

Abstract
Objective:
Prior research has documented the influence of social norms on health-related behaviors, though social norms may affect behaviors in more complex ways than have conventionally been modeled. The present research evaluates parent norms and teens’ own attitudes as moderators of associations between perceived peer norms and diet and physical activity behaviors (both health-promoting and health-impairing) in a national sample of U.S. adolescents.
Methods:
Adolescent participants (N = 1,859; ages 12–17) from the 2014 Family Life, Activity, Sun, Health, and Eating (FLASHE) study reported on the extent to which their friends eat fruits and vegetables; eat junk food or drink sugary drinks; exercise; and watch TV, play on the computer, or play electronic games most days of the week. They also reported on their own attitudes and behaviors as well as their parents’ corresponding behaviors and rules.
Results:
Perceived peer norms were associated with teens’ own health-promoting behaviors such as fruit and vegetable consumption and physical activity as well as health-impairing behaviors such as junk food consumption and sedentary habits. Teens who reported liking fruits and vegetables or physical activity or perceiving congruent descriptive parental norms demonstrated the strongest positive associations between peer norms and their own behavior.
Conclusions:
Perceived social norms may play a significant role in both health-impairing and health-promoting behaviors, particularly when congruent with attitudes or descriptive parental norms about those behaviors. The findings may inform interventions such as social norms marketing campaigns that aim to change perceptions of peer norms for health-promoting behavior.
Keywords: health behavior, social norms, adolescent behavior, physical activity, diet
Social norms exert profound influences on human behavior and experience across the lifespan. Many prominent theories of health behavior acknowledge the impact of social comparisons and perceived social norms, with supportive evidence in a wide variety of domains (e.g., Klein & Rice, in press; Miller & Prentice, 2016) and meta-analyses suggesting modest but reliable effect sizes (d = .41 in correlational studies; Conner & Sparks, 2015; d = .36 in experimental studies; c.f., attitudes d = .38, self-efficacy d = .47; Sheeran et al., 2016). Recent reviews attest to the propensity for peer norms to shape physical activity and dietary behavior during adolescence in particular (McClain, Chappuis, Nguyen-Rodriguez, Yaroch, & Spuijt-Metz, 2009; Salvy, De La Haye, Bowker, & Hermans, 2012; Sawka, McCormack, Nettel-Aguirre, Hawe, & Doyle-Baker, 2013; Stok, de Vet, de Ridder, & de Wit, 2016) with important implications for health. Beyond the more proximal health outcomes associated with patterns of diet, physical activity, and sedentary behavior in adolescence (e.g., obesity, type 2 diabetes), dietary and activity-related habits established during this period may extend into subsequent stages of the life course (Kelder, Perry, Klepp, & Lytle, 1994; Janz, Dawson, & Mahoney, 1999; Larson, Neumark-Sztainer, Hannan, & Story, 2007; Merten, Williams, & Shriver, 2009). This potentially enduring influence of adolescent behaviors on health outcomes underscores the importance of understanding determinants of those behaviors, and thus, opportunities to improve them.
Though the influence of social norms on adolescent health-related behaviors may be best documented in the domains of risky behaviors such as alcohol consumption and tobacco use (Cooke, Dahdah, Norman, & French, 2016), prior research has demonstrated that social norms predict dietary and activity-related behaviors as well (Baker, Little, & Brownell, 2003). Subsequent studies have further clarified processes by which both peer and parental norms may influence adolescent behavior by distinguishing between descriptive norms (i.e., how other people actually behave) and injunctive norms (i.e., what other people approve of) and by more precisely assessing more specific forms of behavior. For instance, one study of adolescents in the United Kingdom revealed robust associations between descriptive norms and teens’ own dietary behaviors (i.e., consumption of fruits and vegetables, sugar-sweetened beverages, and unhealthy snacks), yet no association between injunctive norms and teens’ own dietary behaviors (Lally, Bartle, & Wardle, 2011). The same research also suggested that teens overestimated their peers’ consumption of snacks and sugar-sweetened beverages while underestimating their consumption of fruits and vegetables.
Personal attitudes toward health-related behaviors are often considered in tandem with social norms. In fact, research on alcohol consumption among young adults suggests that attitudes may exert an even stronger influence on drinking behavior than peer norms (DiBello, Miller, Neighbors, Reid, & Carey, 2018). Although much prior research has modeled the joint influence of peer norms, parent norms, and personal attitudes on adolescent behavior as suggested by the Theory of Planned Behavior (Ajzen, 1985), these constructs likely unfold and interact in more complex ways than are conventionally modeled. For example, bidirectional and cyclical processes likely abound as in the case of peer norms and physical activity behavior: adolescents seem to befriend peers who engage in comparable levels of physical activity, and they in turn emulate their friends’ activity patterns (De La Haye, Robins, Mohr, & Wilson, 2011). Providing further evidence of interrelations among norms and attitudes, another study demonstrated that attitudes mediate the influence of injunctive norms on behavior, whereas descriptive norms are directly related to behaviors (Reid et al., 2018), and further, that normative information is particularly influential in the absence of strong attitudes.
The present research builds on previous work by evaluating the relative importance of perceived norms regarding peers (operationalized here as friends) and parents in adolescent behavior among a large sample of U.S. teenagers, considering both health-promoting and health-impairing behaviors in the domains of diet and physical activity. Hypothesis 1 was that perceived peer norms would be strongly associated with adolescent behavior in the contexts of fruit and vegetable consumption and physical activity as well as junk food consumption and sedentary behavior. Hypothesis 2 was that perceived parental norms – both descriptive (i.e., how respondents think their parents behave) and injunctive (i.e., what respondents think their parents approve of) – would be associated with adolescent behaviors as well, though to a lesser extent than peer norms. This pattern has been documented consistently in other studies, even in the domain of diet and physical activity (e.g., Baker et al., 2003), though not with distinctions between types of norms and health-promoting as well as health-impairing forms of behavior.
