

Abstract
Background and Aims:
Sudden cardiac deaths remain a major health problem worldwide. Most of these cases generally involve out of hospital cardiac arrest, making the role of bystander resuscitation very crucial. In the developing countries, illiteracy and scarcity of health professionals is a great barrier to cardiopulmonary resuscitation (CPR) training. Video-based CPR training can offer an easily accessible modality in these situations. Hence, this study was conducted with an aim to assess the efficacy of video-based training in comparison to the traditional instructor-based CPR training in layman.
Methods:
This prospective cross-over observational study included 109 undergraduate university students attending voluntary resuscitation training and were randomly divided into two groups of video-based demonstration (VBD) and instructor-based demonstration (IBD) of compression only life support (COLS). They were then assessed for psychomotor skill development (Laerdal Simpad Plus Q-CPR) and perception about the quality of training methodology as primary and secondary objectives, respectively.
Results:
Population characteristics were similar in both the groups. In the VBD, scene safety was performed by 95.2% and call for help by 97.6%, and by 76.1% each in the IBD group (P < 0.05). Response to compression time (RCT) was significantly shorter in VBD (35 ± 9 sec) as compared to IBD (54 ± 14 sec) (P < 0.001). However, the proportion of participants performing response check, correct site identification, and other parameters were comparable.
Conclusion:
Video-based COLS training significantly decreased the RCT by 35% compared to traditional instructor-based training. However, other features of high-quality CPR remain comparable.
Key words: Compression only life support, cardiopulmonary resuscitation, simulation, training technique
INTRODUCTION
Approximately, six million sudden cardiac deaths (SCDs) occur annually due to ventricular tachyarrhythmia. The survival rate from sudden cardiac arrest is less than 1% worldwide and close to 5% in the United States. In the Indian subcontinent, the most common cause of arrest is a cardiovascular disease accounting for almost 60–65% cases.[1] The most common prearrest rhythm (63%) abnormality at the time of SCD is ventricular tachycardia, which if managed timely can be reverted back to sinus rhythm.[2] Appropriately executed bystander cardiopulmonary resuscitation (CPR) can drastically increase survival rates. However, according to available statistical data, it was achieved in less than 30% of out of hospital arrests.[3] Further, the awareness of cardiopulmonary resuscitation in the Indian population is less than 1%.
The training to the primary responders (laypersons) can be given using didactic lectures, video sessions, or simulation-based training. Recently, the use of simulator-based education has seen a surge due to its ability to simulate varied clinical scenarios in the interactive, reproducible, and safe environment. It further helps in learning about mistakes made during emergency situations, thus providing recommendations for changes in teaching and education. The use of a simulation-based training programme has shown to improve the quality of resuscitation efforts in actual cardiac arrest events.[4]
Traditional training in CPR requires a course stretched over a period of days, trained instructors and involves a course fee. Hence, we conducted this study with the hypothesis that video-based training will be an effective alternative to traditional CPR training for laypersons in India, to overcome the barriers in performing CPR.
METHODS
This prospective observational study involved undergraduate university students (layperson for CPR) attending a resuscitation programme on a voluntary basis. For the purpose of recruitment, emails, messages and pamphlets were distributed in different departments of university 1 week before the scheduled day of the programme. Participants not interested in joining study or with prior CPR training were excluded [Figure 1].
Figure 1.
