

Abstract
Background
Asthma guidelines aim to guide health practitioners to optimise treatment for patients to minimise symptoms, improve or maintain good lung function, and prevent acute exacerbations. The principle of asthma guidelines is based on a step‐up or step‐down regimen of asthma medications to maximise health using minimum doses. Fractional exhaled nitric oxide (FeNO) is a marker of eosinophilic inflammation and tailoring asthma medications in accordance to airway eosinophilic levels may improve asthma outcomes such as indices of control or reduce exacerbations, or both.
Objectives
To evaluate the efficacy of tailoring asthma interventions based on fractional exhaled nitric oxide (FeNO), in comparison to not using FeNO, that is, management based on clinical symptoms (with or without spirometry/peak flow) or asthma guidelines (or both), for asthma‐related outcomes in children.
Search methods
We searched the Cochrane Airways Group Specialised Register of Trials, the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, Embase and reference lists of articles. The last searches were in June 2016.
Selection criteria
All randomised controlled trials (RCTs) comparing adjustment of asthma medications based on FeNO levels compared to those not using FeNO, that is, management based on clinical symptoms or asthma guidelines (or both) involving children.
Data collection and analysis
We reviewed results of searches against predetermined criteria for inclusion. Two review authors independently selected relevant studies, assessed trial quality and extracted data. We contacted study authors for further information with responses provided from three.
Main results
The review included nine studies; these studies differed in a variety of ways including definition of asthma exacerbations, FeNO cut‐off levels used (12 parts per billion (ppb) to 30 ppb), the way in which FeNO was used to adjust therapy and duration of study (6 to 12 months). Of 1426 children randomised, 1329 completed the studies. The inclusion criteria for the participants in each study varied but all had a diagnosis of asthma. There was a significant difference in the number of children having one or more asthma exacerbations over the study period, they were significantly lower in the FeNO group in comparison to the control group (odds ratio (OR) 0.62, 95% confidence interval (CI) 0.49 to 0.80; 1279 participants; 8 studies). The number needed to treat for an additional beneficial outcome (NNTB) over 52 weeks was 10 (95% CI 7 to 20). There was no difference between the groups when comparing exacerbation rates (mean difference (MD) ‐0.37, 95% CI ‐0.8 to 0.06; 736 participants; 4 studies; I2 = 67%). The number of children in the FeNO group requiring oral corticosteroid courses was lower in comparison to the children in the control group (OR 0.63, 95% CI 0.48 to 0.83; 1169 participants; 7 studies; I2 = 0%). There was no statistically significant difference between the groups for exacerbations requiring hospitalisation (OR 0.75, 95% CI 0.41 to 1.36; 1110 participants; 6 studies; I2 = 0%). There were no significant differences between the groups for any of the secondary outcomes (forced expiratory volume in one second (FEV1), FeNO levels, symptom scores or inhaled corticosteroid doses at final visit). The included studies recorded no adverse events.
Three studies had inadequate blinding and were thus considered to have a high risk of bias. However, when these studies were removed in subgroup analysis, the difference between the groups for the primary outcome (exacerbations) remained statistically significant. The GRADE quality of the evidence ranged from moderate (for the outcome 'Number of participants who had one or more exacerbations over the study period') to very low (for the outcome 'Exacerbation rates'), based on lack of blinding, statistical heterogeneity and imprecision.
Authors' conclusions
In this updated review with five new included studies, tailoring asthma medications based on FeNO levels (in comparison with primarily guideline management) significantly decreased the number of children who had one or more exacerbations over the study period but did not impact on the day‐to‐day clinical symptoms or inhaled corticosteroid doses. Therefore, the use of FeNO to guide asthma therapy in children may be beneficial in a subset of children, it cannot be universally recommended for all children with asthma.
Further RCTs need to be conducted and these should encompass different asthma severities, different settings including primary care and less affluent settings, and consider different FeNO cut‐offs.
Plain language summary
Can exhaled nitric oxide be used to adjust asthma medications in children with asthma?
Background
We investigated whether exhaled (breathing out) nitric oxide (a marker in the breath which can show a type of lung inflammation) can be useful to adjust asthma medications in children with asthma instead of following the usual ways that asthma medications are adjusted to get the best dose to control the asthma. Exhaled nitric oxide levels are easily obtained by getting the person to breathe into a commercially available analyser.
Study characteristics
We included all randomised controlled trials that compared adjustment of asthma medications by either usual clinical care (control group) versus using exhaled nitric oxide. The participants included in the trials had asthma diagnosed as per relevant asthma guidelines.
The evidence is current to June 2016 when the searches were last completed.
The review included nine studies (involving 1426 children) that varied in a several ways including length of the study, exhaled nitric oxide cut‐off levels used for altering medicines and the way each study defined flare‐ups or attacks (called exacerbations). The studies ranged from 6 to 12 months in length. The exhaled nitric oxide cut‐off values used by the different studies as a basis for decreasing or increasing medicines also varied.
The mean age of the participants ranged from 10 to 14 years old.
Key results
In this review, we found that guiding asthma medicines based on exhaled nitric oxide (compared to a control group) was beneficial in reducing the number of children who had at least one exacerbation during the study. In the control group where therapy was guided according to clinical symptoms, 40 children out of 100 had at least one exacerbation over 48.5 weeks, compared to 28 out of 100 children where treatment was guided by exhaled nitric oxide. However, we found no difference between groups in other measures of asthma severity that impact on day‐to‐day clinical symptoms or inhaled corticosteroid dose (medications used to control asthma). Therefore, using exhaled nitric oxide levels to adjust asthma therapy may reduce the number of attacks that children with asthma have but does not impact on the day‐to‐day symptoms.
Quality of the evidence
The level of evidence found ranged from moderate, when comparing the two groups for the number of children who had one or more exacerbations, to very low when comparing the number of exacerbations.
Summary of findings
Summary of findings for the main comparison. Tailoring asthma treatment using fractional exhaled nitric oxide versus clinical symptoms.
| Tailoring asthma treatment using fractional exhaled nitric oxide vs clinical symptoms | ||||||
| Patient or population: children with asthma Setting: outpatient Intervention: asthma treatment tailored on FeNO Comparison: asthma treatment tailored on clinical symptoms | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with clinical symptoms | Risk with asthma treatment tailored on FeNO | |||||
| Number of participants who had ≥ 1 exacerbations over study period (48.5 weeks) |
40 per 100 | 29 per 100 (25 to 35) | OR 0.62 (0.49 to 0.8) | 1279 (8 RCTs) | ⊕⊕⊕⊝ Moderate1 | ‐ |
| Number of asthma exacerbations per 52 weeks (exacerbation rate) | The mean number of asthma exacerbations per 52 weeks (exacerbation rate) was 1.66 | The mean number of asthma exacerbations per 52 weeks (exacerbation rate) in the intervention group was 0.37 lower (0.8 lower to 0.06 higher) | MD ‐0.37 (‐0.8 to 0.06) | 736 (4 RCTs) | ⊕⊝⊝⊝ Very low2 | ‐ |
| ICS dose at final visit (budesonide equivalent) | The mean ICS dose at final visit (budesonide equivalent) was 483 μg/day | The mean ICS dose at final visit (budesonide equivalent) in the intervention group was 63.95 μg/day higher (51.89 lower to 179.79 higher) | ‐ | 317 (3 RCTs) | ⊕⊕⊕⊝ Moderate3 | ‐ |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; FeNO: fractional exhaled nitric oxide; ICS: inhaled corticosteroid; MD: mean difference; OR: odds ratio; RCT: randomised controlled trial | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect. Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect. | ||||||
1Three studies carrying 23.7% of the analysis weight were at high risk of performance bias and detection bias due to the lack of blinding (downgraded one level risk of bias) (de Jongste 2008; Verini 2010; Voorend‐van Bergen 2015).
2One study carrying 11% of the analysis weight was open labelled which may have introduced detection bias (Verini 2010). A random‐effects sensitivity analysis substantially changed the result to MD ‐0.37 (95% CI ‐0.8 to 0.06). There was also statistical heterogeneity in the analysis (I2 = 67%, P = 0.03) (downgrade three levels for risk of bias, imprecision and heterogeneity).
3One study carrying 47% of the analysis weight was single blinded and participants were aware of their allocation group (downgraded one level for performance bias) (Voorend‐van Bergen 2015).
Background
Description of the condition
Asthma is one of the most common chronic diseases in children. Acute attacks (exacerbations) are common in children with asthma and some require more intensive treatment in hospital. Hospitalisations for asthma account for 12% to 21% (Anderson 2007; Akinbami 2009) of hospitalisations worldwide (Gupta 2006). Thus, prevention of exacerbations, particularly severe exacerbations, is one goal of good asthma management. The second component in asthma management is monitoring of asthma control (by subjective and objective measures) (National Asthma Council 2014; BTS/SIGN 2016; GINA 2016). Subjective measures usually involve a series of questions used for clinical assessment, diary cards and quality of life (QoL) questionnaires. Traditional objective methods include peak flow, spirometry and degree of airway hyper‐responsiveness (Zacharasiewicz 2005). Newer and arguably more sensitive methods include measurement of airway inflammation such as airway cellularity in induced sputum or fractional exhaled nitric oxide (FeNO).
Airway inflammation associated with asthma can be eosinophilic or neutrophilic (Douwes 2002). Arguably, asthma management is best tailored in accordance to the type of airway inflammation, as corticosteroids are more beneficial in eosinophilic inflammation (Wardlaw 2000); inhaled corticosteroids (ICS) reduce exacerbations and improve symptoms and asthma control (Wardlaw 2000). There are several ways to quantify airway eosinophilic inflammation, such as determining the percentage of eosinophils in the sputum and FeNO. FeNO correlates with other markers of asthma, for example, eosinophilia in induced sputum (Jatakanon 1998), and bronchial reactivity in non‐steroid treated people (Dupont 1998).
Description of the intervention
The principle of asthma management is based on a step‐up or step‐down regimen of asthma medications to reduce airway inflammation, control symptoms and reduce exacerbations. Therefore, tailoring of asthma medications in accordance to levels reflective of airway eosinophilia may improve asthma control or reduce exacerbations, or both. Obtaining induced sputum samples and sputum analysis is labour intensive and not widely available in most routine clinical settings. Hypertonic saline, used to induce sputum may also temporarily increase asthma symptoms (such as wheeze, cough and chest tightness) and sputum is not always successfully obtained in young children. Thus, measures of FeNO confer some advantage over measurements of sputum eosinophils. However, assessment of FeNO levels do not provide any data on non‐eosinophilic inflammation and the equipment required to measure FeNO is relatively expensive.
FeNO levels can be measured using commercially available analysers. These analysers vary in several ways that include methods of measurements (online or offline), complexity, setup, calibration procedures, sampling tube design, measuring chamber and the way expiratory flow is controlled (Müller 2005). The stationary analysers measure FeNO by chemoluminescence whilst the portable FeNO analysers measure FeNO using electrochemistry.
How the intervention might work
As FeNO is reflective of airway eosinophilia in some circumstances, FeNO can be considered as a biomarker. For asthma, FeNO levels can potentially be used in children with asthma to:
monitor airway eosinophilia;
verify the adherence to ICS; and
predict upcoming asthma exacerbations.
Reduction of airway inflammation improves symptoms and asthma control (Wardlaw 2000). Hence, the use of FeNO levels to tailor asthma medications in children with asthma may improve asthma control or reduce exacerbations, or both.
Why it is important to do this review
A previous Cochrane Review included both adults and children (Petsky 2009). Given the clinical heterogeneity between children and adults with asthma, rather than update that review, we undertook separate reviews for children and adults. This review focuses on children and there is a similar systematic review that includes only adults (Petsky 2016).
A systematic review evaluating the efficacy of tailoring asthma interventions based on FeNO levels will be useful to guide clinical practice in children with asthma. Using FeNO routinely in clinical practice adds to the burden of asthma care and resource utilisation. In addition, routine use of FeNO to guide use of asthma medications may improve asthma control and reduce exacerbations and hospitalisations related to asthma.
Objectives
To evaluate the efficacy of tailoring asthma medications based on fractional exhaled nitric oxide (FeNO), in comparison to not using FeNO, that is, management based on clinical symptoms (with or without spirometry/peak flow) or asthma guidelines (or both), for asthma‐related outcomes in children.
Methods
Criteria for considering studies for this review
Types of studies
We included randomised controlled trials (RCTs) comparing adjustment of asthma medications based on FeNO levels in comparison to those not using FeNO, that is, management based on clinical symptoms (with or without spirometry/peak flow) or current asthma guidelines, or both. We included studies reported as full‐text, abstract only, and unpublished data.
Types of participants
We included children/adolescents with a diagnosis of asthma according to guideline‐defined criteria.
We excluded participants with the following comorbidities/characteristics: eosinophilic bronchitis, asthma related to an underlying lung disease such as bronchiectasis and chronic obstructive pulmonary disease or diagnostic categories such as 'cough variant asthma' and 'wheezy bronchitis'.
Types of interventions
We included RCTs comparing adjustment of asthma medications based on FeNO levels versus control groups where FeNO is not used to adjust asthma medications. Control group interventions may have included use of clinical symptoms (with or without spirometry/peak flow) to guide adjustment of asthma medications. Studies that included the use of other interventions were included if all participants had equal access to such interventions. We included trials of at least 12 weeks' duration.
Types of outcome measures
Primary outcomes
-
Asthma exacerbations during follow‐up defined as:
number of participants who had one or more exacerbation over the study period;
number of exacerbations per 52 weeks (exacerbation rate);
severe exacerbations requiring oral corticosteroids;
severe exacerbation requiring hospitalisations.
Secondary outcomes
Objective measurements of asthma control (forced expiratory volume in one second (FEV1), peak flow, airway hyper‐responsiveness).
FeNO level.
Symptoms of asthma as reported in asthma QoL score.
ICS dose at final visit.
Reporting one or more of the outcomes listed here was not an inclusion criteria for this review.
Search methods for identification of studies
Electronic searches
We identified studies from the Cochrane Airways Group's Specialised Register (CAGR), which is maintained by the Information Specialist for the Group. The Register contains trial reports identified through systematic searches of bibliographic databases including the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, Embase, CINAHL, AMED and PsycINFO, and handsearching of respiratory journals and meeting abstracts (see Appendix 1 for further details). We searched all records in the CAGR using the search strategy in Appendix 2.
We also conducted a search of ClinicalTrials.gov (www.ClinicalTrials.gov) and the World Health Organization (WHO) trials portal (www.who.int/ictrp/en/). We searched all databases from their inception to the present, and we imposed no restriction on language of publication. All searches were undertaken by the Cochrane Airways Group central team (by Elizabeth Stovold) and the latest search was undertaken on 30 June 2016.
Searching other resources
We checked reference lists of all primary studies and review articles for additional references. We searched relevant manufacturers' websites for trial information.
We searched for errata or retractions from included studies published in full‐text on PubMed (www.ncbi.nlm.nih.gov/pubmed), and reported the date this was done within the review.
Data collection and analysis
Selection of studies
Two review authors (HP, KK) independently screened titles and abstracts for inclusion of all the potential studies we identified with the search and coded them as 'retrieve' (eligible or potentially eligible/unclear) or 'do not retrieve'. We then retrieved the full‐text study reports/publication and two review authors (HP, KK) independently screened the full‐text and identified studies for inclusion, and identified and recorded reasons for exclusion of the ineligible studies. We planned to resolve any disagreement through discussion or, if required, consult a third review author (AC). We identified and excluded duplicates and collate multiple reports of the same study so that each study, rather than each report, was the unit of interest in the review. We recorded the selection process in sufficient detail to complete the PRISMA flow diagram and Characteristics of excluded studies table.
