

Abstract
Introduction
This observational study investigated the incidence of distal radius fractures in children, to determine whether the rate is rising, the effect of seasonal variation on incidence and whether fracture type and rate of surgical intervention has changed, to help in determining costs for secondary care and to aid resource allocation.
Materials and methods
All paediatric patients(n = 6529) who sustained a distal radius fracture over an eight-year period (2007–2014) were identified. Poisson regression modelling was used to identify change in trends.
Results
There was no change in distal radius fracture incidence, rate of surgical intervention (P = 0.36) or fracture type (P = 0.70). Overall incidence was 337 fractures per 100,000 patient/years. The highest fracture incidence was seen in older school boys (708 per 100,000 patient/years, P < 0.005). Overall fracture rate was lower in winter (P < 0.005). Incidence is highest in summer and the main variation is related to season.
Discussion
These data can help to predict accurately the number of children presenting to the emergency department with wrist fractures depending on the time of year.
Keywords: Paediatric, Fracture, Wrist fracture, Distal radius fracture, Epidemiology
Introduction
Childhood fractures are common and are a significant healthcare burden. Around 20–30% of children in the UK will attend accident and emergency each year with an injury.1,2 Some 9% of these injuries will be children with fractures.3,4 Wrist fractures are the most common childhood fracture, with up to 25% of fractures affecting the distal radius.5,6
Despite the magnitude of the problem there is minimal evidence in the literature regarding the incidence and epidemiology of these fractures in the UK. Most studies do not determine accurate incidence rates for the at-risk paediatric population. Evidence from Scandinavia, Europe, Japan and the United States has suggested that the incidence of distal radius fracture in children is increasing,5,7–10 with some studies also reporting an increase in the rate of surgical intervention.11,12
An understanding of fracture epidemiology is vitally important to assist in determining expected costs secondary to injury and allocation of healthcare resources. Our aim was to calculate accurate age and gender specific incidence rates for children sustaining a distal radius fracture in our region and determine whether the incidence is increasing across our eight-year study period. Trends in surgical intervention were also investigated. We attempted to establish whether there was any annual, seasonal or weekly trend in fracture incidence and review data of the location where fractures are sustained to permit understanding of where preventative strategies may be beneficial.
Materials and methods
Leicester General Hospital provides care to a population of approximately one million people living in the city and the surrounding counties. All children sustaining an orthopaedic injury within these areas are referred for review and follow up at this centre, allowing comprehensive capture of all such presentations within the resident population.
Details of all children presenting to the unit with a radiographically confirmed fracture of the distal radius (AO classification 23-M, 23r-M, 23u-M, 23-E, 23-rE) between 1 January 2007 and 31 December 2014 were recorded in an established hospital database.13 Data on age, gender, anatomical site of injury and the location and date of the injury were collected. Data were recorded for all patients on initial presentation to the accident and emergency department so included those discharged straight from the department or who did not attend subsequent follow-up in the region. There are four minor injury units in the region which refer children with fractures to our unit. They are initially seen in the accident and emergency department so would also be captured in the database. The population at risk was identified by obtaining the annual gender and age specific population data for Leicester for 2007–14, inclusive, from the UK National Office for Statistics. The total population at risk was calculated by the addition of the numbers for the three regions.
The patients were grouped according to their age into toddlers (0–2 years), preschool (2–5 years), younger school children (5–10 years) and older schoolchildren (10–16 years). Location of fracture, when recorded, was reported as occurring at home, at school, in the street, in a public place, in the workplace, during sporting activity, following road traffic collision or other location. Location data were available for 84% of fractures. As these data were incomplete, percentage of injury per location was calculated for comparison rather than incidence rate.
Investigation of trends was performed in three ways:
Comparison between 2007 and 2014 – 100 patients were randomly identified from 2007, the first year in the time period studied. They were compared with another 100 patients from the last year studied, 2014. Age, gender, rate of surgical intervention and type of surgery were recorded. Radiographs were reviewed to identify the anatomical location of the fracture.
Biennial sampling – equal numbers of male and female children were randomly selected from two-year samples (2007/08, 2009/10, 2011/12, 2013/14) according to age group stratification. The number of children was chosen to sample approximately 10% of each gender per age group: 20 toddlers (10 boys, 10 girls), 20 preschool children (10 boys, 10 girls), 40 young school children (20 boys, 20 girls) and 60 older school children (30 boys, 30 girls). Fracture type, treatment and surgical procedure, if required, were recorded.
