

Abstract
Introduction:
Factors that occur between consecutive pregnancies may influence repeated excessive gestational weight gain (GWG) and infants born large-for-gestational age (LGA). We examined inter-pregnancy interval, weight retention, and GWG in women’s 1st pregnancy as predictors of excessive GWG and LGA in women’s 2nd pregnancy.
Study Design:
We used data from women’s first 2 live births during the First Baby Study, a 3-year prospective observational cohort of first-time mothers (N=549). GWG was calculated as weight at delivery minus pre-pregnancy weight for 1st and 2nd pregnancies and categorized using the Institute of Medicine guidelines. Weight retention at 6 and 12 months and inter-pregnancy interval (time from 1st live birth to conception of 2nd infant) were quantified. Infants were considered LGA if birthweight was ≥90th percentile for gestational age.
Results:
Many (51.7%) women exceeded GWG recommendations in both pregnancies. Women who exceeded guidelines in their 1st pregnancy had 5.08 (p<0.01) greater odds for exceeding guidelines in their 2nd pregnancy, compared to women who did not exceed guidelines in their 1st pregnancy. Inter-pregnancy interval and weight retention had no association with exceeding guidelines in women’s 2nd pregnancy. Exceeding guidelines in women’s 1st pregnancy resulted in 4.48 (p<0.01) greater odds of first-born infants being LGA, while exceeding guidelines in women’s 2nd pregnancy resulted in 1.82 greater odds of second-born infants being LGA (p=0.02), compared to women who met guidelines in their 1st or 2nd pregnancy, respectively.
Conclusions:
Exceeding GWG guidelines in women’s 1st pregnancy predicted exceeding guidelines in their 2nd pregnancy, independent of inter-pregnancy-interval and weight retention.
Keywords: infant, IOM gestational weight gain guidelines, large-for-gestational age, multiparous, postpartum weight retention
INTRODUCTION
Excessive gestational weight gain (GWG) during pregnancy is associated with an increased risk of adverse health outcomes for both mothers and their offspring, such as gestational diabetes, hypertension, postpartum weight retention (PPWR), and infants born large-for-gestational age (LGA) (Siega-Riz et al., 2009; Viswanathan et al., 2008). As such, the Institute of Medicine (IOM) established guidelines for GWG based on women’s pre-pregnancy body mass index (BMI) (Rasmussen & Yaktine, 2009). The Centers for Disease Control and Prevention reported that among women, 39% with normal weight, 59% with overweight, and 56% with obesity exceed these GWG recommendations in the US (Dalenius, Brindley, Smith, Reinold, & Grummer-Strawn, 2012). For women, excessive GWG, coupled with associated PPWR across multiple pregnancies, can lead to accumulated weight gain during childbearing years and set the stage for life-long obesity development in adulthood (Rooney, Schauerger, & Mathiason, 2005; Linne, Dye, Barkeling, & Rössner, 2003). For offspring, excess GWG can have long-term metabolic health implications through fetal programing, including an increased risk for childhood obesity (Patti, 2013). Infant birth weight has been associated with the prenatal environment, and it is a predictor for future health outcomes (Boney, Verma, Tucker, & Vohr, 2005); therefore, this outcome can be used to further understand how repeated excessive GWG impacts women’s offspring.
When examining GWG guidelines, the IOM committee recommended additional research to better understand how maternal characteristics, such as parity, influence GWG (Rasmussen & Yaktine, 2009). Two previous studies have characterized GWG across women’s subsequent pregnancies, finding that women with excessive GWG in one pregnancy had increased odds of excessive GWG in the following pregnancy (Waring, Moore Simas, & Liao, 2013; Chin et al., 2010). Yet, factors that occur between pregnancies have rarely been considered. For example, a longer inter-pregnancy interval (i.e., period between the end of one pregnancy and the beginning of the next) may allow women more time to lose weight gained from their first pregnancy, thus reducing the possibility of weight carried forward into the second pregnancy, and consequently excessive GWG and larger infant birth weight in their second pregnancy. Specifically, how these inter-pregnancy factors influence excessive GWG and infant birth weight across women’s subsequent pregnancies remains unknown, largely owing to the need for longitudinal data to prospectively examine these temporal relationships.
Using data from the First Baby Study (Kjerulff et al., 2013), we examined patterns of GWG and LGA across multiparous women’s 1st and 2nd pregnancies and tested predictors (e.g. GWG in 1st pregnancy, PPWR, inter-pregnancy interval) for exceeding GWG guidelines in women’s 2nd pregnancy. We hypothesized that exceeding GWG in women’s 1st pregnancy (GWG1st) and PPWR would be positively associated with exceeding GWG in women’s 2nd pregnancy (GWG2nd), whereas inter-pregnancy interval would be negatively associated with GWG2nd (Davis et al., 2014). Further, we hypothesized women who exceeded guidelines for both GWG1st and GWG2nd would have greater odds of LGA in second-born infants than women who exceeded GWG in neither or only one pregnancy.
