

Abstract
An estimation of the appropriate tubing depth for fixation is helpful to prevent inadvertent endobronchial intubation and prolapse of cuff from the vocal cord. A feasible estimation formula should be established. We measured the anatomical length of the upper-airway tract through the oral and nasal pathways on cephalometric radiographs and tried to establish the estimation formula from the height of the patient. The oral upper-airway tract was measured from the tip of the incisor to the vocal cord. The nasal upper-airway tract was measured from the tip of the nostril to the vocal cord. The tracts were smoothly traced by using software. The length of the oral upper-airway tract was 13.2 ± 0.8 cm, and the nasal upper-airway tract was 16.1 ± 0.9 cm. We found no gender difference (p > .05). The correlations between the patients' height and the length of the oral and nasal upper-airway tracts were 0.692 and 0.760, respectively. We found that the formulas (height/10) − 3 (in cm) for oral upper-airway and (height/10) + 1 (in cm) for nasal upper-airway tract are the simple fit estimation formulas. The average error and standard deviation of the estimated values from the measured values were 0.50 ± 0.66 cm for the oral tract and 0.39 ± 0.63 cm for the nasal tract. Thus, considering the length of the intubation marker of each product (DM), we would like to propose the length of tube fixation as (height/10) + 1 + DM for nasal intubation and (height/10) − 3 + DM for oral intubation. In conclusion, the estimation formulas of (height/10) − 3 + DM and (height/10) + 1 + DM for oral and nasal intubation, respectively, are within almost 1 cm error in most cases.
Key Words: General anesthesia, Intubation tube, Oral intubation, Nasal intubation, Tracheal, Larynx, Cephalogram
An inappropriate endotracheal tube depth can inadvertently lead to endobronchial intubation or damage to vocal cords by the endotracheal tube cuff. Such errors can result in adverse events impairing ventilation or injury to the vocal cords.1,2 Auscultation is a widely applied procedure used to confirm bilateral ventilation and rule out endobronchial intubation. However, the sensitivity of auscultation is not sufficiently high (66%).3 Confirming the depth of endotracheal tubes is helpful for preventing endobronchial intubation.4
Certain situations are more commonly associated with intubation length errors. The main-stem intubation rate increases by as much as 28% in emergency cases, such as cardiac arrest.5 Malposition of the endotracheal tube is common and more critical in newborns and infants.6 Thus, several clinical studies have been performed and various formulas have been proposed for newborns and infants.7,8 Because the fixation tube length is not as critical for adults as it is for infants, a formula for the optimal insertion length has not been considered, and average distances such as the 20/22 or 21/23 (cm, female/male) rule have instead been simply applied. A simple method to determine appropriate tube length for intubation could help to avoid endotracheal tube malposition.
For dental anesthesia, the nasal pathway is usually selected for endotracheal intubation. The length of the upper-airway tract through the nasal pathway has not been well documented but is likely to be correlated with patient height. The recommended lengths for the fixation of endotracheal tubing have been proposed based on patient height. Several formulas have been suggested for different ethnic populations.9–13 These formulas seem to vary among ethnicities. Here, we explored the variations in the lengths of the upper-airway tract through the nasal and oral pathways using cephalometric radiographs and examined whether a simple formula could be used to estimate the length of endotracheal tubing for fixation in adult Japanese patients.
METHODS
Inclusion and Exclusion Criteria
This study included patients who were 16 years or older and who had undergone cephalometric radiography examinations using the Cephalostat cephalometric unit (Asahiroenrgen Ind Co Ltd, Kyoto, Japan) for orthodontic treatments requiring elective maxillofacial surgery at Showa University Dental Hospital between July 2013 and March 2017. Patients whose cephalometric radiogram landmarks were difficult to gauge were excluded. These cases included patients with a defect of the incisor alveolus, a missing incisor, or obstacles to identifying the incisor tip such as the presence of artificial materials, orthodontic brackets, or fixation plates. The protocol for this retrospective clinical examination was approved by the Research Ethics Committee of Showa University Dental Hospital.
Measurement Criteria
We measured the anatomical lengths of the upper-airway tract through the oral and nasal pathways on the cephalometric radiograms as follows: the oral upper-airway tract was measured from the tip of the incisors to the arytenoid cartilage (to which the vocal cords attach) through the hard palate, the soft palate, and the palatine uvula, and the nasal upper-airway tract was measured from the tip of the nostrils to the arytenoid cartilage through the concha nasalis media and the posterior wall of the pharynx (Figure 1). We set measurement markers on the route of intubation tubing and measured the tract using a DICOM viewer (Array Corp, Tokyo, Japan). The tracts were smoothly traced using software (AOC mini, Version 1.3; Array Corp) built into the DICOM viewer. Because the cephalometric unit produced a 10% magnification (1.1:1 vs 1.0:1 image:true value), the values were corrected with a factor 1.0/1.1. We then examined whether the length of the pathway was correlated with the height of the patient measured before operation and developed estimation formulas using (patient height/10) + an integer (in cm).
