

Abstract
Background
Emergency workers such as firefighters are cataloged within the most demanding and injurious professions globally. Considering the health and safety implications in firefighting, a lot of research needs to be conducted to examine how firefighters' task characteristics and their work demand influence the development of work-related musculoskeletal disorders (WMSDs). This study therefore examines how the task characteristics of firefighters moderates the relationship between their work demand and the development of WMSDs.
Methods
Convenient sampling was employed to select 320 firefighters in the Greater Accra region of Ghana. Data were analyzed using descriptive statistics, correlation, and regression.
Results
The findings revealed that work demand and task characteristics have significant positive effects on WMSDs. Again, the task characteristics of firefighters moderates the relationship between their work demand and WMSDs.
Conclusion
Since the study shows that task characteristics influences the relationship between work demand and WMSDs, it is vital for managers to constantly modify the nature of tasks performed by and work demand of emergency workers to minimize the development of WMSDs and other industrial health complications.
Keywords: firefighters, task characteristics, work demand, work-related musculoskeletal disorders
1. Introduction
Even though the demanding nature of every work can pose adverse health effects to workers, professionals employed in highly demanding work settings can be more vulnerable. Reports by the International Labour Organization (ILO) [1] shows that an annual estimated 2.2 million deaths are due to industrial illnesses and accidents. Globally, emergency workers such as firefighters, the army, the police, rescue workers and health workers fall within the highly demanding and injurious occupational groups. Although there is high demand associated with emergency work, demands placed on firefighters in developing countries appear to be abnormally high as compared to those in advanced countries. For instance, a report by International Labour Organization [2] approximated that firefighter to citizen ratio in developed countries (European nations) was 1:1,000–1,200, while developing countries (Mali) had a ratio of 1:33,435, which is extremely high. Additionally, the escalating fire outbreaks in developing countries such as Ghana are likely to increase the work demand of firefighters [3]. The Ghana National Fire Service (GNFS) fights over 1000 fires annually. For instance, in 2015, the GNFS fought 6214 fires nationwide [3]. Beside, work-related musculoskeletal disorders (WMSDs) have been linked with work stress, high workload and demand, low job control, and work monotony (Cañadas-De la Fuente et al.; Norlund et al) [4], [5]. These situations might not be too different from that of the GNFS due to the nature of their work.
Work demand has been defined by Jones and Fletcher [6] “as the degree to which the working environment contains stimuli that require some effort” (p. 34). High work demand causes undesirable consequences if they necessitate additional effort beyond the normal way of attaining work targets (Demerouti et al) [7]. Nunes [8] defined “work-related musculoskeletal disorders as a wide range of inflammatory and degenerative conditions affecting muscles, tendons, ligaments, joints, peripheral nerves, and supporting blood vessels” (p. 121). Musculoskeletal complaints may occur when muscles or tendons are overextended or over-used beyond their capabilities. Among the likely ergonomic risk causes of WMSD are repetitive motion, awkward posture, forceful exertions, pressure points, and static postures. According to Kim and Soergel [9], task characteristics can be considered “either objectively to measure the inherent structural nature of a task or subjectively to measure the perception of task performers” (p. 4). Task characteristics therefore imply the relationship between a job and the job performer. Typically, the firefighting profession is characterized by uncertainty, exposure to human loss, shift work, and traumatic incidences among others. With regards to workers in the firefighting profession, the nature of their jobs might require additional effort, which might culminate into musculoskeletal complaints. In Ghana, firefighters work under conditions of high speed, uncertainty, repetitive bending, exposure to extreme heat and smoke, long hours of standing, stress, and exposure to biological hazards such as blood of victims they salvage (Cañadas-De la Fuente et al) [3].
Some researchers have reported incidences of WMSDs among firefighters, other professions, and the general public. Kim et al [10] for example examined the predictors of WMSDs among 21,466 Korean male fire service workers. It was found that physical environment, work demand, organizational structure, occupational climate, inadequate rewards, and job insecurity had relationships with the manifestation of WMSDs. In Canada also, Cole et al [11] found that sex, education, job insecurity, high levels of physical exertion, and high levels of psychological demands have positive associations with work-related repetitive strain injuries. Both the Korean and Canadian studies employed the Nordic questionnaire and revealed that heavy work demand placed on workers can lead to the development of musculoskeletal complaints. While Kim et al [10] emphasized on how the work setting and physical demand of work predict WMSDs, Cole et al [11] highlighted the association between psychological work demand and WMSDs. It is therefore suggestive that both physical and psychological work demand influence WMSDs. However, both studies did not indicate how the task characteristics of firefighting affected their health.