METHODS
Study design
The First Baby Study was a 3-year longitudinal, prospective cohort study. Enrolled participants delivered their first child between January 2009 and April 2011. The primary purpose of the study was to investigate the association between mode of first delivery and subsequent childbearing (Kjerulff et al., 2013). In-depth telephone interviews occurred during women’s third trimester (baseline) and at 1, 6, 12, 18, 24, 30, and 36 months postpartum. Birth certificate and hospital discharge data were obtained for participant’s first birth, and birth certificate data were obtained for subsequent births that occurred during the 3-year study duration.
Participants
Women were eligible to participate in the First Baby Study if they were: 1) 18-35 years of age, 2) first-time mothers with a singleton pregnancy, 3) fluent in English or Spanish, and 4) residing in Pennsylvania and planning to deliver in a Pennsylvania hospital. Women were excluded if they: 1) planned for their infant to be adopted, 2) had a previous stillbirth at >20 weeks gestation, 3) planned to have a tubal ligation while hospitalized for delivery, 4) did not have a telephone, and 5) could not commit to the 3-year study duration. Women were recruited from childbirth education classes, hospital tours, obstetrician offices, low-income clinics, and a variety of community venues. Prior to enrollment, all participants signed an informed consent approved by the Penn State College of Medicine Institutional Review Board and the participating hospitals located throughout Pennsylvania.
Of the 3,006 women in the First Baby Study, we used data for women with ≥2 pregnancies that resulted in live births during the 3-year study duration (n=942). For women who had >2 pregnancies, we used data only on their first and second pregnancy that resulted in live births. If a woman’s first or second pregnancy resulted in multiple births (e.g. twins, triplets) or a miscarriage/abortion/stillbirth, this pregnancy was not considered and instead, the subsequent pregnancy resulting in a live birth was used. We did not include women with underweight (BMI <18.5m/kg2) (n=43) or who gained less than the IOM recommendations for appropriate weight gain during pregnancy (n=176) (Rasmussen & Yaktine, 2009). Participants whose first or second infant was born prematurely (<37 weeks gestation; n=60) were also excluded. The final subsample of women who met these inclusion criteria and had complete data on GWG and infant birth weight in both pregnancies was N=549.
Measures
The majority of measures were self-reported by the mother, via telephone surveys conducted by trained researchers employed by the Penn State Harrisburg Center for Survey Research. Demographic information, such as race, ethnicity, education, marital status, and weight prior to women’s first pregnancy, were collected at baseline. Weight prior to women’s second pregnancy was reported during the postpartum survey immediately following conception of their second-born infant. Women’s weight at each delivery and birth weight for first- and second-born infants were obtained from the birth certificate data. To maximize all available data, when women’s delivery weight was missing from the birth certificate data, we used self-reported weight at delivery from their telephone survey. GWG was calculated as weight at delivery minus pre-pregnancy weight for both pregnancies. Women were categorized as meeting or exceeding IOM GWG guidelines based on pre-pregnancy BMI status (Rasmussen & Yaktine, 2009). Infants were classified as LGA if birth weight was ≥90th percentile for gestational age according to sex-specific percentiles based on a U.S. national data (Oken, Kleinman, Rich-Edwards, & Gillman, 2003).
Body mass index
Women’s BMI prior to their first pregnancy (BMI1st) was calculated using self-reported pre-pregnancy height and weight obtained at baseline (Shin, Chung, Weatherspoon, & Song, 2014). Women’s BMI prior to their second pregnancy (BMI2nd) was calculated using self-reported height from baseline and pre-pregnancy weight obtained from the postpartum survey completed immediately following conception of their second-born infant. These BMI values were used to classify women as having normal weight (BMI 18.5-24.9 kg/m2), having overweight (BMI 25-29.9 kg/m2), and having obesity (BMI >30 kg/m2). Meeting versus exceeding GWG guidelines for each pregnancy were based on BMI prior to that specific pregnancy.
Postpartum weight retention
PPWR was calculated as weight at 6 and 12 months following the birth of women’s first infant minus pre-pregnancy weight. Any weight >0lbs was considered PPWR (Hill, McPhie, & Skouteris, 2016; Ronnberg, Hanson, Ostlund, & Nilsson, 2016) and was treated as a continuous variable. Women who were pregnant again by 5 (n=9) or 11 months (n=115) postpartum were excluded only from analyses on PPWR at 6 and 12 months, respectively.
