

Abstract
Background
People with febrile neutropaenia are usually treated in a hospital setting. Recently, treatment with oral antibiotics has been proven to be as effective as intravenous therapy. However, the efficacy and safety of outpatient treatment have not been fully evaluated.
Objectives
To compare the efficacy (treatment failure and mortality) and safety (adverse events of antimicrobials) of outpatient treatment compared with inpatient treatment in people with cancer who have low‐risk febrile neutropaenia.
Search methods
We searched the Cochrane Central Register of Controlled Trials (CENTRAL; 2018, Issue 11) in the Cochrane Library, MEDLINE via Ovid (from 1948 to November week 4, 2018), Embase via Ovid (from 1980 to 2018, week 48) and trial registries (National Cancer Institute, MetaRegister of Controlled Trials, Medical Research Council Clinical Trial Directory). We handsearched all references of included studies and major reviews.
Selection criteria
Randomised controlled trials (RCTs) comparing outpatient with inpatient treatment for people with cancer who develop febrile neutropaenia. The outpatient group included those who started treatment as an inpatient and completed the antibiotic course at home (sequential) as well as those who started treatment at home.
Data collection and analysis
Two review authors independently assessed trial eligibility, methodological quality, and extracted data. Primary outcome measures were: treatment failure and mortality; secondary outcome measures considered were: duration of fever, adverse drug reactions to antimicrobial treatment, duration of neutropaenia, duration of hospitalisation, duration of antimicrobial treatment, and quality of life (QoL). We estimated risk ratios (RRs) with 95% confidence intervals (CIs) for dichotomous data; we calculated weighted mean differences for continuous data. Random‐effects meta‐analyses and sensitivity analyses were conducted.
Main results
We included ten RCTs, six in adults (628 participants) and four in children (366 participants). We found no clear evidence of a difference in treatment failure between the outpatient and inpatient groups, either in adults (RR 1.23, 95% CI 0.82 to 1.85, I2 0%; six studies; moderate‐certainty evidence) or children (RR 1.04, 95% CI 0.55 to 1.99, I2 0%; four studies; moderate‐certainty evidence). For mortality, we also found no clear evidence of a difference either in studies in adults (RR 1.04, 95% CI 0.29 to 3.71; six studies; 628 participants; moderate‐certainty evidence) or in children (RR 0.63, 95% CI 0.15 to 2.70; three studies; 329 participants; moderate‐certainty evidence).
According to the type of intervention (early discharge or exclusively outpatient), meta‐analysis of treatment failure in four RCTs in adults with early discharge (RR 1.48, 95% CI 0.74 to 2.95; P = 0.26, I2 0%; 364 participants; moderate‐certainty evidence) was similar to the results of the exclusively outpatient meta‐analysis (RR 1.15, 95% CI 0.62 to 2.13; P = 0.65, I2 19%; two studies; 264 participants; moderate‐certainty evidence).
Regarding the secondary outcome measures, we found no clear evidence of a difference between outpatient and inpatient groups in duration of fever (adults: mean difference (MD) 0.2, 95% CI ‐0.36 to 0.76, 1 study, 169 participants; low‐certainty evidence) (children: MD ‐0.6, 95% CI ‐0.84 to 0.71, 3 studies, 305 participants; low‐certainty evidence) and in duration of neutropaenia (adults: MD 0.1, 95% CI ‐0.59 to 0.79, 1 study, 169 participants; low‐certainty evidence) (children: MD ‐0.65, 95% CI ‐1.86 to 0.55, 2 studies, 268 participants; moderate‐certainty evidence). With regard to adverse drug reactions, although there was greater frequency in the outpatient group, we found no clear evidence of a difference when compared to the inpatient group, either in adult participants (RR 8.39, 95% CI 0.38 to 187.15; three studies; 375 participants; low‐certainty evidence) or children (RR 1.90, 95% CI 0.61 to 5.98; two studies; 156 participants; low‐certainty evidence).
Four studies compared the hospitalisation time and found that the mean number of days of hospital stay was lower in the outpatient treated group by 1.64 days in adults (MD ‐1.64, 95% CI ‐2.22 to ‐1.06; 3 studies, 251 participants; low‐certainty evidence) and by 3.9 days in children (MD ‐3.90, 95% CI ‐5.37 to ‐2.43; 1 study, 119 participants; low‐certainty evidence). In the 3 RCTs of children in which days of antimicrobial treatment were analysed, we found no difference between outpatient and inpatient groups (MD ‐0.07, 95% CI ‐1.26 to 1.12; 305 participants; low‐certainty evidence).
We identified two studies that measured QoL: one in adults and one in children. QoL was slightly better in the outpatient group than in the inpatient group in both studies, but there was no consistency in the domains included.
Authors' conclusions
Outpatient treatment for low‐risk febrile neutropaenia in people with cancer probably makes little or no difference to treatment failure and mortality compared with the standard hospital (inpatient) treatment and may reduce time that patients need to be treated in hospital.
Plain language summary
Outpatient treatment for cancer patient with low‐risk febrile neutropaenic event is effective.
Review question Is outpatient treatment with antibiotics safe and effective for people with cancer who have low neutrophil levels (type of white blood cell) and develop a fever (called febrile neutropaenia), usually as a result of chemotherapy?
Background Neutrophils (a type of white blood cell) are key to fighting bacterial infections. People treated for cancer often have low neutrophil levels, which is called neutropaenia, most commonly because of chemotherapy treatment. This leaves them susceptible to infection, which can become serious and potentially life‐threatening very quickly. This is called neutropaenic sepsis. For many years, people with cancer who develop a fever whilst they are neutropaenic (called neutropaenic fever) have been given antibiotics to prevent them from developing overwhelming neutropaenic sepsis. Depending of the duration of neutropaenia, as well as type of cancer, age and other symptoms, patients can fall in to two risk groups: high‐ or low risk of developing a serious infection. Recently, treatment with oral antibiotics (medicine given as liquid or tablets by mouth) has been proven to be as effective as intravenous (medicine injected into a vein) treatments. However, it is unclear whether providing treatment in an outpatient setting is as safe as therapy administered in a hospital setting.
Study characteristics Ten studies (994 participants) provided information for the review. These ten studies compared outpatient antibiotic therapy (491 participants) versus inpatient therapy (503 participants) in people with cancer who developed febrile neutropaenia. Six studies were conducted in adults (628 participants) and four studies were in children (366 participants). These ten trials compared effectiveness in terms of the disappearance of signs of infection (mainly fever) and nine studies assessed the effect on mortality (death). Eight studies recorded the number of treatment days for the fever to resolve. Five studies compared the duration of neutropaenia between out‐ and inpatients. Five studies analysed duration of antibiotics usage and six looked at the duration of hospitalisation.Two studies assessed quality of life for patients.
In eight of the 10 studies, outpatient antibiotic therapy was part of an early discharge programme, i.e. antibiotics were given for a few days in the hospital and then the participants was discharged home. In the other two studies, the antibiotics were started at home.
Key results Outpatient antibiotic therapy is probably as effective as inpatient therapy in people (both in adults and children) with cancer who develop febrile neutropaenia for improving the signs of infection, including reducing fever. There was probably little or no difference in mortality between the outpatient therapy and inpatient therapy, as well as in the duration of treatment with antibiotics, or frequency of adverse events related to the use of antibiotics. Treatment as an outpatient may reduce the number of days patients need to be treated in hospital.
Certainty of the evidence In general, the studies were of moderate certainty.
Summary of findings
Background
Description of the condition
Infections are common in people with cancer and neutropaenia (an absolute neutrophil count (ANC) < 500/mm3 or a count of < 1000 cells/mm3 with a predicted decrease to < 500 cells/mm3). Since these infections are associated with complications, and because fever is often the first and only sign of infection, previous treatment guidelines recommended administration of parenteral (intravenous (IV) or intramuscular (IM)) empirical broad‐spectrum antibiotics, as well as keeping patients in hospital until the clinical signs of infection disappear (Bodey 1966; Hughes 1997; Hughes 2002).
Febrile (fever) neutropaenic patients have heterogeneous outcomes; approximately 50% to 60% of patients do not develop life‐threatening complications or fatal infections (Buchanan 1993; Mullen 1990; Orudjev 2002), between 48% and 60% have established or occult infections (hidden or not obvious signs of infection), around 20% or more patients with profound neutropaenia (neutrophil counts < 100 cells/mm3) have bacteraemia, and a very small percentage of patients (4% to 6%) die as a consequence of a severe bacterial infection (Santolaya 2002; Talcott 1988; Talcott 1992). Thus, according to the different clinical features and outcomes, febrile neutropaenic episodes might be regarded as low‐ or high‐risk for development of severe infections or serious medical complications. In low‐risk episodes, fever episodes resolve uneventfully. In contrast, patients with high‐risk episodes can have life‐threatening conditions, such as hypotension (low blood pressure), respiratory failure, dehydration or uncontrolled bleeding (Santolaya 2002; Talcott 1988).
Identification of low‐risk patients is useful and leads to a less aggressive empirical antimicrobial therapy. Predictive models were created to discriminate between low‐risk and high‐risk patients (Delebarre 2014; Talcott 1992). These prognostic scales are based on laboratory and clinical findings during the initial patient assessment in the routine clinical setting (Elting 1997; Klaassen 2000; Mesters 2000; Santolaya 2002; Soker 2001; Talcott 1992).The first scale was developed and validated in 1988 by Talcott and colleagues (Talcott 1988; Talcott 1992). In 2000, an international prospective study established an improved risk assessment model, based on clinical criteria – the Multinational Association for Supportive Care in Cancer (MASCC) index (Klastersky 2000). Current guidelines for adult people with cancer recommend using this scale to classify febrile neutropaenia episodes (Heinz 2017; IDSA 2010; Klastersky 2016). For paediatric patients, different scales have been proposed (Alexander 2002; Ammann 2003; Santolaya 2002) but specific recommendations for their use have not been published (Lehrnbecher 2017).
Most patients with a febrile neutropaenic episode show no apparent infection source. In approximately 30%, the infection is localised, mainly in the upper respiratory tract or skin, and in 20% to 40% of these infections the episode can be microbiologically documented. It has been observed that the incidence of Gram‐negative organisms has declined and Gram‐positive infections account for 60% to 70% of all microbiologically documented infections in febrile neutropaenic patients (IDSA 2010; Kamana 2005). Accordingly, recommendations for empirical antimicrobial therapy have changed during the last decades, but the general principle for the selection of antimicrobial agents still remains. For high‐risk patients, intravenous (IV) administration of broad‐spectrum antibiotics with activity against Gram‐negative and Gram‐positive bacteria is the standard treatment. For low‐risk patients, there are two alternatives, outpatient therapy with oral antibiotics (Hidalgo 1999), or hospitalisation with IV broad‐spectrum antibiotics and then switching to oral treatment and discharge (Talcott 2011).
Antibacterial agents must be selected according to local epidemiology. For low‐risk patients, a variety of schemes have been used, including monotherapy and combinations, by oral or parenteral (intravenous, intramuscular) routes. Some examples are amoxicillin with clavulanate (Gupta 2009; Klaassen 2000a), ciprofloxacin (Freifeld 1999; Hidalgo 1999), amoxicillin‐clavulanate plus ciprofloxacin (Klastersky 2006) ceftriaxone (Gupta 2009; Sebban 2008), or aztreonam‐clindamycin (Rubenstein 1993).
In 2008, Carstensen and Sorensen published a systematic review of outpatient treatment in febrile neutropaenia (Carstensen 2008); ten RCTs were included, with six reporting only full outpatient treatment and four comparing outpatient versus inpatient treatment. Of note, mortality and antibiotic‐related side effects were not reported separately according to the intervention (full outpatient, hospital‐based management or early discharge). Since this report, other RCTs have been published (Brack 2012; Orme 2014; Talcott 2011). A meta‐analysis comparing the effectiveness of empirical antibiotic therapy, either orally or intravenously, was published in 2013 (Vidal 2013). Twenty‐two RCTs were included: in six trials, treatment was given in an outpatients setting; in three trials, authors compared oral treatment between outpatients and inpatients; in two trials, initial therapy was in an inpatient setting and continued in an outpatient setting, and in the rest, all received intra‐hospital treatment. Results demonstrated that oral treatment is as effective as intravenous antibiotic treatment in selected febrile neutropaenic patients, since death and failure rates were similar for both methods, although confidence intervals (CI) were wide: risk ratios (RR) 0.95 (95% CI 0.54 to 1.68) and RR 0.95 (95% CI: 0.85 to 1.07), respectively.
Description of the intervention
Current recommended empiric antimicrobial treatment for low‐risk febrile neutropaenic patients is based on multiple clinical trials and observational studies. There are several alternatives and combinations: one is the election of the route of administration of antimicrobials, and the other is the setting to complete the scheme (outpatient or inpatient). RCTs in the settings are limited in comparing the dose and type of antimicrobials. In some studies, the authors have assessed different types of antibiotics and less aggressive strategies, such as sequential intravenous to oral therapy, or early hospital discharge with continued outpatient therapy. A number of clinical trials have evaluated the effectiveness of inpatient‐administered oral antibiotics (Kamana 2005; Klaassen 2000a).
