

Abstract
Objective
To evaluate the functional outcome of the remplissage technique, the healing of the capsulotenodesis of the infraspinatus tendon in Hill-Sachs lesion, and the degree of fatty infiltration of the infraspinatus muscle and its postoperative strength.
Methods
Twenty-five patients with recurrent anterior dislocation of the shoulder and Hill-Sachs lesion with a Hardy index > 20% who underwent the remplissage arthroscopic technique were evaluated with a minimum follow-up of 1 year. Patients underwent a clinical evaluation (Carter-Rowe and Walch-Duplay functional scores, measurement of range of motion and strength) and a magnetic resonance imaging (MRI) exam on the operated shoulder.
Results
Eighty-eight percent and 92% of the patients had good or excellent scores in the functional assessments of the Carter-Rowe and Walch-Duplay scores, respectively. A mean difference of - 1 kg in the strength of the operated limb was observed when compared with the contralateral limb ( p < 0.001), as well as a mean difference of 10° in external rotation 1 and 2 ( p < 0.001), also compared with the contralateral side. All of the patients who underwent an MRI exam presented high-grade filling of the Hill-Sachs lesion by capsulotenodesis, as well as absence of or minimal fatty infiltration in the infraspinatus muscle.
Conclusion
The remplissage technique had good/excellent functional score results, despite the discrete, albeit statistically significant, loss of strength and of external rotation amplitude. Successful capsulotenodesis healing and filling of the Hill-Sachs defect were demonstrated.
Keywords: shoulder, joint instability, recurrence, Bankart lesions, arthroscopy
Introduction
A posterosuperior lesion at the humeral head associated with glenohumeral dislocation was described by Hill et al in 1940 1 and, since then, it has gained increasing importance in the evaluation of anterior shoulder instability. Its 47% incidence after first dislocations can increase up to 84% in clinically recurring anterior dislocations, 2 3 and its participation in these lesions and in treatment failures after the isolated repair of an essential Bankart lesion is widely recognized.
Burkhart et al 4 described the term engaging Hill-Sachs for impaction fractures that, for their depth and orientation, allow their engagement at the glenoid border during abduction and external rotation (ER). Yamamoto et al 5 improved this concept through the glenoid track, which allowed, through a preoperative computed tomography (CT) scan, the evaluation of the risk of a Hill-Sachs lesion engaging at the glenoid border.
The relevance and the diagnosis of Hill-Sachs lesion evolved along with its therapeutic approach. In this context, Wolf et al 6 described an arthroscopic technique of lesion filling with the posterior capsule and the infraspinatus tendon to render it extra-articular and prevent engaging. This technique was called remplissage, a French term for filling.
The present study aims to:
Evaluate the functional outcome of the remplissage technique;
Evaluate the healing of the capsulotenodesis at the Hill-Sachs defect;
Evaluate the degree of fatty infiltration in the infraspinatus muscle in the postoperative period;
Evaluate the external rotation force of the shoulder in the postoperative period.
We hypothesized that the remplissage technique promotes a satisfactory healing of the posterior capsulotenodesis and provides excellent clinical results with no major repercussions on the range of motion of the shoulder and on the strength and quality of the infraspinatus muscle.
Material and Methods
Selection of the Patients
This was an analytical, retrospective study of individuals submitted to an arthroscopic repair surgery of the Bankart lesion associated with the remplissage technique for the treatment of anterior shoulder instability.
Between 2009 and 2015, 34 patients (34 shoulders) were submitted to an arthroscopic repair of anterior shoulder instability with the remplissage technique by surgeons from the Shoulder Group of the Hospital Ortopédico in Belo Horizonte, in the state of Minas Gerais, Brazil. From these patients, nine were not located or did not agree to participate in the present study. The minimum follow-up period was of 12 months, and the maximum follow-up period was of 84 months, with an average of 33.3 months. The mean age at the time of the procedure was 32.2 years old (ranging from 18 to 51 years old), and the dominant limb was approached in 60% of the cases. Regarding gender, 20% of the patients were female. The mean age at the first instability event was 24 ± 6 years old, and 88% of the patients had presented with at least one dislocation episode (requiring a medical reduction). In addition, 24% of the patients presented recurrent subdislocations. Among the patients able to inform the number of dislocation episodes, the average was two episodes before the procedure. The mean interval between the first instability event and the procedure was 5 years.
