

Abstract
Purpose:
Biomarkers aiding treatment optimization in metastatic castration-resistant prostate cancer (mCRPC) are scarce. Presence or absence of androgen receptor (AR) splice variants, AR-V7 and ARv567es, in mCRPC patient circulating tumor cells (CTCs) may be associated with taxane treatment outcomes.
Experimental design:
A novel digital droplet PCR (ddPCR) assay assessed AR splice variant expression in CTCs from patients receiving docetaxel or cabazitaxel in TAXYNERGY (NCT01718353). Patient outcomes were examined according to AR splice variant expression, including prostate-specific antigen (PSA)50 response and progression-free survival (PFS).
Results:
Of 54 evaluable patients, 36 (67%) were AR-V7+, 42 (78%) were ARv567es+, 29 (54%) were double positive and 5 (9%) were double negative. PSA50 response rates at any time were numerically higher for AR-V7- vs AR-V7+ (78% vs 58%; p=0.23) and for ARv567es- vs ARv567es+ (92% vs 57%; p=0.04) patients. When AR-V mRNA status was correlated with change in nuclear AR from Cycle 1 Day 1 to Day 8 (n=24), AR-V7+ patients (n=16) had a 0.4% decrease vs a 12.9% and 26.7% decrease in AR-V7-/ARv567es- (n=3) and AR-V7-/ ARv567es+ (n=5) patients, respectively, suggesting a dominant role for AR-V7 over ARv567es. Median PFS was 12.02 vs 8.48 months for AR-V7- vs AR-V7+ (HR=0.38; p=0.01), and 12.71 vs 7.29 months for ARv567es- vs ARv567es+ (HR=0.37; p=0.02). For AR-V7+, AR-V7-/ARv567es+, and AR-V7-/ ARv567es- patients, median PFS was 8.48, 11.17 and 16.62 months, respectively (p=0.0013 for trend).
Conclusions:
While detection of CTC-specific AR-V7 and ARv567es by ddPCR both influenced taxane outcomes, AR-V7 primarily mediated the prognostic impact. Absence of both variants was associated with the best response and PFS with taxane treatment.
Keywords: mCRPC, ARv567es, AR-V7, cabazitaxel, docetaxel
Statement of translational relevance:
Patients with metastatic castration-resistant prostate cancer (mCRPC) have several treatment options; however, intrinsic and acquired resistance to various treatment modalities is common. Future standards of care could be shaped by prognostic and/or predictive biomarkers, such as androgen receptor (AR) splice variants. We have investigated the association between AR-V7 and ARv567es splice variant expression and response in patients receiving taxanes in the TAXYNERGY study (NCT01718353). TAXYNERGY evaluated the benefit of an early switch from docetaxel to cabazitaxel or vice versa in patients with chemotherapy-naïve mCRPC. Absence of both variants at baseline was associated with the best prostate-specific antigen response and progression-free survival in patients receiving taxanes. AR nuclear localization did not change following taxane treatment in AR-V7+ or double-negative patients, suggesting AR-V7 may be dominant over ARv567es. Our results indicate that absence of AR splice variants may be associated with a superior response to taxane treatment in mCRPC.
Introduction
Despite numerous newly available treatment options for patients with metastatic castration-resistant prostate cancer (mCRPC), optimizing response rates and longer-term outcomes remains a major challenge. Most mCRPC tumors remain dependent on active signaling from the androgen receptor (AR), primarily due to aberrant alterations of the AR, including activating mutations, copy number gains, and expression of AR-splice variants which lack the ligand binding domain and function as constitutively active transcription factors in the nucleus (1–4). Taxanes and AR-targeted agents, such as abiraterone and enzalutamide, represent the standard treatment for patients with mCRPC (5). Recent findings suggest that some tumors exhibit intrinsic or acquired resistance to these agents, and that resistance to AR-targeted therapies may be identified prior to treatment using the molecular alterations of the AR as biomarkers of response (6–8). For example, expression of AR-V7 mRNA alone (6, 9), or in combination with prostate-specific antigen (PSA) transcripts (10), in patient liquid biopsies has been correlated with resistance to abiraterone and enzalutamide. Taxane chemotherapy is the standard of care for patients with mCRPC and is the only chemotherapy that prolongs survival in these patients; however, predictive biomarkers of response to taxanes have not been identified.
Predictive biomarkers of response to specific therapies are scarce, and the choice of appropriate treatment from available options is further complicated by evidence of cross-resistance between different treatment modalities (8, 11).
We previously showed that the nuclear translocation of AR proteins, a prerequisite for AR transcriptional activity, is microtubule-dependent and as such may be predictive of response to taxane treatment (12–14). This mechanism was clinically validated in the prospective clinical trial, TAXYNERGY, where the taxane-induced decrease in AR nuclear localization (%ARNL) in patient circulating tumor cells (CTCs) was associated with higher rates of PSA response in patients treated with docetaxel or cabazitaxel (14). As most mCRPC tumors retain their dependence on androgen signaling, the expression of mutant forms or splice variants of AR in the primary tumor, CTCs and blood plasma have been assessed as potential prognostic and/or predictive biomarkers. However, the impact of AR splice variant expression on taxane clinical response has not been prospectively determined.
The two most prevalent AR splice variants are the truncated variant AR-V7 and the exon-skipping variant ARv567es. Both are expressed in primary prostate tumors and metastases (15, 16). AR-V7 mRNA expression in CTCs and blood plasma of patients with mCRPC has been associated with resistance to the AR-targeted agents, abiraterone and enzalutamide (9, 17–19). A structural domain differentiating the two variants is the hinge domain, which mediates microtubule binding and is present in ARv567es but absent from AR-V7 (12). Since this hinge domain is required for microtubule binding, AR-V7 is microtubule independent and demonstrates relative taxane resistance whereas ARv567es has reduced affinity for microtubules despite the presence of the hinge domain, which confers relative sensitivity compared with full-length AR (AR-FL), in LuCap xenografts (12, 20). The functional protein domains of full-length AR and both splice variants are shown in Figure 1. Earlier clinical studies in mCRPC have not shown a significant association between AR-V7 expression and response to taxane chemotherapy (21); while the impact of ARv567es expression has not been evaluated.
