

Abstract
[Purpose] This study aimed to investigate the plantar contact condition in females and to clarify the relationship between the foot alignment and floating toes classified in static and dynamic conditions. [Participants and Methods] The participants were 122 females. We evaluated the plantar contact condition, calculated the floating toe score, and classified the floating toes of the participants. The floating toes were classified into improvable and unimprovable floating toe groups based on the floating toe score measured in dynamic conditions. Furthermore, foot alignment was evaluated in 35 participants randomized and extracted from the contact toe and the improvable and unimprovable floating toe groups. [Results] The Arch Height Index in the unimprovable floating toe group was significantly smaller than that in the improvable floating toe group. The digitus minimus varus angle in the unimprovable floating toe group was significantly larger than that in the improvable floating toe group. No significant differences were observed in other items. [Conclusion] This study revealed that the foot alignment between the improvable and unimprovable floating toe groups has different features. However, no significant difference was found in the foot alignment between the contact and floating toe groups. Henceforth, it is necessary to evaluate and classify floating toes considering the functional aspects.
Key words: Floating toe, Foot alignment, Pedoscope
INTRODUCTION
The main functions of the toes are prehensile or ambulatory ability1). The toes play an important role in walking and dynamic balance2, 3). The phenomenon wherein the toes do not contact the surface when standing or walking is called “floating toe”4).
Previously, most reports on floating toes were the sequelae after toe surgery5). However, the occurrence of floating toe in normal adults and children has recently been reported4, 6,7,8). Moreover, the prevalence of floating toe has been reported to increase in infants in Japan9). In addition, it has been clarified that floating toe decreases toe-grip strength and forward transfer ability6), and possibly increases the mechanical stress on the knee and the lower back when walking10). However, there is no consensus on the occurrence factor and treatment of floating toe.
Toe deformities, such as hallux valgus, are often found in female and elderly individuals11), and they are reported to be related to other foot alignment12). Foot deformities and malalignments can be a trigger for floating toe, but this relationship has not been clarified. The purpose of this study was to investigate the plantar contact condition in healthy adult female and to clarify the relationship between floating toe and foot alignment.
PARTICIPANTS AND METHODS
The participants consisted of 122 healthy adult female (mean age, 22.8 ± 2.1 years; height, 159.2 ± 5.3 cm; weight, 51.9 ± 6.3 kg). Furthermore, they had no lower extremity pathology that may have interfered with exercise within the past 6 months. Recruitment for participants was posted on nearby hospitals and universities with a recruitment document. In this study, we targeted only female, among whom the prevalence of foot deformation such as hallux valgus is higher than among men13). Ethical approval for this study was obtained from Ethics review committee of Gunma Chuo Hospital (Approval code: 2015-026). This study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all the participants, and rights of all participants were protected.
In this study, we evaluated the plantar contact condition for all participants. The floating toe score was calculated, and the floating toe group was classified. Subsequently, foot alignment was evaluated in 35 individuals extracted from the classified participants. The extraction method was randomly performed using Excel’s random number table.
We captured the plantar contact condition using a self-built Pedoscope (width: 50 cm, depth: 50 cm, height: 50 cm) with reference to previous studies14) (Fig. 1). Pedoscope is a device that captures the plantar contact condition by setting a participant on the tempered glass stage and using a digital camera (EX-FC150, CASIO COMPUTER Co., Ltd.). Unlike the ink-type footprint, the foot plantar contact condition can be possibly captured when the posture is stabilized. The plantar contact condition was measured using the total reflection of light; hence, we evaluated the plantar contact condition by making the room as dark as possible, the participants could see the target point. The participants stood barefoot on the tempered glass of Pedoscope with legs 5 cm apart and gazed at the target point 2 m ahead and eyes’ height and on the level while keeping the quiet standing position. Measurement was performed under three conditions: quiet standing condition, toe grip stance condition, and forward transfer condition. The quiet standing condition was a comfortable standing position, the toe grip stance condition was the effort of contacting the glass with the toe, and in the forward transfer condition, the center of gravity of the body was moved forward as much as possible with the heel contacted. We calculated the floating toe score and classified the participants into four groups6). To calculate the floating toe score of the 10 toes of both feet, 2 points were given if a toe contacted clearly on the image, 1 point was given if a toe contacted unclearly or partially, and no points were given if the toe had no contact; points were summed from 0 to 20 points (Fig. 2). If the floating toe score at the quiet standing condition was ≥18 points and the big toe on both sides were 2 points, the participants were placed in the “contact toe” (CT) group; those with 11 to 17 points or not belong to other groups were placed in the “incomplete contact toe” (ICT) group, and those with ≤10 points were placed in the floating toe group. Furthermore, the floating toe group was classified into two groups. Using the score at the toe-grip condition or forward transfer condition, one with ≥18 points and <18 points was classified as the “improvable floating toe” (IFT) and “unimprovable floating toe” (UFT) groups6), respectively. Foot alignment measurement was conducted for 3 groups excluding ICT group.
