 2011 {published data only}
- Longworth HL, Kingdon CK. Fathers in the birth room: what are they expecting and experiencing? A phenomenological study. Midwifery 2011;27(5):588‐94. [DOI] [PubMed] [Google Scholar]
Lundgren 2010 {published data only}
- Lundgren I. Swedish women's experiences of doula support during childbirth. Midwifery 2010;26(2):173‐80. [DOI] [PubMed] [Google Scholar]
Maher 2004 {published data only}
- Maher J. Midwife interactions with birth support people in Melbourne, Australia. Midwifery 2004;20(3):273‐80. [DOI] [PubMed] [Google Scholar]
McGarry 2016 {published data only}
- McGarry A, Stenfert Kroese B, Cox R. How do women with an intellectual disability experience the support of a doula during their pregnancy, childbirth and after the birth of their child?. Journal of Applied Research in Intellectual Disabilities 2016;29(1):21‐33. [DOI] [PubMed] [Google Scholar]
McLeish 2018 {published data only}
- McLeish J, Redshaw M. A qualitative study of volunteer doulas working alongside midwives at births in England: mothers' and doulas' experiences. Midwifery 2018;56:53‐60. [DOI] [PubMed] [Google Scholar]
Pafs 2016 {published data only}
- Pafs J, Rulisa S, Musafili A, Essen B, Binder‐Finnema P. 'You try to play a role in her pregnancy' ‐ a qualitative study on recent fathers' perspectives about childbearing and encounter with the maternal health system in Kigali, Rwanda. Global Health Action 2016;9:31482. [DOI] [PMC free article] [PubMed] [Google Scholar]
Premberg 2011 {published data only}
- Premberg A, Carlsson G, Hellstrom AL, Berg M. First‐time fathers' experiences of childbirth‐‐a phenomenological study. Midwifery 2011;27(6):848‐53. [DOI] [PubMed] [Google Scholar]
Price 2007 {published data only}
- Price S, Noseworthy J, Thornton J. Women's experience with social presence during childbirth. MCN. The American Journal of Maternal Child Nursing 2007;32(3):184‐91. [DOI] [PubMed] [Google Scholar]
Qian 2001 {published data only}
- Qian X, Smith H, Zhou L, Liang J, Garner P. Evidence‐based obstetrics in four hospitals in China: an observational study to explore clinical practice, women's preferences and provider's views. BMC Pregnancy and Childbirth 2001;1(1):1. [DOI] [PMC free article] [PubMed] [Google Scholar]
Sapkota 2012 {published data only}
- Sapkota S, Kobayashi T, Takase M. Husbands' experiences of supporting their wives during childbirth in Nepal. Midwifery 2012;28(1):45‐51. [DOI] [PubMed] [Google Scholar]
- Sapkota S, Kobayashi T, Takase M. Women's experience of giving birth with their husband's support in Nepal.. British Journal of Midwifery 2013;19(7):426‐32. [Google Scholar]
Schroeder 2005 {published data only}
- Schroeder C, Bell J. Doula birth support for incarcerated pregnant women. Public Health Nursing 2005;22(1):53‐8. [DOI] [PubMed] [Google Scholar]
Shimpuku 2013 {published data only}
- Shimpuku Y, Patil CL, Norr KF, Hill PD. Women's perceptions of childbirth experience at a hospital in rural Tanzania. Health Care for Women International 2013;34(6):461‐81. [DOI] [PubMed] [Google Scholar]
Shlafer 2015 {published data only}
- Shlafer RJ, Hellerstedt WL, Secor‐Turner M, Gerrity E, Baker R. Doulas' perspectives about providing support to incarcerated women: a feasibility study. Public Health Nursing 2015;32(4):316‐26. [DOI] [PMC free article] [PubMed] [Google Scholar]
Somers‐Smith 1999 {published data only}
- Somers‐Smith MJ. A place for the partner? Expectations and experiences of support during childbirth. Midwifery 1999;15(2):101‐8. [DOI] [PubMed] [Google Scholar]
Stevens 2011 {published data only}
- Stevens J, Dahlen H, Peters K, Jackson D. Midwives' and doulas' perspectives of the role of the doula in Australia: a qualitative study. Midwifery 2011;27(4):509‐16. [DOI] [PubMed] [Google Scholar]
Thorstensson 2008 {published data only}
- Thorstensson S, Nissen E, Ekstrom A. An exploration and description of student midwives' experiences in offering continuous labour support to women/couples. Midwifery 2008;24(4):451‐9. [DOI] [PubMed] [Google Scholar]
Torres 2013 {published data only}
- Torres JM. Breast milk and labour support: lactation consultants' and doulas' strategies for navigating the medical context of maternity care. Sociology of Health & Illness 2013;35(6):924‐38. [DOI] [PubMed] [Google Scholar]
Torres 2015 {published data only}
- Torres JM. Families, markets, and medicalization: the role of paid support for childbirth and breastfeeding. Qualitative Health Research 2015;25(7):899‐911. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Adejoh 2018 {published data only}