The enrolled patients presented with recurrent shoulder anterior dislocation of traumatic origin, and a Bankart lesion associated with a Hill-Sachs lesion evidenced by a magnetic resonance imaging (MRI) exam, with a minimum Hardy index of 20% in a CT scan. Patients with associated rotator cuff lesions, as well as with fractures at the humeral proximal third or with bony Bankart lesion > 20% and postsurgical follow-up period of < 1 year were excluded from the trial.
Surgical Technique
Under general anesthesia and brachial plexus block, the patient is placed in contralateral recumbency, with the trunk in a 30° posterior inclination, and the affected limb in 50° abduction and 15° anterior flexion, under 7 kg vertical axillary and fixed longitudinal traction. 7
The shoulder joint is accessed through the traditional posterior portal, 2 cm medial and 2 cm inferior to the posterolateral angle of the acromion. The visualization of the Hill-Sachs lesion requires the removal of the vertical traction and the increase of the longitudinal traction to open the space between the deltoid and the greater tubercle of the humerus. A percutaneous portal is created distally to the lateral border of the acromion and its location is determined with a puncture needle, positioning it in the central point of the Hill-Sachs lesion. The area is opened with a bone shaver blade without deepening the lesion. Next, one or two 5-mm anchors are positioned, according to the size of the bone defect ( Fig. 1 ). We use preferentially two anchors, one at the superomedial margin, and the other at the inferomedial aspect of the lesion, separated by a minimal distance of ∼ 1 cm. The anchors should not be positioned further than 2 cm apart from each other due to the risk of inferior involvement of the teres minor. 8 Sutures are passed through the posterior capsule and the infraspinatus tendon with a penetrator, the U-suture is prepared, and the repairs are left to be fixed at the end of the procedure ( Fig. 2 ). The anteroinferior and anterosuperior portals are prepared with the inside-out method, through the rotator interval, at the superior border of the subscapular tendon and at the anterior margin of the acromion adjacent to the bicipital long head tendon, respectively, and sustained by 8.5 mm cannulae. The arthroscope is then introduced from the posterior portal to the anterosuperior cannula, and a 7.5 mm cannula is introduced at the posterior portal for instrumentation.
Fig. 1.

Anchor positioning at Hill-Sachs lesion.
Fig. 2.

U-suture prepared for capsulotenodesis.
The standard repair of the Bankart lesion is performed with anchors at 1-, 3- and 5-hour positions for the right shoulder, or the equivalent of 7-, 9- and 11-hour for the left shoulder, which are introduced at the glenoid anterior border with a maximum joint medialization of 2 mm. Then, a capsulotenodesis is performed at the Hill-Sachs lesion, and the previously passed U-suture is fixed. The intra-articular view of the defect filling of the Hill-Sachs lesion is then obtained (indirect suture visualization) ( Fig. 3 ).
Fig. 3.