A more primary aim of the present research was to qualify associations between social norms and teen behaviors by testing moderation effects, acknowledging potentially competing or congruent influences from peers and parents and the potential importance of teens’ own attitudes. Prior research has established that peers and parents are both compelling sources of social influence on adolescent health behaviors (e.g., McClain et al., 2009), but modeling interactions between them allows for greater clarity in understanding their simultaneous influence. When norms are congruent, it is conceivable that peer and parent norms may have substitutable, additive, or synergistic associations with peer behavior; data from a large sample are necessary to test such patterns. Likewise, personal attitudes about specific behaviors may moderate the association between peer norms and the focal behavior. Although peer norms likely shape attitudes about various behaviors (Cialdini, 2003; Reid & Aiken, 2013; Reid et al., 2018), attitudes may also operate as a psychological filter through which norms are perceived. Consequently, personal attitudes could amplify the effects of congruent social norms and attenuate the influence of incongruent social norms. The present research uses psychosocial and behavioral data from a national sample of adolescents to address the potentially interacting forces that shape both health-promoting and health-impairing forms of dietary and activity-related behavior.
Methods
Data were drawn from the Family Life, Activity, Sun, Health, and Eating (FLASHE) study, a publicly available cross-sectional internet-based national survey of U.S. adolescents and a parent/caregiver administered in 2014 with an overall response rate of 29.4% (N = 1,479 dyads who completed all sections of the questionnaire). The present study used all available adolescent data, resulting in a study sample of N = 1,859. The FLASHE study was approved by the Westat, Inc. and National Cancer Institute Special Studies Institutional Review Boards. Further details about FLASHE development and methodology are available elsewhere (Nebeling et al., 2017; Oh et al., 2017).
Measures
Participants completed psychosocial and behavioral measures corresponding to fruit and vegetable consumption, junk-food consumption, physical activity, and sedentary behavior. Peer norms for these behaviors were assessed by prompting adolescent participants to indicate their agreement with statements (one item per behavior) such as “My friends eat fruits and vegetables [eat junk food or drink sugary drinks; exercise; watch TV, play on the computer, or play electronic games] most days of the week,” using a response scale ranging from 1 (strongly disagree) to 5 (strongly agree).
Parental descriptive norms were assessed by prompting adolescent participants to indicate their agreement with statements (one item per behavior) such as “My parent(s) try to eat fruits and vegetables [avoid eating junk food or drinking sugary drinks; be physically active; limit their screen time] when I’m around,” using a response scale ranging from 1 (strongly disagree) to 5 (strongly agree).
Parental injunctive norms were assessed using a series of three items corresponding to each behavior. Item wording varied somewhat across behaviors, but representative prompts included: “My parent(s) have to make sure that I eat enough fruits and vegetables,” “My parent(s) decide how much junk food or sugary drinks I can have,” and “It’s okay for my parent(s) to make rules about how much time I spend being physically active/playing.” Response scales ranged from 1 (strongly disagree) to 5 (strongly agree). The items in each domain demonstrated adequate internal consistency (α = .70 – .79).
Several items assessed teen preferences or attitudes pertaining to fruit and vegetables consumption (“fruit like apples, bananas, melon, etc., counting fresh, frozen, canned, or dried fruit;” “a green salad, or other non-fried vegetables like carrots, broccoli, green beans, corn, etc.”) and junk-food consumption (“sugar-sweetened drinks like Capri Sun, Sunny D, Arizona Tea, etc.;” “regular soda or pop like Coke, Pepsi, Sprite, Dr. Pepper, etc.”), using response scales ranging from 1 (strongly dislike) to 5 (strongly like). To match the behavioral scope of other measures, these were aggregated within domains to produce one composite (mean; α = .67) measure of preferences for fruits and vegetables and one composite (mean; α = .57) measure of preferences for sugar-sweetened beverages. A separate item assessed agreement with the prompt, “If I were to be physically active most days of the week it would be fun,” using a response scale from 1 (strongly disagree) to 5 (strongly agree). No comparable measures assessed attitudes toward sedentary behavior.
Derived variables pertaining to behavior were included in the dataset. Of these, estimated cups of fruits and vegetables consumed per day and frequency of junk-food and sugar-sweetened beverage consumption were calculated from responses to items adapted from the Dietary Screener Questionnaire (National Cancer Institute) and the National Youth Physical Activity and Nutrition Survey (Centers for Disease Control and Prevention). Minutes of weekly physical activity (both in and out of school) and sedentary behavior (outside of school only) during a typical week were calculated from responses to the Youth Activity Profile (Saint-Maurice & Welk, 2014) and calibrated with temporally matched wrist-actigraphy data obtained from a subsample of participants (Saint-Maurice et al., 2017). More information about behavioral variables is available at the FLASHE website (http://cancercontrol.cancer.gov/brp/hbrb/flashe.html) and in print (Saint-Maurice et al., 2017; Smith et al., 2017).
In addition to psychosocial and behavioral measures, respondents provided sociodemographic information, including age, gender, race, and household income (reported by parents and recoded into a binary variable indicating annual income above or below $100,000).
