

Abstract
Background:
Diet has an important role to play in the well-being of human body.
Aims:
The study intends to establish the “hypothesis of conscious, selective, and self-destruction i.e., deregulated autophagy of skin and hair in low dietary protein scenario” by determining the facial profile, clinical presentation, and histopathological correlation of deficient protein intake and missing of meals in a tertiary care aesthetic skin institute.
Methods:
A total of 98 patients of skin- and hair-related complaints were enrolled in the study and a histopathological correlation was established by skin and scalp biopsies in high and low protein groups.
Results:
A significant number of subjects (68.4%) were taking less than half of the recommended daily allowance of proteins and faced problems like hair fall, acne, pigmentation, vitiligo, hirsutism, melasma, and premature aging. Subjects missing breakfast were found to have hypothyroidism, diffuse hairfall, autoimmune disorders like vitiligo, lichen planus, and alopecia areata. Histopathological images from submental area showed loose and fragmented collagen in high carbohydrate group in comparison to high protein group where thick, uniformly stained collagen bundles were found in dermis. Histopathology of scalp tissue showed chronic perifollicular inflammatory infiltrate and fibrosis in high carbohydrate group which was absent in histopathology specimen of high protein group. Patients taking early and nutrient-rich breakfast had higher mean protein intakes and less severe skin and hair problems suggesting a role of circadian rhythm as well.
Conclusion:
Dietary protein adequacy and early breakfast have significant role in preventing self-destruction or deregulated autophagy in trichology and cosmetic dermatology and may prevent various autoimmune, inflammatory, and metabolic diseases.
Keywords: Aging, autophagy, circadian rhythm, hair fall, melasma, protein
Introduction
In the pursuit of lasting and rewarding therapeutic strategies for youthful skin, healthy hair, and perfect bodies, today's dermatologists are venturing into uncharted territories and endeavoring to enhance the gifts of nature. But as we are looking more on the microscopic levels, we have probably missed the larger picture. Most of us have heard the phrase “You are what you eat.” Ever since Jean Anthelme Brillat Savarin opened the debate by proposing this idea, it has intrigued researchers and laymen equally. So, is it true “our skin and hair are also what we eat?” The particular macronutrient that caught our attention was protein, considered the building block of our body, skin, and hair not being any exception; but how our body deals with latter two in deficient nutrition scenario needs to be established.
Aims of Study
The study was undertaken to establish the proposed “hypothesis of conscious, selective, self-destruction, or non-renewal of skin and hair i.e., deregulated autophagy by body in low protein scenario.”
Methods
A total of 98 subjects aged >15 years attending the clinic over a period of 1 month for skin- and hair-related indications like acne, hairfall, premature aging, melasma, periorbital hyperpigmentation (POH), and post-inflammatory hyperpigmentation (PIH) were enrolled in the study. Many subjects also had coexisting cutaneous diseases, like vitiligo, psoriasis, tinea corporis, acanthosis nigricans (AN), macular amyloidosis and medical conditions, like hypothyroidism, diabetes, hypertension, and coronary artery disease. A detailed dietary history was taken with special emphasis on timings of each diet, quality, and quantity of nutrients in food. Protein intake was calculated using the standard protein content of common food items as outlined by the National Institution of Nutrition, Hyderabad, India[1] and other nutritional guidelines[2] [Table 1]. An average protein intake of 60 g in males and 55 g in females was considered adequate, though an intake of 0.8–1.0 g/kg/day should be considered optimal on an individual basis.
Table 1.
Protein content of major Indian food items
| Food item | Portion size (g) | Protein content/per portion (g) | Carbohydrates (g) | Fat (g) |
|---|---|---|---|---|
| Cereals/millets | 30 | 3 | 20 | 0.8 |
| Pulses | 30 | 6 | 15 | 0.7 |
| Milk | 100 ml | 3 | 5 | 3 |
| Egg (whole) Egg white=2/3rd protein of whole egg |
50 | 6 4 |
NA | 7 |
| Meat/chicken | 50 | 9 | NA | 7 |
| Fish [codfish (18g), tuna fish (30g), salmon (20g) per 100g] | 50 | 13 | NA | 5 |
| Green leafy vegetables | 100 | 3.6 | NA | 0.4 |
| Roots/tubers | 100 | 1.3 | 18 | NA |
| Other vegetables | 100 | 1.7 | 0.2 | |
| Fruits | 100 | 10 | NA |
As per the diet pattern of the patient, we classified their facial profile as carbohydrate face, deficient face, and a balanced face. High-resolution digital pictures were taken to observe the difference in different types of faces.
Ten subjects were randomly selected from high protein and low protein group each and their scalp and submental skin biopsies were performed to analyze the condition of skin and hair follicles.
Statistical analysis of data were done using frequency tables, one-way analysis of variance (ANOVAs) test, one sample t-test, independent t-test, and Fisher's exact test for association.
Results and Observations
Common presentation
Out of 98 patients attending the outpatient department, females (61) outnumbered males (37). Acne vulgaris was the most frequently encountered complaint, followed by androgenetic alopecia (AGA), POH and melasma [Table 2].
Table 2.