Inter-pregnancy interval
Inter-pregnancy interval was calculated as the number of months between the birth of the first infant and the conception date of the second infant. The conception date for the second infant was the self-reported date of the woman’s last menses. Inter-pregnancy interval was calculated between consecutive live births.
Statistical analysis
Descriptive statistics on demographic variables are reported. Chi-square analyses explored the associations between categorical variables, such as meeting versus exceeding GWG recommendations and pre-pregnancy BMI status. Logistic regression models were used to test our first hypothesis on associations of GWG1st, PPWR, and inter-pregnancy interval on GWG2nd and our second hypothesis of GWG on LGA in first- and second-born infants. Odds ratios (OR) were considered significant if the 95% confidence intervals (CI) did not include 1.0. All analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC). Statistical significance was defined a priori as p<0.05.
Covariates
Based on prior research, maternal age, BMI1st, race, ethnicity, education, marital status, pregnancy loss during the inter-pregnancy interval, and smoking during women’s first pregnancy (assumed to be time-invariant) (Rasmussen & Yaktine, 2009; Hall, Venkatesh, & Greenberg, 2016) were tested as independent predictors of GWG2nd. Only BMI1st was associated with GWG2nd (p<0.01) and therefore included as a covariate in analyses of GWG2nd. Similarly, based on prior research, maternal age, race, ethnicity, education, marital status, pregnancy loss during the inter-pregnancy interval, and smoking during women’s first pregnancy at birth were tested for independent associations with infant birth weight. Maternal ethnicity, education, and smoking during first pregnancy were associated with infant birth weight (p<0.05) and therefore included as covariates in analyses of infant birth weight. Pregnancy loss was tested as a predictor of inter-pregnancy interval and PPWR at 6 and 12 months. Among these, pregnancy loss was associated with PPWR at 12 months (p=0.04), and therefore was included as a covariate in models containing PPWR at 12 months.
RESULTS
Maternal Weight During and Between Pregnancies
Among our sample, >90% were White, married, and college-educated (Table 1). Of women with a normal BMI1st, 13.6% had overweight and 0.3% had obesity, according to BMI2nd. Of women with an overweight BMI1st, 11.7% had normal weight and 14.9% had obesity, according to BMI2nd. Of women with an obese BMI1st, none had normal weight and 5.3% had overweight, according to BMI2nd. Of women with a normal BMI1st, 47.8% met GWG guidelines for their 1st pregnancy, while 14.9% of women with overweight and 18.1% of women with obesity met GWG guidelines for their 1st pregnancy (p<0.01). Of women with a normal BMI2nd, 51.6% met GWG guidelines for their 2nd pregnancy, while 21.4% of women with overweight and 20.4% of women with obesity met GWG guidelines for their 2nd pregnancy (p<0.01). The majority of women (56.5%) retained weight at 6 months postpartum, while 39.6% retained weight at 12 months. Of women who retained weight, average PPWR was 11.1±11.2 lbs (mean±SD) at 6 months and 10.8±10.1 lbs at 12 months. PPWR at 6 and 12 months did not vary by BMI1st. Women who exceeded guidelines for GWG1st had greater PPWR at 6 and 12 months (6.0±13.8 lbs and 1.0±12.9 lbs, respectively), compared to PPWR for women who met guidelines for GWG1st (−1.1±8.9 and −2.9±10.5 lbs, respectively). The average inter-pregnancy interval was 16.3±5.8 months and did not vary by BMI1st or GWG1st.
Table 1.
