

Abstract
Background
This study investigated how whole-body vibration (WBV), exercise, and their interactions influence core muscle activity in healthy young adults.
Material/Methods
Twenty-three healthy young adults (8 males and 15 females; age: 21.87±2.33 years) participated in the study. The activities of muscle multifidi (MM), rectus abdominis muscle (RM), erector spinae (ES), abdominis obliquus externus (AOE), and abdominis obliquus internus (AOI) were measured through surface electromyography (sEMG) while participants were performing 4 different exercise forms under 3 WBV conditions (condition 1: 5 Hz, 2 mm; condition 2: 10 Hz, 2 mm; and condition 3: 15 Hz, 2 mm) and a no-WBV condition in single experimental sessions.
Result
The WBV frequency of 15 Hz is the best vibration stimulation for core muscles in all of the exercises (P<0.05). Single bridge is a better exercise for RM and AOE (P<0.05) compared with other exercises, and crunches is the best exercise for MM, AOI, and ES (P<0.05). Significant interaction effect was observed in different frequencies and exercises (P>0.05) except for AOI (F=0.990, P=0.378).
Conclusions
High vibration frequencies can lead to enhanced exercise benefits within an appropriate frequency range, and different exercises have diverse effects on various muscles. Single bridge and crunches are appropriate exercise forms for lumbar-abdominal muscles.
MeSH Keywords: Abdominal Muscles, Back Muscles, Electromyography, Exercise, Vibration
Background
Whole-body vibration (WBV) training has been largely used in sports medicine and rehabilitation [1,2]. Vibration is a kind of oscillatory motion that physiologically stimulates the human body to induce changes and achieve treatment goals [3]. The basic principle of WBV is that subjects are susceptible to three-dimensional vibration stimulation when they stand on a vibrating platform. Vibration then stimulates muscle spindles and activates α-motoneurons [4]. Muscle contraction is often stimulated by a stretch reflex during vibration. WBV alternately stimulates momentary muscle relaxation and contraction, thereby activating muscle and nerve fibers and strengthening the neuromuscular system [5,6]. Therefore, WBV is utilized to improve various dysfunctions [7,8]. However, these studies have focused on the effects of vibration training in improving related functions, such as muscle strength and power [9], balance [10], bone health [11], or pain [12], and studies on the dose–effect relationship have been rarely performed. The human body experiences the effects of amplitude, vibration frequency, and exercise to trigger muscle activities when an individual stands on a vibrating platform [13], but most studies on WBV have considered only one parameter in testing protocols. Appropriate protocols and dose-response relationship have yet to be established because of lack of relevant research.
To address these knowledge gaps, we applied surface electromyography (sEMG) in this study to observe the recruitment of sEMG signals of the lumbar and abdominal muscles of subjects undergoing training on a vibration platform under different conditions. On the basis of previous studies [14–16], we hypothesized that: 1) a high vibration frequency enhances exercise benefits within an appropriate frequency range; 2) different exercise forms activate various lumbar and abdominal muscles; and 3) a significant interaction occurs between exercise and vibration frequency during lumbar and abdominal muscle activation.
Material and Methods
Subjects
Twenty-three healthy volunteers (8 males and 15 females; age: 21.87±2.33 years; weight: 60.21±9.83 kg; height: 168.33±8.52 cm) without any history of remarkable lumbar or lower limb problems and systemic or neurological diseases participated in this study. The exclusion criteria were: (i) prior experience of WBV training, (ii) participation in any systematic training programs at least 2 days per week, (iii) history of operation, severe trauma, and/or fracture, (iv) presence of musculoskeletal diseases, (v) any chronic diseases (e.g., diabetes mellitus and epilepsy), (vi) use of any medication that affects neuromuscular performance the last 2 weeks, and (vii) pregnancy. Demographic characteristics of the participants were obtained at baseline assessment. This study was approved by the Ethics Committee of Shanghai University of Sports, and all subjects gave their informed written consent before joining this study.
Experimental procedure
Equipment and devices
A WBV machine generating vertical vibration was used (AV-009; BodyGreen, Taiwan, China) at a vibration frequency range of 5–35 Hz and an amplitude of 2 mm. MyoResearch XP Master version 1.07.17 (Noraxon, Inc., Scottsdale, USA) was utilized to record the sEMG signals from the target muscles. The method of electrode attachment was based on the European Union recommendation standard.