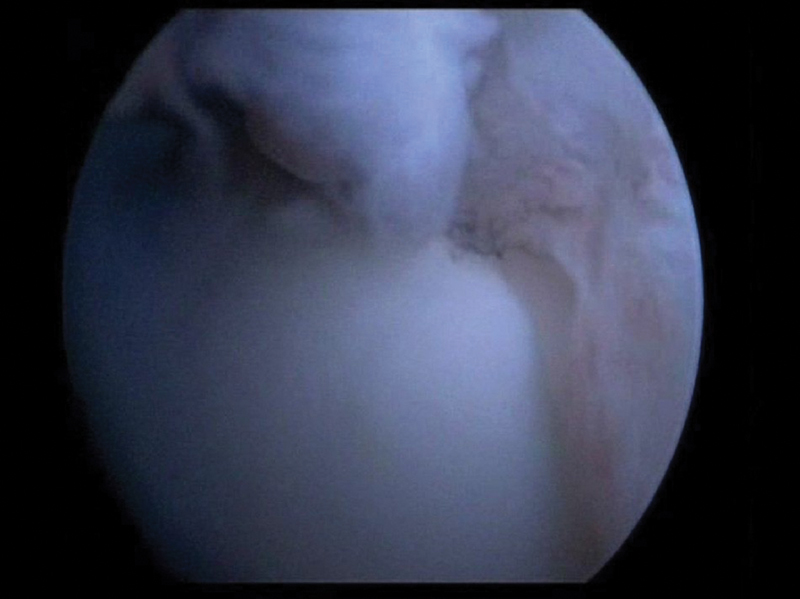
Intra-articular view of the filling of the Hill-Sachs lesion defect.
Postoperative Period
Immobilization with an abduction cushion device for 6 weeks to maintain neutral rotation avoids capsulotenodesis stress, releases active elbow, wrist and fingers flexion and extension from the first postoperative day, and allows pendulum shoulder movements from the 2 nd week on. Physical therapy rehabilitation starts, and it comprises three phases: the first one, for pain relief and passive and self-passive range of motion gain; in the second, isometric muscle strengthening of the rotator cuff begins; finally, the third phase consists of isotonic muscle strengthening. A progressive proprioception training is performed since the first phase.
Clinical and Functional Evaluation
The clinical evaluation consisted of questions aimed to determine the demographical and specific features of the clinical instability. The functional evaluation used the Carter-Rowe 9 and the Walch-Duplay scores, 10 considering criteria such as: stability, assessing apprehension, as well as subdislocation or the recurrence of dislocation; mobility, assessing the range of motion in anterior elevation and in external and medial rotation; and function, inquiring about work and/or sport limitations and pain. Using the predetermined protocol, 11 the ranges of motion were evaluated with a goniometer, and the ER force with the elbow flexed at 90 degrees and the arm in a neutral position was assessed with a simple kitchen scale.
Postoperative Image Evaluation
Filling Index Score of Remplissage and Goutallier Evaluation
At the end of the evaluation, the patients were asked to undergo an MRI of the shoulders to analyze the defect filling of the Hill-Sachs lesion and the fatty infiltration of the infraspinatus muscle. The classification was based on the filling index score of remplissage (FISOR), 12 which classifies the filling, evaluated at the axial and sagittal planes, in five grades: complete filling (4 points), partial with small residual defect (3 points), partial with large residual defect (2 points), minimal filling (1 point) and complete filling failure (zero points). Lastly, the points from the axial and sagittal planes were added, determining 5 outcomes groups: excellent (7-8 points), good (5-6 points), regular (3-4 points), bad (1-2 points), and no filling (zero points).
Adaptation to the Filling Index Score of Remplissage
Since our evaluation considered patients submitted to an MRI with no contrast media (complying with their request for not using these agents), with the arm in ER, and only axial imaging sequence available, only the final FISOR classification methodology was considered. The examination was performed with the arm in ER for infraspinatus tendon relaxation, aiming to highlight a possible healing failure.
Regarding our evaluation of the healing of the capsulotenodesis, originally classified in five groups, the clustering of low-grade filling (FISOR 0–2) and high-grade filling (FISOR 3–4) was required to improve the statistical analysis.
Statistical Analysis
The variables were analyzed for their distribution type with the Kolmogorov-Smirnov test; force and ER variables were compared with the two-tailed Student t-test. The significance level was set at p < 0.05.
The present research was approved by the Ethics Committee under the number CAAE 62694016.7.0000.5125.