In children, Paganni used ciprofloxacin in low‐risk patients after intravenous broad‐spectrum antibiotics (Paganini 2001). In another study, 126 episodes were evaluated in inpatients where intravenous ceftriaxone showed a success rate of 78%, which was similar (76%) when the same treatment was administered at home (Karthaus 1998). Meanwhile, Mustafa and colleagues demonstrated the safety of outpatient ceftriaxone treatment in a pilot study with 19 children; 18 children completed at‐home treatment and only one required hospitalisation as fever persisted for over 48 hours (Mustafa 1996). Another clinical trial showed an 89% success rate with ciprofloxacin as ambulatory (outpatient) treatment, after a 24‐hour hospital stay. In this study, participants who needed re‐hospitalisation completed treatment intravenously without complications (Malik 1995). Other forms to deliver empirical antimicrobial treatment to low‐risk patients include at‐home administration of short‐term antibiotic schemes (Chamilos 2005; Cherif 2004; Cherif 2006) or the suspension of antibiotics after the first 24 hours (Nijhuis 2005).
How the intervention might work
In general, the outcome measures used to evaluate the empirical antibiotic therapy in low‐risk patients include defervescence (reduction in fever) after initiating the antibiotics (Chamilos 2005), hospital readmission (Malik 1995), treatment failure (change of initial empirical antibiotic scheme) (Mustafa 1996), death (Malik 1995; Mustafa 1996), adverse events, and costs (Santolaya 2004). Also some authors (Freifeld 1999; Kamana 2005; Kern 1999) have suggested that oral antibiotic therapy may improve quality of life (QoL).
Interestingly, although there are some clinical trials that show the effectiveness and safety of outpatient antimicrobial therapy for low‐risk paediatric participants, in a study that explored the feasibility to deliver this type of therapy, 71% of health‐care professionals and 53% of parents would choose ambulatory therapy (Sung 2004). This could suggest that both patients and health‐care professionals have doubts about the safety of this type of treatment. Quezada and colleagues corroborated these findings in an observational study with children experiencing fever and neutropaenia; in about one‐quarter of episodes, either the family or treating physician did not find the prospect of outpatient care appealing (Quezada 2007). This may be related to the side effects reported (Kamana 2005), because some participants treated with at‐home therapy have needed re‐hospitalisation (Elting 2008), or because this approach requires an organised approach and 24 hours, 7 days per week response capacity, educational strategies for families and health‐care professionals, as well as a good doctor‐patient relationship (Hughes 2002;Santolaya 2010). Identification of low‐risk patients as candidates for outpatient management is the first step, but to ensure the effectiveness of this strategy, every issue needs to be addressed (Klastersky 2013).
Why it is important to do this review
A systematic review was published in 2008 about the effectiveness and safety of outpatient febrile neutropaenia management of low‐risk people with cancer. The authors included only clinical trials in adult participants and concluded that outpatient empirical antimicrobial therapy was safe, effective, and comparable to hospital‐based therapy. However, three of the nine trials did not have a control group (Carstensen 2008).
Considering that outpatient management in recent years has become an alternative for febrile neutropaenia low‐risk patients and the frequency of published studies with this approach has increased, this systematic review aims to analyse the efficacy and safety of outpatient antimicrobial therapy in people with cancer with febrile neutropaenia. If the evidence supports this alternative, this could impact care by decreasing the number of nosocomial (treatment‐related) infections, decrease of exposure to antimicrobials, acquisition of resistant bacteria, decrease of costs and increase of available resources, and improve the quality of life and patient satisfaction.
Objectives
To compare the efficacy (treatment failure and mortality) and safety (adverse events of antimicrobials) of outpatient treatment compared with inpatient treatment in people with cancer who have low‐risk febrile neutropaenia.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs) comparing inpatient empirical antimicrobial therapy with outpatient management for low‐risk febrile neutropaenic people with cancer, using any oral or intravenous antibiotics.
Types of participants
Febrile neutropaenic people, both adults or children, with cancer considered as low risk for development of severe infections or serious medical complications.
Types of interventions
Outpatient treatment with any oral or intravenous antibiotics, either as monotherapy or combination therapy, administered at home. This group included early hospital discharge after a short course of antibiotics in hospital.
Inpatient treatment with any oral or intravenous antibiotics, either as monotherapy or combination therapy, administered during hospitalisation.
Types of outcome measures
Primary outcomes:
Treatment failure: a composite end point comprising one or more of the following: death; persistence, recurrence, or worsening of clinical signs or symptoms of presenting infection; modification of initial empirical antibiotic scheme (Consensus panel 1990; Feld 1998; Feld 2002). If studies defined treatment failure differently, the outcome was considered as reported in the study.
All‐cause mortality at 30 days follow‐up.
Secondary outcomes
Duration of fever (days after the start of the intervention).
Adverse drug reactions related to the antibiotic regimen, such as nausea, vomiting, diarrhoea.
Duration of neutropaenia (days after the start of the intervention).
Duration of hospitalisation (hospital stay as reported in the study, including re‐hospitalisations in treatment failure).
Duration of antimicrobial treatment (days after the start of the intervention).
Quality of life (as reported in the study).
Search methods for identification of studies
Electronic searches
We searched the following databases up to 29 November 2018:
the Cochrane Central Register of Controlled Trials (CENTRAL; 2018, Issue 11) in the Cochrane Library (Appendix 1);
MEDLINE via Ovid (1948 to November week 4, 2018) (Appendix 2);
Embase via Ovid (1980 to 2018 week 48) (Appendix 3);
LILACS (1990 to November 2018) (Appendix 4).
The search included ongoing trials and unpublished trials in the following trial databases: National Cancer Institute, MetaRegister of Controlled Trials, Medical Research Council Clinical Trial Directory.
Searching other resources
We inspected the references of all identified studies as well as major reviews for more studies. We also searched the following conference proceedings for unpublished trials: ICAAC (Interscience Conference on Antimicrobial Agents and Chemotherapy), ASH (Annual Meeting ‐ American Society of Hematology), IDSA (Infectious Diseases Society of America), ECCMID (European Congress of Clinical Microbiology and Infectious Diseases).
Data collection and analysis
Selection of studies
Two review authors (ODCM and SRC) independently inspected the abstract of each reference identified by the search and applied the inclusion criteria. We obtained all possible relevant abstracts as full‐text articles and two review authors (ODCM and SRC) independently further assessed these for inclusion.
We documented the reasons for exclusion and we resolved any disagreements by consensus.
Data extraction and management
Two review authors independently extracted data from included trials (OCM, MVK). We resolved any disagreements by consensus or by involving a third person (RRR or MGMN). We documented and discussed the extraction data. We collected all data on an intention‐to‐treat basis, whenever possible.
We identified trials by the name of the first author and year in which the trial was first published and ordered chronologically.
We extracted, checked, and recorded the following data:
1) Characteristics of the trials
Date, location, and setting trial (e.g. inpatients or ambulatory patients (outpatients))
Case definitions used (inclusion and exclusion criteria)
Country
Sponsor of trial (specified, known or unknown)
Design (intention‐to‐treat, method of randomisation, and allocation)
2) Characteristics of participants
Number of participants in each group
Age (median, mean)
Type of participant (child, adult)
Gender
Underlying malignancy (haematological or solid)
Neutrophil count in each group (below 1,000 or 500 or 100/mm3)
3) Characteristics of interventions
Type of intervention: exclusively as inpatient; exclusively as outpatient; early discharge (e.g. 24 hours to 48 hours as inpatient, then as outpatient)
Initially with intravenous (IV) therapy followed by oral therapy
4) Characteristics of outcome measures
Treatment failure
Mortality
Duration of fever
Adverse drug reactions related to the antibiotics
Duration of neutropaenia
Duration of hospitalisation
Duration of antimicrobial treatment
Quality of life
Assessment of risk of bias in included studies
Two review authors (RRR, OCM) assessed the methodological quality of included RCTs in accordance with guidelines in the Cochrane Handbook (Higgins 2011). Each quality component was classified according to 'Risk of bias' assessment tool as low, high, or unclear risk of bias.
Sequence generation
The method of randomisation was noted on the data extraction form. We coded the randomisation of participants to intervention groups as: low risk of bias (e.g. a computer‐generated random sequence or a table of random numbers), high risk of bias (e.g. date of birth, clinic ID, number, or surname), unclear (insufficient information).
Allocation concealment
We coded the concealment of allocation sequence as low risk of bias (e.g. central allocation, sealed envelopes), high risk of bias (e.g. open random allocation, envelopes unsealed), unclear (e.g. not reported, insufficient information).
Blinding of participants, personnel, outcome assessors
Low risk of bias (e.g. blinding of personnel or participants, or non‐blinding but appropriately assessed), high risk of bias (e.g. incomplete blinding or no blinding when outcome measure would be likely to be biased), unclear (e.g. insufficient data).
Incomplete outcome data
Low risk of bias (e.g. no missing data, missing data balanced between groups), high risk of bias (e.g. missing data of one or more of the primary outcome measures), unclear (insufficient information).
Selective reporting
Low risk of bias (e.g. all expected outcomes were reported), high risk of bias (e.g. not all of the primary outcomes were reported), unclear (insufficient information).
Measures of treatment effect
From each individual trial, for dichotomous variables (treatment failure, mortality, adverse drug reactions), the proportion was calculated by dividing the number of events in each group with the total population in the group. For continuous variables (duration of fever, duration of neutropaenia, duration of antimicrobial treatment, and duration of hospitalisation), we extracted means and standard deviations (SDs) reported from each group. If the median was reported, and the 95% confidence interval (CI) was available, then the SD was calculated. In studies where only median and range was reported, the data were extracted as reported.
Unit of analysis issues
The statistical unit of the analysis was the individual participant.
Dealing with missing data
Some studies did not report the standard deviation, which was calculated from the median and CIs.
Assessment of heterogeneity
For the interpretation of heterogeneity, the number of participants in each RCT, magnitude and direction of the effect, as well as the CIs were taken into account. For example, in the children's studies, the outcome variable (treatment failure) results of the intervention pointed in both directions. We assessed the level of heterogeneity (degree of difference between the results of different trials) between the results of the trials initially by inspection of the graphical presentations and by calculating a test of heterogeneity (Chi‐squared, I2) (Deeks 2001; Higgins 2003). We considered substantial heterogeneity levels if I2 was more than 50%.
Assessment of reporting biases
Due to the paucity of studies in each analysis, a funnel plot could not be analysed.
Data synthesis
We pooled the results from clinically similar studies in meta‐analyses using Review Manager 2014 (RevMan 5).
For any dichotomous outcomes, we pooled RRs, with 95% CIs;
For continuous outcomes, we pooled the weighted mean differences (MD) with 95% CIs between the treatment arms.
All meta‐analyses were performed using a random‐effects model (Mantel‐Haenszel method).
Summary of findings and certainty of evidence
Two review authors (RRR, OCM) independently rated the quality for each outcome. We provided a source and rationale for each assumed risk cited in the table(s) and we used the GRADE system to rank the certainty of the evidence using the GRADEprofiler Guideline Development Tool (GRADEproGDP) and the guidelines provided in Chapter 12.2 of the Cochrane Handbook (Schünemann 2011). We presented a summary of the evidence in a 'Summary of findings' table, which provides key information about the best estimate of the magnitude of the effect, in relative terms and absolute differences for each relevant comparison of alternative management strategies, the number of participants and studies addressing each important outcome, and the rating of the overall confidence in the effect estimates for the comparisons of each major primary outcome, including potential harms, as outlined in the Types of outcome measures section:
Treatment failure;
Mortality;
Duration of fever;
Adverse drug reactions related to the antibiotic regimen;
Duration of neutropaenia;
Duration of hospitalisation;
Duration of antimicrobial treatment.
We downgraded the evidence from 'high' certainty by one level for serious (or by two for very serious) concerns for each limitation:
High‐certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate‐certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.
Low‐certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect.
Very low‐certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect.
Subgroup analysis and investigation of heterogeneity
Considering that adult cancer patients are different from paediatric patients, all the data were presented separated for each group.
We performed subgroup analyses to investigate the effects of the type of intervention (exclusively inpatient versus exclusively outpatient; inpatient versus early discharge).
Results
Description of studies
Results of the search
See PRISMA flow diagram Figure 1.
1.