Total sample – the full data set was analysed for trends in age, location of injury, incidence per season, year and day of week.
Radiographical analysis was carried out by two observers, a junior orthopaedic trainee and a senior orthopaedic specialty registrar. Patients for sampling were identified randomly using a computer program by an independent observer.
Poisson regression modelling techniques were used to investigate variation in overall trends. A model was constructed assessing variables against fracture incidence rate, with an offset of the log of the population. This gives individual P-values for each data item to demonstrate any significant variation from expected along with magnitude and direction of the change. The Kruskal–Wallis test was used to compare non-parametric data and the Chi square test to compare categorical data.
Results
During the study period the accident and emergency department saw 6529 children aged 16 years or under with a distal radius fracture. Overall incidence rate across the eight-year study period was 337/100,000 children per year. The male to female ratio was 64% : 36% (4012 : 2517; Table 1).
Table 1.
Total number of children per age group and gender presenting to the emergency department with a distal radius fracture across the study period.
| Age group | Sex | Year | ||||
| 2007/08 | 2009/10 | 2011/12 | 2013/14 | Patients (n) | ||
| Toddler | Male | 30 | 25 | 34 | 26 | 115 |
| Female | 38 | 34 | 30 | 28 | 130 | |
| Preschool | Male | 66 | 67 | 78 | 77 | 288 |
| Female | 86 | 75 | 92 | 83 | 336 | |
| Younger school age | Male | 238 | 267 | 307 | 292 | 1104 |
| Female | 236 | 255 | 282 | 288 | 1061 | |
| Older school age | Male | 648 | 649 | 604 | 604 | 2505 |
| Female | 250 | 256 | 253 | 231 | 990 | |
| Totals | 1592 | 1628 | 1680 | 1629 | 6529 | |
Toddlers accounted for 3.8% (245/6529) of the study group. Incidence rate was 82/100,000 children per year. The incidence rate ratio (IRR) comparing girl toddlers with boys was not significant (IRR 1.18, 95% confidence interval, CI, 0.92–1.52). Of the children in the study, 9.6% (624/6529) were of preschool age. The incidence rate for this group was 160/100,000 children per year. Incidence was significantly higher for preschool boys (n = 176 boys, n = 144 girls, IRR 1.23, 95% CI 1.05–1.44). Younger school-aged children accounted for 33.2% (2165/6529) of cases. The incidence rate was 384/100,000 per year. There was no difference in incidence rates between boys and girls (boys 381, girls 387, IRR 1.01, 95% CI 0.933–1.104). Older school children made up 53.5% (3495/6529) of the study group. The incidence rate for this group was 509/100,000 children per year with the rate for boys (n = 708) more than double that of girls (n = 298, IRR 2.38, 95% CI 2.21–2.56).
Comparison between 2007 and 2014
Comparison of demographics, anatomical site of fracture and treatment of 100 random patients from 2007 and 2014 revealed no difference in gender, age, fracture type, rate of surgical intervention or type of surgery (Table 2).
Table 2.
Comparison of demographics, fracture type and treatment method of 100 random patients from 2007 and 100 patients from 2014.
| 2007 | 2014 | P-value | |
| Patients (n) | 100 | 100 | |
| Male : Female | 62 : 38 | 61 : 39 | 0.84 |
| Mean age (years) | 9.8 (1.2–16.2) | 10.0 (1.2–16.4) | 0.71 |
| Age group: | |||
| Toddler | 7 | 1 | 0.09 |
| Pre-school | 4 | 9 | |
| Young school | 36 | 37 | |
| Older school | 53 | 53 | |
| Operated | 22 | 26 | 0.36 |
| MUA | 17 | 21 | |
| Internal fixation | 5: plate 3, k-wire 1, fn 1 | 5: plate 2, k-wire 3 | |
| Fracture type: | |||
| Physeal | 13 | 10 | 0.70 |
| Metaphyseal | 73 | 78 | |
| Distal diaphyseal | 14 | 12 |
fn, flexible nails; MUA, manipulation under anaesthesia.
Biennial sampling
There was no change in fracture type sustained across any of the age groups over the study period. No obvious trend was seen in rate of surgery across the sampled patients. Surgery was rare in toddlers. Boys underwent more surgical procedures overall (boys n = 42, girls n = 24, P = 0.011; Table 3).