- Adejoh SO, Olorunlana A, Olaosebikan O. Maternal health: a qualitative study of male partners' participation in Lagos, Nigeria. International Journal of Behavioral Medicine 2018;25(1):112‐22. [DOI] [PubMed] [Google Scholar]
Alcantara 2016 {published data only}
- Alcantara ST, Mattos DV, Liégio Matão ME, Alves MC. Feelings experienced by parturients in reason the inclusion of the partner in the parturition process. Journal of Nursing UFPE / Revista de Enfermagem UFPE 2016;10:4735‐40. [Google Scholar]
Anono 2018 {published data only}
- Anono EL, Ochola S, Wawire S, Ogada I, Ndedda C, Kungu JK. Community perceptions towards the new role of traditional birth attendants as birth companions and nutrition advocates in Kakamega County, Kenya. Maternal & Child Nutrition 2018;14(Suppl 1):1‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
Banda 2010 {published data only}
- Banda G, Kafulafula G, Nyirenda E, Taulo F, Kalilani L. Acceptability and experience of supportive companionship during childbirth in Malawi. BJOG 2010;117(8):937‐45. [DOI] [PubMed] [Google Scholar]
Behruzi 2010 {published data only}
- Behruzi R, Hatem M, Fraser W, Goulet L, Ii M, Misago C. Facilitators and barriers in the humanization of childbirth practice in Japan. BMC Pregnancy and Childbirth 2010;10:25. [DOI] [PMC free article] [PubMed] [Google Scholar]
Behruzi 2011 {published data only}
- Behruzi R, Hatem M, Goulet L, Fraser W. The facilitating factors and barriers encountered in the adoption of a humanized birth care approach in a highly specialized university affiliated hospital. BMC Women's Health 2011;11:53. [DOI] [PMC free article] [PubMed] [Google Scholar]
Behruzi 2014 {published data only}
- Behruzi R, Hatem M, Goulet L, Fraser WD. Perception of humanization of birth in a highly specialized hospital: let's think differently. Health Care for Women International 2014;35(2):127‐48. [DOI] [PubMed] [Google Scholar]
Binfa 2016 {published data only}
- Binfa L, Pantoja L, Ortiz J, Gurovich M, Cavada G, Foster J. Assessment of the implementation of the model of integrated and humanised midwifery health services in Chile. Midwifery 2016;35:53‐61. [DOI] [PubMed] [Google Scholar]
Bowers 2002 {published data only}
- Bowers BB. Mothers' experiences of labor support: exploration of qualitative research. JOGN Nursing; Journal of Obstetric, Gynecologic, and Neonatal Nursing 2002;31(6):742‐52. [DOI] [PubMed] [Google Scholar]
Bramadat 1993 {published data only}
- Bramadat IJ, Driedger M. Satisfaction with childbirth: theories and methods of measurement. Birth 1993;20(1):22‐9. [DOI] [PubMed] [Google Scholar]
Brodrick 2008 {published data only}
- Brodrick A. Exploring women's pre‐birth expectations of labour and the role of the midwife. Evidence Based Midwifery 2008;6(2):65‐70. [Google Scholar]
Brookes 1991 {published data only}
- Brookes HB. Experiences of childbirth in Natal Indian Women. Curationis 1991;14(4):4‐9. [DOI] [PubMed] [Google Scholar]
Bruggemann 2005 {published data only}
- Bruggemann OM, Parpinelli MA, Osis MJ. Evidence on support during labor and delivery: a literature review. Cadernos de Saude Publica 2005;21(5):1316‐27. [DOI] [PubMed] [Google Scholar]
Bruggemann 2008 {published data only}
- Bruggemann OM, Parpinelli MA. Using quantitative and qualitative approaches in knowledge production. Revista da Escola de Enfermagem da U S P 2008;42(3):563‐8. [DOI] [PubMed] [Google Scholar]
Cagle 1999 {published data only}
- Cagle CS. Women experienced communion, strength, and understanding of their partners' feelings by having their partners present at the birth of their babies [commentary on Bondas‐Salonen T. How women experience the presence of their partners at the births of their babies. QUAL HEALTH RES 1998;8(6):784‐800]. Evidence‐based Nursing 1999;2:59. [Google Scholar]
Callister 1992 {published data only}
- Callister LC. The meaning of childbirth experience to the Mormon woman... this paper was awarded the 1991 Joseph P. Daley Memorial Prize Paper from the American Society of Psychosomatic Obstetric and Gynecology. Journal of Perinatal Education 1992;1(1):50‐7. [Google Scholar]
Carter 2002 {published data only}
- Carter M. Husbands and maternal health matters in rural Guatemala: wives' reports on their spouses' involvement in pregnancy and birth. [Erratum appears in Soc Sci Med. 2003 Feb;56(4):899]. Social Science & Medicine 2002;55(3):437‐50. [DOI] [PubMed] [Google Scholar]
Chalmers 1987 {published data only}
- Chalmers B. The father's role in labour‐‐views of Pedi women. South African Medical Journal 1987;72(2):138‐40. [PubMed] [Google Scholar]
Chalmers 1994 {published data only}