Data extraction and management
We used a data collection form for study characteristics and outcome data which was piloted on at least one study in the review. One review author (HP) extracted study characteristics from included studies. A second review author (KK) spot‐checked study characteristics for accuracy against the trial report. We then extracted the following study characteristics.
Methods: study design, total duration of study, details of any 'run‐in' period, number of study centres and location, study setting, withdrawals and date of study.
Participants: number, mean age, age range, gender, severity of condition, diagnostic criteria, baseline lung function, smoking history, inclusion criteria and exclusion criteria.
Interventions: intervention, comparison, concomitant medications and excluded medications.
Outcomes: primary and secondary outcomes specified and collected, and time points reported.
Notes: funding for trial, and notable conflicts of interest of trial authors.
Two review authors (HP, KK) independently extracted outcome data from included studies from current search. We noted in the Characteristics of included studies table if outcome data were not reported in a usable way. We resolved disagreements by consensus or by involving a third review author (AC). One review author (HP) transferred data into Review Manager 5 (RevMan 2014). We double‐checked that data were entered correctly by comparing the data presented in the systematic review with the study reports.
Assessment of risk of bias in included studies
Two review authors (HP, KK) independently assessed risk of bias for each new study using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We planned to resolve any disagreements by discussion or by involving another review author (AC). We assessed the risk of bias according to the following domains.
Random sequence generation.
Allocation concealment.
Blinding of participants and personnel.
Blinding of outcome assessment.
Incomplete outcome data.
Selective outcome reporting.
Other bias.
We graded each potential source of bias as high, low or unclear and provided a quote from the study report together with a justification for our judgement in the 'Risk of bias' table. We then summarised the risk of bias judgements across different studies for each of the domains listed. We planned to blind separately for different key outcomes where necessary (e.g. for unblinded outcome assessment, risk of bias for all‐cause mortality may be very different from for a participant‐reported pain scale). Where information on risk of bias related to unpublished data or correspondence with a trialist, we noted this in the 'Risk of bias' table.
When considering treatment effects, we considered the risk of bias for the studies that contributed to that outcome.
Assessment of bias in conducting the systematic review
We conducted the review according to the published protocol and reported any deviations from it in the Differences between protocol and review section of the systematic review.
Measures of treatment effect
We analysed dichotomous data as odds ratios (OR) and continuous data as mean difference (MD) or standardised mean difference (SMD) with 95% confidence intervals (CI). We then entered data presented as a scale with a consistent direction of effect.
We undertook meta‐analyses only where it was meaningful (i.e. if the treatments, participants and the underlying clinical question were similar enough for pooling to make sense).
We narratively described skewed data reported as medians and interquartile ranges.
Where multiple trial arms were reported in a single trial, we included only the relevant arms. If two comparisons (e.g. drug A versus placebo and drug B versus placebo) were combined in the same meta‐analysis, we halved the control group to avoid double‐counting.
Unit of analysis issues
For dichotomous data, we reported the proportion of participants contributing to each outcome in comparison with the total number randomised. For rate ratios of common events whereby one participant may have more than one event, we used generic inverse variance (GIV) analysis. The rate ratios were taken from the published papers and the standard errors calculated from CIs or P values published in the papers. We had planned for cross‐over studies, to calculate the mean treatment differences from raw data, and variances extracted or imputed and entered as a fixed‐effect (GIV) outcome, to provide summary weighted differences and 95% CIs.
Dealing with missing data
We contacted investigators or study sponsors to verify key study characteristics and obtain missing numerical outcome data where possible (e.g. when a study was identified as abstract only). Where this was not possible, and the missing data were thought to introduce serious bias, we explored the impact of including such studies in the overall assessment of results by a sensitivity analysis.
Assessment of heterogeneity
We described any heterogeneity between the study results and tested it to see if it reached statistical significance using a Chi2 test. We planned to include the 95% CI estimated using a random‐effects model whenever there were concerns about statistical heterogeneity. Heterogeneity was considered significant when the P value is less than 0.10 (Higgins 2011). We then used the I2 statistic to measure heterogeneity among the trials in each analysis. If we identified substantial heterogeneity, we reported it and explored possible causes by prespecified subgroup analysis.
Assessment of reporting biases
We were unable to pool more than 10 trials, so did not create and examine a funnel plot to explore possible small‐study and publication biases.
Data synthesis
We included the results from studies that met the inclusion criteria and reported any of the outcomes of interest in the subsequent meta‐analyses. We calculated the summary weighted RR and 95% CI (fixed‐effect model) using Review Manager 5 (RevMan 2014). For rate ratios of common events whereby one participant may have more than one event, we used GIV. The rate ratios were taken from the published papers and the standard errors calculated from CIs or P values published in the papers. For cross‐over studies, we planned to calculate the mean treatment differences from raw data, and extract or impute variances and enter them as fixed‐effect GIV outcomes, to provide summary weighted differences and 95% CI. Numbers needed to treat were calculated from the pooled OR and its 95% CI applied to a specified baseline risk using an online calculator (Cates 2008). The outcome indices were assumed to be normally distributed continuous variables so the MDs in outcomes could be estimated. If studies reported outcomes using different measurement scales, we estimated the SMD.
'Summary of findings' table
We created a 'Summary of findings' table using the following outcomes:
number of participants who had one or more exacerbations over the study period;
number of asthma exacerbations per 52 weeks,
ICS dose at final visit.
The 'Summary of findings' table in the previous combined review (Petsky 2009) was amended to reflect new data and restricted to the inclusion criteria. We used the five GRADE considerations (study limitations, consistency of effect, imprecision, indirectness and publication bias) to assess the quality of a body of evidence as it relates to the studies which contribute data to the meta‐analyses for the prespecified outcomes. We then used methods and recommendations described in Section 8.5 and Chapter 12 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011) using GRADEpro software (GRADEpro GDT 2015). We justified all decisions to downgrade or upgrade the quality of studies using footnotes and we made comments to aid reader's understanding of the review where necessary.
Subgroup analysis and investigation of heterogeneity
We planned the following subgroup analyses:
basis for adjustment of ICS in the control group (guideline driven monitoring versus non‐guideline driven);
use of spirometry or peak flow as an adjunctive monitoring tool for adjustment of medications versus non‐use of spirometry or peak flow;
baseline ICS dose at commencement of intervention (low‐medium (< 800 μg/day of budesonide equivalent) versus high dose (800 μg/day or more of budesonide equivalent);
FeNO cut‐offs for adjustment of medications (20 parts per billion (ppb) or less versus more than 20 ppb);
FeNO cut‐offs, based on presence of atopy.
Sensitivity analysis
We carried out the following sensitivity analyses.
Sensitivity analysis excluding studies with a high risk of bias based on the 'Risk of bias' assessment. We removed studies that did not have adequate allocation concealment and sequence generation.
Variation in the inclusion criteria. We removed studies that included children not receiving ICS at recruitment.
Differences in the medications used in the intervention and comparison group. We removed studies that adjusted medications only for one arm.
Analysis comparing the random‐effects model to a fixed‐effect model.
Analysis by 'strategy received'. We removed studies with hierarchy management protocols that only considered use of steroids for each step (i.e. without consideration for using montelukast or long‐acting beta‐agonist (LABA), or both, at any point).
Results
Description of studies
See: Characteristics of included studies; Characteristics of excluded studies; Characteristics of ongoing studies tables.
Results of the search
From the searches, the CAGR identified 1084 potentially relevant titles (Figure 1). We identified an additional 129 titles through searches of ClinicalTrials.gov (www.ClinicalTrials.gov) and the WHO trials portal (www.who.int/ictrp/en/). After assessing the abstracts, we obtained 30 papers for consideration after removing duplicates. We excluded 14 papers due to non‐randomisation or treatment not being based on FeNO. Of the potential 16 papers, nine included children or adolescents and the remaining seven were based on adults, which are presented in a separate Cochrane Review (Petsky 2016).
1.
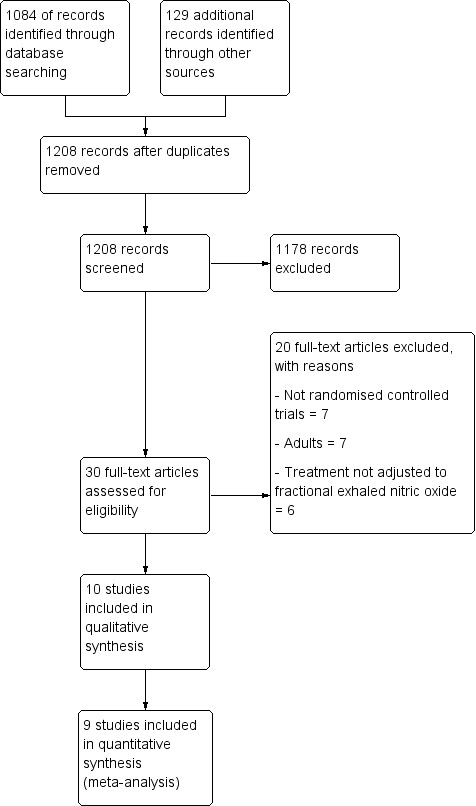
Prisma flow diagram.
Included studies
The review included nine studies (see Characteristics of included studies). The nine studies involved 1426 randomised participants with 1329 completing the trials (Pijnenburg 2005; Fritsch 2006; Szefler 2008; de Jongste 2008; Verini 2010; Pike 2013; Peirsman 2014; Petsky 2015; Voorend‐van Bergen 2015). Of these nine studies, five were new (i.e. were not in the previous (Petsky 2009) review).
Study design
All nine studies were parallel‐group studies. Five were multicentre studies (Szefler 2008; de Jongste 2008; Pike 2013; Peirsman 2014; Voorend‐van Bergen 2015), one was dual centre (Petsky 2015), and three were single‐centre studies (Pijnenburg 2005; Fritsch 2006; Verini 2010).
One study used a three‐arm strategy to adjust ICS (Voorend‐van Bergen 2015). The strategy arms were: web group, where treatment was adjusted monthly based on the web‐based Asthma Control Test (ACT) score; FeNO group, where treatment was adjusted according to FeNO and ACT score at four‐monthly clinic visits; or standard care, where treatment was adjusted according to the ACT score during clinic visits. For this review, we considered the FeNO with ACT score strategy arm as the intervention group and the standard care strategy as the control group.
Of the nine studies; four were double blind (Pijnenburg 2005; Szefler 2008; Pike 2013; Petsky 2015), three were single blind (Fritsch 2006; Peirsman 2014; Voorend‐van Bergen 2015), and two had no blinding (de Jongste 2008; Verini 2010).
The study duration varied ranging from 6 to 12 months (Table 2). Each study defined exacerbations differently (Table 2).
1. Included studies definitions.
| Study ID | Exacerbation definition | FeNO strategy (FeNO levels in ppb) | Symptom strategy | Duration |
| de Jongste 2008 | No definition provided (OCS courses and hospitalisation data included in exacerbation results) |
In children aged 6 to 10 years: < 20 and ≤ 60 symptom score = step down/discontinue > 20 and ≤ 60 symptom score = increase < 20 and > 60 symptom score = no change > 20 and > 60 symptom score = step up In children aged > 10 years: < 25 and ≤ 60 symptom score = step down/discontinue > 25 and ≤ 60 symptom score = increase < 25 and > 60 symptom score = no change > 25 and > 60 symptom score = step up |
Below range (< 10) = step down/discontinue In range (10 to 60) = no change Above range (> 60) = step up |
30 weeks |
| Fritsch 2006 | 4 parameters: OCS because of asthma symptoms, non‐scheduled visit because of asthma symptoms, > symptom score to 2, < FEV1 (in litres) > 10% compared to previous visit, or a combination of these |
≤ 20 and FEV1 ≥ 80%, symptom score 0 or 1 and SABA use < 6 = step down ≤ 20 and FEV1 < 80% or symptoms score > 1 or SABA use ≥ 6 = step up Participant on SABA on demand only: > 20 and FEV1 ≥ 80%, symptom score 0 or 1 and SABA use < 6 = step up Participant on ICS: > 20 and FEV1 ≥ 80%, symptom score 0 or 1 and SABA use < 6 = same step > 20 and FEV1 < 80% or symptoms score > 1 or SABA use ≥ 6 = step up |
Austrian asthma guidelines: FEV1 ≥ 80%, symptom score 0 or 1 and SABA use < 6 = step down FEV1 < 80% or symptoms score > 1 or SABA use ≥ 6 = step up |
6 months |
| Peirsman 2014 | As per GINA guidelines | ≤ 20 and controlled = step down ≤ 20 and partially controlled consider LTRA > 20 = step up |
GINA guidelines | 12 months |
| Petsky 2015 | Respiratory events requiring OCS | Elevated FeNO = step up Low FeNO for 2 visits = step down Elevated FeNO defined as: ≥ 10 with no positive SPT ≥ 12 with 1 positive SPT ≥ 20 with ≥ 2 positive SPT |
Asthma symptom diary card Score < 10 in previous week = step down Score increased ≥ 15% since previous week = step up |
12 months |
| Pijnenburg 2005 | No definition provided (OCS courses included in results) |
≤ 30 and symptom score ≤ 14 = step down ≤ 30 and symptom score > 14 = no change > 30, regardless of symptoms = step up |
Symptom score ≤ 14 second time = step down Symptom score ≤ 14 first time = no change Symptom score > 14 = step up |
12 months |
| Pike 2013 | ≥ 48 hours > asthma symptoms or therapy or < PEF (≥25%). Mild: increase SABA only Moderate: requiring systemic corticosteroids Severe: requiring hospitalisations ≥ 8 hours |
≤ 15 and well controlled = step down < 25 and poorly controlled = LABA maximised ≥ 25 or FeNO doubled from baseline = step up If FeNO remained raised after 2 x steps (SIGN/BTS steps) ICS not increased again unless participant poorly controlled |
SIGN/BTS guidelines | 12 months |
| Szefler 2008 | Admissions to hospital, unscheduled visits and prednisone use for asthma |
NHLBI guidelines and FeNO ≤ 20 and Level 1 = no change 20.1 to 30 and Level 2 = step up 30.1 to 40 and Level 3 = 2 steps > 40 and Level 4 = 3 steps or 2 steps and OCS course |
NHLBI guidelines | 46 weeks |
| Verini 2010 | According to ATS/ERS criteria and requiring SABA. |
At 6 month visit only: < 12 = step down or no change > 12 = step up |
As per GINA: | 12 months |
| Voorend‐van Bergen 2015 | No definition provided (OCS courses and hospitalisation data included in exacerbation results) |
If ACT ≥ 20 and: FeNO < 25 = step down FeNO ≥ 25 to < 50 = no change FeNO ≥ 50 = step up If ACT < 20 and: FeNO ≥ 25 = step up FeNO < 25 = no change |
ACT results: < 20 = step up ≥ 20 = no change or step down |
12 months |
ACT: Asthma Control Test; ATS: American Thoracic Society; BTS: British Thoracic Society; ERS: European Respiratory Society; FeNO: fractional exhaled nitric oxide; FEV1: forced expiratory volume in first second; GINA: Global initiative for asthma; ICS: inhaled corticosteroids; LTRA: leukotriene receptor antagonist; NHLBI: National Heart, Lung, and Blood Institute; OCS: oral corticosteroids; ppb: parts per billion; SABA: short‐acting beta2 agonist; SIGN: Scottish Intercollegiate Guidelines Network; SPT: skin prick test.
Participants
The nine studies had different inclusion criteria for the participants. All studies included participants with asthma which was defined as per current guidelines.
Fractional exhaled nitric oxide strategy
The intervention arm in all nine studies, although primarily based on FeNO level, differed in the cut‐off for FeNO for change in therapy. Petsky 2015 was the only study which utilised different cut‐offs for the presence of atopy.