Fig. 1.
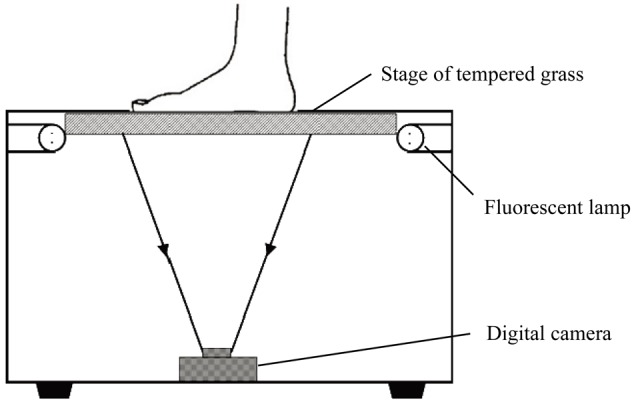
Shooting situation in self-build Pedoscope.
Fig. 2.

Plantar contact condition of Pedoscope and floating toe score.
Foot alignment measurement was performed using the arch height index (AHI), the transverse arch length index (TALI), the hallux valgus angle (HVA), the digitus minimus varus angle (DMVA), and the subtalar joint angle (STJA). The position of the measurement was standing in all items. AHI divided the navicular height by the foot length. Navicular height was taken from the floor to the rough surface of the navicular bone and the foot length was the distance from the posterior surface of the heel to the toes15). TALI divided the foot width by the foot length. The foot width was taken as the distance to the end of the first and fifth metatarsophalangeal joint protrusion. AHI and TALI were measured using a tape measure. HVA was taken as the angle between the long axis of the first metatarsal bone and the proximal phalange. DMVA was taken as the angle between the long axis of the fifth metatarsal bone and the proximal phalange. STJA was taken as the angle formed by the bisector of the distal one third lower leg and the posterior aspect of the calcaneus16). Pronation and supination were indicated as plus and minus, respectively. HVA, DMVA, and STJA were measured using a goniometer.
Statistical analysis was performed using SPSS version 22.0 for Windows. The foot alignment results among the three groups of CT, IFT, and UFT groups were compared. The Shapiro-Wilk test was used to assess the normality of data. As a result, since normality was not recognized, Kruskal-Wallis test was performed, and multiple comparison test was performed for items for which significant difference was recognized. The significant level of these analysis was set at 5%.
RESULTS
Because of the evaluation on plantar contact condition, 51 individuals (41.8%) had floating toes, and the number of floating toes was 97 toes (first toe: 18, second toe: 18, third toe: 3, fourth toe: 3, and fifth toe: 55). The results of classification were 13 (10.6%), 57 (46.7%), 15 (12.2%), and 37 (30.3%) in the CT, ICT, IFT, and UFT groups, respectively (Fig. 3).
Fig. 3.
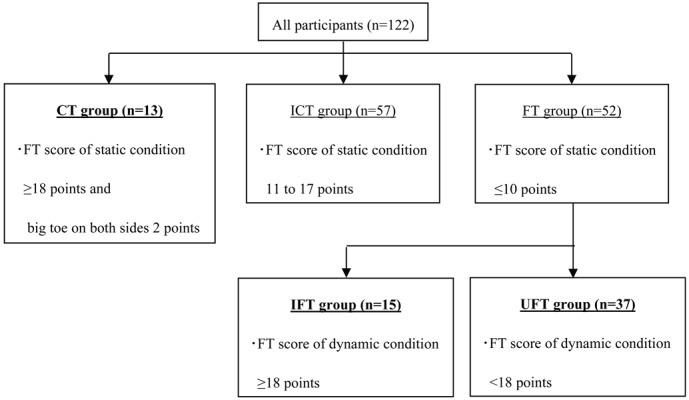
Result of floating toe classification.
CT: contact toe; ICT: incomplete toe; FT: floating toe; IFT: improvable floating toe; UFT: unimprovable floating toe; static condition: quiet standing condition; dynamic condition: toe-grip or forward transfer condition.