Results
Functional Results
The average Carter-Rowe score was 91 ± 14 (ranging from 50 to 100), with 88% of good and excellent results 9 , while the average Walch-Duplay score was 92 ± 10 (ranging from 70 to 100), with 92% of good and excellent results 10 ( Tables 1 and 2 ).
Table 1. Carter-Rowe score cluster.
| n | % | |
|---|---|---|
| ≤ 50 (bad) | 1 | 4 |
| 51–74 (regular) | 2 | 8 |
| 75–89 (good) | 2 | 8 |
| 90–100 (excellent) | 20 | 80 |
| Total | 25 | 100 |
Table 2. Walch-Duplay score cluster.
| n | % | |
|---|---|---|
| ≤ 50 (bad) | 0 | 0 |
| 51–74 (regular) | 2 | 8 |
| 75–89 (good) | 10 | 40 |
| 90–100 (excellent) | 13 | 52 |
| Total | 25 | 100 |
The ER force showed an average difference of - 0.92 kg when compared with the contralateral shoulder ( Table 3 ).
Table 3. Comparison of the external rotation force with the contralateral shoulder.
| n | Average (kg) | Standard deviation | Average difference | 95% CI | p -value | |
|---|---|---|---|---|---|---|
| Operated side | 25 | 8.96 | 2.67 | −0.92 | (−1.44; −0.40) | < 0.001 |
| Non-operated side | 25 | 9.88 | 2.88 |
Abbreviations: CI, confidence interval
Regarding the range of motion, there was an average difference of 10° when considering a ER at 0° abduction (ER1) and of 10° when considering a ER at 90∘ abduction (ER2), once again when compared with the contralateral shoulder ( Table 4 ).
Table 4. External rotation at 0∘ (ER1) and 90∘ (ER2) abduction compared with the contralateral shoulder.
| n | Average (kg) | Standard deviation | Average difference | 95% CI | p -value | |
|---|---|---|---|---|---|---|
| ER1 operated side | 25 | 77.04 | 14.6 | −10.04 | (− 14.74; −5.34) | < 0.001 |
| ER1 contralateral | 25 | 87.08 | 7.07 | |||
| ER2 operated side | 25 | 94.52 | 12.37 | −10 | (− 14.26; −5.74) | < 0.001 |
| ER2 contralateral | 25 | 104.52 | 14.61 |
Abbreviations: CI, confidence interval.; ER, external rotation
Concerning the recurrence of instability, 4 patients (16%) were positive at the apprehension clinical examination, and only 1 (4%) complained of a postoperative subdislocation episode. None of the evaluated patients presented a postoperative dislocation episode.
Imaging Results
From the 25 evaluated patients, 16 complied with a control MRI. According to the adaptation to the FISOR score, 12 all of them presented high-grade filling ( Fig. 4A and B ) ( Table 5 ). Fatty infiltration was also evaluated by the Goutallier classification; 11 patients showed no evidence of fatty infiltration (stage 0), and 4 presented evidence of fatty streaks (stage 1).
Fig. 4.

A, partial filling with small residual defect of the Hill-Sachs lesion on magnetic resonance imaging; B, complete filling.
Table 5. Filling Index Score of Remplissage.
| Filling | n | % |
|---|---|---|
| FISOR 0 (no filling) | 0 | 0 |
| FISOR 1 (low-grade filling) | 0 | 0 |
| FISOR 2 (low-grade filling) | 0 | 0 |
| FISOR 3 (high-grade filling) | 4 | 25 |
| FISOR 4 (high-grade filling) | 12 | 75 |
Abbreviations: FISOR, filling index score of remplissage
Discussion
The remplissage technique has been used in the approach to Hill-Sachs off-track lesions with no major glenoid bony injuries, always associated with the arthroscopic repair of a Bankart lesion. This technique is widely supported, both biomechanically 13 and clinically, with satisfactory functional results, low recurrence indexes, and a mild reduction of ER, with no functional repercussion. 14 15 16 17 18 19 20 21 These benefits and the complication index of < 1%, 14 excluding recurrences, which is considerably lower than the one observed in the open procedures, make the remplissage a good option in the therapeutic armamentarium of anterior instability.