Figure 1. AR structural domains, comparison with AR splice variants and the predicted effect of taxane treatment on AR splice variant nuclear localization.

AR-FL associates with microtubules and uses them as tracks for ligand-induced nuclear translocation. Taxane treatment inhibits AR-FL nuclear accumulation and activity downstream of microtubule stabilization (13, 41). AR-FL binds microtubules via its hinge domain, which is retained in ARv567es but absent in AR-V7 (12). Taxane treatment inhibits microtubule dynamics and is predicted to differentially affect the nuclear localization of each variant as follows: AR-FL is kept inactive in the cytoplasm (top right); AR-V7 nuclear localization is unaffected, due to the hinge-less AR-V7 association with MTs (middle right); and ARv567es nuclear localization is partially impaired (bottom right). The latter is due to the fact that the entire C-terminal AR domain (exons 2–8) mediates maximal MT association (AR-FL), while the hinge domain (present in ARv567es), is the minimum functional domain required for MT binding, albeit not as extensively as the entire C-terminus (12).
AR, androgen receptor; CE, cryptic exon; DBD, DNA-binding domain; FL, full length; LBD, ligand-binding domain; NTD, N-terminal domain; MT, microtubule.
Based on our mechanistic studies (12) we hypothesized that AR-V7 expression would be associated with decreased clinical response to taxane chemotherapy, while ARv567es expression would confer increased taxane sensitivity. To test this hypothesis, we designed a novel droplet digital PCR (ddPCR) assay to assess the expression of ARv567es and AR-V7 splice variants, and AR-FL, in patient-derived CTCs. The assay is highly specific and sensitive down to single cells, and avoids co-amplification of the recently described AR-V9 variant, which is highly homologous to the AR-V7 transcript (22). This assay was used to quantify all three AR transcripts simultaneously by ddPCR in CTCs from patients with mCRPC, in a prospective clinical trial.
The Phase II TAXYNERGY (NCT01718353) study demonstrated the benefit of an early taxane switch from docetaxel to cabazitaxel or vice versa in patients with mCRPC who failed to achieve at least a 30% PSA reduction by Cycle 5 Day 1 (C5D1). Overall, 56% of patients (35 of 63 patients) achieved at least a 50% PSA reduction; 40% (25 patients) achieved the response by C5D1 and 16% (10 patients) after C5D1 (14). In the exploratory biomarker analyses presented here, we assessed the prevalence of AR-V7 and ARv567es, as presence or absence of signal by ddPCR, in patients enrolled in the TAXYNERGY study, and determined their association with PSA response rates and progression-free survival (PFS). We show that patients who had an absence of AR-V7 mRNA expression had numerically higher PSA response rates and longer PFS, while ARv567es expression also appeared to have an impact on these clinical outcomes. Interestingly, our data show that absence of both AR variants was associated with superior PSA response and longer PFS.
Patients and methods
Study design
TAXYNERGY was a non-comparative randomized Phase II study that enrolled chemotherapy-naïve patients with progressive mCRPC. Patients were randomly assigned 2:1 to initial treatment with docetaxel 75 mg/m2 or cabazitaxel 25 mg/m2 every 3 weeks. Patients achieving at least a 30% PSA decline from baseline by C5D1 continued to receive the same taxane, whereas those who did not achieve at least a 30% PSA decline were switched to the alternative taxane at C5D1. Treatment continued until disease progression, death, unacceptable toxicity, or withdrawal of consent (14).
Ethical Consideration
The protocol complied with recommendations of the 18th World Health Congress (Helsinki, 1964) and all applicable amendments. The study was approved by the institutional review board at each participating center and conducted in compliance with guidelines for Good Clinical Practice. Patients provided written informed consent before participation.
Patient sample processing and RNA extraction
As part of this study, peripheral blood samples were collected from each patient at baseline prior to initiating protocol treatment and at various time points on and after treatment, in EDTA tubes and shipped to Weill Cornell Medicine within 24 hours of the time of blood draw (14). CTCs from the whole blood of patients with mCRPC were captured using the prostate-specific membrane antigen-based geometrically enhanced differential immunocapture microfluidic device as previously described (23, 24). All patients provided written informed consent.
Droplet digital PCR
ddPCR is a digital PCR method based on water-oil emulsion droplet technology (25, 26). The ddPCR system partitions nucleic acid samples into 20,000 nanoliter-sized droplets and PCR amplification is carried out within each droplet. Unlike traditional qPCR, ddPCR allows for absolute quantification of the transcript without the need for normalization or external reference genes (27–30).
Total RNA was extracted from the enriched CTCs pool using the RNAeasy Plus Micro kit (Qiagen) as per manufacturer’s instructions. After PCR, droplets that contained a template had a fluorescent signal (positive droplets) that distinguished them from the droplets without a template (negative droplets). Number of target molecules was calculated from the ratio of detected positive droplets to total droplets, using Poisson distribution analysis. We used the CTC-derived mRNA as input for the ddPCR reactions arrayed in 96-well format using commercially available multiplexed master mixes of PCR enzyme/buffer from the One-Step RT ddPCR Advanced Kit for Probes (Bio-Rad). Primers and probes specific for AR-FL, ARv567es, and AR-V7 were used to generate amplicons for each transcript and can be found in Supplementary Table 1. AR-FL, ARv567es, and AR-V7 transcript quantifications were carried out on a QX200 ddPCR system with automated droplet generation (Bio-Rad Laboratories), as described previously (28–0). As is standard practice, no threshold was applied to the ddPCR values (10, 31, 32). Transcript copy numbers for each patient can be found in Supplementary Table 2. The assay is highly specific for each transcript, which was confirmed using HEK293T cells transfected with plasmids encoding AR-FL, AR-V7 or ARV567es. In these validation assays, each primer set specifically amplified its intended target. Positive and negative controls were included in every assay to ensure optimal primer performance. The primers/probes used for AR-V7 do not co-amplify the recently discovered and highly homologous AR-V9 variant transcript (20). The assay sensitivity was assessed in spike-in experiments demonstrating single-cell AR-V detection (Supplementary Figure 1). Briefly, we spiked the human prostate cancer cell line 22RV1, which expresses endogenous AR-FL and AR-V7 into healthy donor (HD) blood processed through the GEDI device, following the same protocol as for the patient sample processing used herein. Our results showed that the assay can reliably and repeatedly detect AR-FL and AR-V7 transcripts from a single prostate cancer cell in the presence of healthy donor peripheral blood mononuclear cells. No AR-V transcripts were detected in healthy donor (HD) blood run through the GEDI, while AR-FL was detected in 6/10 HD samples (Supplementary Figure 2).