Distribution of dermatological conditions in study subjects
| Dermatological/trichological problem | Percentage |
|---|---|
| Acne | 28.57 |
| Androgenetic alopecia (AGA) | 20.40 |
| Periorbital hyperpigmentation (POH) | 14.28 |
| Melasma | 12.24 |
| Female pattern baldness (FPB) | 11.22 |
| Hirsutism | 10.20 |
| Post-inflammatory hyperpigmentation (PIH) | 9.18 |
| Premature aging | 9.18 |
| Telogen effluvium (TE) | 8.16 |
| Macular amyloidosis | 8.16 |
| Seborrheic capitis | 7.14 |
| Vitiligo | 6.12 |
| Striae | 4.08 |
| Acanthosis nigricans (AN) | 4.08 |
| Tinea infections | 4.08 |
| Alopecia areata (AA) | 3.06 |
| Psoriasis | 3.06 |
Dietary pattern
Most of the patients (91.83%) were taking <50 g/day of protein i.e., less than recommended daily allowance (RDA) and 68.36% were severely deficient (<30 g/day of protein intake) [Table 3].
Table 3.
Protein intake groups according to daily intake
| Protein intake (g/day) | No. of subjects (n) | Percentage |
|---|---|---|
| 10-30 (severe deficiency/poor intake) | 67 | 68.36 |
| 30-50 (moderate deficiency/low intake) | 23 | 23.47 |
| ≥50 (no deficiency/optimal intake) | 8 | 8.16 |
| Total | 98 | 100.0 |
The vegetarians (61.2%) outnumbered non-vegetarians and were significantly deficient in protein intake (P value 0.005) [Table 4].
Table 4.
Protein intake according to type of diet (vegetarian/non-vegetarian)
| Protein intake (g/day) | Vegetarians (%) | Non-vegetarians (%) |
|---|---|---|
| <20 | 21 (35) | 7 (18.4) |
| 20-30 | 26 (43.3) | 13 (34.2) |
| 30-40 | 10 (16.7) | 10 (26.3) |
| 40-50 | 0 (0.0) | 3 (7.9) |
| ≥50 | 3 (5.0) | 5 (13.2) |
| Total | 60 | 38 |
Most of the patients (67.3%) were taking late breakfast and a significant number of patients (20.4%) missed it completely. Only 12.2% patients were taking their breakfast early in the morning i.e., by 8.30 a.m. Mean protein intakes were higher (35.42g) in patients taking their breakfast early as compared to those who missed breakfast (15.64g) and late takers (9.39 g) with a statistically significant difference (P value 0.017) [Table 5].
Table 5.
Daily protein intake according to breakfast timings
| Breakfast timings |
Total | |||
|---|---|---|---|---|
| On time | Late | Miss | ||
| Protein (g/day) | ||||
| <20 | 1 | 21 | 6 | 28 |
| 8.3% | 31.8% | 30.0% | 28.6% | |
| 20-30 | 4 | 30 | 5 | 39 |
| 33.3% | 45.5% | 25.0% | 39.8% | |
| 30-40 | 2 | 13 | 5 | 20 |
| 16.7% | 19.7% | 25.0% | 20.4% | |
| 40-50 | 1 | 0 | 2 | 3 |
| 8.3% | 0.0% | 10.0% | 3.1% | |
| ≥50 | 4 | 2 | 2 | 8 |
| 33.3% | 3.0% | 10.0% | 8.2% | |
| Total | 12 | 66 | 20 | 98 |
| 100.0% | 100.0% | 100.0% | 100.0% | |
Among hypothyroid patients (n = 11), more than half were taking breakfast late and one-thirds missed it. Similarly, 57.14% of vitiligo patients missed their breakfast and rest all had it late.
Age group, gender, and dietary co-relation
Majority of patients (73.5%) were <35 years of age and females (62.2%). Females were more deficient in protein intake than males (P value 0.050).
More than half of the patients who belonged to upto 25 years (53.85%) and 26–35 years age group (69.56%) were severely deficient in protein intake (<30 g/day). In patients aged 36–45 years and above, maximum number (85.7% and 75%, respectively) belonged to this category. The diseases encountered varied in different age groups are given in [Table 6].
Table 6.
Conditions encountered in protein-deficient subjects
| Dermatological and trichological conditions encountered in patients taking less than half of their recommended daily intake (<30 g/day of protein) | |
|---|---|
| Age group | Conditions encountered |
| Up to 25 years | Acne (30.77%), hirsutism (26.92%), TE (15.38%), andAGA (11.54%) |
| 26-35 years | Melasma (19.56%), AGA (17.39%), acne (13.04%), POH and PIH (13.04%), and vitiligo (10.87%) |
| 36-45 years andabove | POH (34.61%), aging (30.77%), macular amyloidosis (23.08%) |
TE=Telogen effluvium, AGA=Androgenetic alopecia, POH=Periorbital hyperpigmentation, PIH=Post-inflammatory hyperpigmentation
Hair disorders
The common clinical causes of hairfall included AGA, female pattern baldness (FPB), telogen effluvium (TE), and alopecia areata (AA). About 90% of AGA patients were deficient in protein, with 55% of them severely deficient (<30 g/day protein). Most of FPB patients (90.90%) and three-fourths (75%) of TE patients were severely deficient [Chart 1].