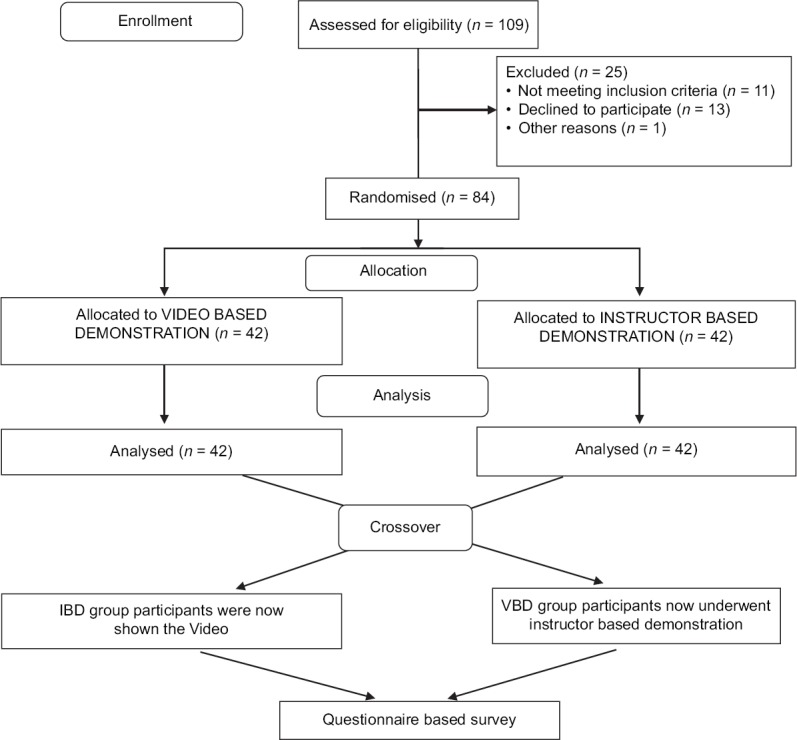
CONSORT flow diagram showing the enrolment, allocation, and analysis of the participants
A total of 109 persons registered initially, out of which 25 people were excluded from the study. Remaining 84 participants were randomly divided into two groups of video-based demonstration (VBD) and instructor-based demonstration (IBD) subsequent to informed consent for analysis and publication of the findings. In group VBD, the participants were shown a compression-only life support video in the local language. In the group IBD, a single-trained instructor demonstrated the steps of compression only cardiopulmonary resuscitation with a similar contact time of 9 min as of VBD.[5] Following this training, the participants in both the groups were asked to perform the steps of resuscitation for a given scenario of an adult patient who collapsed and fell unconscious in the middle of the road.
The primary objective was an assessment of psychomotor skill development in layperson in a simulated scenario as a part of compression-only cardiopulmonary resuscitation training. The secondary objective was the perception of lay responders about the quality of training methodology.
The evaluation of skills was based on a structured checklist [Table 1] reflecting essential actions for resuscitation and successful outcome on Resusci Anne Advanced Skill Trainer (Laerdal Medical, Norway). The performance was assessed by two trainers watching independently. Clinical actions that were performed as per the compression only life support (COLS) guidelines of Indian Society of Anaesthesiologist were scored as “performed” and any deviation from guideline was scored as “nonperformed” .[6] Depth, rate, recoil and overall performance were assessed by Laerdal Simpad Plus System. Response to compression time (RCT) from check response to first compression and chest compression fraction (CCF) was also recorded. Following the skill assessment, the groups were rotated and were asked to complete the survey based on a structured questionnaire regarding the realism of scenario, emotional connect during training, and the value of simulated scenario in helping them to provide resuscitation.
Table 1.
Checklist for the assessment of cardiopulmonary resuscitation skill development
| Parameters | VBD (n=42) |
IBD (n=42) |
P |
|---|---|---|---|
| Scene safety performed (n) | 40 | 32 | 0.02 |
| Unresponsiveness checked (n) | 39 | 36 | 0.48 |
| Call for help (n) | 41 | 32 | 0.007 |
| Correct site for compression identified (n) | 40 | 36 | 0.26 |
| Response to compression time (sec) | 35±9 | 54±14 | <0.001 |
| Chest compression fraction (%) | 87% | 82% | 0.43 |
| Mean depth (mm) | 57±18 | 53±24 | 0.39 |
| Mean rate of compression (per minute) | 106±26 | 110±21 | 0.44 |
| Mean adequate recoil (%) | 74 | 71 | 0.75 |
| Overall CPR score >90% (n) | 38 | 40 | 0.66 |
n – Number of rescuers, VBD – Video-based demonstration, IBD – Instructor-based demonstration, P≤0.05 is considered statistically significant (Source: original)
Quantitative data were assessed using t-test, quantitative data with Chi-square test, and the questionnaire regarding their perception of the level of realism of the simulated scenarios and the value of simulation in helping them to provide COLS was analyzed using proportional analysis. The analysis was performed using Graph Pad Prism 5.00 (Graph Pad Software, San Diego, CA, USA) as appropriate. A P value < 0.05 was taken as statistically significant.
