

Abstract
Objective:
We explored whether abortion attitudes differed by respondents’ sex and country-level abortion policy context.
Methods:
Data were collected between 2010 and 2014 from 69,901 respondents from 51 countries. Abortion attitudes were scored on a ten-point Likert scale (1=“never justifiable”; 10=“always justifiable”). Country-level abortion policy context was dichotomized as “less restrictive” or “more restrictive.” We conducted linear regression modeling with cluster effects by country to assess whether respondents’ sex and abortion policy context were associated with abortion attitudes, controlling for sociodemographic characteristics.
Results:
On average, women had more supportive abortion attitude scores than men (Mean=3.38 SD=2.76 versus Mean =3.24 SD=2.82, p<0.001). Respondents in countries with more restrictive policy contexts had less supportive attitudes than those in less restrictive contexts (Mean=2.55 SD=2.39 versus Mean=4.09 SD=2.96, p<0.001). In regression models, abortion attitudes were more supportive among women than men (b=0.276, p<0.001) and in less restrictive versus more restrictive countries (b=0.611, p<0.001). Younger, educated, divorced, non-religious, and employed respondents had more supportive scores (all p<0.05).
Conclusions:
Systematic differences were observed in attitudes toward abortion by respondents’ sex and policy context. Promoting gender equity and the legality of safe abortion across populations and settings may increase acceptance of abortion in both sexes worldwide.
Keywords: Autonomy, attitudes, beliefs, gender differences, reproductive health
Introduction
Approximately 40% of the 213 million pregnancies that occurred worldwide in 2012, or 85 million pregnancies, were unintended (G Sedgh, Singh, and Hussain 2014). Unintended pregnancy has been associated with significant health and social consequences for women, their families, and society (Finer and Zolna 2011; Singh, Sedgh, and Hussain 2010). Some research has suggested that women who experience unintended pregnancy are at increased risk for depression, anxiety, intimate partner violence, and maternal mortality, and offspring are at increased risk of inadequate healthcare, insufficient nutrition, and infant and child mortality (Korenman, Kaestner, and Joyce 2015). The social consequences of unintended pregnancy are also significant - with women facing stigmatization from their families and communities, curtailed education and employment opportunities, and increased poverty (Bankole and Malarcher 2010; Molina et al. 2010; Hindin 2012).
For many women, induced abortion can be an effective way to manage unintended pregnancy and the significant health and social risks associated with it. Induced abortion has been defined as “the intentional termination of a pregnancy by medical or surgical means before the fetus can be viable” (Cunningham et al. 2013). Indeed, the induced abortion rate in 2012 was 35 induced abortions per 1,000 women of reproductive age (15 to 44 years) (Gilda Sedgh et al. 2016). While the abortion incidence rate has decreased in developed countries in North America and Europe, the rate remains unchanged in developing country contexts, which often have restrictive abortion laws (Gilda Sedgh et al. 2016). Even where abortion is illegal, it is clandestinely practiced; approximately 40% of women who need post abortion care related to unsafe abortion do not seek it (Gilda Sedgh et al. 2016). Even so in 2012, approximately 6.9 million women sought care for abortion complications (Gilda Sedgh et al. 2016). Reasons that women give for seeking abortion include financial or material constraints, timing of the pregnancy, partner factors, and a need to focus energy and resources on existing children (Biggs, Gould, and Foster 2013; Kirkman et al. 2009). Where abortion is safe and legal, negative outcomes are rare, with no evidence of long-term mental or physical health morbidity (Charles et al. 2008; Biggs et al. 2014; Raymond and Grimes 2012). Thus, for some women, unintended pregnancy may be best resolved with a safe induced abortion. In fact, findings from the Turn Away study indicate that in many cases, women who received desired abortions were better off than women who refused abortions (Roberts et al. 2014; D. Foster et al. 2015; D. G. Foster et al. 2018). For example, research from this study showed that those who received abortions had lower rates of intimate partner violence, better mental health symptoms shortly following the clinic visit, and improved economic standing compared to those turned away (Roberts et al. 2014; D. Foster et al. 2015; D. G. Foster et al. 2018). However, unsafe abortion, defined as “a procedure for terminating a pregnancy performed by persons lacking the necessary skills or in an environment not in conformity with minimal medical standards or both”, contributes to maternal mortality, infertility, and reproductive morbidity (Gipson, Koenig, and Hindin 2008; Gerdts et al. 2015; Ganatra, Tunçalp, and Bart 2014). Despite limitations in available estimation methods, maternal mortality attributable to unsafe abortion persists despite advances in access to medication abortion (Gerdts et al. 2015).
Women may experience barriers to safe abortion access at multiple levels. At the individual level, behavioral theory would suggest that women’s attitudes, perceived norms, and knowledge of abortion may prevent them from considering and pursuing it as an option (Montano and Kasprzyk 2008). Pregnancy termination may be against women’s personal, moral and religious beliefs. Thus, while women’s attitudes toward abortion, including their own and/or those of others in their community, have not been systematically described, attitudes likely have implications for abortion decisions, service seeking, other behaviors, and experiences. Some research, for instance, has shown that a woman’s abortion attitudes are related to the type of procedure that she elects, with women having negative attitudes opting against a surgical procedure (Kerns et al. 2012). The majority of existing studies have focused on abortion attitudes in the clinical setting; however, little is known about women’s abortion attitudes at the population level. Additionally, potential differences in abortion attitudes by samples, contexts, and sociodemographic groups across the world have been understudied.
At the interpersonal level, pervasive gender roles and existing power imbalances in regards to couples’ reproductive decision-making may contribute to sex-based differences in abortion attitudes. Unintended pregnancy resolution disagreements can result in partner violence, denial of the pregnancy, and withdrawal of financial support in global settings including Ghana and Uganda (Silverman et al. 2010; Moore, Jagwe-Wadda, and Bankole 2011; Schwandt et al. 2013). Disparities in abortion acceptability among men and women may ultimately preclude women from pursuing pregnancy termination, achieving reproductive autonomy, and fulfilling their desired fertility. Existing research has shown inconclusive results surrounding differences in abortion attitudes by sex of respondent (Begun and Walls 2015; Barkan 2014). While much of the existing, older literature shows that sex differences in abortion attitudes are not significant, Hertel and Russell (2007) showed differences in abortion attitudes by sex in the United States when controlling for the employment status of the woman (Hertel and Russell 2007; Misra 1998). However, it remains an important question, and potential differences in abortion attitudes among men and women across the world have not been systematically examined.
