

Abstract
Introduction:
Breast cancer is one of the leading causes of cancer deaths among women in India today. Overall outcome of this disease is largely dependent on early detection and medical intervention. Breast self-examination (BSE) is an easy, cost effective, and safe method of screening for the same.
Materials and Methods:
A cross-sectional descriptive questionnaire-based study was conducted among female IT professionals and their scores in the fields of knowledge, attitude, and practice were calculated. The scores were categorized linearly as good, fair, and poor, then analyzed in detail. The correlation between knowledge and attitude, attitude and practice, and knowledge and practice were ascertained using the Spearman's rank correlation coefficient.
Results:
About 356 women spanning from 18 to 55 years of age were included in the study, out of which 44 women (12.35%) gave family history of breast cancer. The mean scores in knowledge, attitude, and practice fields were 18.17 ± 2.90, 27.07 ± 8.14, and 19.11 ± 5.08, respectively. Spearman's rank correlation coefficient revealed that knowledge and attitude were not correlated, attitude and practice were not correlated; but knowledge and practice were extremely correlated.
Conclusion:
Educational programs to create awareness regarding breast cancer and its occurrence, risk factors, screening including BSE, symptoms, need for early help-seeking practices, diagnosis, and treatment modalities are the need of the hour.
Keywords: Breast cancer, breast self-examination, primary prevention, screening
Introduction
Today, India is witnessing a soaring increase in the number of patients being diagnosed with breast cancer at a young age. Breast cancer recently surpassed cervical cancer and has become the most common cancer among Indian women. The age-adjusted incidence rate of carcinoma of the breast was found as high as 41 per 100,000 women for Delhi, followed by Chennai (37.9), Bangalore (34.4), and Thiruvananthapuram District (33.7). There has been a significant increase in the incidence of breast cancer over the years and it continues to rise steadily.[1] Breast cancer-associated mortality is eminent, being the fifth highest due to cancer and the most common cause of death due to cancer among women.[2]
Early detection plays a pivotal role in the prevention of breast cancer. The 5-year survival rate has reached approximately 85% with early detection, whereas later detection has decreased the survival rate to 56%.[3] Breast cancer is made distinct from other types of cancers by the fact that it occurs in a noticeable organ and can be detected and treated at an early stage.[4] Most of the breast tumors diagnosed in an early stage have been self-discovered.[5]
Initially, breast cancer does not produce symptoms. However, as the tumor enlarges, symptoms manifest in the form of painless lump in the breast, lump under the armpit, breast tenderness, swelling or thickness of skin over the breast, and spontaneous discharge of the nipple (particularly if bloody, erosion, or inversion in the nipple).[6]
Recommended precautionary techniques to reduce breast cancer morbidity and mortality include breast self-examination (BSE), clinical breast examination (CBE), and mammography.[7] However, the latter two require a visit to the doctor and use of specialized equipment. BSE is an easy, quick, convenient, private, cost free, and safe practice that requires no paraphernalia.
Despite being an old technique, BSE is not frequently practiced or has been practiced incorrectly for many reasons. Previous studies show that the primary barriers for the poor practicing of BSE were forgetfulness, lack of time, ignorance, fear/anxiety, and low level of education.[8,9,10,11] It is therefore important to determine the level of knowledge regarding BSE, as well as the attitude and practice among women in our community to recognize their acceptance, belief, and the magnitude of current practice.
Bangalore, Silicon Valley of India, is home to over 900 Information Technology (IT) companies and houses numerous female employees. The idea behind choosing them was that they come from an educated background and are more likely to be acquainted with the subject, at the same time have risk factors for breast cancer. Hence this study was undertaken with the objectives to assess knowledge, attitude, and practice of BSE among the IT professionals and to correlate between knowledge, attitude, and practice.
