

Abstract
Development of systems for perinatal regionalization and for the provision of risk-appropriate maternal care is a key strategy to decrease maternal morbidity and mortality. Regionalized systems pertaining to neonatal care are broadly implemented in many states, but networks for risk-appropriate maternal care are lacking. In response to increases in maternal morbidity and mortality over the past decade, the American College of Obstetricians and Gynecologists (ACOG) and the Society for Maternal-Fetal Medicine (SMFM) developed and published the levels of maternal care guidelines in 2015. The guidelines are designed to promote collaboration among maternal facilities and health care providers with the goal that pregnant women receive care at a facility appropriate for their risk. The Centers for Disease Control and Prevention (CDC) developed the Levels of Care Assessment Tool in 2013 to assist states and jurisdictions in assessing maternal and neonatal levels of care in alignment with the national guidelines published by ACOG and SMFM and the American Academy of Pediatrics, respectively. With the goal of promoting levels of maternal care, ACOG and SMFM developed and piloted the levels of maternal care verification program. Fourteen facilities across three states (Georgia, Illinois, and Wyoming) participated in the pilot. A multidisciplinary team representing organizations with expertise in maternal risk-appropriate care performed an onsite comprehensive review of the maternal services available in each facility using the results from the CDC Levels of Care Assessment Tool as a previsit screening. A verification program that could be implemented on a local, state, or regional scale is being developed leveraging the lessons learned from the pilot.
Perinatal regionalization, also referred to as riskappropriate care, is a strategy for improving maternal and neonatal health outcomes and was first promoted by the March of Dimes in the 1976 report, “Toward Improving the Outcome of Pregnancy.”1 Risk-appropriate care provisions support women and neonates receiving care in a facility staffed with personnel and resources that matches their risk. In response to “Toward Improving the Outcome of Pregnancy,” states began to develop coordinated regional systems for perinatal care. In addition to facilities with a range of capabilities, these systems may include a regional (or tertiary) care center. Regional centers provide both the highest level of perinatal care and support facilities in their region with education, outreach, and maternal and neonatal transport.
Subsequent versions of “Toward Improving the Outcome of Pregnancy” and editions of the Guidelines for Perinatal Care broadened the focus to include comprehensive perinatal care and expanded definitions for levels of care based on the most recent available evidence.2,3 Neonatal levels of care currently classify facilities into levels I–IV based on functional capabilities and are organized within a tiered, regionalized system of neonatal care.4 Emphasis on improved neonatal outcomes based on specific interventions inadvertently resulted in a focus primarily on neonatal criteria and health. In an effort to encourage the same developments for maternal health, and amid concerns over increasing maternal morbidity and mortality in the United States,5,6 the American College of Obstetricians and Gynecologists (ACOG) and the Society for Maternal-Fetal Medicine (SMFM) published the levels of maternal care Obstetric Care Consensus in 2015.7 The structure of the newly developed levels of maternal care guidance is similar to the neonatal levels; each level (I–IV plus birth centers) describes minimum capabilities related to health care provider availability and facility resources (Box 1). Furthermore, this Obstetric Care Consensus provides guidance in which congruency between maternal and neonatal level is not the goal, but rather encourages and supports health care provided at a facility that best matches the risk of the woman and newborn independently.
Box 1. Levels of Maternal Care Definitions.
Birth Center
Peripartum care of low-risk women with uncomplicated term singleton pregnancies with a vertex presentation who are expected to have an uncomplicated delivery
Level I: Basic Care
Uncomplicated pregnancies with the ability to detect, stabilize, and initiate management of unanticipated problems that occur during the antepartum, intrapartum, or postpartum period until the patient can be transferred
Level II: Specialty Care
Level I facility plus care of appropriate high-risk conditions, both directly admitted and transferred from another facility
Level III: Subspecialty Care
Level II facility plus care of more complex maternal medical conditions, obstetric complications, and fetal conditions
Level IV: Regional Perinatal Center
Level III facility plus onsite medical and surgical care of the most complex maternal conditions and critically ill women and fetuses
CENTERS FOR DISEASE CONTROL AND PREVENTION LEVELS OF CARE ASSESSMENT TOOL
States and jurisdictions engaged in the Collaborative Improvement and Innovation Network to Reduce Infant Mortality identified maternal and neonatal riskappropriate care as one of six priority strategies.8 Specifically, this strategy aims to ensure that higher risk neonates and mothers receive care at a hospital with facilities and personnel appropriate for their needs. In an effort to effectively define and monitor levels of care among facilities, these jurisdictions collaborated with staff at the CDC to develop a tool that addressed the need for a user-friendly and standardized approach to assess facilities’ resources and capabilities for maternal and neonatal care.