Finally, from macrosocial perspective, abortion is legally restricted and socially and culturally unaccepted in many places worldwide. Restrictive policies and negative social norms concerning abortion serve as structural barriers – leaving women without access to safe, skilled providers and in fear of imprisonment (G Sedgh et al. 2015; Harries et al. 2015), with limited, risky options to resolve their pregnancy through unsafe abortion or unwanted childbirth and to bear the consequences of social stigma (Cockrill and Nack 2013; Levandowski et al. 2012; Shellenberg et al. 2011). Some research has shown that abortion stigma is associated with non-disclosure of unintended pregnancy and abortion, delayed or lack of care-seeking for post-abortion complications, and use of unsafe abortion services, despite the availability of safer, legal options (Shellenberg et al. 2011). The broader sociopolitical contexts of abortion likely affect women’s (and men’s) individual attitudes and experiences, though the influence of sociopolitical contexts on abortion attitudes worldwide is not well understood.
We conducted a global comparison of abortion attitudes among a multi-country sample of women and men across the world and examined factors associated with abortion attitudes. This research was conceptually guided by a socio-ecological model that suggest that individual, interpersonal and macrosocial influences affect an individual’s attitudes towards abortion. The aim of this study was to examine whether significant differences existed in abortion attitudes by the sex of the respondent. We hypothesized that, at a global level, women would be more accepting of abortion than men. In addition, we investigated whether the abortion policy context of a country was associated with respondents’ abortion attitudes. We hypothesized that more restrictive countries would have less accepting respondents compared to countries where abortion was more accessible.
Methods
Study Sample
Data were drawn from the sixth wave of the World Values Survey (WVS), a world-wide assessment of values and their effect on social and political life (“World Values Survey: Fieldwork and Sampling” 2015). The WVS is a global initiative, based in Sweden but dependent on the efforts of a network of global scholars and social scientists (“World Values Survey: Fieldwork and Sampling” 2015). This multi-national survey used a common questionnaire to collect data on a wide variety of values, including economic development, democratization, women’s status and gender roles, perceived well-being, religion, and social capital/social support (“World Values Survey: Fieldwork and Sampling” 2015). The WVS has been conducted since 1981 and has collected nationally representative data from individuals in countries comprising over 90% of the world’s population (“World Values Survey: Fieldwork and Sampling” 2015). Currently, the WVS has collected information from over 400,000 respondents and is the largest time series investigation of people’s attitudes and values to date (“World Values Survey: Fieldwork and Sampling” 2015)
Approximately 30 randomly selected primary sampling units (PSUs) were identified for data collection within a given country. Within these PSUs, participants age 18 years or above were randomly sampled from the entire population of those who were 18 years of age or above or by a quota sample (if PSUs were probabilistically generated and clusters are small) (“World Values Survey: Fieldwork and Sampling” 2015). The survey was then implemented by a local professional data collection team, and interviews are either collected face-to-face or by telephone if the respondent was not physically accessible (“World Values Survey: Fieldwork and Sampling” 2015). Each local Principal Investigator (PI) was responsible for oversight of the data collection process, for ensuring that the data collection procedures followed the protocol and that the data were sufficiently clean (“World Values Survey: Fieldwork and Sampling” 2015). All participants provided informed consent for their participation in the survey. The present analyses represent a secondary analysis of this de-identified and publicly available dataset and was therefore determined by the IRB at the University of Michigan to be “not-regulated” (eresearch ID: HUM00130989).
Wave six of data collection occurred between 2010 and included face-to-face interviews with 74,042 men and women ages 18 years and older in fifty-two countries. Approximately 1,000 participants were selected in each participating country, and as previously mentioned, stratified random sampling was used to ensure nationally representative samples (“World Values Survey: Fieldwork and Sampling” 2015). The WVS did not report response rates by country. For our analysis, we excluded respondents with incomplete data on abortion attitudes (n=4,141), our primary outcome of interest. Our final analytic sample comprised 69,901 men and women from fifty-one countries.
Measures
Abortion attitudes:
Our primary outcome of interest was measured as respondents’ beliefs about whether abortion is justifiable via a single WVS item: “Please tell me for each of the following actions (abortion), whether you think it can always be justified, never be justified, or something in between.” The response options ranged from 1 (never justifiable) to 10 (always justifiable). We treated abortion attitudes as a continuous measure because it lacked Likert anchors and because this treatment was consistent with that of other authors who have used the same variable (Ted G Jelen 2015).
Country-level abortion policy context:
Using the classification system developed by the Guttmacher Institute (Singh et al, 2009), respondents’ countries were coded for the level of abortion policy restriction using an ordinal scale from 0 to 5: 0=Prohibited altogether (no explicit exceptions); 1=To save the life of the woman; 2=To preserve physical health (or save the life of the woman); 3=To preserve mental health (or any of the previous reasons); 4=Socioeconomic grounds (and all of the above reasons); 5=Without restriction as to reason (although gestational limits may be imposed). In analyses, we examined the abortion policy context as a country-level independent variable in several ways (e.g., ordinal, continuous, dichotomous). We conducted sensitivity analyses using different treatments of this variable. Results were similar; so, we present the dichotomized measure to reflect contexts where abortion was more restricted (0–3) versus less restricted/liberal (4–5). This dichotomous treatment provides a more straightforward interpretation of the effects of policy environment.
Gender equality in education:
We included a measure of the respondent’s attitudes towards gender equality in education as a proxy indicator for the respondent’s general views on gender equality. Respondents were asked about their level of agreement with the following statement: “A university education is more important for a boy than for a girl.” Response options included strongly agree, agree, disagree, and strongly disagree. This was treated as a categorical variable with strongly agree as the reference group.
Respondents’ Sex and Sociodemographic Characteristics:
Respondents’ sex, recorded by the interviewer as male or female, was also treated as a key independent variable. Additional sociodemographic factors examined as covariates included: age (continuous), educational attainment (categorical: no formal education [reference group], some or completed primary, some or completed secondary technical, some or completed secondary, and some or completed university), marital status (categorical: married [reference group], unmarried/single, living together, and divorced, separated, or widowed), religiosity (categorical: importance of religion in life: very important [reference group], rather important, not very important, and not at all important), and employment (categorical: full time, part time, or self employment [reference group], retired, housewife, student, unemployed, and other).
Analysis
We used descriptive statistics to describe the sample and summarize abortion attitudes and Student’s independent t-tests and oneway ANOVA to examine differences in abortion attitudes by policy context, sex, and other covariates. We conducted multiple linear regression modeling to examine relationships while accounting for cluster effects at the country level. We also examined multi-level models with country-level random intercepts and slopes. Primary results were similar across models; we present models with cluster effects. Finally, we also examined models stratified by abortion policy context (less restrictive versus more restrictive). All available sociodemographic covariates were considered for inclusion in regression models, given their theoretical and statistical relevance. All theoretically important variables (age, sex, employment, educational attainment, religiosity, marital status, gender equality in education, and abortion policy restriction) were included in bivariate and multivariable models. Bivariate results are presented as weighted means (M) with standard deviations (SD) and p-values (p). Multivariable results are presented as adjusted beta coefficients (B) with 95% confidence intervals (CI). P-values were considered significant with two-tailed tests at <0.05. We applied survey weights and used the SVY series of commands in STATA 13 (College Station, TX) to account for the complex sampling and survey design. We selected this as the most appropriate treatment of the data because the clustered treatment of the data requires fewer assumptions than hierarchical linear modeling and because we did not have additional covariates at the country level (Primo and Jacobsmeier 2007).