Efficacy assessments
PSA levels were measured before treatment administration at each cycle and at the end-of-treatment visit, and then every 3 months at each follow-up visit until progression, death or study cut-off. PSA response was recorded as at least a 50% (PSA50) reduction from baseline either by C5D1 (prior to switch) or at any point during the entire treatment continuum.
PFS was defined as the time between randomization and the first documentation of radiographic tumor progression (using RECIST 1.1), clinical progression (including skeletal-related events, increasing pain requiring escalation of narcotic analgesics, urinary obstruction, etc.), PSA progression, or death from any cause. PFS was required to be confirmed at least 3 weeks after initial assessment.
Statistical considerations
Descriptive statistics were used to present the results: mean, standard deviation, median, range, number, and percentage of patients. To relate the presence of splice variants to response, standard chi-square procedures were used. To relate the presence of splice variants to PFS, Kaplan–Meier, Cox regression, and log-rank techniques were employed.
Results
Study population
Of 63 patients enrolled, 61 received taxane treatment. No new safety concerns were identified (14). AR splice variant expression data at baseline and treatment response data were available for 54 patients. For the nine excluded patients, reasons for exclusion included no PSA results (n = 1), non-evaluable CTC mRNA at baseline (n = 6), and randomized but not treated patients (n = 2). Median age was 71 years (range 53–84); 37%, 59% and 4% had an Eastern Cooperative Oncology Group performance status of 0, 1 and 2, respectively; and 43% (23 patients) had received prior AR-targeted therapy (Table 1). Baseline characteristics for this subgroup of patients from TAXYNERGY were generally similar to those published for the overall patient population in the TAXYNERGY study (14). Thirty-six were randomized to initial treatment with docetaxel, and 18 to initial treatment with cabazitaxel.
Table 1.
Baseline characteristics
| All | AR-V7-/ARv567es- | AR-V7-/ ARv567es+ | AR-V7+ | |
|---|---|---|---|---|
| N = 54 | n = 5 | n = 13 | n = 36 | |
| Median age, years (range) | 71 (53–84) | 64 (57–80) | 71 (53–81) | 71 (53–84) |
| Race, n (%) | ||||
| Caucasian/White | 46 (85.2) | 4 (80.0) | 12 (92.3) | 30 (83.3) |
| Black | 7 (13.0) | 1 (20.0) | 1 (7.7) | 5 (13.9) |
| Asian | 1 (1.9) | 0 | 0 | 1 (2.8) |
| ECOG PS, n (%) | ||||
| 0 | 20 (37.0) | 3 (60.0) | 7 (53.8) | 10 (27.8) |
| 1 | 32 (59.3) | 2 (40.0) | 6 (46.2) | 24 (66.7) |
| 2 | 2 (3.7) | 0 | 0 | 2 (5.6) |
| Gleason Score at diagnosis, n (%) | ||||
| ≤ 6 | 7 (13.7) | 1 (25.0) | 3 (23.1) | 3 (8.8) |
| 7 | 13 (25.5) | 1 (25.0) | 3 (23.1) | 9 (26.5) |
| 8─10 | 31 (60.8) | 2 (50.0) | 7 (53.8) | 22 (64.7) |
| Prior prostatectomy, n (%) | 24 (44.4) | 2 (40.0) | 6 (46.2) | 16 (44.4) |
| Prior new-generation AR-targeted therapy, n (%) | 23 (42.6) | 1 (20.0) | 5 (38.5) | 17 (47.2) |
| Median PSA, ng/mL (range) | 92.1 (2.4–1558.0) |
20.8 (3.9–832.1) |
89.0 (19.3–713.8) |
113.1 (2.4–1558.0) |
| Albumin, g/dL (SD) | 39.0 (4.874) | 40.8 (2.388) | 39.2 (4.604) | 38.7 (5.242) |
| Hemoglobin, g/dL (SD) | 12.24 (1.409) | 13.16 (1.336) | 12.23 (1.266) | 12.12 (1.465) |
| Alkaline phosphatase, U/L (SD) | 217.8 (260.35) | 78.6 (23.33) | 232 (287.8) | 218.5 (266.13) |
| LDH > ULN, n (%) | 17 (32.7) | 0 | 6 (46.2) | 11 (32.4) |
| Metastases, n (%) | ||||
| Bone | 49 (90.7) | 5 (100.0) | 6 (46.2) | 34 (94.4) |
| Lymph nodes | 28 (51.9) | 3 (60.0) | 10 (76.9) | 14 (38.9) |
| Visceral | 22 (40.7) | 3 (60.0) | 5 (38.5) | 14 (38.9) |
| Other | 11 (20.4) | 0 | 2 (15.4) | 9 (25.0) |
AR, androgen receptor; ECOG PS, Eastern Cooperative Oncology Group performance status; LDH, lactate dehydrogenase; PSA, prostate-specific antigen; SD, standard deviation; ULN, upper limit of normal.
Androgen receptor splice variant expression
Among the 54 patients, 67% (36 patients) and 78% (42 patients) were AR-V7+ and ARv567es+ by ddPCR at baseline, respectively. Forty-nine (91%) were positive for either or both splice variants, and only five (9%) were double negative (Supplementary Figure 3). ddPCR splice variant expression appeared to be numerically more frequent in those patients who had received prior AR-targeted agents. Prior AR-targeted agents had been given in 33% vs 45% of patients who were ARv567es- vs ARv567es+, and 33% vs 47% of patients who were AR-V7- vs AR-V7+. Baseline characteristics by splice variant expression are shown in Table 1. Of note, patients with either splice variant had a numerically higher median PSA level, and ARv567es+ patients had a numerically higher frequency of visceral metastases (Table 1).
