

History
The coronoid of the ulna is an important stabilizer of the elbow. It is the anterior bony buttress to the ulnohumeral joint, preventing posterior subluxation of the elbow [4, 11]. It also serves as a soft tissue attachment site for important stabilizers of the elbow including the anterior joint capsule, the medial collateral ligament, the lateral ulnar collateral ligament, and the brachialis muscle [3].
Although fractures of the coronoid are relatively uncommon, occurring in 2% to 10% of elbow dislocations [10, 19], they often are accompanied by ligamentous injuries associated with more-persistent elbow instability. Fractures that have greater than 50% involvement of the coronoid have been shown in an anatomic study to contribute to posterior subluxation of the elbow in the absence of other injuries [3]. Therefore, correctly identifying and managing these fractures to restore alignment and stability of the elbow is important and may prevent persistent instability and subsequent posttraumatic arthrosis [8].
Owing to the complexity of coronoid fractures and concomitant elbow injuries, a uniform classification system that guides management and anticipates prognosis would be helpful to clinicians. The original classification system for coronoid fractures was described in 1989 by Regan and Morrey [15]; in that study, they stratified these fractures based on percentage of coronoid involvement. Regan and Morrey [15] reported on 35 patients with coronoid fractures. They noted an increase in the risk of dislocation, and corresponding decreases in elbow function (based on the elbow performance index) and ROM, an increase in subsequent operations, and an increase in the risk of heterotopic ossification as the size of the fracture fragment increased.
Purpose
Elbow stability is based on numerous factors, including the bony anatomy of the coronoid and its soft tissue attachments [4, 11]. Given the complexity of elbow instability, Regan and Morrey [15, 16] initiated a retrospective study to quantify the role of the coronoid in elbow stability. Their goal was to establish a classification based on plain radiographs that could guide management and help determine prognosis. The resulting radiographically driven classification scheme attempted to associate morphologic features of fractures with stability and patient function. This classification derives primarily from the idea that elbow stability generally decreases as the size of the coronoid fracture increases.
Classification/Description
The Regan-Morrey classification stratifies coronoid fractures in three groups based on the proportion of the coronoid involved as delineated on the lateral radiographic views of the elbow. Type I fractures are an avulsion of the tip of the coronoid. Type II fractures are a single or comminuted fragment involving less than 50% of the coronoid. Type III fractures involve greater than 50% of the coronoid. An “A” modifier is added for fractures without dislocation, and a “B” modifier is added for fractures with an associated dislocation (Fig. 1).
Fig. 1.
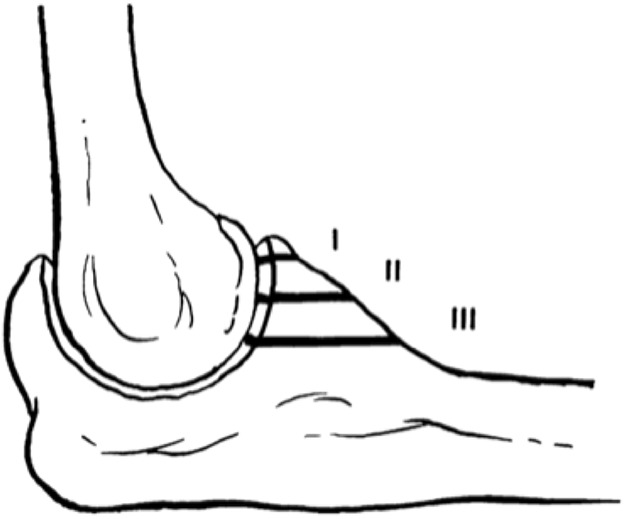
The Regan-Morrey classification stratifies coronoid fractures based on coronoid fragment size on a single lateral radiograph of the elbow. (Published with permission from Springer from Samii A, Zellweger R. Fractures of the coronoid process of the ulna: which ones to fix and which ones to leave alone: a review. Eur J Trauma Emerg Surg, 2008;34:113-119.)
Validation
The initial Regan-Morrey classification system was based on the proportion of the coronoid involved with the fracture as seen on the lateral radiograph of the elbow. To our knowledge, no study has been performed specifically validating inter- and intraobserver reliability of the classification system based on plain radiographs alone.
However, Lindenhovius et al. [9] performed a study looking at inter- and intraobserver reliability of the Regan-Morrey classification with the addition of two-dimensional (2-D) and three-dimensional (3-D) CT scans to supplement radiographs. They found “fair” interobserver reliability with 2-D CT (κ = 0.40) and improved “moderate” interobserver reliability with added 3-D CT (κ = 0.51; p < 0.001). Intraobserver agreement was determined to be “moderate” for the Regan-Morrey classification system (κ = 0.51).
The association between fragment size and ROM and patient-reported outcomes has been evaluated. Adams et al. [1] performed a retrospective study of 103 coronoid fractures and found that with increased fragment size on the Regan-Morrey classification system, patients had decreased ROM at followup. Mean flexion to extension arc was 134° in Type IA fractures, 125° in Type IB, 120° in Types IIA and IIB, 111° in Type IIIA, and 113° in Type IIIB fractures (p = 0.01). Increased fragment size also was associated with concomitant elbow injuries and use of operative fixation.