Our group indicated the performance of the remplissage technique when the Hardy index was ≥ 20% 22 , the Hill-Sachs lesion was off-track, and the associated glenoid bone loss was < 25%.
Previous studies 6 15 16 17 18 19 20 21 cite recurrence rates ranging from 0 to 12%; a systematic review indicates an average rate of 5.4%. 14 Comparison was difficult due to the different definitions of recurrence. Some authors define treatment failure as dislocations, while others define it as a positive apprehension test at the postoperative period. In our casuistry, 4 patients (16%) were positive at the apprehension test, and only 1 (4%) had a postoperative subdislocation episode. There were no dislocation recurrences in the evaluated individuals. All of the individuals reported satisfaction with the outcome of the surgical treatment. Two patients presented with adhesive capsulitis during the postoperative rehabilitation, with good evolution.
Regarding the objective functional evaluation, represented by functional scores, good to excellent postoperative outcomes predominate in the literature, with mean Carter-Rowe scores of 83 to 91 points. 15 16 17 18 19 Boileau et al 15 had 87% of good to excellent results in the Walch-Duplay score, and Merolla et al 17 presented 96% of good to excellent results for both scores. We had similar indexes, of 88%, of good to excellent results at the Carter-Rowe score, and of 92% for the Walch-Duplay score.
Another literary controversy is the impact of remplissage at the ER of the shoulder. Previous studies showed a loss of 1.9° to 10° with statistical relevance, 15 16 17 while others demonstrated mild losses with no statistical relevance. 14 19 21 Once again, it is difficult to compare these trials due to the differences in the measurement techniques, in the shoulder position, and in the contrast with the contralateral side. As already mentioned, we obtained results with statistically significant losses in ER, of approximately 10°, both in ER1 and ER2. It is worth mentioning that this fact is not accompanied by damages at the objective (scores) or subjective (reported satisfaction with the treatment) functional evaluations.
Since the approach to the infraspinatus tendon is a part of the surgical technique, we have decided to evaluate the influence of its possible deficit on the global force of ER of the shoulder, measured in ER1. The fatty infiltration of the muscle belly was also evaluated with MRI exams.
At the evaluation of the ER force, there was a significant difference of ∼ 1 kg compared with the measurement of the contralateral side, unlike the results obtained by Merolla et al 17 and by Zhu et al, 18 who did not find significant differences in these measurements. Since the functional scores did not include a force measurement, its comparison with their results would not be relevant.
Image evaluation through MRI showed that all of the 16 patients who agreed with the examination presented, at most, fatty streaks at the muscular belly (Goutallier 1); this finding is consistent with the results from Park et al. 23 Regarding the filling of the Hill-Sachs lesion defect, the fact that all patients presented good to excellent filling (high-grade filling) according to the adaptation performed by our group makes a statistical analysis impractical, as well as the comparison with function, range of motion, or force.
Rhee et al 12 concluded that FISOR is a useful measurement criterion to evaluate structural results after the remplissage procedure. The original work reported 82.6% of good/excellent results for 23 patients. Regular, poor or negative results were obtained in 17.4% of the evaluated patients, with no clinical correlation. The FISOR classification was not used in its original form at the present work due to variations in the MRI exams, that is, examinations performed without contrast media and with the operated arm in ER to relax the infraspinatus tendon and thus allow a better evaluation of the filling of the Hill-Sachs defect. With this adaptation, we obtained 100% of good and excellent results (high-grade filling), unlike the original work, as mentioned above.
The limitations of the present study are the following: 1) regarding the imaging results, the comparative evaluation of the healing and filling of the Hill-Sachs defect was limited by the adaptation performed by our group in the original FISOR score. This adaptation was required due to the different protocols employed to obtain the postoperative images; 2) short minimum follow-up (12 months), lack of a control group, and a high index of loss at follow-up.
