

Supplemental Digital Content is available in the text.
Keywords: patient transfer, registries, stroke, thrombectomy, time to treatment
Abstract
Background and Purpose—
To assess the effect of inter-hospital transfer on time to treatment and functional outcome after endovascular treatment (EVT) for acute ischemic stroke, we compared patients transferred from a primary stroke center to patients directly admitted to an intervention center in a large nationwide registry.
Methods—
MR CLEAN (Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands) Registry is an ongoing, prospective, observational study in all centers that perform EVT in the Netherlands. We included adult patients with an acute anterior circulation stroke who received EVT between March 2014 to June 2016. Primary outcome was time from arrival at the first hospital to arterial groin puncture. Secondary outcomes included the 90-day modified Rankin Scale score and functional independence (modified Rankin Scale score of 0–2).
Results—
In total 821/1526 patients, (54%) were transferred from a primary stroke center. Transferred patients less often had prestroke disability (227/800 [28%] versus 255/699 [36%]; P=0.02) and more often received intravenous thrombolytics (659/819 [81%] versus 511/704 [73%]; P<0.01). Time from first presentation to groin puncture was longer for transferred patients (164 versus 104 minutes; P<0.01, adjusted delay 57 minutes [95% CI, 51–62]). Transferred patients had worse functional outcome (adjusted common OR, 0.75 [95% CI, 0.62–0.90]) and less often achieved functional independence (244/720 [34%] versus 289/681 [42%], absolute risk difference −8.5% [95% CI, −8.7 to −8.3]).
Conclusions—
Interhospital transfer of patients with acute ischemic stroke is associated with delay of EVT and worse outcomes in routine clinical practice, even in a country where between-center distances are short. Direct transportation of patients potentially eligible for EVT to an intervention center may improve functional outcome.
Endovascular treatment (EVT) has been proven effective in patients with acute ischemic stroke (AIS) because of an intracranial large vessel occlusion (LVO) of the anterior circulation.1 The effect of EVT is highly time-dependent and a reduction in onset-to-treatment time increases the chance of good functional outcome for the patient.2,3
Studies focusing on workflow characteristics identified interhospital transfer as one of the main causes of treatment delay in the recent randomized controlled trials.4,5 Patients with AIS are often first presented at the nearest primary stroke center to provide rapid treatment with intravenous thrombolytics (IVT). If the diagnostic workup indicates eligibility for EVT, the patient is then transferred to an intervention center with facilities for EVT (drip-and-ship). Analysis of data from a US registry suggested that this drip-and-ship method increases time to treatment and decreases the odds of good functional outcome in daily clinical practice.6 However, the effect of inter-hospital transfer might be different in a more densely populated region with short between-center distances and a well-organized acute stroke care system.
We investigated the frequency of interhospital transfer and the characteristics of transferred patients in a large nationwide cohort in the Netherlands: MR CLEAN Registry (Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands). We aimed to assess the effect of interhospital transfer on time to treatment and functional outcome in routine clinical practice.
Methods
Study Design
Detailed methods of the MR-CLEAN Registry have been reported previously.7 The MR-CLEAN Registry is an ongoing, prospective, observational study in all centers that perform EVT in the Netherlands. Registration started in March 2014, directly after the final inclusion in MR-CLEAN. All 18 intervention centers in the Netherlands, of which 16 centers participated in the MR-CLEAN trial, registered their patients. All data were centrally collected and checked for completeness and consistency. The imaging assessment committee assessed imaging and the adverse event committee scored the safety parameters.
The central medical ethics committee of the Erasmus MC University Medical Center, Rotterdam, the Netherlands, evaluated the study protocol and granted permission to perform the study as a registry. Data will not be made available to other researchers as no patient approval has been obtained for sharing coded data. However, syntax and output files of statistical analyses are available from the corresponding author on reasonable request.
Study Population
All consecutive patients with AIS in the anterior and posterior circulation who received arterial groin puncture in the angiosuite have been registered. For the current analysis, we used data of patients treated between March 2014 to June 2016. We included patients adhering to the following criteria: age ≥18 years; treatment in a center that participated in the MR-CLEAN trial; and presence of an intracranial proximal arterial occlusion in the anterior circulation (intracranial carotid artery [ICA/ICA-T], middle cerebral artery [M1/M2] or anterior cerebral artery [A1/A2]), demonstrated by computed tomography (CT) angiography. EVT could consist of arterial catheterization followed by mechanical thrombectomy and thrombus aspiration, with or without delivery of a thrombolytic agent. Patients arrived either directly at the intervention center or were transferred from one of the primary stroke centers (Figure 1). Emergency Medical Services in the Netherlands identify potential stroke patients using the face, arm, speech test, and transport patients with an onset time of <6 hours to the closest stroke center with IVT and EVT facilities.
Figure 1.