The FeNO cut‐offs used for the studies are presented in Table 2.
Control group
Five of the nine studies utilised existing asthma guidelines to adjust treatment in the control group (Fritsch 2006; Szefler 2008; Verini 2010; Pike 2013; Peirsman 2014). Three studies used participant‐reported symptoms (Pijnenburg 2005; de Jongste 2008; Petsky 2015), and one utilised the Asthma Control Questionnaire (ACQ) (Voorend‐van Bergen 2015). The control group strategies are described in Table 2.
Outcomes
The primary outcomes of the studies also varied. Three studies used symptom‐free days (de Jongste 2008; Peirsman 2014; Voorend‐van Bergen 2015), three studies used asthma exacerbations (Verini 2010; Pike 2013; Petsky 2015), three studies included ICS cumulative doses (Pijnenburg 2005; Verini 2010; Pike 2013), one study used number of days with symptoms (Szefler 2008), and another used FEV1 (Fritsch 2006). The definitions of exacerbations were different among the studies (Table 2).
The secondary outcomes also varied between the studies. Four studies included asthma exacerbations (Fritsch 2006; Pike 2013; Peirsman 2014; Voorend‐van Bergen 2015), four studies used dose of ICS (Fritsch 2006; de Jongste 2008; Petsky 2015; Voorend‐van Bergen 2015), three studies included spirometry (de Jongste 2008; Petsky 2015; Voorend‐van Bergen 2015), and Petsky 2015 and de Jongste 2008 used asthma QoL questionnaires.
We contacted study authors to request further data, or data that could be included in the meta‐analysis; three study authors provided data (Pike 2013; Petsky 2015; Voorend‐van Bergen 2015).
The study characteristics are described in the Characteristics of included studies table.
Excluded studies
We recorded the reasons for excluding the 20 studies in the Characteristics of excluded studies table. The most common reasons for exclusion were: not an RCT (seven studies), treatment not adjusted according to FeNO (six studies), and population was not children or adolescents (seven studies). One further study was found in abstract form only (Duong‐Quy 2015). We contacted this study author in January 2016 and they confirmed that the paper is in preparation, therefore this study was judged to be ongoing and will be included in the next update (Duong‐Quy 2015).
Risk of bias in included studies
The full details of risk of bias judgements is described under the 'Risk of Bias' section in the Characteristics of included studies table and is summarised in Figure 2. Overall, the methodological quality of the included studies was good.
2.
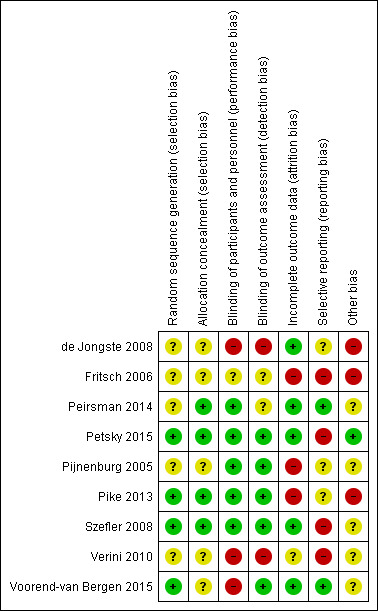
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Four studies described generation of randomisation sequence (Szefler 2008; Pike 2013; Petsky 2015; Voorend‐van Bergen 2015), and it was unclear in five studies (Pijnenburg 2005; Fritsch 2006; de Jongste 2008; Verini 2010; Peirsman 2014). The method of allocation concealment was adequate in four studies (Szefler 2008; Pike 2013; Peirsman 2014; Petsky 2015), and unclear in five (Pijnenburg 2005; Fritsch 2006; de Jongste 2008; Verini 2010; Voorend‐van Bergen 2015).
Blinding
Risk associated with participant blinding was low when the blinding of the assessors was reported based on information provided by authors of the studies. These included comments from the studies such as "a third party provided advice on treatment decisions" and "both arms of the study received the same follow‐up including measurements and tests".
Risk of detection bias due to inadequate blinding of outcome assessors was high in three studies (de Jongste 2008; Verini 2010; Voorend‐van Bergen 2015), and unclear in one study (Fritsch 2006), as there was not enough information in the published article. Five studies were at low risk of bias (Pijnenburg 2005; Szefler 2008; Pike 2013; Peirsman 2014; Petsky 2015).
Incomplete outcome data
Five studies were at low risk of attrition bias (Szefler 2008; de Jongste 2008; Peirsman 2014; Petsky 2015; Voorend‐van Bergen 2015). Three studies were at high risk of attrition bias as they reported unbalanced dropout rates (Fritsch 2006; Pijnenburg 2005; Pike 2013). Verini 2010 did not report on dropouts and was therefore judged at unclear risk of attrition bias.
Selective reporting
Reporting bias was low in two studies with all outcomes being reported (Peirsman 2014; Voorend‐van Bergen 2015). Three studies were at unclear risk of reporting bias as there was inadequate information in the published articles (Pijnenburg 2005; de Jongste 2008; Pike 2013). Four studies were at high risk of reporting bias as some of the secondary outcomes were not reported or incorrect analyses methods were used (Fritsch 2006; Szefler 2008; Verini 2010; Petsky 2015).
Other potential sources of bias
Another source of bias was the success of obtaining FeNO levels at each visit according to current guidelines. Five studies did not report the success of obtaining FeNO at each time point (Pijnenburg 2005; Szefler 2008; Verini 2010; Peirsman 2014; Voorend‐van Bergen 2015). One study reported that they successfully obtained FeNO at each visit (Petsky 2015). Two studies were at high risk as they reported technical problems with the FeNO analysers including 11 out of 77 analysers showing drift in calibration after the study (Fritsch 2006; de Jongste 2008). Pike 2013 was at high risk as they reported not following current guidelines by only doing a single measurement of FeNO at each visit.
Effects of interventions
See: Table 1
See Table 1 for the main comparisons.
Primary outcome: asthma exacerbations
Three studies used asthma exacerbations as their primary outcome but the definition differed among the studies (described in Table 2), as did the way the outcome was measured and presented (Verini 2010; Pike 2013; Petsky 2015). Three studies reported a reduction in asthma exacerbations in the intervention arm compared to the control arm (Verini 2010; Peirsman 2014; Petsky 2015). For the various types of exacerbations, we combined data into the meta‐analysis, as described below.
1.1 Number of participants who had one or more exacerbations over the study period
See Analysis 1.1.
1.1. Analysis.
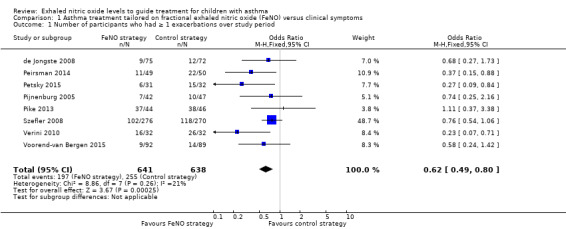
Comparison 1 Asthma treatment tailored on fractional exhaled nitric oxide (FeNO) versus clinical symptoms, Outcome 1 Number of participants who had ≥ 1 exacerbations over study period.
Combined data from eight studies showed that the number of participants experiencing an exacerbation was significantly lower (P = 0.0002) in the FeNO group compared to the control (clinical symptom) group over the study period (OR 0.62, 95% CI 0.49 to 0.8; 1279 participants; 8 studies; I2 = 21%) (de Jongste 2008; Peirsman 2014; Petsky 2015; Pijnenburg 2005; Pike 2013; Szefler 2008; Verini 2010; Voorend‐van Bergen 2015). There was some statistical heterogeneity among the studies but it was not significant (I2 = 21%). In the control group where therapy was guided according to clinical symptoms, 40 children out of 100 had at least one exacerbation over 48.5 weeks, compared to 29 (95% CI 25 to 35) out of 100 for those where treatment was guided by FeNO. The number needed to treat to show an additional beneficial outcome (NNTB) over 52 weeks was 10 (95% CI 7 to 20) (Figure 3).
3.
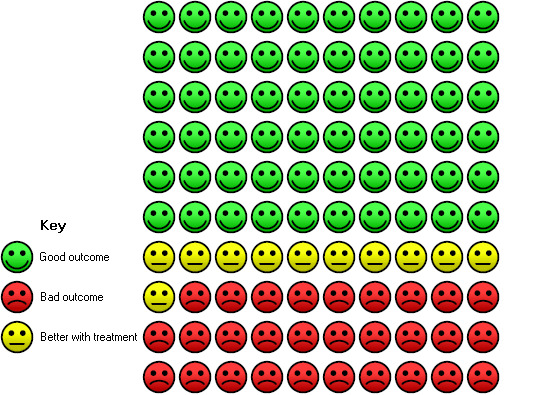
In the control group, 40 children out of 100 had exacerbations over one year, compared to 29 (95% confidence interval (CI) 25 to 35) out of 100 for the active treatment group. Number needed to treat for one additional beneficial outcome = 10 (95% CI 7 to 20).
1.2 Number of exacerbations per 52 weeks (exacerbation rates)
See Analysis 1.2.
1.2. Analysis.
Comparison 1 Asthma treatment tailored on fractional exhaled nitric oxide (FeNO) versus clinical symptoms, Outcome 2 Number of asthma exacerbations per 52 weeks (exacerbation rates).
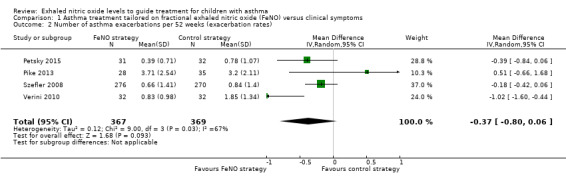
Combined data from four studies for the outcome of exacerbation rate (over 52 weeks) found no differences between the groups (P = 0.09) (MD ‐0.37, 95% CI ‐0.80 to 0.06; 736 participants; 4 studies) (Szefler 2008; Verini 2010; Pike 2013; Petsky 2015). As there was statistical heterogeneity among the studies (I2 = 67%, P = 0.03), we used a random‐effects analysis. The statistical heterogeneity could be accounted for by the skew in some of the studies data. The rate of exacerbation over the 52 weeks in the control group ranged from 0.78 to 3.2.
1.3 Number of participants who had severe exacerbations requiring hospitalisation
See Analysis 1.3.
1.3. Analysis.
Comparison 1 Asthma treatment tailored on fractional exhaled nitric oxide (FeNO) versus clinical symptoms, Outcome 3 Number of participants with severe exacerbations requiring hospitalisation.
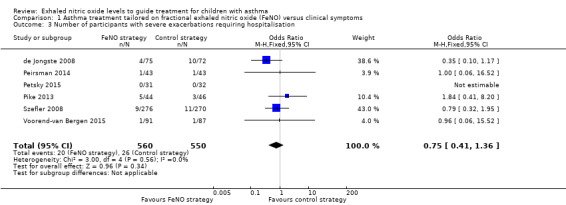
Five studies reported hospitalisations due to worsening of asthma symptoms (de Jongste 2008; Szefler 2008; Pike 2013; Peirsman 2014; Voorend‐van Bergen 2015), and another study reported that no participants were hospitalised (Petsky 2015). In the meta‐analysis, there was no significant difference (P = 0.37) between groups; 20 children in the FeNO group versus 26 in the control group required hospitalisation (OR 0.75, 95% CI 0.41 to 1.36; 1110 participants; 6 studies; I2 = 0%).
1.4 Number of participants who had severe exacerbations requiring rescue oral corticosteroids
See Analysis 1.4.
1.4. Analysis.
Comparison 1 Asthma treatment tailored on fractional exhaled nitric oxide (FeNO) versus clinical symptoms, Outcome 4 Number of participants with severe exacerbations requiring rescue oral corticosteroids.
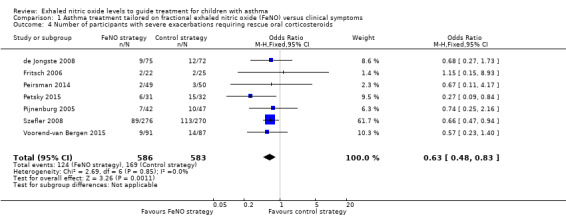
Seven studies reported using rescue oral corticosteroids (de Jongste 2008; Fritsch 2006; Peirsman 2014; Petsky 2015; Pijnenburg 2005; Szefler 2008; Voorend‐van Bergen 2015). The meta‐analysis showed a significantly fewer children (P = 0.001) in the FeNO group required rescue oral corticosteroids compared to the control group (OR 0.63, 95% CI 0.48 to 0.83; 1169 participants; 7 studies; I2 = 0%).
Secondary outcomes
1.5 FEV1% predicted at final visit
See Analysis 1.5.
1.5. Analysis.
Comparison 1 Asthma treatment tailored on fractional exhaled nitric oxide (FeNO) versus clinical symptoms, Outcome 5 FEV1 %predicted at final visit.
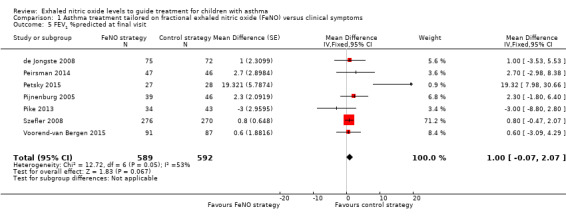
We combined the final visit FEV1% predicted from seven studies in a meta‐analysis and we found no significant difference between the groups (P = 0.12; MD 1.0, 95% CI ‐0.07 to 2.07; 1181 participants; 7 studies; I2 = 0%) (de Jongste 2008; Peirsman 2014; Petsky 2015; Pijnenburg 2005; Pike 2013; Szefler 2008; Voorend‐van Bergen 2015). The two remaining studies reported no significant difference between the two groups, but as details were not provided, we could not include the data in the meta‐analysis (Fritsch 2006;Verini 2010).
1.6 FeNO geometric mean level at final visit
See Analysis 1.6.
1.6. Analysis.
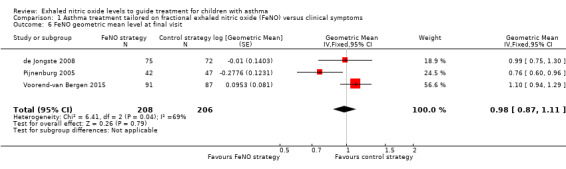
Comparison 1 Asthma treatment tailored on fractional exhaled nitric oxide (FeNO) versus clinical symptoms, Outcome 6 FeNO geometric mean level at final visit.
We combined the final visit's FeNO geometric mean (GM) from three studies in a meta‐analysis (de Jongste 2008; Pijnenburg 2005; Voorend‐van Bergen 2015). The data were heavily skewed and ratio of GM was the most appropriate analysis to use. There was no significant difference between the groups (GM 0.99, 95% CI 0.87 to 1.11; 414 participants; 3 studies; I2 = 69%). The remaining six studies could not be included in the meta‐analysis but reported that there was no significant difference between the groups at the final visit (Fritsch 2006; Peirsman 2014; Petsky 2015; Pike 2013; Szefler 2008; Verini 2010). Fritsch 2006, and Peirsman 2014 reported that there was a decreased trend in FeNO levels for the FeNO group at the final visit but this was not significant.
1.7 Symptom score: Asthma Control Test
See Analysis 1.7.
1.7. Analysis.
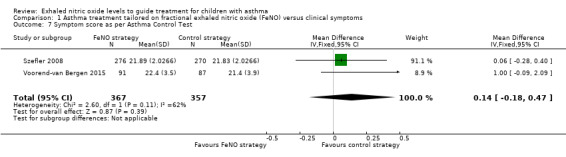
Comparison 1 Asthma treatment tailored on fractional exhaled nitric oxide (FeNO) versus clinical symptoms, Outcome 7 Symptom score as per Asthma Control Test.