Doornberg and Ring [6] also looked retrospectively at coronoid fragment size and associated injury patterns. They found an association between Regan-Morrey Type III coronoid fractures with olecranon fracture-dislocation and Regan-Morrey Type II fractures with terrible triad injuries (elbow dislocation with radial head and coronoid fractures) and posteromedial rotation instability pattern fracture-dislocations. Of the 24 patients with an olecranon fracture-dislocation, 22 had Regan-Morrey Type III fractures (92%). All patients studied with terrible triad injuries and 82% of patients (nine of 11) with varus posteromedial rotational instability fracture-dislocations were classified as having Type II fractures.
An anatomic study also has confirmed the relationship of important soft tissue attachments to the three sizes of fracture fragments described by the classification. Cage et al. [3] performed a cadaver study correlating soft tissue attachments with the three Regan-Morrey fracture types. In cadaver elbows, they found that the Regan-Morrey Type I fracture fragment represented a shear fracture of the coronoid tip sustained as it passed beneath the humeral trochlea during subluxation or dislocation. Because the anterior capsular attachment was, on average, 6.4 mm distal to the tip of the coronoid, Type I coronoid tip fractures often did not involve capsular avulsions. The anterior capsule did attach to the Regan-Morrey Type II fragment, whereas the brachialis was attached to Regan-Morrey Type III fragment. A Type III fracture was associated with the loss of integrity of the anterior bundle of the medial collateral ligament insertion, so Cage et al. [3] suggested that a Type III fracture may destabilize the elbow.
Limitations
The main limitations of the Regan-Morrey classification system stem from its simplicity. Because the system was based on fragment size on a lateral radiograph alone, a criticism of the classification is its inability to fully describe morphologic features of a fracture and guide surgical management. Fracture planes in the anterior to posterior plane, such as those seen in anteromedial facet fractures, may be missed on a single, lateral radiograph. The anteromedial facet is particularly vulnerable to injury from a varus force [5] and can be associated with complex instability patterns such as varus posteromedial rotatory instability [13, 14]. Recognition of this anteromedial facet fragment, which is not accounted for in the Regan-Morrey classification, may imply a distinct pattern of elbow instability and alter surgical decision-making. Advanced imaging in the form of 2-D and even 3-D CT scans has increased our understanding of the fracture patterns present in these complex injuries. Oblique patterns, impaction, and comminution are poorly seen on radiographs alone but are now more readily observed with the addition of CT [2, 18].
Another limitation is the lack of specific thresholds to define Types I and II fractures. The original classification defined Type I fractures as a shear avulsion fracture of the tip of the coronoid, whereas Type II fractures involved less than 50% of the coronoid. This has allowed for uncertainty regarding potential overlap between the two types. Some authors, including Doornberg and Ring [6] have used the location of insertion of the joint capsule on the fragment as a cutoff point between Types I and II based on anatomic studies. They considered any fracture 5 mm distal to the tip of the coronoid as Type II, because an anatomic study showed that the capsule inserts an average of 6.4 mm distal to the coronoid tip [3].
Although the bony contribution of the coronoid is important for stability [3], this simple classification system does not take into account the sometimes-severe soft tissue injury that often is associated with these fractures, the fracture mechanism, or associated fracture patterns. The system simply identifies the relative fragment size in a single plane and presence or absence of dislocation. Coronoid fractures can exist as one component of the terrible-triad injury along with elbow dislocation and radial head fracture [17]. Doornberg et al. [7] evaluated the mean height of the coronoid fracture fragment in coronoid fractures associated with a terrible triad injury. The coronoid fragment was an average of 35% of the total height of the coronoid. They contended that although these fragments appear small on radiographs, they remain important to elbow stability. Mellema et al. [12] additionally looked at fracture patterns associated with traumatic elbow instability, concluding that the knowledge of fracture pattern and associated injury can help guide surgical exposure and management of coronoid fractures.
Further classification of coronoid fractures has been proposed after Regan and Morrey’s original article to increase understanding of complex fracture patterns and associated injuries. O’Driscoll et al. [13] proposed a new system of classification considering anatomic location, amount of coronoid fractured, comminution, elbow stability, and associated injuries. In this system, a Type 1 fracture involves the tip of the coronoid, a Type 2 involves a fracture of the anteromedial facet of the coronoid, and Type 3 involves a fracture of the coronoid at the base. Subtypes then are added for further description of size, location, and number of fragments. Although this classification may be more complex than the original Regan-Morrey classification, this increased detail may better aid in surgical decision-making, although studies to document advantages of the O’Driscoll classification over the Regan-Morrey classification have not been published, to the best of our knowledge..