- Chalmers B, Meyer D. Companionship in the perinatal period. A cross‐cultural survey of women's experiences. Journal of Nurse‐midwifery 1994;39(4):265‐72. [DOI] [PubMed] [Google Scholar]
Chamberlain 2000 {published data only}
- Chamberlain M, Barclay K. Psychosocial costs of transferring indigenous women from their community for birth. Midwifery 2000;16(2):116‐22. [DOI] [PubMed] [Google Scholar]
Chaturvedi 2015 {published data only}
- Chaturvedi S, Costa A, Raven J. Does the Janani Suraksha Yojana cash transfer programme to promote facility births in India ensure skilled birth attendance? A qualitative study of intrapartum care in Madhya Pradesh. Glob Health Action 2015;8:27427. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cheung 2009 {published data only}
- Cheung NF, Mander R, Wang X, Fu W, Zhou H, Zhang L. The planning and preparation for a 'homely birthplace' in Hangzhou, China. Evidence Based Midwifery 2009;7(3):101‐6. [Google Scholar]
Chi 2018 {published data only}
- Chi PC, Urdal H. The evolving role of traditional birth attendants in maternal health in post‐conflict Africa: a qualitative study of Burundi and northern Uganda. SAGE Open Medicine 2018;6:2050312117753631. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cipolletta 2011 {published data only}
- Cipolletta S, Balasso S. When everything seems right: the first birth experience of women in an Italian hospital. Journal of Reproductive & Infant Psychology 2011;29(4):374‐81. [Google Scholar]
Corbett 2012 {published data only}
- Corbett CA, Callister LC. Giving birth: the voices of women in Tamil Nadu, India. MCN. The American Journal of Maternal Child Nursing 2012;37(5):298‐305; quiz 306‐7. [DOI] [PubMed] [Google Scholar]
Crissman 2013 {published data only}
- Crissman HP, Engmann CE, Adanu RM, Nimako D, Crespo K, Moyer CA. Shifting norms: pregnant women's perspectives on skilled birth attendance and facility‐based delivery in rural Ghana. African Journal of Reproductive Health 2013;17(1):15‐26. [PubMed] [Google Scholar]
de Melo 2013 {published data only}
- Melo RM, Brito RS. The fathers' perception about their presence in the labor room during the birth of their child: a descriptive study. Online Brazilian Journal of Nursing 2013;12:596‐8. [Google Scholar]
Dim 2011 {published data only}
- Dim CC, Ikeme AC, Ezegwui HU, Nwagha UI. Labor support: an overlooked maternal health need in Enugu, south‐eastern Nigeria. Journal of Maternal‐Fetal and Neonatal Medicine 2011;24(3):471‐4. [DOI] [PubMed] [Google Scholar]
DiMatteo 1993 {published data only}
- DiMatteo MR, Kahn KL, Berry SH. Narratives of birth and the postpartum: analysis of the focus group responses of new mothers. Birth 1993;20(4):204‐11. [DOI] [PubMed] [Google Scholar]
Duggan 2012 {published data only}
- Duggan R, Adejumo O. Adolescent clients' perceptions of maternity care in KwaZulu‐Natal, South Africa. Women and Birth 2012;25(4):e62‐7. [DOI] [PubMed] [Google Scholar]
El‐Nemer 2006 {published data only}
- El‐Nemer A, Downe S, Small N. She would help me from the heart: an ethnography of Egyptian women in labour. Social Science and Medicine 2006;62:81‐92. [DOI] [PubMed] [Google Scholar]
Essoka 2000 {published data only}
- Essoka GC, Magai DM, Mbweza E, Mtenje M, Malava G, Masaza H, et al. Pain as a mutual experience for patients, nurses and families: a perspective from Lilongwe, Malawi. Journal of Cultural Diversity 2000;7(1):17‐9. [PubMed] [Google Scholar]
Etowa 2012 {published data only}
- Etowa JB. Black women's perceptions of supportive care during childbirth. International Journal of Childbirth Education 2012;27(1):27‐32. [Google Scholar]
Flemming 2009 {published data only}
- Flemming SE, Eide P. Grand multips perceptions of professional labor support: a word from the experts. Communicating Nursing Research 2009;42:489. [Google Scholar]
Gibbins 2001 {published data only}
- Gibbins J, Thomson AM. Women's expectations and experiences of childbirth. Midwifery 2001;17(4):302‐13. [DOI] [PubMed] [Google Scholar]
Green 2007 {published data only}
- Green J, Amis D, Hotelling BA. Care practice #3: continuous labor support. Journal of Perinatal Education 2007;16(3):25‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Grewal 2008 {published data only}
- Grewal SK, Bhagat R, Balneaves LG. Perinatal beliefs and practices of immigrant Punjabi women living in Canada. JOGN Nursing; Journal of Obstetric, Gynecologic, and Neonatal Nursing 2008;37(3):290‐300. [DOI] [PubMed] [Google Scholar]
Hallgren 1999 {published data only}