Table 3.
Number of surgical procedures performed in the age and gender specific sampled groups over the study period.
| Age group | Patients (n) | Sex | Patients requiring surgical intervention | |||
| 2007/08 | 2009/10 | 2011/12 | 2013/14 | |||
| Toddler | 10 | Male | 0 | 0 | 1 | 1 |
| 10 | Female | 0 | 0 | 0 | 0 | |
| Preschool | 10 | Male | 1 | 2 | 4 | 1 |
| 10 | Female | 0 | 0 | 1 | 1 | |
| Younger school age | 20 | Male | 4 | 5 | 6 | 2 |
| 20 | Female | 2 | 2 | 1 | 5 | |
| Older school age | 30 | Male | 5 | 2 | 2 | 6 |
| 30 | Female | 2 | 2 | 6 | 2 | |
Incidence
There was no overall change in incidence across the eight years investigated (Fig 1). The only significant change in incidence across all years, age groups and gender was a higher than expected number of fractures in preschool children (boys and girls combined) in 2011 (P = 0.0085). There was no difference in the pattern of trends between the age groups.
Figure 1.
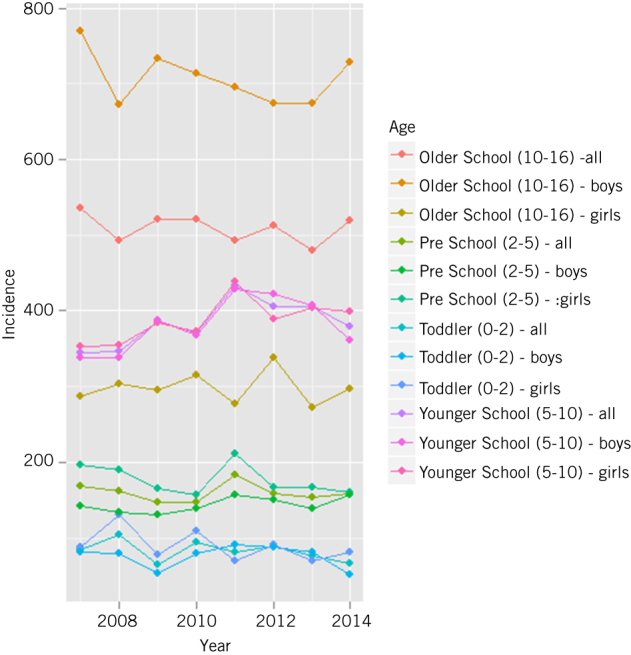
Incidence rate (100,000 children per year) by age group and gender per year.
Seasonality
There was a significantly lower rate of fractures in winter and higher rate in spring and summer for children in all the age groups except toddlers (P <= 0.0001; Fig 2). There was no change seen across the seasons for toddlers. Comparing the trends between the age groups showed significant differences in the pattern of the trends between all the age groups.
Figure 2.
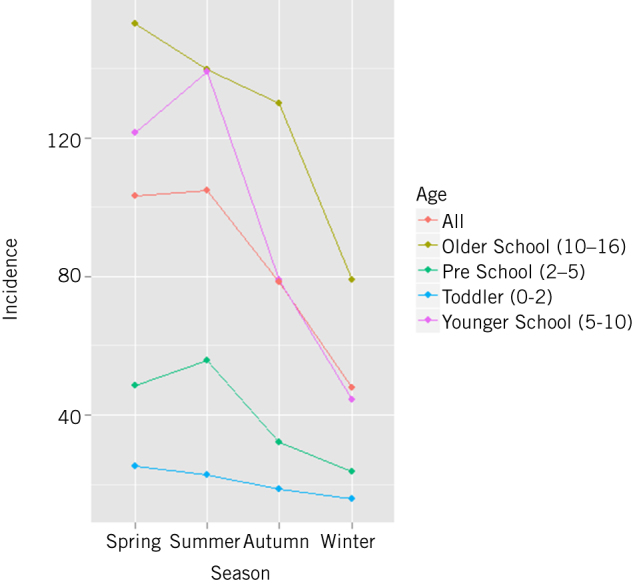
Incidence rate (100,000 children per year) by age group per season.
Days of the week
Older children suffered fewer fractures on Saturdays (P = 0.028) and Tuesdays (P = 0.023; Fig 3). When the results of all ages were combined, fewer fractures were seen on Saturdays (P = 0.014) but there were no other differences. The other age groups showed no variability per day of the week. Older children suffered fractures in a different pattern compared with other age groups (P = 0.007). There was no difference in the trend pattern between the other age groups.