Chart 1.
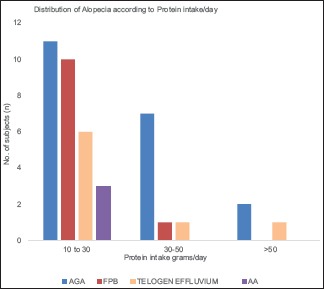
Alopecia distribution
Skin disorders
Among patients showing visible signs of aging like photodamage, pigmentation, fine and deep wrinkles; 88.88% patients were severely deficient. All patients of striae and macular amyloidosis and most of AN (75%) had severe deficiency (intake <30 g/day) [Chart 2].
Chart 2.
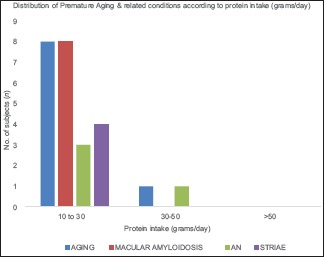
Aging distribution
Most of the patients of melasma (91.66%), POH (92.85%), and PIH (88.88%) were severely deficient in protein intake [Chart 3]. Half of acne patients (50%) and more than two-thirds of hirsutism patients (70%) had severe protein deficiency (<30 g/day) [Chart 4]. Majority of vitiligo patients (83.33%) were severely deficient in protein (<30 g/day). All patients had concomitant vitamin D deficiency, 71.43% were hypothyroid, and 57.14% had vitamin B12 deficiency. Majority of patients having dermatophytic infections (75%) and many of seborrheic dermatitis patients (42.85%) were poor protein takers.
Chart 3.
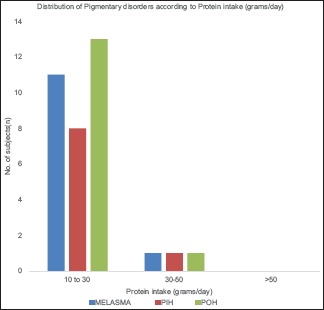
Pigmentary disorders distribution
Chart 4.
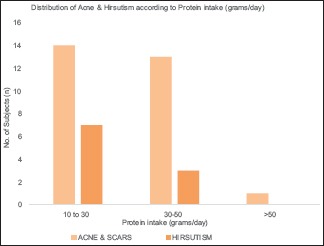
Acne and hirsutism
Histopathology findings
The scalp [Figure 1] and submental [Figure 2] skin biopsies (H and E stain) from high protein group revealed lesser thickness of epidermis and dermis due to more compact and regularly arranged collagen bundles as compared to low protein (high carbohydrate) group which had thicker epidermis and dermis, with loosely placed and lesser number of collagen fibrils and plump fibroblasts [Figures 3 and 4].
Figure 1.
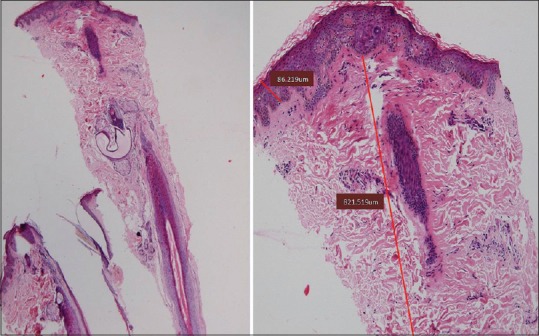
Hematoxylin and eosin stain (H and E) image of scalp biopsy from a subject in high protein group (×10 resolution)
Figure 2.
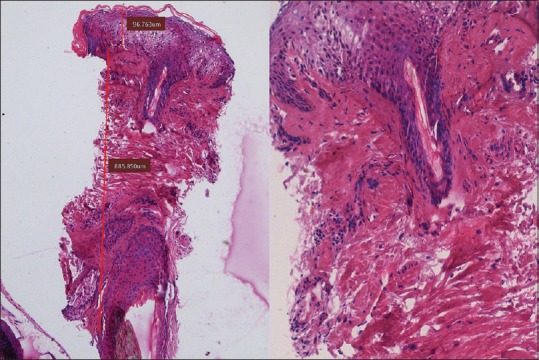
Hematoxylin and eosin stain (H and E) image of skin biopsy from submental region in a subject in high protein group (×10 resolution)
Figure 3.
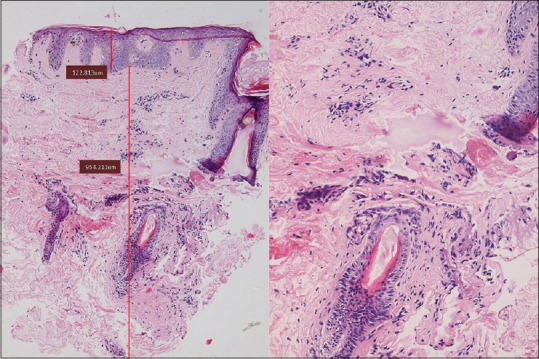
Hematoxylin and eosin stain (H and E) image of skin biopsy from submental region in a subject in low protein group (×10 resolution)
Figure 4.