RESULTS
Population characteristics were similar in both the groups [Table 2]. In the VBD, scene safety was performed by 40 people (95.2%) and call for help by 41 (97.6%) which was 32 (76.1%) and 32 (76.1%) respectively in the IBD group (P < 0.05). Response check, correct site identification and CCF (87% in VBD and 82% in IBD) were comparable in both the groups (P > 0.05). However, the RCT was significantly shortened by 35% in VBD (35 ± 9 sec) as compared to IBD (54 ± 14 sec) (P < 0.001). The mean depth was 57 ± 18 and 53 ± 24 mm (P > 0.05), mean rate of compression was 106 ± 26 and 110 ± 21 (P > 0.05), and mean chest recoil was 74% and 71% in VBD and IBD, respectively. Overall, CPR score of >90% was performed by 38 participants (90.47%) in VBD group and 40 (95.2%) in IBD group (P > 0.05) [Table 1]. As per the survey after rotating all the 84 participants to both groups, 94% believed that VBD was a realistic experience and 96% believed that was interesting enough to retain the concentration. A total of 100% believed that VBD engaged them emotionally, while 100% said IBD was not feasible for large groups. And 92% were confident that VBD made them confident in handling such situations in real life [Table 3].
Table 2.
Participants characteristics
| Characteristics | VBD (n=42) |
IBD (n=42) |
P |
|---|---|---|---|
| Age (years) | 41.3±8.7 | 39.2±10.4 | 0.32 |
| Sex (M:F) | 27:15 | 20:22 | 0.19 |
| Level of education | |||
| Below Senior Secondary School (n) | 0 | 0 | 1.00 |
| Above Senior Secondary School (n) | 42 | 42 | 1.00 |
| Prior CPR training (n) | 0 | 0 | 1.00 |
VBD – Video-based demonstration, IBD – Instructor-based demonstration, n – Number of participants, mean±standard deviation, M:F – Male:female, P≤0.05 is considered significant (Source: original)
Table 3.
Assessment of quality of cardiopulmonary resuscitation training
| Perception | Participants (n=84) |
|
|---|---|---|
| VBD | IBD | |
| Realism of scenario (realistic experience) | 79 (94.05%) | 5 (5.95%) |
| Is it interesting enough to retain your concentration during the session? | 81 (96.42%) | 3 (3.57%) |
| Emotional engagement during training | 84 (100%) | 0 |
| Feasibility in large groups | 84 (100%) | 0 |
| Confident in handling a real situation | 77 (91.66%) | 7 (8.33%) |
n – Number of rescuers, VBD – Video-based demonstration, IBD – Instructor-based demonstration (Source: original)
DISCUSSION
In this study, the authors assessed the video- and instructor-based training for COLS and found that video-based demonstration surpasses in initial steps of resuscitation notably RCT while remained comparable in terms of high-quality CPR characteristics.
For lay rescuer resuscitation, early recognition and activation of emergency services play a very vital role in increasing the chances of survival of victims of cardiac arrest outside the hospital.[7,8] Swor et al. established that delays prior to an emergency call may be present in as many as half of all out of the hospital cardiac arrest (OHCA) and is associated with poorer survival.[9]
In developing countries, where there is a scarcity of emergency medical professionals, training and preparing the lay persons who are actually the primary responders in cases of emergencies can be helpful in improving the outcome.[10,11] We trained the participants with video- and instructor-based demonstration in a simulated scenario and evaluated them on Laerdal Simpad plus Q-CPR feedback simulator. It was observed that participants trained with video-based performed better than instructor-based training for initial steps of resuscitation, such as scene safety, call for help, and RCT. As early bystander CPR generates a small but crucial amount of blood flow to the vital organs especially the brain, there is a significant reduction in the degree of cerebral damage and consequent increase in the time frame for successful resuscitation, defibrillation, and advanced cardiac support.[12,13] In fact, time from collapse to CPR and defibrillation has been termed as the most critical modifiable element associated with better neurological outcome and recent literature recommends to decrease the time to first compression.[14] The authors believe that the decreased RCT in video-based training could be due to video's clear instructions to practice, the images and contextualising reality that remove the learning obstacle. The available literature shows that the ability of students to learn is enhanced by incorporation of multimedia, such as pictures, audio, and video as it utilises various modalities that stimulates the senses and make the audience more receptive to the data.[15] Though video-based training seems to be passive, they very well keep the behaviorally inactive learner engaged, by stimulating their thinking and learning abilities. In fact, well-presented systematic instructions and messages promote very high cognitive activity required for learning, understanding, and retention by the viewers. Associated sound and musical effects further influence the affective domain of the learners.[16] Videos further strengthens internal consistency, makes comparison of data and information easy across the students/audience and between different sessions, help them retain the data for longer duration and repeatability as and when required.[15,17]
