

Abstract
Gas does not occur naturally in the cardiovascular system, although it is not unusual to identify it on imaging. The true incidence is difficult to know as asymptomatic cases are rarely recorded. In iatrogenic instance, this occurs when atmospheric air enters the cardiovascular system from a high to low pressure, or when gas is forcibly injected into a vessel. The source of air must be promptly identified and treatment must be expedited to reduce morbidity and mortality. This pictorial review aims to give an overview of the causes (with particular emphasis on the conditions that may be encountered by a Radiologist), appearances of cardiovascular gas, and any subsequent treatment.
Air or gas embolism
Venous gas
The presence of air in a closed system requires a connection between the gas and the vasculature with a pressure gradient to facilitate the flow. Venous gas is commonly iatrogenic from vascular access. Air buoyancy in a fluid medium results in bubbles rising to nondependent positions. Common sites include pulmonary artery, brachiocephalic vein, superior vena cava and right atrial appendage (Figure 1). Small locules get reabsorbed but physiological effects of larger volumes of air are similar to that of pulmonary embolism.
Figure 1.

Inadvertent introduction of air in the brachiocephalic vein (block arrow, left) due to insufficient line priming. ECG-gated cardiac CT angiogram (right) shows a small persistent locule (arrow) of air in the RA. RA, right atrium.
Incidence in radiology literature varies between 0.1 and 1% for embolism developed during central venous catheter manipulation (Figure 2),1 and 11–23%2 following contrast medium injection. With inappropriate priming, power injectors can deliver ≥400 ml air in <5 s. Infusion rate and speed, total amount of air, patient position and baseline health status determine the consequence. The volume of air required to cause death is approximately 200–300 ml; this is clinically important as 100 ml of air per second could flow through a 14-gauge needle with 5 cm pressure gradient.3 Complications can occur with as little as 20 ml of air, essentially the length of an unprimed i.v. infusion tubing.
Figure 2.
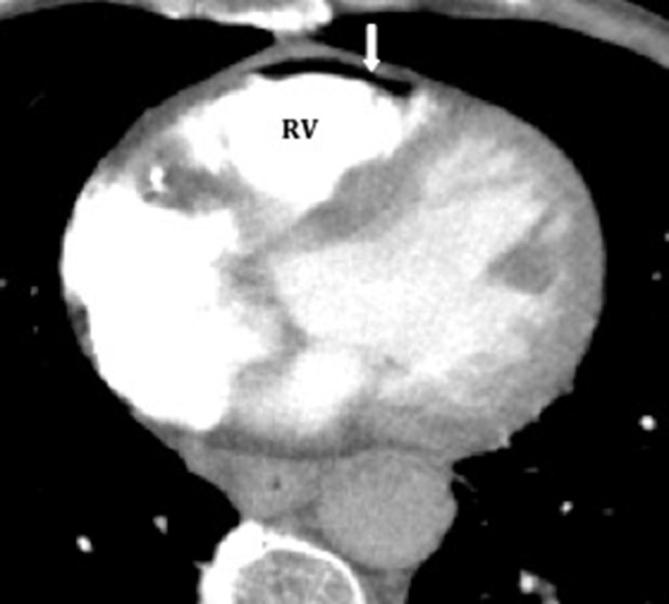
Air embolism in the RV and RVOT in a 37-year-old male following withdrawal of a central venous catheter. RV, right ventricle; RVOT, right ventricular outflow tract.
Neurosurgery is another common source of gas embolism, as many patients are operated in sitting posture. (Figure 3) Other high-risk procedures include but are not limited to cardiovascular surgery, endovascular and laparoscopic procedures.
Figure 3.

Cerebral air embolism in a 45-year-old female post spinal surgery. She became confused and disorientated following flushing of a central venous catheter in a sitting position.
Immediate symptoms include chest pain, dyspnea, headache and blurred vision. In severe cases, dysrhythmias and cardiac arrest will ensue.
If symptomatic, the patient should be placed in Trendelenburg position (head lower than feet) to discourage carotid artery propagation and left lateral decubitus (Durant’s maneuver) to displace the air to the right apex, and prevent further migration into pulmonary artery. High-flow 100% oxygen can correct hypoxemia and increases the diffusion gradient for bubble shrinkage. Hyperbaric oxygen promotes nitrogen absorption. Increased ambient pressure reduces bubble diameter to 82% (45% volume reduction), facilitating microcirculatory passage.4 Hyperbaric oxygen has clear benefit if instituted within 6 h but availability is limited to specialist centers. Supportive measures include colloid administration and inotropes to maintain end organ perfusion. Aspiration of air from the central line, cardiopulmonary resuscitation and chest massage should be instituted where appropriate.
Venous embolism has the potential to become arterial with catastrophic cardiac and neurological consequences. This is called paradoxical embolism, and happens when bubbles shunt at the pulmonary capillary level, or if there is an intracardiac shunt such as patent foramen ovale, atrial or ventricular septal defect. Gas does not normally travel across patent foramen ovales due to higher left atrial pressure but right to left shunting can occur with increasing right atrial pressure, e.g. pulmonary hypertension, hypotension, Eisenmenger syndrome (Figure 4).
Figure 4.