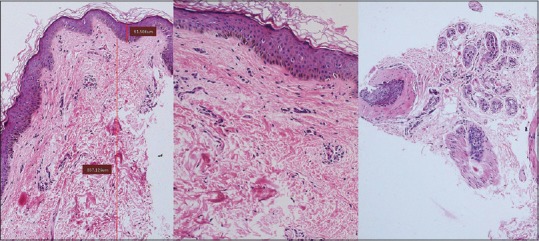
Hematoxylin and eosin stain (H and E) image of scalp biopsy from a subject in low protein group (×10 resolution), marked perifollicular inflammation, and fibrosis seen
Scalp biopsy from low protein group showed perifollicular chronic inflammatory infiltrate and perifollicular fibrosis [Figure 4], whereas high protein group follicles showed normal follicular structure [Figure 1].
These findings were also confirmed and correlated in scalp videodermoscopic analysis [Figure 5].
Figure 5.

Videodermoscopic evidence of thinning of hair follicle, perifollicular fibrosis (black circle), complete disappearance of hair follicle, and atrophic scar (blue circle) on other side in scalp video microscopy (×50) in a patient with chronic telogen effluvium taking deficient protein diet (<20 g/day) and missing breakfast for many years
Facial phenotypes
Majority of patients (69.80%) had carbohydrate face, 20% had deficient face, and only 10.20% had a balanced-looking face [Figures 6–8].
Figure 6.

Photograph showing carbohydrate face (carb face) with heavy, loose saggy skin with ill-defined jawline or bony prominences, outline periorbital pigmentation or puffiness
Figure 8.
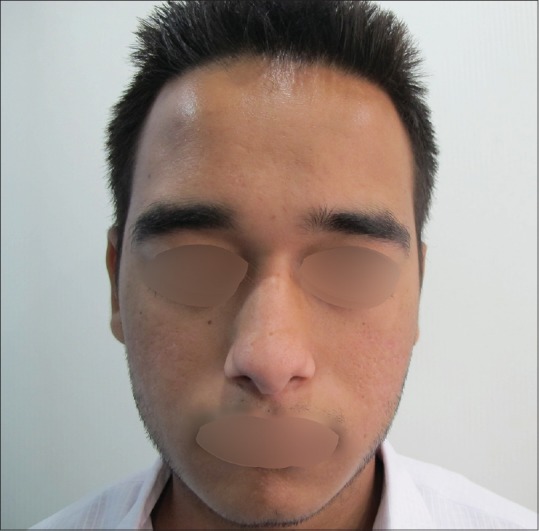
Photograph showing balanced face with good volume in mid face and well-defined jawline without hollow or puffy eyes
Figure 7.

Photograph showing deficient face with chiselled look, firm skin, well-defined jaw line but hollowness around eyes and mid face
Discussion
The Indian diet system has the advantage that most of the food cooked is fresh and free of preservatives, but the downside is lack of awareness of the actual food value. Our textbooks do not highlight the problems faced due to protein deficiency; as most of the literature we follow is written by western population who usually consumes protein-rich diet and face less problems like psoriasis, diabetes, dyslipidemias, and other metabolic syndromes than we do. The aim of this study is to highlight the deficiency of proteins consumed, various disorders faced, and how body handles this deficiency.
Most of essential work of human body are handled by proteins; like maintaining structure of all tissues, enzymes of metabolic reactions, repair of wear and tear besides providing immunity to infections. It is imperative that a constant supply of nutrients in food is maintained as “fuel to machine” for the efficient working of array of these processes. Amino acids are a unique entity as the “letters” indispensable to the DNA-dependent “writing” of proteins. Hence, without simultaneous availability of all amino acids, no protein synthesis takes place and the first metabolic response is catabolism to maintain the integrity of protein machinery of cells and tissues. This causes a general aging of all structural (collagen, elastin) as well as functional proteins e.g., enzymes, antibodies, and eventual loss of their efficiency.[3,4]
Protein deficiency was encountered in most of the patients reporting to our clinic, most of them taking not even half of the required daily intake (<30 g/day) and more than one-fourth were very poor eaters (<20 g/day). Surprisingly the population visiting the clinic is affluent and easily affording various treatments. The dietary deficiency was mostly due to lack of awareness about the quality of food, busy job profiles, faulty lifestyle, or crash dieting for quick weight loss.
Breakfast emerged as the most important meal as patients eating breakfast on time fared much better than late eaters and missers in terms of daily protein intake. Breakfast missers, surprisingly had better intakes than late eaters, probably because they compensated protein intake in lunch time. Late takers are usually housewives who want to finish work and then eat or late risers or night shift workers who take brunch (mostly deprived of pulses), miss lunch altogether and take some quick snacks or junk food in the evening.
The higher mean protein intake observed in non-vegetarian patients can be explained by higher protein content of animal proteins. Though this gives an impression that non-vegetarian diets are richer in terms of protein, a noteworthy thing is that animal foods have higher saturated fat and cholesterol content, hence not making them a completely healthy choice. Vegetarian proteins, combined judiciously can provide essential amino acids, reasonably good amount of proteins in addition to phytochemicals, fiber, and numerous micronutrients.[5] It is recommended by the authors that the intake should be increased in accordance with the demand. The diurnal variation of body should be respected by taking protein-rich meal balanced with only natural carbohydrates like fresh fruits and nuts early in morning, preferably before 8 a.m., corresponding with endogenous cortisol surge.