Videos made in the local environment and using local languages add to the video's advantages for training purposes. It can provide a valued teaching tool that allows better visualisation of steps, offer media-rich audio, and visual stimulation covering a wider spectrum of the learning styles or preferences.[18] Though instructor-based demonstration enhances communication skills, technical aspects, and increases student confidence they are associated with problems like shortage of faculty, difficulty in the visualisation of the demonstration by students, nonrepeatability along with time and financial constraints.[19]
The quality of cardiopulmonary resuscitation is also an important contributor to the successful outcome. We in our study observed that compression rate, depth, and CCF were similar in both the groups. Visual elements help people to quickly absorb information more efficiently and effectively due to emotional content.[20] They engage the imagination and heighten creative thinking by stimulating other areas of the brain, which in turn leads to a more profound and accurate understanding of the presented material.[21] It also has been shown that emotions play an essential role in decision-making, perception, learning, and they influence the very mechanisms of rational thinking.[22,23] In a study by Mir et al., he reported that videotaped demonstrations can be as effective as live demonstrations in transmitting clinical knowledge and skills to medical students.[24] Initial studies comparing video self-instruction to traditional CPR training have all found VSI training to be at least as effective as, if not better than, traditional CPR training in terms of learning the key psychomotor skills, even when they were re-assessed at 3 months.[25,26] Despite the fact that our study has few limitations such as being a mannequin-based study and replication of findings in actual scenario cannot be ascertained, nonassessment of patient outcome, and no follow-up to assess retention, it is still advantageous as video-based training is found to be less labor consuming and cost-effective.[25,26,27,28,29] Further, video's flexibility of use have been cited as an important advantage for training in developing countries and it can be an effective tool for raising awareness.[30]
The questionnaire-based survey of our study revealed that videos made the participants more confident about handling a real situation as they saw that timely intervention saved the life and they could emotionally connect with the relatives of the patient and could feel their happiness when the patient recovers. They appreciated the realism of the scenario in contrast to the instructor-based training which is more technical and mechanical. Interviews with bystanders have provided valuable insight into the emotional milieu associated with OHCA events, with many reporting that panic, fear of poor performance, and lack of training were common deterrents to performing bystander CPR.[31] However, it is also clear that delayed or failed recognition of cardiac arrest may also contribute to a lack of bystander action, with as many as 80% of bystanders without first-aid training failing to recognise the signs of cardiac arrest.[32]
The authors opine that the video-based training for compression only resuscitation can be an effective tool for creating awareness among people about the importance of timely intervention. The authors believe that the findings of the study can be extrapolated to create effective CPR awareness programmes with the use of short CPR videos on national television (prime time) every day, or at set intervals or in public places like cinema halls, or in stadiums before matches, etc.
CONCLUSION
Video-based COLS training significantly improved the initial recognition and RCT (-Δ35%) compared to traditional instructor- based training. However, other features of high-quality CPR remain comparable.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
The authors acknowledge the contribution of Dr. Poojangi Varshney, Dr. Mohd Luqman, and Dr. Sania Parveen in organizing COLS training programme.