Correlation between AR-V mRNA expression and AR protein nuclear localization
Our first report of TAXYNERGY, revealed a significant correlation between PSA response rate to taxane chemotherapy and change in CTC AR nuclear localization (%ARNL). Patients with biochemical response to taxanes had a significant decrease in %ARNL at C1D8 compared with C1D1 (baseline) (14). As the ARNL immunofluorescence assay does not differentiate between AR-FL or AR-V, we sought to correlate AR-V mRNA expression at baseline with change in %ARNL (C1D8-C1D1). Twenty-four of the 54 patients had %ARNL data at both C1D1 and C1D8 (Table 2 and 3; Figure 2). As many of the samples co-expressed both variants, to determine the relative impact of each we initially categorized the samples into four groups (double positive, double negative, AR-V7+/ARv567es-, and AR-V7-/ARV567es+). Of these 24 patients, 13 were double positive, three were double negative, three were AR-V7+/ARv567es- and five were AR-V7-/ARv567es+. Patients who were AR-V7+/ARv567es- had a 1.9% decrease in %ARNL, compared with a 26.7% decrease in patients who were AR-V7-/ARv567es + (not shown). Furthermore, double-positive patients had a change of 0% (not shown). These data taken together, suggest a dominant role for AR-V7 in driving taxane resistance. Due to the small number of patients in each group and since the presence of AR-V7 seemed to have a dominant effect over ARv567es, results are presented in three groups: AR-V7+ (regardless of ARv567es status), ARv567es+/AR-V7-, and double negative (Figure 2, Table 3). Patients who were double negative had a 12.9% decrease in %ARNL compared with a 26.7% decrease in patients who were AR-V7-/ARv567es+ compared with a negligible 0.4% decrease in patients who were AR-V7+ (p = 0.08 for trend) (Table 3). Comparison of the change in %ARNL between AR-V7+ vs AR-V7- patients, regardless of ARv567es expression, revealed a 21.5% decrease in %ARNL in AR-V7- patients vs a 0.4% decrease in AR-V7+ patients (p=0.0023) (Table 2).
Table 2.
PSA outcomes and %ARNL according to AR-V7 and ARv567es expression
| AR-V7+n = 36 | AR-V7- n = 18 |
|
|---|---|---|
| PSA50 at C5D1, n (%) | 13 (36) | 11 (61) |
| p-value | 0.09 | |
| PSA50 at any time, n (%) | 21 (58) | 14 (78) |
| p-value | 0.23 | |
| n = 16 | n = 8 | |
| C1D1 %ARNL, mean (SD) | 62.5 (14.3) | 63. (14.6) |
| C1D8 %ARNL, mean (SD) | 62.2 (15.2) | 42.1 (11.1) |
| C1D8 – C1D1 %ARNL, mean (SD) | −0.4 (13.2) | −21.5 (22.1) |
| p-value | 0.0023 | |
| ARv567es+ n = 42 |
ARv567es- n = 12 |
|
| PSA50 at C5D1, n (%) | 16 (38) | 8 (67) |
| p-value vs Group 1 | 0.11 | |
| PSA50 at any time, n (%) | 24 (57) | 11 (92) |
| p-value | 0.04 | |
| n = 18 | n = 6 | |
| C1D1 %ARNL, mean (SD) | 63.7 (16.8) | 62.6 (13.6) |
| C1D8 %ARNL, mean (SD) | 56.3 (17.4) | 55.2 (17.0) |
| C1D8 – C1D1 %ARNL, mean (SD) | −7.4 (11.8) | −7.4 (21.3) |
| p-value | 0.9985 | |
AR, androgen receptor; ARNL, androgen receptor nuclear localization; C1D1, Cycle 1 Day 1; C1D8, Cycle 1 Day 8; C5D1, Cycle 5 Day 1; PSA50, 50% reduction from baseline in prostate-specific antigen; SD, standard deviation.
Table 3.
PSA outcomes and %ARNL in AR-V7+ patients and AR-V7- patients with or without ARv567es expression
| Group 1 | Group 2 | Group 3 | ||
|
AR-V7-/
and ARv567es- n = 5 |
AR-V7-/ ARv567es+n = 13 |
All AR-V7+n = 36 |
Total n = 54 |
|
| PSA50 at C5D1, n (%) | 4 (80.0%) | 7 (53.9) | 13 (36.1) | 24 (44.4) |
| p-value vs Group 1 | 0.31 | 0.26 | ||
| p-value vs Group 2 | 0.06 | |||
| Trend Group 1 > Group 2 > Group 3 | 0.1748 | |||
| PSA50 at any time, n (%) | 5 (100.0) | 9 (69.2) | 21 (58.3) | 35 (64.8) |
| p-value vs Group 1 | 0.16 | 0.49 | ||
| p-value vs Group 2 | 0.07 | |||
| Trend Group 1 > Group 2 > Group 3 | 0.33 | |||
| GROUP 1 | GROUP 2 | GROUP 3 | ||
|
AR-V7-/
and ARv567es- n = 3 |
AR-V7-/ ARv567es+n = 5 |
All AR-V7+ n = 16 |
Total n = 24 |
|
| C1D1 %ARNL, mean (SD) | 56.9 (19.2) | 67.6 (11.6) | 62.5 (14.3) | 62.9 (14.1) |
| C1D8 %ARNL, mean (SD) | 44.1 (4.8) | 41.0 (14.1) | 62.2 (15.2) | 55.5 (16.8) |
| C1D8 – C1D1 %ARNL, mean (SD) | −12.9 (15.4) | −26.7 (25.4) | −0.4 (13.2) | −7.4 (19.1) |
| p-value vs Group 1 | 0.52 | 0.08 | ||
| p-value vs Group 2 | 0.52 | |||
| Trend Group 1 > Group 2 > Group 3 | 0.08 | |||
AR, androgen receptor; ARNL, androgen receptor nuclear localization; C1D1, Cycle 1 Day 1; C1D8, Cycle 1 Day 8; C5D1, Cycle 5 Day 1; PSA50, 50% reduction from baseline in prostate-specific antigen; SD, standard deviation.
Figure 2. Waterfall plot of percentage change in AR nuclear localization at C1D8 compared with C1D1 in patients stratified by AR-V status.

Dotted line represents the mean change in %ARNL for all patients.AR, androgen receptor; SD, standard deviation
Efficacy outcomes
Splice variant expression and PSA outcomes are presented in Table 2 and Table 3. PSA50 response at C5D1 was observed in 61.1% of AR-V7- patients vs 36.1% of AR-V7+ patients (p = 0.09) (Table 2). Similar trends were observed for PSA50 response at any time during the study, which was recorded in 77.8% of AR-V7- patients vs 58.3% of AR-V7+ patients (p = 0.23).