Also, the study by Park and Jang [12] revealed that excessive shock in the upper limit was significantly attributed to less decision opportunity at work, and work demand had a significant relationship with neck and shoulder complaints. Further, it was found that control over time was related to neck complaints whereas both high demand and low decision opportunity significantly predicted shoulder and neck complaints among females. In Brazil, Fonseca and Fernandes [13] found that work-related musculoskeletal complaints in the neck, shoulder, or upper back and the lower back had relationships with physical work demand (handling heavy materials, poor back position, and repetitive tasks), psychosocial demands, and hazardous physical fitness. From the findings, the nature of tasks assigned to workers can lead to the development of WMSDs. Also, musculoskeletal complaints in distal upper parts can be related to physical work demand (repetitive and energetic tasks) as well as number of years in service. This points to the necessity for interventions to fit in both the organizational elements of work and adaptations in the physical environment and in the characteristics of work assignments. The findings of Park and Jang [12] and Fonseca and Fernandes [13] are akin since they both highlight how high work demand and task characteristics relate to WMSDs. Task-related issues such as lack of control over work and minimal participation in decisions regarding work can cause workers WMSDs, highlighting the need for task assessment. In the United States, Krause et al. [14] similarly revealed that people with high exposures to physical workload and ergonomic complaints were 3.24–5.42 times more probable to report extreme musculoskeletal conditions than those with lower exposures. It was also reported by Shaik et al [15] that age, work experience, and working hours per week had significant association with WMSDs. This hints that aside the influence of work demand and task characteristics on WMSDs, the age, work experience, and hours of work done by firefighters can also influence the development of WMSDs.
Even though the demanding nature of tasks performed by firefighters can affect the development of WMSDs, the nature of tasks they perform appear to effect the relationship. This study therefore seeks to examine whether the work demand and task characteristics of firefighters relate to the development of WMSDs and to also find out whether task characteristics moderates the relationship between work demand and WMSDs (Fig. 1).
Fig. 1.
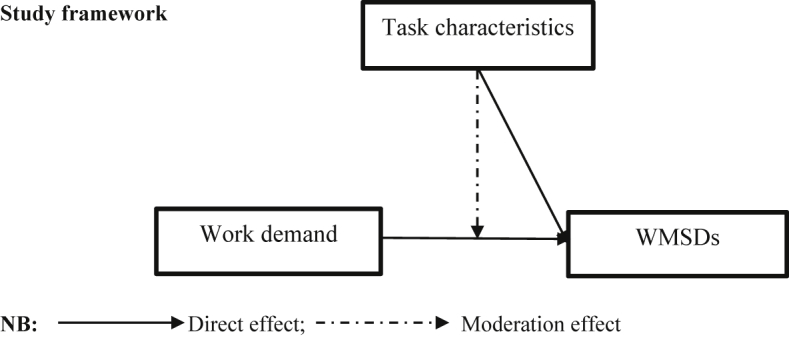
A model of work demand, WMSDs, and task characteristics.
Hypotheses
-
H1
Firefighters' work demand will have a significant positive effect on the development of WMSDs
-
H2
Firefighters' task characteristics will have a significant positive effect on the development of WMSDs
-
H3
Firefighters' task characteristics will moderate the relationship between the work demand and WMSDs
2. Materials and methods
2.1. Study design and sampling
Using a cross-sectional survey design, the study sampled 320 out of a total of 1367 firefighters in the Greater Accra Regional Fire Command, Ghana. The Greater Accra Region was selected because of its high record of fire outbreaks in Ghana (GNFS) [3]. Also, respondents were selected through convenient sampling. Participants were sampled from the lowest rank (Recruit firefighter) to the highest rank (Chief fire officer).