Conclusion
Our experience with the remplissage technique presented good to excellent functional results (observed in ∼ 90% of the patients) and good capsulotenodesis healing results. The results suggest that there was no morphological or functional damage to the infraspinatus, and that the mild loss of ER had no major functional repercussions. Further studies are required, with higher numbers of patients and a more detailed investigation of their sports activity, to draw more solid conclusions about these subjects.
Conflitos de Interesse Os autores declaram não haver conflitos de interesse.
Trabalho desenvolvido no Hospital Ortopédico, Belo Horizonte, MG, Brasil. Publicado originalmente por Elsevier Editora Ltda. © 2018 Sociedade Brasileira de Ortopedia e Traumatologia.
Work developed at the Hospital Ortopédico, Belo Horizonte, MG, Brazil.
Referências
- 1.Hill H A, Sachs M D. The grooved defect of the humeral head: a frequently unrecognized complication of dislocations of the shoulder joint. Radiology. 1940:690–700. [Google Scholar]
- 2.Calandra J J, Baker C L, Uribe J. The incidence of Hill-Sachs lesions in initial anterior shoulder dislocations. Arthroscopy. 1989;5(04):254–7. doi: 10.1016/0749-8063(89)90138-2. [DOI] [PubMed] [Google Scholar]
- 3.Spatschil A, Landsiedl F, Anderl W, Imhoff A, Seiler H, Vassilev I et al. Posttraumatic anterior-inferior instability of the shoulder: arthroscopic findings and clinical correlations. Arch Orthop Trauma Surg. 2006;126(04):217–22. doi: 10.1007/s00402-005-0006-4. [DOI] [PubMed] [Google Scholar]
- 4.Burkhart S S, De Beer J F. Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy. 2000;16(07):677–94. doi: 10.1053/jars.2000.17715. [DOI] [PubMed] [Google Scholar]
- 5.Yamamoto N, Itoi E, Abe H, Minagawa H, Seki N, Shimada Y et al. Contact between the glenoid and the humeral head in abduction, external rotation, and horizontal extension: a new concept of glenoid track. J Shoulder Elbow Surg. 2007;16(05):649–56. doi: 10.1016/j.jse.2006.12.012. [DOI] [PubMed] [Google Scholar]
- 6.Wolf E M, Pollack M E. Hill-Sachs “remplissage”: an arthroscopic solution for the engaging Hill-Sachs lesion. Arthroscopy. 2004;20 01:e14–5. doi: 10.1016/j.arthro.2008.03.015. [DOI] [PubMed] [Google Scholar]
- 7.Godinho G G, Souza J MG, Freitas J MA, Santos F ML, Vieira A W, João F M. Tratamento da instabilidade anterior do ombro: experiência com a técnica de Morgan. Rev Bras Ortop. 1997;32(04):265–71. [Google Scholar]
- 8.Garcia G H, Degen R M, Liu J N, Kahlenberg C A, Dines J S. Accuracy of suture passage during arthroscopic remplissage-what anatomic landmarks can improve it?: a cadaveric study. Orthop J Sports Med. 2016;4(08):2.325967116663497E15. doi: 10.1177/2325967116663497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rowe C R, Patel D, Southmayd W W. The Bankart procedure: a long-term end-result study. J Bone Joint Surg Am. 1978;60(01):1–16. [PubMed] [Google Scholar]
- 10.Walch G.Directions for the use of quotation of anterior instabilities of the shoulder 2013;5(1):45–56 [Google Scholar]
- 11.Jain N B, Wilcox R B, III, Katz J N, Higgins L D. Clinical examination of the rotator cuff. PM R. 2013;5(01):45–56. doi: 10.1016/j.pmrj.2012.08.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Rhee Y G, Cho N S, Yoo J H, Lee W G. Filling Index Score of Remplissage (FISOR): a useful measurement tool to evaluate structural outcome after remplissage. J Shoulder Elbow Surg. 2015;24(04):613–20. doi: 10.1016/j.jse.2014.08.024. [DOI] [PubMed] [Google Scholar]