- Hallgren A, Kihlgren M, Forslin L, Norberg A. Swedish fathers' involvement in and experiences of childbirth preparation and childbirth. Midwifery 1999;15(1):6‐15. [DOI] [PubMed] [Google Scholar]
Hatamleh 2013 {published data only}
- Hatamleh R, Shaban IA, Homer C. Evaluating the experience of Jordanian women with maternity care services. Health Care for Women International 2013;34(6):499‐512. [DOI] [PubMed] [Google Scholar]
Hoga 2011 {published data only}
- Hoga LA, Gouveia LM, Manganiello A, Higashi AB, Souza Zamo Roth F. The experience and role of the companion during normal labor and childbirth: a systematic review of qualitative evidence. JBI Library of Systematic Reviews 2011;9(64 Suppl):1‐13. [DOI] [PubMed] [Google Scholar]
Howarth 2011 {published data only}
- Howarth A, Swain N, Treharne GJ. First‐time New Zealand mothers' experience of birth: importance of relationship and support. New Zealand College of Midwives Journal 2011;28(4):489‐94. [Google Scholar]
Ith 2013 {published data only}
- Ith P, Dawson A, Homer C S. Women's perspective of maternity care in Cambodia. Women and Birth 2013;26(1):71‐5. [DOI] [PubMed] [Google Scholar]
Johansson 2015 {published data only}
- Johansson M, Fenwick J, Premberg A. A meta‐synthesis of fathers' experiences of their partner's labour and the birth of their baby. Midwifery 2015;31(1):9‐18. [DOI] [PubMed] [Google Scholar]
Karlstrom 2015 {published data only}
- Karlstrom A, Nystedt A, Hildingsson I. The meaning of a very positive birth experience: focus groups discussions with women. BMC Pregnancy and Childbirth 2015;15:251. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kempe 2013 {published data only}
- Kempe A, Theorell T, Noor‐Aldin Alwazer F, Christensson K, Johansson A. Yemeni women's perceptions of own authority during childbirth: what does it have to do with achieving the Millennium Development Goals?. Midwifery 2013;29(10):1182‐9. [DOI] [PubMed] [Google Scholar]
Kgokgothwane 2002 {published data only}
- Kgokgothwane D, Nolte A. The views of Botswana adults towards support during childbirth. Health SA Gesondheid 2002;7(1):82‐92. [Google Scholar]
Larkin 2012 {published data only}
- Larkin P, Begley CM, Devane D. 'Not enough people to look after you': an exploration of women's experiences of childbirth in the Republic of Ireland. Midwifery 2012;28(1):98‐105. [DOI] [PubMed] [Google Scholar]
Maimbolwa 2003 {published data only}
- Maimbolwa MC, Yamba B, Diwan V, Ransjo‐Arvidson AB. Cultural childbirth practices and beliefs in Zambia. Journal of Advanced Nursing 2003;43(3):263‐74. [DOI] [PubMed] [Google Scholar]
Maluka 2018 {published data only}
- Maluka SO, Peneza AK. Perceptions on male involvement in pregnancy and childbirth in Masasi District, Tanzania: a qualitative study. Reproductive Health 2018;15(1):68. [DOI] [PMC free article] [PubMed] [Google Scholar]
Mami 2013 {published data only}
- Mami G. Women's delivery care needs in rural Bangladesh: recommendations for skilled birth attendants. Journal of Japan Academy of Midwifery 2013;27(2):226‐36. [Google Scholar]
Maputle 2018 {published data only}
- Maputle MS. Support provided by midwives to women during labour in a public hospital, Limpopo Province, South Africa: a participant observation study. BMC Pregnancy and Childbirth 2018;18(1):210. [DOI] [PMC free article] [PubMed] [Google Scholar]
Martins 2008 {published data only}
- Martins CA, Siqueira KM, Tyrrell MA, Barbosa MA, Carvalho SM, Santos LV. Familiar dynamics in situation of birth and puerperal. Revista Eletronica de Enfermagem 2008;10(4):1015‐25. [Google Scholar]
McLemore 2017 {published data only}
- McLemore MR, Warner Hand Z. Making the case for innovative reentry employment programs: previously incarcerated women as birth doulas ‐ a case study. International Journal of Prisoner Health 2017;13(3‐4):219‐27. [DOI] [PubMed] [Google Scholar]
Mselle 2018 {published data only}
- Mselle LT, Kohi TW, Dol J. Barriers and facilitators to humanizing birth care in Tanzania: findings from semi‐structured interviews with midwives and obstetricians. Reproductive Health 2018;15(1):137. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ojelade 2017 {published data only}
- Ojelade OA, Titiloye MA, Bohren MA, Olutayo AO, Olalere AA, Akintan A, et al. The communication and emotional support needs to improve women's experience of childbirth care in health facilities in Southwest Nigeria: a qualitative study. International Journal of Gynaecology & Obstetrics 2017;139 Suppl 1:27‐37. [DOI] [PubMed] [Google Scholar]
Papagni 2006 {published data only}