2.2. Instrumentation
A self-reported questionnaire was used for the data collection. The questionnaire had four sections: demography, work demand, WMSDs, and task characteristics. The demographic section comprised of items such as: gender, age, and number of working hours. Van Veldhoven and Meijman's [16] 8-item questionnaire was adapted to measure the work demand of firefighters. Rated on a 5-point Likert scale (1: strongly disagree to 5: strongly agree), the questionnaire had an original Cronbach α coefficient of 0.87 and had typical statements like “I have to work fast.” The Cronbach α value for this study is 0.80. The task characteristics subscale of Van Zyl and Van der Walt's [17] Experience of Work and Life Circumstances questionnaire was used to measure firefighters' task characteristics. A total of 11 questions out of the 14 original items in the scale were used based on experts' opinion. Items for this scale were rated on a 5-point Likert scale (1: very low, 2: low, 3: neutral, 4: high, and 5: very high), with reliabilities ranging between 0.83 and 0.92. A typical item on the scale was “degree of uncertainty”. The new Cronbach α coefficient for this study is 0.72.
Lastly, WMSDs was measured using the standardized Nordic questionnaire (Kuorinka et al) [18]. The Nordic questionnaire measures pains, hurts, or aches in any of nine (9) body parts (neck, shoulder, elbow, wrist, upper back, lower back, hip, knee, and ankle) for the last 12 months. Items were rated on a 5-point Likert scale (1: very unlikely, 2: unlikely, 3: neutral, 4: likely, and 5: very likely) with a Cronbach α coefficient of 0.92.
Variables that could affect firefighters' development of WMSDs were controlled for in this study. They are sex (Cole et al) [11], age (Shaik et al) [15], and working hours (Park and Jang) [12]. These variables were included because they had relationships with WMSDs in previous studies and could account for some variance in WMSDs. Sex being a dichotomous variable was coded as (0 male, 1 female), age was coded as (1 if 25–34 yrs, 0 otherwise), (1 if 35–44 yrs, 0 otherwise), (1 if 45–55 yrs, 0 otherwise); and (1 if more than 55 yrs, 0 otherwise), while 18–24 yrs was coded as 0 and used as the reference group. Working hours had four levels: (1 more than 6 hour but less than 8 hour, 0 otherwise), (1 more than 8 hour but less than 10 hour, 0 otherwise), (1 more than 10 hour but less than 12 hour, 0 otherwise), and (1 more than 12 hour, 0 otherwise), whereas 6 hour or less was the reference category and coded as 0.
2.3. Data collection and analysis
Data for this study were collected from March–May 2016. Questionnaires were personally administered to firefighters within the Greater Accra Regional Command. Ethical considerations such as approval, informed consent, voluntarily participation, confidentiality, and anonymity were adhered to. In terms of data analysis, the Predictive Analytics Software, version 22.0, was the analytical tool used. Respondents' demography was analyzed descriptively. Correlation test was preliminarily used to test for relationships among variables. Further, a multiple hierarchical regression analysis was used to test for the direct effects of work demand and task characteristics on WMSDs as well as the moderation effect of task characteristics on the relationship between work demand and WMSDs.
3. Results
3.1. Assumption testing
Assumptions of normality and multicollinearity were tested. From Table 1, the z-scores of skewness were (−0.110, −1.272, and −0.206) for work demand, task characteristics, and WMSDs, respectively. The Kurtosis z-scores were (−0.305, −0.430, and −1.367) for work demand, task characteristics, and WMSDs, respectively. All variables fell within the normality thumb of rule (−1.96 to 1.96), hence all variables were normally distributed. Again, all variables had correlates below 0.8, showing signs of no multicollinearity as shown in Table 4. Also missing data were controlled through expectation maximization approach (Table 2, Table 3).
Table 1.
Normality testing
| Variable | Skewness | Std. error | z-scores | Kurtosis | Std. error | z-scores |
|---|---|---|---|---|---|---|
| 1. WD | −0.015 | 0.136 | −0.110 | −0.083 | 0.272 | −0.305 |
| 2. TCs | −0.173 | 0.136 | −1.272 | −0.117 | 0.272 | −0.430 |
| 3. WMSDs | −0.028 | 0.136 | −0.206 | −0.372 | 0.272 | −1.367 |
Std. error, standard error; TCs, task characteristics; WD, work demand; WMSDs, work-related musculoskeletal disorders.
Table 4.