Air within the LV (white arrow) in a hypotensive male. The air was most likely introduced during injection of contrast medium and got in to the LV via a PFO which was difficult to see on this non-ECG-gated CT. Bubble ECHO in a different patient with a PFO (arrowhead). LV, left ventricle; PFO, patent foramen ovale.
Arterial gas
Arterial embolism is mostly iatrogenic from inadvertent injection. Necrotizing fasciitis is an aggressive soft tissue infection that can cause rapidly fatal epidermal to deep muscle destruction. (Figure 5). Intramural air in necrotizing gastroenteritis directly enters the pulmonary vein through inferior vena cava or indirectly from portal venous shunts. Subsequently, arterial entry is through microscopic right-left shunt. Aggressive infections with gas producing organisms has the potential to invade adjacent vasculature (Figure 6).
Figure 5.

Necrotising fascitis in an 80-year-old female with extensive intravascular air (left: block arrow IVC & arrowhead aorta; right: block arrow air in femoral veins). There is extensive muscle destruction in the left gluteus (star) & air tracking along the subcutaneous tissues on the right (thin arrow). IVC, inferior vena cava.
Figure 6.

A 77-year-old male with a large pre-sacral necrotic lesion (notched arrow, left panel) with bone destruction & vascular invasion. This was secondary to a colonic malignancy complicated by infection as well as left hydronephrosis and air in the left renal vein and IVC (arrow, right panel). IVC, inferior vena cava.
Decompression illness is associated with barotrauma-related arterial gas or bubbles from dissolved gas in the blood induced by environmental decompression.
Left atrial gas
Percutaneous left atrial ablation is a treatment for refractory atrial fibrillation. Ablation catheters are placed around the pulmonary vein in the posterior left atrial wall. Atrial-oesophageal fistulation is a rare complication (0.04%) of thermal injury with potential high fatality.5 (Figure 7) Early diagnosis is pivotal as assiduous treatment including stenting and/or surgical intervention is required.
Figure 7.

A 47-year-old male presented with sepsis and haemorrhagic stroke following radiofrequency ablation for atrial fibrillation. There is cerebral air embolism (black arrow, left panel) on Head CT and air (black arrow middle panel) within the LA on the initial thoracic CT. Few days later, an ECG-gated CT showed resorption of the LA air and a low attenuation tract between the oesophagus (white arrow—nasogastric tube) and LA in keeping with an atrio-oseophageal fistula. LA, left atrium.
A dreaded complication of percutaneous lung biopsy is systemic or left atrial air embolism with reported incidence of 0.02–0.21%.6 The biopsy needle open to atmospheric pressure can accidentally puncture pulmonary vein or form bronchovenous fistula. As little as 0.5–1.0 ml of pulmonary venous air can cause cardiac arrest from coronary air embolus.7
Pericardial gas
The pericardium is a true potential space and so, gas within the sac is uniformly lucent, changes with position and is limited by pericardial reflections. On radiographs, the cardiac silhouette is surrounded by a translucent rim with thin line of parietal pericardium (halosign) (Figure 8). Air does not extend above the aortic arch, a feature used to differentiate pneumopericardium from pneumomediastinum. Band of air outline the normally invisible parts of diaphragm, producing the continuous left hemidiaphragm sign. A sudden decrease of >2 cm in the cardiac silhouette or 32% reduction in cardiac size, (“small heart sign”) predicts impending tension pneumomediastinum. Clinical signs of pneumopericardium can occur with 60 ml of air with rapid entry compared to 500 ml without haemodynamic changes with gradual accumulation.8
Figure 8.

Pneumopericardium (notched black arrow) following cardiac surgery [note endotracheal tube, arrowhead & Swan-Ganz catheter (block arrow)].
Pneumopericardium is a rare complication of blunt and penetrating chest injury and usually self-limiting under 4 days to 2 weeks but delayed tension can occur in about 10%. Traumatic pneumopericardium is often associated with surgical emphysema and pneumomediastinum (Figure 9).
Figure 9.