- Papagni K, Buckner E. Doula support and attitudes of intrapartum nurses: a qualitative study from the patient's perspective. Journal of Perinatal Education 2006;15(1):11‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Pascali‐Bonaro 2004 {published data only}
- Pascali‐Bonaro D, Kroeger M. Continuous female companionship during childbirth: a crucial resource in times of stress or calm. Journal of Midwifery & Women's Health 2004;49(4 Suppl 1):19‐27. [DOI] [PubMed] [Google Scholar]
Pyone 2014 {published data only}
- Pyone T, Adaji S, Madaj B, Woldetsadik T, Broek N. Changing the role of the traditional birth attendant in Somaliland. International Journal of Gynaecology & Obstetrics 2014;127(1):41‐6. [DOI] [PubMed] [Google Scholar]
Ramashwar 2008 {published data only}
- Ramashwar S. Nigerian women would like to receive social support during childbirth. International Family Planning Perspectives 2008;34(4):202‐3. [Google Scholar]
Raven 2015 {published data only}
- Raven J, Broek N, Tao F, Kun H, Tolhurst R. The quality of childbirth care in China: women's voices: a qualitative study. BMC Pregnancy and Childbirth 2015;15:113. [DOI] [PMC free article] [PubMed] [Google Scholar]
Richards 1992 {published data only}
- Richards MP. Doulas and the quality of maternity services. Birth 1992;19(1):40‐1. [DOI] [PubMed] [Google Scholar]
Sapkota 2014 {published data only}
- Sapkota S, Sayami JT, Manadhar MD, Erlandsson K. Nepalese mothers’ experiences of care in labour. Evidence Based Midwifery 2014;12(4):127‐32. [Google Scholar]
Sauls 2004 {published data only}
- Sauls DJ. Adolescents' perception of support during labor. Journal of Perinatal Education 2004;13(4):36‐42. [DOI] [PMC free article] [PubMed] [Google Scholar]
Shahoei 2014 {published data only}
- Shahoei R, Khosravy F, Zaheri F, Hasheminasab L, Ranaei F, Hesame K, et al. Iranian Kurdish women's experiences of childbirth: a qualitative study. Iranian Journal of Nursing and Midwifery Research 2014;19(7 Suppl 1):S112‐7. [PMC free article] [PubMed] [Google Scholar]
Shimpuku 2010 {published data only}
- Shimpuku Y. Mothers' perceptions of childbirth experience at the hospital in rural Tanzania [Ph.D.]. Chicago: University of Illinois at Chicago, Health Sciences Center, 2010. [Google Scholar]
Simmonds 2012 {published data only}
- Simmonds DM, West L, Porter J, Davies M, Holland C, Preston‐Thomas A, et al. The role of support person for Ngaanyatjarra women during pregnancy and birth. Women and Birth 2012;25(2):79‐85. [DOI] [PubMed] [Google Scholar]
Spiby 2016 {published data only}
- Spiby H, McLeish J, Green J, Darwin Z. 'The greatest feeling you get, knowing you have made a big difference': survey findings on the motivation and experiences of trained volunteer doulas in England. BMC Pregnancy and Childbirth 2016;16(1):289. [DOI] [PMC free article] [PubMed] [Google Scholar]
Steel 2013 {published data only}
- Steel A, Diezel H, Johnstone K, Sibbritt D, Adams J, Adair R. The value of care provided by student doulas: an examination of the perceptions of women in their care. Journal of Perinatal Education 2013;22(1):39‐48. [DOI] [PMC free article] [PubMed] [Google Scholar]
Steel 2015 {published data only}
- Steel A, Frawley J, Adams J, Diezel H. Trained or professional doulas in the support and care of pregnant and birthing women: a critical integrative review. Health & Social Care in the Community 2015;23(3):225‐41. [DOI] [PubMed] [Google Scholar]
Story 2012 {published data only}
- Story WT, Burgard SA, Lori JR, Taleb F, Ali NA, Hoque DM. Husbands' involvement in delivery care utilization in rural Bangladesh: a qualitative study. BMC Pregnancy and Childbirth 2012;12:28. [DOI] [PMC free article] [PubMed] [Google Scholar]
Tarlazzi 2015 {published data only}
- Tarlazzi E, Chiari P, Naldi E, Parma D, Jack SM. Italian fathers' experiences of labour pain. British Journal of Midwifery 2015;23(3):188‐94. [Google Scholar]
Theuring 2010 {published data only}
- Theuring S, Nchimbi P, Jordan‐Harder B, Harms G. Partner involvement in perinatal care and PMTCT services in Mbeya Region, Tanzania: the providers' perspective. AIDS Care 2010;22(12):1562‐8. [DOI] [PubMed] [Google Scholar]
Udofia 2012 {published data only}
- Udofia EA, Akwaowo CD. Pregnancy and after: what women want from their partners ‐ listening to women in Uyo, Nigeria. Journal of Psychosomatic Obstetrics & Gynecology 2012;33(3):112‐9. [DOI] [PubMed] [Google Scholar]
Vikstrom 2016 {published data only}
- Vikstrom A, Barimani M. Partners' perspective on care‐system support before, during and after childbirth in relation to parenting roles. Sexual & Reproductive Healthcare 2016;8:1‐5. [DOI] [PubMed] [Google Scholar]
Yuenyong 2008 {published data only}