Figure 1. .

A cephalometric analysis of oral and nasal airway length. We employed 4 landmarks for oral airway and 5 landmarks for nasal airway. These landmarks were smoothly connected by using the DICOM viewer.
Statistics
Data are presented as the mean ± SD. The correlation coefficient is presented as Pearson r. The reproducibility of the estimation formula was evaluated using a Bland-Altman plot.14 The level of significance was determined as p < .05.
RESULTS
A total of 100 patients (50 men and 50 women) were included in this study. This sample size is recommended for Bland-Altman plot analyses.15 For the men, the median age was 25.0 ± 8.2 years and the median height was 172.8 ± 6.6 cm. For the women, the median age was 24.3 ± 7.6 years and the median height was 160.3 ± 6.0 cm. The average length of the oral upper-airway tract was 13.2 ± 0.8 cm (13.7 ± 0.7 cm for men, 12.7 ± 0.5 cm for women), and that of the nasal upper-airway tract was 16.1 ± 0.9 cm (16.8 ± 0.8 cm for men, 15.4 ± 0.5 cm for women). The correlations between patient height and the lengths of the oral and nasal upper-airway tracts were 0.691 (Figure 2) and 0.760 (Figure 3), respectively. We found that the following simple formulas were useful for estimating the lengths of the upper-airway tracts: for the oral pathway, (height/10) − 3 (in cm), and for the nasal pathway, (height/10) + 1 (in cm) (Figures 4 and 5). The derived simple fit estimation did not significantly differ between the sexes, and the same additional integers (−3 for the oral pathway, +1 for the nasal pathway) were suitable for both sexes. The average errors and standard deviations of the estimated values from the measured values were 0.50 ± 0.66 cm for the oral tract and 0.39 ± 0.63 cm for the nasal tract. We did not find a significant fixed or proportional bias for either estimation in nasal tract estimation (p > .05), whereas a significant fixed bias was confirmed in oral tract estimation (p < .05).
Figure 2.

Correlation between patient height and oral tract length. A strong correlation between patient height and the length of the oral tract was confirmed (r = 0.691; p > .01). No significant difference was seen between separate plots for men and women.
Figure 3.

Correlation between patient height and nasal tract length. A strong correlation between patient height and the length of the nasal tract was confirmed (r = 0.760; p > .01). No significant difference was seen between separate plots for men and women.
Figure 4.
Bland-Altman plots for the bias between the estimated and measured values of oral tract length. A significant fixed bias was observed (p < .05).
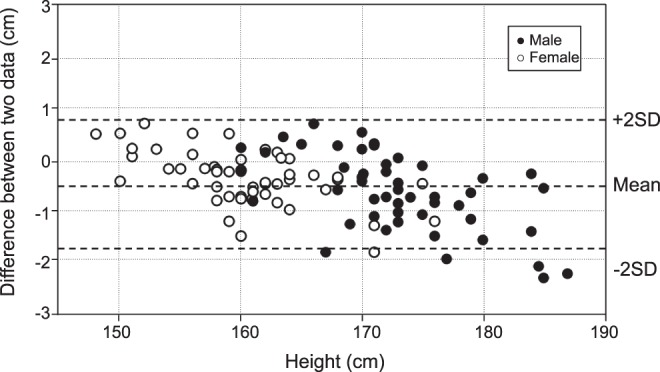
Figure 5.

Bland-Altman plots for the bias between the estimated and measured values of nasal tract length. No significant fixed bias or proportional bias was observed (p > .05).
DISCUSSION
Endobronchial intubation must be reliably detected. Auscultation of bilateral chest walls can be performed to confirm tracheal intubation. However, Sitzwohl et al4 reported that auscultation alone is inadequate for assessing the depth of endotracheal tube insertion even when performed by experienced anesthetists, and the combination of depth confirmation and observation of the chest wall movements improves the accuracy of tube positioning. Pleural ultrasound confirmation has also been suggested to avoid tube malposition instead of auscultation.3 Average tube depths are frequently used to avoid endobronchial intubation. The optimal insertion tube depth for oral intubation is considered to be 20 cm for women and 22 cm for men (20/22 rule)4 or 21 cm for women and 23 cm for men (21/23 rule),2 depending on ethnicity. Such rough estimations, however, can lead to inadvertent endobronchial intubation or inadequate insertion. Ideally, tube fixation should be customized according to the height of individuals.