Foot alignment measurement was performed in 13 participants in the CT group (mean age, 23.3 ± 1.7 years; height, 159.0 ± 4.8 cm; body weight, 49.5 ± 7.7 kg), 11 in the IFT group (mean age, 23.2 ± 2.2 years; height, 157.4 ± 5.7 cm; body weight, 50.1 ± 7.7 kg), and 11 in the UFT group (mean age, 23.7 ± 1.7 years; height, 160.0 ± 6.2 cm; body weight, 51.4 ± 4.8 kg). We analyzed 70 feet in 35 individuals. No significant difference was observed in the basic information between the groups. The results of the foot alignment measurement in each group are shown in Table 1. The AHI in the UFT group (15.5% ± 2.5%) was significantly smaller than that in the IFT group (17.6% ± 2.2%). The DMVA in the UFT group (15.5° ± 5.5°) was significantly bigger than that in the IFT group (11.3° ± 5.4°). No significant difference was observed in the other items.
Table 1. Comparison of the foot alignment measurement in each group.
| CT group n=13 (13) |
IFT group n=11 (15) |
UFT group n=11 (37) |
|
|---|---|---|---|
| AHI (%) | 17.0 ± 2.4 | 17.6 ± 2.2* | 15.5 ± 2.5* |
| TALI (%) | 40.1 ± 2.3 | 41.0 ± 2.1 | 40.7 ± 3.1 |
| HVA (°) | 20.5 ± 5.8 | 19.3 ± 8.3 | 18.6 ± 7.5 |
| DMVA (°) | 14.6 ± 6.7 | 11.3 ± 5.4* | 15.5 ± 5.5* |
| STJA (°) | 8.9 ± 5.5 | 6.9 ± 6.7 | 8.0 ± 4.7 |
CT: contact toe; IFT: improvable floating toe; UFT: unimprovable floating toe; AHI: Arch Height Index; TALI: Transverse Arch Length Index; HVA: Hallux Valgus Angle; DMVA: Digitus Minimus Varus Angle; STJA: Subtalar Joint Angle.
n=the extracted participants (participants before extraction).
Differences were compared multiple comparison test. *p<0.01.
DISCUSSION
In this study, as well as in previous studies, the floating toe has been revealed to exist in healthy adults. Significant difference was observed between AHI and DMVA between the IFT and UFT groups in the foot alignment. However, no significant difference was found between the CT and both floating toe groups.
The AHI was significantly lower in the UFT group than that in the IFT group. Moreover, the AHI of the UFT group was confirmed to be lower than that in the CT group. In the previous studies, the UFT group has low toe-grip force compared with the CT group6, 7), and the forward transfer performance is significantly lower in the UFT group than that in the CT and IFT groups6). In the previous study, no significant difference was found in the arch ratio between the healthy and floating toe groups, and as a consideration, both groups with high and low arch ratio exist4). In this study, we classified the floating toe group into the IFT and UFT groups, and as a result, a significant difference was confirmed in both groups. It is conceivable that the UFT group in which the toe contacts are insufficient for dynamic tasks (i.e., toe-grip stance and forward transfer conditions) may have insufficient in the load on the toes even when walking etc. One of the roles of the toes in walking is to increase the base of support by contacting with the metatarsal head in the late stance phase and to increase the rigidity of the foot by tension of the plantar fascia and toe flexor muscles1). In the UFT group, the function of the toes is speculated to not sufficiently exert performances, leading to dysfunction of the toe flexor muscles. As a result, moving down of the medial longitudinal arch may occur. In addition, compared with the healthy group, the floating toe group increases the acceleration of the knees and the lower back during walking; thus, there is a risk of increasing the mechanical stress on them10). In this way, the floating toe group has been considered not to maintain the rigidity of the foot as the medial longitudinal arch decreases, causing deterioration of the braking of the center of gravity and propulsion capability.
During walking, the rear foot (i.e., heel) receives a load, and the forefoot has different roles, such as push-off from the ground17). In addition, the toes are equally loaded with the metatarsal heads during walking2), hence, an overload to the metatarsal heads in the UFT group is predicted in conditions, such as push-off phase. Overloading on the metatarsal heads leads to instability of the metatarsophalangeal joint and changes in the tone of the plantar intrinsic muscles, and it is conceivable that lead to the decrease in the AHI and increase in the DMVA. From this, loading stress on the metatarsal heads has been considered to cause a decrease in the AHI and an increase in the DMVA in the UFT group. It is also conceivable that the decrease of the AHI and the increase of the DMVA will cause floating toes due to the decreased rigidity of the foot part and reduction of the toe flexor muscles. From this, it is conceivable that the decrease of the AHI and the increase of the DMVA and the floating toe are mutually involved.