- Yuenyong S, Jirapaet V, O'Brien BA. Support from a close female relative in labour: the ideal maternity nursing intervention in Thailand. Journal of the Medical Association of Thailand 2008;91(2):253‐60. [PubMed] [Google Scholar]
References to studies awaiting assessment
Bruggemann 2007 {published data only}
- Bruggemann OM, Osis MJ, Parpinelli MA. Support during childbirth: perception of health care providers and companions chosen by women. Revista de Saude Publica 2007;41(1):44‐52. [PubMed] [Google Scholar]
Bruggemann 2016 {published data only}
- Bruggemann OM, Ebsen ES, Ebele RR, Batista BD. Possibilities of inclusion of the partner in deliveries in public institutions. Ciencia & Saude Coletiva 2016;21(8):2555‐64. [DOI] [PubMed] [Google Scholar]
de Carvalho 2003 {published data only}
- Carvalho ML. Fathers' participation in childbirth at a public hospital: institutional difficulties and motivations of couples. Cadernos de Saude Publica / Ministerio da Saude, Fundacao Oswaldo Cruz, Escola Nacional de Saude Publica 2003;19 Suppl 2:S389‐98. [DOI] [PubMed] [Google Scholar]
de Souza 2015 {published data only}
- Souza FB, Souza BS, Vitório ML, Mota Zampieri MdeF, Petters GV. Fathers' perceptions about their experiences as birth companions. Revista Mineira de Enfermagem 2015;19(3):576‐83. [Google Scholar]
Florentino 2007 {published data only}
- Florentino LC, Gualda DM. The companion participation during the childbirth process according to humanization perspective. Nursing (São Paulo) 2007;10(110):319‐23. [Google Scholar]
Fu 2001 {published data only}
- Fu Y, Lee T, Yeh P. The lived experience of women accompanied by husbands in labor ward. Journal of Nursing 2001;48(4):51‐60. [Google Scholar]
Hoga 2007 {published data only}
- Hoga LA, Pinto Cleusa MS. The partner's presence in delivery care: the professionals' experience. Investigacion & Educacion en Enfermeria 2007;25(1):74‐81. [Google Scholar]
Jamas 2013 {published data only}
- Jamas MT, Hoga LA, Reberte LM. Women's narratives on care received in a birthing center. Cadernos de Saude Publica 2013;29(12):2436‐46. [DOI] [PubMed] [Google Scholar]
Nakano 2007 {published data only}
- Nakano AM, Silva LA, Beleza AC, Stefanello J, Gomes FA. Support during the labor and delivery process: viewpoint of companions of women giving birth. Acta Paulista de Enfermagem 2007;20(2):131‐7. [Google Scholar]
Perazzini 2017 {published data only}
- Perazzini de Sá AM, Alves VH, Pereira RD, Lutterbach Branco Riker BM, Paula E, Soanno Marchiori GR. The right to access and accompanying of labor and childbirth: women's point of view. Journal of Nursing UFPE / Revista de Enfermagem UFPE 2017;11(7):2683‐90. [Google Scholar]
Ribeiro 2018 {published data only}
- Ribeiro JF, Sousa YE, Sousa LV, Matías Coelho DM, Cipriano Feitosa V, Alves Cavalcante MF, et al. The father's perception on his presence during the parturitive process. Journal of Nursing UFPE / Revista de Enfermagem UFPE 2018;12(6):1586‐92. [Google Scholar]
Rocha 2018 {published data only}
- Rocha de Souza MA, Loewen Wall M, Morais Chaves Thuler AC, Souza Freire MH, Atherino dos Santos EK. Experience of the parturient's assistant in the delivery process. Journal of Nursing UFPE / Revista de Enfermagem UFPE 2018;12(3):626‐34. [Google Scholar]
Rossi 2016 {published data only}
- Rossi Kissula Souza SR, Gualda DMR. The experience of women and their coaches with childbirth in a public maternity hospital. Texto & Contexto Enfermagem 2016;25(1):1‐9. [Google Scholar]
Santos 2009 {published data only}
- Santos DS, Nunes IM. Doulas in delivery assistance: perceptions of nursing professionals. Anna Nery School Journal of Nursing / Escola Anna Nery Revista de Enfermagem 2009;13(3):582‐8. [Google Scholar]
Vanuzzi 2017 {published data only}
- Vanuzzi MN, Antunes WL, Cremonese L, Alende Prates L, Simões Timm M, Beatriz Ressel L. Care practices carried out by the partner in the pregnant woman's [Práticas de cuidado realizadas pelo companheiro na perspectiva da gestante]. Journal of Nursing UFPE / Revista de Enfermagem UFPE 2017;11:4574‐8. [Google Scholar]
Additional references
Ames 2017
- Ames HM, Glenton C, Lewin S. Parents' and informal caregivers' views and experiences of communication about routine childhood vaccination: a synthesis of qualitative evidence. Cochrane Database of Systematic Reviews 2017, Issue 2. [DOI: 10.1002/14651858.CD011787.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Atlas.ti [Computer program]
- Scientific Software Development GmbH. Atlas.ti. Version 7.5.18. Berlin, Germany: Scientific Software Development GmbH, 1999.