Demographics of mother and infant participants (N=549)
| Mother Demographics | First pregnancy | Second pregnancy |
|---|---|---|
| Age at enrollment (years) | 28.5±3.3 | |
| Pre-pregnancy BMI (kg/m2) | 25.7±5.1 | 26.2±5.6 |
| Normal weight (%) | 54.8 | 50.5 |
| Overweight (%) | 28.1 | 29.0 |
| Obese (%) | 17.1 | 20.6 |
| Race/ethnicity (%) | ||
| White | 95.8 | |
| African American | 1.6 | |
| Other | 2.6 | |
| Non-Hispanic | 97.5 | |
| Education (%) | ||
| High school degree or less | 6.2 | |
| Some college/technical school | 18.2 | |
| College degree or higher | 75.6 | |
| Marital status (%) | ||
| Married | 94.9 | |
| Not married | 5.1 | |
| Smoked during pregnancy (%) | 4.0 | |
| GWG (lbs) by BMI category | 37.8±11.9 | 34.8±10.6 |
| Normal weight | 38.6±9.9 | 36.5±8.4 |
| Overweight | 38.9±14.3 | 35.1±11.5 |
| Obese | 33.2±12.2 | 30.2±12.5 |
| IOM GWG guidelines (%) | ||
| Met guidelines | 33.5 | 36.4 |
| Exceeded guidelines | 66.5 | 63.6 |
| Infant demographics | First born | Second born |
| Gestational age at birth (weeks) | 39.4±1.1 | 39.2±1.0 |
| Birth weight (g) | 3511.4±440.2 | 3628.0±422.2 |
| <2500 (low) (%) | 0.7 | 0.4 |
| 2500-4000 (normal) (%) | 84.5 | 79.4 |
| >4000 (high) (%) | 14.8 | 20.0 |
| Large-for-gestational age (%) | 10.8 | 17.7 |
| Male sex (%) | 53.9 | 51.3 |
Data is presented as mean±SD or as % when noted. Body mass index (BMI); Gestational weight gain (GWG); Institute of Medicine (IOM)
Gestational weight gain in women’s first versus second pregnancies
On average, GWG1st was greater than GWG2nd (p<0.01, Table 1). Of the women who met guidelines for GWG1st, 78.3% had normal weight; of the women who exceeded guidelines for GWG1st, 35.9% had overweight and 21.1% had obesity. Of the women who met guidelines for GWG2nd, 71.5% had normal weight; of the women who exceeded guidelines for GWG2nd, 35.8% had overweight and 25.8% had obesity. Almost half of the women exceeded GWG guidelines in both pregnancies (51.7%), while only 21.7% of the women met GWG guidelines in both pregnancies (Figure 1). Of the women who exceeded GWG guidelines in just one pregnancy, more exceeded guidelines for GWG1st compared to GWG2nd (14.8% vs. 11.8%, respectively; Figure 1).
Figure 1.
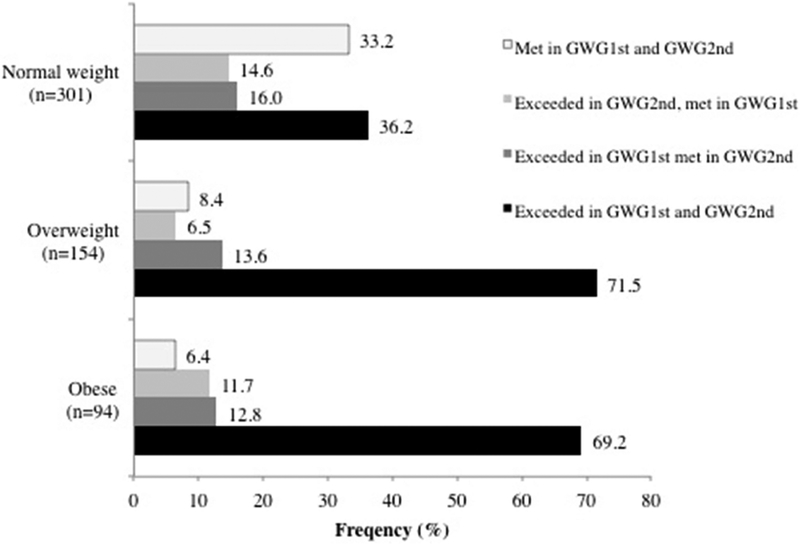
Differences in the frequency of exceeded versus met guidelines for GWG1st and GWG2nd, categorized by body mass index prior to first pregnancy. Normal weight: p<0.01; Overweight: p<0.01; Obese: p=0.06. Criteria for exceeded vs. met guidelines based on body mass index prior to each respective pregnancy. Gestational weight gain in first pregnancy (GWG1st); Gestational weight gain in second pregnancy (GWG2nd). N=549.
Predictors of exceeding GWG in women’s second pregnancy
The independent associations of GWG1st, PPWR, and inter-pregnancy interval on GWG2nd are as follows. Women who exceeded guidelines for GWG1st had 5.08 greater odds (95% CI: 3.38 – 7.62, p<0.01) of exceeding guidelines for GWG2nd, compared to women who met guidelines for GWG1st. PPWR at 6 and 12 months was not associated with GWG2nd (OR: 1.02; 95% CI: 1.00 – 1.03, p=0.04; OR: 0.99; 95% CI: 0.98 – 1.01, p=0.54; respectively). Inter-pregnancy interval did not predict exceeding guidelines for GWG2nd (OR: 1.01; 95% CI: 0.98 – 1.04, p=0.52). The combined associations of exceeding guidelines for GWG1st, PPWR at 6 months, and inter-pregnancy interval on exceeding guidelines for GWG2nd (Table 2) indicate GWG1st was the only significant predictor of exceeding guidelines for GWG2nd (p<0.01).