Analytic Strategy
SAS 9.3 was used for all analyses. Data on social norms (including peer norms, parental descriptive norms, and parental injunctive norms) and sociodemographic characteristics (age, gender, race, and household income status) were submitted to four separate linear regression analyses corresponding with the four behavioral domains assessed: fruit and vegetable consumption, junk-food consumption, physical activity, and sedentary behavior. A second set of models sought to evaluate interactions among these potential sources of social influence by testing whether associations between peer norms and teen behavior were moderated by parental norms or teen attitudes toward the behavior, though attitudes were not measured in the domain of sedentary behavior. Although the testing and interpretation of interaction effects conventionally supersedes underlying main effects, the present strategy involved first constructing simple models as a baseline test of the relative strength of associations in each domain and then adding further complexity by introducing interaction terms for the distinct purpose of more comprehensively modeling how these factors likely unfold in lived experience. These overarching moderation effects should be given priority in interpreting the results. All models controlled for age, gender, race, and household income. All available data were analyzed (with listwise deletion), but the pattern of results did not change in subsequent analyses using a subsample of participants with complete cases (n = 1,109).
Results
Descriptive Statistics
The average age among adolescent respondents was 14.47 (SD = 1.61; range = 12–17), and 50.24% of respondents identified as female. Respondents primarily identified as non-Hispanic White (63.69%); 10.08% of respondents identified as Hispanic, 16.99% identified as non-Hispanic Black, and 9.24% identified as members of another racial or ethnic group. Adolescents in households with an annual income below $100,000 represented 79.35% of the sample. Although the FLASHE study involved a nationwide sample and screened a sample of panelists balanced to population demographics of the U.S., the survey methodology prioritized enrolling complete parent-adolescent dyads that would be similar to the U.S. population over obtaining a representative final sample. As such, characteristics of study dyads were skewed in patterns consistent with other panel or web surveys (e.g., higher rates of participants identifying as non-Hispanic White and endorsing high levels of socioeconomic status; Oh et al., 2017). See Table 1 for distributions of sociodemographic variables and health-related behaviors (described at length elsewhere; Nebeling et al., 2017).
Table 1.
Distribution of respondent sociodemographic characteristics and health-related behaviors from the FLASHE survey, 2014, N = 1,859
| n | % | |
|---|---|---|
| Age (years) | ||
| 12 | 224 | 13.32 |
| 13 | 336 | 19.98 |
| 14 | 280 | 16.65 |
| 15 | 305 | 18.13 |
| 16 | 331 | 19.68 |
| 17 | 206 | 12.25 |
| Missing | 177 | |
| Sex | ||
| Female | 843 | 50.24 |
| Male | 835 | 49.76 |
| Missing | 181 | |
| Race/Ethnicity | ||
| Hispanic or Latino/a | 168 | 10.08 |
| Non-Hispanic Black | 283 | 16.99 |
| Non-Hispanic White | 1061 | 63.69 |
| Non-Hispanic Other | 154 | 9.24 |
| Missing | 193 | |
| Household Income Status | ||
| Below $100,000 | 1406 | 79.35 |
| $100,000 or greater | 366 | 20.65 |
| Missing | 87 | |
| Fruit and Vegetable Consumption | ||
| 0 to < 3 cups per day | 1280 | 83.28 |
| 3 to < 5 cups per day | 228 | 14.83 |
| 5 or more cups per day | 29 | 1.89 |
| Missing | 322 | |
| Junk Food and Sugar-Sweetened Beverages | ||
| 0 to < 3 times per day | 862 | 57.43 |
| 3 to < 5 times per day | 424 | 28.25 |
| 5 or more times per day | 215 | 14.32 |
| Missing | 358 | |
| Physical Activity (calibrated) | ||
| 0 to 599 min/week | 161 | 11.20 |
| 600 to 749 min/week | 427 | 29.71 |
| 750 or more min/week | 849 | 59.08 |
| Missing | 422 | |
| Sedentary Behavior (out of school, calibrated) | ||
| 0 to 1319 min/week | 104 | 7.17 |
| 1320 to 1439 min/week | 1078 | 74.34 |
| 1440 or more min/week | 268 | 18.48 |
| Missing | 409 | |
Note: Health-related behaviors are categorized here to illustrate general distributions of responses, though they were analyzed as continuous variables. The measure of physical activity analyzed in the present research represents scores derived from the Youth Activity Profile that were further calibrated based on actigraphy data collected from a subset of participants. As described elsewhere, these estimates are specific to the assumptions adopted in the calibration process and should not be considered relative to absolute guidelines for weekly physical activity (Saint-Maurice et al., 2017; Welk et al., 2017).
Inspection of the distributions of responses to the four items pertaining to peer norms revealed negative skewness in all four behavioral domains. Modal responses regarding unhealthy behaviors (i.e., peer consumption of junk food and sugar-sweetened beverages, peer use of electronic devices) tended to be near the endpoints of the scale (e.g., “somewhat agree” and “strongly agree” that “my friends eat junk food or drink sugary drinks most days of the week”), whereas modal responses regarding healthy behaviors (e.g., peer consumption of fruits and vegetables, peer physical activity) tended to fall near the center of the scale (i.e., “neither disagree nor agree” and “somewhat agree” that “my friends exercise most days of the week”). See Table 2 for descriptive statistics.
Table 2.