Materials and Methods
A cross-sectional descriptive study was conducted among 356 female IT professionals aged 18 years and above. The study was carried out from May to August 2017. Ethical clearance was obtained from the Institutional Ethical Committee. Written informed consent was obtained from the participants. Anonymity and confidentiality of the responses were assured to the women taking part in the study. Females who had pain in the breast and were already diagnosed with breast cancer were excluded from the study. The sample size was calculated based on a previous study conducted among dental students in Hyderabad.[12]
A pre-tested, close-ended questionnaire was employed to review the knowledge, attitude, and practice of BSE in these women.[13] The questionnaire comprised of 35 questions – 15 on knowledge, 13 on attitude, and 7 on practice. Categorical response of TRUE/FALSE/DON’T KNOW was used to answer knowledge-based questions. A 5-point Likert scale (STRONGLY AGREE/AGREE/NEUTRAL/NOT AGREE/STRONGLY DISAGREE) was used for attitude opinion. A similar ordinal (NEVER/SELDOM/NEUTRAL/FREQUENT/ALWAYS) was used to enquire about practice. For positive knowledge, item score “2” was used for correct responses, “1” for don’t know, and “0” for incorrect response. For a positive attitude item, a score of “5,” “4,” “3,” “2,” and “1” were used for strongly disagree, agree, neutral, disagree, and strongly disagree, respectively. For practice, an item score of “1,” “2,” “3,” “4,” and “5” were given for never, seldom, neutral, frequently, and always, respectively. The score was reversed for all the negative items and the overall score was calculated.
Mean and standard deviation were calculated for each of the parameters. The scores obtained for knowledge, attitude, and practice were categorized for further analysis. Data were analyzed using percentages and the Spearman's rank correlation coefficient (rho) using the IBM Statistical Package for Social Sciences (SPSS) version 21.
Health education regarding causes, prevention of breast cancer, and correct method of BSE was imparted to the participants in the form of interactive sessions and handouts after collection of data.
Results
A total of 356 women were included in the study. The response and completion rates were 100%. All 356 women were aware of breast cancer. Women spanning from 18 to 55 years of age participated in this study. Majority, i.e., 60.11% belonged to 18–28 years of age and only 1.68% were between 48 to 58 years as shown in Table 1.
Table 1.
Distribution of participants according to age
| Age (years) | Number of participants | Percentage of participants (%) |
|---|---|---|
| 18-28 | 214 | 60.11 |
| 28-38 | 106 | 29.77 |
| 38-48 | 30 | 8.42 |
| 48-58 | 6 | 1.68 |
| Total | 356 | 100 |
All women in the study were graduates at minimum and the qualifications ranged up to Ph.D. Monthly income of most of the participants (%) was between Rs. 20,000–50,000 as shown in Table 2.
Table 2.
Distribution of participants according to income
| Monthly income (rupees) | Number of participants | Number of participants (%) |
|---|---|---|
| <20,000 | 64 | 17.9 |
| 20,000-50,000 | 140 | 39.3 |
| 50,000-1,00,000 | 78 | 21.9 |
| 1,00,000-2,00,000 | 28 | 7.8 |
| >2,00,000 | 46 | 12.9 |
| Total | 356 | 100 |
A total of 44 women (12.35%) gave family history of breast cancer, the most frequently affected relative being an aunt.
Knowledge scores
The mean score was 18.17 ± 2.90 with a minimum score of 12 and a maximum of 26. The scores were grouped into good knowledge, i.e., 25–30, fair knowledge, i.e., 15–25, and no knowledge, i.e., 0–15.
The number of people who had good knowledge (>25) turned out to be 2 (0.5%) out of 356. Although, the fraction of people with good knowledge was expected to be low, our results are quite dismal. This can primarily be attributed to the lack of structured/standardized education at pre-University and University levels. Highest number of respondents were found to be knowledgeable (15–25), i.e., 328 (92.1%). This could be due to partial knowledge gained through the internet, print, film media, by word of mouth through friends, relatives, and first-hand information from people who suffered from breast cancer, and finally infrequently due to guesswork.
Attitude scores
The mean score was 27.07 ± 8.14 with a minimum score of 13 and a maximum of 64. The scores were categorized into good attitude, i.e., 50–65, reasonable attitude, i.e., 31–50, and poor attitude, i.e., 13–26.
According to our study, almost 68% of the respondents were found to have poor attitude (<30) toward BSE. There are a multitude of reasons for this. Some of the cardinal reasons being social stigma and social norms, which do not make it comfortable for women to talk/learn about and be familiar with their own body, and not to mention popular culture which freely allows for sexualization of the breasts. There is an unspoken and undefined gap in communication between spouses and parents in most families. Fear, lack of knowledge, and a lackadaisical attitude are also contributors.