Table 2.
Predictors for exceeding guidelines in GWG2nd (n=529)
| Exceeding guidelines in GWG2nd |
|||
|---|---|---|---|
| Odds ratio | 95% CI | p value | |
| Exceeding guidelines in GWG1st | 5.42 | 3.49 – 8.42 | <0.01 |
| Postpartum weight retention at 6 months | 1.00 | 0.98 – 1.01 | 0.68 |
| Inter-pregnancy interval | 1.00 | 0.97 – 1.04 | 0.90 |
Gestational weight gain in 1st pregnancy (GWG1st); Gestational weight gain in 2nd pregnancy (GWG2nd); Confidence interval (CI). Predictors tested in a single model and adjusted for pre-pregnancy body mass index. Odds ratios compared to women who met guidelines in GWG2nd
Birth weight for first and second born infants
There was a no association between BMI1st and odds of first-born infants being LGA (p>0.05). For BMI2nd, women with obesity had 2.65 (CI: 1.53 – 4.61, p<0.01) greater odds of second-born infants being LGA, compared to women with normal weight. There was no difference between normal versus overweight BMI2nd on LGA for second-born infants (p=0.87). Women who exceeded guidelines for GWG1st had 4.48 (CI: 1.99 – 10.10, p<0.01) greater odds of first-born infants being LGA, compared to women who met guidelines. Similarly, women who exceeded guidelines for GWG2nd had 1.82 (CI: 1.11 – 2.99, p=0.02) greater odds of second-born infants being LGA, compared to women who met guidelines. Women who exceeded GWG guidelines in both pregnancies had 2.81 (CI: 1.42 - 5.57, p=0.03) greater odds of second-born infants being born LGA, compared to women who met GWG guidelines in both pregnancies, and 1.37 (CI: 0.67 - 2.81, p=0.03) greater odds of second-born infants being LGA, compared to women who exceeded guidelines in their second pregnancy only. The associations of GWG and pre-pregnancy BMI, when tested in the same model, on first and second-born infants born LGA are listed in Table 3. PPWR at 6 months and inter-pregnancy interval were not associated with second-born infants being LGA (p>0.05).
Table 3.
Pre-pregnancy BMI and GWG as predictors of infant LGA at birth
| LGA age at birth |
||||||
|---|---|---|---|---|---|---|
| First born infants (n=549) | Second born infants (n=544) | |||||
| Odds ratio | CI | p value | Odds ratio | CI | p value | |
| Overweight BMI* | 1.54 | 0.81 – 2.94 | 0.52 | 1.38 | 0.79 – 2.42 | 0.69 |
| Obese BMI* | 1.62 | 0.76 – 3.46 | 0.44 | 2.35 | 1.32 – 4.16 | 0.01 |
| Exceeded GWG guideliines | 3.77 | 1.62 – 8.77 | <0.01 | 1.51 | 0.90 – 2.55 | 0.12 |
Pre-pregnancy body mass index (BMI); Gestational weight gain (GWG); Large-for-gestational age (LGA);
Normal weight BMI was used as the reference group. BMI and GWG from first and second pregnancies were used for first and second-born infant analyses, respectively. Analyses were adjusted for the following covariates: maternal ethnicity, education, and smoking during first pregnancy.
DISCUSSION
This secondary data analysis revealed a majority of women exceeded GWG guidelines across both their first and second pregnancies (51.7%). Specifically, women who exceeded GWG guidelines in their first pregnancy tended to exceed GWG guidelines in their second pregnancy, independent of inter-pregnancy interval and PPWR. Exceeding GWG guidelines in both pregnancies was associated with greater odds for LGA in second-born infants, compared to women who met GWG guidelines in both pregnancies. These longitudinal, prospective data support the current literature and advance our understanding of GWG by parity in revealing that, independent of PPWR and inter-pregnancy interval, excessive GWG is a strong predictor for persistent, increased maternal and infant weight outcomes across multiple pregnancies.