Two studies reported ACT results; the meta‐analysis showed no significant difference between groups (MD 0.14, 95% CI ‐0.18 to 0.47; 724 participants; 2 studies; I2 = 62%) (Szefler 2008; Voorend‐van Bergen 2015).
1.8 Symptom score as per Paediatric Asthma Caregiver's Quality of Life Questionnaire (PACQLQ)
See Analysis 1.8.
1.8. Analysis.
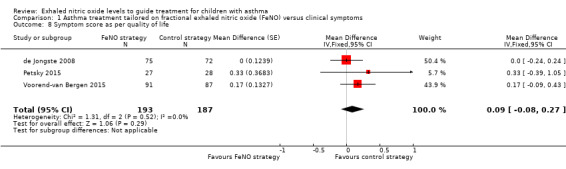
Comparison 1 Asthma treatment tailored on fractional exhaled nitric oxide (FeNO) versus clinical symptoms, Outcome 8 Symptom score as per quality of life.
Combined data from three studies found no significant difference between groups for the PACQLQ (MD 0.09, 95% CI ‐0.08 to 0.27; 380 participants; 3 studies; I2 = 0%) (de Jongste 2008; Petsky 2015; Voorend‐van Bergen 2015).
1.9 Inhaled corticosteroid dose at final visit (budesonide equivalent in micrograms per day)
See Analysis 1.9.
1.9. Analysis.
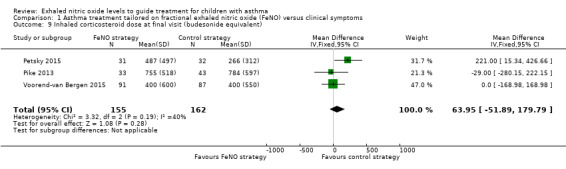
Comparison 1 Asthma treatment tailored on fractional exhaled nitric oxide (FeNO) versus clinical symptoms, Outcome 9 Inhaled corticosteroid dose at final visit (budesonide equivalent).
Three studies reported final ICS doses that could be included in a meta‐analysis; there was no significant difference between the groups (MD 63.95 μg/day, 95% CI ‐51.89 to 179.79; 317 participants; 3 studies; I2 = 40%) (Pike 2013; Petsky 2015; Voorend‐van Bergen 2015). Using a random‐effects model, the difference between the groups remained nonsignificant (MD 65.88 μg/day, 95% CI ‐86.71 to 218.47).
Four studies reported that there was no difference in daily ICS doses between the groups at the final visit (Pijnenburg 2005; de Jongste 2008; Verini 2010; Peirsman 2014). The remaining two studies reported that the control group had lower doses of ICS at the end of the study (Fritsch 2006; Szefler 2008).
1.10 Cost effectiveness of the intervention
One study (Voorend‐van Bergen 2015) published a separate paper (Beerthuizen 2016) assessed the cost of the strategies in their three‐armed trial (standard care, web‐based strategy and FeNO‐based). They reported no significant difference in costs or quality‐adjusted life years between the groups. The web‐based strategy (this arm not included in this systematic review) was 77% more cost effective from a healthcare perspective, whereas the FeNO‐based strategy had an 83% chance of being most cost effective from a societal perspective.
Subgroup analysis and investigation of heterogeneity
1. Based on adjustment of inhaled corticosteroid in the control group (guideline‐driven versus others)
When testing for subgroup differences there was no significant difference between the subgroups for either exacerbation outcome (Analysis 1.10; Analysis 1.11).
1.10. Analysis.
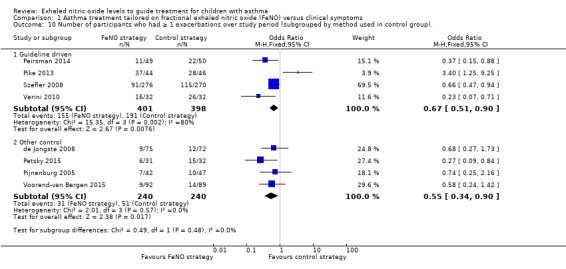
Comparison 1 Asthma treatment tailored on fractional exhaled nitric oxide (FeNO) versus clinical symptoms, Outcome 10 Number of participants who had ≥ 1 exacerbations over study period (subgrouped by method used in control group)..
1.11. Analysis.
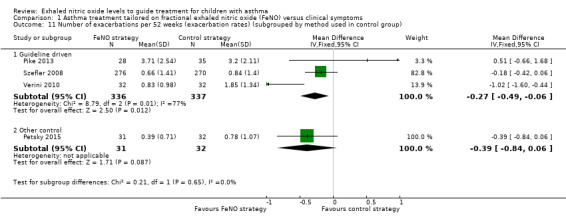
Comparison 1 Asthma treatment tailored on fractional exhaled nitric oxide (FeNO) versus clinical symptoms, Outcome 11 Number of exacerbations per 52 weeks (exacerbation rates) (subgrouped by method used in control group).
Four of the studies utilised asthma guidelines as the basis of adjusting medications in the control group (Szefler 2008; Verini 2010; Pike 2013; Peirsman 2014). In this subgroup, for the primary outcome of number of participants with one or more exacerbations, the significant difference between the groups was still present, favouring the FeNO group (OR 0.67, 95% CI 0.51 to 0.90). In the studies that used other methods for adjusting medications as the control group, also fewer children in the FeNO group had exacerbations compared to the control group (OR 0.55, 95% CI 0.34 to 0.90). Likewise, there was a significant difference between the groups for the outcome of exacerbation rates for the studies where the control groups' management was guideline‐driven (MD ‐0.27, 95% CI ‐0.49 to ‐0.06), as well as for the studies where the control groups' management was not guideline‐driven (i.e. other) (MD ‐0.39, 95% CI ‐0.84 to 0.06). However, there was significant statistical heterogeneity in this subgroup analyses when considering only the guideline‐driven studies.
2. Use of spirometry or peak flow as an adjunctive monitoring tool for adjustment of medications (versus non‐use of spirometry or peak flow)
Five studies utilised spirometry when adjusting medications in the control group (Fritsch 2006; Szefler 2008; Verini 2010; Pike 2013; Peirsman 2014); however, spirometry was not the sole measurement for adjusting the medications, therefore this subgroup analysis could not be done. As per Table 2, all five studies used asthma guidelines which included participant‐reported symptoms, SABA use and spirometry.
3. Baseline inhaled corticosteroid dose at commencement of intervention (low‐medium (< 800 μg/day of budesonide equivalent) versus high dose (800 μg/day or more of budesonide equivalent))
In six studies, the median ICS dose at baseline was less than 800 μg/day of budesonide equivalent (Pijnenburg 2005; Fritsch 2006; de Jongste 2008; Peirsman 2014; Petsky 2015; Voorend‐van Bergen 2015). However, none of the studies analysed their data based on baseline ICS dose, hence this subgroup analysis could not be done.
One study did not provide the daily ICS dosage in micrograms per day so could not be included in this subgroup analysis (Verini 2010).
4. Fractional exhaled nitric oxide cut‐offs for adjustment of medications (20 ppb or less versus more than 20 ppb)
Three studies adjusted medications when the FeNO levels were 20 ppb or less as described in Table 2 (Fritsch 2006; Verini 2010; Petsky 2015). When considering this in the subgroup analysis, the results were similar to the main analyses.
By removing Pijnenburg 2005; Szefler 2008; de Jongste 2008; Pike 2013; Peirsman 2014; and Voorend‐van Bergen 2015 (in Analysis 1.1) who adjusted medications when FeNO was greater than 20 ppb from the first outcome (number of participants who had one or more exacerbations), the difference between groups remained statistically different (P = 0.0007; OR 0.25, 95% CI 0.11 to 0.56; I2 = 0%). Likewise, for the second outcome of exacerbation rates, by removing Szefler 2008 and Pike 2013, the difference between groups favoured the FeNO group (MD ‐0.63, 95% CI ‐0.98 to ‐0.27; I2 = 65%).
5. Fractional exhaled nitric oxide cut‐offs, based on presence of atopy
Only one study considered atopy in their algorithm for FeNO levels (Petsky 2015). Removing this study from the primary outcomes of exacerbations, the meta‐analyses results still significantly favoured the FeNO group. For the first outcome, the number of participants who had more than one exacerbation over the study period, the difference between groups remained statistically different (OR 0.65, 95% CI 0.51 to 0.85; I2 = 9%). Likewise, for the exacerbation rates, removing Petsky 2015 from the FeNO group also resulted in a statistically difference between groups (MD ‐0.27, 95% CI ‐0.49 to ‐0.06; I2 = 77%).
Sensitivity analyses
1. Excluding studies with a high risk of bias based on the 'Risk of bias' assessment
There were three included studies which had no blinding (de Jongste 2008; Verini 2010; Voorend‐van Bergen 2015). However, when the data from these studies was removed it did not alter the results of the primary outcome (exacerbations) found in the main analyses. Summary data for the number of participants who had one or more exacerbations over the study period (OR 0.67, 95% CI 0.50 to 0.89; 887 participants; 5 studies) and exacerbation rate (MD ‐0.2, 95% CI ‐0.41 to 0.0; 672 participants; 3 studies) still favoured the FeNO group.
2. Variation in the inclusion criteria
Three studies reported that not all included children were receiving ICS at recruitment (Fritsch 2006; Verini 2010; Pike 2013). Removing Verini 2010 and Pike 2013 from the analyses resulted in similar results (i.e. outcomes favoured the FeNO group); the number of participants who had one or more exacerbations (OR 0.64, 95% CI 0.49 to 0.84; 1125 participants; 6 studies). Likewise, the group differences for exacerbation rate remained significantly different between groups favouring the FeNO group (MD ‐0.23, 95% CI ‐0.43 to ‐0.02; 609 participants; 2 studies).
3. Differences in the medications used in the intervention and comparison group
There were no studies that adjusted medications only for one arm, therefore this planned sensitivity analysis was not undertaken.
4. Analysis using random‐effects model
Using a random‐effects model did not change the significant group differences between the groups (i.e. favoured the FeNO group), in the number of participants who had one or more exacerbations over the study period (OR 0.58, 95% CI 0.42 to 0.81; 1279 participants; 8 studies).
Due to the high levels of heterogeneity (I2 = 67%), we used a random‐effects model to analyse number of exacerbations per 52 weeks, which resulted in a non‐statistically significant estimate favouring the FeNO group (MD ‐0.37, 95% CI ‐0.80 to 0.06; 736 participants; 4 studies). There was a significant difference between groups when a fixed‐effect model was applied (MD ‐0.30, 95% CI ‐0.49 to ‐0.10; 736 participants; 4 studies), but this latter model is considered less appropriate in the context of high levels of heterogeneity.
5. Analysis by 'strategy received'
One study used a hierarchy management protocol that was based solely on the use of steroids for each step (i.e. without consideration for using montelukast or LABA, or both, at any point) (Pijnenburg 2005). Removing this study from the analyses did not alter the significant group differences found in the main analyses. The number of participants who had one or more exacerbations over the study period favoured the FeNO arm (OR 0.62, 95% CI 0.48 to 0.8; 1190 participants; 7 studies).
Discussion
Summary of main results
The nine RCTs included in this review involved 1426 children (1329 completed). The studies varied in many aspects including the FeNO levels used, the algorithms, study duration and the strategy used for the control arm.
All studies reported our review's primary outcome (exacerbation). However, the studies defined exacerbation in various ways. Data from eight studies were combined for the meta‐analysis of the outcome, number of participants having one or more asthma exacerbation. Significantly fewer children in the FeNO group had exacerbations compared to the control group (OR 0.58, 95% CI 0.45 to 0.75). The NNTB over 52 weeks was 9 (95% CI 6 to 15). There was no difference between the groups when comparing the exacerbation rates (MD ‐0.37, 95% CI ‐0.8 to 0.06). When combining seven studies, we found that fewer children in the FeNO group required rescue courses of oral corticosteroids compared to controls (OR 0.63, 95% CI 0.48 to 0.83). However, there was no difference between the groups for severe exacerbations requiring hospitalisation (OR 0.75, 95% CI 0.41 to 1.4). There were 20 hospitalisations in the FeNO group versus 26 in the control group.
In the subgroup analyses, the main analyses for the primary outcome of exacerbations continued to favour the FeNO group when restricting the analysis to the studies that utilised guidelines for the control group (number of participants who had one or more exacerbation: OR 0.67, 95% CI 0.51 to 0.90; exacerbation rate: MD ‐0.27, 95% CI‐0.49 to ‐0.06). There was no statistical difference between the subgroups in these analyses.
In the sensitivity analyses, the only changes seen in the primary outcome analyses was when we applied the fixed‐effect analysis to the outcome exacerbation rates per 52 weeks. As per our protocol, we chose to perform our primary analysis of this outcome with a random‐effects model, which is more appropriate in the context of the substantial heterogeneity detected (I2 = 67%). Unlike the random‐effects model, the fixed‐effect model resulted in a statistically significant estimate favouring the FeNO group (MD ‐0.30, 95% CI ‐0.49 to ‐0.10; 736 participants; 4 studies). However, the number of participants who had one or more exacerbation over the study period (analysed primarily with a fixed‐effect model) remained favourable towards the FeNO group when a sensitivity analysis was performed with a random‐effects model (OR 0.58, 95% CI 0.42 to 0.81).
In contrast to the data relating to exacerbations, there was no significant difference between groups for any of the secondary outcomes (FEV1, FeNO levels, symptom scores or final ICS dose).
Overall completeness and applicability of evidence
This review included nine studies but not all studies could be included in every outcome for the meta‐analyses. The meta‐analyses consisted of data from two to eight studies. The number of children for the various outcomes ranged from 317 (outcome: ICS dose at final visit) to 1297 (outcome: Number of participants who had one or more exacerbations over the study period). Therefore, the completeness of the review was limited by the available data, although we contacted the authors of the included studies for additional data.
Two of the primary outcomes ('Number of participants who had one or more exacerbations over the study period' and 'Severe exacerbations requiring oral corticosteroids') favoured the FeNO arm, however there was no significant group differences for 'Exacerbation rate', 'Severe exacerbations requiring hospitalisation' or for any secondary outcomes (symptom scores, FeNO at end of study, FEV1 at end of study or ICS doses). There were no changes in the primary outcomes when subgroup analysis was undertaken with FeNO group being favoured in three out of four of the primary analyses.
All nine studies were hospital‐based and undertaken since the early 2000's in affluent countries; three in the Netherlands (Pijnenburg 2005; de Jongste 2008; Voorend‐van Bergen 2015), one in Austria (Fritsch 2006), one in Belgium (Peirsman 2014), one in Australia (Petsky 2015), one in the UK (Pike 2013), one in the USA (Szefler 2008), and one in Italy (Verini 2010). There is a gap of evidence from the low‐income countries, therefore limiting this review's findings in resource‐poor settings. Likewise, none of the included studies were from a primary care setting, therefore restricting interpretation of these findings to hospital settings only (as children looked after in primary care are likely to have less severe asthma).
Guidelines on the interpretation of FeNO levels suggest using a cut‐off of less than 20 ppb as normal and more than 35 ppb as reflective of the presence of inflammation in children (Dweik 2011). However, it remains unknown how other significant influences of FeNO should be considered. These influences include ethnicity (ATS 2005) and atopy (Petsky 2015). Further, the FeNO cut‐off values used to adjust the medications varied among the studies although it could be argued that the cut‐off used should be individualised with each child having their own baseline FeNO value. None of the studies used this approach. Thus, it remains unknown how best to use FeNO values.
Also, as FeNO levels reflect airway eosinophilia in steroid‐naive people, the results of the review are unlikely to apply to those children with non‐eosinophilic asthma.