Figure 3.
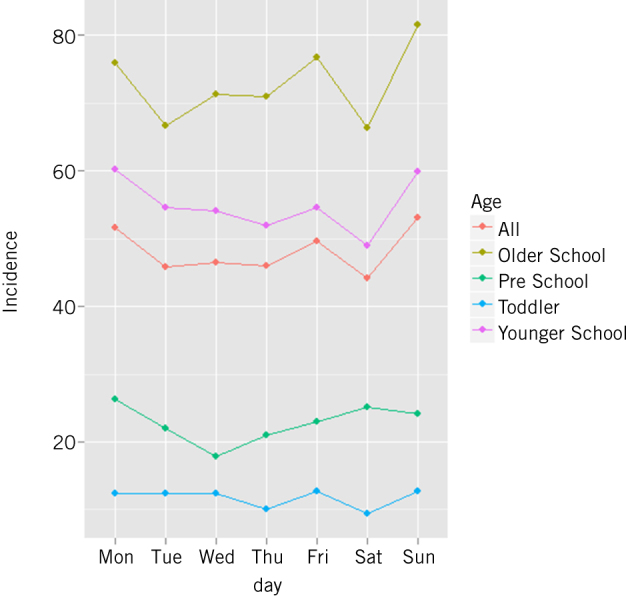
Incidence rate (100,000 children per year) by age group per day of the week.
Age
There was a significant change in the mean age across the study years for all children combined (P = 0.04; mean age: 2007, 10.17 years, 2014, 9.92 years; Fig 4a). There was no difference when boys and girls where investigated separately, although the overall trend in boys suggested mean age was falling (boys; P = 0.08, girls; P = 0.68; Fig 4b,c). Further sub-analysis of all children by age group and gender did not demonstrate any difference.
Figure 4.
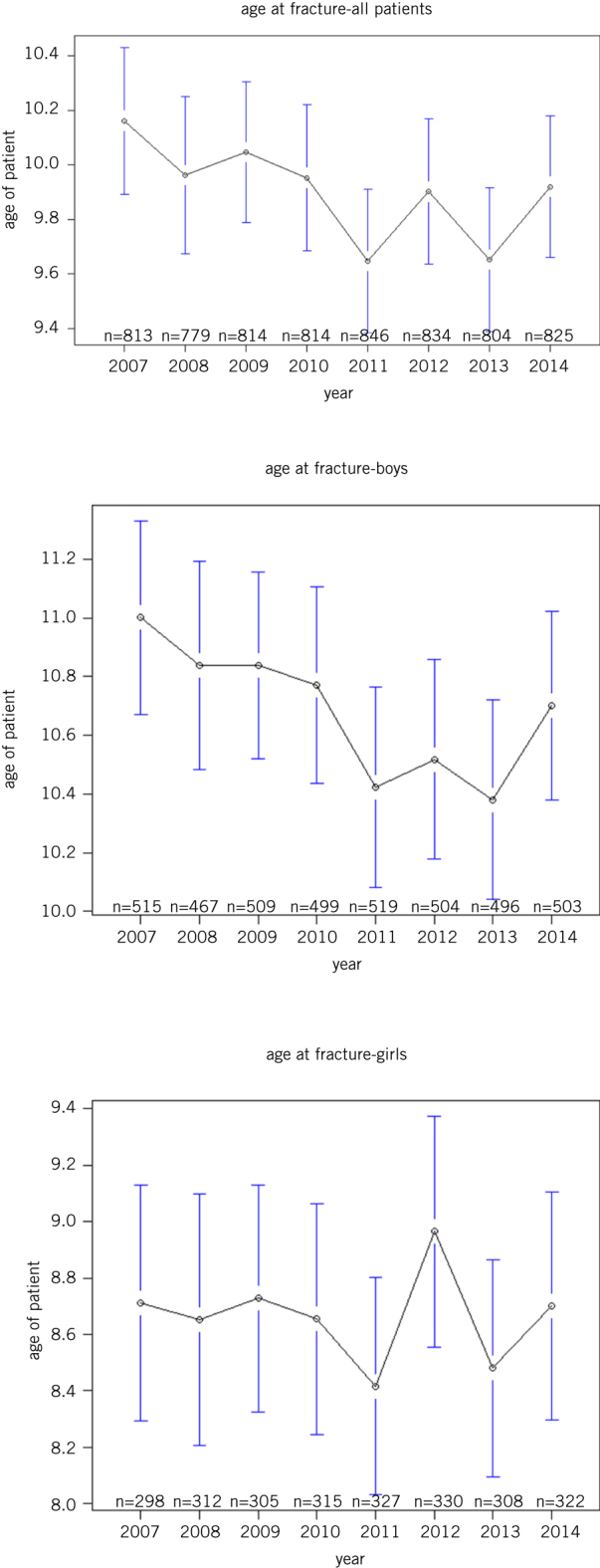
Mean age at fracture, with 95% confidence intervals, for all patients (a), boys (b) and girls (c) for each year of the study period.