Results
Characteristics of the sample
The mean age of the respondents was 42 years (range 16–99 years, SD 16.67 years) (Table 1). The sample comprised higher proportions of respondents who were female (52.3%), had any education (95.2%), and were married (56.5%). Half of respondents (49.4%) reported that religion was very important to them, and 55.3% reported that they were employed.
Table 1:
Sociodemographic characteristics of the sample (n=69,901)
| Mean | SD | % | n | |
|---|---|---|---|---|
| Age, years | 42.15 | 16.67 | ||
| Female | 52.33 | 36,558 | ||
| Education | ||||
| No formal education | 4.85 | 3,360 | ||
| Some or completed primary education | 15.60 | 10,802 | ||
| Some or completed secondary technical education | 27.16 | 18,808 | ||
| Some or completed secondary education | 24.66 | 17,082 | ||
| Some or completed university education | 27.73 | 19,205 | ||
| Marital status | ||||
| Married | 56.51 | 39,399 | ||
| Unmarried/single | 24.95 | 17,394 | ||
| Living together as married | 6.40 | 4,465 | ||
| Divorced or separated | 5.99 | 4,175 | ||
| Widowed | 6.15 | 4,285 | ||
| Religiosity | ||||
| Very important | 49.36 | 34,053 | ||
| Rather important | 20.87 | 14,395 | ||
| Not very important | 17.12 | 11,812 | ||
| Not at all important | 12.65 | 8,724 | ||
| Employment Status | ||||
| Working full time, part time, or self employed | 55.27 | 38,499 | ||
| Retired | 12.71 | 8,854 | ||
| Housewife | 14.88 | 10,367 | ||
| Student | 7.80 | 5,436 | ||
| Unemployed | 7.92 | 5,515 | ||
| Other employment status | 1.41 | 983 | ||
| Gender equality in education: A university education is more important for a boy than for a girl | ||||
| Strongly agree | 9.48 | 6,477 | ||
| Agree | 14.15 | 9,668 | ||
| Disagree | 45.17 | 30,856 | ||
| Strongly disagree | 31.19 | 21,307 | ||
| Abortion policy restrictions | ||||
| More restrictive | 49.15 | 33,867 | ||
| Less restrictive | 50.85 | 35,045 | ||
Age: n=69,792; Female: n=69,866; Education: n=69,257; Marital status: n=69,718; Religiosity: n=68,984; Employment: n=69,654; Gender equality in education: n=68,308, Abortion policy restriction: n=68,912
Half (49.2%) lived in countries where abortion was more restricted, including places where it was prohibited altogether, legal to save the life of the woman, and legal to preserve the physical and/or mental health of the woman (Figure 1).
Figure 1:
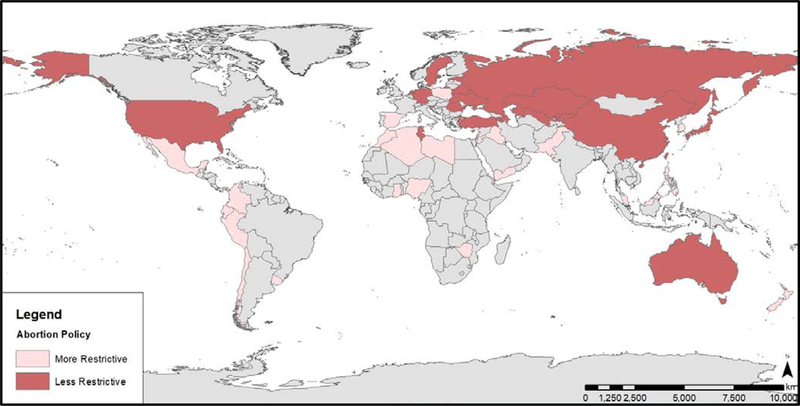
World Values Survey Countries by Abortion Policy
Associations between abortion attitudes, respondents’ sex, and abortion policy context
The mean abortion attitudes score for the sample was 3.31 (SD 2.80, range 1–10). Abortion attitude scores differed by sex of the respondent (p<0.05), with males having less supportive attitudes (Mean=3.24, SD=2.76) than females (Mean=3.38, SD=2.82) (Table 2). Also, significant differences were observed in mean abortion score by the respondent’s views on gender equality in education (p<0.05). Those who strongly agreed that university education was more important for boys had a mean score of 2.46 (SD=2.32) compared to a mean score of 3.77 (SD=3.08) for those who strongly disagreed. (Table 2). Abortion attitude scores also differed by abortion policy context (Table 2), with respondents living in more restrictive countries having less supportive attitudes (Mean=2.55, SD=2.39) than those in living in less restrictive countries (Mean=4.09, SD=2.96) (p<0.05). For instance, respondents from Sweden had the most supportive views of abortion (Mean=8.0) while those in Pakistan believing that it was rarely justifiable (Mean=1.52) (Figure 2). When stratified by country-level policy context (less versus more restrictive), differences in abortion attitudes by sex of the respondent were noted for fifteen countries (Figure 3). In most countries, women were more supportive of abortion than men, but in the Netherlands, Spain, and Trinidad and Tobago, the opposite trend was noted. Additionally, there were significant differences in mean abortion attitude scores by education, marital status, and religiosity (p<0.001) (Table 2).
