

Introduction
Bladder cancer is one of the most common cancers of men between the ages of 60 and 70 years, but its occurrence in young pregnant female is very rare, with less than 50 cases reported so far. Herein we report a rare case of a patient presenting with a papillary transitional cell carcinoma of the urinary bladder in the second trimester of pregnancy. We describe the management dilemmas encountered and the treatment option selected to optimize outcome for the patient and neonate. Patient had an uneventful pregnancy outcome and no recurrence.
Case History
A 30-year-old non-smoking second gravida in second trimester of pregnancy was consulting for routine ANC in OPD. She was carrying dichorionic diamniotic twins. NT scan was normal, and she had no complaints till then. In the anomaly scan at 19 weeks of pregnancy, the ultrasonologist noticed a well-defined bladder polyp measuring 17 mm × 9 mm × 14 mm, post which she was counseled for cystoscopy but did not give consent for the same.
She followed up at 23 weeks of pregnancy with complaints of painless hematuria, nocturia and urinary frequency. She did not have dysuria, fevers, chills, nausea, vomiting, flank pain or weight loss. She denied any history of urinary tract infections or nephrolithiasis. No history of tobacco use or occupational or chemical exposure could be elicited (Fig. 1).
Fig. 1.

Ultrasound image at 19 weeks showing polyp
Physical examination revealed a uterus of 28 weeks’ size. The fetal parts were easily palpable, and fetal heart rates were normal for both diamniotic twins. Vaginal examination was normal. Blood tests including hemoglobin, hematocrit and coagulation studies were normal. Her urine showed microscopic hematuria. Ultrasound revealed bladder polyp of same size, on the posterior wall of the urinary bladder. Urine culture was sterile.
After intensive and multiple counselings, she agreed to get investigated for urinary bladder growth. Patient underwent cystoscopy at 26 weeks of gestation under general anesthesia with medicines glycopyrrolate (dose of 0.01 mg/kg), midazolam(0.05 mg/kg), fentanyl (2 mcg/kg), propofol (2 mg/kg). She was given injection of hydroxy progesterone intramuscularly (500 mg) pre-operative. A 1.5 cm × 2 cm papilliferous growth was found on the posterior wall with a narrow pedicle. Another small 1 cm × 2 cm papilliferous growth was also found on posterior wall. The trigone and the bladder neck were not involved, bilateral orifices had clear efflux of urine, and there were no other mucosal lesions. Using a 26 F resectoscope, complete transurethral resection (TUR) of the tumors was performed, including the detrusor and was sent for pathological examination, which showed a low-grade transitional cell carcinoma (TCC) with no muscle or lamina propria invasion (stage pTa).
Postoperatively she was put on uterine relaxant—Tab isoxsuprine 10 mg twice a day × 7 days and then once a day × 15 days. She was also put on micronized progesterone 300 mg vaginally × 15 days (Figs. 2, 3).
Fig. 2.