In our review, there was a discordance between the beneficial effect of using FeNO to guide asthma therapy for exacerbations compared to other clinically important outcomes such as QoL, asthma control and lung function. One possible reason relates to a type‐1 error (insufficient sample size). However, 724 participants used the ACQ and 380 participants used the PACQLQ. Thus, it is unlikely that there was a type‐1 error present.
Lastly, none of the studies included in this review undertook a cost analyses and its absence limits the applicability in 'real‐life' clinical practice.
Quality of the evidence
The 'Summary of findings' table summarises the evidence for the three main outcomes relating to exacerbations and ICS dose. Overall the quality of evidence was very low to moderate using the GRADE system. As two studies were not blinded (de Jongste 2008; Verini 2010) and another (Voorend‐van Bergen 2015) was single blinded this reduced our confidence in these studies as they introduced bias. Removing these studies for the sensitivity analysis, still showed a reduction in the number of exacerbations in the FeNO group. However, we downgraded the evidence using GRADE to moderate as displayed in Table 1.
We downgraded the outcome of exacerbation rate to very low due to the statistical heterogeneity (I2 = 67%, P = 0.03), imprecision and risk of bias. The fact that a random‐effects model showed no difference between the groups, whereas a fixed‐effect model did show a difference, demonstrates the imprecision and potential skew of the data. The study that likely contributed to the statistical heterogeneity was that of Pike 2013 who stated that their data for exacerbation rates was skewed when they provided further data to us. Consequently, they reported their published data as medians and interquartile ranges.
Potential biases in the review process
We are unaware of any biases in the review process. We used a comprehensive search strategy and adhered to the protocol. Two review authors (HP, KK) independently assessed the risk of bias. We contacted the corresponding authors of all the studies for raw data to include in the meta‐analysis. One review author and the review editor (Christopher Cates) independently checked data extraction, risk of bias assessment and downgrading decisions for the 'Summary of findings' tables to minimise the risk of bias in the review process.
As two of the review authors (HP, AC) conducted one of the studies included in this review (Petsky 2015), a separate review author (KK) made final decisions on this paper's risk of bias.
Agreements and disagreements with other studies or reviews
This review updated a previous Cochrane Review (Petsky 2009), which included studies involving children and adults. The decision was to separate the review based on population ages and the increased clinical trials on the subject. The original review included two adult studies and four paediatric studies involving 1010 participants (Petsky 2009). This paediatric review includes nine studies with 1329 children completing. A separate systematic review on adults includes seven studies with 1546 participants completing (Petsky 2016). The review in adults found similar results to this paediatric review.
Results from the original review (Petsky 2009) were different to those of this current review. The old review found no significant difference between the groups for the primary outcome of exacerbations. The four paediatric papers included in the original review reported that the FeNO group experienced fewer exacerbations in comparison to the control group, but the difference was not significant (P = 0.06) when combining three studies in a meta‐analysis (OR 0.75, 95% CI 0.55 to 1.01) (Pijnenburg 2005; Fritsch 2006; Szefler 2008; de Jongste 2008). However, combining the data from eight studies in this review showed that the number of participants experiencing an exacerbation was significantly lower (P = 0.0002) in the FeNO group compared to the control group (OR 0.62, 95% CI 0.49 to 0.80) (Pijnenburg 2005; Szefler 2008; de Jongste 2008; Verini 2010; Pike 2013; Peirsman 2014; Petsky 2015; Voorend‐van Bergen 2015). There was no heterogeneity between the studies (I2 = 21%).
Lu 2015 completed a meta‐analysis comparing the use of FeNO versus guideline‐based management for children with asthma. They included six studies with 506 participants. Their results were similar to this Cochrane Review. Lu and coworkers described that significantly fewer participants in the FeNO group had exacerbations compared to the control group (more than one exacerbation: OR 0.69, 95% CI 0.53 to 0.90; P = 0.005). As with this Cochrane Review, Lu 2015 described no difference between groups for the outcomes of FeNO levels, FEV1 or ICS dose.
Gomersal and colleagues conducted a systematic review but did not undertake a meta‐analysis comparing FeNO‐guided management with any other monitoring strategy for children with asthma (Gomersal 2016). Their review included seven studies and the authors stated that there was a "trend towards reduced exacerbation and increased medications use" in the FeNO group. Furthermore, they identified issues with heterogeneity between the algorithms and included cohorts. They concluded that the benefits of utilising FeNO monitoring in children with asthma remains ambiguous.
There are no guidelines currently that recommend the use of FeNO routinely in monitoring asthma. However, guidelines from the National Institute for Health and Care Excellence are currently focusing on the impact and feasibility of implementing FeNO in a diagnosis algorithm (NICE interim findings 2016).
Authors' conclusions
Implications for practice.
This review has demonstrated that tailoring asthma medications based on exhaled nitric oxide (FeNO) levels significantly reduces the number of children with one or more exacerbation (defined as any exacerbation or rescue oral corticosteroid courses but not hospitalisations) during the study period. However, use of the FeNO strategy was not beneficial for exacerbation rates, or the secondary outcomes of forced expiratory volume in one second (FEV1), FeNO levels, inhaled corticosteroid doses or symptom scores. Exacerbation rates were only significantly different between groups when the less appropriate fixed‐effect model was applied to this outcome.
Thus, the use of FeNO to guide therapy decisions for medication children with asthma cannot be universally advocated. The intervention may be most useful in a subset of children with asthma.
Implications for research.
Further double‐blind, parallel group, randomised controlled trials are required. Studies should be conducted in primary care and consider various cut‐offs for FeNO levels and other significant influences of FeNO levels such as atopy, sex and ethnicity. A 'one size fits all' approach in relation to FeNO levels may not be providing a clear picture. The effect of tailoring asthma medications based on different levels of asthma severity should also be considered. Further cost analyses and adverse events of inhaled and oral corticosteroids would provide additional important information.
Feedback
Queries about numbers of participants analysed, 20 February 2019
Summary
We are analysing the Clinical Questions for exhaled nitric oxide levels to guide the treatment in children with asthma, including latest articles with reference to this Cochrane Review, in order to revise the asthma guidelines in Japan. We are of the opinion that the Cochrane Review is a wonderful systematic review, and request responses to the following questions.
Q1. We recognize that the analysis of systematic review is based on the intention‐to‐treat (ITT) analysis. However, the per‐protocol analysis (PPT) has been conducted in many analyses. Please do explain how they were used.
Analysis 1.2Pike 2013 28 3.71 (2.54) 35 3.2 (2.11) The number of patients of Pike 2013 described in other analyses were 44 (FeNO strategy) and 46 (control strategy).
Analysis 1.6de Jongste 2008 50 39 The number of patients of Pike 2013 described in other analyses were 75 (FeNO strategy) and 72 (control strategy).
Analysis 1.5 and p.45 Analysis 1.6 The number of patients of Pijnenburg 2005 in analysis 1.5 were 39 for FeNO strategy and 46 for control strategy, whereas they were 42 and 47 in analysis 1.6, respectively.
Analyses 1.3, 1.4, 1.7, 1.9 Although 'Analysis 1.1' in Voorend‐van Bergen 2015 was based on the ITT number (FeNo strategy N = 92, control strategy N = 89), it was analysed based on the PPT number (FeNo strategy N = 91, control strategy N = 87) since analysis 1.3.
Q2. Analysis 1.1Szefler 2008 91/276 115/270 We would like to raise another question about the number of people with exacerbations. You have described the same number in analysis 1.4 that analysed the number of patients requiring rescue oral corticosteroids. However, Szefler 2008 defined asthma exacerbations as conditions of hospital admissions, unscheduled visits, and/or prednisone use in the statistical methods section (p.1067 to 1068). Furthermore, they have separately described ≥ 1 prednisolone course and ≥1 exacerbations in Table 3. Please do provide a clarification on how to calculate the data.
Q3. Finally, we have a question about the paper mentioned in the text. You have mentioned that five studies reported hospitalisation due to worsening of the asthma symptoms (Fritsch 2006, Szefler 2008, Pike 2013, Peirsman 2014, and Voorend‐van Bergen 2015). However, the number of patients that required hospitalisation has not been described by Fritsch 2006, and the analysis 1.3 figure does not include Fritsch 2006.
Reply
Q1‐1: We wrote to the authors for raw data to allow inclusion in our meta‐analysis. We received this information and reported it in our analysis. Participant dropouts throughout the study meant the full 52 weeks of data were not available for all outcomes. For analysis 1.2 (Number of exacerbations per 52 weeks), the number of participants analyzed appears less than the number of patients reported as having completed the study. We are not able to explain the reason for this apparent inconsistency.*
Q1‐2: The numbers quoted refer to the study by de Jongste 2008 (not Pike). We recognise this as an error in our data and have now corrected the participant numbers. This does not change the results of the study.
Initial results were (GM 0.98, 95%CI 0.87 to 1.11; 356 participants; 3 studies; I2 = 69%). The corrected results are (GM 0.99, 95% CI 0.87 to 1.11; 414 participants; 3 studies; I2 = 69%).
Q1‐3: We used the total number of participants measured for lung function, in accordance with usual Cochrane policy. Use of the full number randomised would have given too much weight to the study due to increased precision around effect estimates in response to greater participant numbers. We acknowledge this may have looked like a per protocol analysis.
Q1‐4: Please refer Q1‐3 (above) as the reason is the same.
Q2: This misinformation arose as a result of an unintended error. This has now been amended in line with the information provided in Table 3.
The significant differences between these outcomes (Outcomes 1.1, 1.3 and 1.4) have not changed as a result of this, however the NNTB has altered from 9 (95% CI 6 to 15) to 10 (95% CI 7 to 20).
Q3: Thank you. As described in analysis 1.3, deJongste 2008 had 4 hospitalisations in the FeNO arm and 10 in the control arm (not Fritsch 2006). There was a mistake in our text that has now been amended to read: "Five studies reported hospitalisations due to worsening of asthma symptoms (de Jongste 2008; Szefler 2008; Pike 2013; Peirsman 2014; Voorend‐van Bergen 2015)…" Thank you for advising us of this error.
* this response was amended in response to a further query from the feedback submitters.
Contributors
Feedback authors: Yu Kuwabara, Tetsuharu Manabe, Yuri Takaoka. Systematic review members of the Japanese Pediatric Guideline for the Treatment and Management of Asthma 2020 in the Japanese Society of Pediatric Allergy and Clinical Immunology.
Review authors: Helen Petsky, Kayleigh Kew, Anne Chang.
What's new
| Date | Event | Description |
|---|---|---|
| 20 May 2019 | Amended | Feedback response clarified in response to a further query from feedback submitters. Additional text added to Q1‐1 as follows "...for all outcomes. For analysis 1.2 (Number of exacerbations per 52 weeks), the number of participants analyzed appears less than the number of patients reported as having completed the study. We are not able to explain the reason for this apparent inconsistency." |
History
Protocol first published: Issue 1, 2015 Review first published: Issue 11, 2016
| Date | Event | Description |
|---|---|---|
| 19 March 2019 | Feedback has been incorporated | Feedback added see Feedback 1. Correction to data, no changes to final conclusions. |
| 9 January 2017 | Amended | Sentence amended to make the meaning clearer. |
Acknowledgements
We thank Elizabeth Stovold for conducting the relevant searches.
We also thank the study authors who provided further data to allow inclusion of their data into the meta‐analyses: Katy Pike, Marielle Pijnenburg (Voorend‐van Bergen 2015).
We are grateful to Dr Christopher Cates, the Contact Editor for this review, who commented critically on the review and assisted in the data analyses.
The Background and Methods sections of this review are based on a standard template used by Cochrane Airways.
Appendices
Appendix 1. Sources and search methods for the Cochrane Airways Group Specialised Register (CAGR)
Electronic searches: core databases
| Database | Frequency of search |
| CENTRAL (the Cochrane Library) | Monthly |
| MEDLINE (Ovid) | Weekly |
| Embase (Ovid) | Weekly |
| PsycINFO (Ovid) | Monthly |
| CINAHL (EBSCO) | Monthly |
| AMED (EBSCO) | Monthly |
Hand‐searches: core respiratory conference abstracts
| Conference | Years searched |
| American Academy of Allergy, Asthma and Immunology (AAAAI) | 2001 onwards |
| American Thoracic Society (ATS) | 2001 onwards |
| Asia Pacific Society of Respirology (APSR) | 2004 onwards |
| British Thoracic Society Winter Meeting (BTS) | 2000 onwards |
| Chest Meeting | 2003 onwards |
| European Respiratory Society (ERS) | 1992, 1994, 2000 onwards |
| International Primary Care Respiratory Group Congress (IPCRG) | 2002 onwards |
| Thoracic Society of Australia and New Zealand (TSANZ) | 1999 onwards |
MEDLINE search strategy used to identify trials for the CAGR
Asthma search
1. exp Asthma/
2. asthma$.mp.
3. (antiasthma$ or anti‐asthma$).mp.
4. Respiratory Sounds/
5. wheez$.mp.
6. Bronchial Spasm/
7. bronchospas$.mp.
8. (bronch$ adj3 spasm$).mp.
9. bronchoconstrict$.mp.
10. exp Bronchoconstriction/
11. (bronch$ adj3 constrict$).mp.
12. Bronchial Hyperreactivity/
13. Respiratory Hypersensitivity/
14. ((bronchial$ or respiratory or airway$ or lung$) adj3 (hypersensitiv$ or hyperreactiv$ or allerg$ or insufficiency)).mp.
15. ((dust or mite$) adj3 (allerg$ or hypersensitiv$)).mp.
16. or/1‐15
Filter to identify RCTs
1. exp "clinical trial [publication type]"/
2. (randomised or randomised).ab,ti.
3. placebo.ab,ti.
4. dt.fs.
5. randomly.ab,ti.
6. trial.ab,ti.
7. groups.ab,ti.
8. or/1‐7
9. Animals/
10. Humans/
11. 9 not (9 and 10)
12. 8 not 11
The MEDLINE strategy and RCT filter are adapted to identify trials in other electronic databases.