Table 2:
Unadjusted associations between abortion attitude scores and sociodemographic characteristics
| n | Mean abortion attitude score | Standard Deviation | p-value | |
|---|---|---|---|---|
| Age group, years | <0.001 | |||
| 17 to 19 | 4,698 | 3.08 | 2.73 | |
| 20 to 29 | 15,253 | 3.07 | 2.66 | |
| 30 to 39 | 14,283 | 3.22 | 2.73 | |
| 40 to 49 | 12,618 | 3.35 | 2.83 | |
| 50 to 59 | 10,301 | 3.54 | 2.87 | |
| 60 to 69 | 7,468 | 3.65 | 2.95 | |
| 70+ | 5,280 | 3.50 | 2.84 | |
| Gender | <0.001 | |||
| Male | 33,308 | 3.24 | 2.76 | |
| Female | 36,558 | 3.38 | 2.82 | |
| Education | <0.001 | |||
| No formal education | 3,360 | 2.06 | 1.97 | |
| Some or completed primary | 10,802 | 2.70 | 2.53 | |
| Some or completed secondary technical | 18,808 | 3.19 | 2.72 | |
| Some or completed secondary | 17,082 | 3.35 | 2.76 | |
| Some or completed university | 19,205 | 3.92 | 2.98 | |
| Marital status | <0.001 | |||
| Married | 39,399 | 3.17 | 2.71 | |
| Unmarried/single | 17,394 | 3.28 | 2.78 | |
| Living together as married | 4,465 | 4.09 | 3.18 | |
| Divorced or separated | 4,175 | 4.12 | 3.03 | |
| Widowed | 4,285 | 3.14 | 2.64 | |
| Religiosity | <0.001 | |||
| Very important | 34,053 | 2.30 | 2.18 | |
| Rather important | 14,395 | 3.44 | 2.62 | |
| Not very important | 11,812 | 4.52 | 2.91 | |
| Not at all important | 8,724 | 5.37 | 3.18 | |
| Employment | <0.001 | |||
| Full time, part time or self-employed | 38,499 | 3.45 | 2.84 | |
| Retired | 8,854 | 3.56 | 2.83 | |
| Housewife | 10,367 | 2.80 | 2.56 | |
| Student | 5,436 | 3.25 | 2.77 | |
| Unemployed | 5,515 | 2.95 | 2.68 | |
| Other employment status | 983 | 3.38 | 2.86 | |
| A university education is more important for a boy than for a girl | <0.001 | |||
| Strongly agree | 6,477 | 2.46 | 2.32 | |
| Agree | 9,668 | 2.87 | 2.42 | |
| Disagree | 30,856 | 3.30 | 2.73 | |
| Strongly disagree | 21,307 | 3.77 | 3.08 | |
| Abortion policy restriction | <0.001 | |||
| More restrictive | 33,867 | 2.55 | 2.39 | |
| Less restrictive | 35,045 | 4.09 | 2.96 | |
Results are from unadjusted Student’s T-tests and one way ANOVA comparisons of mean abortion attitude scores. P-values significant at p<0.05.
Sub-samples based on missing data: Age: n=69,792; Female: n=69,866; Education: n=69,257; Marital status: n=69,718; Religiosity: n=68,984; Employment: n=69,654; Gender equality in education: n=68,308, Abortion policy restriction: n=68,912
Figure 2: Unadjusted mean abortion scores for the countries in the WVS.
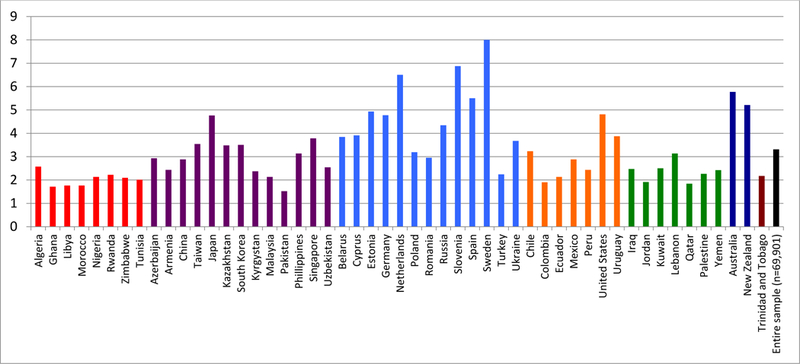
WVS = World Values Survey. *Mean abortion attitude score on scale of 1 (never justifiable) to 10 (always justifiable). Mean scores range from 1.52 (Pakistan) to 8.00 (Sweden).
Figure 3:
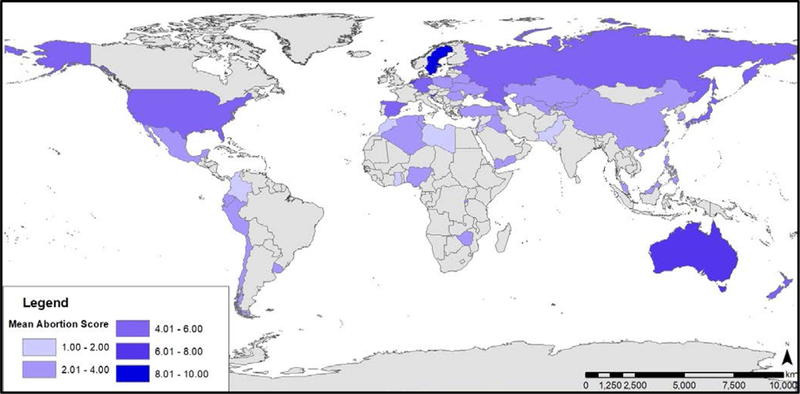
Unadjusted mean abortion scores presented by country
In multivariable regression models, respondents’ sex, abortion policy context, and all sociodemographic covariates remained significantly associated with abortion attitudes (Table 3). Women were more accepting of abortion than men and had, on average, an attitude score that was 0.210 points higher than men (95% CI 0.163, 0.256, p<0.001). This was true even when controlling for attitudes about gender equality in education, which was also associated with abortion attitudes. Compared to those who strongly agreed that university education is more important for boys, respondents who strongly disagreed had abortion attitudes scores that were, on average, 0.607 points higher (95% CI 0.535, 0.679, p<0.001). Respondents living in less restrictive abortion policy contexts had 0.646-point higher abortion attitude scores than those living in more restrictive contexts (95% CI 0.545, 0.692, p<0.001). Increasing age (B=0.014) and educational attainment were associated with more favorable abortion attitudes. Compared to respondents who thought religion was very important, decreasing level of religiosity was associated with higher scores (range B=0.794 to B=2.492 , Table 3, p-values<0.001). Compared to married respondents, those who were unmarried/single, cohabiting, or divorced/separated had higher attitude scores (range B=0.301 to B=0.539, p-values<0.001) while widowed respondents had lower scores (B=−0.236, p<0.001). Finally, compared to respondents who were employed, those who were retired, housewives, and unemployed had lower abortion attitude scores (range B=−0.286 to B=−0.134, p-values<0.001).