In partial support of our hypothesis, women with excessive GWG in their first pregnancy had 5.42 greater odds of excessive GWG in their second pregnancy, while inter-pregnancy interval and PPWR at 6 months had no association on excessive GWG in women’s second pregnancy. These findings are consistent with similar research that found adjusted odds ratios ranging 2.6 – 5.4 for women exceeding GWG in a given pregnancy on exceeding GWG in a subsequent pregnancy (Waring et al., 2013; Chin et al., 2010). Together these findings support prenatal care and interventions that emphasize appropriate GWG, specifically for primiparous mothers. Providing first-time mothers with the knowledge and resources needed to achieve appropriate GWG can set a foundation for subsequent healthy weight gain trajectories and positive long-term weight outcomes for both mother and child. Healthy behavior changes made during interventions that target primiparous mothers should be tested for positive, carry-over effects during later pregnancies. Further, our results suggest that among multiparous women, prenatal counseling should strongly consider GWG from a woman’s previous pregnancy to inform tailored guidance. For example, women who exceeded GWG guidelines in their first pregnancy may need more intensive strategies to help them achieve GWG in their next pregnancy. Novel methodology, such as adaptive, time-varying interventions (Dong et al., 2012; Savage, Downs, Dong, & Rivera, 2014) provide a framework in which future GWG interventions can be tailored based on factors from a women’s first pregnancy.
Previous research shows the parity-GWG relationship as directionally inconsistent (Hill et al., 2017). Therefore, we explored patterns of GWG and characteristics of the inter-pregnancy interval to further understand this relationship. For example, we quantified women whose pre-pregnancy BMI category changed from before their first to before their second pregnancy, as this would indicate different GWG recommendations for each pregnancy. Only 16% of women had pre-pregnancy BMI categories that differed, with the majority going from having normal weight to having overweight. This is similar to findings by Waring et al. (2013), in that most women have a consistent pre-pregnancy BMI category and therefore consistent GWG recommendation for both pregnancies. Further, the majority of women who did change pre-pregnancy BMI categories (73%) either met GWG guidelines in both pregnancies or exceeded guidelines in both pregnancies. This suggests that a change in pre-pregnancy BMI category for subsequent pregnancies did not largely impact meeting GWG guidelines in one pregnancy but exceeding guidelines in the other. Rather, behavioral changes during the postpartum period that impact lifestyle factors may have established new habits that contributed to a greater GWG in their second pregnancy. For example, reduced exercise (Brown, Heesch, & Miller, 2009), time constraints in caring for their first-born infant that lead to changes in eating behaviors (Carter-Edwards et al., 2009), and/or increased stress (Whitaker, Young-Hyman, Vernon, & Wilcox, 2015) during the postpartum time period may contribute to a greater GWG in women’s second pregnancy, yet very little research has examined these factors in the context of a subsequent pregnancy.
We originally hypothesized a longer inter-pregnancy interval would increase women’s time for losing weight gained from the previous pregnancy, and therefore be negatively associated with subsequent GWG. We found a positive association between exceeding guidelines for GWG1st and PPWR. There was no association between PPWR at 6 and 12 months on exceeding guidelines for GWG2nd. The average weight retained in our sample may explain these findings, in addition to the lack of association for inter-pregnancy interval on subsequent GWG. The average PPWR provided marginal potential for this association; yet, there was large variability in PPWR, suggesting that future research examine this association among women with a greater likelihood for substantial PPWR (e.g. women who are younger, African American, Hispanic, and have lower incomes or less education) (Endres et al., 2015). Women in our sample were predominately White, non-Hispanic, and college educated, thus limiting the heterogeneity of our sample and generalizability of our findings. Further, we used self-reported weight data to calculate GWG and PPWR, which is practical and cost efficient for this large sample size, yet subject to recall and response bias (Gorber, Tremblay, Moher, & Gorber, 2007). Given this was a prospective observational study, we are not able to infer causality. As a solution, future research should consider using propensity scores on observational data of larger samples sizes (Austin, 2011).
Previous research has shown a positive association between exceeding GWG guidelines and infants born LGA, yet is limited to examining this association within a single pregnancy (Zhao, Xu, Wu, Huang, & Cao, 2017; Goldstein et al., 2017). Our findings show that women who exceeded GWG guidelines in both their first and second pregnancy did not have greater odds of their second-born infant being LGA, compared to women who exceeded GWG guidelines in their second pregnancy only. Based on these observational data, the influence of GWG on infant birth weight seems to occur within a single pregnancy (i.e., second pregnancy GWG on second-born infant birth weight), rather than a cumulative effect across multiple pregnancies (i.e., first and second pregnancy GWG on second-born infant birth weight). Among women who exceed GWG guidelines in their first pregnancy, future research should test if meeting GWG guidelines in their second pregnancy decreases the odds of LGA for their second-born infant. Interventions and prenatal counseling among women who exceeded GWG guidelines in their first pregnancy should encourage the adoption of healthy behaviors postpartum and during their second pregnancy, to meet GWG guidelines in their second pregnancy. This may increase the potential for a healthy birth weight among second-born infants, and establish the foundation for a healthy weight gain trajectory into early childhood (Salahuddin, Pérez, Ranjit, Hoelscher, & Kelder, 2017).