Correlation matrix of study variables (N = 320)
| Variables | M | SD | Age | WHrs | WD | TC | WMSDs |
|---|---|---|---|---|---|---|---|
| Age | 2.88 | 1.04 | 1.00 | ||||
| WHrs | 4.10 | 1.10 | −0.18** | 1.00 | |||
| WD | 29.24 | 4.17 | −0.03 | −0.01 | 1.00 | ||
| TCs | 38.68 | 6.42 | 0.16** | 0.09 | 0.23** | 1.00 | |
| WMSDs | 32.28 | 8.44 | 0.05 | −0.13 | 0.23** | 0.26** | 1.00 |
M, mean; SD, standard deviation; TCs, task characteristics; WD, work demand; WHrs, working hours; WMSDs, work-related musculoskeletal disorders.
**Correlation is significant at p < 0.01, Sig. (2- tailed).
Table 2.
Demographic characteristics of respondents
| Characteristics N (%) | Work demand |
p | Task characteristics |
p | WMSDs |
p | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | ||||||||
| Sex | 0.288 | 0.429 | 0.171 | |||||||
| Male | 234 (73.1) | 29.406 | 4.012 | 39.141 | 6.359 | 32.581 | 8.195 | |||
| Female | 86 (26.9) | 28.802 | 4.560 | 37.419 | 6.432 | 31.453 | 9.086 | |||
| Age | 0.977 | 0.001 | 0.932 | |||||||
| >18 ≤ 24 yrs | 26 (8.1) | 29.269 | 3.822 | 34.423 | 6.894 | 31.615 | 9.261 | |||
| >25 ≤ 34 yrs | 104 (32.5) | 29.365 | 4.304 | 38.115 | 6.274 | 32.096 | 8.209 | |||
| >35 ≤ 44 yrs | 87 (27.2) | 29.299 | 4.179 | 39.655 | 7.307 | 32.000 | 8.790 | |||
| >45 ≤ 55 yrs | 90 (28.1) | 29.133 | 3.901 | 39.778 | 4.962 | 32.789 | 8.410 | |||
| >55 yrs | 13 (4.1) | 28.615 | 5.796 | 37.539 | 5.695 | 33.385 | 7.411 | |||
| WHrs | 0.907 | 0.526 | 0.071 | |||||||
| ≤6 hour | 3 (0.9) | 27.667 | 3.215 | 37.000 | 2.646 | 28.333 | 7.572 | |||
| >6 ≤ 8 hour | 21 (6.6) | 29.905 | 4.182 | 36.619 | 5.705 | 33.190 | 5.173 | |||
| >8 ≤ 10 hour | 97 (30.3) | 29.247 | 4.831 | 38.412 | 6.5188 | 34.010 | 7.359 | |||
| >10 ≤ 12 hour | 18 (5.6) | 29.000 | 4.678 | 38.944 | 6.421 | 33.667 | 5.466 | |||
| >12 hour | 181 (56.6) | 29.216 | 3.757 | 39.061 | 6.477 | 31.171 | 9.362 | |||
p, significance level, SD, standard error; WHrs, Working hours; WMSDs, work-related musculoskeletal disorders.
Table 3.