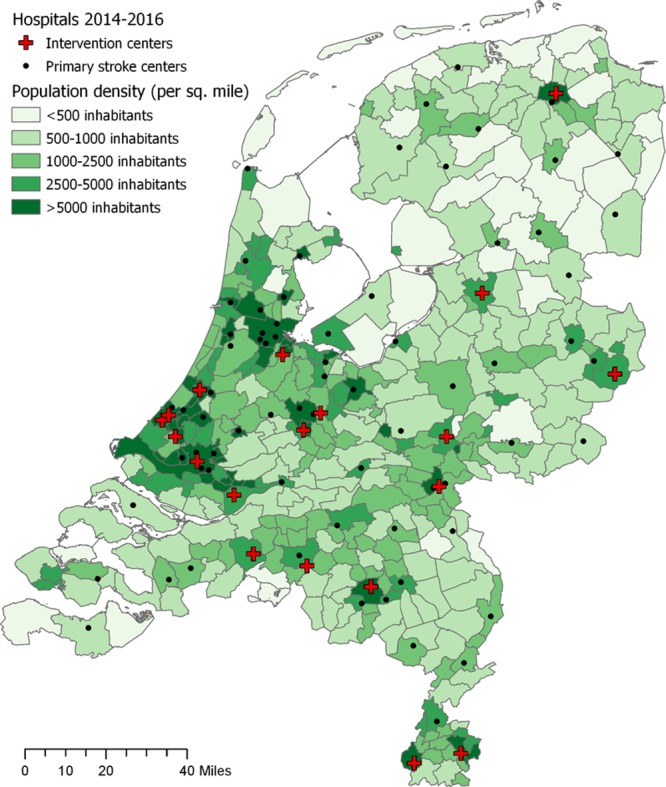
Map of the Netherlands including primary stroke centers, intervention centers, and population density.
Definitions and Outcome Measures
Time of stroke onset was defined as the moment of witnessed onset of stroke symptoms or, when exact onset was unknown, the moment that the patient was last seen well. Admission outside office hours was defined as time of arrival at the intervention center on working days between 5 pm and 8 am, during weekend days or national festive days. All transfer patients received a noncontrast CT in the primary stroke center, and most transfer patients received a CT-angiography before transfer to an intervention center. Imaging was not routinely repeated on arrival at the intervention center, but only in case of a clinical indication (eg, deterioration or substantial improvement). Imaging characteristics were assessed based on the first scan made (for transferred patients in the primary stroke center, for direct patients in the intervention center). Transfer-related travel time between each primary stroke center and the receiving intervention center was estimated using the TomTom MyDrive application (version 4.2.1.3495, available on https://mydrive.tomtom.com). A ratio of 0.85 was subsequently applied on each calculated time to approach the transfer-related travel time that an ambulance would actually need. This ratio is based on measured travel times of ambulances in a previous study in the Netherlands.8 The door in door out time in the primary stroke center was then estimated by subtracting the transfer-related travel time from the reported time from door of the primary stroke center to door of the intervention center.
Primary outcome was the time from first presentation to start of treatment, defined as the interval between arrival at the first hospital to arterial groin puncture. Secondary outcomes included: time from arrival at intervention center to groin puncture; time from stroke onset to groin puncture; the modified Rankin Scale (mRS) at 90 days after stroke; functional independence, defined as mRS score of 0–2; mortality at 90 days; successful reperfusion at the end of EVT, defined as an extended Thrombolysis in Cerebral Infarction score ≥2B9; and occurrence of symptomatic intracranial hemorrhage. Intracranial hemorrhage was defined as symptomatic if patients died or deteriorated neurologically (an increase of ≥4 points on National Institutes of Health Stroke Scale [NIHSS] score compared with NIHSS before worsening), and the hemorrhage was related to the clinical deterioration (according to the Heidelberg Bleeding Classification).10
Statistical Analysis
We compared patients transferred from a primary stroke center with patients who were directly admitted to an intervention center. Baseline characteristics were compared using χ2 test for categorical variables, independent samples t test for normally distributed continuous variables, and Mann-Whitney U test for nonnormal distributed continuous variables. Time intervals were expressed as medians with interquartile range. For regression analyses, missing data were imputed using multiple imputations by chained equations based on relevant covariates and outcome.
Linear regression analyses were used to assess the effect of transfer on time intervals. Prespecified adjustments were made for age, baseline NIHSS score, prestroke mRS score, treatment with IVT, hypertension (baseline systolic blood pressure >185 mm Hg and diastolic blood pressure >110 mm Hg), location of occlusion, Alberta Stroke Program Early CT Score on noncontrast CT, collateral score on CT angiography, the use of general anesthesia, and admission outside office hours. The effect of transfer on functional outcome was assessed using an ordinal logistic regression analysis for the shift in mRS score at 90 days. Binary logistic regression analyses were used for functional independence, mortality, successful reperfusion, and occurrence of symptomatic intracranial hemorrhage. These analyses were adjusted for the following prespecified variables: age, baseline NIHSS score, prestroke mRS score, history of ischemic stroke or transient ischemic attack, treatment with IVT, location of occlusion, Alberta Stroke Program Early CT Score, collateral score, and time from onset to first hospital.
All analyses were performed using R software (Version 3.4.4, R Foundation) with the rms package (version 5.1-2).