Descriptive statistics and bivariate correlations among peer norms, parent norms, and teen attitudes and behavior from the FLASHE survey, 2014, N = 1,859
| Correlation Coefficients |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Domain | Variable | Min | Max | Mean | SD | Teen Behavior |
Peer Norm |
Parent Model |
Parent Rule |
|
| Fruit and vegetable consumption (cups/day) | Teen Behavior | 0.24 | 9.47 | 2.16 | 1.05 | - | ||||
| Peer Norm | 1 | 5 | 3.35 | 1.06 | 0.26 | - | ||||
| Parent Model | 1 | 5 | 4.09 | 1.05 | 0.19 | 0.11 | - | |||
| Parent Rule | 1 | 5 | 3.44 | 1.08 | 0.21 | 0.16 | 0.45 | - | ||
| Teen Attitude | 1 | 5 | 4.11 | 0.90 | 0.30 | 0.20 | 0.16 | 0.13 | ||
| Junk food and sugar-sweetened beverages (frequency/day) | Teen Behavior | 0 | 27 | 3.23 | 2.63 | - | ||||
| Peer Norm | 1 | 5 | 4.03 | 0.93 | 0.13 | - | ||||
| Parent Model | 1 | 5 | 3.12 | 1.26 | −0.08 | −0.05 | - | |||
| Parent Rule | 1 | 5 | 3.32 | 1.02 | 0.05 | 0.06 | 0.36 | - | ||
| Teen Attitude | 1 | 5 | 3.96 | 1.00 | 0.26 | 0.12 | −0.16 | 0.08 | ||
| Physical activity (minutes/week) | Teen Behavior | 441 | 1163 | 781.80 | 138.52 | - | ||||
| Peer Norm | 1 | 5 | 3.54 | 1.18 | 0.23 | - | ||||
| Parent Model | 1 | 5 | 3.19 | 1.24 | 0.17 | 0.17 | - | |||
| Parent Rule | 1 | 5 | 3.09 | 1.01 | 0.25 | 0.13 | 0.53 | - | ||
| Teen Attitude | 1 | 5 | 4.11 | 0.93 | 0.26 | 0.33 | 0.12 | 0.11 | ||
| Sedentary behavior outside of school (minutes/week) | Teen Behavior | 1228 | 1700 | 1393 | 65.51 | - | ||||
| Peer Norm | 1 | 5 | 4.08 | 0.96 | 0.11 | - | ||||
| Parent Model | 1 | 5 | 2.59 | 1.29 | −0.04 | −0.08 | - | |||
| Parent Rule | 1 | 5 | 3.07 | 1.11 | −0.09 | 0.06 | 0.62 | - | ||
Note: Correlations that are significant at the level of p < .01 are displayed in bold text. Units specified for each domain apply only to the measure of teen behavior. Peer norms, parent modeling, parent rules, and teen attitudes were assessed using single items or aggregates of single items with 5-point response scales ranging from “strongly disagree” or “strongly dislike” to “strongly agree” or “strongly like.”
Primary Analyses
Perceived social norms were significantly associated with teen behavior across all four behaviors, controlling for sociodemographic characteristics; see Table 3 for all parameter estimates. Further, peer norms were more closely associated with each teen behavior than parental norms, including fruit and vegetable consumption (β = .23, p < .01) and physical activity (β = .17, p < .01). In both of these cases, the magnitude of the effect was over twice as large as the effects of corresponding descriptive norms for parents (βFV = .11, p < .01; βPA = .06, p < .01).
Table 3.
Regression analyses testing associations among peer norms, parent norms, and teen attitudes and behavior from the FLASHE survey, 2014, N = 1,859
| Outcome | Predictor | β | B | SE | p |
|---|---|---|---|---|---|
| Fruit and vegetable consumption (cups/day) |
Peer Norm | 0.23 | 0.23 | 0.03 | <.01 |
| Parent Norm (Descriptive) | 0.11 | 0.11 | 0.03 | <.01 | |
| Parent Norm (Injunctive) | 0.13 | 0.13 | 0.03 | <.01 | |
| Junk food and sugar-sweetened beverage consumption (frequency/day) |
Peer Norm | 0.12 | 0.34 | 0.08 | <.01 |
| Parent Norm (Descriptive) | −0.10 | −0.21 | 0.06 | <.01 | |
| Parent Norm (Injunctive) | 0.06 | 0.15 | 0.08 | .05 | |
| Physical activity (minutes/week) | Peer Norm | 0.16 | 19.34 | 1.54 | <.01 |
| Parent Norm (Descriptive) | 0.06 | 6.63 | 1.70 | <.01 | |
| Parent Norm (Injunctive) | 0.03 | 4.08 | 2.12 | .06 | |
| Sedentary behavior outside of school (minutes/week) |
Peer Norm | 0.12 | 8.57 | 1.72 | <.01 |
| Parent Norm (Descriptive) | 0.02 | 1.18 | 1.60 | .46 | |
| Parent Norm (Injunctive) | −0.06 | −3.22 | 1.88 | .09 | |
Note: All models include age, gender, race, and household income status as covariates. Parental descriptive norms in the context of junk food consumption and sedentary behavior were assessed in terms of limiting the health-impairing behavior, so higher values of that variable should align with lower values of teen behavior.
Although patterns of teen behavior were consistently aligned with descriptive norms from peers and parents in most behavioral domains, parental injunctive norms were less consistently associated with teen behavior. Notable examples include the positive association between parental injunctive norms (i.e., stricter rules or expectations) and teen junk-food consumption (β = .06, p = .05), as well as a non-significant association in the context of sedentary behavior (β = −0.06, p = .09).
Moderation analyses.
Subsequent analyses tested whether parental norms moderated the association between peer norms and teen behavior in each domain. Although the three-way interaction among peer norms, descriptive parental norms, and injunctive parental norms was not statistically significant, two-way interactions were significant for both health-promoting behaviors. In the case of fruit and vegetable consumption, injunctive parental norms moderated the association between peer norms and teen behavior (B = 0.06, SE = 0.02, p = .02). Model-implied simple slopes revealed that the association was only significant at high levels of injunctive parental norms (B = 0.30, SE = 0.13, p = .02); that is, only teens whose parents set rules about eating fruits and vegetables reported intake that aligned with that of their peers. In the domain of physical activity, the association between peer norms and teen behavior was stronger when teens perceived stronger descriptive parental norms (i.e., teens who perceived their parents were more active; B = 3.46, SE = 1.32, p = .01), whereas the association between peer norms and teen behavior was weaker when teens perceived stronger injunctive parental norms (i.e., teens whose parents set rules about physical activity; B = −5.14, SE = 1.61, p < .01). Model-implied simple slopes suggested that the association between peer norms and teen behavior was significant at all levels of parental descriptive norms, but strongest among teens who strongly agreed that their parents tried to be physically active around them (B = 37.07, SE = 6.80, p < .01). Probing parental injunctive norms as the focal moderator revealed that the positive association between peer norms and teen behavior was significant only in cases where teens perceived weak injunctive norms from their parents (B = 14.63, SE = 3.83, p < .01).