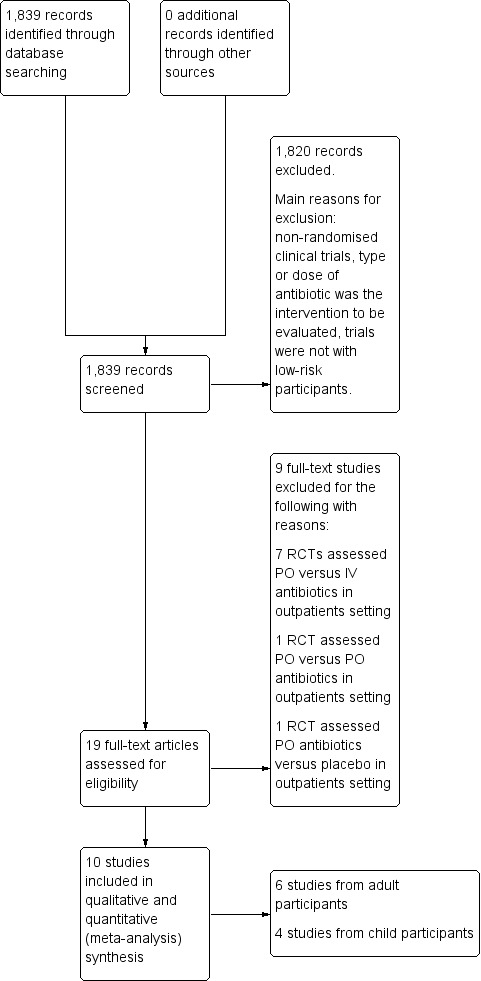
Study flow diagram.
The search strategy identified 1839 publications, after title and abstract screening. We considered 19 as potentially relevant publications and obtained the full‐text versions for further evaluation. We included a total of ten randomised controlled trials (RCTs) which fulfilled all the inclusion criteria (Ahmed 2007; Brack 2012; Hidalgo 1999; Innes 2003; López‐Hernández 2010; Malik 1995; Orme 2014; Rapoport 1999; Santolaya 2004; Talcott 2011). We reported details of each in the Characteristics of included studies table.
Included studies
The ten RCTs we identified had been published between 1995 and 2014 and included a total of 994 participants (range: 45 to 169 participants per trial). Half of the trials were single‐centre studies (Ahmed 2007; Hidalgo 1999; Innes 2003; López‐Hernández 2010; Orme 2014), and the other half were multicentre studies (Brack 2012; Malik 1995; Rapoport 1999; Santolaya 2004; Talcott 2011).
The single‐centre studies were performed in Spain (Hidalgo 1999), UK (Innes 2003), Egypt (Ahmed 2007), Mexico (López‐Hernández 2010) and Australia (Orme 2014). In the case of multicenter studies, three (Malik 1995; Santolaya 2004; Talcott 2011) were carried out in hospitals in one country (Egypt, Chile, and USA, respectively); one study was carried out in hospitals in Switzerland and Germany (Brack 2012) and one (Rapoport 1999) in six countries (South Africa, Colombia, Israel, Perú, Argentina, Spain).
Type of participants
Of the total participants, 52.3% were women, with a male to female ratio of 0.91. In five studies, the ages of participants ranged from 18 to 81 years (Hidalgo 1999; Innes 2003; Malik 1995; Rapoport 1999; Talcott 2011). Four studies included paediatric participants only (under 18 years) (Ahmed 2007; Brack 2012; Orme 2014; Santolaya 2004) and in the remaining study (López‐Hernández 2010), the age of participants ranged from 10 to 63 years (this study was included in the analysis for adults).
With regard to the type of cancer, five studies included participants diagnosed with leukaemia, lymphoma, and solid tumours (Ahmed 2007; Brack 2012; Malik 1995; Santolaya 2004; Talcott 2011); in three studies, participants had solid tumours and lymphomas (Hidalgo 1999; Innes 2003; Rapoport 1999); in one study, participants had acute lymphoblastic leukaemia and solid tumours (Orme 2014), and in another participants had only acute lymphoblastic leukaemia (López‐Hernández 2010). Thus, it should be noted that in all of the 10 studies, participants with leukaemia and lymphoma were included, ranging from 4.7% to 100% (median 39%).
Low‐risk febrile neutropaenic definitions
In additional Table 3, we describe the criteria used to consider low‐risk febrile episodes in the included studies. The definitions were not standardised, but criteria were consistent with regard to the following aspects: participants must not have comorbidities requiring hospitalisation, focal and/or severe infections, or relapse of the disease, and must not be receiving intensive chemotherapy.
1. Criteria used to consider low‐risk febrile episodes.
| Author | Type of participants | Low risk definition used |
| Malik 1995 | Adults | Participants that did not have any of the following: history of recurrent pyrexia or undetermined origin; shock (systolic blood pressure < 80 mmHg or peripheral circulatory failure); any comorbid condition requiring hospitalisation (except anaemia or thrombocytopaenia); and expectation of prolonged neutropaenia (> 7 days) based on aplastic anaemia, myelodysplasia, leukaemia or other causes, except if leukaemia patients were receiving consolidation of maintenance therapy or growth stimulation factors. |
| Rapoport 1999 | Adults | Patients that did not have renal failure requiring dialysis, suspected meningitis, known HIV infection, septic shock, or likelihood to expire within 48 h of study entry. |
| Hidalgo 1999 | Adults | Patients with an Eastern Cooperative Oncology Group (ECOG) performance status of 0 to 2, and did not have any of the following: progression of their malignant disease; signs or symptoms of a potentially severe infection (hypotension, oliguria, altered mental status, tachypnoea, respiratory failure, clotting abnormality, or acidosis); a serious focal infection (pneumonia, extensive cellulitis, meningitis, or pyelonephritis); hypercalcaemia; uncontrolled bleeding; cardiac, renal or liver failure; or another comorbid condition that required admission to the hospital. |
| Innes 2003 | Adults | Participants were required to be haemodynamically stable with no signs or symptoms that required intravenous fluid support, and adequate renal function. Participants must not have a coexisting medical condition that would require targeted or prolonged duration of antibiotic therapy (e.g. cellulitis, abscess, pneumonia, CVC tunnel infection). |
| López‐Hernández 2010 | Adults | Patients with acute leukaemia in complete remission, absence of an identifiable focus of infection (except for acute respiratory infections); absence of comorbidity conditions or organ failure (except for bone marrow); expected recovery of neutropaenia (> 0.10 x 109/L) in the next 8 days. |
| Talcott 2011 | Adults | Participants were evaluated for risk assessment criteria by the author. Participants did not have an indication for hospitalisation (other than fever); systemic hypotension; altered mental status; respiratory failure or inadequate oral fluid intake during 24 h observation; AIDS‐associated malignancy; neutropaenia arising from more than 21 days of chemotherapy and intensive chemotherapy requiring bone marrow or peripheral stem‐cell support. For leukaemia, participants must have bone marrow‐proven complete remission, and without leukaemia, no evidence of disease progression after the initial chemotherapy regimen or at least two cycles of a subsequent regimen. |
| Santolaya 2004 | Children | Participants were evaluated with a previously validated risk prediction model. Participants with less than 90 mg/L serum‐C reactive protein (CRP), absence of hypotension, absence of relapse or leukaemia as cancer type, platelet count of > 50,000/μL and > 7 days of receiving chemotherapy were classified as low risk. |
| Ahmed 2007 | Children | The following criteria must be fulfilled at 72 h: afebrile for a minimum of 24 h prior to the assessment point; negative initial blood cultures or two negative repeat blood cultures (24 h apart) if initially positive; absence (or substantial resolution) of manifestations of localised infection; Lansky performance scale 80 to 100, Karnosfy scale 80 to 100 if > 16 years; neutrophil absolute count > 100 μL; patient not in or after first induction therapy for acute myeloblastic leukaemia; discharge destination 1 h travel time from the medical centre. |
| Brack 2012 | Children | Participants had to fulfil 10 predefined low‐risk criteria: diagnosis not AML/mature B‐ALL/NHL; bone marrow involvement < 25%; no comorbidity requiring hospitalisation: no arterial hypotension, no hypo‐oxygenation [SpO2 < 94% at ambient air], no radiologically defined pneumonia, no focal infection, initial blood cultures negative and fever always < 39.5°C. |
| Orme 2014 | Children | Patients were considered low risk if they had: no signs of septic shock (including hypotension, tachycardia, delayed capillary refill or rigor); no significant comorbidities requiring inpatient monitoring or treatment including clinical focus of infection, pain, mucositis, vomiting, diarrhoea, or dehydration; no acute myeloid leukaemia diagnosis (AML), mature B‐cell lymphoma diagnosis, or were not in the induction phase of acute lymphoblastic leukaemia, or were not receiving predominantly high dose stem cell‐supported chemotherapy. |
AIDS: acquired immune deficiency syndrome AML: acute myeloid leukaemia B‐ALL: Cell B‐ acute lymphoblastic leukaemia CRP: serum‐C reactive protein CVC: central venous catheter ECOG: Eastern Cooperative Oncology Group NHL: non‐Hodgkin lymphoma
Intervention
It is important to mention that in most of the RCTs (N = 8) the intervention was early discharge: participants were kept under surveillance for 24 to 72 hours in hospital before returning home (Ahmed 2007; Brack 2012; Innes 2003; López‐Hernández 2010; Orme 2014; Rapoport 1999; Santolaya 2004; Talcott 2011). In only two studies, participants were discharged almost immediately after randomisation (Hidalgo 1999; Malik 1995), so, these two trials compared empiric antimicrobial therapy in exclusively outpatient versus exclusively inpatient settings. In these two studies, the proportion of participants with solid tumours were 69.2% and 89.5%.
As for the type of empirical antimicrobial therapy used, hospitalised participants were given intravenous treatment in nine studies and in only one study participants received oral ofloxacin (Malik 1995). In contrast, participants who were discharged to their home received the antimicrobial treatment orally in six studies (Brack 2012; Hidalgo 1999; Innes 2003; López‐Hernández 2010; Malik 1995; Santolaya 2004) and, in four studies (Ahmed 2007; Orme 2014; Rapoport 1999; Talcott 2011), treatment was administered parenterally by nurses.
Empirical antimicrobial schemes used differed among studies. In hospitalised participants, the combination of two antimicrobials was used in most studies, whereas three studies used monotherapy: ofloxacin (Malik 1995), imipenem (Ahmed 2007) or cefepime (Orme 2014). In the five outpatient studies, ofloxacin (Hidalgo 1999; Malik 1995), cefuroxime (Santolaya 2004), gatifloxacin (López‐Hernández 2010), or cefepime (Orme 2014) was administered as monotherapy.
Excluded studies
We excluded nine studies for reasons described in the Characteristics of excluded studies table. Reasons for exclusion were the following:
Studies which randomised oral versus intravenous antibiotic treatment in outpatients: seven trials (Gupta 2009; Minotti 1999; Mullen 1999; Paganini 2001; Paganini 2003; Petrilli 2000; Rubenstein 1993);
Studies which randomised two oral antibiotics in outpatients: one trial (Kern 2013);
Studies which randomised oral antibiotic treatment and placebo in outpatients: one trial (Klaassen 2000).
Risk of bias in included studies
See Figure 2 and Figure 3 for visual representations of the assessment of risk of bias across all studies and for each item in the included studies. See the section Risk of bias in included studies for further information about the bias identified within the individual studies.
2.
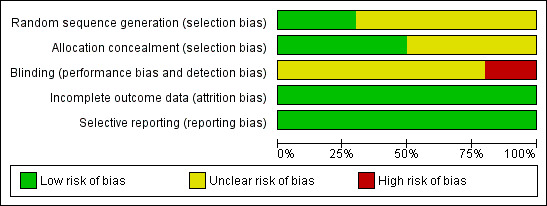
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
3.
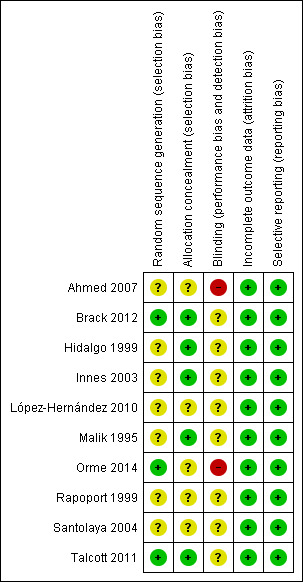
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
The randomisation process was adequately performed in only three studies (Brack 2012; Orme 2014; Talcott 2011); in the other seven trials, it was not possible to determine how the randomisation was done. Allocation concealment was adequate in five studies (classified as having low risk of bias) (Brack 2012; Hidalgo 1999; Innes 2003; Malik 1995; Talcott 2011). In the remaining five studies, the method of allocation concealment was not reported, so they were classified as having unclear risk of bias (Ahmed 2007; López‐Hernández 2010; Orme 2014; Rapoport 1999; Santolaya 2004) (Figure 2).
Blinding
It was clearly reported that two studies were unblinded (Ahmed 2007; Orme 2014). The other eight trials were classified as having an uncertain risk of bias because the authors did not accurately describe the blinding process. However, blinding was unlikely since it was obvious that empirical antimicrobial therapy was being received in or out of hospital. Therefore, in all 10 trials, detection bias could have been present.
Incomplete outcome data
According to data reported in the 10 trials, all participants included in the studies had complete follow‐up.
Selective reporting
In each of the 10 trials, the outcomes described in the methods section were reported appropriately.
Other potential sources of bias
For this review, the presence of any other bias that might influence the results was not apparent.