Descriptive analysis of variables/items (N = 320)
| Variables/Items | M | SD |
|---|---|---|
| Work demand | 29.244 | 4.168 |
| 1. Do you have to work fast? | 4.219 | 0.907 |
| 2. Do you have too much work to do? | 3.984 | 0.901 |
| 3. Do you have to work extra hard to finish a task? | 4.138 | 0.927 |
| 4. Do you work under time pressure? | 4.000 | 1.059 |
| 5. Can you do your work in comfort? | 3.003 | 1.328 |
| 6. Do you have to deal with a backlog at work? | 3.113 | 1.182 |
| 7. Do you have problems with the pace of work? | 3.328 | 1.145 |
| 8. Do you have problems with the workload? | 3.459 | 1.190 |
| Task characteristics | 38.678 | 6.415 |
| 1. Degree of uncertainty | 3.641 | 1.206 |
| 2. Exposure to human loss | 3.634 | 1.265 |
| 3. Interpersonal tension | 3.050 | 1.256 |
| 4. Shift work | 3.794 | 1.036 |
| 5. Overloading/underloading | 3.384 | 1.100 |
| 6. Traumatic incidents | 3.728 | 1.070 |
| 7. Accountability for decisions taken under pressure | 3.684 | 1.090 |
| 8. Terrible sensory experiences | 3.719 | 1.118 |
| 9. Serious fires in which people are trapped | 3.753 | 1.079 |
| 10. The danger of injuries to and illness of firefighters | 4.244 | 0.968 |
| 11. Slow response time | 2.047 | 1.299 |
| Work-related musculoskeletal disorders | 32.278 | 8.444 |
| 1. Neck | 3.338 | 1.405 |
| 2. Shoulder | 3.600 | 1.207 |
| 3. Elbow | 3.497 | 1.169 |
| 4. Wrist/hands | 3.731 | 1.143 |
| 5. Upper back | 3.938 | 1.003 |
| 6. Lower back | 3.831 | 1.151 |
| 7. One or both hips/thighs | 3.422 | 1.282 |
| 8. One or both knees | 3.491 | 1.254 |
| 9. Ankle | 3.431 | 1.253 |
M, mean; SD, standard deviation; TC, Task characteristics; WD, Work demand; WMSDs, Work-related musculoskeletal disorders.
3.2. Demography
.
3.3. Variables description
.
3.4. Relationship testing
.
3.5. Predicting WMSDs
Hypothesis 1
Firefighters' work demand will have a significant positive effect on the development of WMSDs.
The first hypothesis sought to test the relationship between firefighters' work demand and the development of WMSDs. In testing this hypothesis, a Pearson's correlation test was carried out. From Table 4, there was a significant positive relationship between work demand and WMSDs (r = 0.23, p < 0.01). Further, a regression analysis was conducted to determine the predictive ability of work demand on WMSDs. From Table 5 (step 2), firefighters' work demand has a significant positive effect on WMSDs (β = 0.226, p < 0.01) after controlling for sex and age. Also work demand explained 5.1% (ΔR2 = 0.051) of variance in WMSDs. Hence hypothesis 1 was supported.
Hypothesis 2
Firefighters' task characteristics will have a significant positive effect on the development of WMSDs.
The second hypothesis sought to find out whether there is a relationship between firefighters' task characteristics and WMSDs. A Pearson's product moment correlation was used to test the relationship between task characteristics and WMSDs. From Table 4, task characteristics have a significant positive relationship with WMSDs (r = 0.26, p < 0.01). Further test was carried out to determine the causal effect of task characteristics on WMSDs. A regression test was carried out to test for the effect. From Table 5 (step 3), firefighters' task characteristics has a significant positive effect on WMSDs (β = 0.214, p < 0.01) after controlling for sex and age. Further, task characteristics accounted for 4.2% (ΔR2 = 0.042) of variance in WMSDs. The findings therefore support hypothesis 2.
Hypothesis 3
Firefighters' task characteristics will moderate the relationship between their work demand and WMSDs.
The third hypothesis sought to test whether firefighters' task characteristics moderates the relationship between their work demand and WMSDs development. To test for moderation, a 4-step hierarchical regression was carried out (Baron and Kenny) [19]. To prevent high multicollinearity, work demand and task characteristics were centered (Aiken and West) [20] before creating their interaction term (WD × TC). From Table 5, sex and age were used as control variables to predict WMSDs in step 1. Sex (β = -0.057, p > 0.05) and age (β = 0.043, p > 0.05) did not significantly predict WMSDs. The two control variables accounted for a 0.5% variance in WMSDs (R2 = 0.005). Work demand was entered in step 2 which had a significant positive effect on WMSDs (β = 0.226, p < 0.01) and accounted for 5.1% of variance in WMSDs (ΔR2 = 0.051). In step 3, task characteristics was added. Task characteristics had a significant positive effect on WMSDs (β = 0.214, p < 0.01) and also accounted for a 4.2% (ΔR2 = 0.042) variance in WMSDs. The interaction term between work demand and task characteristics (WD × TC) was added in step 4. It had a significant negative effect on WMSDs (β = -0.174, p < 0.01) and accounted for a significant variance of 2.8% in WMSDs (ΔR2 = 0.028) holding other factors constant. Together, all variables accounted for 12.6% variance in WMSDs (R2 = 0.126). The output suggests that task characteristics moderate the relationship between the work demand of firefighters and WMSDs. Hence, hypothesis 3 was supported.