REFERENCES
- 1.Madhavan SR, Reddy S, Panuganti PK, Joshi R, Mallidi J, Raju K, et al. Epidemiology of sudden cardiac death in rural South India-insights from the andhra pradesh rural health initiative. Indian Pacing Electrophysiol J. 2011;1:93–102. [PMC free article] [PubMed] [Google Scholar]
- 2.Deo R, Albert CM. Epidemiology and genetics of sudden cardiac death. Circulation. 2012;125:620–37. doi: 10.1161/CIRCULATIONAHA.111.023838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mutchner L. The ABCs of CPR--again. Am J Nurs. 2007;107:60–9. doi: 10.1097/00000446-200701000-00024. [DOI] [PubMed] [Google Scholar]
- 4.Wayne DB, Sinddall VJ, Butter J, Fudala MJ, Wade LD, Feinglass J, et al. A longitudinal study of internal medicine residents’ retention of advanced cardiac life support skills. Acad Med. 2006;81(10 Suppl):S9–12. doi: 10.1097/00001888-200610001-00004. [DOI] [PubMed] [Google Scholar]
- 5.Bentley JW, Van Mele P. Sharing ideas between cultures with videos. International Journal of Agricultural Sustainability. 2011;9:258–63. [Google Scholar]
- 6.Ahmed SM, Garg R, Divatia JV, Chakra Rao SSC, Mishra BB, Kalandoor MV, et al. Compression-only life support (COLS) for cardiopulmonary resuscitation by layperson outside the hospital. Indian J Anaesth. 2017;61:867–73. doi: 10.4103/ija.IJA_636_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Nehmea Z, Andrew E, Cameron P, Bray JE, Meredith IT, Bernard S, et al. Direction of first bystander call for help is associated with outcome from out-of-hospital cardiac arrest. Resuscitation. 2013;85:42–8. doi: 10.1016/j.resuscitation.2013.08.258. [DOI] [PubMed] [Google Scholar]
- 8.Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, De Simone G, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2010 update: A report from the American Heart Association. Circulation. 2010;121:e46–215. doi: 10.1161/CIRCULATIONAHA.109.192667. [DOI] [PubMed] [Google Scholar]
- 9.Swor RA, Compton S, Domeier R, Harmon N, Chu K. Delay prior to calling 9-1-1 is associated with increased mortality after out-of-hospital cardiac arrest. Prehosp Emerg Care. 2008;12:333–8. doi: 10.1080/10903120802100902. [DOI] [PubMed] [Google Scholar]
- 10.Chandrasekaran S, Kumar S, Bhat SA, Saravankumar, Shabbir PM, Chandrasekaran V. Awareness of basic life support among medical, dental, nursing students and doctors. Indian J Anaesth. 2010;54:121–6. doi: 10.4103/0019-5049.63650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Businger A, Rinderknecht S, Blank R, Merki L, Carrel T. Students’ knowledge of symptoms and risk factors of potential life-threatening medical conditions. Swiss Med Wkly. 2010;140:78–84. doi: 10.4414/smw.2010.12951. [DOI] [PubMed] [Google Scholar]
- 12.Waalewijn RA, Nijpels MA, Tijssen JG, Koster RW. Prevention of deterioration of ventricular fibrillation by basic life support during out-of-hospital cardiac arrest. Resuscitation. 2002;54:31–6. doi: 10.1016/s0300-9572(02)00047-3. [DOI] [PubMed] [Google Scholar]
- 13.Berg R, Hilwig R, Kern K, Ewy G. Pre countershock cardiopulmonary resuscitation improves ventricular fibrillation median frequency and myocardial readiness for successful defibrillation from prolonged ventricular fibrillation: A randomized, controlled swine study. Ann Emerg Med. 2002;40:563–70. doi: 10.1067/mem.2002.129866. [DOI] [PubMed] [Google Scholar]
- 14.Bobrow BJ, Panczyk M. Time to compress the time to first compression. J Am Heart Assoc. 2018;7:e009247. doi: 10.1161/JAHA.118.009247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Singh U. Use of Multimedia Technology in Library. 2016. [Last accessed on 2019 Feb 15]. Available from: https://www.researchgate.net/publication/303549082 .