PSA50 responses at C5D1 were observed in 38% of ARv567es+ patients (regardless of AR-V7 status) vs 67% of ARv567es- patients (p=0.11). For PSA50 at any time (Table 2), responses were observed in 57% of ARv567es+ patients vs 92% of ARv567es- patients (p=0.04). However, when patients were divided into three subgroups, in order to model a dominant role of AR-V7, 80% of AR-V7-/ ARv567es- patients had a >50% PSA decline by Cycle 5 vs 53.9% in AR-V7-/ ARv567es+ patients (p=0.31) (Table 3). In double negative patients, all patients had a >50% PSA decline at any time on study vs 69.2% of AR-V7-/ ARv567es+ patients (p = 0.16) (Table 3). Median AR-V7 and ARv567es copy numbers at baseline were numerically lower in PSA responders than in PSA non-responders; however, the difference was not statistically significant, and overall variability was very high (Supplementary Table 3).
Median PFS was 16.6 months for double negative patients compared with 11.2 months for AR-V7-/ ARv567es+ (p = 0.18), and 8.5 months for AR-V7+ patients (p = 0.004). (Figure 3). For the AR-V7- vs AR-V7+ comparison, median PFS was 12.0 vs 8.5 months (hazard ratio = 0.38, p = 0.01). The p-value for the trend across AR-V7-/ ARv567es-, AR-V7-/ ARv567es+ and AR-V7+ was 0.0013. For the ARv567es vs ARv567es+ comparison, median PFS was 12.7 vs 7.3 months (hazard ratio = 0.37, p = 0.02) (Figure 3).
Figure 3. Kaplan–Meier curve of progression-free survival for A) AR-V7- vs AR-V7+; B) ARv567es- vs ARv567es+ and C) AR-V7-/ARv567es- vs AR-V7-/ARv567es+ vs all AR-V7+.
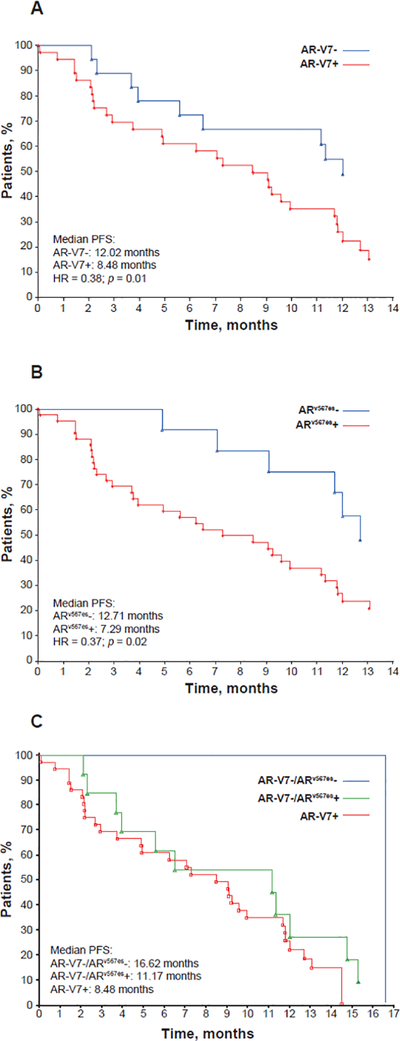
A) For AR-V7- (regardless of ARv567es status) vs AR-V7+, p = 0.01; B) for ARv567es- (regardless of AR-V7 status) vs ARv567es+, p = 0.02; C) for AR-V7-/ARv567es- vs AR-V7-/ARv567es+, p = 0.18; for AR-V7-/ARv567es- vs AR-V7+, p = 0.004; for AR-V7-/ARv567es+ vs AR-V7+, p = 0.32. The trend for AR-V7-/ ARv567es-, AR-V7-/ ARv567es+ and AR-V7+ was 0.0013.
AR, androgen receptor.
Discussion and conclusions
In light of the high frequency of intrinsic and acquired resistance to treatment observed in mCRPC, and the increasing number of treatment options, future standards of care could be shaped by prognostic and/or predictive biomarkers. In this context, AR splice variants are appealing, as most tumors retain their dependence on AR signaling even after acquiring a castration-resistant phenotype (33).
In this study, we used CTC isolation and a specific ddPCR assay for the detection of AR-FL, AR-V7 and ARv567es expression. AR splice variant positivity by ddPCR appeared to be more frequent than in prior studies using CTCs to detect AR-V7 expression by RT-qPCR, which reported AR-V7 positivity in 19–55% of samples (6, 18, 21, 34, 35). On the other hand, when ddPCR was used to quantify AR-V7 expression in CRPC patient-derived CTCs or whole blood, AR-V7 positivity was reported in 50–95% of patients (10, 31, 36).
Taken together, these data support the observation that ddPCR has increased sensitivity in detecting low template transcript copies (37–39), and are consistent with our own results, showing that AR-V7 was present in 67% of evaluable patients with mCRPC at baseline, ARv567es in 78% and AR-FL in 93%. Regarding quantitation of ARv567es mRNA expression in patient samples, there is only one study that employs RT-qPCR to detect ARv567es in whole blood and reports ARv567es positivity in 32% of CRPC patients (40).
Taxanes stabilize microtubules, which in prostate cancer impairs trafficking of the AR into the nucleus (41, 42). The prospective TAXYNERGY study was the first to associate clinical outcome with taxane treatment and AR nuclear localization in patient CTCs (14). Mechanistically, we showed that AR-FL binds microtubules via its C-terminus hinge domain, which is retained in ARv567es but absent in AR-V7 (12) (Figure 1).