Experimental program
WBV was administered at 3 different frequencies and 1 amplitude: 5 Hz, 2 mm; 10 Hz, 2 mm; and 15 Hz, 2 mm. The group without any vibration intensity was used to prepare for standardization. All of the subjects were required to practice 4 different exercises forms, producing a total of 16 testing conditions. In total, each exercise was performed for 130 s (4 times for 10 s each time with a 30-s break between each frequency), with a 5-min rest between exercises. While participants performed the exercises, we recorded the lumbar-abdominal muscles sEMG. The sequence of the vibration frequency and exercise performed was randomized for each individual participant to minimize the potential bias arising from order effect. The 4 exercise forms were as follows: (1) For single bridge, subjects flexed one leg and straightened the other leg. They then extended the hip and buttocks and maintained the position; (2) For planking, the patients held a push-up-like position with the body weight on the forearms, elbows, and toes, while keeping the trunk straight; (3) For side stay, they lay on the side and supported the body between the forearm and the knee to the feet; (4) For crunches, they maintained a supine position and curled the shoulders toward the pelvis, and could place their hands behind or beside the neck or crossed over the chest. The WBV group received WBV during the 4 types of exercises, while when no-WBV group performed exercises without WBV. The sEMG signal of the muscle multifidi (MM), rectus abdominis muscle (RM), erector spinae (ES), abdominis obliquus externus (AOE), and abdominis obliquus internus (AOI) of both sides were recorded using the Noraxon system.
Data were collected in a single experimental session, and all of the experimental processes were accomplished at the same test sites. Before the subjects began the test, they were instructed by the same therapist to adapt to the training process and repeat the training 3 times. The surface EMG signal of 10 s was recorded, and each training interval was 60 s [17].
EMG interference test
The subjects kept relaxed and sat next to the vibrator to collect the target muscle’s EMG signals for 10 s. The vibration frequencies were set as follows: 0 Hz, 0 mm; 5 Hz, 2 mm; 10 Hz, 2 mm; and 15 Hz, 2 mm. The RMSs of electromyography were calculated and examined by multiple comparison, and the results showed no significant difference between the groups, showing that the vibration instrument and the frequency regulation had no significant effect on the sEMG signal.
Data collection and analysis
EMG data were collected at 1000 Hz by using MyoResearch XP Master version 1.07.17 (Noraxon, Inc., Scottsdale, USA). Each of the 12 groups sustained exercise for 10 s and we recorded the original pyroelectric signal. The original muscle electrical signals from which the sEMG signal of the dominant side was selected were processed with a 10–500 Hz noise by utilizing MATLAB [18]. For the 4 static exercises, the middle 5 s of the data was used to calculate the EMG root mean square (RMS). The RMS represents muscle activation, and a large value indicates high levels of muscle activation [19]. For the standardization of sEMG data, the value of EMG rms under WBV was compared with the value of EMG rms under no-WBV, which was considered as the degree of muscle activity during WBV training [20].
Data analysis
Statistical analyses were performed with IBM SPSS version 20.0 (IBM, Armonk, NY). Data were reported as mean and standard error. A appropriate ANOVA model would offer information about: (1) The overall effect of vibrational frequency (whether any conspicuous difference in target muscles activation was observe amidst the 4 different frequencies measured), and one-way ANOVA was performed; (2) The primary effect of different exercise forms (whether any overall significant distinction in target muscles activation amidst the 4 exercise forms), and one-way ANOVA was performed; (3) Two-way ANOVA with repeated measures (within-subject factors: frequency, exercise) was used to explore the interaction effect between different vibration frequencies and exercise forms. The statistical significance level was set at p<0.05.
Results
Demographics
Twenty-three healthy volunteers (8 males and 15 females; age: 21.87±2.33 years; weight: 60.21±9.83 kg; height: 168.33±8.52 cm) were included in our study. All the participants had their demographic data recorded by the same physical therapist, and all the statistics are expresses as mean and standard deviation. Table 1 shows the muscle activities during different exercises with no-WBV training.
Table 1.