The CDC Levels of Care Assessment Tool provides a means for jurisdictions to assess facility level of care in alignment with the 2015 ACOG and SMFM and 2012 American Academy of Pediatrics guidance specific to both maternal and neonatal care staffing and resource capabilities and encourages conversations among stakeholders in the provision of risk-appropriate care.4,7,9 To keep respondent burden to a minimum, the assessment tool is web-based and focuses on the criteria necessary to distinguish between levels of care. A maternal and a neonatal level of care are determined based on the overall responses.9 Interest in the tool has grown beyond jurisdictions participating in the Collaborative Improvement and Innovation Network to Reduce Infant Mortality and as of May 2018, 14 jurisdictions have chosen to implement the CDC Levels of Care Assessment Tool.
AMERICAN COLLEGE OF OBSTETRICIANS AND GYNECOLOGISTS LEVELS OF MATERNAL CARE VERIFICATION PROGRAM
In an effort to further support the vision of consistent interpretation of the 2015 guidelines, ACOG and SMFM invited the CDC, the National Perinatal Information Center, and the Arizona Perinatal Trust to form a multidisciplinary core team to develop a levels of maternal care verification program. A summary of the steps involved in the development and implementation of the verification program is provided in Figure 1. In addition to representatives from these organizations, clinicians representing the American Academy of Family Physicians, the American College of Nurse-Midwives, and the Association of Women’s Health, Obstetric and Neonatal Nurses were also included in the core team. This verification program involved a comprehensive onsite review to verify the maternal level of care of a hospital in alignment with ACOG and SMFM guidelines. In developing the verification program, the core team also aimed to expand on the work achieved with the Levels of Care Assessment Tool by using a hospital’s Levels of Care Assessment Tool results as the initial step in the verification process. The core team designed an assessment tool for the onsite review, which would also serve to corroborate the hospital’s Levels of Care Assessment Tool responses. The assessment tool was formatted as a checklist and patterned after the Obstetric Care Consensus criteria listed for each level of care. The assessment tool went through several iterations and was tested by one of the maternal– fetal medicine physicians in the core team at their facility. Several members of the core team also traveled to Arizona to attend a training session, including a mock site visit, led by the Arizona Perinatal Trust. The Arizona Perinatal Trust oversees a voluntary certification program for levels of care in Arizona, which matches hospital capabilities and capacity to established criteria through a self-assessment process and a site visit by a team of peer professionals.10
Fig. 1.
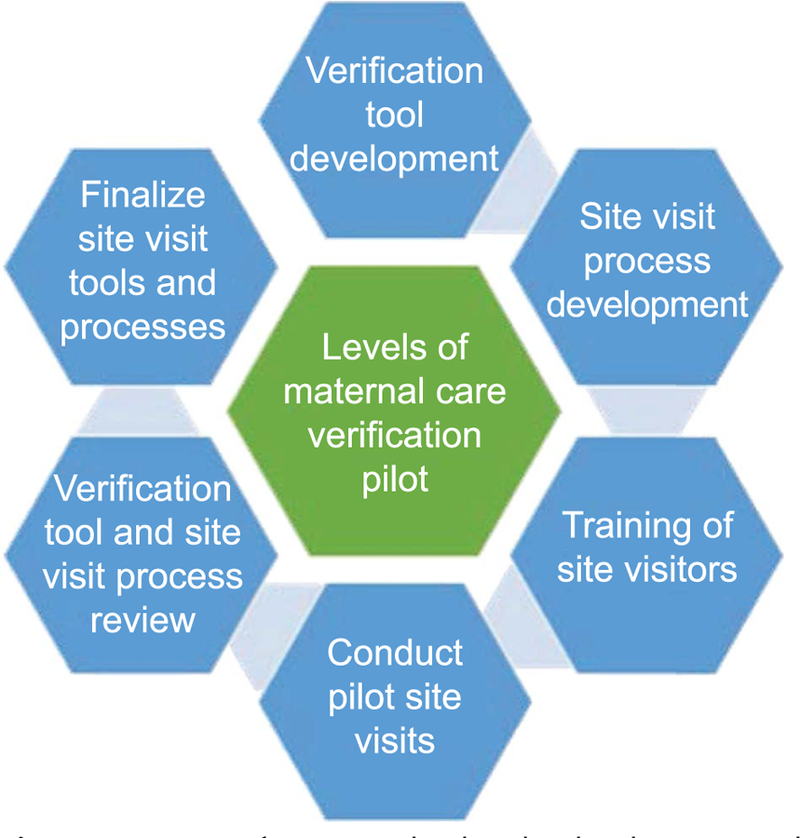
Summary of steps involved in the development and implementation of the levels of maternal care verification program. Zahn. Levels of Maternal Care Verification Pilot. Obstet Gynecol 2018.