Separate analyses tested whether teen attitudes moderated associations between peer norms and teen behavior. Although the two sets of moderation analyses (peer norms x parent norms; all norms x teen attitudes) are presented separately here, supplemental analyses confirmed that the pattern of results was unchanged when all interaction terms were included in a single model. Of the three behaviors with available data, teen attitudes moderated the association between peer norms and behavior in the context of fruit and vegetable consumption (B = 0.08, SE = 0.03, p < .01) and physical activity (B = 4.18, SE = 1.45, p < .01). In both cases, model-implied simple slopes suggested that the positive association between peer norms and teen behavior was stronger when teens endorsed positive attitudes toward the behavior as well. However, in the case of fruit and vegetable consumption, even teens who reported that they did not like or dislike fruits and vegetables (i.e., those selecting the midpoint of the response scale) demonstrated a positive association between perceived peer norms and their own behavior (B = 0.10, SE = 0.04, p = .01), suggesting the potential for social influence on healthy diets as long as the foods in question were perceived to be at least unobjectionable (see Figure 1). The same pattern emerged in the case of physical activity, such that even teens who reported feeling neutral about physical activity demonstrated a significant positive association between perceived peer norms and their own behavior (B = 9.97, SE = 2.22, p < .01), see Figure 2. Teen attitudes did not moderate the association between parental norms and teen behavior in any domain, nor did they moderate the association between peer norms and teen behavior in the domain of junk-food consumption.
Figure 1. Model-implied simple slopes illustrating the association between peer norms and teen behaviors in the context of fruit and vegetable consumption at varying levels of teen attitudes.
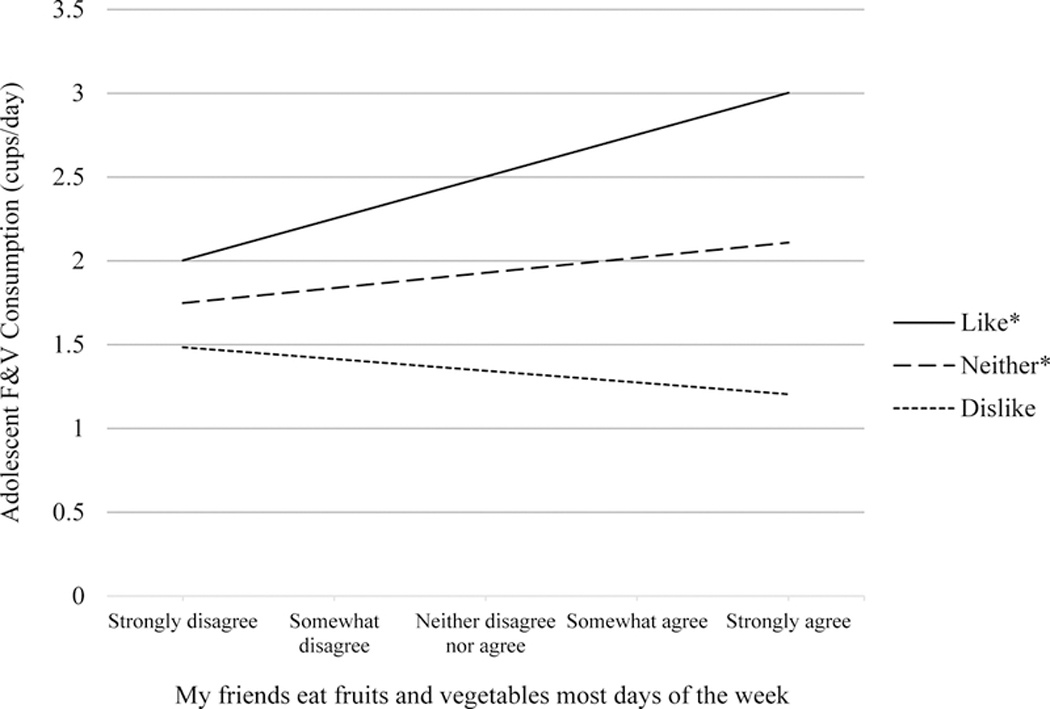
Note: Continuous variables were mean-centered in simple slope analyses. The simple slopes for participants who indicated that they strongly liked fruits and vegetables (“Like”) and participants who indicated that they neither disliked nor liked fruits and vegetables (“Neither”) were statistically significant (BLike = 0.25, p < .01; BNeither = .09, p = .02). The simple slope for participants who strongly disagreed (“Dislike”) was not statistically significant (BDislike = −0.07, p = .41).
Figure 2. Model-implied simple slopes illustrating the association between peer norms and teen behaviors in the context of physical activity at varying levels of teen attitudes.