Table 3:
Multivariable linear regression model of sociodemographic factors associated with abortion attitude scores (n=68,222 in 50 countries*)
| Variable | Coefficient | SE | p | 95% Confidence Interval |
|
|---|---|---|---|---|---|
| LB | UB | ||||
| Age | 0.014 | 0.001 | <0.001 | 0.012 | 0.016 |
| No formal education | Reference | ||||
| Some or completed primary | 0.189 | 0.045 | <0.001 | 0.101 | 0.276 |
| Some or completed secondary- technical | 0.371 | 0.043 | <0.001 | 0.287 | 0.456 |
| Some or completed secondary | 0.422 | 0.044 | <0.001 | 0.335 | 0.510 |
| University level education | 0.831 | 0.044 | <0.001 | 0.744 | 0.918 |
| Male | Reference | ||||
| Female | 0.210 | 0.024 | <0.001 | 0.163 | 0.256 |
| Married | Reference | ||||
| Unmarried/single | 0.301 | 0.031 | <0.001 | 0.239 | 0.362 |
| Cohabitating | 0.611 | 0.047 | <0.001 | 0.519 | 0.703 |
| Divorced or Separated | 0.539 | 0.050 | <0.001 | 0.442 | 0.636 |
| Widowed | −0.236 | 0.047 | <0.001 | −0.328 | −0.143 |
| Religion very important | Reference | ||||
| Religion rather important | 0.794 | 0.028 | <0.001 | 0.739 | 0.849 |
| Religion not very important | 1.698 | 0.033 | <0.001 | 1.633 | 1.763 |
| Religion not at all important | 2.492 | 0.040 | <0.001 | 2.412 | 2.572 |
| Full time, part time, or self -employed | Reference | ||||
| Retired | −0.286 | 0.041 | <0.001 | −0.366 | −0.205 |
| Housewife | −0.138 | 0.033 | <0.001 | −0.204 | −0.073 |
| Student | −0.001 | 0.045 | 0.980 | −0.089 | 0.087 |
| Unemployed | −0.134 | 0.039 | 0.001 | −0.211 | −0.057 |
| Other | −0.092 | 0.087 | 0.292 | −0.263 | 0.079 |
| Strongly agree boy’s education more important | Reference | ||||
| Agree | 0.090 | 0.040 | 0.026 | 0.011 | 0.169 |
| Disagree | 0.240 | 0.035 | <0.001 | 0.172 | 0.308 |
| Strongly disagree | 0.607 | 0.037 | <0.001 | 0.535 | 0.679 |
| More restrictive abortion policy | Reference | ||||
| Less restrictive abortion policy | 0.646 | 0.024 | <0.001 | 0.545 | 0.692 |
Results are from multivariable linear regression models of abortion attitude scores and include a country level cluster effect. Results presented as adjusted beta coefficients with standard errors, p-values, and 95% confidence intervals (UB = upper bound, LB = lower bound). P-values significant at alpha <0.05.
Palestine not included due to lack of available abortion policy data
Finally, in models stratified by abortion policy context, sex differences and other sociodemographic factors associated with abortion attitudes remained similar across less restrictive and more restrictive countries (results not shown). Findings were also consistent in multi-level models with random effects at the country level.
Discussion
Attitudes toward abortion likely operate across all levels of women’s environments and shape women’s experiences with pregnancy decision-making and (adverse) reproductive health outcomes. To date, population- and multi-level studies on abortion attitudes have been scarce, especially those accounting for potential differences among women and men, by country, and sociopolitical climate. In our multi-national study of women and men in the World Values Survey, differences in abortion attitudes by sex of the respondent were notable and existed across countries and policy contexts - both where abortion is and is not heavily restricted. In general, women were more supportive of abortion than men, even after controlling for important covariates like education, age, religiosity, and employment. These findings are consistent with some older research on abortion attitudes in the United States as well as more recent work that has identified religiosity as a suppressor variable in studies of sex-based differences in abortion attitudes (Hertel and Russell 2007; Barkan 2014).
Recent studies in Sub-Saharan Africa complement the findings from this study related to gendered abortion attitudes. Findings from South Africa and Uganda suggest that males have more negative views of abortion than women and that in some cases, men’s negative attitudes toward abortion can serve as barriers to safe abortion and post-abortion care (Moore, Jagwe-Wadda, and Bankole 2011; Patel and Kooverjee 2009). In addition, males in the South African study reported wanting to be more involved in abortion decision-making, suggesting a desire to limit women’s autonomy in this realm (Patel and Johns 2009; Patel and Kooverjee 2009). Moreover, research on pregnancy coercion and birth control sabotage has shown that different fertility intentions among partners with inequitable power dynamics can result in a loss of women’s reproductive control and put women at risk for unintended pregnancy (Miller et al. 2010). While the results of the present study did not investigate male desires to be involved in abortion decisions or their intentions to limit autonomy, these findings provide important directions for future research. Taken together, the global phenomenon of low male acceptance of abortion highlighted in our study and low male involvement in family planning and pregnancy decision-making generally appear to be an important area for further research on women’s access to abortion services.
Notably, we did find several interesting country-level exceptions to trends in abortion attitudes by respondents’ sex. Liberal sociopolitical and cultural norms around sexual and reproductive health broadly and abortion specially have been well-documented in Northern Europe (e.g. Netherlands) and to a lesser extent western Europe (e.g. Spain). However, it is unclear why men in the Trinidad and Tobago would be more supportive than their female counterparts, and abortion has been relatively understudied in this setting. Interestingly, like other researchers, we did find a wide range of other sociodemographic factors associated with abortion attitudes. It is likely that these associations vary considerably at the country level, although the data were not well suited to test such differences across individual countries (Misra 1998; Carter, Carter, and Dodge 2009; Hertel and Russell 2007; Patel and Johns 2009). For example, age, urban/rural location, religiosity, race, household income, workforce participation, and educational attainment are all likely highly correlated (and may even interact with) with differences in abortion attitudes by sex within countries (Misra 1998; Carter, Carter, and Dodge 2009; Hertel and Russell 2007; Patel and Johns 2009). Additional research is needed to provide a more nuanced understanding of country-specific factors affecting attitudes toward abortion for women and men across the globe.
At the macrosocial level, respondents in our study from less restrictive abortion policy contexts were more accepting of abortion than those in countries where abortion was heavily restricted. From a sociopolitical perspective, abortion stigma has been more pronounced in countries where abortion is highly restricted compared to countries where it is less restricted (Shellenberg et al. 2011). In Shellenberg et al’s qualitative work, restrictive state policies translated to negative community norms around abortion, which in turn was related to individuals’ attitudes and belief systems (Shellenberg et al. 2011). Abortion is a contentious issue that motivates political engagement, including voting behavior, and ultimately the population’s representation in government (T. G. Jelen and Wilcox 2003); public opinion is an important component of policy development and reform. Thus, more accepting societies are those in which abortion services are legally available and where women are not forced to pursue unsafe options and risk their health and lives. In many cases, grassroots feminist movements drive changes in cultural climates and abortion policies (Klugman and Budlender 2001). Public health and medical professionals are also important players in cultural change and in promoting safe and legal access to abortion care.