The core team pilot-tested the verification program from March to September 2017 with 14 hospitals in three states. Based on their vested interest in risk-appropriate care and successful implementation of the Levels of Care Assessment Tool, the core team selected Georgia, Illinois, and Wyoming as the pilot states. These three states are geographically and demographically diverse and have approached levels of care in different ways, ranging from having no formal process for levels of care to an official designation process written into legislation. Staff at the CDC facilitated contact with the individuals who had championed the implementation of the Levels of Care Assessment Tool at the state health departments so that the core team could invite them to collaborate on this project. In turn, the state health departments either reached out to hospitals to gauge their interest in participating or suggested hospitals for ACOG to contact.
The American College of Obstetricians and Gynecologists worked with perinatal leadership at pilot facilities to plan a half-day onsite visit, and members of the core team conducted the visits. Each site visit team included a minimum of two clinicians (eg, obstetrician–gynecologist, maternal–fetal medicine subspecialist, certified nurse–midwife, family medicine physician, or all of these), and a staff member from ACOG. Other members of the core group participated in some visits, and representatives from the state’s ACOG District or Section, state department of health, and Association of Women’s Health, Obstetric and Neonatal Nurses, and a representative from CDC were invited to observe the visit.
The site visit pilot process involved previsit activities, including completion of forms and submission of policies and procedures documents by facilities. The site visit team reviewed these documents, along with the facility’s Levels of Care Assessment Tool results, before the scheduled visit. On site, the team introduced the levels of maternal care program to facility personnel, received an overview of the facility’s maternity services, and completed the assessment tool. Personnel at the facility who were typically involved in the site visit included the perinatal unit director, the obstetrics nurse manager (if different for the perinatal unit director), the chair or chief of the obstetric service, the director of maternal–fetal medicine services, as applicable, and, as applicable, representatives from the anesthesia service, certified nurse–midwife service, family medicine service if involved in providing obstetric care, and hospitalist service. Other participants included representatives from the intensive care unit and nursery or neonatal intensive care unit as applicable, and representatives from ancillary services, including laboratory, radiology, and pharmacy. Hospital leadership were also invited and participated, including the chief medical officer, chief nursing officer, and senior hospital administrators. The final part of the agenda included an informal discussion, in which the facility’s perinatal team shared their feedback on the site visit process and assessment tool and received highlights and recommendations from the site visit team on their maternal services. After the site visits, the facility received a report with their verified level of maternal care, highlights, and recommendations; the facility also was offered an optional follow-up phone conversation with the site visit team if the facility desired. Postvisit feedback was solicited from the members of the site visit teams as well as from the visited facilities.
LESSONS LEARNED
The level assessed using the responses from the Levels of Care Assessment Tool matched the level verified by the onsite review for 7 of the 14 levels of maternal care facilities (50%). With corrected information about a facility obtained during the levels of maternal care site visit, Levels of Care Assessment Tool–assessed levels matched the levels of maternal care–verified levels for the remaining seven facilities. Some areas in which the Levels of Care Assessment Tool did not match the onsite review included interpretation of the availability of obstetric ultrasonography, the availability of magnetic resonance imaging, and the interpretation of availability of maternal–fetal medicine subspecialists, primarily related to access to these physicians (through in-house presence or telephone consultation). By leveraging the experience of the pilots, the CDC identified a few primary challenges with obtaining correct information through the Levels of Care Assessment Tool. Respondents may inadvertently skip the instruction page and answer questions based on their own interpretation, which may differ from the intent. In some facilities, the tool was completed by one staff member, whose responses reflected their knowledge of the facility’s maternal services. The CDC staff has refined some of the wording on questions and enhanced the guidance for completion of the Levels of Care Assessment Tool. Facilities are now encouraged to employ a minimum of two individuals to review the responses before submission, ideally including a representative from both the neonatal and maternal units.