The results of this study revealed that the foot alignment has different features between the IFT and UFT groups. However, no significant difference was found in the foot alignment between the CT and both floating toe groups, which was different from the hypothesis that floating toes occur together with complex malalignment of the foot. In this study, the participants were classified based on the presence or absence of improvement of toe contacts during dynamic tasks (i.e., toe-grip stance and forward transfer conditions). This classification is to evaluate comprehensively based on the contact condition of all the toes. However, each toe has different roles in anatomical and structural characteristics, and their functions are also different. Furthermore, foot malalignment leads to various dysfunctions and disorders11, 18, 19). Therefore, it is considered necessary to evaluate and classify floating toes, considering functional aspects from now on.
Conflicts of interest
None.
REFERENCES
- 1.Lambrinudi C: Use and abuse of toes. Postgrad Med J, 1932, 8: 459–464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hughes J, Clark P, Klenerman L: The importance of the toes in walking. J Bone Joint Surg Br, 1990, 72: 245–251. [DOI] [PubMed] [Google Scholar]
- 3.Chou SW, Cheng HY, Chen JH, et al. : The role of the great toe in balance performance. J Orthop Res, 2009, 27: 549–554. [DOI] [PubMed] [Google Scholar]
- 4.Fukuyama K, Maruyama H: Occurrence of floating toe from the viewpoint of the structure of foot arch. J Phys Ther Sci, 2011, 23: 33–36. [Google Scholar]
- 5.Migues A, Slullitel G, Bilbao F, et al. : Floating-toe deformity as a complication of the Weil osteotomy. Foot Ankle Int, 2004, 25: 609–613. [DOI] [PubMed] [Google Scholar]
- 6.Fukuyama K, Osanai M, Maruyama H: Determination of floating toes by toe-grip strength and forward transfer. Rigakuryouho Kagaku, 2013, 28: 109–113. [Google Scholar]
- 7.Tasaka S, Matsubara K, Nishiguchi S, et al. : Association between floating toe and toe grip strength in school age children: a cross-sectional study. J Phys Ther Sci, 2016, 28: 2322–2325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Araki T, Masuda T, Jinno T, et al. : Incidence of floating toe and its association with the physique and foot morphology of Japanese children. J Phys Ther Sci, 2015, 27: 3159–3162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Harada S: A study on physical structures of preschool children’s feet compared between 1980 and 2000. Kutsuno Igaku, 2002, 15: 14–18. [Google Scholar]
- 10.Uritani D, Sakamoto C, Fukumoto T: Effect of floating toes on knee and trunk acceleration during walking: a preliminary study. J Phys Ther Sci, 2017, 29: 361–364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Menz HB, Lord SR: The contribution of foot problems to mobility impairment and falls in community-dwelling older people. J Am Geriatr Soc, 2001, 49: 1651–1656. [PubMed] [Google Scholar]
- 12.Kalen V, Brecher A: Relationship between adolescent bunions and flatfeet. Foot Ankle, 1988, 8: 331–336. [DOI] [PubMed] [Google Scholar]
- 13.Roddy E, Zhang W, Doherty M: Prevalence and associations of hallux valgus in a primary care population. Arthritis Rheum, 2008, 59: 857–862. [DOI] [PubMed] [Google Scholar]
- 14.Fukuyama K, Maruyama H: The determination of floating toes and reliability of its assessment. Rigakuryoho Kagaku, 2012, 27: 497–502. [Google Scholar]
- 15.Bonci CM: Assessment and evaluation of predisposing factors to anterior cruciate ligament injury. J Athl Train, 1999, 34: 155–164. [PMC free article] [PubMed] [Google Scholar]
- 16.Elveru RA, Rothstein JM, Lamb RL, et al. : Methods for taking subtalar joint measurements. A clinical report. Phys Ther, 1988, 68: 678–682. [DOI] [PubMed] [Google Scholar]
- 17.Katahira K, Tsukahara S, Fujiwara M, et al. : Carbon-fiber foot-force sensor system for gait analysis. Fukushima J Med Sci, 1984, 30: 29–37. [PubMed] [Google Scholar]
- 18.Mickle KJ, Munro BJ, Lord SR, et al. : ISB Clinical Biomechanics Award 2009: toe weakness and deformity increase the risk of falls in older people. Clin Biomech (Bristol, Avon), 2009, 24: 787–791. [DOI] [PubMed] [Google Scholar]
- 19.Bennett PJ: A randomized clinical assessment of foot pronation and its relationship to patellofemoral syndrome. J Cur Pod Med, 1988, 37: 8–11. [Google Scholar]