Effects of interventions
Summary of findings for the main comparison. Outpatients compared to inpatients ‐ adults for people with cancer who develop a low‐risk febrile neutropaenic event.
| Outpatients compared to inpatients ‐ adults for people with cancer who develop a low‐risk febrile neutropaenic event | ||||||
| Patient or population: Adult patients with cancer who develop a low‐risk febrile neutropaenic event Setting: Oncology of tertiary care hospitals Intervention: Outpatient empirical antimicrobial therapy Comparison: Inpatient empirical antimicrobial therapy | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with inpatients ‐ adults | Risk with outpatients ‐ adults | |||||
| Treatment failure | Study population | RR 1.23 (0.82 to 1.85) | 628 (6 RCTs) | ⊕⊕⊕⊝ MODERATE 1 | ||
| 112 per 1000 | 138 per 1000 (92 to 207) | |||||
| Mortality | Study population | RR 1.04 (0.29 to 3.71) | 628 (6 RCTs) | ⊕⊕⊕⊝ MODERATE | ||
| 12 per 1000 | 13 per 1000 (4 to 46) | |||||
| Duration of fever (days) | Mean days of fever was 3.6 | Mean days of fever was on average 0.2 higher (95% CI 0.36 lower to 0.76 higher) |
‐ | 169 (1 RCT) | ⊕⊕⊝⊝ LOW 2 3 | |
| Adverse drugs reactions | Study population | RR 8.39 (0.38 to 187.15) | 375 (3 RCTs) | ⊕⊕⊝⊝ LOW 3 4 | ||
| 5 per 1000 | 45 per 1000 (2 to 1000) | |||||
| Duration of neutropaenia (days) | Mean days of neutropaenia was 4.7 | Mean days of neutropaenia was on average 0.1 higher (95% CI 0.59 lower to 0.79 higher) | ‐ | 169 (1 RCT) | ⊕⊕⊝⊝ LOW 2 3 | |
| Duration of hospitalisation (days) | Mean days of hospitalisation ranged from 4.4 to 8. | Mean days of hospitalisation was on average ‐1.64 lower (95% CI ‐2.22 lower to ‐1.06 lower) | ‐ | 251 (3 RCTs) | ⊕⊕⊝⊝ LOW 5 | |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; OR: Odds ratio; | ||||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1 Four studies had appropriate allocation processes; in only one study the randomisation process was well stated; none were blinded. 2 The allocation process was appropriate, but randomisation and blinding were unclear. 3 CIs were wide. 4 In two studies, the allocation process was appropriate; in one study, the randomisation process was well stated. Blinding was unclear in three studies. 5 The allocation process was appropriate in only one study. Randomisation and blinding in the three studies were unclear.
Summary of findings 2. Outpatients compared to inpatients ‐ children for people with cancer who develop a low‐risk febrile neutropaenic event.
| Outpatients compared to inpatients ‐ children for people with cancer who develop a low‐risk febrile neutropaenic event | ||||||
| Patient or population: Children with cancer who develop a low‐risk febrile neutropaenic event Setting: Oncology or tertiary care hospitals Intervention: Outpatient empirical antimicrobial therapy Comparison: Inpatient empirical antimicrobial therapy | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with inpatients ‐ children | Risk with outpatients ‐ children | |||||
| Treatment failure | Study population | RR 1.04 (0.55 to 1.99) | 366 (4 RCTs) | ⊕⊕⊕⊝ MODERATE 1 | ||
| 94 per 1000 | 98 per 1000 (52 to 187) | |||||
| Mortality | Study population | RR 0.63 (0.15 to 2.70) | 329 (3 RCTs) | ⊕⊕⊕⊝ MODERATE 2 | ||
| 25 per 1000 | 15 per 1000 (4 to 66) | |||||
| Duration of fever (days) | Mean days of fever ranged from 2.4 to 3.6 | Mean days of fever was on average ‐0.06 lower (95% CI ‐0.84 lower to 0.71 higher) | ‐ | 305 (3 RCTs) | ⊕⊕⊝⊝ LOW 3 4 | |
| Adverse drug reactions | Study population | RR 1.90 (0.61 to 5.98) | 156 (2 RCTs) | ⊕⊕⊝⊝ LOW 4 5 | ||
| 53 per 1000 | 100 per 1000 (32 to 315) | |||||
| Duration of neutropaenia (days) | Mean days of neutropaenia ranged from 3.9 to 12.3 | Mean days of neutropaenia was on average ‐0.65 lower (95% CI ‐1.86 lower to 0.55 higher) | ‐ | 268 (2 RCTs) | ⊕⊕⊕⊝ MODERATE 6 | |
| Duration of hospitalisation (days) | Mean days of hospitalisation was 10.4 | Mean days of hospitalisation was on average ‐3.9 lower (95% CI ‐5.37 lower to ‐2.43 lower) | ‐ | 119 (1 RCT) | ⊕⊕⊝⊝ LOW 7 | |
| Duration of antimicrobial treatment (days) | Mean days of antimicrobial treatment ranged from 4.8 to 10.4 | Mean days of antimicrobial treatment was on average ‐0.07 lower (95%CI ‐1.26 lower to 1.12 higher) | ‐ | 305 (3 RCTs) | ⊕⊕⊝⊝ LOW 3 8 | |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; OR: Odds ratio; | ||||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1 The randomisation process was well stated in two studies; allocation was appropriate in one study; blinding was not done in two studies and was unclear in two studies. 2 Randomisation was unclear in three studies; the allocation process was well stated in one study; blinding was unclear in two studies and in one was not done. 3 The randomisation process was well stated in one study; allocation was unclear in three studies; blinding was not done in two studies and in one study was unclear. 4 CIs were wide. 5 The randomisation process was well stated in one study; allocation was unclear in two studies; blinding was not done in two studies. 6 The randomisation and allocation processes were unclear in two studies; blinding was not done in one study and was unclear in one study. 7 Randomisation and allocation were unclear; blinding was not done. 8 Statistical tests suggested substantial heterogeneity.
Primary outcomes
Treatment failure
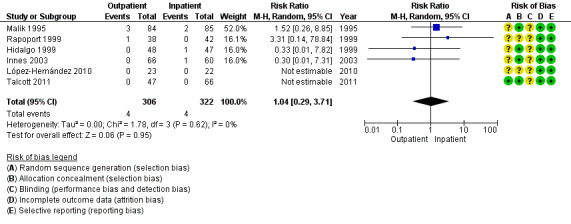
Ten RCTs, six studies in adults (628 participants) (Hidalgo 1999; Innes 2003; López‐Hernández 2010; Malik 1995; Rapoport 1999; Talcott 2011) and four in children (366 participants) (Ahmed 2007; Brack 2012; Orme 2014; Santolaya 2004) reported treatment efficacy. The outpatient management of low‐risk febrile neutropaenia showed no clear difference when compared to the inpatient group, either in adult participants (RR 1.23, 95% CI 0.82 to 1.85; P = 0.33, I2 0.0%; moderate‐certainty evidence) (Analysis 1.1, Figure 4) or in children (RR 1.04, 95% CI 0.55 to 1.99; P = 0.53; I2 0%; moderate‐certainty evidence) (Analysis 2.1).
1.1. Analysis.
Comparison 1 Outpatients versus inpatients ‐ adults, Outcome 1 Treatment failure.
4.

Forest plot of comparison: 1 Outpatients versus inpatients ‐ adults, outcome: 1.1 Treatment failure.
2.1. Analysis.
Comparison 2 Outpatients versus inpatients ‐ children, Outcome 1 Treatment failure.
Mortality
All but one trial (Orme 2014) reported mortality. We also found no clear difference between outpatient and inpatient groups, both for adults (RR 1.04, 95% CI 0.29 to 3.71; P = 0.95, I2 0.0%; six studies, 628 participants; moderate‐certainty evidence) (Analysis 1.2, Figure 5) or children (RR 0.63, 95% CI 0.15 to 2.70; P = 0.53; I2 0.0%; three studies, 329 participants; moderate‐certainty evidence) (Analysis 2.2).
1.2. Analysis.
Comparison 1 Outpatients versus inpatients ‐ adults, Outcome 2 Mortality.
5.
Forest plot of comparison: 1 Outpatients versus inpatients ‐ adults, outcome: 1.2 Mortality.
2.2. Analysis.
Comparison 2 Outpatients versus inpatients ‐ children, Outcome 2 Mortality.
Secondary outcomes
Duration of fever
Eight studies analysed duration of fever; four in adult participants (López‐Hernández 2010; Malik 1995; Rapoport 1999; Talcott 2011) and four in children (Ahmed 2007; Brack 2012; Orme 2014; Santolaya 2004). Meta‐analysis could only be done with one study in adult participants (Malik 1995) comparing an outpatient group against an inpatient group, and no differences were found (MD 0.20 days, 95% CI ‐0.36 to 0.76; P = 0.48; 169 participants; low‐certainty evidence) (Analysis 1.3). Similar findings (P > 0.05) were found in the other three studies; one reported that, in both groups, the median time for fever to resolve was two days (Rapoport 1999), while in another (López‐Hernández 2010), the median for the two groups was three days with a range of one to seven days for the inpatient group and one to six days for the outpatient group. Talcott and colleagues (Talcott 2011) reported that the average was 3.4 days (range 1 to 14) and 3.2 days (range 0 to 13), respectively.
1.3. Analysis.
Comparison 1 Outpatients versus inpatients ‐ adults, Outcome 3 Duration of fever (days).
In the four studies of children, there was also no evidence of a difference, nor in a meta‐analysis including three of these studies (Ahmed 2007; Orme 2014; Santolaya 2004) (MD ‐0.06 days, 95% CI ‐0.84 to 0.71; P = 0.08, I2 61%; 305 participants; low‐certainty evidence) (Analysis 2.3), or in the study by Brack and colleagues (Brack 2012), which reported that the median for the inpatient group was 1.5 days (range 0 to 10) and 1.0 day (range 0 to 11) for the outpatient group (P = 0.19).
2.3. Analysis.
Comparison 2 Outpatients versus inpatients ‐ children, Outcome 3 Duration of fever (days).
Adverse drug reactions related to the antibiotic regimen
We extracted data on adverse effects related to the antibiotic regimen from five RCTs; three of adult participants (Innes 2003; Malik 1995; Rapoport 1999) and two of children (Ahmed 2007; Orme 2014). Among adult participants, in one RCT (Rapoport 1999), no adverse events were reported in any of the two groups; In the other two studies, there were more adverse events in the outpatient group; however, there was no evidence of a difference between outpatient and inpatient groups (RR 8.39, 95% CI 0.38 to 187.15; P = 0.18; I2 66% ; three studies, 375 participants; low‐certainty evidence) (Analysis 1.4). Also, in the two RCTs of children there were more adverse events in the outpatient group, but no difference statistically (RR 1.90, 95% CI 0.61 to 5.98; P = 0.27; 156 participants; low‐certainty evidence) (Analysis 2.4). These adverse events were mainly related to digestive intolerance to oral antimicrobial treatment (diarrhoea, nausea, vomiting); only one study reported that the use of imipenem caused nausea and vomiting in the inpatient group (Ahmed 2007).
1.4. Analysis.
Comparison 1 Outpatients versus inpatients ‐ adults, Outcome 4 Adverse drug reactions.
2.4. Analysis.
Comparison 2 Outpatients versus inpatients ‐ children, Outcome 4 Adverse drug reactions.
It should be noted that failure of empirical antimicrobial treatment in the outpatient group, in some cases, was due to adverse events. One RCT (Innes 2003) reported that three of the 10 failures were caused by vomiting (one participant) or severe oesophagitis (two participants).
Duration of neutropaenia
Three RCTs of adults reported duration of neutropaenia (Malik 1995; Rapoport 1999; Talcott 2011); there was no evidence of a difference between the outpatient group and inpatient group in the Malik study (Malik 1995) (MD 0.10, 95% CI ‐0.59 to 0.79; P = 0.78; 169 participants; low‐certainty evidence) (Analysis 1.5). Rapoport and colleagues reported that the median for neutrophil recovery for two groups was three days, with no evidence of a difference between the groups (Rapoport 1999). Similar findings were reported in the study by Talcott (Talcott 2011); 4.1 days (range 1 to 10) was the mean time for neutropaenia recovery in the outpatient group, and 4.2 days (range 1 to 15) in the outpatient group (P = 0.80).
1.5. Analysis.
Comparison 1 Outpatients versus inpatients ‐ adults, Outcome 5 Duration of neutropaenia (days).
In two studies of children, the days with neutropaenia were reported (Santolaya 2004; Ahmed 2007); there was also no evidence of a difference between groups (MD ‐0.65, 95% CI ‐1.86 to 0.55; P = 0.29, I2 0%; 268 participants; moderate‐certainty evidence) (Analysis 2.5).
2.5. Analysis.
Comparison 2 Outpatients versus inpatients ‐ children, Outcome 5 Duration of neutropaenia (days).
Duration of hospitalisation
Meta‐analysis of hospitalisation time was performed in three RCTs of adults (Innes 2003; López‐Hernández 2010; Rapoport 1999), in which shorter hospital stay was obtained in the outpatient group compared to the inpatient group. (MD ‐1.64, 95% CI ‐2.22 to ‐1.06; P < 0.0001, I2 0%; 251 participants; low‐certainty evidence) (Analysis 1.6).