Appendix 2. Search strategy to identify relevant trials from the CAGR
#1 AST:MISC1
#2 MeSH DESCRIPTOR Asthma Explode All
#3 asthma*:ti,ab
#4 #1 or #2 or #3
#5 MeSH DESCRIPTOR Nitric Oxide
#6 nitric* NEXT oxide*
#7 FeNO
#8 eNO
#9 "airway inflammation"
#10 "exhaled NO"
#11 biomarker*:ti,ab
#12 #5 or #6 or #7 or #8 or #9 or #10 or #11
#13 #4 and #12
[Note: in search line #1, MISC1 denotes the field in which the reference has been coded for condition, in this case, asthma]
Appendix 3. Search strategy to identify relevant trials for ClinicalTrials.gov and World Health Organization trials portal
"exhaled nitric oxide" AND "asthma" AND "clinical trials"
Data and analyses
Comparison 1. Asthma treatment tailored on fractional exhaled nitric oxide (FeNO) versus clinical symptoms.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Number of participants who had ≥ 1 exacerbations over study period | 8 | 1279 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.62 [0.49, 0.80] |
| 2 Number of asthma exacerbations per 52 weeks (exacerbation rates) | 4 | 736 | Mean Difference (IV, Random, 95% CI) | ‐0.37 [‐0.80, 0.06] |
| 3 Number of participants with severe exacerbations requiring hospitalisation | 6 | 1110 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.75 [0.41, 1.36] |
| 4 Number of participants with severe exacerbations requiring rescue oral corticosteroids | 7 | 1169 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.63 [0.48, 0.83] |
| 5 FEV1 %predicted at final visit | 7 | 1181 | Mean Difference (Fixed, 95% CI) | 1.00 [‐0.07, 2.07] |
| 6 FeNO geometric mean level at final visit | 3 | 414 | Geometric Mean (Fixed, 95% CI) | 0.98 [0.87, 1.11] |
| 7 Symptom score as per Asthma Control Test | 2 | 724 | Mean Difference (IV, Fixed, 95% CI) | 0.14 [‐0.18, 0.47] |
| 8 Symptom score as per quality of life | 3 | 380 | Mean Difference (Fixed, 95% CI) | 0.09 [‐0.08, 0.27] |
| 9 Inhaled corticosteroid dose at final visit (budesonide equivalent) | 3 | 317 | Mean Difference (IV, Fixed, 95% CI) | 63.95 [‐51.89, 179.79] |
| 10 Number of participants who had ≥ 1 exacerbations over study period (subgrouped by method used in control group). | 8 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 10.1 Guideline driven | 4 | 799 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.67 [0.51, 0.90] |
| 10.2 Other control | 4 | 480 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.55 [0.34, 0.90] |
| 11 Number of exacerbations per 52 weeks (exacerbation rates) (subgrouped by method used in control group) | 4 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 11.1 Guideline driven | 3 | 673 | Mean Difference (IV, Fixed, 95% CI) | ‐0.27 [‐0.49, ‐0.06] |
| 11.2 Other control | 1 | 63 | Mean Difference (IV, Fixed, 95% CI) | ‐0.39 [‐0.84, 0.06] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
de Jongste 2008.
| Methods | Prospective, open‐label, randomised, multicentre, parallel group study where ICS was adjusted every 3 weeks based on FeNO and symptom scores, or symptom scores alone. 4 randomised participants (2 in FeNO group, 2 in symptom group) were excluded from final results due to severe non‐compliance (2), inappropriate inclusion (no allergy 1) and moving abroad (1). Study duration 30 weeks. |
|
| Participants | 151 children randomised. FeNO group = 75: mean age 11.6 yrs (SD 2.6), 46 boys, 29 girls. Symptom group = 72: mean age 11.8 yrs (SD 4.3), 54 boys, 18 girls. Inclusion criteria: participants aged 6 to 18 yrs, stable mild‐moderate asthma, diagnosed according to GINA guidelines, treatment with 200 μg to 1000 μg of inhaled budesonide or equivalent daily for 2 months prior to randomisation, and RAST class ≥ 2, or a positive SPT to ≥ 1 airborne allergen. Exclusion criteria: active smoking, previous admission to an ICU for asthma and concomitant disease that might affect FeNO. |
|
| Interventions | All participants scored asthma symptoms in an electronic diary over 30 weeks. FeNO group: participants received a portable FeNO analyser. Data were transmitted daily to the co‐ordinating centres. Participants were telephoned every 3 weeks and their steroid dose was adapted according to FeNO and symptoms. Control group: participants were treated according to symptoms. Children were seen at 3, 12, 21 and 30 weeks for examination, assessment of FeNO, spirometry before and after salbutamol, and recording of adverse events. |
|
| Outcomes | Primary outcome: proportion of symptom‐free days over the last 12 study weeks. Secondary outcomes: cumulative symptom scores, ICS dose as budesonide equivalent, FEV1 and reversibility, FeNO0.05, prednisone courses, emergency visits, hospitalisations for asthma and PACQLQ scores. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Insufficient information in the published article. |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information of randomisation in published article. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open label study ‐ no blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Open label study ‐ no blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | "Intention to treat analysis was performed for all subjects who were enrolled" (stated in published article). |
| Selective reporting (reporting bias) | Unclear risk | Outcomes were reported incompletely and were unable to be included in the meta‐analysis. |
| Other bias | High risk | The calibration of the NIOX Minos after the study showed drift outside the manufacturer's specifications in 11 of 77 instruments. The article has also reported that "a number" of the Niox Mino's had to be replaced as a risk of malfunctioning was detected. The study was supported by the company (Aerocrine AB, Sweden) who manufactured the FeNO analyser. |
Fritsch 2006.
| Methods | A prospective, randomised, single‐blind parallel trial examining the inclusion of repeated FeNO measurements into asthma monitoring over 6 months. In the FeNO group, treatment was based on symptoms, beta‐agonists use, lung function and FeNO. Treatment of the control group was based on symptoms, beta‐agonists use and lung function only. 5 participants dropped out, unsure of when these occurred. Over the 6 months, there were 5 visits at 6‐week intervals. |
|
| Participants | 52 participants entered the study. FeNO group: n = 22; mean age 11.3 yrs (SD 3.4), 14 boys, 8 girls. Control group: n = 25; mean age 12.1 yrs (SD 2.8), 14 boys, 11 girls. Attended paediatric pulmonology outpatient clinic from University Children's Hospital, Vienna. Inclusion: aged 6 to 18 yrs with asthma diagnosis as based on American Thoracic Society's criteria. Positive SPT or RAST > 1. Exclusion: children who had received oral or IV steroid treatment 4 weeks prior to their first visit. |
|
| Interventions | Participants were run‐in for 4 weeks. Randomised at visit 1 then outpatient visits at 6, 12, 18 and 24 weeks. FeNO group: treatment based on symptoms, beta‐agonist use, lung function and FeNO. Control group: treatment based on symptoms, beta‐agonist use and lung function. |
|
| Outcomes | Primary outcome: FEV1 Secondary outcomes: number of exacerbations, MEF 50%predicted, better symptom control, lower SABA and ICS dose. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Insufficient information of randomisation in published article. No details on randomisation methods. |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information of randomisation in published article. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Single blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Insufficient information provided, unsure of who was aware of group allocation. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Insufficient information provided on why dropouts occurred. |
| Selective reporting (reporting bias) | High risk | Primary outcome not reported completely to allow data to be entered into the meta‐analysis. |
| Other bias | High risk | FeNO measurements could not be performed in 23 observations due to technical problems, whether this provided a bias was unclear. Aerocrine (analyser manufacturer) assisted with data analysis. |
Peirsman 2014.
| Methods | Randomised, single‐blind, parallel study comparing asthma treatment adjusted based on GINA guidelines (clinical group) vs treatment guided by FeNO (FeNO group). Participants had 5 visits (baseline, and months 3, 6, 9 and 12). 6 children did not complete the study (4 in clinical group, 2 in FeNO group). |
|
| Participants | 99 children randomised. FeNO group: n = 49; mean age 10.6 yrs (SD 2.2), 33 boys, 16 girls. Clinical group: n = 50; mean age 10.7 yrs (SD 2.1), 33 boys, 17 girls. Children recruited from 7 Belgian hospitals. Inclusion criteria: children with mild‐to‐severe asthma according to GINA guidelines for > 6 months and allergic sensitisation (i.e. positive SPT or specific IgE antibodies against inhalant allergens). Exclusion criteria: significant comorbidity, acute asthma exacerbation or taken experimental medication 4 weeks prior to the screening visit, hospitalisation or systemic corticosteroids 12 weeks prior to screening visit (or both), or OCS dependency. |
|
| Interventions | FeNO group: treatment aimed to keep FeNO below 20 ppb. Clinical group: treatment based on GINA guidelines (i.e. reporting of symptoms, need for rescue treatment in preceding 2 weeks and FEV1). |
|
| Outcomes | Primary outcome: symptom‐free days using first 4 questions from childhood ACT. Secondary outcomes: occurrence of exacerbations, unscheduled asthma‐related contacts, hospital or emergency department admissions, non‐attendance to school and career's work absence. |
|
| Notes | Study funded partially by Merck & Co and FeNO analysers supplied by Aerocrine but neither were involved in any part of the study. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Described as an RCT but no methods reported. |
| Allocation concealment (selection bias) | Low risk | Stated that an independent nurse blinded to all participant characteristics allocated the children to the 2 groups. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Participants were blinded and physicians blinded to FeNO in clinical group only. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Physician blinded to FeNO in clinical group. Insufficient information in published article for FeNO group and whether physician was blinded to clinical symptoms in the FeNO group. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropout rate was low and balanced. |
| Selective reporting (reporting bias) | Low risk | All outcome data were presented in published article. |
| Other bias | Unclear risk | No information provided on the success in obtaining FeNO measurements at each visit. |
Petsky 2015.
| Methods | Randomised, double‐blind, parallel study evaluated whether a treatment strategy based on FeNO levels, adjusted for atopy (FeNO group), in comparison to treatment strategy based on clinical symptoms (control group) could reduce asthma exacerbations. Participants had 10 visits over 12 months (run‐in, initial, months 1, 2, 3, 4, 6, 8, 10 and 12). 8 children did not complete the study (4 in FeNO group and 4 in control group). |
|
| Participants | FeNO group: n = 31, median age 10.17 yrs (IQR 6.56 to 12.69), 18 boys, 13 girls. Symptom group: n = 32, median age 10.08 yrs (IQR 6.25 to 12.44), 13 boys, 19 girls. Inclusion criteria: children aged > 4 yrs with persistent asthma, prescribed anti‐inflammatory asthma treatment and receiving their care primarily through 2 hospitals (Brisbane and Hong Kong). Exclusion criteria: underlying cardio‐respiratory illnesses such as bronchiectasis or tracheomalacia, inability to take ICS or LABA, or previous poor adherence to medications as documented in medical charts. |
|
| Interventions | FeNO group: treatment adjusted on FeNO levels and atopic status. Symptom group: treatment adjusted as recorded on asthma symptom diary card. |
|
| Outcomes | Primary outcome: severe exacerbations defined as respiratory events requiring course of OCS with or without hospitalisation. Secondary outcomes: FEV1 % predicted, asthma QoL, symptom scores and dose of ICS at end of study (budesonide equivalent). |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation done by an independent individual off site through computer generation. |
| Allocation concealment (selection bias) | Low risk | Allocation fully concealed using opaque covers. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double blind ‐ decisions to adjust therapy was made by investigators who blinded to participant's group, and parents and children blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Treatment determined by primary physician. Two review authors listed as study authors (HP and CA). They could not be blinded but they did not make decisions in this study. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropout rates low. Intention to treat analyses were used. |
| Selective reporting (reporting bias) | High risk | Secondary outcomes not reported in sufficient details in the published paper to include in a meta‐analysis. |
| Other bias | Low risk | None noted. |
Pijnenburg 2005.
| Methods | Randomised, double‐blind study evaluating whether titrating steroids on FeNO improved asthma management in children. Stratified by baseline FeNO (> 30 or < 30 ppb) and dose of ICS (> 400 μg/day or < 400 μg/day of budesonide or equivalent). Neither participants nor physicians were aware of which group they were randomised to. 7 dropouts: 3 during run‐in, 3 from FeNO group (1 admitted to ICU) and 1 from symptom group. Study duration 12 months, with 5 visits at 3‐monthly intervals. |
|
| Participants | 89 children randomised from 108 invited from outpatient clinic. FeNO group n = 39: mean age 11.9 yrs (SD 2.9), 25 boys, 14 girls. Symptom group n = 46: mean age 12.6 yrs (SD 2.8), 30 boys, 16 girls. Inclusion: use of ICS at constant dose for at least 3 months preceding study. Atopy defined as RAST class ≥ 2 for at least 1 airborne allergen. |
|
| Interventions | Children were run‐in for 2 weeks, then 3‐monthly visits. FeNO group: FeNO‐guided ICS dosing according to predetermined algorithm. Symptom group: symptom scores influenced ICS dosing. |
|
| Outcomes | Primary outcome: cumulative steroid dose (sum of mean daily steroid doses of visits 1 to 5). Secondary outcomes: mean daily symptom score, mean daily number of bronchodilator doses taken, % of symptom‐free days during the last 4 weeks of the study, number of oral prednisone courses during the study, and provocative dose of methacholine causing a 20% fall in FEV1, FVC and MEF25 during final visit. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Insufficient information of randomisation in published article. |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information of randomisation in published article. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double blind ‐ parents and physician were blinded to allocated group. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Investigators provided the physician with an ICS dose recommendation according to predetermined algorithm. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Dropout rates low but unbalanced between groups. |
| Selective reporting (reporting bias) | Unclear risk | All outcomes reported, however the symptom scores could not be included in meta‐analyses. |
| Other bias | Unclear risk | No information provided on the success in obtaining FeNO measurements at each visit. |
Pike 2013.
| Methods | Randomised, double‐blind, parallel‐group trial. Participants were assigned to either FeNO‐based or standard management strategy arms, and asthma treatment adjusted according to a predetermined algorithm. Participants and physicians not aware of their allocation. Study duration 12 months with study visits every 2 months. 13 children did not complete the study; 10 in FeNO group (8 withdrew, 1 non‐adherence to protocol, 1 life‐threatening exacerbation) and 3 withdrew in Standard management group. |
|
| Participants | 90 children randomised from 96 screened. FeNO group n = 44: mean age 10.51 yrs (SD 2.62), 21 boys, 23 girls. Standard management group n = 46: mean age 11.42 yrs (SD 2.69), 30 boys, 16 girls. Inclusion criteria: aged 6 to 17 yrs, clinical diagnosis of asthma and treatment with beclomethasone dipropionate/budesonide ≥ 400 μg/day or fluticasone ≥ 200 μg/day. Asthma diagnosed upon a history of symptoms, ≥ 15% increase in FEV1 with bronchodilator or diurnal PEF variability ≥ 15%. |
|
| Interventions | Participants needed to be stabilised prior to randomisation, then 2 monthly visits. FeNO group: FeNO measurements and symptom control. Standard management group: symptom control as per blinded clinician (reliever use, FEV1). |
|
| Outcomes | Change in ICS dose, exacerbation frequency, FeNO measurements and lung function. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated block randomisation according to site. Stratified by ICS dose (400 μ/day to 800 μg/day or > 800 μg/day of beclomethasone dipropionate equivalent). |
| Allocation concealment (selection bias) | Low risk | Computer‐generated block randomisation according to site. Stratified by ICS dose (400 μg/day to 800 μg/day or > 800 μg/day beclomethasone dipropionate equivalent). |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double blind ‐ parents and physician were blinded to allocated group. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | A blinded clinician categorised asthma control level and therapy decisions were made by an independent clinician following a predetermined algorithm. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 10 children from FeNO group vs 3 children from standard management group did not complete the study. |
| Selective reporting (reporting bias) | Unclear risk | Baseline data not shown and reported as such in publication. |
| Other bias | High risk | Single measurement of FeNO taken at each visit, not as per American Thoracic Society/European Respiratory Society guidelines. |
Szefler 2008.