Muscle activation measured in the no-vibration condition.
| Single bridge | Plank | Side stay | Crunches | |
|---|---|---|---|---|
| MM | 44.41±16.74 | 7.55±2.33 | 29.69±13.59 | 19.42±14.51 |
| ES | 41.23±22.70 | 12.28±6.80 | 50.19±36.57 | 17.14±9.51 |
| AOE | 12.86±6.72 | 45.78±18.33 | 56.19±36.57 | 64.54±68.67 |
| AOI | 10.74±4.72 | 84.03±51.74 | 63.55±44.63 | 142.45±89.67 |
| RM | 15.50±23.65 | 69.91±46.15 | 70.20±111.59 | 113.39±132.13 |
Activity of MM
There were significant differences between diverse frequencies in single bridge (F=25. 406, P<0.001), plank (F=88.703, P<0.001), side stay (F=17.119, P<0.001), and crunches (F=6.802, P<0.001). In different exercises, significant differences were detected at 5 Hz (F=1.005, P=0.394), 10 Hz (F=5.459, P<0.001), and 15 Hz (F=6.376, P<0.001) (Figure 1). Then, the result of post hoc analysis indicated that the highest muscle activation of MM was observed in crunches with 15 Hz. Significant difference was discovered in the interaction effect of exercise and frequency (F=5.175, P<0.001), indicating that the benefit of WBV on MM was related to these 2 factors.
Figure 1.
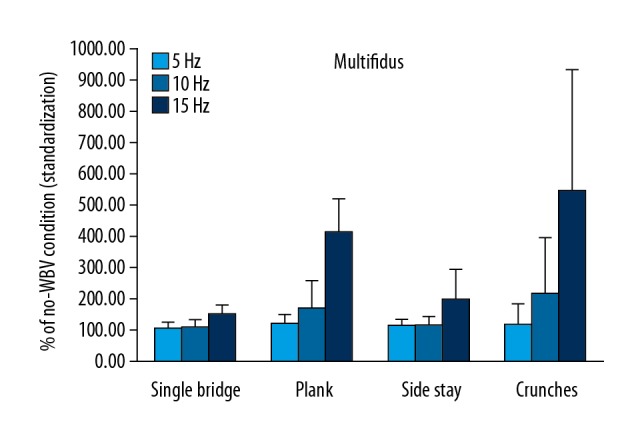
Muscle activity of MM induced by WBV.
Activity of RM
The effect of WBV on RM was significantly influenced by different exercises at all 3 frequencies. In different exercises, significant differences were detected at 5 Hz (F=2.435, P=0.070), 10 Hz (F=0.510, P=0.676), and 15 Hz (F=4.063, P=0.009) (Figure 2). The activation rate of RM was the highest when the vibration condition was 15 Hz with single bridge. Significant differences were discovered in the interaction effect of exercise and frequency (F=4.224, P=0.02).
Figure 2.

Muscle activity of RM induced by WBV.
Muscle activity of ES
The effect of WBV on ES was significantly affected at 15 Hz (F=4.625, P=0.005). Significant differences were detected between different frequencies in single bridge (F=4.267, P=0.018), plank (F=6.538, P=0.003), side bridge (F=5.723, P=0.005), and crunches (F=4.661, P=0.013) (Figure 3). The result of post hoc analysis indicated that the highest muscle activation of ES was observed in crunches with 15 Hz. Significant differences were observed in the interaction effect of exercise and frequency (F=3.054, P=0.020).
Figure 3.

Muscle activity of ES induced by WBV.
Muscle activity of AOE
The effect of WBV on AOE was significantly influenced by different exercises at all 3 frequencies. In different exercises, significant differences were detected at 15 Hz (F=18.987, P<0.001) (Figure 4). The result of post hoc analysis indicated that the highest muscle activation of AOE was observed in crunches with 15 Hz. The difference of exercise × frequency interaction effect was significant (F=9.806, P<0.001).
Figure 4.

Muscle activity of AOE induced by WBV.
Muscle activity of AOI
Significant differences were observed between various frequencies in single bridge (F=32.654, P<0.001), plank (F=4.729, P=0.012), and side stay (F=3.816, P=0.027) (Fig. 5). No significant differences were detected in various exercises at all 3 frequencies. The result of post hoc analysis indicated that the highest muscle activation of AOE was observed in single bridge with 15 Hz. The differences of exercise × frequency interaction effect were not significant (F=0.990, P=0.378).