Because taxane treatment inhibits microtubule dynamics, it has been shown to differentially affect the nuclear localization of AR splice variants in preclinical models (12). Indeed, our results show that AR-V7- patients have a greater reduction in AR percent nuclear localization compared with AR-V7+ patients (Table 2 and Figure 2). AR-FL is kept inactive in the cytoplasm, whereas the nuclear localization of AR-V7 is not affected; accordingly, tumors with AR-V7 would be predicted to be less sensitive to taxanes. The hinge domain that is retained in ARv567es is the minimum functional domain required for microtubule binding, albeit it does not bind as extensively as the entire C-terminus of AR. In line with this, taxane treatment has been shown to partially impair the nuclear localization of ARv567es in vitro (12) (Figure 1), and ARv567es expression would be expected to confer intermediate taxane sensitivity in vivo. Although one study reported that both AR-V7 and ARv567es bind poorly to microtubules (20), their expression was associated with a role for both variants in sensitivity to taxane treatment, which is consistent with our data presented here.
In the 9% of patients in our study with undetectable levels of either splice variant, but with AR-FL expression, we observed exceptionally high response rates of 80–100%. Still, the presence of either splice variant was associated with relatively high rates of PSA decline; PSA50 response rates at any time were 58% (AR-V7) and 57% (ARv567es), similar to the overall high PSA responses in the TAXYNERGY study as a whole. This may reflect the additional AR-independent mechanisms of action that taxanes are thought to have combined with a shift towards earlier therapy for mCRPC and the fact that more than half of the patients in this study were not previously exposed to abiraterone or enzalutamide (13).
In this study, we attempted to ascertain the association of treatment outcomes (PSA response and PFS) with expression of ARv567es and AR-V7 by ddPCR at baseline. The difference in response rates and PFS between AR-V7+ and AR-V7- patients observed in the present study is similar to that in a previous study (18), in which patients had received a median of 4 (range 2–7) prior AR-targeted therapies and had a 46% frequency (17 of 37 patients) of AR-V7 by RT-PCR. Those AR-V7+ patients had a PSA50 response rate of 41%, compared with 65% in AR-V7- patients, but the sample size was small. It was concluded that AR-V7 presence by RT-PCR was not associated with primary taxane resistance although outcomes were numerically better in patients who were AR-V7- compared with those who were AR-V7+ (18). The negative prognostic value of AR-V7 positivity was further supported by another study using a CTC-based nuclear-specific protein immunofluorescence assay, which demonstrated worse overall survival associated with taxane therapy in AR-V7+ versus AR-V7- patients (HR [95% CI]: 3.1 [1.4–7.0]; p<0.001) (43). Another study investigated treatment of 79 patients with progressive mCRPC using cabazitaxel (after prior docetaxel); 29 patients were evaluable with at least 10 CTCs in 7.5 mL blood at baseline (assessed by CellSearch). Although not the primary endpoint, AR-V7 status by RTqPCR was also assessed. The PSA50 response rate was 28.6% for AR-V7- patients and 8.3% for AR-V7+ patients (p = NS). PFS was also numerically longer for AR-V7- patients (6 months) compared with AR-V7+ patients (4 months). These authors concluded that cabazitaxel efficacy in the post-docetaxel setting was independent of AR-V7 expression by RTqPCR (21). Our data also support mechanistic results, as AR-V7+ patients had a lower decrease in AR nuclear localization after taxane therapy than AR-V7- patients (Table 3). Taken together, though the three clinical studies are individually underpowered to detect a more moderate effect of AR-V7 on taxane sensitivity, all studies provide trends supporting the hypothesis that the presence of AR-V7 may confer modest taxane resistance, albeit significantly less than that on AR signaling or CYP17 inhibitors.
In our initial studies, we utilized LuCaP 86.2, a human xenograft tumor in which ARv567es is the predominant splice variant, and LuCaP 23.1, a human xenograft expressing both wildtype AR and AR-V7 (12). We previously showed that docetaxel treatment inhibits tumor growth and nuclear localization of AR in LuCaP86.2 tumors, but had minimal effect on LuCaP 23.1 tumors, suggesting that the ARv567es splice variant conferred relatively greater taxane sensitivity than AR-V7 (12). Although our clinical results with AR-V7 are consistent with our a priori hypothesis and with previously published data, our results with ARv567es are different likely due to the fact that the xenograft model is completely dependent on ARv567es expression and transcriptional activity for growth. Thus, even an intermediate effect on this variant’s nuclear localization by taxane treatment would result in an amplified drug sensitivity phenotype. In addition, our earlier data showed that the entire C-terminus region of AR (including the hinge domain; see Figure 1) mediates maximum association with microtubules in vitro, whereas the hinge domain when expressed alone is partially associated with microtubule polymers, suggesting that a larger AR structural region is required for maximum binding. In this context, we would hypothesize that AR-FL would be the most sensitive to taxane treatment, followed by ARv567es and AR-V7; our clinical results provide evidence in support of this hypothesis.
Of note, this is one of the first reports describing ARv567es expression in patient-derived CTCs, and the association of the expression levels with patient outcomes in mCRPC. The presence of the ARv567es amplicon was confirmed in patient-derived CTCs by direct Sanger sequencing (Supplementary Figure 4). These analyses were exploratory and involved low patient numbers; consequently, most of the differences found were numerical and did not reach statistical significance. Therefore, we cannot conclude that AR variants have definitive prognostic or taxane predictive characteristics. Future studies should involve larger patient numbers and take into account simultaneous presence and relative expression levels of all AR splice variants.
In summary, we examined outcomes of patients with mCRPC enrolled in the TAXYNERGY study according to their expression of AR splice variants by ddPCR. PSA response rates were numerically superior in double negative patients vs ARv567es+/AR-V7- patients vs AR-V7+ patients at baseline. PFS was longest in double negative patients who did not express either splice variant. PFS was longer with taxane therapy in AR-V7- patients compared with AR-V7+ patients. Absence of AR splice variants by ddPCR appears to be associated with superior response and PFS to cabazitaxel or docetaxel in patients with mCRPC.
Supplementary Material
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Acknowledgments
This study was sponsored by Sanofi; editorial support was provided by Amber Wood and Olga Ucar of MediTech Media, funded by Sanofi.