The various other demographic and psychosocial factors we measured and treated as covariates were also highly associated with abortion attitudes among this sample. Our results were generally consistent with other research demonstrating differences in abortion attitudes across different age, educational attainment, marital status, religiosity and employment groups. We found that for each category of increased education, respondent abortion attitudes are, on average, more favorable, for example, with a nearly a one-point increase (B=0.831) in abortion attitudes among university educated respondents to those with no formal education. Others have reported more accepting abortion attitudes with higher levels of education (Mosley et al. 2017). Additionally, religiosity and abortion attitudes has been widely studied (Adamczyk and Valdimarsdóttir 2018; Patel and Johns 2009; Barkan 2014; Begun et al. 2016). In the US context, Adamczyk and Valdimarsdóttir (2018) found that both individual level religiosity and the religiosity of one’s geographic location affect the individual’s attitudes towards abortion. In fact, as the religiosity of an individual’s county increases, both religious and secular individuals become more conservative (anti-abortion) in their views. Our World Values Survey analysis found the same trend but did not provide measures of community or country-level religiosity. Finally, we noted a relationship between employment status and abortion attitudes, with employment (full-, part-time or self) being associated with more positive abortion attitudes. Jelen and colleagues (2002) also showed that employment status was an effect modifier in the relationship between respondent sex and abortion attitudes in their U.S. sample, with women who stayed home having very low acceptance for abortion compared to employed men and women (Ted G Jelen, Damore, and Lamatsch 2002). Research is needed to test the robustness of employment as an effect modifier between respondent sex and abortion attitudes in global settings.
Beyond sociodemographic differences though, the role of the education-related gender equality in influencing abortion attitudes appeared to be salient and is a factor potentially highly relevant to male-female attitude differences. We found more favorable attitudes toward abortion among respondents who strongly agreed that a boy’s education is more important than a girl’s, compared to those who less strongly agreed, with an almost linear effect of declining levels of agreement. However, our main effects of sex on abortion attitudes were consistent even after controlling for this gender education equality variable, which would suggest that our findings are likely not solely attributed to gender norm differences. In fact, we did not measure gender identify, rather we were limited to a traditional survey item on biological sex. Future studies consider more domains and measures of attitudes towards gender, gender norms, and gender equality, for instance equality in employment, political leadership, household decision-making, and reproductive decision making, as they may relate to beliefs about abortion.
Our study had a number of limitations. First, while our research was guided by a social-ecological model, our final model did not employ a formal multi-level statistical approach. We controlled for the country level clustering but did not have access to other variables measured at the country level. Further research should investigate country level effects, including gender norms within a country, economic development context, and political leadership within the country. These factors, measured at the country level, are likely to shape the context of abortion attitudes and should be included in future research. Second, data were not available at the partner level, and thus we cannot draw conclusions about inter-relationship differences in abortion attitudes. Third, the measurement of abortion attitudes using a single Likert scale item was likely insufficient to capture the nuance of abortion attitudes. More comprehensive measures that we hope to consider in our future work include series of questions about approval of abortion in a number of different situations or a vignette-based approach (Hans and Kimberly 2014). A related limitation was the lack of specificity in terms of the term abortion, which could encompass medication abortion, surgical abortion (MVA, D&E, D&X), and unsafe abortion. A more comprehensive abortion attitudes measure should include these levels of detail. Additional limitations included the cross-sectional nature of the survey which did not allow for a temporal understanding of the relationships between the variables. Furthermore, both recall bias as well as social desirability bias were possible in responses. Depending on the setting, social desirability bias could have biased the responses either toward more or less accepting attitudes towards abortion. Methods such as anonymous web-based surveys may be well-suited for abortion attitudes research to address social desirability. Finally, while the use of a large, multi-level survey allowed us to estimate abortion attitudes across settings, it likely introduced variability for which we could not adequately account in our models, with the inclusion of many diverse countries that did not allow us to test country-specific effects. Future work should better characterize abortion attitudes in individual countries, particularly where abortion remains restricted, illegal, and culturally unacceptable.
Despite these limitations, findings from our multi-country assessment demonstrated differences in abortion attitudes between men and women, with men less likely to support abortion in most cases. Findings also pointed to the importance of policy context in abortion attitudes - where abortion was restricted, attitudes were less supportive. New studies considering partner-level data and more comprehensive abortion attitudes measures should be undertaken to understand the implications of differences in abortion attitudes among men and women for women’s reproductive autonomy. Additional research, especially drawing upon qualitative methods, can provide insight into relationships between the abortion policy and public attitudes, and inform public health interventions to de-stigmatize abortion, promote gender equality in family planning attitudes and decisions, and increase women’s access to legal and safe services. Ultimately, increased global acceptance of abortion is needed to improve women’s and couples’ options for pregnancy decision-making and resolution and women’s reproductive autonomy and health and wellbeing worldwide.
Figure 4: Unadjusted differences in mean abortion attitudes scores by respondents’ sex for selected countries (p<0.05).
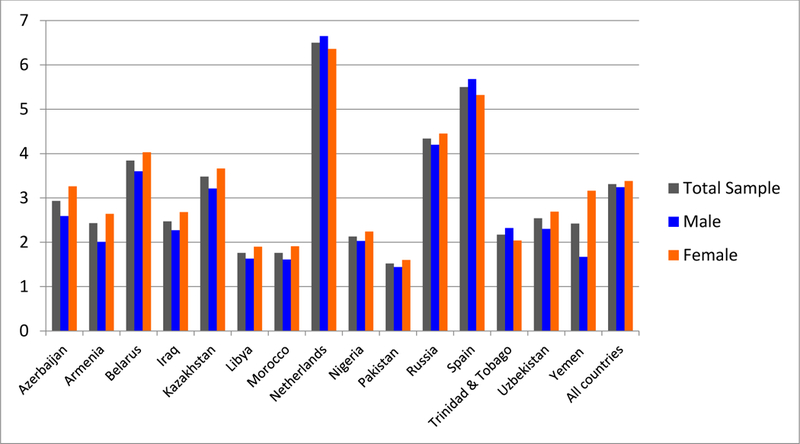
*Mean abortion attitude scores for selected countries with statistically significant differences by respondents’ sex (through student’s t-tests), on scale of 1 (never justifiable) to 10 (always justifiable). Results presented for total sample and by respondents’ sex