| Methods | Randomised, double‐blind, parallel‐group trial. Participants had their asthma management based on standard treatment as per NAEPP guidelines of or standard treatment modified based on measurements of FeNO. Participants and physicians were unaware of the treatment assignment. Study duration 46 weeks, with visits every 6 to 8 weeks. 12 randomised participants were lost to follow‐up before the first outcome data were collected. During the 46‐week follow‐up, 17 participants in FeNO group dropped out and 23 in the control group. |
|
| Participants | 546 participants randomised from 780 children screened. FeNO group n = 276: mean age 14.4 yrs, 146 boys, 130 girls. Control group n = 270: mean age 14.4 yrs, 142 boys, 128 girls. Inclusion criteria: aged 12 to 20 yrs, diagnosed with asthma by their physician, symptoms of persistent asthma or evidence of uncontrolled disease as defined by NAEPP guidelines, and residents of urban census tracts in which at least 20% of households had incomes below the federal poverty threshold. |
|
| Interventions | Run‐in period of 3 weeks then scheduled visits every 6 to 8 weeks for 46 weeks. At each visit FeNO was measured, days of asthma symptoms assessed, use of rescue drugs, pulmonary function, use of health care, adherence to treatment regimen and missed days of school because of asthma. FeNO group: standard treatment modified based on measurements of FeNO. Control group: standard treatment based on the guidelines of NAEPP. |
|
| Outcomes | Primary outcome: number of days with asthma symptoms. Secondary outcomes: admission to hospital, unscheduled visits to emergency departments or clinics, prednisone courses for asthma, asthma exacerbations, days of wheeze, days of interference with activities, nights of sleep deprivation, days of school or work missed, and days of interruption of guardian's activities. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Centralised block randomisation with a block size of 10. Randomisation sequence was generated from a random number table and was stratified by site using statistical software. |
| Allocation concealment (selection bias) | Low risk | Randomisation sequence generated from a random number table and stratified by site using statistical software. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Double blind ‐ participants and physician. A computer program generated the treatment option for each participant according to their allocation. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | All individual participant data were entered into a computer program which selected the treatment option for that participant based on their allocation and the treatment step. A co‐ordinator aware of the treatment allocation gave the physician the appropriate treatment regimen, as generated by the computer algorithm. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropout was low and balanced between groups. Analysis done on intention to treat. |
| Selective reporting (reporting bias) | High risk | No explanation given for missing data. Secondary outcome, days of interruption to guardian's activities, not reported. Adherence reported but stated only run‐in period adherence measured with built‐in dose counter. |
| Other bias | Unclear risk | No information published on the success of obtaining FeNO measurements. On enrolment, doses of ICS were increased by mean of 219 μg (95% CI 199 to 238) which is a large increase and could influence the reporting of participants. |
Verini 2010.
| Methods | Randomised, open‐label, parallel‐group trial. Participants had their asthma treatment adjusted based on GINA guidelines (GINA group) or GINA guidelines and FeNO measurements (FeNO group). Study duration 12 months with 3 visits (baseline, months 6 and 12). All children completed the study. |
|
| Participants | FeNO group n = 32: mean age 10.7 yrs (SD 2.4), 18 boys, 14 girls. GINA group n = 32: mean age 11.3 yrs (SD 2.1), 18 boys, 14 girls. Inclusion criteria: all children had been admitted for allergic asthma and the diagnosis physician based according to ATS/ERS criteria. |
|
| Interventions | Children reviewed 3 times over 12 months' study duration. At baseline and month 12 visits all children had clinical evaluation, allergy evaluation (SPT and IgE), lung function tests, FeNO measurement, diary card and asthma score therapy prior to randomisation. GINA group: at month 6 had diary card and clinical evaluation. FeNO group: at month 6 had diary card, clinical evaluation, lung function test, FeNO measurement and asthma score therapy. |
|
| Outcomes | No clear definition given of outcomes, however asthma severity score, asthma exacerbation frequency and asthma therapy score were the main items reported in results section. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information given regarding randomisation. |
| Allocation concealment (selection bias) | Unclear risk | No information given regarding randomisation. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open label ‐ both physician and participant knew allocation group. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | No blinding, therefore high risk of detection bias. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No mention of dropouts, however stated whole study population was assessed at baseline, 6 months and at end of study. |
| Selective reporting (reporting bias) | High risk | Lung function results not reported for any time points despite being measured in both groups at all visits. Additionally, baseline and final FeNO measurements were not included for the GINA group. |
| Other bias | Unclear risk | No funding information provided. No information given on the success of obtaining FeNO levels at each visit. |
Voorend‐van Bergen 2015.
| Methods | Multicentre, prospective, single‐blind, parallel‐group, 3‐armed RCT. 2 monitoring strategies compared with standard care. Web‐based strategy used ACT to adjust treatment via a website at 1 monthly intervals. FeNO‐based strategy used FeNO and ACT. Standard care strategy used ACT at 4 monthly visits. The physicians were blinded to allocation, FeNO and ACT. Treatment plans were given to the physicians through local investigators based on the study algorithms. Study duration 12 months with visits at 4 monthly intervals. 1 randomised participant from web‐based group did not complete the 12‐month follow‐up. |
|
| Participants | 272 children randomised from 481 screened. Web‐based group n = 91: mean age 10.6 yrs (SD 2.8), 60 boys, 31 girls. FeNO group n = 92: mean age 10.3 yrs (SD 2.9), 62 boys, 30 girls. Standard care group n = 89: mean age 10.2 yrs (SD 3.2), 61 boys, 28 girls. Inclusion criteria: aged 4 to 18 yrs, atopic asthma based on clinical symptoms, previous bronchodilator response > 9% increase in FEV1, previous airway hyper‐responsiveness to methacholine. |
|
| Interventions | Run‐in period of 4 weeks, then 4 monthly visits. At each visit FeNO, ACT and diary was assessed. Additionally, at visit 1 and visit 4 FEV1 and PD20 were measured. Web group: treatment modified by ACT and adherence. FeNO group: treatment modified by ACT and FeNO. Standard care group: treatment modified by ACT. |
|
| Outcomes | Primary outcome: changes from baseline of proportion of symptom‐free days. Secondary outcomes: changes from baseline of ACT, daily symptom score, daily bronchodilator use, daily ICS dose, asthma‐related QoL, dose of methacholine causing a 20% fall in FEV1 (PD20), FVC, FEV1 and MEF25 and exacerbations during the study. |
|
| Notes | We used the standard care strategy as the control group and did not consider the web‐based strategy in this review. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation program on study website, equal randomisation (1:1:1). |
| Allocation concealment (selection bias) | Unclear risk | Randomisation done through computer program on study website but no explanation if concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Single blinded ‐ participants not blinded to allocation. Physician blinded to allocation. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Investigators not blinded provided the physicians with treatment advice based on the study algorithm. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All outcomes reported when including the supplementary material. |
| Selective reporting (reporting bias) | Low risk | All outcomes reported when including the supplementary material. |
| Other bias | Unclear risk | FeNO was measured using 2 different analysers, 1 chemiluminescence and 1 portable. Not explained if individual participants used the same type at each visit. |
ACT: Asthma Control Test; CI: confidence interval; FeNO: fractional exhaled nitric oxide; FeNO0.05: fractional exhaled nitric oxide at an expiratory flow rate of 50 mL/second;
FEV1: forced expiratory volume in one second; FVC: forced vital capacity; GINA: Global Initiative for Asthma; ICS: inhaled corticosteroid; ICU: intensive care unit; Ig: immunoglobulin; IQR: interquartile range; IV: intravenous; LABA: long‐acting beta2 agonist; MEF25: maximal expiratory flow at 25% of vital flow capacity; MEF 50%predicted: maximum expiratory flow at 50% of predicted; n: number of participants; NAEPP: National Asthma Education and Prevention Program; OCS: oral corticosteroid; PD20: administered dose of a substance in the inhaled aerosol which causes the FEV1 to fall by 20%; PEF: peak expiratory flow; PACQLQ: Paediatric Asthma Caregiver's Quality of Life Questionnaire; ppb: parts per billion; QoL: quality of life; RAST: radioallergosorbent test; RCT: randomised controlled trial; SABA: short‐acting beta2 agonist; SD: standard deviation; SPT: skin prick test; yrs: years.
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Anderson 2012 | Treatment not adjusted according to FeNO. Randomised, cross‐over trial evaluating the dose response of inhaled corticosteroids in adults with asthma and elevated FeNO. |
| Calhoun 2012 | Did not include children/adolescents but based in adult population. Included in adult Cochrane systematic review by same authors (Petsky 2016). |
| Gelb 2006 | Not a RCT or treatment based on FeNO. Prospective study to assess FeNO and spirometry to predict asthma exacerbations. |
| Griese 2000 | Not a RCT or treatment based on FeNO. Prospective study to assess FeNO in comparison to symptoms adjusted using clinical symptoms. |
| Hashimoto 2011 | Study did not include children/adolescents but based in adult population. Included in adult Cochrane systematic review by same authors (Petsky 2016). |
| Honkoop 2015 | Study did not include children/adolescents but based in adult population. Included in adult Cochrane systematic review by same authors (Petsky 2016). |
| Jatakanon 1999 | Treatment not based on FeNO. Randomised into 2 double‐blind, placebo‐controlled studies (1 parallel study involving 3 groups receiving budesonide 110 μg/day, budesonide 400 μg/day or placebo. Second was a cross‐over randomised study to receive budesonide 1600 μg or placebo). |
| Jones 2001 | Not a RCT. Observational study to determine if FeNO is useful in diagnosing and predicting loss of asthma control. Participants had ICS withdrawn until loss of control or for a maximum of 6 weeks. |
| Jones 2002 | Treatment not based on FeNO. Double‐blind, parallel‐group, placebo‐controlled trial of budesonide 50 μg/day, 100 μg/day, 200 μg/day or 500 μg/day. |
| Kharitonov 1996 | Not a RCT. Observational study of the effect of increasing and then reducing the dose of ICS on FeNO, lung function and symptoms in people with asthma. |
| Kharitonov 2002 | Treatment not adjusted according to FeNO. Double‐blind, placebo‐controlled, parallel‐group study of budesonide 100 μg or 400 μg or placebo daily dose in people with mild asthma. |
| Lim 1998 | Excluded as treatment not adjusted according to FeNO. Randomised, longitudinal study monitoring the effect of increasing anti‐inflammatory medication or to continue unchanged using conventional measures of lung function, symptom scores, medication usage and peak expiratory flow rate variability. |
| Malerba 2008 | Excluded as non‐randomised. Prospective observational study including 14 participants with asthma who had asthma treatment adjusted based on sputum eosinophil counts and FeNO. |
| Powell 2011 | Excluded as study did not include children/adolescents but based in adult population. Included in adult Cochrane systematic review by same authors (Petsky 2016). |
| Shaw 2007 | Excluded as study did not include children/adolescents but based in adult population. Included in adult Cochrane systematic review by same authors (Petsky 2016). |
| Smith 2005 | Excluded as study did not include children/adolescents but based in adult population. Included in adult Cochrane systematic review by same authors (Petsky 2016). |
| Syk 2013 | Excluded as study did not include children/adolescents but based in adult population. Included in adult Cochrane systematic review by same authors (Petsky 2016). |
| Zacharasiewicz 2005 | Not a RCT. Prospective and observation study in children using non‐invasive measures (FeNO, induced sputum and exhaled breath condensate) to monitor airway inflammation to result in optimal treatment. |
FeNO: fractional exhaled nitric oxide; ICS: inhaled corticosteroid; RCT: randomised controlled trial.
Characteristics of ongoing studies [ordered by study ID]
Duong‐Quy 2015.
| Trial name or title | Exhaled NO (FeNO) Measurement used to Determine Asthma Control, Dose of Inhaled Corticosteroid and Cost in a Developing Country. |
| Methods | People with uncontrolled asthma with FeNO > 25 ppb included. Classified into 3 groups according to intervention used to determine therapy. |
| Participants | Unknown |
| Interventions | Group 1: used GINA guidelines. Group 2: used GINA + FeNO. Group 3: used FeNO alone. |
| Outcomes | ICS dose, exacerbations, cost. |
| Starting date | Unknown. |
| Contact information | Sy Duong‐Quy email sduongquy.jfvp@gmail.com. |
| Notes | Contacted Prof Duong‐Quy January 2016, he stated that the article will be submitted in the 'near future'. |
FeNO: fractional exhaled nitric oxide; GINA: Global Initiative for Asthma; ICS: inhaled corticosteroid; ppb: parts per billion.
Differences between protocol and review
We added an additional secondary outcome: 'Symptoms of asthma' as reported in the Asthma Control Score. This was added after retrieving articles to include that reported Asthma Control Score.
Contributions of authors
All authors reviewed the manuscript.
HP and KK extracted the data and performed the analysis.
HP and AC wrote the manuscript.
Sources of support
Internal sources
-
Children's Hospital Foundation, Australia.
Support to the research team accommodating AC and HP
-
St George's, University of London, UK.
Kayleigh Kew
External sources
-
National Health Medical Research Council, Australia.
Support for AC and postdoctoral scholarship for HP through a Centre of Research Excellence
-
Asthma Australia, Australia.
Early career fellowship for HP commenced in 2016
-
National Institute for Health Research, UK.
- This project was supported by the National Institute for Health Research (NIHR), via Cochrane Infrastructure, Cochrane Programme Grant or Cochrane Incentive funding to the Airways Group. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, National Health Service or the Department of Health.
Declarations of interest
HP and AC: have conducted one RCT (Petsky 2015), which was one of the included studies in this review.
KK: none known.