Results
In total, 1627 consecutive patients treated with EVT for AIS were included in the MR-CLEAN Registry between March 2014 and June 2016. We excluded 101 patients for the following reasons: age below 18 years (n=2); EVT performed in a non-MR-CLEAN center (n=20) and occlusion of the posterior circulation (n=79). The remaining 1526 patients were included in the analyses (Figure 2). Of these patients, 821 (53.8%) were transferred from a primary stroke center, and 705 (46.2%) were presented directly to an intervention center. The percentage of transferred patients ranged between 3.4% and 77% per intervention center.
Figure 2.
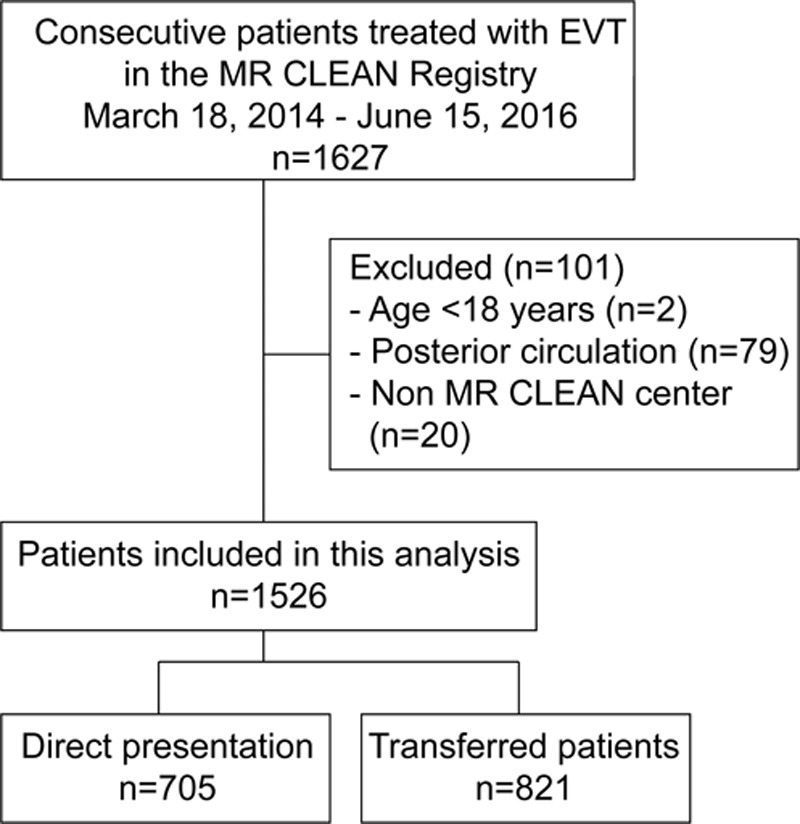
Flowchart of patient selection. EVT indicates endovascular treatment.
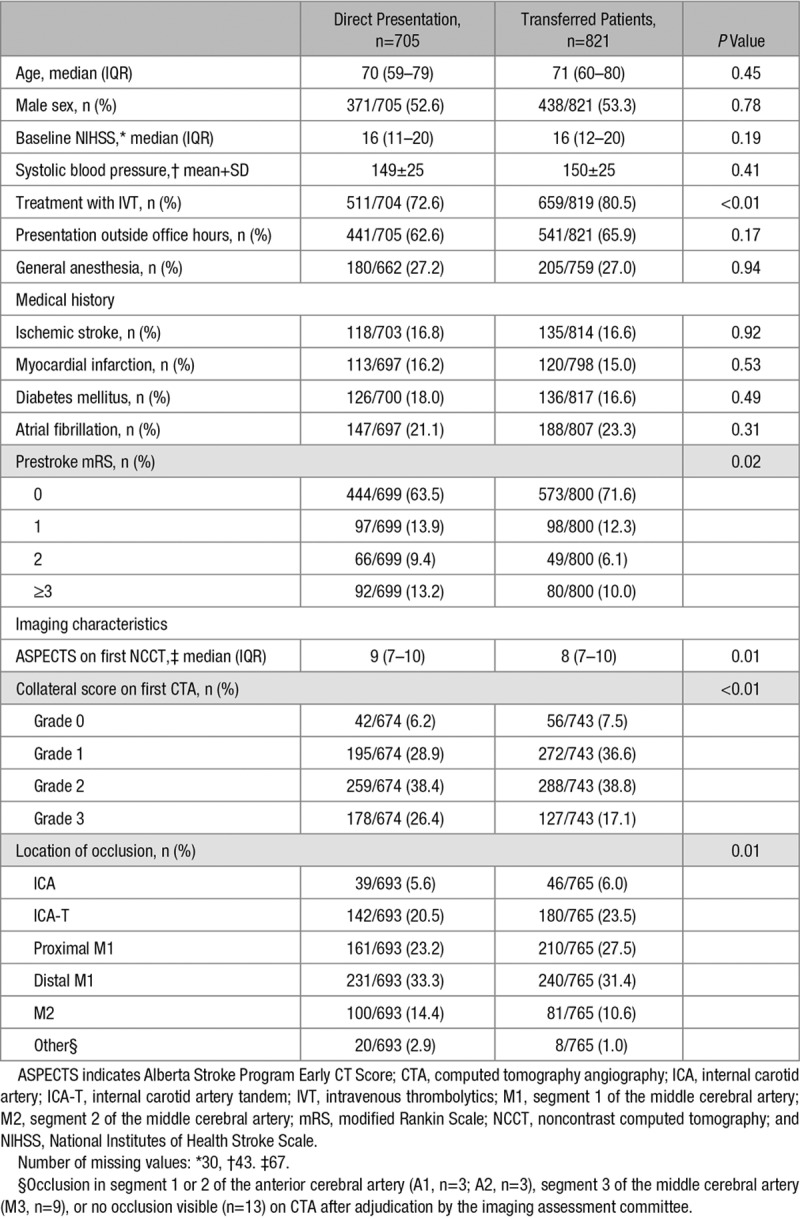
Baseline Characteristics
Demographics and baseline stroke severity were similar in both groups: median age was 71 years for transferred patients versus 70 years for directly admitted patients; 53% of all patients were men, and median NIHSS at baseline was 16 for both groups (Table 1). Transferred patients were more often treated with IVT (80.5% versus 72.6%; P<0.01) and had less often prestroke disability (mRS≥1, 28.4% versus 36.5%; P=0.02). Imaging characteristics were less favorable for transferred patients, with lower Alberta Stroke Program Early CT Score (median 8 versus 9; P=0.01) and more often absent or poor collaterals (collateral score 0–1, 44.1% versus 35.2%; P<0.01). Transferred patients less often had an occlusion of segment 2 of the middle cerebral artery (10.6% versus 14.4%; P=0.01). Imaging was repeated in 49/821 (6%) and 39/821 transfer patients (4.8%]) for noncontrast CT and CT-angiography, respectively.
Table 1.
Baseline Characteristics
Treatment Times
The median time from arrival at the first hospital to groin puncture was longer for transferred patients than for patients who were directly admitted to an intervention center (164 versus 104 minutes; P<0.01, Table 2). The adjusted difference was 57 minutes (95% CI, 51–62 minutes), in favor of patients who were admitted directly (Tables 3 and 4). After subtraction of the mean estimated transfer-related travel time (23 minutes), this time