- 13.Hartzler R U, Bui C N, Jeong W K, Akeda M, Peterson A, McGarry M et al. Remplissage of an off-track Hill-Sachs lesion is necessary to restore biomechanical glenohumeral joint stability in a bipolar bone loss model. Arthroscopy. 2016;32(12):2466–76. doi: 10.1016/j.arthro.2016.04.030. [DOI] [PubMed] [Google Scholar]
- 14.Buza J A, III, Iyengar J J, Anakwenze O A, Ahmad C S, Levine W N. Arthroscopic Hill-Sachs remplissage: a systematic review. J Bone Joint Surg Am. 2014;96(07):549–55. doi: 10.2106/JBJS.L.01760. [DOI] [PubMed] [Google Scholar]
- 15.Boileau P, O'Shea K, Vargas P, Pinedo M, Old J, Zumstein M. Anatomical and functional results after arthroscopic Hill-Sachs remplissage. J Bone Joint Surg Am. 2012;94(07):618–26. doi: 10.2106/JBJS.K.00101. [DOI] [PubMed] [Google Scholar]
- 16.Haviv B, Mayo L, Biggs D. Outcomes of arthroscopic “remplissage”: capsulotenodesis of the engaging large Hill-Sachs lesion. J Orthop Surg Res. 2011;6:29. doi: 10.1186/1749-799X-6-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Merolla G, Paladini P, Di Napoli G, Campi F, Porcellini G. Outcomes of arthroscopic Hill-Sachs remplissage and anterior Bankart repair: a retrospective controlled study including ultrasound evaluation of posterior capsulotenodesis and infraspinatus strength assessment. Am J Sports Med. 2015;43(02):407–14. doi: 10.1177/0363546514559706. [DOI] [PubMed] [Google Scholar]
- 18.Zhu Y M, Lu Y, Zhang J, Shen J W, Jiang C Y. Arthroscopic Bankart repair combined with remplissage technique for the treatment of anterior shoulder instability with engaging Hill-Sachs lesion: a report of 49 cases with a minimum 2-year follow-up. Am J Sports Med. 2011;39(08):1640–7. doi: 10.1177/0363546511400018. [DOI] [PubMed] [Google Scholar]
- 19.Franceschi F, Papalia R, Rizzello G, Franceschetti E, Del Buono A, Panascì M et al. Remplissage repair—new frontiers in the prevention of recurrent shoulder instability: a 2-year follow-up comparative study. Am J Sports Med. 2012;40(11):2462–9. doi: 10.1177/0363546512458572. [DOI] [PubMed] [Google Scholar]
- 20.Gracitelli M EC, Helito C P, Malavolta E A, Ferreira Neto A A, Benegas E, Prada F Set al. Results from filling “remplissage” arthroscopic technique for recurrent anterior shoulder dislocation Rev Bras Ortop20115;4606684–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Garcia G H, Wu H H, Liu J N, Huffman G R, Kelly J D., IV Outcomes of the remplissage procedure and its effects on return to sports: average 5-year follow-up. Am J Sports Med. 2016;44(05):1124–30. doi: 10.1177/0363546515626199. [DOI] [PubMed] [Google Scholar]
- 22.Hardy P, Lopes R, Bauer T, Conso C, Gaudin P, Sanghavi S. New quantitative measurement of the hill-sachs lesion: aprognostic factor for clinical results of arthroscopic glenohumeral stabilization. Eur J Orthop Surg Traumatol. 2012;22:541–7. [Google Scholar]
- 23.Park M J, Garcia G, Malhotra A, Major N, Tjoumakaris F P, Kelly J D., IV The evaluation of arthroscopic remplissage by high-resolution magnetic resonance imaging. Am J Sports Med. 2012;40(10):2331–6. doi: 10.1177/0363546512456974. [DOI] [PubMed] [Google Scholar]