Another study has highlighted the importance of nutrition in managing alopecia wherein scalp biopsies have shown that following good nutrition, there is a high spurt in cell division and growth rate in the dermal papilla cells as these cells require a good supply of nutrients to re-enter the anagen phase from a resting phase.[6] A high-fat diet is believed to reduce the levels of sex hormone binding globulin (SHBG) resulting in higher dihydrotestosterone (DHT) conversion rates at the hair follicle level aggravating AGA.[7]
Findings in our study present a similar trend that as majority of patients of FPB and TE had poor protein intakes. Few patients traced back the onset of hairfall with decrease in their dietary intake due to crash diets, postpartum period, or stress. Most of the AGA patients also had deficient protein intakes and a high carbohydrate/fat diet. A noteworthy finding in AGA patients was that many of them had a positive family history but of lesser severity and presentation in later life. The authors believe that low protein intake, missing breakfast, and faulty lifestyle hastened the onset and increased the severity of AGA. Another striking observation in two of AGA patients was that inspite of an intake of >50g/day of protein, they were simultaneously doing intense physical activities. This increased the protein requirements and led to diversion of amino acids toward muscles and a selective protein deprivation of hair. These patients were taking post workout protein-rich diet at night time but missed or had late breakfast. While ideally this should have compensated the protein deficit, the severity of their hair loss suggested otherwise. Thus concluding; missing breakfast or late breakfast is another important determinant in addition to poor protein and nutrient intake.
Our scalp biopsies endorse the finding of hair follicle destruction with perifollicular inflammation and fibrosis in low protein group (clinically carbohydrate facies) [Figure 4] while high protein group (clinically balanced facies) showed normal follicular structure [Figure 1]. Since hair is entirely protein by structure, it may be hypothesized that hair follicle fibrosis and destruction may be body's conscious decision of self-destruction to conserve proteins for more active and vital tissues like muscles. Authors suggest this phenomenon as “Hypothesis of conscious selective self-destruction and non-renewal” to maintain more important structures and functions.
The gross protein content of skin is around 22% and collagen is the most abundant protein in human body.[8] Hydroxyproline and hydroxylysine required for collagen synthesis are the metabolic dead end of proline and lysine, hence to maintain maximum physicochemical performance, “fresh” proline and lysine should be inserted in the newly synthesized collagen propeptide.[3] From these facts, stems a corollary that adequate amino acid intake to supply substrate and vitamin C as a cofactor for prolyl and lysyl hydroxylase is essential for maintaining existing collagen framework as well as neocollagenesis.[9]
All our patients showing aging were deficient in protein intakes, resulting in a compromise in collagen and elastin synthesis and efficiency of enzymes like matrixmetalloproteinases (MMPs) which help in degradation of old proteins.[9]
The skin biopsy of low protein subject with clinical carbohydrate facies revealed loose, fragmented low quality collagen [Figure 3] as compared to high protein subject (balanced facies) [Figure 2] where the collagen bundles were compactly arranged, delaying the aging process by holding the underlying subcutaneous tissue thus preventing overall sagging of skin and subcutis.
Similar observations were seen in patients of macular amyloidosis and AN, both of these conditions representing accelerated aging. Macular amyloidosis involves amyloid fibrils derived from keratin after epidermal damage and keratinocyte apoptosis.[10] Poor protein intake may contribute to this entity by increased senescence of keratin and inability to repair epidermal damage. In AN, high-carbohydrate and low-protein diet accelerates the insulin resistance, leading to keratinocyte and dermal fibroblast proliferation, resulting in hyperpigmentation and papillomatous appearance.[11]
All patients with striae were protein deficient indicating deficient collagen, elastin and fibronectin production and subsequently decreased tensile strength of skin.[12]
Relationship of acne with high glycemic index diets has long been proposed and debated.[13,14] A high glycemic index and low protein diet can lead to hyperinsulinemia and a cascade of endocrine triggers like raised insulin-like growth factor-1(IGF-1) and androgens, resulting in acne.[15] In our study as well, half of the acne patients belonged to the severe protein deficiency (<30 g/day) group.
More than two-thirds of hirsutism patients demonstrated a similar poor protein intake (<30 g/day). Poor protein intake leading to decreased SHBG levels and high circulating free testosterone and DHT levels may be the probable reason behind these observations and represent an area for further research.
A striking observation was low protein intake in almost all the patients of pigmentary disorders like melasma, PIH, and POH. The authors believe that poor amino acid supply limits the capacity of skin to repair the photodamage and decreases the keratinocyte turnover rate along with the accumulation of melanin. In cases of POH, poor protein intakes and decreased collagen turnover led to increased periorbital skin laxity and capillary fragility, thereby triggering the vascular component of POH and aggravating the melanocytic pigmentation.[16]
Most of vitiligo and AA patients were hypothyroid, vitamin D and B12 deficient, besides consuming low protein daily and missing or delaying breakfast; summarizing most of them were overall poor eaters. All hypothyroid patients were taking late breakfast or missing it and presented with issues like melasma, pigmentation, aging, and hair fall which may be attributed to late or missed breakfast as thyroid gland is most active in early morning after pituitary stimulus. A deficient nutritional supply of iodine, which can easily be provided by a pinch of salt, during these crucial hours, might lead to hypothyroidism.