difference was 39 minutes. Transferred patients arrived slightly earlier after stroke onset at the first hospital (50 versus 55 minutes; P<0.01), but time from onset to arrival at the intervention center was much longer (174 versus 55 minutes; P<0.01). Median door-to-needle times for patients that received IVT were slightly longer for transferred patients (26 versus 24 minutes; P=0.02). Although the interval from arrival at the intervention center to start of treatment was shorter for transferred patients (47 versus 104 minutes; P<0.01, adjusted difference −58 minutes [95% CI, −62 to −54]), the total time from onset to groin puncture was still substantially longer in these patients (230 versus 170 minutes; P<0.01, adjusted difference 40 minutes [95% CI, 31 to 48]). The median duration of the endovascular procedure was similar in both groups (63 versus 62 minutes; P=0.79).
Table 2.
Treatment Times, Presented as Medians With Interquartile Range

Table 3.
Outcome Measures: Time Intervals

Table 4.
Outcome Measures: Clinical Outcomes

Clinical Outcome
There was a significant shift towards worse functional outcome in transferred patients (adjusted common odds ratio [OR] 0.75 [95% CI, 0.62–0.90]; Figure 3). Transferred patients less often achieved functional independence when compared with directly admitted patients (mRS 0–2, 33.9% versus 42.4%; absolute risk difference −8.5% [95% CI, −8.7 to −8.3]), also after (adjustment OR, 0.69 [95% CI, 0.54–0.89]; Tables 3 and 4). Mortality rates were not significantly different between the 2 groups (adjustment OR, 1.27 [95% CI, 0.97–1.66]). There were no significant differences in successful reperfusion rate (adjustment OR, 1.13 [95% CI, 0.91–1.39]) and occurrence of symptomatic intracranial hemorrhage (adjustment OR, 0.87 [95% CI, 0.56–1.36]).
Figure 3.
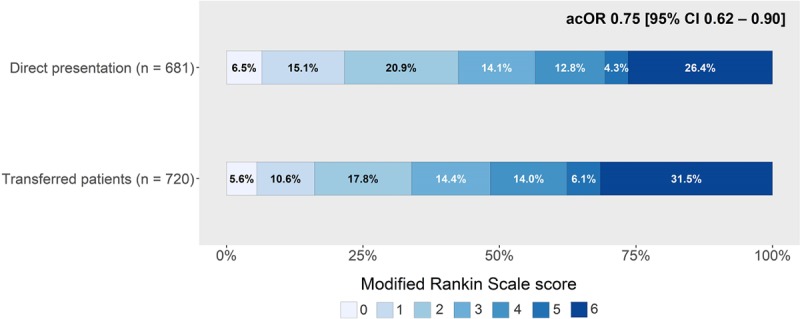
Functional outcome measured with the modified Rankin Scale score at 90 days. Functional outcome for patients presented directly in intervention center vs transferred from a primary stroke center (125 missing values). Transferred patients had worse functional outcomes than directly presented patients (adjusted common odds ratio [acOR] 0.75 [95% CI, 0.62–0.90]).