Our study demonstrated that the length of the upper-airway tract is correlated with patient height. The tract length increases by approximately 1 cm for every 10 cm of height. This finding is not new, as “height/10 ± an integer” has been proposed in several articles for the distance from the fixation site to the laryngeal inlet.10,13
The fixation depth, however, requires the addition of the distance between the distal edge of the intubation guide mark and the tip of the endotracheal tube (DM)12 (Figure 6) to the length of the upper-airway tract. Chong et al12 reported that the DM length varies among brands from 74 to 96 mm for 7.0–8.5-mm internal diameter tubing. Thus, the DM should be considered when determining the depth length for fixation. We would like to propose that the length of tube fixation should be height/10 + 1 + DM (in cm) for nasal intubation and height/10 − 3 + DM (in cm) for oral intubation. The DM can be fixed if the same brand of endotracheal tubing is always used at a hospital.
Figure 6.

Intubation marker of the endotracheal tube. The distance to add to the airway length to help ensure appropriate tube depth (DM; distance between the distal edge of intubation guide mark and the tip).
The airway tract length may differ among ethnicities. We compared the reported lengths of oral airway tracts corresponding to our measurement with other data from Korea, Thailand, India, and Australia.9,11,13,16 The shortest reported length of the oral upper airway tract in women was 9.5 cm in the report from Thailand, and the longest was 14.9 cm in the report from Korea. The shortest reported length of the oral upper airway tract in men was 10.8 cm in the report from Thailand, and the longest was 16.8 cm in the report from Korea. Both of these studies used fiber-optic scopes. Our data were intermediate between these previous reports. These differences might be attributable, however, to the heights of the subjects.
For the nasal tract, only 2 other sets of data were available, from Thailand and Australia.13,16 The longest reported length in men was 19.8 cm in the report from Australia, and the shortest was 15.6 cm in the report from Thailand. The longest reported length in women was 18.0 cm in the report from Australia, and the shortest was 14.9 cm in the report from Thailand. Our data for both sexes were intermediate between these data. These differences are also likely to be attributable to the height of the subjects.
The difference in lengths between the nasal pathway and the oral pathway, however, has not been thoroughly examined. A simple estimation formula for guiding tracheal tube fixation was formerly proposed to be (height/10) + 2 cm for oral intubation and (height/10) + 8 cm for nasal intubation in Australian patients.13 Techanivate et al16 reported that a suitable fixed length of endotracheal tube for Thai patients was (height/10) + 4 cm for oral intubation and (height/10) + 9 cm for nasal intubation. Thus, the differences in distance between the proposed oral and nasal tracts in these 2 samples were 6 and 5, respectively. Our study demonstrated that the difference between the 2 tracts was only 4 cm, which is shorter than the previously reported results. The nasal cavity comprises the upper, middle, and lower tracts. We choose the middle route to insert the endotracheal tubing because the incidence of epistaxis is thought to be lower than that for the upper tract.17 The insertion of the tube through the upper tract can injure the Kiesselbach area and the sphenopalatine artery, leading to arterial bleeding. Therefore, the lower or middle route should be chosen to ensure patient safety; however, the upper route can sometimes be chosen if the direction of the nostril's orifice naturally leads toward an upper route. Consequently, the difference between the results of our study and those of previous reports might be attributable to differences in the route through the nasal cavity. We measured the length of the lower route though the concha nasalis inferior and found that it was approximately 2 cm shorter than the middle route. The upper route seems to be the longest pathway. This may explain the smaller difference between the oral and nasal tracts in our study, compared with previous reports.
We also showed that the difference in airway tract length is attributable to height, and not sex itself. Plots of the correlation between height and airway length showed a minimal difference in the slopes between sexes. Our results agree with those of Pak et al,9 who reported no difference between sexes.9
In the present study, the average errors and the standard deviations of the estimated values from the measured values were 0.50 ± 0.66 cm for the oral tract (Figure 4) and 0.39 ± 0.63 cm for the nasal tract (Figure 5). The variation putatively caused by this estimation formula corresponds to a maximum of 1.32 cm (95% CI) for oral intubation and 1.26 cm (95% CI) for nasal intubation. Such a small degree of variation is feasible for clinical use. We also have to take account of the fixed bias in the oral tract estimation. We should consider that taller patients may have longer oral tract length than the estimated value.
Our study had some limitations. Because the patients were limited to adults, this formula cannot be used for pediatric patients. Furthermore, the ethnicity of the patients was limited to Japanese. Thus, this formula might not be applicable to other ethnicities. Our study was also performed retrospectively; thus, the actual optimal tube length could not be confirmed during orthognathic surgery. A prospective study is needed to confirm the appropriateness of this proposed formula, and further study is needed to validate our results. We did not analyze the data according to the type of facial deformity. If we accumulate enough examples of each deformity, it would be worthwhile to examine whether or not the length may vary according to the type of facial deformity.