A 22-year-old male with anterior penetrating stab wound. The sagittal image (left panel) shows the track of air (thin arrow) from the skin surface. The pericardial gas (white star) is causing tension pneumopericardium.
Iatrogenic procedures, e.g. pericardiocentesis, can introduce pericardial gas (Figure 10a) as can pericardiotomy meant to treat effusions (Figure 11). Pneumopericardium following cardiac surgery can be related to pneumothorax or barotrauma. Pyopneumopericardium occurs with infection by gas producing organisms (Figure 10b) or from fistulation, e.g. rupture of pyogenic lung abscesses. Propagation of malignant diseases in contiguous organs can create abnormal communication, e.g. gastropericardial fistulas.
Figure 10.

A (left): 55-year-old male with a large amount of air (black arrow) in a simple pericardial effusion (black star) following pericardiocentesis. b (Right): complex pericardial collection in a 47- year-old immunosuppressed male with enhancing parietal & visceral pericardium with locules of air secondary to streptococcal infection.
Figure 11.

Pericardial tamponade secondary to colonic herniation (block arrow) complicating a surgically created pericardial window, well demonstrated on a chest radiograph (left) and coronal CT (right).
Clinical progression varies from spontaneous resolution to tamponade. Treatment depends on the stability of the patient's condition. Tension pneumopericardium is treated similar to pericardial effusion, with a drain or pericardiotomy.
Portomesenteric gas
On CT, portal vein gas is seen as tubular branches of decreased attenuation extending to within 2 cm of the liver capsule. Mesenteric vein gas appears as low attenuation branches in the mesenteric bowel border. Commonest cause of portomesenteric gas is bowel ischaemia (Figure 12) but its presence in itself does not necessarily indicate mortality. Damage to the bowel wall (gas insufflation, ileus, trauma) can cause mucosal disruption, allowing intraluminal gas to become intravascular. In neonates, the presence of pneumatosis intestinalis, portal venous gas, or a combination is pathognomonic of necrotizing enterocolitis.
Figure 12.

A 87-year-old male with infarcted bowel complicated by extensive vascular gas (arrows: gas in portal vein (top left), SMV (top right), aorta (bottom left), SMA (bottom right), pulmonary artery (bottom left). Also note air within the spleen and left kidneys (arrowheads-top panel): (b) it is not entirely clear if the gas was within the wall of the right atrium or in the mid right coronary artery. An ECG-gated CT would have helped to characterise this further but the patient suffered a massive cardiac arrest and died shortly after the current CT. SMA, superior mesenteric artery; SMV, superior mesenteric vein.
Cavernous sinus gas
Cavernous sinus gas is generally an incidental finding on routine head CTs (Figure 13), secondary to air embolism from i.v. access and does not require treatment. In the context of trauma, sphenoid or skull base fracture need to be excluded.
Figure 13.

Incidental air in the cavernous sinus (block arrow) on an unenhanced CT head.
Gas containing implanted devices
Total artificial heart
Total artificial heart is an intricate mechanical circulatory support used as bridge to transplantation. Native ventricles are replaced by two polyurethane ventricles each with 70 ml stroke volume and occupy a volume of 400 cc within the chest.9 Native valves are replaced by mechanical single leaflet tilting discs to regulate flow direction. (Figure 14) The shape of the air-filled ventricles alters according to cardiac cycle, and should not be mistaken for pathological air collections or pneumomediastinum.
Figure 14.

Total artificial heart-echo (left) CT (middle), chest radiograph (right). Notched arrows represent the device within the right and left ventricles. Echocardiography elegantly demonstrates a strong reflection due to the difference in the acoustic impedance between the air and blood. Note the four prosthetic valves on the radiograph.
Intra-aortic balloon pump
Intra-aortic balloon pump is a circulatory assist device that works via counterpulsation, with balloon inflation during diastole to improve coronary circulation, and deflation pre-systole to reduce afterload. The 4 mm radiopaque marker tip should lie 2 cm above carina. The 25 cm long polyethylene balloon inflated with helium or carbon dioxide is visualised during diastole as a tubular lucency. (Figure 15). Common complication is malposition. If too high, the balloon can occlude arch vessels with risk of stroke or limb ischaemia. If too low, there is risk of renal and mesenteric arterial occlusion.
Figure 15.