IMPLICATIONS FOR PRACTICE AND/OR POLICY
Our findings have implications for clinical practice as they emphasize the need for prenatal counseling and clinical interventions to promote behavioral strategies to help women meet GWG guidelines, beginning in their first pregnancy. This guidance can help to prevent repeated excess weight gain and possible weight accumulation across subsequent pregnancies. In our sample, postpartum weight retention and inter-pregnancy interval had no association with exceeding GWG in women’s second pregnancy. Instead, postnatal and prenatal counseling for women’s second pregnancy should consider women’s weight gain from their first pregnancy. Further, the association between exceeding GWG guidelines and increased odds of infants born LGA was evident in women’s first, but not second, pregnancy, thus supporting the need for emphasized guidance during women’s first pregnancy to improve the health of their first-born infant.
CONCLUSION
This secondary data analysis provides novel insight on patterns and predictors of GWG and infant birth weight, using a large, prospective cohort of first time mothers at enrollment. Meeting GWG guidelines in women’s first pregnancy provided optimal mother and infant weight outcomes and established a healthy weight trajectory for future pregnancies, independent of their inter-pregnancy interval and PPWR. These findings provide a better understanding of weight-related factors across subsequent pregnancies that can be used to tailor prenatal counseling by medical professionals and intervention development for multiparous women.
Acknowledgments
Funding statement: This project is funded, in part, under a grant with the Pennsylvania Department of Health using Tobacco CURE funds. The Department specifically disclaims responsibility for any analyses, interpretations or conclusions. The First Baby Study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institutes of Health, grant R01 HD052990.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
REFERENCES
- 1.Austin PC (2011). An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behavioral Research, 46, 399–424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Boney CM, Verma A, Tucker R, & Vohr BR (2005). Metabolic syndrome in childhood: associations with birth weight, maternal obesity, and gestational diabetes mellitus. Pediatrics, 115, e290–296. [DOI] [PubMed] [Google Scholar]
- 3.Brown WJ, Heesch KC, & Miller YD (2009). Life events and changing physical activity patterns in women at different life stages. Annals of Behavioral Medicine, 37, 294–305. [DOI] [PubMed] [Google Scholar]
- 4.Carter-Edwards L, Østbye T, Bastian LA, Yarnall KSH, Krause KM, & Simmons TJ (2009). Barriers to adopting a healthy lifestyle: insight from postpartum women. BMC Research Notes, 2, 161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Chin JR, Krause KM, Ostbye T, Chowdury N, Lovelady CA, & Swamy GK (2010). Gestational weight gain in consecutive pregnancies. American Journal of Obstetrics & Gynecology, 203, 279.e1–6. [DOI] [PubMed] [Google Scholar]
- 6.Dalenius K, Brindley P, Smith B, Reinold C, & Grummer-Strawn L (2012). Pregnancy nutrition surveillance 2010 report U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; Atlanta, GA. [Google Scholar]
- 7.Davis EM, Babineau DC, Wang X, Zyzanski S, Abrams B, Bodnar L, & Horwitz R (2014). Short inter-pregnancy intervals, parity, excessive pregnancy weight gain and risk of maternal obesity. Maternal and Child Health, 18, 3, 554–562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Dong Y, Rivera DE, Thomas DM, Navarro-Barrientos JE, Downs DS, Savage JS, & Collins LM (2012). A dynamical systems model for improving gestational weight gain behavioral interventions. Proceedings of the American Control Conference, 4059–4064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Endres LK, Straub H, McKinney C, Plunkett B, Minkovitz CS, Schetter CD, … Shalowitz MU (2015). Postpartum weight retention risk factors and relationship to obesity at one year. Obstetrics & Gynecology, 125, 144–152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Goldstein RF, Abell SK, Ranasinha S, Misso M, Boyle JA, Black JA, … . Teede HJ (2017). Association of gestational weight gain with maternal and infant outcomes: a systematic review and meta-analysis. Journal of the American Medical Association, 17, 2207–2225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Gorber SC, Tremblay M, Moher D, & Gorber B (2007). A comparison of direct vs. self-report measures for assessing height, weight and body mass index: a systematic review. Obesity Reviews, 8, 307–326. [DOI] [PubMed] [Google Scholar]