Location of injury
There was no change within any age group or gender in the location that injury took place during the eight-year study period. Significant differences were observed between all age groups (Fig 5).
Figure 5.
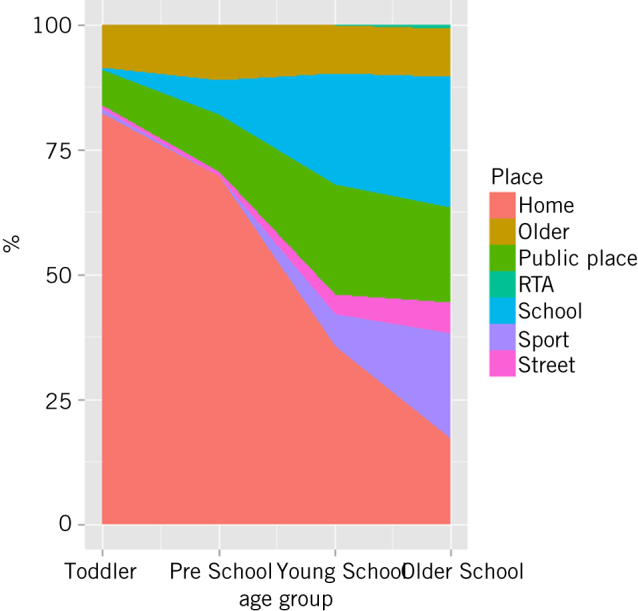
Location where injury took place by age group (RTA, road traffic accident).
Discussion
In this study, we describe the epidemiology of paediatric distal radius fractures in one unit in the UK. Gender and age group specific incidence rates are reported. Age distribution of patients was consistent with that previously described.9,14 Similar to other studies, the majority of patients were male. Fracture incidence did not increase over the study period.
Overall incidence rate was 337 fractures per 100,000 patient years. UK data for comparison are scarce. Many authors have reported results for different age ranges and some include all forearm fractures (Table 4).15,16 Cooper et al carried out a large study of over 80,000 children’s fractures using the general practitioner research database and noted an incidence rate of 393 per 100,000 patient years, which is broadly comparable to our results.3 They included all forearm fractures and patients up to the age of 18 years, which may explain the higher incidence. Other UK studies also reported a higher incidence than we found. In Glasgow, an incidence rate of 411 per 100,000 was seen in children aged up to 12 years, although fractures of the whole forearm were included.17 Lyons et al reported an incidence of 1289 distal radius fractures per 100,000 children aged up to 14 in South Wales.14 The authors acknowledged that this rate was exceptionally high but were unable to find an obvious cause. Social deprivation is known to be associated with paediatric wrist fractures.18 Leicester is one of the least deprived regions, so this may be a reason why our findings were lower than the other UK studies.
Table 4.
comparison of published incidence rates (100,000 children per year) for paediatric forearm and distal radius fractures.
| Study | Location | Incidence rate | Fractures (n) | Population at risk (patient years) | Study period (years) | Age group | Site |
| This study | Leicester, UK | 337 | 6529 | 1,937,656 | 8 | 0–16 | distal radius |
| Park et al, 201320 | South Korea | 801 | 83472 | 10,000,000a | 5 | 0–19 | forearm |
| Bell et al, 201217 | Glasgow, UK | 411 | 439 | 106,772 | 1 | 0–12 | forearm |
| Hedström et al, 20109 | Sweden | 591 | 393b | 34,239c | 14 | 0–19 | distal radius |
| Randsborg et al, 200915 | Norway | 470 | 362 | 77,470 | 1 | 0–16 | distal radius |
| Cooper et al, 20043 | UK | 393 | 25,271 | 7,000,000a | 10 | 0–18 | forearm |
| Brudvik et al, 200316 | Norway | 660 | 461 | – | 1 | 0–16 | distal radius |
| Khosla et al, 20035 | Rochester, US | 373 | 469 | – | 3d | 0–35 | distal radius |
| Lyons et al, 199914 | South Wales, UK | 1289e | 888 | 68,231 | 1 | 0–14 | distal radius |
a Approximation of annual at-risk population.