Practice scores
The mean score was 19.11 ± 5.08 with a minimum score of 11 and a maximum of 35. The scores are classified as good practice, i.e., 21–35 and poor practice, i.e., <21.
An astonishing number of 222 respondents were found to be knowledgeable about BSE but had a bad attitude. It is interesting to note that the two respondents who scored the highest on knowledge, scored considerably low on attitude that means knowledge alone is not enough to have a positive attitude. Discomfort, unfamiliarity, and unpleasant past experiences might also have contributed to a negative influence on attitude and practice of BSE, as evidenced by 204 respondents being knowledgeable but ranking poor on practice. Lack of information on BSE and its procedure from authentic sources, poor attitude due to the aforementioned reasons, busy work schedules, and lack of foresight could be the causes for poor practice scores seen in 222 candidates. Knowledge, attitude and practice scores are shown in Figure 1.
Figure 1.
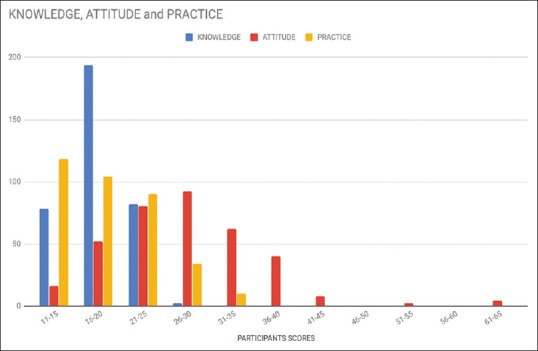
Knowledge, attitude and practice scores
Correlation between knowledge and attitude – Spearman's rank correlation coefficient − 0.087 (P = 0.102) hence establishing that knowledge and attitude are not correlated.
Correlation between attitude and practice – Spearman's rank correlation coefficient −0.243 (P < 0.001) thus attitude and practice are correlated.
Correlation between knowledge and practice – Spearman's rank correlation coefficient +0.204 (P < 0.001) therefore knowledge and practice are extremely correlated.
Spearman's rank correlation coefficient values for age and knowledge, attitude and practice were +0.299, −0.213, and +0.211, respectively. There was a positive correlation between age and knowledge, age and practice, however, a negative correlation between age and attitude as shown in Table 3.
Table 3.
Correlation between knowledge, attitude, and practice
| Correlation between | Spearman’s rank correlation coefficient | P | Inference |
|---|---|---|---|
| Knowledge and attitude | −0.087 | 0.102 | Not correlated |
| Attitude and practice | −0.243 | <0.001 | Correlated |
| Knowledge and practice | +0.204 | <0.001 | Correlated |
Detailed analysis of the data revealed that only four women who had good attitude scores also had good practice scores, implying that despite having a good attitude, the lack of knowledge is preventing them from practicing BSE.
Discussion
Non-communicable diseases are the new epidemics, affecting both developed and developing countries. Treatment of such diseases is lifelong, a costly affair, and often associated with various other complications. Primary prevention in the form of health education is the governing factor for the control of diseases like cancer, a common non-communicable disease. One of the noteworthy positive findings of this study is that all the women were aware of breast cancer. This can be attributed to their high levels of education and internet exposure.
The knowledge, attitude, and practice scores obtained from this study are higher than previously ascertained levels among dental students in Hyderabad, India.[12] The mean age of the participants in our study (28.865 ± 7.009) is much above that of study conducted among the dental students (19.6 ± 1.38). The reason could be older women have been through pregnancies, breastfed their children, and hence may be more familiar with matters concerning BSE.
Scores when compared with those from a study conducted in a suburban area of Terengganu, Malaysia revealed lower scores in the knowledge and practice, but higher attitude scores.[13] Breast cancer screening policies in Malaysia mandate that every woman between the age of 20–39 years must undergo CBE once in 3 years and women >40 years must undergo it every year. These features might have contributed to better attitude outcome. They also offer subsidies on mammography.[14] In a study conducted among female health workers in Iran, it was found that the knowledge about breast cancer and performing BSE was 79.8%, and 72.45% of them have positive attitudes; but only 39.5% of the women performed BSE regularly every month. A significant relationship was found between the attitudes and the university degree of the health workers and between age, university degree, and the times of taking part in education classes with performing BSE.[15] The study conducted on female dental students in Hyderabad, India revealed inadequate scores in knowledge, attitude, and practice fields.[12] These two studies reveal the lack of practice of BSE among health care professionals despite having good knowledge about importance of breast cancer, role of early detection, and method of BSE. These caregivers should themselves practice it and encourage other women to do the same.