Discussion
In this large, nationwide cohort study, more than half of the patients with AIS treated with EVT were transferred from a primary stroke center. These patients had significant longer time intervals between first presentation and start of treatment, between symptom onset and start of treatment, and a lower chance of achieving good functional outcome. Even when we accounted for the travel time required to transfer a patient to an intervention center, start of treatment was still delayed by half an hour in transferred patients compared with patients who were directly admitted to an intervention center.
From earlier studies, we know that treatment delay translates to a decreased chance of achieving a favorable outcome.2 However, because of selection bias and time delay associated with informed consent procedures, data from randomized trials may not always reflect daily practice. The STRATIS Registry (Systematic Evaluation of Patients Treated With Neurothrombectomy Devices for Acute Ischemic Stroke) included 984 patients from a large region in the United States of America after the implementation of EVT as standard care.6 Similar to our study, the authors found that transferred patients had longer treatment times and worse functional outcomes when compared with direct admitted patients. However, their time analyses included only patients with successful reperfusion, which is not a fair representation of routine clinical practice. Also, distances between hospitals in rural areas of the USA are much larger than in our region, and time delays in primary hospitals—for instance because of initiation of IVT—are generally longer in the USA than in the Netherlands.8,11,12 Results from an earlier small study in a region with short distances, including only 1 primary stroke center and 1 intervention center, showed that treatment times were longer for transferred patients, and the difference between the 2 groups for functional outcome was similar to our study.13
The Netherlands is a small, densely populated country, with 82 hospitals that provide 24/7 acute stroke care. Approximately 99.8% of the Dutch population has the ability to reach an emergency department within 45 minutes.14 Our country has short between-center distances. This is emphasized by the fact that the mean transfer time was only 23 minutes, indicating that these results probably reflect the acute stroke care logistics in other highly populated regions. Although the observed in-hospital workflow times in this study were almost an hour shorter than in the MR-CLEAN trial in the Netherlands,15 there is still room for improvement. It has been suggested that increased experience, reflected in higher volumes of patients treated with EVT, leads to shorter treatment times and, subsequently, improved functional outcomes.16 Workflow times in our cohort do gradually decrease over time from 2014 until 2016. A decline in the median door-to-groin time (with the door of the first hospital as start) was observed for both transfer patients (187–149 minutes) and direct patients (123–97 minutes). However, the times achieved in our cohort are still longer when compared with other studies reporting workflow times. Additional interventions to optimize patient transfer management (eg, holding the initial ambulance primary stroke center until the decision of EVT eligibility has been made, streamlining transfer protocols, improving cloud-based image sharing, and transporting transfer patients directly to the angiosuite) might be useful to further reduce transfer-related delay in the future.17–20
Prehospital transportation of stroke patients suspected of LVO directly to an intervention center decreases time to EVT, but the potential harm of delaying IVT should be taken into account as well. We know, however, that the chance of achieving recanalization with IVT before thrombectomy in patients with LVO is low.21 Therefore, we should focus on finding an algorithm to predict LVO early, so that emergency medical services can present these patients directly to the intervention center.22,23 Implementing such a triage protocol has already shown to be feasible and seems to improve treatment times.24 One ongoing randomized trial in Catalonia, Spain, is evaluating the effect of the mothership versus the drip-and-ship strategy on functional outcome, among patients with a high likelihood of having a LVO identified with the RACE score (RACECAT [Direct Transfer to an Endovascular Center Compared to Transfer to the Closest Stroke Centre in Acute Stroke Patients With Suspected Large Vessel Occlusion], URL: https://www.clinicaltrials.gov. Unique identifier: NCT02795962). Although this trial will provide class I evidence on whether a mothership model improves functional outcome, it will be challenging to translate its results to regions with other geographic and demographic conditions. Modeling studies showed that differences in transportation times and treatment times affect the optimal transportation strategy and that triage protocols should, therefore, be based on regional characteristics and individual likelihood of LVO.25–28
There were a number of baseline imbalances between the 2 groups. First, transferred patients more often received IVT. One of the reasons that could explain this observation is that patients who passed the time window for IVT are probably more often directly transported to an intervention center. Second, transferred patients more often had proximal occlusions (ie, ICA, ICA-T, and proximal M1) when compared with directly admitted patients. It could be that physicians hesitate to transport a patient with a more distal occlusion towards the intervention center, as earlier studies showed that these occlusions generally respond well to IVT.29 Another observation that might be explained by a selection mechanism in the intervention center is that transferred patients less often had prestroke disability. This suggests that patients with favorable characteristics are more likely to be transferred to an intervention center. However, imaging characteristics, assessed at the hospital of first presentation, were slightly less favorable for transferred patients. After adjustment for these baseline imbalances, we still found an 8.5% decrease in the chance of achieving functional independence after interhospital transfer.