b Number of fractures from 2006–07 only.
c Mean annual at-risk population.
d results 1999–2001 shown; results also presented from four 3-year time periods from 1969 to 2001.
e Standardised fracture rate.
We did not demonstrate an increase in fracture incidence across our eight-year study period for total fractures or any gender or age specific group studied. This is in contrast to a large number of studies from across the world. In Finland, the incidence of paediatric forearm fractures increased by 31% from 1983 to 2005.19 Four of five of these fractures were of the distal radius. This was despite an overall significant 18% decrease in all children’s fractures during the same time period. These findings are similar to others reported from Sweden, the United States and Japan.5,7–10,20 Another Finnish study found a significant increase in children being hospitalised due to fractures from 1997 to 2006 with a 62% increase in surgery for forearm fractures.21 De Putter et al investigated wrist fracture trends in children and adolescents in Holland, a country with a similar climate to the UK, from 1997 to 2009.22 They found a significant increase in fracture incidence for children aged 5–9 years and 10–14 years, with the strongest increase in the age group 10–14 years. This was thought to be due to increased incidence rates during football and gymnastics at school.
The reasons for a change in fracture incidence rate are likely to be complex and multifactorial. Trampoline use has risen considerably, with a concurrent rise in trampoline-related injuries.23 Other studies have suggested increased fracture rates in Sweden may be due to a recent increase in physical activity and participation in team sports among Swedish children.24 Physical activity and sporting activities increase fracture risk while a sedentary lifestyle may protect against falls and injury.25 Therefore, a high incidence of fracture may suggest an active, fit population that is likely to remain healthy as adults. Conversely, our stable fracture incidence may reflect a sedentary population not engaged in vigorous activity.
Concerningly, paediatric wrist fractures have been shown to be associated with low bone mineral density, often occurring due to minor trauma.26,27 As with an adult wrist fracture, a forearm fracture may be an indicator of poor bone health in children.28 Activity levels, reduced calcium intake, vitamin D deficiency and poor nutrition are likely to be contributing factors. Increasing obesity is linked to poor mobility and balance, with overweight children sustaining higher energy injuries even with falls at low heights.29
Age and gender differences in fracture incidence were similar to those previously reported. Incidence rates were highest in the older school age group (10–16 years), with fractures being more common in boys.29,30 Fracture risk is related to changes in bone mineral density during the pubertal growth spurt. At this time, bones lengthen considerably with comparatively small, slow increase in bone mineral content.31 Behavioural changes and risk taking is thought to explain the gender differences.32
Fracture incidence was highest in spring and summer for children aged 2–16 years. There was no link with seasonality for those aged 0–2 years. These findings are consistent with other studies. Summer has previously been shown to be the most common season for childhood injuries, with the warmer weather encouraging outdoor activities.33 In the older school-age group, spring was the most common season for fracture, but not significantly higher than summer. Ryan et al studied 929 children with forearm fractures in Washington DC and found that the rate of fracture was highest in spring.26 They felt this might be due to low vitamin D levels, which are lowest in spring and winter. Our results may suggest a similar trend. Another reason may be the harder pitches seen in spring towards the end of the football and rugby seasons.
Patients attended hospital with a fracture less frequently on a Saturday, with older school children also attending less frequently on a Tuesday. The overall results were influenced by the larger number of children in the younger and older school-age groups. Our data were collected on attendance to the emergency department and it is likely that children with less severe fractures may not present until the day after their injury if they initially try to self-treat or the injury occurs in the evening. Fridays and Mondays are days when sports are less likely to take place therefore fewer patients may sustain injuries on these days and then present on Saturday or Tuesday. There was a trend for higher incidence rates on Sunday and Monday. These findings would be consistent with sporting activities and injuries taking place at the weekend with medical attention subsequently being sought on Sunday and Monday.