IABP—white notched arrow within the Ao in a 75-year-old male following a large myocardial infarction. Middle panel—subsequently, the patient developed liver (black arrow) & gastric infarction (white arrow). Right panel is a different case with IABP and large volume of free air (white star) due to visceral perforation secondary to extensive gut ischaemia. Ao, aorta; IABP, Intra-aortic balloon pump.
Post-endovascular aneurysm repair (EVAR)
Endovascular aneurysm repair is a minimally invasive intervention for treating abdominal aortic aneurysms. Gas locules within the excluded aneurysm is common in the early post procedural CT and does not necessarily represent infection (Figure 16). Perigraft air is rare beyond 1 week but is not pathognomonic of infection until 4–7 weeks after surgery. Persistent perigraft fluid beyond 3 months is suspicious for infection. Aortoenteric fistula demonstrates ectopic gas, focal bowel wall thickening, contrast medium extravasation in to bowel lumen and paraprosthetic leakage of enteric contrast material.10
Figure 16.

A 75-year-old male with an endovascular stent graft. Note the peri-graft air bubble (notched arrow) within the aneurysm sac (Ao—aortic lumen). The differential includes stent graft infection and aorto-enteric fistula. However, in an asymptomatic patient, the air could be normal in the immediate post-procedural period. Courtesy of Dr Ilyas Shazad. Ao, aorta.
Conclusion
A wide variety of non-anatomical gas is frequently encountered in the cardiovascular system on imaging. Radiologists should be aware of common causes of gas and gas-containing devices within the cardiovascular system, and be confident with strategies to minimise iatrogenic gas within the imaging department, and also be aware of the management of the rare cases of symptomatic patients.
Contributor Information
Sze Mun Mak, Email: makszemun@doctors.org.uk.
Deepa Gopalan, Email: deepa.gopalan@btopenworld.com.
REFERENCES
- 1. Vesely TM. Air embolism during insertion of central venous catheters. J Vasc Interv Radiol 2001; 12: 1291–5. doi: 10.1016/S1051-0443(07)61554-1 [DOI] [PubMed] [Google Scholar]
- 2. Sodhi KS, Das PJ, Malhotra P, Khandelwal N. Venous air embolism after intravenous contrast administration for computed tomography. J Emerg Med 2012; 42: 450–1. doi: 10.1016/j.jemermed.2009.11.025 [DOI] [PubMed] [Google Scholar]
- 3. Orebaugh SL. Venous air embolism: clinical and experimental considerations. Crit Care Med 1992; 20: 1169–77. [DOI] [PubMed] [Google Scholar]
- 4. Edsell ME, Kirk-Bayley J. Hyperbaric oxygen therapy for arterial gas embolism. Br J Anaesth 2009; 103: 306–7. doi: 10.1093/bja/aep186 [DOI] [PubMed] [Google Scholar]
- 5. Martinek M, Bencsik G, Aichinger J, Hassanein S, Schoefl R, Kuchinka P, et al. Esophageal damage during radiofrequency ablation of atrial fibrillation: impact of energy settings, lesion sets, and esophageal visualization. J Cardiovasc Electrophysiol 2009; 20: 726–33. doi: 10.1111/j.1540-8167.2008.01426.x [DOI] [PubMed] [Google Scholar]
- 6. Ibukuro K, Tanaka R, Takeguchi T, Fukuda H, Abe S, Tobe K. Air embolism and needle track implantation complicating CT-guided percutaneous thoracic biopsy: single-institution experience. AJR Am J Roentgenol 2009; 193: W430–W436. doi: 10.2214/AJR.08.2214 [DOI] [PubMed] [Google Scholar]
- 7. Goldfarb B, Bahnson HT. Early and late effects on the heart of small amounts of air in the coronary circulation. J Thorac Cardiovasc Surg 1980; 80: 708–17. [PubMed] [Google Scholar]
- 8. MAURER ER, Mendez FL, Finklestein M, Lewis R. Cardiovascular dynamics in pneumopericardium and hydropericardium. Angiology 1958; 9: 176–179. doi: 10.1177/000331975800900306 [DOI] [PubMed] [Google Scholar]
- 9. Tang DG, Shah KB, Hess ML, Kasirajan V. Implantation of the syncardia total artificial heart. J Vis Exp 2014; 89. doi: 10.3791/50377 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Orton DF, LeVeen RF, Saigh JA, Culp WC, Fidler JL, Lynch TJ, et al. Aortic prosthetic graft infections: radiologic manifestations and implications for management. Radiographics 2000; 20: 977–93. doi: 10.1148/radiographics.20.4.g00jl12977 [DOI] [PubMed] [Google Scholar]