Strengths of our study include that the analyses were performed with data from one of the largest cohorts of consecutive patients treated with EVT, with individual patient data from all stroke intervention centers in the Netherlands. It strongly reflects daily clinical practice, including a relatively large number of transferred patients. A number of limitations also warrant comment. Despite the fact that the MR-CLEAN Registry is a nationwide study with consecutive inclusion of patients, our study is not completely free from a risk of selection bias. Patients with an LVO who did not receive EVT, for example, due to clinical improvement on arrival, were not included in the study. Some patients who were initially admitted to a primary stroke center may not have been transferred to an intervention center because the time window would have been passed by the moment they would arrive in the intervention center or because there was uncertainty about treatment eligibility in case of an M2 occlusion. These patients could have been treated if they had been transported directly to the intervention center. Since the MR-CLEAN Registry only contains data of patients who actually received EVT, we cannot estimate the size and impact of this patient population. The negative effect of a drip-and-ship strategy might, therefore, be larger in real life. Another limitation of our study is that we had no recorded door in door out times available to distinguish between in-hospital delay in the primary stroke center and delay because of the actual travel time between the primary stroke center and intervention center. We estimated the average interhospital travel times using the TomTom MyDrive application and then calculated the estimated door in door out times. Also, we used multiple imputation for time from first presentation to groin puncture, since time of arrival in the first hospital was missing for 13% of the patients. The difference between transferred patients and directly admitted patients in time from first presentation to groin puncture was comparable with the difference in time from onset to groin puncture, a variable that was available for all patients. We, therefore, believe that it has little impact on the validity of our results. Last, even though we adjusted for differences in prognostic factors, residual confounding might still influence our results.
Conclusions
In conclusion, these results from a large national cohort show that interhospital transfer of ischemic stroke patients eligible for EVT is associated with longer treatment times and worse functional outcome in clinical practice, even in a country where between-center distances are short. Direct transportation of EVT candidates to an intervention center might reduce treatment delay and thereby may improve functional outcome.
Sources of Funding
The Multicenter Randomized Clinical trial of EVT for AIS in the Netherlands (MR–CLEAN) Registry was partly funded by the Applied Scientific Institute for Neuromodulation (Toegepast Wetenschappelijk Instituut voor Neuromodulatie), the Erasmus University Medical Center, the Academic Medical Center Amsterdam, and the Maastricht University Medical Centre.
Disclosures
Academic Medical Center Amsterdam received funds from Stryker for consultations by C. Majoie and Y. Roos Erasmus University Medical Center received funds from Stryker and Bracco Imaging by D. Dippel. H. Marquering is co-founder and shareholder of Nico.lab. C. Majoie and Y. Roos own stock in Nico.lab. C. Majoie also reports research grants from the Applied Scientific Institute for Neuromodulation, the Dutch Heart Foundation, the European Commission and Stryker. D. Dippel received compensation for travel costs by Stryker and Medtronic. D. Dippel also reports research grants from Dutch Heart Foundation, Brain Foundation Netherlands, the Netherlands Organisation for Health Research and Development, and Health Holland Top Sector Life Sciences & Health, and unrestricted grants from AngioCare BV, Medtronic/Covidien/EV3, Medac Gmbh/Lamepro, Penumbra Inc, Stryker, Top Medical/Concentric, Thrombolytic Science LLC, and Stryker European Operations BV.
Supplementary Material
Footnotes
Drs Venema, Groot, Coutinho, and Roozenbeek contributed equally.
Guest Editor for this article was Natan M. Bornstein, MD.
The MR CLEAN Registry collaborators and corresponding affiliations are listed in the online-only Data Supplement.
The online-only Data Supplement is available with this article at https://www.ahajournals.org/doi/suppl/10.1161/STROKEAHA.118.024091.
References
- 1.Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM, et al. HERMES collaborators. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 2016;387:1723–1731. doi: 10.1016/S0140-6736(16)00163-X. doi: 10.1016/S0140-6736(16)00163-X. [DOI] [PubMed] [Google Scholar]