1.6. Analysis.
Comparison 1 Outpatients versus inpatients ‐ adults, Outcome 6 Duration of hospitalisation (days).
In two studies of children, fewer days of hospitalisation were also reported, both in the study of Ahmed 2007 (MD ‐3.9, 95% CI ‐5.37 to ‐2.43; P < 0.00001; 119 participants; low‐certainty evidence) (Analysis 2.6), and in that of Santolaya 2004 which reported a mean of 1.0 day (range 1 to 2) in the outpatient group, and a mean of 5.3 days (range 3 to 9) in the inpatient group (P < 0.001).
2.6. Analysis.
Comparison 2 Outpatients versus inpatients ‐ children, Outcome 6 Duration of hospitalisation (days).
Duration of antimicrobial treatment
Only one RCT of adult participants included this outcome (Rapoport 1999); the authors reported that the median for the inpatient group was 6.3 days and 6.0 days for the outpatient group.
Four studies of children compared treatment time of antimicrobial use between the two groups, but only three were included in the meta‐analysis (Ahmed 2007; Orme 2014; Santolaya 2004). We found no evidence of a difference in the number of days of antimicrobial treatment between outpatient and inpatient groups: MD ‐0.07, 95% CI ‐1.26 to 1.12; P = 0.10, I2 57%; 305 participants; low‐certainty evidence) (Analysis 2.7). Brack and colleagues also found no evidence of a difference (Brack 2012), the median for the outpatient group was five days (range 3 to 18) and for the inpatient group was five days (range 2 to 19) (P = 0.34).
2.7. Analysis.
Comparison 2 Outpatients versus inpatients ‐ children, Outcome 7 Duration of antimicrobial treatment (days).
Quality of life (QoL)
Only two studies explored QoL in participants with low‐risk febrile episodes. In the first study (Talcott 2011), the trial authors reported that pain decreased for home care of adult participants and slightly increased for hospitalised participants (change, ‐13.1 versus. 2.72; P = 0.01). They also indicated that the role function subscale of the EORTIC QLQ C‐30 increased in both groups, but less for home‐care participants than for hospitalised participants (change, 0.58 versus 0.78; P = 0.05); however, emotional function scores increased for home‐care participants and declined for hospitalised participants (change, 3.27 versus ‐6.94; P = 0.04). They did not find evidence of differences relating to the consumer satisfaction or general well‐being instruments.
Most recently, Orme 2014 compared QoL every day during the low‐risk episode in child participants. They used a modified version of a QoL instrument used previously in children receiving home chemotherapy (Close 1995); this is a visual analogue scale which assesses seven patient variables and six parent variables. The authors reported that baseline questionnaires were similar between the outpatient and inpatient groups. In the outpatient group, parents showed higher level of QoL on days 2, 3 and 4; however, they showed higher levels of concern about their child's condition and a lower level of confidence in their ability to care for the child. Meanwhile, the responses of QoL from children trended higher in the outpatient group, particularly for sleep and appetite.
Analysis according to type of intervention
In order to determine if there was a difference in the results according to the type of intervention (early discharge or exclusively outpatient), we performed analyses only for the main outcome variable, treatment failure. Meta‐analysis of the 4 RCTs in adults (Innes 2003; López‐Hernández 2010; Rapoport 1999; Talcott 2011) with early discharge (RR 1.48, 95% CI 0.74 to 2.95; P = 0.26, I2 0%; 364 participants moderate‐certainty evidence) (Analysis 3.1) was similar to the results of the exclusively outpatient (Hidalgo 1999; Malik 1995) meta‐analysis (RR 1.15, 95% CI 0.62 to 2.13; P = 0.65, I2 19%; two studies; 264 participants; moderate‐certainty evidence) (Analysis 4.1).
3.1. Analysis.
Comparison 3 Early discharge ‐ adults, Outcome 1 Treatment failure.
4.1. Analysis.
Comparison 4 Exclusively outpatient vs Exclusively inpatient, Outcome 1 Treatment failure.
Discussion
Summary of main results
This systematic review synthesised the evidence from 10 RCTs comparing inpatient empirical antimicrobial therapy versus outpatient management for patients with low‐risk febrile neutropaenia. The results showed no evidence of differences between outpatient and inpatient treatment of low‐risk febrile neutropaenia in terms of treatment failure and mortality, in either adults or children. Of note, given the risk of bias detected, and the wide 95% CIs for main outcome measures, particularly for RCTs in children, we have only moderate‐certainty about the results.
It is also important to consider that there were only two RCTs comparing outpatient versus inpatient treatments, so most of the data were from RCTs exploring an early discharge strategy. In addition, more than 60% of the participants were patients with diagnoses of solid tumours.
When considering other outcome measures, the different meta‐analyses showed that resolution of fever, duration of neutropaenia, and adverse drug reactions were similar between the outpatient and the inpatient groups; however, for these outcome measures there was low‐certainty of evidence, so the difference between the two interventions may be substantially different from the estimated effect. It should be noted that, in six RCTs, there was consistency in the reduction of the length of hospitalisation in the outpatient strategy, both in trials of adults and children. As for quality of life, more evidence is needed to determine if there is any advantage between the two interventions.
In conclusion, this meta‐analysis shows that there is low to moderately‐certain evidence to support the conclusion that outpatient treatment is as effective as inpatient treatment for people with low‐risk febrile neutropaenia, in either an adult or paediatric population. It should also be considered that the number of RCT published so far is limited.
Overall completeness and applicability of evidence
Outpatient therapy for the administration of empiric antimicrobial therapy may be a safe alternative to inpatient therapy for low‐risk cancer patients with an episode of febrile neutropaenia.
It is important to consider that the main intervention in this meta‐analysis was not standardised. Almost all studies used the early discharge approach for participants with low‐risk febrile neutropaenia episodes. In only two studies, participants assigned to outpatient treatment were discharged immediately after the administration of the first antibiotic dose (Hidalgo 1999; Malik 1995). All other studies used the early discharge strategy, where participants were inpatients and observed for 24 to 72 hours and, during this time, the first doses of empirical (usually intravenous) broad spectrum antimicrobial therapy were administered. Any participants who then fulfilled low‐risk criteria after clinical reassessment received outpatient treatment. The results of this systematic review and meta‐analysis are more directed towards the early discharge approach than immediate outpatient treatment.
The definition of low risk must be taken into account. Unlike adult patients, there is no accepted definition for 'low risk' in children with cancer. In the included RCTs, there were several variations in the criteria used to consider 'low risk' for serious infection, such as fever, type of chemotherapy, type of tumour, hypotension, relapse, count of platelets. This difference in the criteria used has been documented in studies that evaluated the risk stratification in children (Delebarre 2014). In adults, MASCC risk index for febrile neutropaenia has been incorporated in clinical guidelines since 2010; in this systematic review, only one study (Talcott 2011) used a MASCC risk index to select the participants.
Quality of the evidence
In general, the quality of the RCTs was of low‐ to moderate‐certainty according to the GRADE approach (Table 1; Table 2). The major problems in the 'risk of bias' assessment of the studies was related to randomisation, blinding, and the allocation processes. In only three studies did the authors appropriately report how randomisation was performed. In the six other studies, randomisation was classified as uncertain as it was not clearly specified how the randomisation sequence was done. In five studies, allocation concealment was carried out correctly.
Blinding was either not performed or unclear in all studies. The intervention consisted of providing the empirical antimicrobial therapy in the participants' homes or when hospitalised. As either intervention was obvious, then there may have been detection bias for certain outcomes such as the disappearance of fever and adverse effects, but nor for mortality.
Despite the fact that we observed no evidence of differences between adults and children for the early discharge approach and exclusive outpatients versus exclusive inpatients in the sensitivity analyses, the wide CIs obtained from most of the main outcome measures, should to be taken into account in the interpretation of the results.
Potential biases in the review process
This systematic review was carried out in accordance with the guidelines of Cochrane with assistance from the Information Specialist from the Cochrane Gynaecological, Neuro‐oncology & Orphan Cancers Group. We made every attempt to include published and unpublished studies. However, there remains the possibility that there may be other unpublished trials that we did not identify. This means that we may have unwittingly perpetuated a publication bias.
A meta‐analysis could not be performed for all the RCTs, as the outcomes (duration of antimicrobial treatment, duration of hospitalisation, duration of neutropaenia, and duration of fever in days), were reported as medians, and we did not contact the authors asking for the raw data.
Funnel plots could not be undertaken because the number of studies in adults and children was less than ten, therefore, publication bias could not be measured.
Agreements and disagreements with other studies or reviews
Systematic reviews have been published in the past on the use of empirical outpatient therapy. In 2011, Teuffel and colleagues (Teuffel 2011) carried out a meta‐analysis with 14 RCTs to determine the effectiveness of outpatient management of cancer patients with febrile neutropaenia. Of the 14 RCTs, six compared inpatient versus outpatient management, including 738 participants; results were: RR 0.81 (95% CI 0.32 to 2.71) for treatment failure, and RR 1.11 (95% CI 0.41 to 3.05) for mortality. In the present review, we included the same six studies plus four more that were published more recently, and found similar results. The other eight studies in the review by Teuffel and colleagues compared only the route of drug administration in the outpatient setting.
Unlike Teuffel and colleagues, in this review we evaluated other outcome measures such as fever, hospitalisation, adverse effects, and quality of life, but not the route of antibiotic administration. Another meta‐analysis found that the rates of treatment failure and mortality in adults and children receiving oral or intravenous antibiotic treatments were comparable, provided that the participants were haemodynamically stable, had no organ failure, could take oral medications, did not have pneumonia, central line infection or a severe soft‐tissue infection, and did not suffer from acute leukaemia (Vidal 2013). More recently, Loeffen and colleagues (Loeffen 2016) analysed very early discharge versus early discharge versus non‐early discharge in children with cancer and febrile neutropaenia. They found only two RCTs that met the selection criteria, and reported that meta‐analysis was not possible because the timing defined for participants’ discharge was different, as were the risk stratification models used. In this review, we included both studies (Brack 2012; Santolaya 2004) and integrated them into the meta‐analyses because the criteria we used were not so restricted.
Recently, in the updated recommendations for adult outpatient management (IDSA 2018), it was recommended that patients with low‐risk febrile neutropaenia should receive initial doses of antimicrobials within one hour of triage and be monitored for four hours or more before discharge. Our review supports this recommendation for outpatient treatment, but only two of six studies evaluated this approach.
Authors' conclusions
Implications for practice.
Outpatient therapy for the administration of empiric antimicrobial treatment may be an alternative strategy to inpatient therapy for low‐risk cancer patients with an episode of febrile neutropaenia in both adults and children. However, most of the evidence comes of RCTs for early discharge, rather than solely outpatient treatment, and therefore includes the administration of the initial doses of antimicrobials as inpatients and monitoring for twenty‐four hours or more before discharge.
Implications for research.
There is a need for RCTs that evaluate outpatient treatment strategies in neutropaenic people with cancer, including low‐income locations, especially in paediatric populations. In a new RCT with the main outcome of treatment failure, based on this meta‐analysis, approximately 622 participants would be necessary in each group to find a difference of 4% between groups. To expand knowledge, RCTs are required where a sole outpatient strategy is evaluated, not just early discharge.
In contrast with the adult population, for whom there is a formal classification for risk assessment (MASCC scoring system) (Klastersky 2000), for children with cancer and febrile neutropaenia, there is no accepted risk classification. Studies or consensus are required to standardise and offer empirical outpatient therapy in low‐risk children. More RCTs are needed in order to assess the advantages of outpatient treatment, related to different outcomes, including quality of life, cost, and feasibility.
To improve the evidence, in future RCTs, the criteria of low risk should be standardised (particularly in children); in addition, a correct random assignment and allocation concealment of the included participants should be ensured. Besides mortality and treatment failure, the outcome variables that need to be evaluated in more depth are duration of fever, adverse effects of antimicrobials, days of hospitalisation, quality of life, patient satisfaction, and costs.
What's new
| Date | Event | Description |
|---|---|---|
| 8 April 2019 | Amended | Minor typographical corrections made. |
Acknowledgements
We thank Robin Grant and Jo Morrison for clinical and editorial advice, Gail Quinn, Clare Jess, and Tracey Harrison for their contribution to the editorial process, and Jane Hayes and Jo Platt for designing the search strategy.
This project was supported by the National Institute for Health Research, via Cochrane Infrastructure funding to the Cochrane Gynaecological, Neuro‐oncology and Orphan Cancer Group. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS, or the Department of Health.