Footnotes
Disclosures of Conflicts of Interest
Scott T. Tagawa received research funding and consultancy fees from Sanofi. Emmanuel S. Antonarakis is a paid consultant/advisor to Janssen, Astellas, Sanofi, Dendreon, Medivation, ESSA, AstraZeneca, Clovis, and Merck; received research funding to his institution from Janssen, Johnson & Johnson, Sanofi, Dendreon, Genentech, Novartis, Tokai, Bristol Myers-Squibb, AstraZeneca, Clovis, and Merck; and is the co-inventor of a biomarker technology that has been licensed to Qiagen. John Stewart, Atef Zaher and Ted P. Szatrowski are employees of Sanofi. Brian J Kirby received research funding from Sanofi. Fred Saad received research funding from Sanofi, Janssen, Astellas and Bayer, and consultancy fees from Janssen, Astellas and Bayer. Seaho Kim received support from the National Cancer Institute (NCI)-funded NIH T32 postdoctoral training grant (T32 CA203702) on Molecular and Translational Oncology Research. Giuseppe Galletti received support from the NCI Grant NIH T32 CA062948 and by the National Center for Advancing Translational Sciences of the NIH under Award Number grant UL1TR002384. Paraskevi Giannakakou received research funding from Sanofi and research support from the NCI R21 CA216800. The content is solely responsible of the authors and does not necessarily represent the official views of the National Institutes of Health. Ada Gjyrezi and Paraskevi Giannakakou have a pending patent application for the AR-V7 and ARv567es ddPCR assays. Daniel Worroll, Karla V. Ballman, Katsuhiro Kita, Shinsuke Tasaki, Yang Bai, Luigi Portella, Mario A. Eisenberger and David M. Nanus have nothing to disclose.
References
- 1.Hu R, Dunn TA, Wei S, Isharwal S, Veltri RW, Humphreys E, et al. Ligand-independent androgen receptor variants derived from splicing of cryptic exons signify hormone-refractory prostate cancer. Cancer Res 2009;69(1):16–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Dehm SM, Schmidt LJ, Heemers HV, Vessella RL, Tindall DJ. Splicing of a novel androgen receptor exon generates a constitutively active androgen receptor that mediates prostate cancer therapy resistance. Cancer Res 2008;68(13):5469–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Qu Y, Dai B, Ye D, Kong Y, Chang K, Jia Z, et al. Constitutively active AR-V7 plays an essential role in the development and progression of castration-resistant prostate cancer. Sci Rep 2015;5:7654. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Caffo O, Maines F, Veccia A, Kinspergher S, Galligioni E. Splice variants of androgen receptor and prostate cancer. Oncol Rev 2016;10(1):297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.National Comprehensive Cancer Network I. NCCN clinical practice guidelines in oncology (NCCN guidelines) prostate cancer version 2.2018. 2018. [DOI] [PMC free article] [PubMed]
- 6.Antonarakis ES, Lu C, Wang H, Luber B, Nakazawa M, Roeser JC, et al. AR-V7 and resistance to enzalutamide and abiraterone in prostate cancer. N Engl J Med 2014;371(11):1028–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Conteduca V, Wetterskog D, Sharabiani MTA, Grande E, Fernandez-Perez MP, Jayaram A, et al. Androgen receptor gene status in plasma DNA associates with worse outcome on enzalutamide or abiraterone for castration-resistant prostate cancer: A multi-institution correlative biomarker study. Ann Oncol 2017;28(7):1508–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Shore N, Heidenreich A, Saad F. Predicting response and recognizing resistance: Improving outcomes in patients with castration-resistant prostate cancer. Urology 2017. [DOI] [PubMed] [Google Scholar]
- 9.Antonarakis ES, Lu C, Luber B, Wang H, Chen Y, Zhu Y, et al. Clinical significance of androgen receptor splice variant-7 mRNA detection in circulating tumor cells of men with metastatic castration-resistant prostate cancer treated with first- and second-line abiraterone and enzalutamide. J Clin Oncol 2017;35(19):2149–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Qu F, Xie W, Nakabayashi M, Zhang H, Jeong SH, Wang X, et al. Association of AR-V7 and prostate-specific antigen RNA levels in blood with efficacy of abiraterone acetate and enzalutamide treatment in men with prostate cancer. Clin Cancer Res 2017;23(3):726–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Maughan BL, Xhou XC, Suzman DL, Nadal R, Bassi S, Schweizer MT, et al. Optimal sequencing of docetaxel and abiraterone in men with metastatic castration-resistant prostate cancer. Prostate 2015;75(15):1814–20. [DOI] [PubMed] [Google Scholar]
- 12.Thadani-Mulero M, Portella L, Sun S, Sung M, Matov A, Vessella RL, et al. Androgen receptor splice variants determine taxane sensitivity in prostate cancer. Cancer Res 2014;74(8):2270–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Darshan MS, Loftus MS, Thadani-Mulero M, Levy BP, Escuin D, Zhou XK, et al. Taxane-induced blockade to nuclear accumulation of the androgen receptor predicts clinical responses in metastatic prostate cancer. Cancer Res 2011;71(18):6019–29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Antonarakis ES, Tagawa ST, Galletti G, Worroll D, Ballman K, Vanhuyse M, et al. Randomized, noncomparative, phase II trial of early switch from docetaxel to cabazitaxel or vice versa, with integrated biomarker analysis, in men with chemotherapy-naive, metastatic, castration-resistant prostate cancer. J Clin Oncol 2017;35(28):3181–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Robinson D, Van Allen EM, Wu YM, Schultz N, Lonigro RJ, Mosquera JM, et al. Integrative clinical genomics of advanced prostate cancer. Cell 2015;161(5):1215–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hornberg E, Ylitalo EB, Crnalic S, Antti H, Stattin P, Widmark A, et al. Expression of androgen receptor splice variants in prostate cancer bone metastases is associated with castration-resistance and short survival. PLoS One 2011;6(4):e19059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Antonarakis ES, Nakazawa M, Luo J. Resistance to androgen-pathway drugs in prostate cancer. N Engl J Med 2014;371(23):2234. [DOI] [PubMed] [Google Scholar]