- 2.Saver JL, Goyal M, van der Lugt A, Menon BK, Majoie CB, Dippel DW, et al. HERMES Collaborators. Time to treatment with endovascular thrombectomy and outcomes from ischemic stroke: a meta-analysis. JAMA. 2016;316:1279–1288. doi: 10.1001/jama.2016.13647. doi: 10.1001/jama.2016.13647. [DOI] [PubMed] [Google Scholar]
- 3.Mulder MJHL, Jansen IGH, Goldhoorn RB, Venema E, Chalos V, Compagne KCJ, et al. MR CLEAN Registry Investigators. Time to endovascular treatment and outcome in acute ischemic stroke: MR CLEAN Registry results. Circulation. 2018;138:232–240. doi: 10.1161/CIRCULATIONAHA.117.032600. doi: 10.1161/CIRCULATIONAHA.117.032600. [DOI] [PubMed] [Google Scholar]
- 4.Menon BK, Sajobi TT, Zhang Y, Rempel JL, Shuaib A, Thornton J, et al. Analysis of workflow and time to treatment on thrombectomy outcome in the Endovascular Treatment for Small Core and Proximal Occlusion Ischemic Stroke (ESCAPE) Randomized, Controlled Trial. Circulation. 2016;133:2279–2286. doi: 10.1161/CIRCULATIONAHA.115.019983. doi: 10.1161/CIRCULATIONAHA.115.019983. [DOI] [PubMed] [Google Scholar]
- 5.Venema E, Boodt N, Berkhemer OA, Rood PPM, van Zwam WH, van Oostenbrugge RJ, et al. Workflow and factors associated with delay in the delivery of intra-arterial treatment for acute ischemic stroke in the MR CLEAN trial. J Neurointerv Surg. 2018;10:424–428. doi: 10.1136/neurintsurg-2017-013198. doi: 10.1136/neurintsurg-2017-013198. [DOI] [PubMed] [Google Scholar]
- 6.Froehler MT, Saver JL, Zaidat OO, Jahan R, Aziz-Sultan MA, Klucznik RP, et al. STRATIS Investigators. Interhospital transfer before thrombectomy is associated with delayed treatment and worse outcome in the STRATIS Registry (Systematic Evaluation of Patients Treated With Neurothrombectomy Devices for Acute Ischemic Stroke). Circulation. 2017;136:2311–2321. doi: 10.1161/CIRCULATIONAHA.117.028920. doi: 10.1161/CIRCULATIONAHA.117.028920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Jansen IGH, Mulder MJHL, Goldhoorn RB MR CLEAN Registry Investigators. Endovascular treatment for acute ischaemic stroke in routine clinical practice: prospective, observational cohort study (MR CLEAN Registry). BMJ. 2018;360:k949. doi: 10.1136/bmj.k949. doi: 10.1136/bmj.k949. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Groot AE, van Schaik IN, Visser MC, Nederkoorn PJ, Limburg M, Aramideh M, et al. Association between i.v. thrombolysis volume and door-to-needle times in acute ischemic stroke. J Neurol. 2016;263:807–813. doi: 10.1007/s00415-016-8076-5. doi: 10.1007/s00415-016-8076-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Goyal M, Fargen KM, Turk AS, Mocco J, Liebeskind DS, Frei D, et al. 2C or not 2C: defining an improved revascularization grading scale and the need for standardization of angiography outcomes in stroke trials. J Neurointerv Surg. 2014;6:83–86. doi: 10.1136/neurintsurg-2013-010665. doi: 10.1136/neurintsurg-2013-010665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.von Kummer R, Broderick JP, Campbell BC, Demchuk A, Goyal M, Hill MD, et al. The Heidelberg bleeding classification: classification of bleeding events after ischemic stroke and reperfusion therapy. Stroke. 2015;46:2981–2986. doi: 10.1161/STROKEAHA.115.010049. doi: 10.1161/STROKEAHA.115.010049. [DOI] [PubMed] [Google Scholar]
- 11.Bray BD, Campbell J, Cloud GC, Hoffman A, Tyrrell PJ, Wolfe CD, et al. Intercollegiate Stroke Working Party Group. Bigger, faster? Associations between hospital thrombolysis volume and speed of thrombolysis administration in acute ischemic stroke. Stroke. 2013;44:3129–3135. doi: 10.1161/STROKEAHA.113.001981. doi: 10.1161/STROKEAHA.113.001981. [DOI] [PubMed] [Google Scholar]
- 12.Fonarow GC, Smith EE, Saver JL, Reeves MJ, Bhatt DL, Grau-Sepulveda MV, et al. Timeliness of tissue-type plasminogen activator therapy in acute ischemic stroke: patient characteristics, hospital factors, and outcomes associated with door-to-needle times within 60 minutes. Circulation. 2011;123:750–758. doi: 10.1161/CIRCULATIONAHA.110.974675. doi: 10.1161/CIRCULATIONAHA.110.974675. [DOI] [PubMed] [Google Scholar]
- 13.Gerschenfeld G, Muresan IP, Blanc R, Obadia M, Abrivard M, Piotin M, et al. Two paradigms for endovascular thrombectomy after intravenous thrombolysis for acute ischemic stroke. JAMA Neurol. 2017;74:549–556. doi: 10.1001/jamaneurol.2016.5823. doi: 10.1001/jamaneurol.2016.5823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kommer GJ, Gijsen R, de Bruin-Kooistra M, Deuning C. Supply and accessibility of emergency hospital care in the Netherlands 2017: analysis of the geographical accessibility of hospitals. Rijksinstituut voor Volksgezondheid en Milieu RIVM. 2017;108:1–71. [Google Scholar]