Figure 5.

Muscle activity of AOI induced by WBV.
Discussion
This study aimed to explore the effects of WBV on lumbar and abdominal muscle activities during common static core muscle exercises. This study could provide important insights into the effects of complex interactions between exercise and vibration frequencies on lumbar and abdominal muscle activities through a combination of various vibration parameters.
Effects of different frequencies on lumbar and abdominal muscles
Results of our study powerfully support the first hypothesis that high WBV frequencies could effectively induce lumbar and abdominal muscle activities in all of the exercises. The activation rate of all muscles was the highest when the vibration frequency was 15 Hz. The body of an individual is susceptible to low-frequency–low-amplitude mechanical stimuli via a vibrating platform during WBV. Vibration stimulates muscle spindles and sends a nerve impulse to initiate muscle contractions through a tonic vibration reflex [21]. This finding is in agreement with the results of some related studies. For example, Desai [22] reported that the activation rates (RMS% MVC) of RM, AOE, and ES in an unstable plane are significantly higher than those in a stable plane in healthy people and patients with low back pain. Simsek [23] designed an experiment to verify the effects of vertical WBV on the EMG signal responses of leg muscle activities and showed a high-percentage increase in EMG activation at high frequencies (maximum of 40 Hz) and amplitude (4 mm; p < 0.05). Muscles usually need to use more energy to maintain balance in an unstable plane, and the RMSs of EMG increase [24,25]. In addition, Stania [26] also found that synchronous high-intensity WBV of long duration significantly enhances the activation of the pelvic floor muscles in young continent women. Therefore, our experimental results revealed that 15 Hz was the best frequency of vibration training in all the chosen frequencies.
Effects of different exercises on lumbar and abdominal muscles
The results showed that the single bridge is a better exercise for RM and AOI, whereas crunches are more suitable for MM, ES, and AOE. MM and ES are both back muscles, while RM, AOE, and AOI are abdominal muscles. All of these muscles maintain the stability of the spine, but the best exercises for them vary because of their anatomical characteristics. The MM is made up of a number of fleshy and tendinous fasciculi, which are composed of a groove on either side of the spinous processes of the vertebrae from the sacrum to the axis. Deep in the spine, the MM spans 3 joint segments and stabilizes the joints at each segmental level; although it is a thin muscle, it is essential for spinal stability. Pre-contraction of MM when starting crunches is needed to assure spinal stability [27,28]. The muscular fibers of the ES form a large fleshy mass that splits in the upper lumbar region into 3 columns – a lateral (iliocostalis), an intermediate (longissimus), and a medial (spinalis); it straightens the back and allows side-to-side rotation [29,30]. The ES contracts to maintain the longitudinal stability of the spine and resists the gravity of the side of the body to maintain lateral stability, so more motor units should be raised to keep the neutral position and prevent lateral flexion of the spine [31]. In general, single bridge and crunches are good exercise forms for back muscles. Pre-contraction of MM when starting crunches contributes to a stable spine. With the flexion of the spine, the pelvis begins to tilt forward, and this action requires a simultaneous contraction of the hip flexors and the ES. To maintain the stability of the spine, the MM contracts effectively when subjects are performing the crunches, and the ES contracts to help the MM maintain stability at this point.
In general, crunches are the best exercise form for abdominal muscles (RM, AOE, and AOI), and it also showed a wonderful effect on abdominal muscles, especially for AOE, according to the results. In addition, RM and AOI show a better activation rate when performing single bridge training. The RM is a pair of muscles that move vertically on both sides of the front wall of the human abdomen. The AOE is located on the lateral and anterior parts of the abdomen. It is a broad, thin, and irregularly quadrilateral muscle whose muscular portion holds the side. Its aponeurosis is in the anterior wall of the abdomen, and the AOI is deep below the AOE. The RM is an important postural muscle [32] that is in charge of flexing the lumbar spine, as in a crunches. AOE and AOI assist in the process, contribute to intra-abdominal pressure, and play an important role in respiration during forceful exhalation [33]. Intra-abdominal pressure should be increased when the abdomen is rolled up. In this process, abdominal muscles must contract to maintain the inner stability of the core area. The single bridge requires flexing one leg and straightening the other leg, then extending the hip and buttocks and maintaining the position. It should be noted that when performing bridge exercise exercises, the abdomen is topped up by the core muscles. Therefore, abdominal muscles can maintain strong contraction during single bridge training.