Conclusion
The Regan-Morrey description of coronoid fractures provides a simple classification of fragment size based on a single lateral radiograph. To our knowledge, no study has validated the Regan-Morrey classification based on radiographs alone, and the reliability using CT scans is only fair to moderate [9], a fact that should be considered very carefully by clinicians who use this classification in practice. Although the classification allows for some understanding of the likely soft tissue attachments and resulting instability patterns based on fragment size, its simplicity hinders full characterization of the fracture planes and more-complex injury patterns such as varus posteromedial instability. Increased understanding of the fracture pattern and instability patterns may be better served with 3-D imaging, and studies to determine whether this is the case should be performed.
Footnotes
Each author certifies that neither he or she, nor any member of his or her immediate family, have funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
References
- 1.Adams JE, Hoskin TL, Morrey BF, Steinmann SP. Management and outcome of 103 acute fractures of the coronoid process of the ulna. J Bone Joint Surg Br. 2009;91:632–635. [DOI] [PubMed] [Google Scholar]
- 2.Adams JE, Sanchez-Sotelo J, Kallina CF. 4th, Morrey BF, Steinmann SP. Fractures of the coronoid: morphology based upon computer tomography scanning. J Shoulder Elbow Surg. 2012;21:782–788. [DOI] [PubMed] [Google Scholar]
- 3.Cage DJ, Abrams RA, Callahan JJ, Botte MJ. Soft tissue attachments of the ulnar coronoid process: an anatomic study with radiographic correlation. Clin Orthop Relat Res. 1995;320:154–158. [PubMed] [Google Scholar]
- 4.Closkey RF, Goode JR, Kirschenbaum D, Cody RP. The role of the coronoid process in elbow stability: a biomechanical analysis of axial loading. J Bone Joint Surg Am. 2000;82:1749–1753. [DOI] [PubMed] [Google Scholar]
- 5.Doornberg JN, de Jong IM, Lindenhovius AL, Ring D. The anteromedial facet of the coronoid process of the ulna. J Shoulder Elbow Surg. 2007;16:667–670. [DOI] [PubMed] [Google Scholar]
- 6.Doornberg JN, Ring D. Coronoid fracture patterns. J Hand Surg Am. 2006;31:45–52. [DOI] [PubMed] [Google Scholar]
- 7.Doornberg JN, van Duijn J, Ring D. Coronoid fracture height in terrible-triad injuries. J Hand Surg Am. 2006;31:794–797. [DOI] [PubMed] [Google Scholar]
- 8.Giannicola G, Calella P, Piccioli A, Scacchi M, Gumina S. Terrible triad of the elbow: is it still a troublesome injury? Injury. 2015;46(suppl 8):S68–S76. [DOI] [PubMed] [Google Scholar]
- 9.Lindenhovius A, Karanicolas PJ, Bhandari M, van Dijk N, Ring D; Collaboration for Outcome Assessment in Surgical Trials. Interobserver reliability of coronoid fracture classification: two-dimensional versus three-dimensional computed tomography. J Hand Surg Am. 2009;34:1640–1646. [DOI] [PubMed] [Google Scholar]
- 10.Linscheid RL, Wheeler DK. Elbow dislocations. JAMA. 1965;194:1171–1176. [PubMed] [Google Scholar]
- 11.Matzon JL, Widmer BJ, Draganich LF, Mass DP, Phillips CS. Anatomy of the coronoid process. J Hand Surg Am. 2006;31:1272–1278. [DOI] [PubMed] [Google Scholar]
- 12.Mellema JJ, Doornberg JN, Dyer GS, Ring D. Distribution of coronoid fracture lines by specific patterns of traumatic elbow instability. J Hand Surg Am. 2014;39:2041–2046. [DOI] [PubMed] [Google Scholar]
- 13.O'Driscoll SW, Jupiter JB, Cohen MS, Ring D, McKee MD. Difficult elbow fractures: pearls and pitfalls. Instr Course Lect. 2003;52:113–134. [PubMed] [Google Scholar]
- 14.Pollock JW, Brownhill J, Ferreira L, McDonald CP, Johnson J, King G. The effect of anteromedial facet fractures of the coronoid and lateral collateral ligament injury on elbow stability and kinematics. J Bone Joint Surg Am. 2009;91:1448–1458. [DOI] [PubMed] [Google Scholar]
- 15.Regan W, Morrey B. Fractures of the coronoid process of the ulna. J Bone Joint Surg Am. 1989;71:1348–1354. [PubMed] [Google Scholar]
- 16.Regan W, Morrey B. Classification and treatment of coronoid process fractures. Orthopedics. 1992;15:845–848. [DOI] [PubMed] [Google Scholar]
- 17.Ring D, Jupiter JB, Zilberfarb J. Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am. 2002;84:547–551. [DOI] [PubMed] [Google Scholar]
- 18.Sanchez-Sotelo J, O'Driscoll SW, Morrey BF. Medial oblique compression fracture of the coronoid process of the ulna. J Shoulder Elbow Surg. 2005;14:60–64. [DOI] [PubMed] [Google Scholar]
- 19.Scharplatz D, Allgower M. Fracture-dislocations of the elbow. Injury. 1975;7:143–159. [DOI] [PubMed] [Google Scholar]