- 15.Fransen PS, Berkhemer OA, Lingsma HF, Beumer D, van den Berg LA, Yoo AJ, et al. Multicenter Randomized Clinical Trial of Endovascular Treatment of Acute Ischemic Stroke in the Netherlands Investigators. Time to reperfusion and treatment effect for acute ischemic stroke: a randomized clinical trial. JAMA Neurol. 2016;73:190–196. doi: 10.1001/jamaneurol.2015.3886. doi: 10.1001/jamaneurol.2015.3886. [DOI] [PubMed] [Google Scholar]
- 16.Gupta R, Horev A, Nguyen T, Gandhi D, Wisco D, Glenn BA, et al. Higher volume endovascular stroke centers have faster times to treatment, higher reperfusion rates and higher rates of good clinical outcomes. J Neurointerv Surg. 2013;5:294–297. doi: 10.1136/neurintsurg-2011-010245. doi: 10.1136/neurintsurg-2011-010245. [DOI] [PubMed] [Google Scholar]
- 17.Ng FC, Low E, Andrew E, Smith K, Campbell BCV, Hand PJ, et al. Deconstruction of interhospital transfer workflow in large vessel occlusion: real-world data in the thrombectomy era. Stroke. 2017;48:1976–1979. doi: 10.1161/STROKEAHA.117.017235. doi: 10.1161/STROKEAHA.117.017235. [DOI] [PubMed] [Google Scholar]
- 18.McTaggart RA, Yaghi S, Cutting SM, Hemendinger M, Baird GL, Haas RA, et al. Association of a primary stroke center protocol for suspected stroke by large-vessel occlusion with efficiency of care and patient outcomes. JAMA Neurol. 2017;74:793–800. doi: 10.1001/jamaneurol.2017.0477. doi: 10.1001/jamaneurol.2017.0477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Jadhav AP, Kenmuir CL, Aghaebrahim A, Limaye K, Wechsler LR, Hammer MD, et al. Interfacility transfer directly to the neuroangiography suite in acute ischemic stroke patients undergoing thrombectomy. Stroke. 2017;48:1884–1889. doi: 10.1161/STROKEAHA.117.016946. doi: 10.1161/STROKEAHA.117.016946. [DOI] [PubMed] [Google Scholar]
- 20.Kansagra AP, Wallace AN, Curfman DR, McEachern JD, Moran CJ, Cross DT, 3rd, et al. Streamlined triage and transfer protocols improve door-to-puncture time for endovascular thrombectomy in acute ischemic stroke. Clin Neurol Neurosurg. 2018;166:71–75. doi: 10.1016/j.clineuro.2018.01.026. doi: 10.1016/j.clineuro.2018.01.026. [DOI] [PubMed] [Google Scholar]
- 21.Bhatia R, Hill MD, Shobha N, Menon B, Bal S, Kochar P, et al. Low rates of acute recanalization with intravenous recombinant tissue plasminogen activator in ischemic stroke: real-world experience and a call for action. Stroke. 2010;41:2254–2258. doi: 10.1161/STROKEAHA.110.592535. doi: 10.1161/STROKEAHA.110.592535. [DOI] [PubMed] [Google Scholar]
- 22.Heldner MR, Hsieh K, Broeg-Morvay A, Mordasini P, Bühlmann M, Jung S, et al. Clinical prediction of large vessel occlusion in anterior circulation stroke: mission impossible? J Neurol. 2016;263:1633–1640. doi: 10.1007/s00415-016-8180-6. doi: 10.1007/s00415-016-8180-6. [DOI] [PubMed] [Google Scholar]
- 23.Smith WS, Lev MH, English JD, Camargo EC, Chou M, Johnston SC, et al. Significance of large vessel intracranial occlusion causing acute ischemic stroke and TIA. Stroke. 2009;40:3834–3840. doi: 10.1161/STROKEAHA.109.561787. doi: 10.1161/STROKEAHA.109.561787. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Zaidi SF, Shawver J, Espinosa Morales A, Salahuddin H, Tietjen G, Lindstrom D, et al. Stroke care: initial data from a county-based bypass protocol for patients with acute stroke. J Neurointerv Surg. 2017;9:631–635. doi: 10.1136/neurintsurg-2016-012476. doi: 10.1136/neurintsurg-2016-012476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Holodinsky JK, Williamson TS, Demchuk AM, Zhao H, Zhu L, Francis MJ, et al. Modeling stroke patient transport for all patients with suspected large-vessel occlusion. JAMA Neurol. 2018;75:1477–1486. doi: 10.1001/jamaneurol.2018.2424. doi: 10.1001/jamaneurol.2018.2424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Schlemm E, Ebinger M, Nolte CH, Endres M, Schlemm L. Optimal transport destination for ischemic stroke patients with unknown vessel status: use of prehospital triage scores. Stroke. 2017;48:2184–2191. doi: 10.1161/STROKEAHA.117.017281. doi: 10.1161/STROKEAHA.117.017281. [DOI] [PubMed] [Google Scholar]
- 27.Benoit JL, Khatri P, Adeoye OM, Broderick JP, McMullan JT, Scheitz JF, et al. Prehospital triage of acute ischemic stroke patients to an intravenous tPA-ready versus endovascular-ready hospital: a decision analysis. Prehosp Emerg Care. 2018;22:722–733. doi: 10.1080/10903127.2018.1465500. doi: 10.1080/10903127.2018.1465500. [DOI] [PubMed] [Google Scholar]
- 28.Parikh NS, Chatterjee A, Díaz I, Pandya A, Merkler AE, Gialdini G, et al. Modeling the impact of interhospital transfer network design on stroke outcomes in a large city. Stroke. 2018;49:370–376. doi: 10.1161/STROKEAHA.117.018166. doi: 10.1161/STROKEAHA.117.018166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Seners P, Turc G, Maïer B, Mas JL, Oppenheim C, Baron JC. Incidence and predictors of early recanalization after intravenous thrombolysis: a systematic review and meta-Analysis. Stroke. 2016;47:2409–2412. doi: 10.1161/STROKEAHA.116.014181. doi: 10.1161/STROKEAHA.116.014181. [DOI] [PubMed] [Google Scholar]