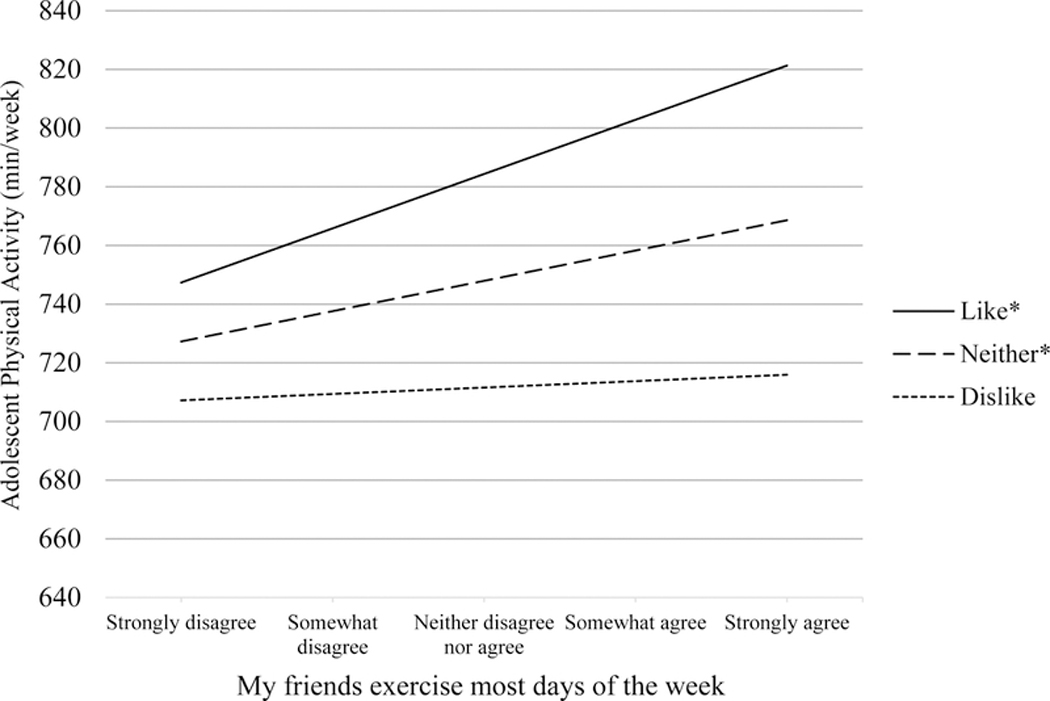
Note: Continuous variables were mean-centered in simple slope analyses. The simple slopes for participants who strongly agreed that it would be fun to be physically active most days of the week (“Like”) and participants who indicated that they neither disagreed nor agreed (“Neither”) were statistically significant (BLike = 18.49, p < .01; BNeither = 10.34, p < .01). The simple slope for participants who strongly disagreed (“Dislike”) was not statistically significant (BDislike = 2.18, p = .64).
Discussion
The present research explored the complex roles that peer and parental norms may play in adolescent diet and physical activity behaviors. Across multiple behaviors – both health-promoting and health-impairing – descriptive peer norms demonstrated stronger associations with adolescent behavior than parental descriptive norms, and parental injunctive norms were inconsistently associated with adolescent behavior. Perhaps more importantly, subsequent analyses identified moderators of the association between perceived peer norms for health-promoting behaviors and adolescent behavior. Whereas the association between peer norms and adolescent physical activity was strongest among teens who perceived that their parents were physically active, injunctive parental norms inconsistently moderated the association between peer norms and adolescent behavior across behaviors. Specifically, the association between peer norms and teen fruit and vegetable consumption was only significant among teens who perceived strong injunctive norms about fruit and vegetable consumption from their parents. However, the association between peer norms and teen physical activity was significant only among teens who perceived weak injunctive norms about physical activity from their parents. Although further research is warranted to replicate and clarify these interactions, a clearer pattern emerged in the case of teens’ attitudes. The association between peer norms and beneficial teen behaviors – eating fruits and vegetables or being physically active – was strongest among teens who reported favorable attitudes toward those behaviors, though even teens who felt mostly neutral about eating fruits and vegetables or being physically active still exhibited statistically significant alignment with perceived peer norms.
The pattern of main effects demonstrating the robust associations between peer norms and adolescent behavior is consistent with prior research (e.g., Baker et al., 2003), though the present findings are notable given the large sample and the variety of behaviors assessed. The present study most significantly expands understanding of social influence on adolescent health behaviors by identifying parental norms and adolescent attitudes as moderators of associations between peer norms and adolescent behaviors. Parental norms emerged as an inconsistent moderator of the association between perceived peer norms and teens’ own behaviors across behavioral domains, which may reflect behavior-specific processes. With little prior research to provide further context, those interaction effects may be considered preliminary findings deserving of future study, including replication attempts and investigations in other domains.
The present research also revealed that teens’ attitudes about physical activity or eating fruits and vegetables moderated associations between perceived norms and behavior. Although different varieties of social norms and personal attitudes are often considered as jointly influencing health-related behaviors (in adolescents as well as adults), they have not conventionally been modeled as interacting variables. It seemed plausible that these constructs may exert competing or additive forces on health-related behaviors (as well as bidirectional or cyclical processes that are beyond the scope of the present study), and indeed, a recent study revealed that ambivalence moderated the influence of injunctive norms on attitudes toward obtaining genetic testing results (Reid et al., 2018). In the present research, adolescents who reported favorable attitudes toward health-promoting behaviors demonstrated the strongest positive associations between perceived peer norms and their own behaviors. In fact, even teens who felt mostly neutral about eating fruits and vegetables or being physically active reported engaging in those behaviors more to the extent that they perceived the behaviors to be normative among their friends.
Although valuable given the sample size and variety of target behaviors, the current dataset is subject to several notable limitations. The FLASHE survey screened a nationally representative sample for enrollment, but recruitment and retention procedures prioritized obtaining complete data from parent-adolescent dyads over complete data from a representative sample (Oh et al., 2017). As such, the estimates and inferences reported herein may not be considered nationally representative. Compared to national patterns of sociodemographic variables, the analytic sample in the current research disproportionately identified as non-Hispanic White and reported higher levels of socioeconomic status. Comparisons on behavioral dimensions are complicated by measurement and the developmental stage of the sample; the actigraphy-calibrated measure of physical activity is not readily comparable to measures widely used in surveillance research (Welk et al., 2017), and considerations of diet and activity in adolescents (especially as related to guidelines or BMI) are necessarily tethered to age and gender.