References:
- Adamczyk Amy, and Margrét Valdimarsdóttir. 2018. “Understanding Americans’ Abortion Attitudes: The Role of the Local Religious Context” Social Science Research 71 (December 2017). Elsevier: 129–44. doi: 10.1016/j.ssresearch.2017.12.005. [DOI] [PubMed] [Google Scholar]
- Bankole A, and Malarcher S. 2010. “Removing Barriers to Adolescents ‘ Information Access Services to Contraceptive and Services.” Population Council 41 (2): 117–24. [DOI] [PubMed] [Google Scholar]
- Barkan Steven E. 2014. “Gender and Abortion Attitudes: Religiosity as a Suppressor Variable.” Public Opinion Quarterly. doi: 10.1093/poq/nfu047. [DOI] [Google Scholar]
- Begun Stephanie, Kattari Shanna K, McKay Kimberly, Winter Virginia Ramseyer, and O’Neill Elizabeth. 2016. “Exploring U.S. Social Work Students’ Sexual Attitudes and Abortion Viewpoints.” Journal of Sex Research 54 (6). Routledge: 1–12. doi: 10.1080/00224499.2016.1186586. [DOI] [PubMed] [Google Scholar]
- Begun Stephanie, and N Eugene Walls. 2015. “Pedestal or Gutter : Exploring Ambivalent Sexism’s Relationship With Abortion Attitudes.” Journal of Women and Social Work 30 (2): 200–215. doi: 10.1177/0886109914555216. [DOI] [Google Scholar]
- Biggs MA, H Gould, and DG Foster. 2013. “Understanding Why Women Seek Abortions in the US.” BMC Women’s Health 13 (29). BMC Women’s Health: 1–13. doi: 10.1186/1472-6874-13-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Biggs MA, Upadhyay UD, Steinberg JR, and Foste DG. 2014. “Does Abortion Reduce Self-Esteem and Life Satisfaction?” Quality of Life Research : An International Journal of Quality of Life Aspects of Treatment, Care and Rehabilitation 23 (9): 2505–13. doi: 10.1007/s11136-014-0687-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carter J Scott Shannon Carter, and Jamie Dodge. 2009. “Trends in Abortion Attitudes by Race and Gender: A Reassessment Over a Four-Decade Period.” Journal of Sociological Research 1 (1): 1–17. [Google Scholar]
- Charles Vignetta E., Polis Chelsea B., Sridhara Srinivas K., and Blum Robert W.. 2008. “Abortion and Long-Term Mental Health Outcomes: A Systematic Review of the Evidence.” Contraception 78 (6). Elsevier Inc.: 436–50. doi: 10.1016/j.contraception.2008.07.005. [DOI] [PubMed] [Google Scholar]
- Cockrill K, and Nack A. 2013. “‘I’m Not That Type of Person’: Managing the Stigma of Having an Abortion.” Deviant Behavior 34: 973–90. [Google Scholar]
- Cunningham F Gary, Leveno Kenneth J, Bloom Steven L, Spong Catherine Y, Dashe Jodi S, Hoffman Barbara L, Casey Brian M, and Sheffield Jeanne S. 2013. “Abortion” In Williams Obstetrics, 24e New York, NY: McGraw-Hill Education; http://accessmedicine.mhmedical.com/content.aspx?aid=1102101697. [Google Scholar]
- Finer Lawrence B, and Mia R Zolna. 2011. “Unintended Pregnancy in the United States: Incidence and Disparities, 2006.” Contraception 84 (5). Elsevier Inc.: 478–85. doi: 10.1016/j.contraception.2011.07.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Foster DG, Steinberg JR, Roberts SCM, Neuhaus J,, and Biggs MA. 2015. “A Comparison of Depression and Anxiety Symptom Trajectories between Women Who Had an Abortion and Women Denied One.” Psychological Medicine 45 (10): 2073–82. doi: 10.1017/S0033291714003213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Foster Diana Greene, Antonia Biggs M, Lauren Ralph, Caitlin Gerdts, Sarah Roberts, and Maria Glymour M. 2018. “Socioeconomic Outcomes of Women Who Receive and Women Who Are Denied Wanted Abortions in the United States.” American Journal of Public Health 108 (3): 407–13. doi: 10.2105/AJPH.2017.304247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ganatra Bela, Özge Tunçalp, and Heidi Bart. 2014. “From Concept to Measurement : Operationalizing WHO ‘ S Definition of Unsafe Abortion.” Bulletin of the World Health Organization 92: 155. doi: 10.2471/BLT.14.136333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gerdts Caitlin, Ozge Tunçalp, Heidi Johnston, and Bela Ganatra. 2015. “Measuring Abortion-Related Mortality: Challenges and Opportunities.” Reproductive Health 12 (1). Reproductive Health: 10–12. doi: 10.1186/s12978-015-0064-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gipson Jessica D., Koenig Michael a, and Hindin Michelle J.. 2008. “The Effects of Unintended Pregnancy on Infant, Child, and Parental Health: A Review of the Literature.” Studies in Family Planning 39 (1): 18–38. doi: 10.1111/j.1728-4465.2008.00148.x. [DOI] [PubMed] [Google Scholar]
- Hans Jason D, and Claire Kimberly. 2014. “Abortion Attitudes in Context: A Multidimensional Vignette Approach.” Social Science Research 48 (November). Elsevier Inc.: 145–56. doi: 10.1016/j.ssresearch.2014.06.001. [DOI] [PubMed] [Google Scholar]
- Harries Jane, Gerdts Caitlin, Momberg Mariette, and Diana Greene Foster. 2015. “An Exploratory Study of What Happens to Women Who Are Denied Abortions in Cape Town, South Africa.” Reproductive Health 12 (1): 1–6. doi: 10.1186/s12978-015-0014-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hertel Bradley R, and Russell Mark C. 2007. “Examining the Absence of a Gender Effect on Abortion Attitudes : Is There Really No Difference ?” Sociological Inquiry 69 (3): 364–81. [Google Scholar]
- Hindin M. 2012. “The Influence of Women ‘ S Early Childbearing on Subsequent Empowerment in Sub Saharan Africa : A Cross National Meta Analysis.”
- Jelen TG, and Wilcox C. 2003. “Causes and Consequences of Public Attitudes Toward Abortion: A Review and Research Agenda.” Political Research Quarterly 56 (4): 489–500. doi: 10.1177/106591290305600410. [DOI] [Google Scholar]
- Jelen Ted G. 2015. “Gender Role Beliefs and Attitudes Toward Abortion: A Cross-National Exploration.” Journal of Research in Gender Studies 5 (1): 11–22. [Google Scholar]
- Jelen Ted G, Damore David F, and Lamatsch Thomas. 2002. “Gender, Employment Status, and Abortion: A Longitudinal Analysis.” Sex Roles 47 (7–8): 321–30. doi: 10.1023/A:1021427014047. [DOI] [Google Scholar]
- Kerns Jennifer, Vanjani Rachna, Freedman Lori, Meckstroth Karen, Eleanor a Drey, and Jody Steinauer. 2012. “Women’s Decision Making Regarding Choice of Second Trimester Termination Method for Pregnancy Complications.” International Journal of Gynecology and Obstetrics 116 (3). International Federation of Gynecology and Obstetrics: 244–48. doi: 10.1016/j.ijgo.2011.10.016. [DOI] [PubMed] [Google Scholar]
- Kirkman Maggie, Rowe Heather, Hardiman Annarella, Mallett Shelley, and Rosenthal Doreen. 2009. “Reasons Women Give for Abortion: A Review of the Literature.” Archives of Women’s Mental Health 12 (6): 365–78. doi: 10.1007/s00737-009-0084-3. [DOI] [PubMed] [Google Scholar]
- Klugman Barbara, and Budlender Debbie. 2001. “Advocating for Abortion Access: Eleven Country Studies.” http://scholar.google.com/scholar?hl=en&btnG=Search&q=intitle:Advocating+for+abortion+access:+Eleven+country+studies#0.
