

Sir,
We report a case of intercostal drain (ICD) placement involving rib resection, which was performed under ultrasound-guided mid-transverse process to pleura (MTP) block. The patient was a 45-year-old female, posted for ICD placement and pleural biopsy because of leftpleural effusion secondary to carcinoma lung. Left-sided fourth rib resection was also planned for the ICD placement since there was crowding of ribs. All her routine biochemical investigations including coagulation profile were within normal limits. We performed the MTP block in the operating room under ultrasound guidance at the T4 level. Tuohy epidural needle was inserted in-plane from a cranial-to-caudal direction [Figure 1a] and 20 ml of 0.5% ropivacaine was injected at the mid-point between the posterior border of the transverse process and the pleura [Figure 1b]. This was followed by insertion of an indwelling catheter through the needle until it was 3 cm beyond the needle tip. Thirty minutes after the block placement, the patient reported decreased sensation to pinprick over the left anterior and lateral chest wall from T2 to T8 dermatomes. Additionally, 50 μg intravenous fentanyl was given at the time of surgical incision. She tolerated the procedure well. Postoperative analgesia was achieved with infusion of 0.2% of ropivacaine at the rate of 4 ml/h via the catheter, which was continued for 48 h. The MTP block has been recently described by Costache et al.[1] and involves deposition of local anaesthetics mid-way between the transverse process and the pleura, which is then believed to reach the paravertebral space by diffusion. This avoids puncturing the superior costo-transverse ligament and entering the paravertebral space which is more invasive and may cause complications like inadvertent pleural injury or intravascular and/or intrathecal injections. In our patient, we choose this block given its ease of performance and minimally invasive nature.
Figure 1.
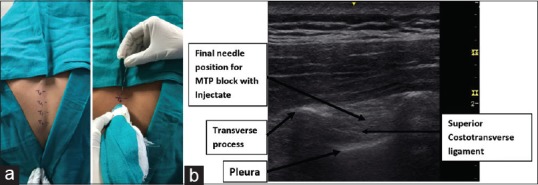
(a) With the patient sitting, the MTP block was performed in-plane at the T4 level on the left side with the needle oriented in a cranial-to-caudal direction. (b) Sono-anatomy of the MTP block. Arrow shows the site of drug deposition. MTP = Mid-transverse process to pleura
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCE
- 1.Costache I, de Neumann L, Ramnanan CJ, Goodwin SL, Pawa A, Abdallah FW, et al. The mid-point transverse process to pleura (MTP) block: A new end-point for thoracic paravertebral block. Anaesthesia. 2017;72:1230–6. doi: 10.1111/anae.14004. [DOI] [PubMed] [Google Scholar]