Table 5.
A hierarchical regression showing predictors of WMSDs
| B | Std. error | β | p | R | R2 | ΔR2 | |
|---|---|---|---|---|---|---|---|
| Step 1 | |||||||
| (Constant) | 32.656 | 1.986 | 0.000 | 0.073 | 0.005 | ||
| Sex | −1.088 | 1.067 | −0.057 | 0.309 | |||
| Age | 0.349 | 0.455 | 0.043 | 0.445 | |||
| Step 2 | |||||||
| (Constant) | 18.719 | 3.891 | 0.000 | 0.237 | 0.056 | 0.051 | |
| Sex | −0.804 | 1.043 | −0.042 | 0.441 | |||
| Age | 0.408 | 0.444 | 0.050 | 0.359 | |||
| WD | 0.458 | 0.111 | 0.226 | 0.000 | |||
| Step 3 | |||||||
| (Constant) | 11.071 | 4.307 | 0.011 | 0.313 | 0.098 | 0.042 | |
| Sex | −0.412 | 1.026 | −0.022 | 0.688 | |||
| Age | 0.120 | 0.442 | 0.015 | 0.787 | |||
| WD | 0.359 | 0.112 | 0.177 | 0.001 | |||
| TCs | 0.282 | 0.074 | 0.214 | 0.000 | |||
| Step 4 | |||||||
| (Constant) | 14.083 | 4.349 | 0.001 | 0.355 | 0.126 | 0.028 | |
| Sex | −0.674 | 1.015 | −0.035 | 0.507 | |||
| Age | 0.012 | 0.437 | 0.002 | 0.978 | |||
| WD | 0.271 | 0.114 | 0.134 | 0.017 | |||
| TCs | 0.294 | 0.073 | 0.224 | 0.000 | |||
| WD × TC | −0.049 | 0.015 | −0.174 | 0.002 | |||
B, unstandardized beta; Std. error, standard error; TCs, task characteristics; β, standardized beta; R2, R square; ΔR2, R2 change; p, significance level; WD, work demand; WD × TC, work demand × task characteristics.
4. Discussions
4.1. Effect of firefighters' work demand on the development of WMSDs
The findings indicate that the work demand of firefighters affect the development of WMSDs. This suggests that increase in firefighters' work demand will lead to higher occurrences of WMSDs. From Table 5, a unit increase in firefighters' work demand will lead to a 22.6% increase in the occurrence of WMSDs, holding other factors constant. The findings buttress the earlier study by Kim et al [10] among Korean firefighters which revealed that work factors such as work demand, structure of organization, work climate, physical environment, lack of job security, and poor rewards significantly affect WMSDs. Fonseca and Fernandes [13] also provide an indication that both physical and psychological work demands cause musculoskeletal complaints. Also, high levels of physical exertion have been reported to result in WMSDs [11]. These findings imply that as the level of demand in firefighting intensifies, it leads to WMSDs. As such, the more firefighters' tasks are characterized by heavy workload, high pressure, speed, and the need to work extra harder to finish their tasks, there is the high likelihood of developing WMSDs. High work demand resulting from such activities can cause strain and pains in body parts of firefighters, leading to WMSDs.
4.2. The effect of firefighters' task characteristics on the development of WMSDs
Firefighters' task characteristics has a significant positive effect on the development of WMSDs. Controlling for age and sex, a change in task characteristics will lead to an increase in incidences of WMSDs. From Table 5, a unit alteration in the task characteristics of firefighters will lead to a 21.4% increase in the development of WMSDs, holding age and sex constant. This implies that repetitive and strenuous tasks can result in musculoskeletal disorders. This means that the nature of tasks performed at work can result in the development of WMSDs. This finding supports earlier reports by Cole et al [11] who found that high levels of physical exertion and psychological demands have positive association with work-related repetitive strain injuries. Therefore, work characteristics such as uncertainties, human loss, standing for long hours, rescuing victims, responding to distress calls, and sight of injured and dead people can culminate in musculoskeletal disorders.