Protein deficiency also interferes in surmounting an adequate immune response by impaired cytokine production and cell-mediated immunity against pathogens, as suggested by the findings in our patients with dermatophyte infections, acne, furuncles, and seborrheic dermatitis.[17]
To summarize, the “Hypothesis of conscious selective self-destruction or non-renewal” in scenario of inadequate protein supply may be body's calculated decision and protective reflex of diverting amino acids to active areas like muscle, immune system, and metabolic enzymes considering skin and hair as relatively non-essential as depicted in Figure 9. It results in shedding of hair and slow repair of skin leading to premature aging and pigmentation. Whether this decision comes from cellular receptors or cytokines in blood remains a mystery and needs to be further established in molecular studies. Also the patients in autoimmune disease group like vitiligo, lichen planus, AA were from very low/poor protein intake group; it is yet to be seen why body is giving signal of self-destruction to certain targets in skin, hair, and other tissues. It may again be a protective reflex either to derive nutrients through destruction of these tissues or to completely abolish the non-renewed senescent proteins releasing antigens, which later cause autoimmune antigen – antibody reactions in genetically predisposed individuals.
Figure 9.
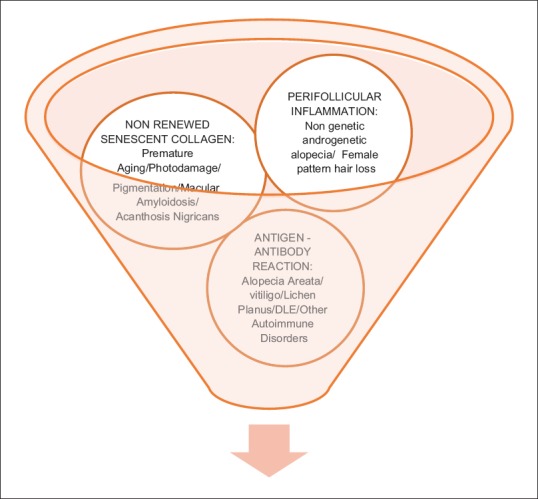
Hypothesis of conscious, selective self-destruction of skin and hair tissue in high-carb low-protein scenario
Few co-associations were strikingly noticed during the study. We suggest a “high-carb low-protein (HCLP) syndrome 1,2 and 3” as depicted in Table 7 for these, three different syndrome complexes due to deficient nutritional pathogenesis existing concomitantly.
Table 7.
Various HCLP (high-carb low-protein) syndromes and their associated dermatological and medical presentations
| Syndrome complex | Dermatological presentation | Medical presentation |
|---|---|---|
| HCLP syndrome 1 Usually follow a diet high on carbs and fats Adolescents and young adults |
Acne Hirsutism Telogen effluvium Seborrhea Perioral pigmentation Periorbital pigmentation Prematureandrogenetic alopecia Post-inflammatory hyperpigmentation Perioral/periorbital pigmentation Acanthosis nigricans Seborrhea |
Weight gain Irregular cycles Polycysticovarian syndrome (PCOS) Hormonal disturbances Gynecomastia Delayed secondary facial hair in males |
| HCLP syndrome 2 Usually missing breakfast or late breakfast/prolonged starvation Commonly seen in middle-aged females and night shift workers |
Melasma Macular amyloidosis Striae Periorbital pigmentation Perioral pigmentation, oral aphthous ulcers Vitiligo, Urticaria Alopecia areata Lichen planus Telogen effluvium |
Hypothyroidism Vitamin D deficiency Vitamin B12 deficiency Deficient iron studies Autoimmune disorders |
| HCLP syndrome 3 Usually follow a diet high on carbs and fats More commonin middle-aged or elderly men or peri-menopausal females |
Psoriasis vulgaris Androgenetic alopecia without genetic predisposition Female pattern hair loss Periorbital pigmentation and tear trough formation Acanthosis nigricans Macular amyloidosis Truncal obesity Skin tags |
Hypertension Type 2 diabetes Hyperinsulinemia Coronary artery disease Obesity Dyslipidemia Hyperuricemia Homocysteinemia |
Though HCLP1 and HCLP 3 syndromes are known to exist in high glycemic diet and insulin resistance scenario but our observations suggest that low protein intake is almost always an integral component in the pathogenesis because low protein Indian diets are usually carbohydrate rich [Figure 10].
Figure 10.