A recent study conducted in a rural area of India by Kumarasamy et al., demonstrated that only 26% of the women were aware of BSE, of which 18% had ever checked their breast, and 5% practiced it regularly. Awareness of BSE was found to be significantly associated with age and educational attainment.[16] A similar study conducted among educated Indian women showed better results as established by Yadav and Jaroli, that only 28% of young college going women were unaware of BSE.[17]
On an international scale, a study conducted in the University of Jordan, including 900 women revealed that 152 participants (34.9%) were aware of BSE, but only 93 (11%) had performed it.[18]
A study on female undergraduate students in the University of Buea, revealed that nearly three quarters of respondents had previously heard of BSE, yet only 9% knew how to perform it. Another key feature emphasized by this study is that 88% of the women found BSE to be important but only 3% performed it regularly. The main reason cited for not performing BSE is lack of knowledge about the same.[19]
According to a study by Gilani et al., conducted in Rawalpindi, Pakistan more than half the participants were aware of the risk factors of breast cancer, had knowledge about breast cancer symptoms, diagnostic modalities, and treatment and its relationship with outcome. Majority (>90%) had a positive attitude and intended to see a doctor immediately if they ever felt a breast lump but had poor (28.3%) practices regarding BSE.[20]
All the above-mentioned studies highlight the insufficiency in the levels of knowledge, attitude, and practice of BSE across the globe and hence an urgent need for health education programs on this subject. Many more women need to be aware and motivated to practice BSE.
The knowledge and practice of BSE are largely correlated as established by this study. Knowledge directly affects practice by improving practice levels among women who already have a good attitude toward BSE.
This study establishes that with increasing age; knowledge and practice trends positively, whereas it does not contribute to an improvement in the attitude. This can be attributed to deep-rooted inhibitions, taboos, and misconceptions about breast cancer and BSE among older women. Societal setting in our country does not appear to be conducive for effective communication and education regarding one's own body and its changes. But on a positive note, from our interactive sessions with the subjects of the study, although not objectively, we could gauge a sense of eagerness and earnestness among them to learn.
Conclusion
This study highlights the need for educational programs to create awareness regarding breast cancer and its occurrence, risk factors, screening including BSE, symptoms, need for early help-seeking practices, diagnosis, and treatment modalities.
The family physicians have a crucial role in screening for breast cancer. The approachable nature and credibility of a family physician in society often makes them the first and only point of contact for women seeking health education. They can provide the tools essential to learn, practice, and destigmatize BSE. By doing so, they can inculcate a culture and environment that normalize BSE, hence encouraging more women to practice it.
Breast cancer awareness levels must be ameliorated by targeting documented barriers. This includes involvement of spouses, family, and the community to have a positive effect on BSE practice. Women need to be motivated to examine their own breasts and to detect any changes at the earliest. Women all over must come together and help each other out. The way ahead is by sharing information about the importance and technique of BSE and setting an example for others to follow as health care professionals, Indians, and women.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
Authors would like to thank the management of the Vydehi Institute of Medical Science and Research Centre for all the facilities provided for this study.
References
- 1.Malvia S, Bagadi SA, Dubey US, Saxena S. Epidemiology of breast cancer in Indian women. Asia Pac J Clin Oncol. 2017;13:289–95. doi: 10.1111/ajco.12661. [DOI] [PubMed] [Google Scholar]
- 2.GLOBOCAN 2012. International Agency for Research on Cancer. World Health Organization. PRESS RELEASE No. 223. 2013. Dec 12, [Last accessed on 2018 Sep 10]. Available from: https://www.iarc.fr/en/media-centre/pr/2013/pdfs/pr223_E.pdf .