Appendices
Appendix 1. CENTRAL search strategy
#1 MeSH descriptor Neutropenia, this term only #2 neutrop* or granulo* or leukop* #3 (#1 OR #2) #4 MeSH descriptor Fever explode all trees #5 MeSH descriptor Bacterial Infections explode all trees #6 MeSH descriptor Sepsis explode all trees #7 fever* or febrile or infect* or sep* #8 (#4 OR #5 OR #6 OR #7) #9 MeSH descriptor Outpatients, this term only #10 outpatient* or out‐patient* #11 early discharge #12 MeSH descriptor Ambulatory Care, this term only #13 ambulatory #14 domicil* or home* #15 (#9 OR #10 OR #11 OR #12 OR #13 OR #14) #16 (#3 AND #8 AND #15)
Appendix 2. MEDLINE search strategy
1 Neutropenia/ 2 neutrop*.mp. 3 granulo*.mp. 4 leukop*.mp. 5 1 or 2 or 3 or 4 6 exp Fever/ 7 exp Bacterial Infections/ 8 exp Sepsis/ 9 fever*.mp. 10 febrile.mp. 11 infect*.mp. 12 sep*.mp. 13 6 or 7 or 8 or 9 or 10 or 11 or 12 14 Outpatients/ 15 (outpatient* or out‐patient*).mp. 16 early discharge.mp. 17 Ambulatory Care/ 18 ambulatory.mp. 19 (domicil* or home).mp. 20 14 or 15 or 16 or 17 or 18 or 19 21 randomized controlled trial.pt. 22 controlled clinical trial.pt. 23 randomized.ab. 24 placebo.ab. 25 drug therapy.fs. 26 randomly.ab. 27 trial.ab. 28 groups.ab. 29 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 30 5 and 13 and 20 and 29
key: mp=title, original title, abstract, name of substance word, subject heading word, unique identifier
Appendix 3. Embase search strategy
1 exp neutropenia/ 2 neutrop*.mp. 3 granulo*.mp. 4 leukop*.mp. 5 1 or 2 or 3 or 4 6 exp fever/ 7 exp bacterial infection/ 8 exp sepsis/ 9 fever*.mp. 10 febrile.mp. 11 infect*.mp. 12 sep*.mp. 13 6 or 7 or 8 or 9 or 10 or 11 or 12 14 outpatient/ 15 (outpatient* or out‐patient*).mp. 16 early discharge.mp. 17 exp ambulatory care/ 18 ambulatory.mp. 19 (domicil* or home).mp. 20 14 or 15 or 16 or 17 or 18 or 19 21 crossover procedure/ 22 randomized controlled trial/ 23 single blind procedure/ 24 random*.mp. 25 factorial*.mp. 26 (crossover* or cross over* or cross‐over).mp. 27 placebo*.mp. 28 (doubl* adj blind*).mp. 29 (singl* adj blind*).mp. 30 assign*.mp. 31 allocat*.mp. 32 volunteer*.mp. 33 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 34 5 and 13 and 20 and 33
key: mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword
Appendix 4. LILACS search strategy
1. Neutropenia or Neutropenia febril or Neutropenia febril por quimioterapia/
2. Cancer/
3. Neoplasia maligna/
Data and analyses
Comparison 1. Outpatients versus inpatients ‐ adults.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Treatment failure | 6 | 628 | Risk Ratio (M‐H, Random, 95% CI) | 1.23 [0.82, 1.85] |
| 2 Mortality | 6 | 628 | Risk Ratio (M‐H, Random, 95% CI) | 1.04 [0.29, 3.71] |
| 3 Duration of fever (days) | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 4 Adverse drug reactions | 3 | 375 | Risk Ratio (M‐H, Random, 95% CI) | 8.39 [0.38, 187.15] |
| 5 Duration of neutropaenia (days) | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 6 Duration of hospitalisation (days) | 3 | 251 | Mean Difference (IV, Random, 95% CI) | ‐1.64 [‐2.22, ‐1.06] |
Comparison 2. Outpatients versus inpatients ‐ children.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Treatment failure | 4 | 366 | Risk Ratio (M‐H, Random, 95% CI) | 1.04 [0.55, 1.99] |
| 2 Mortality | 3 | 329 | Risk Ratio (M‐H, Random, 95% CI) | 0.63 [0.15, 2.70] |
| 3 Duration of fever (days) | 3 | 305 | Mean Difference (IV, Random, 95% CI) | ‐0.06 [‐0.84, 0.71] |
| 4 Adverse drug reactions | 2 | 156 | Risk Ratio (M‐H, Random, 95% CI) | 1.90 [0.61, 5.98] |
| 5 Duration of neutropaenia (days) | 2 | 268 | Mean Difference (IV, Random, 95% CI) | ‐0.65 [‐1.86, 0.55] |
| 6 Duration of hospitalisation (days) | 1 | Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 7 Duration of antimicrobial treatment (days) | 3 | 305 | Mean Difference (IV, Random, 95% CI) | ‐0.07 [‐1.26, 1.12] |
Comparison 3. Early discharge ‐ adults.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Treatment failure | 4 | 364 | Risk Ratio (M‐H, Random, 95% CI) | 1.48 [0.74, 2.95] |
Comparison 4. Exclusively outpatient vs Exclusively inpatient.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Treatment failure | 2 | 264 | Risk Ratio (M‐H, Random, 95% CI) | 1.15 [0.62, 2.13] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Ahmed 2007.
| Methods | Randomised controlled trial | |
| Participants | 119 children (< 18 years old) with cancer, with febrile (> 38.5°C) neutropaenia (< 500 absolute neutrophil count/μL), with anticipated neutropaenia lasting 7 days or longer Single‐centre study | |
| Interventions | 61 participants received ceftriaxone (100 mg/kg/day) plus amikacin (15 mg/kg/day) IV every 24 hours; participants were discharged if during the next 72 h they were afebrile during 24 hours. 58 inpatients received imipenem 80 to 100 mg/kg/day every 6 hours IV. |
|
| Outcomes | Treatment failure, mortality, fever duration, adverse drug reactions, direct costs | |
| Notes | Early discharge criteria was achieved in only 32 of 61 episodes. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding (performance bias and detection bias) All outcomes | High risk | The study was not blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Data of 119 episodes were complete. |
| Selective reporting (reporting bias) | Low risk | All the data were included. |
Brack 2012.
| Methods | Randomised controlled trial | |
| Participants | 61 children (1 to 18 years old) with cancer, with febrile (> 38.5°C) neutropaenia (< 500 absolute neutrophil count//μL), after non‐myeloablative chemotherapy, and low‐risk criteria. Multicentre study from Swiss and German hospitals | |
| Interventions | 27 outpatients received a combination of oral ciprofloxacin (30 mg/kg/day) twice a day plus oral amoxicillin (65 to 80 mg/kg/day) twice a day. 34 inpatients received "empirical intravenous broad spectrum antimicrobial therapy, which covered Gram‐positive cocci plus Gram‐negative bacteria, adapted to local resistance patterns." |
|
| Outcomes | Treatment failure, mortality, fever duration. | |
| Notes | Some participants were randomised more than once. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation was block‐stratified per centre, based on a list of random numbers. |
| Allocation concealment (selection bias) | Low risk | A set of numbered sealed envelopes was available in each centre. |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Data of 61 episodes were complete. |
| Selective reporting (reporting bias) | Low risk | All the data were included. |
Hidalgo 1999.
| Methods | Randomised controlled trial | |
| Participants | 95 adults with cancer (> 18 years old), with febrile (> 38.5°C) neutropaenia (< 500 absolute neutrophil count//μL), with solid tumours treated with conventional doses of chemotherapy, and without comorbidity. Single‐center study | |
| Interventions | 47 outpatients received oral ofloxacin 400 mg twice a day. 48 inpatients received a combination of ceftazidime 2 g every 8 hours IV plus amikacin 500 mg every 12 hours IV. |
|
| Outcomes | Treatment failure, mortality | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Low risk | Sealed envelopes |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Data of 95 episodes were complete. |
| Selective reporting (reporting bias) | Low risk | All the data were included. |
Innes 2003.
| Methods | Randomised controlled trial | |
| Participants | 126 episodes of adults with cancer (> 18 years old), with febrile (> 38.0°C) neutropaenia (< 500 absolute neutrophil count/μL), with solid tumours or lymphomas treated with conventional dose of cytotoxic chemotherapy, and without comorbidity. Single‐center study | |
| Interventions | 66 outpatients after 24 h of hospitalisation were discharged with oral ciprofloxacin 750 mg twice a day plus amoxicillin (500 mg)‐clavulanate (175 mg) every 8 hours for 5 days. 60 inpatients received a combination of gentamicin 80 mg every 8 hours IV plus piperacillin (4 g) plus tazobactam (500 mg) every 8 h IV until hospital discharge. |
|
| Outcomes | Treatment failure, mortality, fever duration, adverse drug reactions, direct costs | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Low risk | Consecutive drawn sealed envelopes |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Data of 126 participants were complete. |
| Selective reporting (reporting bias) | Low risk | All the data were included. |
López‐Hernández 2010.
| Methods | Randomised controlled trial | |
| Participants | 45 acute lymphoblastic leukaemia adult and child participants (> 10 years old), with febrile (> 38.0°C) neutropaenia (< 500 absolute neutrophil count), treated with conventional non‐myeloablative chemotherapy, and without comorbidity. Single‐center study | |
| Interventions | 23 outpatients after 24 h of hospitalisation were discharged with oral gatifloxacin or moxifloxacin 400 mg per day. 22 inpatients received a combination of amikacin 15 mg/kg every 24 hours IV plus ceftriaxone 1 g every 8 hours IV. |
|
| Outcomes | Treatment failure, mortality, fever duration | |
| Notes | All participants received growth factors. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Data of 45 episodes were complete. |
| Selective reporting (reporting bias) | Low risk | All the data were included. |
Malik 1995.
| Methods | Randomised controlled trial | |
| Participants | 169 episodes of adults with cancer (> 16 years old), with febrile (> 38.5°C) neutropaenia (< 500 polymorphonuclear leukocytes), and without any comorbidity. Included participants were from 2 hospitals. | |
| Interventions | Participants with 84 outpatient episodes received oral ofloxacin 400 mg twice a day. Participants with 85 inpatient episodes received oral ofloxacin 400 mg twice a day. |
|
| Outcomes | Treatment failure, mortality, time of fever, adverse drug reactions | |
| Notes | Leukaemia participants received growth factors. Several participants were randomised more than once (47 episodes). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Low risk | Consecutive drawn sealed envelopes |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Data of 169 episodes were complete. |
| Selective reporting (reporting bias) | Low risk | All the data were included. |
Orme 2014.
| Methods | Randomised controlled trial | |
| Participants | 37 children (1 ‐ 18 years old) with cancer, with febrile (> 38.5°C) neutropaenia (< 500 absolute neutrophil count), and with chemotherapy considered as low or moderate intensity. Single‐centre study | |
| Interventions | 19 outpatients received cefepime (50 mg/kg) twice a day IV. 18 inpatients received cefepime (50 mg/kg) twice a day IV. |
|
| Outcomes | Treatment failure, time of fever, adverse drug reactions, quality of life | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote "randomisation was blocked using randomly permuted block sizes.", stratified by disease (acute leukaemia vs other diagnoses) and age (1 to 5 years old vs > 6 years old). |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding (performance bias and detection bias) All outcomes | High risk | The study was unblinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Data of 37 episodes were complete. |
| Selective reporting (reporting bias) | Low risk | All the data were included. |
Rapoport 1999.
| Methods | Randomised controlled trial | |
| Participants | 80 adults with cancer (> 19 years old), with febrile (> 38.0°C) neutropaenia (< 500 absolute neutrophil count), with non‐myeloid malignancies after chemotherapy, and without comorbidity. Multicentre study | |
| Interventions | 38 participants received ceftriaxone (2 g) plus an aminoglycoside (gentamicin, netilmicin, or amikacin) IV every 24 hours; participants were discharged if during the next 48 to 72 hours body temperature decreased. 42 inpatients received ceftriaxone (2 g) plus an aminoglycoside (gentamicin, netilmicin, or amikacin) IV every 24 hours. |
|
| Outcomes | Treatment failure, mortality, time of fever, duration of neutropaenia, adverse drug reactions | |
| Notes | All participants received growth factors. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Data of 80 episodes were complete. |
| Selective reporting (reporting bias) | Low risk | All the data were included, however data reported were not clear for time of defervescence and duration of neutropaenia. |
Santolaya 2004.
| Methods | Randomised controlled trial | |
| Participants | 149 children (< 18 years old) with cancer, with febrile (> 38.5°C) neutropaenia (< 500 absolute neutrophil count), and with low risk of invasive bacterial infection (IBI). Multicentre study | |
| Interventions | 78 participants received ceftriaxone IV (100 mg/kg/day) every 24 h plus teicoplanin IV (10 mg/kg/day) every 24 h during 3 days; if during the next 24 to 36 h participants had a low‐risk episode of IBI, they were discharged. When participants had a favourable evolution therapy, they were switched to oral cefuroxime (50 mg/kg/day). 71 inpatients received ceftriaxone IV (100 mg/kg/day) every 24 h plus teicoplanin IV (10 mg/kg/day) every 24 h. When participants had a favourable evolution therapy after 3 days, they were switched to oral cefuroxime (50 mg/kg/day). |
|
| Outcomes | Treatment failure, mortality, fever duration, direct and indirect costs | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Data of 149 episodes were complete. |
| Selective reporting (reporting bias) | Low risk | All the data were included. |
Talcott 2011.