- 12.Hall ES, Venkatesh M, & Greenberg JM (2016). A population study of first and subsequent pregnancy smoking behaviors in Ohio. Journal of Perinatology, 36, 948–953. [DOI] [PubMed] [Google Scholar]
- 13.Hill B, McPhie S, & Skouteris H (2016). The role of parity in gestational weight gain and postpartum weight retention. Women’s Health Issues, 26, 123–129. [DOI] [PubMed] [Google Scholar]
- 14.Hill B, Bergmeier H, McPhie S, Fuller-Tyszkiewicz M, Teede H, Forster D, … Skouteris H (2017). Is parity a risk factor for excessive weight gain during pregnancy and postpartum weight retention? A systematic review and meta-analysis. Obesity Reviews, 18, 755–764. [DOI] [PubMed] [Google Scholar]
- 15.Kjerulff KH, Velott DL, Zhu J, Chuang CH, Hillemeier MM, Paul IM, & Repke JT (2013). Mode of first delivery and women’s intentions for subsequent childbearing: findings from the First Baby Study. Paediatric and Perinatal Epidemiology, 27, 62–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Linne Y, Dye L, Barkeling B, & Rössner S (2003). Weight development over time in parous women: the SPAWN study–15 years follow-up. International Journal of Obesity and Related Metabolic Disorders, 27, 1516–1522. [DOI] [PubMed] [Google Scholar]
- 17.Oken E, Kleinman KP, Rich-Edwards J, Gillman MW. (2003). A nearly continuous measure of birth weight for gestational age using a United States national reference. BMC Pediatrics, 3, 6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Patti ME (2013). Intergenerational programming of metabolic disease: evidence from human populations and experimental animal models. Cellular and Molecular Life Sciences, 70, 1597–1608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Rasmussen KM, & Yaktine AL (2009). Committee to Reexamine IOM Pregnancy Weight Guidelines; Institute of Medicine; National Research Council Weight Gain During Pregnancy: Reexamining the Guidelines. National Academies Press: Washington, DC. [PubMed] [Google Scholar]
- 20.Ronnberg A, Hanson U, Ostlund I, & Nilsson K (2016). Effects on postpartum weight retention after antenatal lifestyle intervention – a secondary analysis of a randomized controlled trial. Acta Obstetricia et Gynecologica Scandinavica, 95, 999–1007. [DOI] [PubMed] [Google Scholar]
- 21.Rooney BL, Schauberger CW, & Mathiason MA (2005). Impact of perinatal weight change on long-term obesity and obesity-related illnesses. Obstetrics & Gynecology, 106, 1349–1356. [DOI] [PubMed] [Google Scholar]
- 22.Salahuddin M, Pérez A, Ranjit N, Hoelscher DM, & Kelder SH (2017). The association of large-for-gestational-age and infant feeding practices with children’s body mass index z-score trajectories: the Early Childhood Longitudinal Study, Birth Cohort. Clinical Obesity, 7, 307–315. [DOI] [PubMed] [Google Scholar]
- 23.Savage JS, Downs DS, Dong Y, & Rivera DE (2014). Control systems engineering for optimizing a prenatal weight gain intervention to regulate infant birth weight. American Journal of Public Health, 104, 1247–1254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Shin D, Chung H, Weatherspoon L, & Song WO (2014). Validity of Prepregnancy weight status estimated from self-reported height and weight. Maternal and Child Health Journal, 18, 1667–1674. [DOI] [PubMed] [Google Scholar]
- 25.Siega-Riz AM, Viswanathan M, Moos MK, Deierlein A, Mumford S, Knaack J, … Lohr KN (2009). A systematic review of outcomes of maternal weight gain according to the Institute of Medicine recommendations: birthweight, fetal growth, and postpartum weight retention. American Journal of Obstetrics and Gynecology, 201, e1–14. [DOI] [PubMed] [Google Scholar]
- 26.Viswanathan M, Siega-Riz AM, Moos MK, Deierlein A, Mumford S, Knaack J, … Lohr KN (2008). Outcomes of maternal weigh gain. Evidence Report/Technology Assessment (Full Report), 168, 1–223. [PMC free article] [PubMed] [Google Scholar]
- 27.Waring ME, Moore Simas TA, & Liao X (2013). Gestational weight gain within recommended ranges in consecutive pregnancies: A retrospective cohort study. Midwifery, 29, 550–556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Whitaker K, Young-Hyman D, Vernon M, & Wilcox S (2015). Maternal stress predicts postpartum weight retention. Maternal and Child Health Journal, 18, 2209–2217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Zhao R, Xu L, Wu ML, Huang SH, & Cao XJ (2017). Maternal pre-pregnancy body mass index, gestational weight gain influence birth weight. Women and Birth, 31, e20–e25. [DOI] [PubMed] [Google Scholar]