4.3. How firefighters' task characteristics moderate the relationship between their work demand and WMSDs
Task characteristics moderate the relationship between work demand and WMSDs. From Table 5, the interaction term between work demand and task characteristics has a significant negative effect on WMSDs and accounted for a 2.8% variation in WMSDs. Also, a unit modification in the task characteristics of firefighters can lead to a 17.4% reduction of the effect of work demand on WMSDs. The findings therefore suggest that task characteristics reduce the effect of work demand on WMSDs. This outcome conforms to earlier suggestions by Fonseca and Fernandes [13] who opined that interventions such as work adaptations and task modifications have implications for health and job outcomes. These findings highlight the importance of modifying the task characteristics of firefighters to lessen the effect of their work demand on the development of WMSDs. This indicates that alterations of firefighters' tasks (such as uncertainties, exposure to human loss, shift work, speed, etc.) will minimize how work demand causes the development of WMSDs.
4.4. Implications/recommendations
The current study provides some useful insights into industrial health and safety management in emergency work settings. If taken into consideration, such insights can help organizations adjust their work systems to enhance the health and safety of their employees. The work demand placed on workers has the propensity to result in undesirable organizational and health consequences. But a careful adjustment of work demand and task characteristics can provide some beneficial health outcomes.
To begin with, WMSDs is caused by excessive work demand. Incidences of WMSDs can result in various adverse health outcomes such as stress, accidents, permanent disability, and even death. It can also result in undesirable organizational outcomes like low motivation, turnover, and absenteeism among others. The aftermath of these outcomes are inefficiencies, low productivity, and poor service such as slow response rate among fire service workers.
Again, work demand affects WMSDs, such that increase in the work demand of workers leads to increased development of WMSDs. The amount of work assigned to workers can result in the development of musculoskeletal complaints, especially when they will require additional energies. Managers and supervisors are therefore entreated to consider the level of resilience and capabilities of their workers before assigning tasks to them. This to a large extent will prevent either under assigning or over assigning of tasks since they have implications for health.
To add, the study justifies the influence of task characteristics on the effect of work demand on WMSDs. Managers' ability to modify the nature of tasks assigned to workers and how such tasks are performed can be of enormous health benefits to both the employee and the organization. The adoption of working dynamics such as teleworking, job sharing, and job rotation can reduce the amount of demand inherent in various work settings.
4.5. Conclusions
Based on the findings, it is clear that even though increase in employees' work demand can result in the development of WMSDs, the responsibility of altering work depends highly on managers and supervisors. The ability of managers and supervisors to assign the right work to the right person at the right time is key. Particularly, in emergency services, there is the need to screen for bounciness, ability, and easy adaptability among new recruits whenever recruiting fresh firemen and firewomen. The importance of excellent health and safety at the workplace cannot be underemphasized because of its direct and indirect implications for the employee, the organization, and the state as a whole. Therefore, a lot of measures need to be put in place to ensure the good health and safety of workers at all times through proper job designs.
4.6. Limitations of the study
The study is limited in terms of its coverage. Even though there are several emergency professions in Ghana, the study was carried out among only firefighters. Also the study was centered in the Greater Accra region of Ghana. Therefore, results could have been different if the scope of the study was extended to other emergency professions and other geographical regions. Again, the study adopted a quantitative approach which limits the responses of participants. As such, a qualitative study may also be carried out to get in-depth views on firefighters work demand, task characteristics and WMSDs. Lastly, the use of cross-sectional data limits the strength of causality, hence future studies may use panel data to enhance the strength of the causal influence of task characteristics on the relationship between work demand and WMSDs.
Conflicts of interest
The author declares that this is his own original research and, hence, has no conflict of interest.
Acknowledgments
The author wishes to extend his gratitude to Mr. Alex Anlensinya, (PhD candidate) Department of Organisation and Human Resource Management, University of Ghana Business School, for his technical guidance.
Footnotes
Supplementary data related to this article can be found at https://doi.org/10.1016/j.shaw.2018.05.004.