The present research is also limited by relying on cross-sectional data with self-reported measures, precluding temporal – let alone causal – inferences. For example, the finding that stronger injunctive parental norms (i.e., stricter rules) were significantly associated with greater adolescent junk-food consumption could reflect psychological reactance if the behavior is in response to the norms, but it could just as well reflect the fact that parents set stricter rules and expectations in response to teens’ junk-food consumption. Similarly, the self-reported nature of the data also precludes ruling out alternative explanations that involve other well documented social processes, such as the false-consensus effect (Ross, Greene, & House, 1977), in that respondents may have based their perceptions of peer behaviors on their own actions and attitudes (e.g., Henry, Kobus, & Schoeny, 2011). And as noted above, other research has documented the propensity for adolescents to misperceive peers’ attitudes about and consumption of various types of foods (Lally et al., 2011; Perkins et al., 2010). Future research may employ longitudinal assessments, experimental designs, or objective measures as appropriate to overcome these limitations.
Finally, the present inferences are limited by issues of imperfect construct-to-measure alignment that are not uncommon in research involving secondary analysis. For example, the present measure of descriptive parental norms includes an element that may narrow the scope of the question more than the corresponding measure of peer norms. The measure included in the FLASHE questionnaires prompted participants to indicate their agreement with statements (one per behavior) such as “My parent(s) try to eat fruits and vegetables [avoid eating junk food or drinking sugary drinks; be physically active; limit their screen time] when I’m around.” While this statement clearly invokes elements of descriptive norms – how parents tend to behave – the last clause, “when I’m around,” implies awareness that the parent is deliberately trying to model desirable behavior. By contrast, the stem for peer norms simply states, “My friends eat fruits and vegetables […] most days of the week.”
The present findings have direct implications for interventions such as social norms marketing campaigns that aim to change perceptions of peer norms for health-promoting behaviors, suggesting that optimal approaches may attempt to shape teens’ attitudes about diet or physical activity as well as their perceptions of their friends’ behaviors. Testing indirect effects involving norms and attitudes and further clarifying the processes by which teens perceive peer norms for diet and physical activity will be important for informing interventions to improve behaviors. For example, as in other domains, adolescents may misperceive their peers’ attitudes or behaviors related to diet (Lally et al., 2011; Perkins, Perkins, & Craig, 2010), and may be susceptible to pluralistic ignorance if they mistakenly infer attitudes from behaviors (Miller & McFarland, 1987) – for example, inferring that others dislike vegetables from observing others’ avoidance of vegetables when in fact, all are avoiding vegetables because they are simultaneously adhering to the same social norm. Previous research suggests that targeting attitudinal norms may be the optimal approach for correcting pluralistic ignorance (Miller & Prentice, 2016). Though the present study only included measures of (perceived) descriptive peer norms, it would also be valuable to assess perceived injunctive peer norms and attitudes related to health-promoting and health-impairing behaviors in future research.
The present analysis of a large, national dataset underscores the potential impact of social norms on adolescent behaviors, and thus, their potential utility for improving patterns of health-related behaviors. Indeed, even adolescents who indicated that they did not particularly enjoy eating fruits or vegetables or exercising demonstrated statistically significant associations between the behaviors they perceived among their peers and their own patterns of diet and activity. Future interventions may target these modifiable – and potentially additive – constructs to establish healthy habits among adolescents with the potential for enduring benefits.
Contributor Information
Elise L. Rice, Behavioral Research Program, Division of Cancer Control and Population Sciences, National Cancer Institute..
William M. P. Klein, Behavioral Research Program, Division of Cancer Control and Population Sciences, National Cancer Institute..
References
- Ajzen I (1985). From intentions to actions: A theory of planned behavior In Action control (pp. 11–39). Springer Berlin Heidelberg. [Google Scholar]
- Baker CW, Little TD, & Brownell KD (2003). Predicting adolescent eating and activity behaviors: The role of social norms and personal agency. Health Psychology, 22(2), 189. [PubMed] [Google Scholar]
- Cialdini RB (2003). Crafting normative messages to protect the environment. Current Directions in Psychological Science, 12(4), 105–109. [Google Scholar]
- Centers for Disease Control and Prevention. (2010). National Youth Physical Activity and Nutrition Survey. Retrieved from ftp://ftp.cdc.gov/pub/data/yrbs/nypans/2010nypans_questionnaire.pdf.