In addition, two-way ANOVA with repeated measures revealed significant findings, indicating that interaction effects were observed in different frequencies and exercises. Thus, hypothesis 3 was supported by the results.
Clinical implications
Our study results have certain clinical implications. First, WBV can effectually increase lumbar-abdominal muscle activation rate in healthy adults, showing that it might be a useful adjunct intervention to improve muscle activity, including but not restricted to strength, proprioception, and flexibility [34–36]. Considering the characteristic of WBV training, we observed that it is a convenient, effective exercise form that can be performed at home. Applying WBV can effectively increase muscle activity, even in a simple static exercise.
Second, we should find the best combination of vibration intensity and exercises because a significant interaction effect was detected in different frequencies and exercises. Our results indicated that the combination of the vibration intensity of 15 Hz and 2 mm and exercise of single bridge or crunches would be the best choice for improving lumbar-abdominal muscle activation rate. Further research is needed to explore more effective vibration combinations.
Limitations
First, the results of this study can only be generalized to healthy young adults (age: 21.87±2.33 years), and the experimental results cannot fully reflect the situation of healthy subjects at different ages. Second, we only chose 4 static exercise forms to test, and appropriate dynamic exercise forms should be further explored. Third, a Notch filter was applied to minimize relevant artifacts, but it unavoidably eliminated the actual muscle activity signals at a particular frequency. To allow impartial contrasts, we should subject all muscle activity signals to the same filtering process.
Conclusions
A high vibration frequency can lead to enhanced exercise benefits within an appropriate frequency range, and different exercises have various effects on different muscles. Single bridge is an appropriate exercise for RM and AOI, and crunches appear to be the best activator of MM, ES, and AOE. To explore the effects of exercising, we should further investigate additional training parameters of WBV and include healthy subjects and patients suffering from various conditions, such as low back pain, in future studies.
Footnotes
Source of support: The National Natural Science Foundation of China (81501956, 81871844); Fok Ying-Tong Education Foundation of China (161092); Shanghai Municipal Commission of Health and Family Planning (201840346); Shanghai Key Lab of Human Performance (Shanghai University of Sport) (no: 11DZ2261100); “Shuguang Program” supported by Shanghai Education Development Foundation and Shanghai Municipal Education Commission (18SG48); and the Natural Science Foundation of the Jiangsu Higher Education Institutions of China (18KJD320003)
References
- 1.da Costa KSA, Borges DT, de Brito Macedo L, et al. Whole-body vibration on performance of quadriceps after ACL reconstruction: A blinded randomized controlled trial. J Sport Rehabil. 2017;5:1–24. doi: 10.1123/jsr.2017-0063. [DOI] [PubMed] [Google Scholar]
- 2.Morel DS, Dionello CDF, Moreira-Marconi E, et al. Relevance of whole-body vibration exercise in sport: A short review with soccer, diver and combat sport. Afr J Tradit Complement Altern Med. 2017;14:19–27. doi: 10.21010/ajtcam.v14i4S.3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Stania M, Juras G, Słomka K, et al. The application of whole-body vibration in physiotherapy – A narrative review. Physiol Int. 2016;103:133–45. doi: 10.1556/036.103.2016.2.1. [DOI] [PubMed] [Google Scholar]
- 4.Monazzam MR, Shoja E, Zakerian SA, et al. Combined effect of whole-body vibration and ambient lighting on human discomfort, heart rate, and reaction time. Int Arch Occup Environ Health. 2018;91:537–45. doi: 10.1007/s00420-018-1301-z. [DOI] [PubMed] [Google Scholar]