Appendix A. Supplementary data
The following are the supplementary data related to this article:
References
- 1.International Labor Organization . 2016. Workplace stress: a collective challenge. Labour Administration, Labour Inspection and Occupational Safety and Health Branch-(LABADMIN/OSH): Geneva. Available from: www.ilo.org/safeday. [Google Scholar]
- 2.International Labor Organization . 2003. Public emergency services: Social dialogue in a changing environment.http://www.ilo.org/public/english/dialogue/sector/techmeet/jmpes03/jmpes-r.pdf [Google Scholar]
- 3.Ghana National Fire Service . GNFS; The Republic of Ghana: 2016. National fire statistics for the year 2015 (as of December) [Google Scholar]
- 4.Cañadas-De la Fuente G., Vargas C., Luis S.C., García I., Cañadas G., De la Fuente E. Risk factors and prevalence of burnout syndrome in the nursing profession. Int J Nur Stud. 2015;52:240–249. doi: 10.1016/j.ijnurstu.2014.07.001. [DOI] [PubMed] [Google Scholar]
- 5.Norlund S., Reuterwall C., Höög J., Lindahl B., Janlert U., Birgander L.S. Burnout, working conditions and gender–results from the northern Sweden MONICA Study. BMC P Health. 2010;10:326. doi: 10.1186/1471-2458-10-326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Jones F., Fletcher B. Job control and health. In: Schabracq M.J., Winnubst J.A.M., Cooper C.L., editors. Handbook of work and health psychology. Wiley; Chichester, England: 1996. pp. 33–50. [Google Scholar]
- 7.Demerouti E., Bakker A.B., Nachreiner F., Schaufeli W.B. The job demands resources model of burnout. J Appl Psychol. 2001;86:499–512. [PubMed] [Google Scholar]
- 8.Nunes I.L. FAST ERGO-X: a tool for ergonomic auditing and work-related musculoskeletal disorders prevention. Work. 2009;34:133–148. doi: 10.3233/WOR-2009-0912. [DOI] [PubMed] [Google Scholar]
- 9.Kim S., Soergel D. Selecting and measuring task characteristics as independent variables. ASIS & T. 2005 [Google Scholar]
- 10.Kim M.G., Kim K., Ryoo J., Yoo S. Relationship between occupational stress and work-related musculoskeletal disorders in Korean male firefighters. Ann Occup Environ Med. 2013;25:9. doi: 10.1186/2052-4374-25-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Cole D.C., Ibrahim S., Shannon H.S. Predictors of work-related repetitive strain injuries in a population cohort. Am J Public Health. 2005;95:1233–1237. doi: 10.2105/AJPH.2004.048777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Park J., Jang S. Association between upper extremity musculoskeletal disorders and psychosocial factors at work: a review on the job DCS model's perspective. Saf Health Work. 2010;1:37–42. doi: 10.5491/SHAW.2010.1.1.37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Fonseca N.R., Fernandes R.C.P. Factors related to musculoskeletal disorders in nursing workers. Rev Latinoam Enferm. 2010;18:1076–1083. doi: 10.1590/s0104-11692010000600006. [DOI] [PubMed] [Google Scholar]
- 14.Krause N., Scherzer T., Rugulies R. Physical workload, work intensification, and prevalence of pain in low wage workers: results from a participatory research project with hotel room cleaners in Las Vegas. Am J Ind Med. 2005:1–12. doi: 10.1002/ajim.20221. [DOI] [PubMed] [Google Scholar]
- 15.Shaik R., Gotru C.K., Swamy C.G., Sandeep R. The prevalence of musculoskeletal disorders and their association with risk factors in auto rickshaw drivers - a survey in Guntur city. Int J Physiother. 2014;1:2–9. [Google Scholar]
- 16.Van Veldhoven M., Meijman T. NIA; Amsterdam: 1994. The measurement of psychosocial job demands. [Google Scholar]
- 17.Van Zyl, Van der Walt. HSRC; Pretoria: 1991. Manual for the experience of work and Life Circumstances questionnaire. [Google Scholar]
- 18.Kuorinka I., Jonsson B., Kilbom A., Vinterberg H., Biering-Sorensen F., Andersson G., Jorgensen K. Standardized Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987;18:233–237. doi: 10.1016/0003-6870(87)90010-x. [DOI] [PubMed] [Google Scholar]
- 19.Baron R.M., Kenny D.A. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51:1173–1182. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- 20.Aiken L.S., West S.G. Sage; Thousand Oaks, CA: 1991. Multiple regression: testing and interpreting interactions. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.