- 3.Hallal JC. The relationship of health beliefs, health locus of control, and self concept to the practice of breast self-examination in adult women. Nurs Res. 1982;31:137–42. [PubMed] [Google Scholar]
- 4.Taşçı A, Usta YY. Comparison of knowledge and practices of breast self examination (BSE): A pilot study in Turkey. Asian Pac J Cancer Prev. 2010;11:1417–20. [PubMed] [Google Scholar]
- 5.Smith EM, Francis AM, Polissar L. The effect of breast self-exam practices and physician examinations on extent of disease at diagnosis. Prev Med. 1980;9:409–17. doi: 10.1016/0091-7435(80)90235-2. [DOI] [PubMed] [Google Scholar]
- 6.Koo MM, von Wagner C, Abel G, McPhail S, Rubin GP, Lyratzopoulosa G. Typical and atypical presenting symptoms of breast cancer and their associations with diagnostic intervals: Evidence from a national audit of cancer diagnosis. Cancer Epidemiol. 2017;48:140–6. doi: 10.1016/j.canep.2017.04.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Humphrey LL, Helfand M, Chan BK, Woolf SH. Breast cancer screening: A summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2002;137:347–60. doi: 10.7326/0003-4819-137-5_part_1-200209030-00012. [DOI] [PubMed] [Google Scholar]
- 8.Gupta SK, Pal DK, Garg R, Tiwari R, Shrivastava AK, Bansal M. Impact of a health education intervention program regarding breast self-examination by women in a semi-urban area of Madhya Pradesh, India. Asian Pac J Cancer Prev. 2009;10:1113–7. [PubMed] [Google Scholar]
- 9.Hisham AN, Yip CH. Overview of breast cancer in Malaysian women: A problem with late diagnosis. Asian J Surg. 2004;27:130–3. doi: 10.1016/S1015-9584(09)60326-2. [DOI] [PubMed] [Google Scholar]
- 10.Salazar MK. Breast self-examination beliefs: A descriptive study. Public Health Nurs. 2007;11:49–56. doi: 10.1111/j.1525-1446.1994.tb00389.x. [DOI] [PubMed] [Google Scholar]
- 11.Okobia MN, Bunker CH, Okonofua FE, Osime U. Knowledge, attitude and practice of Nigerian women towards breast cancer: A cross-sectional study. World J Surg Oncol. 2006;4:11. doi: 10.1186/1477-7819-4-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Doshi D, Reddy BS, Kulkarni S, Karunakar P. Breast self-examination: Knowledge, attitude, and practice among female dental students in Hyderabad City, India. Indian J Palliat Care. 2012;18:68–73. doi: 10.4103/0973-1075.97476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Rosmawati NH. Knowledge, attitudes and practice of breast self-examination among women in a suburban area in Terengganu, Malaysia. Asian Pac J Cancer Prev. 2010;11:1503–8. [PubMed] [Google Scholar]
- 14.Dahlui M, Ramli S, Bulgiba AM. Breast cancer prevention and control programs in Malaysia. Asian Pac J Cancer Prev. 2011;12:1631–4. [PubMed] [Google Scholar]
- 15.Reisi M, Javadzade SH, Sharifirad G. Knowledge, attitudes, and practice of breast self-examination among female health workers in Isfahan, Iran. J Educ Health Promot. 2013;2:46. doi: 10.4103/2277-9531.117417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kumarasamy H, Veerakumar AM, Subhathra S, Suga Y, Murugaraj R. Determinants of awareness and practice of breast self examination among rural women in Trichy, Tamil Nadu. J Midlife Health. 2017;8:84–8. doi: 10.4103/jmh.JMH_79_16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Yadav P, Jaroli DP. Breast cancer: Awareness and risk factors in college-going younger age group women in Rajasthan. Asian Pac J Cancer Prev. 2010;11:319–22. [PubMed] [Google Scholar]
- 18.Suleiman AK. Awareness and attitudes regarding breast cancer and breast self-examination among female Jordanian students. J Basic Clin Pharm. 2014;5:74–8. doi: 10.4103/0976-0105.139730. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Nde FP, Assob JC, Kwenti TE, Njunda AL, Tainenbe TR. Knowledge, attitude and practice of breast self examination among female undergraduate students in the University of Buea. BMC Res Notes. 2015;8:43. doi: 10.1186/s13104-015-1004-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Gilani SI, Khurram M, Mazhar T, Mir ST, Ali S, Tariq S, et al. Knowledge, attitude and practice of a Pakistani female cohort towards breast cancer. J Pak Med Assoc. 2010;60:205–8. [PubMed] [Google Scholar]