- 5.Alam MM, Khan AA, Farooq M. Effect of whole-body vibration on neuromuscular performance: A literature review. Work. 2018;59:571–83. doi: 10.3233/WOR-182699. [DOI] [PubMed] [Google Scholar]
- 6.Prisby RD, Lafage-Proust MH, Malaval L, et al. Effects of whole-body vibration on the skeleton and other organ systems in man and animal models: What we know and what we need to know. Ageing Res Rev. 2008;7:319–29. doi: 10.1016/j.arr.2008.07.004. [DOI] [PubMed] [Google Scholar]
- 7.Maeda N, Urabe Y, Sasadai J, et al. Effect of whole-body vibration training on trunk-muscle strength and physical performance in healthy adults: Preliminary results of a randomized controlled trial. J Sport Rehabil. 2016;25:357–63. doi: 10.1123/jsr.2015-0022. [DOI] [PubMed] [Google Scholar]
- 8.Ye J, Ng G, Yuen K. Acute effects of whole-body vibration on trunk muscle functioning in young healthy adults. J Strength Cond Res. 2014;28:2872–79. doi: 10.1519/JSC.0000000000000479. [DOI] [PubMed] [Google Scholar]
- 9.Delecluse C, Roelants M, Verschueren S. Strength increase after whole-body vibration compared with resistance training. Med Sci Sports Exerc. 2003;35:1033–104. doi: 10.1249/01.MSS.0000069752.96438.B0. [DOI] [PubMed] [Google Scholar]
- 10.Goudarzian M, Ghavi S, Shariat A, et al. Effects of whole-body vibration training and mental training on mobility, neuromuscular performance, and muscle strength in older men. J Exerc Rehabil. 2017;13:573–80. doi: 10.12965/jer.1735024.512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Saquetto MB, Pereira FF, Queiroz RS, et al. Effects of whole-body vibration on muscle strength, bone mineral content and density, and balance and body composition of children and adolescents with Down syndrome: A systematic review. Osteoporos Int. 2018;29:527–33. doi: 10.1007/s00198-017-4360-1. [DOI] [PubMed] [Google Scholar]
- 12.Kaeding TS, Karch A, Schwarz R, et al. Whole-body vibration training as a workplace-based sports activity for employees with chronic low-back pain. Scand J Med Sci Spor. 2017;27:2027–39. doi: 10.1111/sms.12852. [DOI] [PubMed] [Google Scholar]
- 13.Kiiski J, Heinonen A, Järvinen TL, et al. Transmission of vertical whole-body vibration to the human body. J Bone Miner Res. 2008;23:1318–25. doi: 10.1359/jbmr.080315. [DOI] [PubMed] [Google Scholar]
- 14.Lam MH, Liao LR, Kwok CY, et al. The effect of vertical whole-body vibration on lower limb muscle activation in elderly adults: Influence of vibration frequency, amplitude and exercise. Maturitas. 2016;88:59–64. doi: 10.1016/j.maturitas.2016.03.011. [DOI] [PubMed] [Google Scholar]
- 15.Esmaeilzadeh S, Akpinar M, Polat S, et al. The effects of two different frequencies of whole-body vibration on knee extensors strength in healthy young volunteers: A randomized trial. J Musculoskel Neuron. 2015;15:333–40. [PMC free article] [PubMed] [Google Scholar]
- 16.Lienhard K, Vienneau J, Nigg S, et al. Older adults show higher increases in lower-limb muscle activity during whole-body vibration exercise. J Biomech. 2017;52:55–60. doi: 10.1016/j.jbiomech.2016.12.009. [DOI] [PubMed] [Google Scholar]
- 17.Ebadi S, Ansari NN, Naghdi S, et al. Surface electromyography of the paravertebral muscles in patients with chronic low back pain. J Back Musculoskelet Rehabil. 2013;26:221–26. doi: 10.3233/BMR-130380. [DOI] [PubMed] [Google Scholar]
- 18.Perchthaler D, Hauser S, Heitkamp HC, et al. Acute effects of whole-body vibration on trunk and neck muscle activity in consideration of different vibration loads. J Sports Sci Med. 2015;14:155–62. [PMC free article] [PubMed] [Google Scholar]
- 19.Guo SX, Pang MY, Gao BF, et al. Comparison of sEMG-based feature extraction and motion classification methods for upper-limb movement. Sensors. 2015;15:9022–38. doi: 10.3390/s150409022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Lam FMH, Liao LR, Kwok TCY, et al. The effect of vertical whole-body vibration on lower limb muscle activation in elderly adults: Influence of vibration frequency, amplitude and exercise. Maturitas. 2016;88:59–64. doi: 10.1016/j.maturitas.2016.03.011. [DOI] [PubMed] [Google Scholar]