- Korenman Sanders, Kaestner Robert, and Joyce Ted. 2015. “Consequences for Infants of Parental Disagreement in Pregnancy Intention.” Perspectives on Sexual and Reproductive Health 34 (4): 198–205. doi: 10.2307/3097730. [DOI] [PubMed] [Google Scholar]
- Levandowski Brooke a., Kalilani-Phiri Linda, Kachale Fannie, Awah Paschal, Kangaude Godfrey, and Mhango Chisale. 2012. “Investigating Social Consequences of Unwanted Pregnancy and Unsafe Abortion in Malawi: The Role of Stigma.” International Journal of Gynecology and Obstetrics 118 International Federation of Gynecology and Obstetrics: S167–71. doi: 10.1016/S0020-7292(12)60017-4. [DOI] [PubMed] [Google Scholar]
- Miller E, Decker MR, McCauley HL, Tancredi DJ, Levenson RR, Waldman J, Schoenwald P, and Silverman J. 2010. “Pregnancy Coercion, Intimate Partner Violence, and Unintended Pregnancy.” Contraception 81: 316–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Misra R 1998. “Effects of Age, Gender and Race on Abortion Attitudes.” International Journal of Sociology and Social Policy 18 (9/10): 94–118. [Google Scholar]
- Molina Ramiro Cartes, Carolina Gonzalez Roca, Jorge Sandoval Zamorano, and Electra Gonzales Araya. 2010. “Family Planning and Adolescent Pregnancy.” Best Practice & Research. Clinical Obstetrics & Gynaecology 24 (2). Elsevier Ltd: 209–22. doi: 10.1016/j.bpobgyn.2009.09.008. [DOI] [PubMed] [Google Scholar]
- Montano DE, and Kasprzyk D. 2008. “Theory of Reasoned Action, Theory of Planned Behavior, and the Integrated Behavioral Model” In Health Behavior and Health Education: Theory, Research and Practice, edited by Glanz K, Rimer BK, and Viswanath K, 4th ed., 76–96. San Francisco, CA: Jossey Bass. [Google Scholar]
- Moore Ann M, Gabriel Jagwe-Wadda, and Akinrinola Bankole. 2011. “Mens’ Attitudes about Abortion in Uganda.” Journal of Biosocial Science 43 (1): 31–45. doi: 10.1017/S0021932010000507. [DOI] [PubMed] [Google Scholar]
- Mosley Elizabeth A., King Elizabeth J., Schulz Amy J., Harris Lisa H., Nicole De Wet, and Barbara A Anderson. 2017. “Abortion Attitudes among South Africans: Findings from the 2013 Social Attitudes Survey.” Culture, Health and Sexuality 19 (8). Taylor & Francis: 918–33. doi: 10.1080/13691058.2016.1272715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patel Cynthia J., and Johns Lucinda. 2009. “Gender Role Attitudes and Attitudes to Abortion: Are There Gender Differences?” The Social Science Journal 46 (3): 493–505. doi: 10.1016/j.soscij.2009.02.006. [DOI] [Google Scholar]
- Patel Cynthia J, and Trisha Kooverjee. 2009. “Abortion and Contraception: Attitudes of South African University Students.” Health Care for Women International 30 (6): 550–68. doi: 10.1080/07399330902886105. [DOI] [PubMed] [Google Scholar]
- Primo David M, and Matthew L Jacobsmeier. 2007. “The Practical Researcher: Estimating the Impact of State Policies and Institutions with Mixed-Level Data.” State Politics and Policy Quarterly 7 (4): 446–59. [Google Scholar]
- Raymond Elizabeth G., and Grimes David a. 2012. “The Comparative Safety of Legal Induced Abortion and Childbirth in the United States.” Obstetrics & Gynecology 119 (6): 1271–72. doi: 10.1097/AOG.0b013e318258c833. [DOI] [PubMed] [Google Scholar]
- Roberts Sarah C M, Antonia Biggs M, Chibber Karuna S, Heather Gould, Rocca Corinne H, and Foster Diana G. 2014. “Risk of Violence from the Man Involved in the Pregnancy after Receiving or Being Denied an Abortion.” BMC Medicine 12 (1): 1–7. doi: 10.1186/s12916-014-0144-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwandt HM, A Creanga R Adanu K Danso, Agbenyega T, and Hindin MJ. 2013. “Pathways to Unsafe Abortion in Ghana: The Role of Male Partners, Women and Health Care Providers.” Contraception 88 (4). Elsevier Inc:509–17. doi: 10.1016/j.contraception.2013.03.010. [DOI] [PubMed] [Google Scholar]
- Sedgh G, Singh S, and Hussain R. 2014. “Intended and Unintended Pregnancies Worldwide in 2012 and Recent Trends.” Stud Fam Plann 45 (3): 301–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sedgh G, AH Sylla J Philbin S Keogh, and Ndiaye S. 2015. “Estimates of the Incidence of Induced Abortion And Consequences of Unsafe Abortion in Senegal.” International Perspectives on Sexual and Reproductive Health 41 (1): 11–19. doi: 10.1363/4100115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sedgh Gilda, Bearak Jonathan, Susheela Singh, Akinrinola Bankole, Anna Popinchalk, Bela Ganatra, Clémentine Rossier, et al. 2016. “Abortion Incidence between 1990 and 2014: Global, Regional, and Subregional Levels and Trends.” The Lancet 388 (10041): 258–67. doi: 10.1016/S0140-6736(16)30380-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shellenberg Kristen M, Moore Ann M, Akinrinola Bankole, Fatima Juarez, Adekunbi Kehinde Omideyi, Nancy Palomino, Zeba Sathar, Susheela Singh, and Tsui Amy O. 2011. “Social Stigma and Disclosure about Induced Abortion: Results from an Exploratory Study.” Global Public Health 6 Suppl 1 (September 2015): S111–25. doi: 10.1080/17441692.2011.594072. [DOI] [PubMed] [Google Scholar]
- Silverman Jay G, Decker Michele R, McCauley Heather L, Jhumka Gupta, Elizabeth Miller, Anita Raj, and Goldberg Alisa B. 2010. “Male Perpetration of Intimate Partner Violence and Involvement in Abortions and Abortion-Related Conflict.” American Journal of Public Health 100 (8): 1415–17. doi: 10.2105/AJPH.2009.173393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Singh Susheela, Gilda Sedgh, and Rubina Hussain. 2010. “Unintended Pregnancy: Worldwide Levels, Trends, and Outcomes.” Studies in Family Planning 41 (4): 241–50. doi: 10.1111/j.1728-4465.2010.00250.x. [DOI] [PubMed] [Google Scholar]
- “World Values Survey: Fieldwork and Sampling.” 2015. http://www.worldvaluessurvey.us/WVSContents.jsp.