| Methods | Randomised controlled trial | |
| Participants | 113 episodes of adults with cancer (> 19 years old), with febrile (> 38.0°C) neutropaenia (< 500 absolute neutrophil count), and with low‐risk Talcott criteria. Multicentre study | |
| Interventions | 47 participants were discharged from hospital after 24 h of observation. They received at home either a semisynthetic penicillin and aminoglycoside combination or ceftazidime alone. 66 inpatients received either a semisynthetic penicillin and aminoglycoside combination or ceftazidime alone. |
|
| Outcomes | Treatment failure, mortality, quality of life, direct and indirect costs | |
| Notes | Participants could use colony‐stimulating factors. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "random assignments were computer generated by using blocks and stratified by use of colony‐stimulating factors, participant institution..." |
| Allocation concealment (selection bias) | Low risk | Sequenced sealed envelopes were used. |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Data of 113 episodes were complete for the clinical outcome. However, economic costs were reported in 92 episodes. |
| Selective reporting (reporting bias) | Low risk | With the exception of hospital stay, all the data were included. |
IBI: invasive bacterial infection IV: Intrvenous
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Gupta 2009 | Oral versus IV empirical antimicrobial treatment in outpatients only |
| Kern 2013 | Oral versus oral empirical antimicrobial treatment in outpatients only |
| Klaassen 2000 | Oral empirical antimicrobial treatment versus placebo in outpatients only |
| Minotti 1999 | Oral versus IV empirical antimicrobial treatment in outpatients only |
| Mullen 1999 | Oral versus IV empirical antimicrobial treatment in outpatients only |
| Paganini 2001 | Oral versus IV empirical antimicrobial treatment in outpatients only |
| Paganini 2003 | Oral versus IV empirical antimicrobial treatment in outpatients only |
| Petrilli 2000 | Oral versus IV empirical antimicrobial treatment in outpatients only |
| Rubenstein 1993 | Oral versus IV empirical antimicrobial treatment in outpatients only |
IV: Intravenous
Differences between protocol and review
There was virtually no difference between the protocol and the present review. Although we did not have the means to conduct searches on Heathstar, there is very little chance that there would be more RCTs since, for the searches, we used the largest databases of published articles. We did not contact the authors because we considered that the study reports were clear enough for the purposes of this review.
Contributions of authors
RRR conceived the study, participated in the design of the study, performed the statistical analysis, and helped to draft the manuscript. MVK conceived the study, participated in the design of the study, performed the statistical analysis, and helped to draft the manuscript. MGMN participated in the design of the study, and helped to draft the manuscript. DOCM participated in the study selection, data extraction, and statistical analysis. SRC participated in the study selection and data extraction. All authors read and approved the final manuscript.
Sources of support
Internal sources
None, Other.
External sources
None, Other.
Declarations of interest
RRR: Has worked for Abbott as speaker and consultant in Biostatistics, and works full time for Instituto Mexicano del Seguro Social, which is a government institution. MVK: none known MGMN: none known DOCM: none known SRC: none known
Edited (no change to conclusions)
References
References to studies included in this review
Ahmed 2007 {published data only}
- Ahmed N, El‐Mahallawy HA, Ahmed IA, Nassif S, El‐Beshlawy A, El‐Haddad A. Early hospital discharge versus continued hospitalization in febrile pediatric cancer patients with prolonged neutropenia: a randomized, prospective study. Pediatric Blood & Cancer 2007;49(6):786‐92. [DOI] [PubMed] [Google Scholar]
Brack 2012 {published data only}
- Brack E, Bodner N, Simon A, Liebundgut K, Kühne T, Niggli FK, et al. First‐day step‐down to oral outpatient treatment versus continued standard treatment in children with cancer and low‐risk fever in neutropenia. A randomized controlled trial within the multicenter SPOG 2003 FN Study. Pediatric Blood & Cancer 2012;59(3):423‐30. [DOI] [PubMed] [Google Scholar]
Hidalgo 1999 {published data only}
- Hidalgo M, Hornedo J, Lumbreras C, Trigo JM, Colomer R, Perea S, et al. Outpatient therapy with oral ofloxacin for patients with low risk neutropenia and fever. A prospective, randomized clinical trial. Cancer 1999;85(1):213‐9. [PubMed] [Google Scholar]
Innes 2003 {published data only}
- Innes HE, Smith DB, O'Reilly SM, Clark PI, Kelly V, Marshall E. Oral antibiotics with early hospital discharge compared with in‐patient intravenous antibiotics for low‐risk febrile neutropenia in patients with cancer: a prospective randomised controlled single centre study. British Journal of Cancer 2003;89(1):43‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
López‐Hernández 2010 {published data only}
- López‐Hernández MA, Herrera‐Álvarez W, Sibaja‐Nieto L, Álvarez‐Vera JL. Low‐risk febrile neutropenia in patients with acute lymphoblastic leukemia. Amikacin‐ceftriaxone or oral fluoroquinolones [Neutropenia febril de bajo riesgo en pacientes con leucemia aguda linfoblástica. Amikacina‐ceftriaxona o fluoroquinolonas orales.]. Medicina Interna de México 2010;26(3):219‐25. [Google Scholar]
Malik 1995 {published data only}
- Malik IA, Khan WA, Karim M, Aziz A. Feasibility of outpatient management of fever in cancer patients with low‐risk neutropenia: results of prospective randomized trial. American Journal of Medicine 1995;98(3):224‐31. [DOI] [PubMed] [Google Scholar]
Orme 2014 {published data only}
- Orme LM, Babl FE, Barnes C, Barnett P, Donath S, Ashley DM. Outpatient versus inpatient IV antibiotic management for pediatric oncology patients with low risk febrile neutropenia: a randomized trial. Pediatric Blood & Cancer 2014;61(8):1427‐33. [DOI] [PubMed] [Google Scholar]
Rapoport 1999 {published data only}
- Rapoport BL, Sussmann O, Herrera MV, Schlaeffer F, Otero JC, Pavlovsky S, et al. Ceftriaxone plus once daily aminoglycoside with filgrastim for treatment of febrile neutropenia: early hospital discharge vs. standard In‐patient care. Chemotherapy 1999;45(6):466‐76. [DOI] [PubMed] [Google Scholar]
Santolaya 2004 {published data only}
- Santolaya ME, Álvarez AM, Avilés CL, Becker A, Cofré J, Cumsille MA, et al. Early hospital discharge followed by outpatient management versus continued hospitalization of children with cancer, fever, and neutropenia at low risk for invasive bacterial infection. Journal of Clinical Oncology 2004;22(18):3784‐9. [DOI] [PubMed] [Google Scholar]
Talcott 2011 {published data only}
- Hendricks AM, Loggers ET, Talcott JA. Costs of home versus inpatient treatment for fever and neutropenia: analysis of a multicenter randomized trial. Journal of Clinical Oncology 2011;29(30):3984‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Talcott JA, Yeap BY, Clark JA, Siegel RD, Loggers ET, Lu C, et al. Safety of early discharge for low‐risk patients with febrile neutropenia: a multicenter randomized controlled trial. Journal of Clinical Oncology 2011;29(30):3977‐83. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies excluded from this review
Gupta 2009 {published data only}
- Gupta A, Swaroop C, Agarwala S, Pandey RM, Bakhshi S. Randomized controlled trial comparing oral amoxicillin‐clavulanate and ofloxacin with intravenous ceftriaxone and amikacin as outpatient therapy in pediatric low‐risk febrile neutropenia. Journal of Pediatric Hematology/Oncology 2009;31(9):635‐41. [DOI] [PubMed] [Google Scholar]
Kern 2013 {published data only}
- Kern WV, Marchetti O, Drgona L, Akan H, Aoun M, Akova M, et al. Oral antibiotics for fever in low‐risk neutropenic patients with cancer: a double‐blind, randomized, multicenter trial comparing single daily moxifloxacin with twice daily ciprofloxacin plus amoxicillin/clavulanic acid combination therapy ‐ EORTC infectious diseases group trial XV. Journal of Clinical Oncology 2013;31(9):1149‐56. [DOI] [PubMed] [Google Scholar]
Klaassen 2000 {published data only}
- Klaassen RJ, Goodman R, Pham BA, Doyle JJ. "Low‐risk" prediction rule for pediatric oncology patients presenting with fever and neutropenia. Journal of Clinical Oncology 2000;18(5):1012‐9. [DOI] [PubMed] [Google Scholar]
Minotti 1999 {published data only}
- Minotti V, Gentile G, Bucaneve G, Iori AP, Micozzi A, Cavicchi F, et al. Domiciliary treatment of febrile episodes in cancer patients: a prospective randomized trial comparing oral versus parenteral empirical antibiotic treatment. Supportive Care in Cancer 1999;7(3):134‐9. [DOI] [PubMed] [Google Scholar]
Mullen 1999 {published data only}
- Mullen CA, Petropoulos D, Roberts WM, Rytting M, Zipf T, Chan KW, et al. Outpatient treatment of fever and neutropenia for low risk pediatric cancer patients. Cancer 1999;86(1):126‐34. [PubMed] [Google Scholar]
Paganini 2001 {published data only}
- Paganini H, Rodriguez‐Brieshcke T, Zubizarreta P, Latella A, Firpo V, Casimir L, et al. Oral ciprofloxacin in the management of children with cancer with lower risk febrile neutropenia. Cancer 2001;91(8):1563‐7. [DOI] [PubMed] [Google Scholar]
Paganini 2003 {published data only}
- Paganini H, Gómez S, Ruvinsky S, Zubizarreta P, Latella A, Fraquelli L, et al. Outpatient, sequential, parenteral‐oral antibiotic therapy for lower risk febrile neutropenia in children with malignant disease: a single‐center, randomized, controlled trial in Argentina. Cancer 2003;97(7):1775‐80. [DOI] [PubMed] [Google Scholar]
Petrilli 2000 {published data only}
- Petrilli AS, Dantas LS, Campos MC, Tanaka C, Ginani VC, Seber A. Oral ciprofloxacin vs. intravenous ceftriaxone administered in an outpatient setting for fever and neutropenia in low‐risk pediatric oncology patients: randomized prospective trial. Medical and Pediatric Oncology 2000;34(2):87‐91. [DOI] [PubMed] [Google Scholar]
Rubenstein 1993 {published data only}
- Rubenstein EB, Rolston K, Benjamin RS, Loewy J, Escalante C, Manzullo E, et al. Outpatient treatment of febrile episodes in low‐risk neutropenic patients with cancer. Cancer 1993;71(11):3640‐6. [DOI] [PubMed] [Google Scholar]
Additional references
Alexander 2002
- Alexander SW, Wade KC, Hibberd PL, Parsons SK. Evaluation of risk prediction criteria for episodes of febrile neutropenia in children with cancer. Journal of Pediatric Hematology/Oncology 2002;24(1):38‐42. [DOI] [PubMed] [Google Scholar]
Ammann 2003
- Ammann RA, Hirt A, Lüthy AR, Aebi C. Identification of children presenting with fever in chemotherapy‐induced neutropenia at low risk for severe bacterial infection. Medical and Pediatric Oncology 2003;41(5):436‐43. [DOI] [PubMed] [Google Scholar]
Bodey 1966
- Bodey GP, Buckley M, Sathe YS, Freireich EJ. Quantitative relationships between circulating leukocytes and infection in patients with acute leukemia. Annals of Internal Medicine 1966;64(2):328‐40. [DOI] [PubMed] [Google Scholar]
Buchanan 1993
- Buchanan GR. Approach to treatment of the febrile cancer patient with low‐risk neutropenia. Hematology/Oncology Clinics of North America 1993;7(5):919‐35. [PubMed] [Google Scholar]
Carstensen 2008
- Carstensen M, Sorensen JB. Outpatient management of febrile neutropenia: time to revise the present treatment strategy. Journal of Supportive Oncology 2008;6(5):199‐208. [PubMed] [Google Scholar]
Chamilos 2005
- Chamilos G, Bamias A, Efstathiou E, Zorzou PM, Kastritis E, Kostis E, et al. Outpatient treatment of low‐risk neutropenic fever in cancer patients using oral moxifloxacin. Cancer 2005;103(12):2629‐35. [DOI] [PubMed] [Google Scholar]
Cherif 2004
- Cherif H, Bjorkholm M, Engervall P, Johansson P, Ljungman P, Hast R, et al. A prospective, randomized study comparing cefepime and imipenem‐cilastatin in the empirical treatment of febrile neutropenia in patients treated for haematological malignancies. Scandinavian Journal of Infectious Diseases 2004;36(8):593‐600. [DOI] [PubMed] [Google Scholar]
Cherif 2006
- Cherif H, Johansson E, Bjorkholm M, Kalin M. The feasibility of early hospital discharge with oral antimicrobial therapy in low risk patients with febrile neutropenia following chemotherapy for hematologic malignancies. Haematologica 2006;91(2):215‐22. [PubMed] [Google Scholar]
Close 1995
- Close P, Burkey F, Kasak A, Danz P, Lange B. A prospective, controlled evaluation of home chemotherapy for children with cancer. Pediatrics 1995;95(6):896‐900. [PubMed] [Google Scholar]
Consensus panel 1990
- Consensus panel, Immunocompromised Host Society. The design, analysis,and reporting of clinical trials on the empirical antibiotic management of the neutropenic patient. Report of a consensus panel. Journal of Infectious Diseases 1990;161(3):397‐401. [DOI] [PubMed] [Google Scholar]
Deeks 2001
- Deeks JJ, Altman DJ, Bradburn MJ. Statistical methods for examining heterogeneity and combining results from several studies in meta‐analysis. In: Egger M, Davey Smith G, Altman DG editor(s). Systematic Reviews in Health Care; Meta‐Analysis in Context. 2nd Edition. London: BMJ Publication Group, 2001. [Google Scholar]
Delebarre 2014
- Delebarre M, Macher E, Mazingue F, Martinot A, Dubos F. Which decision rules meet methodological standards in children with febrile neutropenia? Results of a systematic review and analysis.. Pediatric Blood & Cancer 2014;61(10):1786‐91. [DOI] [PubMed] [Google Scholar]
Elting 1997
- Elting LS, Rubenstein EB, Rolston KV, Bodey GP. Outcome of bacteremia in patients with cancer and neutropenia: observations from two decades of epidemiological and clinical trials. Clinical Infectious Diseases 1997;25(2):247‐59. [DOI] [PubMed] [Google Scholar]
Elting 2008
- Elting LS, Lu C, Escalante CP, Giordano SH, Trent JC, Cooksley C, et al. Outcomes and cost of outpatient or inpatient management of 712 patients with febrile neutropenia. Journal of Clinical Oncology 2008;26(4):606‐11. [DOI] [PubMed] [Google Scholar]
Feld 1998
- Feld R. Criteria for response in patients in clinical trials of empiric antibiotic regimens for febrile neutropenia. Is there agreement?. Supportive Care in Cancer 1998;6(5):444‐8. [DOI] [PubMed] [Google Scholar]
Feld 2002
- Feld R, Paesmans M, Freifeld AG, Klastersky J, Pizzo PA, Rolston KV, et al. Methodology for clinical trials involving patients with cancer who have febrile neutropenia: updated guidelines of the Immunocompromised Host Society/Multinational Association for Supportive Care in Cancer, with emphasis on outpatient studies. Clinical of Infectious Diseases 2002;35(12):1463‐8. [DOI] [PubMed] [Google Scholar]
Freifeld 1999
- Freifeld A, Marchigiani D, Walsh T. A double‐blind comparison of empirical oral and intravenous antibiotic therapy for low‐risk febrile patients with neutropenia during cancer chemotherapy. New England Journal of Medicine 1999;341(5):305‐11. [DOI] [PubMed] [Google Scholar]
Heinz 2017
- Heinz WJ, Buchheidt D, Christopeit M, Lilienfeld‐Toal M, Cornely OA, Einsele H, et al. Diagnosis and empirical treatment of fever of unknown origin (FUO) in adult neutropenic patients: guidelines of the Infectious Diseases Working Party (AGIHO) of the German Society of Hematology and Medical Oncology (DGHO). Annals of Hematology 2017;11:1775‐92. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2003
- Higgins JP, Thomson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. British Medical Journal 2003;327(7414):557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org/.