- 21.Cardinale M, Bosco C. The use of vibration as an exercise intervention. Exerc Sport Sci Rev. 2003;31:3–7. doi: 10.1097/00003677-200301000-00002. [DOI] [PubMed] [Google Scholar]
- 22.Desai I, Marshall PW. Acute effect of labile surfaces during core stability exercises in people with and without low back pain. J Electromyogr Kinesiol. 2010;20:1155–62. doi: 10.1016/j.jelekin.2010.08.003. [DOI] [PubMed] [Google Scholar]
- 23.Simsek D. Different fatigue-resistant leg muscles and EMG response during whole-body vibration. J Electromyogr Kinesiol. 2017;37:147–54. doi: 10.1016/j.jelekin.2017.10.006. [DOI] [PubMed] [Google Scholar]
- 24.Cug M, Wikstrom EA, Golshaei B, et al. The effects of sex, limb dominance and soccer participation on knee proprioception and dynamic postural control. J Sport Rehabil. 2016;25:31–39. doi: 10.1123/jsr.2014-0250. [DOI] [PubMed] [Google Scholar]
- 25.Wang XQ. [The effect of core stability exercise on neuromuscular function for non-specific low back pain]. Shanghai University of Sport. 2016 [in Chinese] [Google Scholar]
- 26.Stania M, Chmielewska D, Kwaśna K, et al. Bioelectrical activity of the pelvic floor muscles during synchronous whole-body vibration: A randomized controlled study. BMC Urol. 2015;15:107. doi: 10.1186/s12894-015-0103-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Shao SZ, Zhang EZ, Fu S, et al. Morphological characteristics and functional significance of lumbosacral multifidus muscle. Chin J Clin Anat. 2010;28:17–19. [Google Scholar]
- 28.Sions JM, Coyle PC, Velasco TO, et al. Multifidi muscle characteristics and physical function among older adults with and without chronic low back pain. Arch Phys Med Rehab. 2017;98:51–57. doi: 10.1016/j.apmr.2016.07.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Daggfeldt K, Huang QM, Thorstensson A. The visible human anatomy of the lumbar erector spinae. Spine (Phila Pa 1976) 2000;25:2719–25. doi: 10.1097/00007632-200011010-00002. [DOI] [PubMed] [Google Scholar]
- 30.Paryavi E, Jobin CM, Ludwig SC, et al. Acute exertional lumbar paraspinal compartment syndrome. Spine. 2010;35:1529–33. doi: 10.1097/BRS.0b013e3181ec4023. [DOI] [PubMed] [Google Scholar]
- 31.Dong YL, Wang HF, Zheng YL, et al. Analysis of surface electromyography of lumbo-abdominal muscles in patients with chronic low back pain under different vibration conditions. Chin J Rehab Med. 2018;33:297–303. [Google Scholar]
- 32.Teyhen DS, Rieger JL, Westrick RB, et al. Changes in deep abdominal muscle thickness during common trunk strengthening exercises using ultrasound imaging. J Orthop Sports Phys Ther. 2008;38:596–605. doi: 10.2519/jospt.2008.2897. [DOI] [PubMed] [Google Scholar]
- 33.Hu JY, Chen BL, Dong YL, et al. Test-retest reliability of the intra-abdominal pressure by using pressure biofeedback. Chongqing Med. 2016;45:226–27. 231. [Google Scholar]
- 34.Rees SS, Murphy AJ, Watsford ML. Effects of whole-body vibration exercise on lower-extremity muscle strength and power in an older population: A randomized clinical trial. Phys Ther. 2008;88:462–70. doi: 10.2522/ptj.20070027. [DOI] [PubMed] [Google Scholar]
- 35.Kinser AM, Ramsey MW, O’Bryant HS, et al. Vibration and stretching effects on flexibility and explosive strength in young gymnasts. Med Sci Sports Exerc. 2008;40:133–40. doi: 10.1249/mss.0b013e3181586b13. [DOI] [PubMed] [Google Scholar]
- 36.Lai CC, Tu YKa, Wang TG, et al. Effects of resistance training, endurance training and whole-body vibration on lean body mass, muscle strength and physical performance in older people: A systematic review and network meta-analysis. Age Ageing. 2018;47:367–73. doi: 10.1093/ageing/afy009. [DOI] [PubMed] [Google Scholar]