Beake 2018
- Beake S, Chang YS, Cheyne H, Spiby H, Sandall J, Bick D. Experiences of early labour management from perspectives of women, labour companions and health professionals: a systematic review of qualitative evidence. Midwifery 2018;57:69‐84. [DOI] [PubMed] [Google Scholar]
Bohren 2015a
- Bohren MA, Vogel JP, Hunter EC, Lutsiv O, Makh SK, Souza JP, et al. The mistreatment of women during childbirth in health facilities globally: a mixed‐methods systematic review. PLOS Medicine 2015;12(6):e1001847. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Bohren 2017
- Bohren MA, Hofmeyr GJ, Sakala C, Fukuzawa RK, Cuthbert A. Continuous support for women during childbirth. Cochrane Database of Systematic Reviews 2017, Issue 7. [DOI: 10.1002/14651858.CD003766.pub6] [DOI] [PMC free article] [PubMed] [Google Scholar]
Candy 2011
- Candy B, King M, Jones L, Oliver S. Using qualitative synthesis to explore heterogeneity of complex interventions. BMC medical research methodology 2011;11:124. [DOI] [PMC free article] [PubMed] [Google Scholar]
Colvin 2013
- Colvin CJ, Heer J, Winterton L, Mellenkamp M, Glenton C, Noyes J, et al. A systematic review of qualitative evidence on barriers and facilitators to the implementation of task‐shifting in midwifery services. Midwifery 2013;29(10):1211‐21. [1532‐3099: (Electronic)] [DOI] [PubMed] [Google Scholar]
Colvin 2018
- Colvin CJ, Garside R, Wainwright M, Munthe‐Kaas H, Glenton C, Bohren MA, et al. Applying GRADE‐CERQual to qualitative evidence synthesis findings‐paper 4: how to assess coherence. Implementation Science 2018;13(Suppl 1):13. [DOI] [PMC free article] [PubMed] [Google Scholar]
DONA International, 2018
- DONA International. What is a doula?. www.dona.org/ 2018:Accessed 6 March 2019. [https://www.dona.org/what‐is‐a‐doula/]
Glenton 2013
- Glenton C, Colvin C, Carlsen B, Swartz A, Lewin S, Noyes J, et al. Barriers and facilitators to the implementation of lay health worker programmes to improve access to maternal and child health: qualitative evidence synthesis. Cochrane Database of Systematic Reviews 2013, Issue 10. [DOI: 10.1002/14651858.CD010414.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Glenton 2018
- Glenton C, Carlsen B, Lewin S, Munthe‐Kaas H, Colvin CJ, Tuncalp O, et al. Applying GRADE‐CERQual to qualitative evidence synthesis findings‐paper 5: how to assess adequacy of data. Implementation Science 2018;13(Suppl 1):14. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2017
- Higgins JP, Altman DG, Sterne JA (editors). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS (editors), Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017), Cochrane, 2017. Available from www.training.cochrane.org/handbook.
Hodnett 2013
- Hodnett ED, Gates S, Hofmeyr GJ, Sakala C. Continuous support for women during childbirth. Cochrane Database of Systematic Reviews 2013, Issue 7. [DOI: 10.1002/14651858.CD003766.pub5] [DOI] [PubMed] [Google Scholar]
Kabakian‐Khasholian 2017
- Kabakian‐Khasholian T, Portela A. Companion of choice at birth: factors affecting implementation. BMC Pregnancy and Childbirth 2017;17(1):265. [DOI] [PMC free article] [PubMed] [Google Scholar]
Knape 2013
- Knape N, Schnepp W, Krahl A, zu Sayn‐Wittgenstein F. The efficiency of one‐to‐one support during labour – a literature analysis [Die Eff ektivität der Eins‐zu‐eins‐Betreuung während der Geburt. Eine Literaturübersicht]. Zeitschrift fur Geburtshilfe und Neonatologie 2013;217:161‐72. [DOI: ] [DOI] [PubMed] [Google Scholar]
Lewin 2015
- Lewin S, Glenton C, Munthe‐Kaas H, Carlsen B, Colvin CJ, Gulmezoglu M, et al. Using qualitative evidence in decision making for health and social interventions: an approach to assess confidence in findings from qualitative evidence syntheses (GRADE‐CERQual). PLoS Medicine 2015;12(10):e1001895. [1549‐1676: (Electronic)] [DOI] [PMC free article] [PubMed] [Google Scholar]
Lewin 2018a
- Lewin S, Booth A, Glenton C, Munthe‐Kaas H, Rashidian A, Wainwright M, et al. Applying GRADE‐CERQual to qualitative evidence synthesis findings: introduction to the series. Implementation Science 2018;13(Suppl 1):2. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lewin 2018b
- Lewin S, Bohren M, Rashidian A, Munthe‐Kaas H, Glenton C, Colvin CJ, et al. Applying GRADE‐CERQual to qualitative evidence synthesis findings‐paper 2: how to make an overall CERQual assessment of confidence and create a Summary of Qualitative Findings table. Implementation Science 2018;13(Suppl 1):10. [DOI] [PMC free article] [PubMed] [Google Scholar]
Munabi‐Babigumira 2017