After the completion of the pilot visits, the core team gathered in Washington, DC, in November 2017 to review the levels of maternal care verification program, discuss lessons learned, and determine next steps. The team conducted a critical review of all documents (eg, previsit forms, assessment tool, and verification report) and updated them for use on a broader scale. Particularly related to the assessment tool, the pilot visits provided valuable insight into the potential challenges in the interpretation of some of the level-related criteria. Based on comments from facility staff, the team updated questions in the assessment tool that required clarification.
A key component of the visits was the informal feedback session scheduled at the end. Although strategically included in the agenda for the site visit team and the facility personnel to share comments about the levels of maternal care application and site visit process, it evolved into more crucial conversations about best practices, clinical guidelines, and policies and procedures. The specific conversations varied based on the facility, geographic location, and capabilities, but clinicians on the site visit team provided consultative advice and suggested resources for improving patient care. The staff at level I and II hospitals identified this portion of the site visit as extremely useful and equated it to a complimentary consultation. These discussions highlighted geographic differences and idiosyncrasies between states and the innovative mechanisms created to accommodate such differences. For example, weather in Wyoming can make travel virtually impossible in the winter, necessitating ongoing temporizing care that includes using the state police to procure and deliver blood products. In Georgia, one rural acute care hospital is using telemedicine, through the obstetrician–gynecologist’s office, for fetal assessment consultation by maternal–fetal medicine specialists who are at a higher level hospital. This helps to decrease patient travel and support care at a facility with fewer resources. Additionally, during this discussion, the facility’s perinatal and leadership teams shared their challenges with interpreting and applying the levels of maternal care guidance. Many of the clinicians on the site visit team work at level III and IV facilities, so these discussions helped them better understand the challenges experienced by level I and II facilities. All ACOG clinical guidance documents, including the Obstetric Care Consensus series, undergo rigorous periodic review, and this feedback will be included as part of the review for the levels of maternal care Obstetric Care Consensus.
During the site visits, team members identified a number of resources, including quality improvement and patient safety activities, detailed policies and procedures, staff training and education, and comprehensive nursing competency checklists that could be advantageous to share with other hospitals. The American College of Obstetricians and Gynecologists plans to reach out to the pilot hospitals to request permission to share these resources, and, if approved to use, these resources could be maintained in a repository for other facilities to access. With further implementation of levels of maternal care programs, resources identified as potentially useful could be vetted and added to this repository and serve as a valuable resource library for facilities to use in addressing capabilities related to levels of care. All the pilot facilities were appreciative for having the opportunity to participate in the pilot, share their recommendations for improving the verification program, and receive suggestions for improving patient care.
NEXT STEPS
The core team will develop a “toolkit” for a levels of maternal care verification program that could be implemented on a local, state, or regional scale. This toolkit will contain the forms and documents developed for the verification program and subsequently revised based on the experiences from the pilot, including the onsite assessment tool. Use of these resources would help support implementation of a levels of maternal care program by a health care system or a state-based department of health as well as facilitate communication and collaboration between facilities and systems to achieve regionalized maternal care. It is anticipated that the toolkit will be available in the fall of 2018. Experiences with the pilot underscored the importance of relationship-building between hospitals with different capabilities to establish trust and facilitate the best maternal care by matching a woman’s medical needs with an appropriately resourced hospital.
Another objective of a levels of maternal care program is to develop a centralized “resource site” to aid hospitals in addressing potential challenges and barriers related to implementation of a levels of care program and meeting level-specific criteria. This site will provide an opportunity to share hospital policies, procedures, and other lessons learned related to maternal health. In addition, an “implementation guide” is being developed to address the most common challenges or questions related to implementation. Although the previously described toolkit will be available to aid with development of a verification program, the “implementation guide” is designed to help facilities address level-specific criteria. It is anticipated that this implementation guide would serve as a companion resource to the Obstetric Care Consensus.