Hughes 1997
- Hughes WT, Armstrong D, Bodey GP, Brown A, Edwards J, Feld R, et al. Infectious Diseases Society of America. 1997 guidelines for the use of antimicrobial agents in neutropenic patients with unexplained fever. Clinical Infectious Diseases 1997;25(3):551‐73. [DOI] [PubMed] [Google Scholar]
Hughes 2002
- Hughes WT, Armstrong D, Bodey GP, Bow EJ, Brown AE, Calandra T, et al. 2002 guidelines for the use of antimicrobial agents in neutropenic patients with cancer. Clinical Infectious Diseases 2002;34:730‐51. [DOI] [PubMed] [Google Scholar]
IDSA 2010
- Freifeld AG, Bow EJ, Sepkowitz KA, Boeckh MJ, Ito JI, Mullen CA, et al. Infectious Diseases Society of America. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update. Clinical Infectious Diseases 2011;52(4):427‐31. [DOI] [PubMed] [Google Scholar]
IDSA 2018
- Taplitz RA, Kennedy EB, Bow EJ, Crews J, Gleason C, Hawley DK, et al. Outpatient management of fever and neutropenia in adults treated for malignancy: American Society of Clinical Oncology and Infectious Diseases Society of America Clinical Practice Guideline update. Journal of Clinical Oncology 2018;36(14):1443‐53. [DOI] [PubMed] [Google Scholar]
Kamana 2005
- Kamana M, Escalante C, Mullen CA, Frisbee‐Hume S, Rolston K. Bacterial infections in low‐risk febrile neutropenic patients. Cancer 2005;104(2):422‐26. [DOI] [PubMed] [Google Scholar]
Karthaus 1998
- Karthaus M, Egerer G, Kullmann KH, Ritter J, Jürgens H. Ceftriaxone in the outpatient treatment of cancer patients with fever and neutropenia. European Journal of Clinical Microbiology & Infectious Diseases 1998;17(7):501‐4. [DOI] [PubMed] [Google Scholar]
Kern 1999
- Kern WV, Cometta A, Bock R, Langenaeken J, Paesmans M, Gaya H. Oral versus intravenous empirical antimicrobial therapy for fever in patients with granulocytopenia who are receiving cancer chemotherapy. New England Journal of Medicine 1999;341(5):312‐18. [DOI] [PubMed] [Google Scholar]
Klaassen 2000a
- Klaassen RJ, Allen U, Doyle J. Randomized placebo‐controlled trial of oral antibiotics in pediatric oncology patients at low risk with fever and neutropenia. Journal of Pediatric Hematology/Oncology 2000;22(5):405‐11. [DOI] [PubMed] [Google Scholar]
Klastersky 2000
- Klastersky J, Paesmans M, Rubenstein EB, Boyer M, Elting L, Feld R, et al. The multinational association for supportive care in cancer risk index: a multinational scoring system for identifying low‐risk febrile neutropenic cancer patients . Journal of Clinical Oncology 2000;18(16):3038‐51. [DOI] [PubMed] [Google Scholar]
Klastersky 2006
- Klastersky J, Paesmans M, Georgala A, Muanza F, Plehiers B, Dubreucq L, et al. Outpatient oral antibiotics for febrile neutropenic cancer patients using a score predictive for complications. Journal of Clinical Oncology 2006;24(25):4129‐34. [DOI] [PubMed] [Google Scholar]
Klastersky 2013
- Klastersky J, Paesmans M. The Multinational Association for Supportive Care in Cancer (MASCC) risk index score: 10 years of use for identifying low‐risk febrile neutropenic cancer patients. Supportive Care in Cancer 2013;21(5):1487‐95. [DOI] [PubMed] [Google Scholar]
Klastersky 2016
- Klastersky J, Naurois J, Rolston K, Rapoport B, Maschmeyer G, Aapro M, et al. Management of febrile neutropaenia: ESMO Clinical Practice Guidelines. Annals of Oncology 2016;25(Suppl 5):v111‐8. [DOI] [PubMed] [Google Scholar]
Lehrnbecher 2017
- Lehrnbecher T, Robinson P, Fisher B, Alexander S, Ammann RA, Beauchemin M, et al. Guideline for the management of fever and neutropenia in children with cancer and hematopoietic stem‐cell transplantation recipients: 2017 update. Journal of Clinical Oncology 2017;35(18):2082‐94. [DOI] [PubMed] [Google Scholar]
Loeffen 2016
- Loeffen EA, Poele EM, Tissing WJ, Boezen HM, Bont ES. Very early discharge versus early discharge versus non‐early discharge in children with cancer and febrile neutropenia. Cochrane Database of Systematic Reviews 2016, Issue 2. [DOI: 10.1002/14651858.CD008382.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Mesters 2000
- Mesters RM, Helterbrand J, Utterback BG, Yan B, Chao YB, Fernández JA, et al. Prognostic value of protein C concentrations in neutropenic patients at high risk of severe septic complications. Critical Care Medicine 2000;28(7):2209‐16. [DOI] [PubMed] [Google Scholar]
Mullen 1990
- Mullen CA, Buchanan GR. Early hospital discharge of children with cancer treated for fever and neutropenia: identification and management of the low‐risk patient. Journal of Clinical Oncology 1990;8(12):998‐1004. [DOI] [PubMed] [Google Scholar]
Mustafa 1996
- Mustafa MM, Aquino VM, Pappo A, Tkaczewski I, Buchanan GR. A pilot study of outpatient management of febrile neutropenic children with cancer at low risk of bacteremia. Journal of Pediatrics 1996;128(6):847‐9. [DOI] [PubMed] [Google Scholar]
Nijhuis 2005
- Nijhuis CO, Kamps WA, Daenen SM, Gietema JA, Graaf WT, Groen HJ, et al. Feasibility of withholding antibiotics in selected febrile neutropenic cancer patients. Journal of Clinical Oncology 2005;23(30):7437‐44. [DOI] [PubMed] [Google Scholar]
Orudjev 2002
- Orudjev E, Lange BJ. Evolving concepts of management of febrile neutropenia in children with cancer. Medical and Pediatric Oncology 2002;39(2):77‐85. [DOI] [PubMed] [Google Scholar]
Quezada 2007
- Quezada G, Sunderland T, Chan KW, Rolston K, Mullen CA. Medical and non‐medical barriers to outpatient treatment of fever and neutropenia in children with cancer. Pediatric Blood & Cancer 2007;48(3):273‐7. [DOI] [PubMed] [Google Scholar]
Review Manager 2014 [Computer program]
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Santolaya 2002
- Santolaya ME, Alvarez AM, Aviles CL, Becker A, Cofre J, Enriquez N, et al. Prospective evaluation of a model of prediction of invasive bacterial infection risk among children with cancer, fever, and neutropenia. Clinical Infectious Diseases 2002;35(6):678‐83. [DOI] [PubMed] [Google Scholar]
Santolaya 2010
- Santolaya ME. Supportive care in children. Current Opinion in Oncology 2010;22(4):323‐9. [DOI] [PubMed] [Google Scholar]
Schünemann 2011
- Schünemann HJ, Oxman AD, Higgins JPT, Vist GE, Glasziou P, Guyatt GH. Chapter 11: Presenting results and ‘Summary of findings' tables. In: Higgins JPT, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Sebban 2008
- Sebban C, Dussart S, Fuhrmann C, Ghesquieres H, Rodrigues I, Geoffrois L, et al. Oral moxifloxacin or intravenous ceftriaxone for the treatment of low‐risk neutropenic fever in cancer patients suitable for early hospital discharge. Supportive Care in Cancer 2008;16(9):1017‐23. [DOI] [PubMed] [Google Scholar]
Soker 2001
- Soker M, Colpan L, Ece A, Deveciolu C, Haspolat K. Serum levels of IL‐1 beta, sIL‐2R, IL‐6, IL‐8, and TNF‐alpha in febrile children with cancer and neutropenia. Medical Oncology 2001;18(1):51‐7. [DOI] [PubMed] [Google Scholar]
Sung 2004
- Sung L, Feldman BM, Schwamborn G, Paczesny D, Cochrane A, Greenberg ML, et al. Inpatient versus outpatient management of low‐risk pediatric febrile neutropenia: measuring parents' and healthcare professionals' preferences. Journal of Clinical Oncology 2004;22(19):3922‐9. [DOI] [PubMed] [Google Scholar]
Talcott 1988
- Talcott JA, Finberg R, Mayer RJ, Goldman L. The medical course of cancer patients with fever and neutropenia. Clinical identification of a low‐risk subgroup at presentation. Archives of Internal Medicine 1988;148(12):2561‐8. [PubMed] [Google Scholar]
Talcott 1992
- Talcott JA, Siegel RD, Finberg R, Goldman L. Risk assessment in cancer patients with fever and neutropenia: a prospective, two‐center validation of a prediction rule. Journal of Clinical Oncology 1992;10(2):316‐22. [DOI] [PubMed] [Google Scholar]
Teuffel 2011
- Teuffel O, Ethier MC, Alibhai SM, Beyene J, Sung L. Outpatient management of cancer patients with febrile neutropenia: a systematic review and meta‐analysis. Annals of Oncology 2011;22(11):2358‐65. [DOI] [PubMed] [Google Scholar]
Vidal 2013
- Vidal L, Paul M, Ben‐Dor I, Pokroy E, Soares‐Weiser K, Leibovici L. Oral versus intravenous antibiotic treatment for febrile neutropenia in cancer patients. Cochrane Database of Systematic Reviews 2013, Issue 10. [DOI: 10.1002/14651858.CD003992.pub3] [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Rivas‐Ruiz 2011
- Rivas‐Ruiz R, Villasis‐Keever M, Miranda‐Novales MG. Outpatient treatment for patients with cancer who develop a low‐risk febrile neutropenic event. Cochrane Database of Systematic Reviews 2011, Issue 3. [DOI: 10.1002/14651858.CD009031] [DOI] [PMC free article] [PubMed] [Google Scholar]