Edited (no change to conclusions)
References
References to studies included in this review
de Jongste 2008 {published data only}
- Jongste J, Carraro S, Hop W, the CHARISM Study Group, Baraldi E. Daily telemonitoring of exhaled nitric oxide and symptoms in the treatment of childhood asthma. American Journal of Respiratory and Critical Care Medicine 2008;179(2):93‐7. [DOI: 10.1164/rccm.200807-1010OC] [DOI] [PubMed] [Google Scholar]
Fritsch 2006 {published data only}
- Fritsch M, Uxa S, Horak F, Putschoegl B, Dehlink E, Szepfalusi Z, et al. Exhaled nitric oxide in the management of childhood asthma: a prospective 6‐months study. Pediatric Pulmonology 2006;41(9):855‐62. [DOI: 10.1002/ppul.20455] [DOI] [PubMed] [Google Scholar]
Peirsman 2014 {published data only}
- Peirsman E, Carvelli T, Hage P, Hanssens L, Pattyn L, Raes M, et al. Exhaled nitric oxide in childhood allergic asthma management: a randomised controlled trial. Pediatric Pulmonology 2014;49(7):624‐31. [DOI: ] [DOI] [PubMed] [Google Scholar]
- Peirsman, E. Response to the Editor: "Fractional exhaled nitric oxide‐guided algorithm for children with allergic asthma". Pediatric Pulmonology 2015;50(9):934‐5. [DOI: 10.1002/ppul.23137] [DOI] [PubMed] [Google Scholar]
- Qun Ui, Lee. Fractional exhaled nitric oxide‐guided algorithm for children with asthma. Pediatric Pulmonology 2015;50(9):932‐3. [DOI: 10.1002/ppul.23115] [DOI] [PubMed] [Google Scholar]
Petsky 2015 {published data only}
- Petsky H, Li A, Au C, Kynaston J, Turner C, Chang A. Management based on exhaled nitric oxide levels adjusted for atopy reduces asthma exacerbations in children: a dual centre randomized controlled trial. Pediatric Pulmonology 2015;50(6):535‐43. [DOI: 10.1002/ppul.23064] [DOI] [PubMed] [Google Scholar]
Pijnenburg 2005 {published data only}
- Pijnenburg M, Bakker E, Hop W, Jongste J. Titrating steroids on exhaled nitric oxide in children with asthma. American Journal of Respiratory and Critical Care Medicine 2005;172(7):831‐6. [DOI: 10.1164/rccm.200503-4580C] [DOI] [PubMed] [Google Scholar]
Pike 2013 {published data only}
- Pike K, Selby A, Price S, Warner J, Connett G, Legg J, et al. Exhaled nitric oxide monitoring does not reduce exacerbation frequency or inhaled corticosteroid does in paediatric asthma: a randomised controlled trial. Clinical Respiratory Journal 2013;7(2):204‐13. [DOI: 10.1111/j.1752-699X.2012.00306.x] [DOI] [PubMed] [Google Scholar]
Szefler 2008 {published data only}
- Gruchalla RS, Sampson HA, Matsui E, David G, Gergen PJ, Calatroni A, et al. Asthma morbidity among inner‐city adolescents receiving guidelines‐based therapy: role of predictors in the setting of high adherence. Journal of Allergy and Clinical Immunology 2009;124(2):213‐21. [DOI: 10.1016/j.jaci2009.05.036] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pedersen S, O'Byrne PM. Exhaled nitric oxide in guideline‐based asthma management. Lancet 2008;372(9643):1015‐7. [DOI] [PubMed] [Google Scholar]
- Szefler S, Mitchell H, Sorkness C, Gergen P, O'Connor G, Morgan W, et al. Management of asthma based on exhaled nitric oxide in addition to guideline‐based treatment for inner‐city adolescents and young adults: a randomised controlled trial. Lancet 2008;372(9643):1065‐72. [DOI: 10.1016/S0140-6736(08)61448-8] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taylor DR, Bush A. Clinical use of exhaled nitric oxide measurements. Lancet 2009;373(9661):382. [DOI] [PubMed] [Google Scholar]
Verini 2010 {published data only}
- Verini M, Consilvio N, Pillo S, Cingolani A, Spagnuolo C, Rapino D, et al. FeNO as a marker of airways inflammation: the possible implications in childhood asthma management. Journal of Allergy 2010;2010:pii: 691425. [DOI: 10.1155/2010/691425] [DOI] [PMC free article] [PubMed] [Google Scholar]
Voorend‐van Bergen 2015 {published data only}
- Beerthuizen T, Voorend‐van Bergen S, Hout W, Vaessen‐Verberne A, Brackel H, Landstra A, et al. Cost‐effectiveness of FeNO‐based and web‐based monitoring in paediatric asthma management: a randomised controlled trial. Thorax 2016;71(7):607‐13. [DOI: 10.1136/thoraxjnl-2015-207593] [DOI] [PubMed] [Google Scholar]
- Voorend‐van Bergen S, Vaessen‐Verberne AA, Brackel HJ, Landstra AM, Berg NJ, Hop WC, et al. Monitoring strategies in children with asthma: a randomised controlled trial. Thorax 2015;70(6):543‐50. [DOI: 10.1136/thoraxjnl-2014-206161] [DOI] [PubMed] [Google Scholar]
- Voorend‐van Bergen S, Vaessen‐Verberne AA, Landstra AM, Brackel HJ, Berg NJ, Merkus PJ, et al. Fractional exhaled nitric oxide monitoring does not improve asthma management in children with concordant and discordant asthma phenotypes. American Journal of Respiratory and Critical Care Medicine 2015;192(8):1016‐8. [DOI: 10.1164/rccm.201506-1103LE] [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Anderson 2012 {published data only}
- Anderson WJ, Short PM, Williamson PA, Lipworth BJ. Inhaled corticosteroid dose response using domiciliary exhaled nitric oxide in persistent asthma: the FeNOtype trial. Chest 2012;142(6):1553‐61. [DOI: 10.1378/ches.12-1310] [DOI] [PubMed] [Google Scholar]
Calhoun 2012 {published data only}
- Calhoun W, Ameredes B, King T, Icitovic N, Bleecker E, Castro M, et al. Comparison of physician‐, biomarker‐, and symptom‐based strategies for adjustment of inhaled corticosteroid therapy in adults with asthma. JAMA 2012;308(10):987‐97. [DOI] [PMC free article] [PubMed] [Google Scholar]
Gelb 2006 {published data only}
- Gelb A, Flynn Taylor C, Shinar CM, Gutierrez C, Zamel N. Role of spirometry and exhaled nitric oxide to predict exacerbations in treated asthmatics. Chest 2006;129(6):1492‐9. [DOI: 10.1378/chest.129.6.1492] [DOI] [PubMed] [Google Scholar]
Griese 2000 {published data only}
- Griese M, Koch M, Latzin P, Beck J. Asthma severity, recommended changes of inhaled therapy and exhaled nitric oxide in children: a prospective, blinded trial. European Journal of Medical Research 2000;5(8):334‐40. [PUBMED: 10958766] [PubMed] [Google Scholar]
Hashimoto 2011 {published data only}
- Hashimoto S, Brinke A, Roldaan A, Veen I, Moller G, Sont J, et al. Internet‐based tapering of oral corticosteroids in severe asthma: a pragmatic randomised controlled trial. Thorax 2011;66(6):514‐20. [DOI: 10.1136/thx.2010.153411] [DOI] [PubMed] [Google Scholar]
Honkoop 2015 {published data only}
- Honkoop P, Lijmans R, Termeer E, Snoeck‐Stroband J, Hout W, Bakker M, et al. Symptom‐ and fraction of exhaled nitric oxide‐driven strategies for asthma control: a cluster‐randomized trial in primary care. Journal of Allergy and Clinical Immunology 2015;135(3):682‐8. [DOI: 10.1016/j.jaci.2014.07.016] [DOI] [PubMed] [Google Scholar]
Jatakanon 1999 {published data only}
- Jatakanon A, Kharitonov S, Lim S, Barnes PJ. Effect of differing doses of inhaled budesonide on markers of airway inflammation in patients with mild asthma. Thorax 1999;54(2):108‐14. [DOI: 10.1136/thx.54.2.108] [DOI] [PMC free article] [PubMed] [Google Scholar]
Jones 2001 {published data only}
- Jones SL, Kittelson J, Cowan JO, Flannery EM, Hancox RJ, McLachlan CR, et al. The predictive value of exhaled nitric oxide measurements in assessing changes in asthma control. American Journal of Respiratory and Critical Care Medicine 2001;164(5):738‐43. [DOI: 10.1164/ajrccm.164.5.2012125] [DOI] [PubMed] [Google Scholar]
Jones 2002 {published data only}
- Jones SL, Herbison P, Cowan JO, Flannery EM, Hancox RJ, McLachlan CR, et al. Exhaled NO and assessment of anti‐inflammatory effects of inhaled steroids: dose‐response relationship. European Respiratory Journal 2002;20(3):601‐8. [DOI: 10.1183/09031936.02.00285302] [DOI] [PubMed] [Google Scholar]
Kharitonov 1996 {published data only}
- Kharitonov SA, Yates DH, Chung KF, Barnes PJ. Changes in the dose of inhaled steroid affect exhaled nitric oxide in asthmatic patients. European Respiratory Journal 1996;9(2):196‐201. [PUBMED: 8777950] [DOI] [PubMed] [Google Scholar]
Kharitonov 2002 {published data only}
- Kharitonov SA, Konnelly LE, Corradi M, Montuschi P, Barnes PJ. Dose‐dependent onset and cessation of action of inhaled budesonide on exhaled nitric oxide and symptoms in mild asthma. Thorax 2002;57(1):889‐96. [DOI: 10.1136/thorax.57.10.889] [DOI] [PMC free article] [PubMed] [Google Scholar]
Lim 1998 {published data only}
- Lim S, Jatakanon A, Uasuf C, Chung KF, Barnes PJ. Clinical utility of exhaled nitric oxide as a marker of disease activity in asthma. American Journal of Respiratory and Critical Care Medicine 1998;157(3 Suppl):A611. [Google Scholar]
Malerba 2008 {published data only}
- Malerba M, Ragnoli B, Radaeli A, Tantucci C. Usefulness of exhaled nitric oxide and sputum eosinophils in the long‐term control of eosinophilic asthma. Chest 2008;134(4):733‐9. [DOI: 10.1378/chest.08-0763] [DOI] [PubMed] [Google Scholar]
Powell 2011 {published data only}
- Burgess L, McCaffery K, Powell H, Murphy VE, Gibson PG, Turner RM. The influence of asthma control on psychosocial outcomes for pregnant women with asthma. Journal of Asthma 2015;52(10):1013‐9. [DOI: 10.3109/02770903.2015.1038833] [DOI] [PubMed] [Google Scholar]
- Powell H, Murphy V, Taylor DR, Hensley M, McCaffery K, Giles W, et al. Management of asthma in pregnancy guided by measurement of fraction of exhaled nitric oxide: a double‐blind, randomised controlled trial. Lancet 2011;378(9795):983‐90. [DOI: 10.1016/S0140-6736(11)60971-9] [DOI] [PubMed] [Google Scholar]
- Powell H, Murphy VE, Hensley MJ, Giles W, Clifton VL, Gibson PG. Rhinitis in pregnant women with asthma is associated with poorer asthma control and quality of life. Journal of Asthma 2015;52(10):1023‐30. [DOI: 10.3109/02770903.2015.1054403] [DOI] [PubMed] [Google Scholar]
Shaw 2007 {published data only}
- Shaw D, Berry M, Thomas M, Green R, Brightling C, Wardlaw A, et al. The use of exhaled nitric oxide to guide asthma management ‐ a randomized controlled trial. American Journal of Respiratory and Critical Care Medicine 2007;176(3):231‐7. [DOI: 10.1164/rccm.200610-1427OC] [DOI] [PubMed] [Google Scholar]
Smith 2005 {published data only}
- Smith AD, Cowan J, Brassett KP, Herbison GP, Taylor DR. Use of exhaled nitric oxide measurements to guide treatment in chronic asthma. New England Journal of Medicine 2005;352(21):2163‐73. [ISSN00284793] [DOI] [PubMed] [Google Scholar]
Syk 2013 {published data only}
- Syk J, Malinovschi, Johansson G, Unden A, Andreasson A, Lekander M, et al. Anti‐inflammatory treatment of atopic asthma guided by exhaled nitric oxide: a randomized, controlled trial. Journal of Allergy and Clinical Immunology Practice 2013;1(6):639‐48. [DOI: 10.1016/j.jaip.2013.07.013] [DOI] [PubMed] [Google Scholar]
Zacharasiewicz 2005 {published data only}
- Zacharasiewicz A, Wilson N, Lex C, Erin EM, Li AM, Hansel T, et al. Clinical use of noninvasive measurements of airway inflammation in steroid reduction in children. American Journal of Respiratory and Critical Care Medicine 2005;171(10):1077‐82. [DOI: 10.1164/rccm.200409-1242OC] [DOI] [PubMed] [Google Scholar]
References to ongoing studies
Duong‐Quy 2015 {published data only}
- Duong‐Quy S, Hua‐Huy T, Doan‐Quynh N, Nguyen‐Quoc B, Le‐Quang K, Tran‐Thanh D, et al. A study of exhaled NO (FeNO) measurement used to determine asthma control, dose of inhaled corticosteroid and cost in a developing country. European Respiratory Journal 2015;46(Suppl 59):PA5013. [Google Scholar]
Additional references
Akinbami 2009
- Akinbami LJ, Moorman JE, Garbe PL, Sondik, EJ. Status of childhood asthma in the United States, 1980‐2007. Pediatrics 2009;123(Suppl 3):S131‐45. [DOI: 10.1542/peds.2008-2233C] [DOI] [PubMed] [Google Scholar]
Anderson 2007
- Anderson HR, Gupta R, Strachan DP, Limb ES. 50 years of asthma: UK trends from 1955 to 2004. Thorax 2007;62(1):85‐90. [DOI: 10.1136/thx.2006.066407] [DOI] [PMC free article] [PubMed] [Google Scholar]
ATS 2005
- American Thoracic Society. ATS/ERS recommendations for standardized procedures for the online and offline measurement of FeNO. American Journal of Critical Care and Respiratory Medicine 2005;171(8):912‐30. [DOI: 10.1164/rccm.200406-710ST] [DOI] [PubMed] [Google Scholar]
Beerthuizen 2016
- Beerthuizen T, Voorend‐van Bergen S, Hout W, Vaessen‐Verberne A, Brackel H, Landstra A, et al. Cost‐effectiveness of FeNO‐based and web‐based monitoring in paediatric asthma management: a randomised controlled trial. Thorax 2016;71(7):607‐13. [DOI: 10.1136/thoraxjnl-2015-207593] [DOI] [PubMed] [Google Scholar]
BTS/SIGN 2016
- British Thoracic Society/Scottish Intercollegiate Guidelines Network. British guideline on the management of asthma: a national clinical guideline. www.sign.ac.uk/pdf/SIGN153.pdf (accessed 13 October 2016).
Cates 2008 [Computer program]
- Dr Christopher Cates. Visual Rx. Online NNT calculator. http://www.nntonline.net/. Dr Christopher Cates, 2008.
Douwes 2002
- Douwes J, Gibson P, Pekkanen J, Pearce N. Non‐eosinophilic asthma: importance and possible mechanisms. Thorax 2002;57(7):643‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Dupont 1998
- Dupont LJ, Rochette F, Demedts MG, Verleden GM. Exhaled nitric oxide correlates with airway hyperresponsiveness in steroid‐naive patients with mild asthma. American Journal of Respiratory and Critical Care Medicine 1998;157(3 (pt 1)):894‐8. [DOI] [PubMed] [Google Scholar]
Dweik 2011
- Dweik RA, Boggs PB, Erzurum SC, Irvin CG, Leigh MW, Lundberg JO, et al. An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applications. American Journal of Respiratory and Critical Care Medicine 2011;184(5):602‐15. [DOI: 10.1164/rccm.9120-11ST] [DOI] [PMC free article] [PubMed] [Google Scholar]
GINA 2016
- Global Initiative for Asthma. Global strategy for asthma management and prevention, 2016. ginasthma.org/2016‐gina‐report‐global‐strategy‐for‐asthma‐management‐and‐prevention (accessed 2 August 2016).
Gomersal 2016
- Gomersal T, Harnan S, Essat M, Tappenden P, Wong R, Lawson R, et al. A systematic review of fractional exhaled nitric oxide in the routine management of childhood asthma. Pediatric Pulmonology 2016;51(3):316‐28. [DOI: 10.1002/ppul.23371] [DOI] [PubMed] [Google Scholar]
GRADEpro GDT 2015 [Computer program]
- GRADE Working Group, McMaster University. GRADEpro GDT. GRADE Working Group, McMaster University, 2015.
Gupta 2006
- Gupta R, Anderson HR, Strachan DP, Maier W, Watson L. International trends in admissions and drug sales for asthma. International Journal of Tuberculosis and Lung Disease 2006;10(2):138‐45. [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Jatakanon 1998
- Jatakanon A, Lim S, Kharitonov SA, Chung KF, Barnes PJ. Correlation between exhaled nitric oxide, sputum eosinophils and methacholine responsiveness in patients with mild asthma. Thorax 1998;53(2):91‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lu 2015
- Lu M, Wu B, Che D, Qiao R, Gu H. FeNO and asthma treatment in children. Medicine 2015;94(4):e347. [DOI: 10.1097/MD.0000000000000347] [DOI] [PMC free article] [PubMed] [Google Scholar]
Müller 2005
- Müller KC, Jorres RA, Magnussen H, Holz O. Comparison of exhaled nitric oxide analysers. Respiratory Medicine 2005;99(5):631‐7. [DOI] [PubMed] [Google Scholar]
National Asthma Council 2014
- National Asthma Council Australia, Melbourne, 2014. Australian asthma handbook, Version 1.0. www.nationalasthma.org.au/handbook (accessed 31 October 2014).
NICE interim findings 2016
- National Institute for Health and Care Excellence. Asthma: diagnosing and monitoring of asthma in adults, children and young people. www.nice.org.uk/guidance/indevelopment/gid‐cgwave0640/documents (accessed 18 January 2016).
Petsky 2016
- Petsky HL, Kew KM, Turner C, Chang AB. Exhaled nitric oxide levels to guide treatment for adults with asthma. Cochrane Database of Systematic Reviews 2016, Issue 9. [DOI: 10.1002/14651858.CD011440.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
RevMan 2014 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Wardlaw 2000
- Wardlaw AJ, Brightling C, Green R, Woltmann G, Pavord I. Eosinophils in asthma and other allergic diseases. British Medical Bulletin 2000;56(4):985‐1003. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Petsky 2009
- Petsky HL, Cates CJ, Li A, Kynaston JA, Turner C, Chang AB. Tailored interventions based on exhaled nitric oxide versus clinical symptoms for asthma in children and adults. Cochrane Database of Systematic Reviews 2009, Issue 4. [DOI: 10.1002/14651858.CD006340.pub3] [DOI] [PubMed] [Google Scholar]