- Munabi‐Babigumira S, Glenton C, Lewin S, Fretheim A, Nabudere H. Factors that influence the provision of intrapartum and postnatal care by skilled birth attendants in low‐ and middle‐income countries: a qualitative evidence synthesis. Cochrane Database of Systematic Reviews 2017, Issue 11. [DOI: 10.1002/14651858.CD011558] [DOI] [PMC free article] [PubMed] [Google Scholar]
Munthe‐Kaas 2018
- Munthe‐Kaas H, Bohren MA, Glenton C, Lewin S, Noyes J, Tuncalp O, et al. Applying GRADE‐CERQual to qualitative evidence synthesis findings‐paper 3: how to assess methodological limitations. Implementation Science 2018;13(Suppl 1):9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Noyes 2011
- Noyes J, Popay J, Pearson A, Hannes K, Booth A. Chapter 20: Qualitative research and Cochrane reviews. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Noyes 2018
- Noyes J, Booth A, Lewin S, Carlsen B, Glenton C, Colvin CJ, et al. Applying GRADE‐CERQual to qualitative evidence synthesis findings‐paper 6: how to assess relevance of the data. Implementation Science 2018;13(Suppl 1):4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Odendaal 2015
- Odendaal WA, Goudge J, Griffiths F, Tomlinson M, Leon N, Daniels K. Healthcare workers’ perceptions and experience on using mHealth technologies to deliver primary healthcare services: qualitative evidence synthesis. Cochrane Database of Systematic Reviews 2015, Issue 11. [DOI: 10.1002/14651858.CD011942] [DOI] [PMC free article] [PubMed] [Google Scholar]
Rosen 2004
- Rosen P. Supporting women in labor: analysis of different types of caregivers. Journal of Midwifery & Women's Health 2004;49(1):24‐31. [DOI] [PubMed] [Google Scholar]
Schünemann 2017
- Schünemann H, Brożek J, Guyatt G, Oxman A, editor(s). Handbook for grading the quality of evidence and the strength of recommendations using the GRADE approach (updated October 2013). GRADE Working Group, 2013. Available from gdt.guidelinedevelopment.org/app/handbook/handbook.html.
Shakibazadeh 2018
- Shakibazadeh E, Namadian M, Bohren MA, Vogel JP, Rashidian A, Nogueira Pileggi V, et al. Respectful care during childbirth in health facilities globally: a qualitative evidence synthesis. BJOG 2018;125(8):932‐42. [PUBMED: 29117644] [DOI] [PMC free article] [PubMed] [Google Scholar]
SURE Collaboration 2011
- SURE Collaboration. SURE guides for preparing and using evidence‐based policy briefs: 5. Identifying and addressing barriers to implementing policy options. Version 2.1. www.who.int/evidence/sure/guides (updated November 2011).
Thomas 2008
- Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Medical Research Methodology 2008;8:45. [DOI] [PMC free article] [PubMed] [Google Scholar]
World Health Organization 2012
- World Health Organization. WHO recommendations: optimizing health worker roles to improve access to key maternal and newborn health interventions through task shifting. apps.who.int/iris/bitstream/handle/10665/77764/9789241504843_eng.pdf;jsessionid=9952FE3F427262D89911D784640CF8D6?sequence=1 2012. [http://apps.who.int/iris/bitstream/10665/77764/1/9789241504843_eng.pdf] [PubMed]
World Health Organization 2014a
- World Health Organization. WHO Statement: the prevention and elimination of disrespect and abuse during facility‐based childbirth. www.who.int/reproductivehealth/topics/maternal_perinatal/statement‐childbirth/en/. Geneva, Switzerland, 2014 (accessed prior to 4 November 2016).
World Health Organization 2014b
- World Health Organization. WHO recommendations for augmentation of labour. www.who.int/reproductivehealth/publications/maternal_perinatal_health/augmentation‐labour/en/ 2014. [PubMed]
World Health Organization 2015
- World Health Organization. WHO recommendations on health promotion interventions for maternal and newborn health. www.who.int/maternal_child_adolescent/documents/health‐promotion‐interventions/en/ 2015. [http://apps.who.int//iris/bitstream/10665/172427/1/9789241508742_report_eng.pdf?ua=1] [PubMed]
World Health Organization 2016
- World Health Organization. Standards for improving quality of maternal and newborn care in health facilities. www.who.int/maternal_child_adolescent/documents/improving‐maternal‐newborn‐care‐quality/en/ 2016. [ISBN 9789241511216]
World Health Organization 2018
- World Health Organization. WHO Recommendations: Intrapartum care for a positive childbirth experience. www.who.int/reproductivehealth/publications/intrapartum‐care‐guidelines/en/ 2018. [http://apps.who.int/iris/bitstream/handle/10665/260178/9789241550215‐eng.pdf?sequence=1] [PubMed]
References to other published versions of this review
Bohren 2016
- Bohren MA, Munthe‐Kaas H, Berger B, Tunçalp Ö. Perceptions and experiences of labour companionship: a qualitative evidence synthesis. Cochrane Database of Systematic Reviews 2016, Issue 12. [DOI: 10.1002/14651858.CD012449] [DOI] [PMC free article] [PubMed] [Google Scholar]