Ultrasound image post-TUR
Fig. 3.
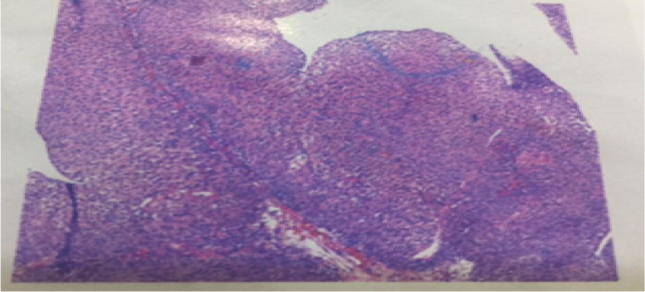
Histopathology
The patient continued her follow-up with no complaints. She went into labor at 35.5 weeks of gestation when she presented with preterm prelabor rupture of membrane (PPROM). She was induced and vaginally delivered twins—a baby girl and a baby boy. Her postnatal period was uneventful.
Post-delivery ultrasound (USG) was repeated. It was normal and showed no signs of any tumor.
She was advised regular follow-up.
Discussion
Urinary bladder cancer is rare in pregnancy, with one review identifying only 27 cases of non-bilharzial urinary bladder carcinoma in pregnant women, 74% presenting with TCC. However, in the general population, more than 90% of urinary bladder cancers are TCCs and more than 70% of all newly diagnosed urinary bladder cancers are superficial. Around 80–90% of patients with urinary bladder cancer present with painless hematuria [1]. In these women, delayed presentation is common because urinary symptoms in pregnancy are often ignored. Majority of times, the bleeding is mistaken for vaginal bleeding. Thus, examination is often performed to exclude placenta praevia, abruptio placentae or retained products following abortion or miscarriage. When recognized as hematuria, complete evaluation should be conducted and urinary bladder cancer considered in the differential diagnosis. Cystitis is the most common cause of hematuria in pregnancy. Although urinary bladder cancer is extremely rare in pregnancy, frank hematuria should be treated with a high index of suspicion. Bladder ultrasound [2] is very helpful in distinguishing the causes of bleeding and will show the urinary bladder filled with clots and frequently the tumor as well. Interestingly, in at least 7 cases this bleeding was mistaken for vaginal bleeding, and it was only subsequently clarified on catheterization or on ultrasonography that the cause of bleeding was a urinary bladder tumor. The importance of accurate history taking and careful clinical examination cannot be emphasized more.
A literature review has failed to find any evidence that pregnancy has deleterious effects on incidence or clinical course of urinary bladder malignancy compared to non-pregnant women of reproductive age. But since urological tumors are very rare in pregnancy, the diagnosis and management can be a challenge and sometimes the diagnosis of urinary bladder malignancy can be late in pregnancy due to confusion with the pregnancy-related symptoms
Flexible cystoscopy under local anesthesia is considered the most useful test in evaluating hematuria in pregnancy. TUR of the bladder tumor under regional or general anesthesia can be performed at any time during pregnancy [3].
The current recommendations for non-muscle invasive bladder tumors (Ta, T1 and Tis) include the diagnosis which mainly depends on cystoscopic examination, biopsy and urine cytology. To date, molecular urinary markers have not improved the combination of cystoscopy and cytology. The standard initial therapy for Ta and T1 papillary tumors is complete macroscopic TUR that includes a part of the underlying muscle, followed by a second TUR if there is a suspicion that the initial one was incomplete
Standard transurethral resection is effective when performed during pregnancy, bearing in mind the need to heed to the anesthetic risks inherent in any operative procedure during pregnancy. Outcome and prognosis after TUR are good. There are no reported cases in the literature about the instillation of mitomycin C for bladder cancer during any stage of pregnancy. One pregnant patient has been given intravesical BCG for bladder carcinoma in situ [4]. In the case of high-grade muscle invasive bladder cancer, delaying treatment until the baby is delivered at term would necessitate a high risk of disease progression and poor prognosis for the mother.
Conclusion
Limited experience has resulted in a paucity of information on the optimum management of pregnant women with cancer. However, reports of single cases or case studies have highlighted the difficult decisions needed and the potential conflict between the management of the tumor and the avoidance of harm to the fetus.
Finally, close collaboration between urologists, obstetricians and medical colleagues is needed for optimal, safe and effective management of bladder tumors during pregnancy.
Dr Shefali Tyagi
has been working as a consultant in Obstetrics and Gynaecology at Cloudnine Hospital, Bellandur (Bengaluru), since August 2017. She is interested in management of high-risk pregnancies.
Ethical Approval
All procedures performed on our patient were in accordance with the ethical standards of the institutional and/or national research committee.
Conflict of interest
Authors declare that there has been no conflict of interest.
References
- 1.Hosseini MM, Zeyghami S, Geramizadeh B. Management of bladder tumor in pregnancy: report a case and review of the literature. Middle East J Cancer. 2012;3(1):27–30. [Google Scholar]
- 2.Yeaton-Massey A, Brookfield KF, Aziz N, Mrazek-Pugh B, Chueh J. Maternal bladder cancer diagnosed at routine first-trimester obstetric ultrasound examination. Obstet Gynecol. 2013;122(2 Pt 2):464–467. doi: 10.1097/AOG.0b013e31828c5a4d. [DOI] [PubMed] [Google Scholar]
- 3.Shrotri KN, Ross GC. Bladder carcinoma presenting during twin pregnancy. J Obstet Gynaecol. 2008;28:750–751. doi: 10.1080/01443610802461813. [DOI] [PubMed] [Google Scholar]
- 4.Lakmichi Mohamed Amine, Zehraoui Reda, et al. Bladder cancer in the second trimester of pregnancy: tough decisions. A case report with review of the literature. Ther Adv Urol. 2012;4(3):139–142. doi: 10.1177/1756287212441961. [DOI] [PMC free article] [PubMed] [Google Scholar]