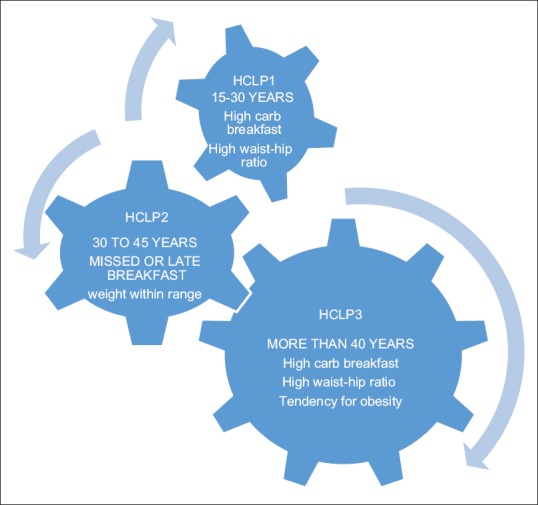
Depiction and interdependence of high-carb low-protein syndromes. HCLP1 may evolve to HCLP3 in later stage with presentation like metabolic syndrome
It is also recommended that the clinician should suggest basic investigations like thyroid function tests, Vitamin D and B12 levels, iron studies, lipid profile, uric acid levels, fasting blood sugar, HBA1C and serum insulin levels (in selected cases) to rule out other nutritional deficiencies. Presence of three clinical and two laboratory investigations simultaneously will confirm the nutritional component of syndrome complex. Deregulated autophagy also plays an important and integral part in mediation of effects of HCLP diet on ectodermal tissues[18,19] [Figure 11].
Figure 11.
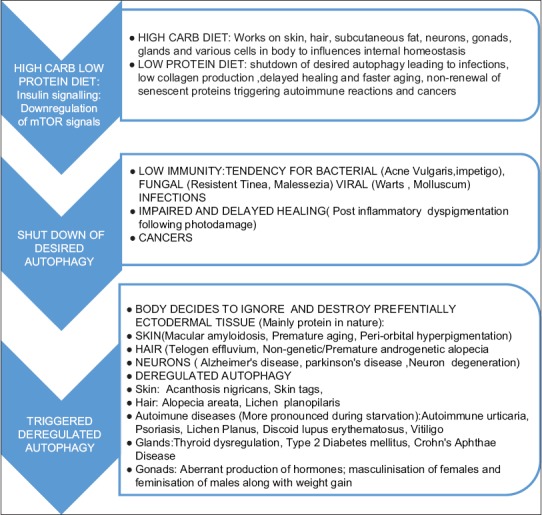
Hypothesis of intracellular high inducibility to high-carb low-protein diet leading to triggered signals in favor of deregulated autophagy: The process is chiefly determined by type of food available to cells; high protein food triggers mTOR signals which further stimulate ribosomal signals for protein translation while high-carb food triggers insulin signals to down regulate mTOR signals in yeasts, plants, and mammals,[18,19] which shuts down desired autophagy and subsequently stimulates deregulated autophagy as demonstrated in figure. Similar signals are sent in hypoxia, prolonged starvation, and reduced ATP levels inside cells to control cell homeostasis as per availability of nutrients. Interestingly nutrigenomics is the upcoming field which highlights epigenetic phenomenon of modifiable genes through right nutrition.[21,22]
The authors would also like to acknowledge that the dietary recommendations of eating early and nutrient dense breakfast along with lighter meals after sunset are among the cornerstones of ancient Indian Vedic philosophy.[20] Sunrise correlates well with morning surge of hormones and digestive enzymes and a decline in body's functional capacity after dusk.
The authors believe that though further in-depth molecular and histopathological studies are needed to fully elucidate the subject. Nevertheless, improving patient's nutritional quality is something which is feasible, cost-effective, and highly rewarding, especially in the scenario when cosmetic treatments have become a multibillion dollar industry. At the same time, it will help in reducing disease burden from metabolic diseases like diabetes, autoimmune disorders, protein energy malnutrition, hypothyroidism, resistant infections like recurrent fungal infections to name a few.
Interestingly, recent researches show that genes are modifiable through a phenomenon called epigenetics.[21] During our lifetime, nutrients can modify physiological, biological, and pathological processes through epigenetic mechanisms that are critical for gene expression. Nutrigenomics is an upcoming science which highlights modulation of epigenetic processes through diet. Specific nutrients may prevent diseases, aging and appearance of various cancers, play a crucial role in embryonic development, and eventually may help in treating genetic disorders and maintaining good health.[21,22]
The limitation of this study is though only protein intake has been evaluated as one macronutrient in this study, multiple macro-and micronutrients have a role in tissue response and pathogenesis of diseases which needs further indepth studies in future.
Conclusion
Protein is an essential macronutrient for optimal functioning, repair, and preventing the selective conscious self-destruction of various structures, especially skin and hair. Correcting coexistent protein deficiency and improving the timings of meals specially breakfast will improve treatment outcomes in trichology and cosmetic dermatology patients and picking up HCLP syndrome early especially by the dermatologists as the primary physicians may have preventive role in treatment of nutritional, autoimmune and metabolic diseases as well as resistant infections.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
Mr. Rajesh Kumar for helping with the statistical work.