- 16.Mayer RE. Multimedia Learning. New York, NY, US: Cambridge University Press; 2001. [Google Scholar]
- 17.Mohamed El-Sayed HE, Elmashad HA, Ibrahim AA. The effectiveness of utilizing video- assisted and lecture cum demonstration method on the nursing students’ knowledge and skills in using partograph. IOSR J Nurs Health Sci (IOSR-JNHS) 2017;6:61–70. [Google Scholar]
- 18.Ramlogan S, Raman V, Sweet J. A comparison of two forms of teaching instruction: Video vs. live lecture for education in clinical periodontology. Eur J Dent Educ. 2014;18:31–8. doi: 10.1111/eje.12053. [DOI] [PubMed] [Google Scholar]
- 19.Packer ME, Scott BJ, Davis DM. An assessment of the influence of clinical demonstrations on the confidence of undergraduate dental students, when treating patients requiring removable partial dentures. Eur J Dent Educ. 1999;3:133–9. doi: 10.1111/j.1600-0579.1999.tb00079.x. [DOI] [PubMed] [Google Scholar]
- 20.Levie WH, Lentz R. Effects of text illustrations: A review of research. Edu Commun Technol J. 1982;30:195–232. [Google Scholar]
- 21.Bobrow D, Norman D. Some principles of memory schemata. In: Bobrow D, Collins A, editors. Representation and Understanding: Studies in Cognitive Science. New York: Academic Press; 1975. pp. 131–149. [Google Scholar]
- 22.Van Oostendorp H, Preece J, Arnold AG. Designing multimedia for human needs and capabilities: Guest editorial for Interacting with Computers Special Issue. Interact Comput. 1999;12:1–5. [Google Scholar]
- 23.Burmark L. Visual Literacy: Learn to See, See to Learn. Assn for Supervision and Curriculum, CA: Berkley; 2002. [Google Scholar]
- 24.Mir MA, Marshall RJ, Evans RW, Hall R, Duthie HL. Comparison between videotape and personal teaching as methods of communicating clinical skills to medical students. Br Med J (Clin Res Ed) 1984;289:31–4. doi: 10.1136/bmj.289.6436.31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Isbye DL, Rasmussen LS, Lippert FK, Rudolph SF, Ringsted CV. Laypersons may learn basic life support in 24 min using a personal resuscitation manikin. Resuscitation. 2006;69:435–42. doi: 10.1016/j.resuscitation.2005.10.027. [DOI] [PubMed] [Google Scholar]
- 26.Lynch B, Einspruch EL, Nichol G, Becker LB, Aufderheide TP, Idris A. Effectiveness of a 30-min CPR self instruction program for lay responders: A controlled randomized study. Resuscitation. 2005;67:31–43. doi: 10.1016/j.resuscitation.2005.04.017. [DOI] [PubMed] [Google Scholar]
- 27.Atkinson PR, Bingham J, McNicholl BP, Loane MA, Wootton R. Telemedicine and cardiopulmonary resuscitation: The value of video-link and telephone instruction to a mock bystander. J Telemed Telecare. 1999;5:242–5. doi: 10.1258/1357633991933783. [DOI] [PubMed] [Google Scholar]
- 28.Todd KH, Braslow A, Brennan RT, Lowery DW, Cox RJ, Lipscomb LE, et al. Randomized, controlled trial of video self-instruction versus traditional CPR training. Ann Emerg Med. 1998;31:364–9. doi: 10.1016/s0196-0644(98)70348-8. [DOI] [PubMed] [Google Scholar]
- 29.Batcheller AM, Brennan RT, Braslow A, Urrutia A, Kaye W. Cardiopulmonary resuscitation performance of subjects over forty is better following half-hour video self instruction compared to traditional four-hour classroom training. Resuscitation. 2000;43:101–10. doi: 10.1016/s0300-9572(99)00132-x. [DOI] [PubMed] [Google Scholar]
- 30.Rico L, Andreas M. Video in Development: Filming For rural Change. Wageningen, Netherlands: CTA; 2009. [Google Scholar]
- 31.Swor R, Khan I, Domeier R, Honeycutt L, Chu K, Compton S. CPR training and CPR performance: Do CPR-trained bystanders perform CPR? Acad Emerg Med. 2006;13:596–601. doi: 10.1197/j.aem.2005.12.021. [DOI] [PubMed] [Google Scholar]
- 32.Breckwoldt J, Schloesser S, Arntz HR. Perceptions of collapse and assessment of cardiac arrest by bystanders of out-of-hospital cardiac arrest (OOHCA) Resuscitation. 2009;80:1108–13. doi: 10.1016/j.resuscitation.2009.06.028. [DOI] [PubMed] [Google Scholar]