The interest in levels of maternal care is clearly growing. Members of the core team have been approached by regional and state health departments and hospital systems interested in the verification program. Several states, including Georgia, Indiana, and Texas, have passed legislation establishing maternal level of care designation for all hospitals providing maternity care.11–13 This reflects the growing national momentum toward improving maternal health and decreasing poor outcomes. With further implementation of levels of care programs, research will be critical to assess the effect of levels of care systems on maternal health outcomes, to help further refine and clarify criteria assigned to levels, and to address costeffectiveness.
DISCUSSION
Levels of maternal care is one piece of a complex puzzle that must be solved to ensure women are receiving the care they need and deserve. Reducing maternal morbidity and mortality is a multifaceted challenge, but ensuring that women are able to access the facility best able to care for her based on her risk factors, complications, and comorbidities is essential. Barriers to accessing the most appropriate levels of care must be overcome. The American College of Obstetricians and Gynecologists, SMFM, and the CDC will continue to work in partnership to improve quality of care and maternal outcomes nationwide.
Acknowledgments
Supported by the American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine to conduct the pilot program.
The findings and conclusions in this publication are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention. No competing financial interests exist.
Footnotes
Financial Disclosure
The authors did not report any potential conflicts of interest.
REFERENCES
- 1.Committee on Perinatal Health. Toward improving the outcome of pregnancy: recommendations for the regional development of maternal and perinatal health services White Plains (NY): March of Dimes National Foundation; 1976. [Google Scholar]
- 2.Berns SD. Toward improving the outcome of pregnancy III: enhancing perinatal health through quality, safety, and performance initiatives While Plains (NY): March of Dimes Foundation; 2011. [Google Scholar]
- 3.Guidelines for perinatal care 8th ed. Washington, DC: American Academy of Pediatrics and the American College of Obstetricians and Gynecologists; 2017. [Google Scholar]
- 4.American Academy of Pediatrics Committee on Fetus And Newborn. Levels of neonatal care. Pediatrics 2012;130:587–97. [DOI] [PubMed] [Google Scholar]
- 5.GBD 2015 Maternal Mortality Collaborators. Global, regional, and national levels of maternal mortality, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016;388:1775–812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Callaghan WM, Creanga AA, Kulklina EV. Severe maternal morbidity among delivery and postpartum hospitalizations in the United States. Obstet Gynecol 2012;120:1029–36. [DOI] [PubMed] [Google Scholar]
- 7.Levels of maternal care. Obstetric Care Consensus No. 2. American College of Obstetricians and Gynecologists. Obstet Gynecol 2015;125:502–15. [DOI] [PubMed] [Google Scholar]
- 8.National Institute for Children’s Health Quality (NICHQ). Collaborative improvement and innovation network to reduce infant mortality (infant mortality CoIIN) Available at: https://www.nichq.org/IMCoIIN. Retrieved May 25, 2018.
- 9.Catalano A, Bennett A, Busacker A, Carr A, Goodman D, Kroelinger C, et al. Implementing CDC’s Level of Care Assessment Tool (LOCATe): a national collaboration to improve maternal and child health. J Womens Health (Larchmt) 2017; 26:1265–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Arizona Perinatal Trust Voluntary Certification Program. Available at: https://azperinatal.org/certification. Retrieved May 25, 2018.
- 11.Georgia General Assembly. 2017–2018 regular session—HB 909: health; designation of perinatal facilities; provisions Available at: http://www.legis.ga.gov/Legislation/en-US/display/20172018/HB/909. Retrieved May 25, 2018.
- 12.Indiana General Assembly 2018 session. Senate Bill 360 Available at: https://iga.in.gov/legislative/2018/bills/senate/360. Retrieved May 25, 2018.
- 13.Texas Office of the Secretary of State, Department of State Health Services. Texas Administrative Code: Title 25, Part 1, Chapter 133, Subchapter K Available at: http://texreg.sos.state.tx.us/public/readtac$ext.ViewTAC?tac_view-55&ti525&pt51&ch5133&sch5K&rl5Y. Retrieved May 25, 2018.