In this large study of UK paediatric distal radius fracture epidemiology we have investigated trends which provide helpful new evidence for healthcare planning and injury prevention. Accurate incidence rates were calculated using gender and age specific data for the relevant year of injury from the UK Office for National Statistics. However, we recognise the limitations of our data. The retrospective nature of analysis of prospectively collected data may predispose to bias, although this should be limited. Other studies we have compared our results with had longer study periods.5,7–10 The organisation of orthopaedic services within our region should ensure comprehensive capture of fractures within the study population and we therefore expect our figures to be accurate.
Some children may have presented to their general practitioner and been managed without referral or through private healthcare. It is likely this would only be a small number of children with minor fractures. The unit is not a major trauma centre. The local major trauma centre opened in 2012 so some seriously injured children with distal radius fractures from our region may have been treated there. We expect this number would be small and it does not seem to have influenced the trends we identified. Our data collected detailing location of injury was incomplete and we have therefore not studied this in detail. We did not obtain information about the nature of the injury or further patient characteristics such as ethnicity or body mass index. We used sampling methods for investigating surgery and fracture types. Radiographical review of all patients in the study would have been extremely time consuming and we believe our sample sizes are large enough to produce meaningful results.
This study offers useful information regarding the epidemiology of paediatric distal radius fractures, which may be of significant clinical value. In contrast to other studies the rate of fractures is not increasing in our region. There was no change seen in rate of surgery or fracture type. The main variation in fracture incidence is related to season. These data can help to predict accurately the probable number of children presenting to emergency departments with wrist fractures at a particular time of year. This helps to plan and use healthcare resources more efficiently and target preventative strategies effectively.
References
- 1.Lyons RA, Lo SV, Heaven M, Littlepage BN. Injury surveillance in children: usefulness of a centralised database of accident and emergency attendances. Inj Prev 1995; (3): 173–176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Walsh SS, Jarvis SN, Towner EM, Aynsley-Green A. Annual incidence of unintentional injury among 54,000 children. Inj Prev 1996; (1): 16–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Cooper C, Dennison M, Leufkens G et al. Epidemiology of childhood fractures in Britain: a study using the general practice research database. J Bone Miner Res 2004; (12): 1,976–1,981. [DOI] [PubMed] [Google Scholar]
- 4.Spady DW, Saunders DL, Schopflocher DP, Svenson LW. Patterns of injury in children: a population-based approach. Pediatrics 2004; (3): 522–529. [DOI] [PubMed] [Google Scholar]
- 5.Khosla S, Melton LJ, Dekutoski B et al. Incidence of childhood distal forearm fractures over 30 years: a population-based study. JAMA 2003; (11): 1,479–1,485. [DOI] [PubMed] [Google Scholar]
- 6.Rennie L, Court-Brown CM, Mok JYQ, Beattie TF. The epidemiology of fractures in children. Injury 2007; (8): 913–922. [DOI] [PubMed] [Google Scholar]
- 7.Mathison DJ, Agrawal D. An update on the epidemiology of pediatric fractures. Pediatr Emerg Care 2010; (8): 594–606. [DOI] [PubMed] [Google Scholar]
- 8.Landin LA. Epidemiology of children’s fractures. J Pediatr Orthop B 1997; (2): 79–83. [DOI] [PubMed] [Google Scholar]
- 9.Hedström EM, Svensson O, Bergström U, Michno P. Epidemiology of fractures in children and adolescents: increased incidence over the past decade: a population-based study from northern Sweden. Acta Orthop 2010; (1): 148–154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hagino H, Yamamoto K, Ohshiro H, Nose T. Increasing incidence of distal radius fractures in Japanese children and adolescents. J Orthop Sci 2000; (4): 356–360. [DOI] [PubMed] [Google Scholar]
- 11.Flynn JM, Jones KJ, Garner MR, Goebel J. Eleven years’ experience in the operative management of pediatric forearm fractures. J Pediatr Orthop 2010; (4): 313–319. [DOI] [PubMed] [Google Scholar]