- 18.Antonarakis ES, Lu C, Luber B, Wang H, Chen Y, Nakazawa M, et al. Androgen receptor splice variant 7 and efficacy of taxane chemotherapy in patients with metastatic castration-resistant prostate cancer. JAMA Oncol 2015;1(5):582–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Scher HI, Lu D, Schreiber NA, Louw J, Graf RP, Vargas HA, et al. Association of AR-V7 on circulating tumor cells as a treatment-specific biomarker with outcomes and survival in castration-resistant prostate cancer. JAMA Oncol 2016;2(11):1441–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Zhang G, Liu X, Li J, Ledet E, Alvarez X, Qi Y, et al. Androgen receptor splice variants circumvent AR blockade by microtubule-targeting agents. Oncotarget 2015;6(27):23358–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Onstenk W, Sieuwerts AM, Kraan J, Van M, Nieuweboer AJ, Mathijssen RH, et al. Efficacy of cabazitaxel in castration-resistant prostate cancer is independent of the presence of AR-V7 in circulating tumor cells. Eur Urol 2015;68(6):939–45. [DOI] [PubMed] [Google Scholar]
- 22.Kohli M, Ho Y, Hillman DW, Van Etten JL, Henzler C, Yang R, et al. Androgen receptor variant AR-V9 is coexpressed with AR-V7 in prostate cancer metastases and predicts abiraterone resistance. Clin Cancer Res 2017;23(16):4704–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kirby BJ, Jodari M, Loftus MS, Gakhar G, Pratt ED, Chanel-Vos C, et al. Functional characterization of circulating tumor cells with a prostate-cancer-specific microfluidic device. PLoS One 2012;7(4):e35976. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Galletti G, Matov A, Beltran H, Fontugne J, Miguel MJ, Cheung C, et al. ERG induces taxane resistance in castration-resistant prostate cancer. Nat Commun 2014;5:5548. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Vogelstein B, Kinzler KW. Digital PCR. Proc Natl Acad Sci U S A 1999;96(16):9236–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Pinheiro LB, Coleman VA, Hindson CM, Herrmann J, Hindson BJ, Bhat S, et al. Evaluation of a droplet digital polymerase chain reaction format for DNA copy number quantification. Anal Chem 2012;84(2):1003–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Zhao H, Wilkins K, Damon IK, Li Y. Specific qPCR assays for the detection of orf virus, pseudocowpox virus and bovine papular stomatitis virus. J Virol Methods 2013;194(1–2):229–34. [DOI] [PubMed] [Google Scholar]
- 28.Doi H, Takahara T, Minamoto T, Matsuhashi S, Uchii K, Yamanaka H. Droplet digital polymerase chain reaction (PCR) outperforms real-time PCR in the detection of environmental DNA from an invasive fish species. Environ Sci Technol 2015;49(9):5601–8. [DOI] [PubMed] [Google Scholar]
- 29.Huggett JF, Taylor MS, Kocjan G, Evans HE, Morris-Jones S, Gant V, et al. Development and evaluation of a real-time PCR assay for detection of pneumocystis jirovecii DNA in bronchoalveolar lavage fluid of HIV-infected patients. Thorax 2008;63(2):154–9. [DOI] [PubMed] [Google Scholar]
- 30.Racki N, Dreo T, Gutierrez-Aguirre I, Blejec A, Ravnikar M. Reverse transcriptase droplet digital PCR shows high resilience to PCR inhibitors from plant, soil and water samples. Plant Methods 2014;10(1):42,014-0042-6. eCollection 2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Ma Y, Luk A, Young FP, Lynch D, Chua W, Balakrishnar B, et al. Droplet digital PCR based androgen receptor variant 7 (AR-V7) detection from prostate cancer patient blood biopsies. Int J Mol Sci 2016;17(8): 10.3390/ijms17081264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Seitz AK, Thoene S, Bietenbeck A, Nawroth R, Tauber R, Thalgott M, et al. AR-V7 in peripheral whole blood of patients with castration-resistant prostate cancer: Association with treatment-specific outcome under abiraterone and enzalutamide. Eur Urol 2017;72:828–834. [DOI] [PubMed] [Google Scholar]
- 33.Galletti G, Leach BI, Lam L, Tagawa ST. Mechanisms of resistance to systemic therapy in metastatic castration-resistant prostate cancer. Cancer Treat Rev 2017;57:16–27. [DOI] [PubMed] [Google Scholar]
- 34.Steinestel J, Luedeke M, Arndt A, Schnoeller TJ, Lennerz JK, Wurm C, et al. Detecting predictive androgen receptor modifications in circulating prostate cancer cells. Oncotarget 2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Lokhandwala PM, Riel SL, Haley L, Lu C, Chen Y, Silberstein J, et al. Analytical validation of androgen receptor splice variant 7 detection in a clinical laboratory improvement amendments (CLIA) laboratory setting. J Mol Diagn 2017;19(1):115–25. [DOI] [PubMed] [Google Scholar]
- 36.Miyamoto DT, Lee RJ, Kalinich M, LiCausi J, Zheng Y, Chen T, et al. An RNA-based digital circulating tumor cell signature is predictive of drug response and early dissemination in prostate cancer. Cancer Discov 2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Brunetto GS, Massoud R, Leibovitch EC, Caruso B, Johnson K, Ohayon J, et al. Digital droplet PCR (ddPCR) for the precise quantification of human T-lymphotropic virus 1 proviral loads in peripheral blood and cerebrospinal fluid of HAM/TSP patients and identification of viral mutations. J Neurovirol 2014;20(4):341–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Sanders R, Mason DJ, Foy CA, Huggett JF. Considerations for accurate gene expression measurement by reverse transcription quantitative PCR when analysing clinical samples. Anal Bioanal Chem 2014;406(26):6471–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Sanders R, Mason DJ, Foy CA, Huggett JF. Evaluation of digital PCR for absolute RNA quantification. PLoS One 2013;8(9):e75296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Liu X, Ledet E, Li D, Dotiwala A, Steinberger A, Feibus A, et al. A whole blood assay for AR-V7 and AR(v567es) in patients with prostate cancer. J Urol 2016;196(6):1758–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Thadani-Mulero M, Nanus DM, Giannakakou P. Androgen receptor on the move: Boarding the microtubule expressway to the nucleus. Cancer Res 2012;72(18):4611–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Zhu ML, Horbinski CM, Garzotto M, Qian DZ, Beer TM, Kyprianou N. Tubulin-targeting chemotherapy impairs androgen receptor activity in prostate cancer. Cancer Res 2010;70(20):7992–8002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Scher HI, Graf RP, Schreiber NA, McLaughlin B, Lu D, Louw J, et al. Nuclear-specific AR-V7 protein localization is necessary to guide treatment selection in metastatic castration-resistant prostate cancer. Eur Urol 2017;71(6):874–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.