References
- 1.Manual A. Dietary guidelines for Indians. [Last accessed on 2019 Feb 06];Nat Inst Nutrition. 2011 2:85–111. Available from: http://ninindia.org/DietaryGuidelinesforNINwebsite.pdf . [Google Scholar]
- 2.Med India.net. (homepage on internet) Chennai: Health calculators, nutrition utilities, protein calculator; 2001. [Last accessed on 2019 Feb 06]. Available from: http://www.medindia.net/patients/calculators/protein-intake-calculator-result.asp . [Google Scholar]
- 3.Dioguardi FS. Nutrition and skin. Collagen integrity: A dominant role for amino acids. Clin Dermatol. 2008;26:636–40. doi: 10.1016/j.clindermatol.2007.09.004. [DOI] [PubMed] [Google Scholar]
- 4.Draelos ZD. Aging skin: The role of diet: Facts and controversies. Clin Dermatol. 2013;31:701–6. doi: 10.1016/j.clindermatol.2013.05.005. [DOI] [PubMed] [Google Scholar]
- 5.Hoffman JR, Falvo MJ. Protein- which is best? J Sports Sci Med. 2004;3:118–30. [PMC free article] [PubMed] [Google Scholar]
- 6.Rajput RJ. Controversy: Is there a role for adjuvants in the management of male pattern hair loss? J Cutan Aesthet Surg. 2010;3:82–6. doi: 10.4103/0974-2077.69016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Spencer DK. The hormonal effects of diet on hair loss. In: Spencer DK, editor. The Bald Truth. New York: Simon and Schuster Inc; 1998. pp. 37–54. [Google Scholar]
- 8.Pai GS, Kamath KN, Kuruvila M. Disorders of connective tissue. In: Valia RG, Valia AR, editors. IADVL Textbook of Dermatology. 3rd ed. Mumbai: Bhalani Publications; 2008. p. 1154. [Google Scholar]
- 9.Traber MG, Stevens JF. Vit C and E: Beneficial effects from a mechanistic perspective. Free Radic Biol Med. 2011;51:1000–13. doi: 10.1016/j.freeradbiomed.2011.05.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lachmann HJ, Hawkin PN. Amyloidosis and the skin. In: Woulf K, Goldsmith L, Katz SI, Gilchrist BA, Paller AS, Lefell DJ, editors. Fitzpatrick's Dermatology in General Medicine. 7th ed. McGraw Hill; 2008. p. 1261. [Google Scholar]
- 11.Higgins SP, Freemark M, Prose NS. Acanthosis Nigricans: A practical approach to evaluation and management. Dermatol Online J. 2008;14:2. [PubMed] [Google Scholar]
- 12.Singh G, Kumar LP. Striae distensae. Indian J Dermatol Venereol Leprol. 2005;71:370–2. doi: 10.4103/0378-6323.16800. [DOI] [PubMed] [Google Scholar]
- 13.Layton AM. Disorders of sebaceous glands. In: Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook's Textbook of Dermatology. 8th ed. Oxford: Wiley-Blackwell Publication; 2010. p. 42.34. [Google Scholar]
- 14.Smith RN, Mann NJ, Braue A, Makelainen H, Varigos GA. A low-glycaemic load diet improves symptoms in acne vulgaris patients: A randomized controlled trial. Am J Clin Nutr. 2007;86:107–15. doi: 10.1093/ajcn/86.1.107. [DOI] [PubMed] [Google Scholar]
- 15.Cordain L, Lindeberg S, Hurtado M, Hill K, Eaton SB, Brand-Miller J. Acne vulgaris. A disease of western civilisation. Arch Dermatol. 2002;138:1584–90. doi: 10.1001/archderm.138.12.1584. [DOI] [PubMed] [Google Scholar]
- 16.Souza DM, Ludtke C, Souza ERM, Scandura KMP, Weber MB. Periorbital Hyperchromia. Surg Cosmet Dermatol. 2011;3:233–9. [Google Scholar]
- 17.Lesourd BM. Nutrition and Immunity in the elderly: Modification of immune responses with nutritional treatments. Am J Clin Nutr. 1997;66:478S–484S. doi: 10.1093/ajcn/66.2.478S. [DOI] [PubMed] [Google Scholar]
- 18.Glick D, Barth S, Macleod KF. Autophagy: Cellular and molecular mechanisms. J Pathol. 2010;221:3–12. doi: 10.1002/path.2697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Diaz-Troya S, Perez-Perez ME, Florencio FJ, Crespo JL. The role of TOR in autophagy regulation from yeast to plants and mammals. Autophagy. 2008;4:851–65. doi: 10.4161/auto.6555. [DOI] [PubMed] [Google Scholar]
- 20.Payyappallimana U, Venkatasubramanian P. Exploring ayurvedic knowledge on food and health for providing innovative solutions to contemporary healthcare. Front Public Health. 2016;31:4–57. doi: 10.3389/fpubh.2016.00057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Choi SW, Friso S. Epigenetics: A new bridge between nutrition and health. Adv Nutr. 2010;1:8–16. doi: 10.3945/an.110.1004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Elsamanoudy AZ, Neamat-Allah MA, Mohammad FA, Hassanien M, Nada HA. The role of nutrition related genes and nutrigenetics in understanding the pathogenesis of cancer. J Microsc Ultrastruct. 2016;4:115–22. doi: 10.1016/j.jmau.2016.02.002. [DOI] [PMC free article] [PubMed] [Google Scholar]