CONCLUSION
In conclusion, the formulas of (height/10) − 3 + DM (in cm) for oral intubation and (height/10) + 1 + DM (in cm) for nasal intubation have an error of about 1 cm or less in most cases and are suitable for estimating appropriate tube lengths for fixation during endotracheal intubation in Japanese patients.
ACKNOWLEDGMENT
We thank Mrs Myrna Taniguchi for her valuable help with the English revision.
REFERENCES
- 1.Caplan RA, Posner KL, Ward RJ, Cheney FW. Adverse respiratory events in anesthesia: a closed claims analysis. Anesthesiology. 1990;72:828–833. doi: 10.1097/00000542-199005000-00010. [DOI] [PubMed] [Google Scholar]
- 2.Cornelius B, Sakai T. Inadvertent endobronchial intubation in a patient with a short neck length. Anesth Prog. 2015;62:66–70. doi: 10.2344/0003-3006-62.1.66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ramsingh D, Frank E, Haughton R, et al. Auscultation versus point-of-care ultrasound to determine endotracheal versus bronchial intubation: a diagnostic accuracy study. Anesthesiology. 2016;124:1012–1020. doi: 10.1097/ALN.0000000000001073. [DOI] [PubMed] [Google Scholar]
- 4.Sitzwohl C, Langheinrich A, Schober A, et al. Endobronchial intubation detected by insertion depth of endotracheal tube, bilateral auscultation, or observation of chest movements: randomised trial. BMJ. 2010. 341:c5943. [DOI] [PMC free article] [PubMed]
- 5.Dronen S, Chadwick O, Nowak R. Endotracheal tip position in the arrested patient. Ann Emerg Med. 1982;11:116–117. doi: 10.1016/s0196-0644(82)80328-4. [DOI] [PubMed] [Google Scholar]
- 6.Morray JP, Geiduschek JM, Caplan RA, Posner KL, Gild WM, Cheney FW. A comparison of pediatric and adult anesthesia closed malpractice claims. Anesthesiology. 1993;78:461–467. doi: 10.1097/00000542-199303000-00009. [DOI] [PubMed] [Google Scholar]
- 7.Boensch M, Schick V, Spelten O, Hinkelbein J. Estimation of the optimal tube length: systematic review article on published formulae for infants and children. Anaesthesist. 2016;65:115–121. doi: 10.1007/s00101-015-0123-6. [DOI] [PubMed] [Google Scholar]
- 8.Lau N, Playfor SD, Rashid A, Dhanarass M. New formulae for predicting tracheal tube length. Paediatr Anaesth. 2006;16(12):1238–1243. doi: 10.1111/j.1460-9592.2006.01982.x. [DOI] [PubMed] [Google Scholar]
- 9.Pak HJ, Hong BH, Lee WH. Assessment of airway length of Korean adults and children for otolaryngology and ophthalmic surgery using a fiberoptic bronchoscope. Korean J Anesthesiol. 2010;59:249–255. doi: 10.4097/kjae.2010.59.4.249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Techanivate A, Kumwilaisak K, Worasawate W, Tanyong A. Estimation of the proper length of nasotracheal intubation by Chula formula. J Med Assoc Thai. 2008;91:173–180. [PubMed] [Google Scholar]
- 11.Varshney M, Sharma K, Kumar R, Varshney PG. Appropriate depth of placement of oral endotracheal tube and its possible determinants in Indian adult patients. Indian J Anaesth. 2011;55:488–493. doi: 10.4103/0019-5049.89880. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Chong DY, Greenland KB, Tan ST, Irwin MG, Hung CT. The clinical implication of the vocal cords-carina distance in anaesthetized Chinese adults during orotracheal intubation. Br J Anaesth. 2006;97:489–495. doi: 10.1093/bja/ael186. [DOI] [PubMed] [Google Scholar]
- 13.Eagle CC. The relationship between a person's height and appropriate endotracheal tube length. Anaesth Intensive Care. 1992;20:156–160. doi: 10.1177/0310057X9202000206. [DOI] [PubMed] [Google Scholar]
- 14.Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1(8476):307–310. [PubMed] [Google Scholar]
- 15.Bland M. How can I decide the sample size for a study of agreement between two methods of measurement? Available at: https://www-users.york.ac.uk/∼mb55/meas/sizemeth.htm Accessed January 11, 2018.
- 16.Techanivate A, Rodanant O, Charoenraj P, Kumwilaisak K. Depth of endotracheal tubes in Thai adult patients. J Med Assoc Thai. 2005;88:775–781. [PubMed] [Google Scholar]
- 17.Ahmed-Nusrath A, Tong JL, Smith JE. Pathways through the nose for nasal intubation: a comparison of three endotracheal tubes. Br J Anaesth. 2008;100:269–274. doi: 10.1093/bja/aem350. [DOI] [PubMed] [Google Scholar]