- Conner M, & Sparks P (2015) Theory of planned behaviour and the reasoned action approach In: Conner Mark and Norman Paul (eds.) Predicting and changing health behaviour: Research and practice with social cognition models. Open University Press, pp. 142–188. [Google Scholar]
- Cooke R, Dahdah M, Norman P, & French DP (2016). How well does the theory of planned behaviour predict alcohol consumption? A systematic review and meta-analysis. Health Psychology Review, 10(2), 148–167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- De La Haye K, Robins G, Mohr P, & Wilson C (2011). How physical activity shapes, and is shaped by, adolescent friendships. Social Science & Medicine, 73(5), 719–728. [DOI] [PubMed] [Google Scholar]
- DiBello AM, Miller MB, Neighbors C, Reid A, & Carey KB (2018). The relative strength of attitudes versus perceived drinking norms as predictors of alcohol use. Addictive Behaviors, 80, 39–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Henry DB, Kobus K, & Schoeny ME (2011). Accuracy and bias in adolescents’ perceptions of friends’ substance use. Psychology of Addictive Behaviors, 25(1), 80–89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kelder SH, Perry CL, Klepp KI, & Lytle LL (1994). Longitudinal tracking of adolescent smoking, physical activity, and food choice behaviors. American Journal of Public Health, 84(7), 1121–1126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klein WMP, & Rice EL (in press). Health cognitions, decision-making and behavior: The ubiquity of social comparison To appear in Suls J, Collins RL, & Wheeler L (Eds.), Social Comparison in Judgment and Behavior. NY: Oxford University Press. [Google Scholar]
- Janz KF, Dawson JD, & Mahoney LT (2000). Tracking physical fitness and physical activity from childhood to adolescence: the Muscatine study. Medicine & Science in Sports & Exercise, 32(7), 1250–1257. [DOI] [PubMed] [Google Scholar]
- Lally P, Bartle N, & Wardle J (2011). Social norms and diet in adolescents. Appetite, 57(3), 623–627. [DOI] [PubMed] [Google Scholar]
- Larson NI, Neumark-Sztainer D, Hannan PJ, & Story M (2007). Family meals during adolescence are associated with higher diet quality and healthful meal patterns during young adulthood. Journal of the American Dietetic Association, 107(9), 1502–1510. [DOI] [PubMed] [Google Scholar]
- McClain AD, Chappuis C, Nguyen-Rodriguez ST, Yaroch AL, & Spruijt-Metz D (2009). Psychosocial correlates of eating behavior in children and adolescents: A review. International Journal of Behavioral Nutrition and Physical Activity, 6(1), 54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Merten MJ, Williams AL, & Shriver LH (2009). Breakfast consumption in adolescence and young adulthood: Parental presence, community context, and obesity. Journal of the American Dietetic Association, 109(8), 1384–1391. [DOI] [PubMed] [Google Scholar]
- Miller DT, & McFarland C (1987). Pluralistic ignorance: When similarity is interpreted as dissimilarity. Journal of Personality and Social Psychology, 53(2), 298–305. [Google Scholar]
- Miller DT, & Prentice DA (2016). Changing norms to change behavior. Annual Review of Psychology, 67, 339–361. [DOI] [PubMed] [Google Scholar]
- National Cancer Institute. (2018). Dietary Screener Questionnaire in the NHANES 2009–2010: Background. Retrieved from http://epi.grants.cancer.gov/nhanes/dietscreen/
- Nebeling LC, Hennessy E, Oh AY, Dwyer LA, Patrick H, Blanck HM, ... & Yaroch AL (2017). The FLASHE study: Survey development, dyadic perspectives, and participant characteristics. American Journal of Preventive Medicine, 52(6), 839–848. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oh AY, Davis T, Dwyer LA, Hennessy E, Li T, Yaroch AL, & Nebeling LC (2017). Recruitment, enrollment, and response of parent–adolescent dyads in the FLASHE study. American Journal of Preventive Medicine, 52(6), 849–855. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perkins JM, Perkins HW, & Craig DW (2010). Misperceptions of peer norms as a risk factor for sugar-sweetened beverage consumption among secondary school students. Journal of the Academy of Nutrition and Dietetics, 110(12), 1916–1921. [DOI] [PubMed] [Google Scholar]
- Reid AE, & Aiken LS (2013). Correcting injunctive norm misperceptions motivates behavior change: A randomized controlled sun protection intervention. Health Psychology, 32(5), 551–560. [DOI] [PubMed] [Google Scholar]
- Reid A, Taber JM, Ferrer RA, Biesecker BB, Lewis K, Biesecker L, & Klein WMP (2018). Associations of perceived norms with intentions to learn genomic sequencing results: Roles for attitudes and ambivalence. Health Psychology, 37(6), 553–561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ross L, Greene D, & House P (1977). The “false consensus effect”: An egocentric bias in social perception and attribution processes. Journal of Experimental Social Psychology, 13(3), 279–301. [Google Scholar]
- Saint-Maurice PF, Kim Y, Hibbing P, Oh AY, Perna FM, & Welk GJ (2017). Calibration and validation of the Youth Activity Profile: The FLASHE study. American Journal of Preventive Medicine, 52(6), 880–887. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saint-Maurice PF, & Welk GJ (2014). Web-based assessments of physical activity in youth: Considerations for design and scale calibration. Journal of Medical Internet Research, 16(12), e269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salvy SJ, De La Haye K, Bowker JC, & Hermans RC (2012). Influence of peers and friends on children’s and adolescents’ eating and activity behaviors. Physiology & Behavior, 106(3), 369–378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sawka KJ, McCormack GR, Nettel-Aguirre A, Hawe P, & Doyle-Baker PK (2013). Friendship networks and physical activity and sedentary behavior among youth: A systematized review. International Journal of Behavioral Nutrition and Physical Activity, 10(130), 1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheeran P, Maki A, Montanaro E, Avishai-Yitshak A, Bryan A, Klein WM, ... & Rothman AJ (2016). The impact of changing attitudes, norms, and self-efficacy on health-related intentions and behavior: A meta-analysis. Health Psychology, 35(11), 1178. [DOI] [PubMed] [Google Scholar]
- Smith TM, Calloway EE, Pinard CA, Hennessy E, Oh AY, Nebeling LC, & Yaroch AL (2017). Using secondary 24-hour dietary recall data to estimate daily dietary factor intake from the FLASHE study dietary screener. American Journal of Preventive Medicine, 52(6), 856–862. [DOI] [PubMed] [Google Scholar]
- Stok FM, de Vet E, de Ridder DT, & de Wit JB (2016). The potential of peer social norms to shape food intake in adolescents and young adults: A systematic review of effects and moderators. Health Psychology Review, 10(3), 326–340. [DOI] [PubMed] [Google Scholar]
- Welk GJ, Saint-Maurice PF, Kim Y, Ellingson LD, Hibbing P, Wolff-Hughes DL, & Perna FM (2017). Understanding and interpreting error in physical activity data: insights from the FLASHE study. American Journal of Preventive Medicine, 52(6), 836–838. [DOI] [PMC free article] [PubMed] [Google Scholar]