- 12.Cheng JCY, Ng BKW, Ying SY, Lam PKW. A 10-year study of the changes in the pattern and treatment of 6,493 fractures. J Pediatr Orthop 1999; (3): 344–350. [PubMed] [Google Scholar]
- 13.Marsh JL, Slongo TF, Agel J et al. Fracture and dislocation classification compendium – 2007: Orthopaedic Trauma Association classification, database and outcomes committee. J Orthop Trauma 2007; (10 Suppl): S1–S133. [DOI] [PubMed] [Google Scholar]
- 14.Lyons RA, Delahunty AM, Kraus D et al. Children’s fractures: a population based study. Inj Prev 1999; (2): 129–132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Randsborg P-H, Sivertsen EA. Distal radius fractures in children: substantial difference in stability between buckle and greenstick fractures. Acta Orthop 2009; (5): 585–589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Brudvik C, Hove LM. Childhood fractures in Bergen, Norway: identifying high-risk groups and activities. J Pediatr Orthop 2003; (5): 629–634. [DOI] [PubMed] [Google Scholar]
- 17.Bell SW, McLaughlin D, Huntley JS. Paediatric forearm fractures in the west of Scotland. Scott Med J 2012; (3): 139–143. [DOI] [PubMed] [Google Scholar]
- 18.Menon MR, Walker JL, Court-Brown CM. The epidemiology of fractures in adolescents with reference to social deprivation. J Bone Joint Surg 2008; (11): 1,482–1,486. [DOI] [PubMed] [Google Scholar]
- 19.Mäyränpää K, Mäkitie O, Kallio E. Decreasing incidence and changing pattern of childhood fractures: a population-based study. J Bone Miner Res 2010; (12): 2,752–2,759. [DOI] [PubMed] [Google Scholar]
- 20.Park MS, Chung CY, Choi I et al. Incidence patterns of pediatric and adolescent orthopaedic fractures according to age groups and seasons in South Korea: a population-based study. Clin Orthop Surg 2013; (3): 161–166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Helenius I, Lamberg TS, Kääriäinen S et al. Operative treatment of fractures in children is increasing. J Bone Joint Surg 2009; (11): 2,612–2,616. [DOI] [PubMed] [Google Scholar]
- 22.de CE, van EF, Looman CW et al. Trends in wrist fractures in children and adolescents, 1997–2009. J Hand Surg 2011; (11): 1,810–1,815. [DOI] [PubMed] [Google Scholar]
- 23.Shankar A, Williams K, Ryan M. Trampoline-related injury in children. Pediatr Emerg Care 2006; (9): 644–646. [DOI] [PubMed] [Google Scholar]
- 24.Raustorp A, Ludvigsson J. Secular trends of pedometer-determined physical activity in Swedish school children. Acta Paediatr 2007; (12): 1,824–1,828. [DOI] [PubMed] [Google Scholar]
- 25.Clark EM, Ness AR, Tobias JH. Vigorous physical activity increases fracture risk in children irrespective of bone mass: a prospective study of the independent risk factors for fractures in healthy children. J Bone Miner Res 2008; (7): 1,012–1,022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ryan M. Forearm fractures in children and bone health. Curr Opin Endocrinol Diabetes Obes 2010; (6): 530–534. [DOI] [PubMed] [Google Scholar]
- 27.Jones IE, Taylor RW, Williams S et al. Four-year gain in bone mineral in girls with and without past forearm fractures: a DXA study. J Bone Miner Res 2002; (6): 1,065–1,072. [DOI] [PubMed] [Google Scholar]
- 28.Goulding A, Jones IE, Taylor R et al. Bone mineral density and body composition in boys with distal forearm fractures: a dual-energy x-ray absorptiometry study. J Pediatr 2001; (4): 509–515. [DOI] [PubMed] [Google Scholar]
- 29.Ryan LM, Teach J, Searcy K et al. Epidemiology of pediatric forearm fractures in Washington, DC. J Trauma 2010; (4 Suppl): 200–205. [DOI] [PubMed] [Google Scholar]
- 30.Nellans KW, Kowalski E, Chung KC. The epidemiology of distal radius fractures. Hand Clin 2012; (2): 113–125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Krabbe S, Christiansen C, Rodbro P, Transbol I. Effect of puberty on rates of bone growth and mineralisation: with observations in male delayed puberty. Arch Dis Child 1979; (12): 950–953. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Joeris A, Lutz N, Wicki B et al. An epidemiological evaluation of pediatric long bone fractures: a retrospective cohort study of 2716 patients from two Swiss tertiary pediatric hospitals. BMC Pediatr 2014; : 314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Kane BE, Mickalide AD, Paul HA. Trauma Season: A National Study of the Seasonality of Unintentional Childhood Injury. Washington, DC: National Safe Kids Campaign; 2001. [Google Scholar]