

Abstract
Background
Intra-articular knee injection with steroid or various other agents have been used to control the local inflammation and relieve pain in the osteoarthritis knee. To achieve the maximal potential therapeutic worth and decrease the complications from the inaccurate knee injection, these medications should be delivered directly into the intra-articular space. Injection technique is one of the most important factors for accuracy of knee injection. Therefore, this study was aimed to propose the new modified anterolateral injection technique for higher accuracy of knee injection in symptomatic osteoarthritis knee without effusion.
Material and methods
Patients with symptomatic osteoarthritis without effusion were included prospectively from May 2014 to May 2015 and randomized into 2 groups for knee injection: Modified anterolateral (MAL), Standard superolateral (SL). Knee injection was performed by one experienced orthopaedic. Accuracy of injection was test by mini air-arthrography technique. The pain from injection were evaluated by visual analog scale (VAS).
Result
132 knees were included, 66 knees were modified anterolateral group same as superolateral group. The modified anterolateral injection was significantly yield the higher accuracy rate than the standard superolateral injection (89% vs 58%, P < 0.05). The pain visual analog scale was not significantly different between the modified anterolateral and standard superolateral injection technique (2.61 vs 2.65, P = 0.917) No adverse events were occurred.
Conclusion
The new modified anterolateral injection yields the higher pooled accuracy rate. From the accuracy and the advantage of the new modified anterolateral injection, this is the preferred injection technique for the symptomatic osteoarthritis without knee effusion.
Keywords: Accuracy, Knee injection, Anterolateral, Superolateral, Backflow
Background
Osteoarthritis (OA) is the most common form of arthritis, involving inflammation and major structural changes of the joint. It is the leading cause of pain, functional disability and socioeconomic involvement.1 Knee is one of the joints most commonly affected by arthritis. The global age-standardized prevalence of knee OA was 3.8%2 and more common in women than male(1.5: 1 to 4:1).3 In the clinical setting, these patients present us with the complaints of pain, stiffness and immobility. Most current therapies are directed toward minimizing pain and swelling, maintaining joint mobility, and reducing associated disability. Intra-articular injection with steroid or various other agents have been used for long time to control the local inflammation and relieve pain. As a result, knee injections are performed by physicians of various specialties. To achieve the maximal potential therapeutic worth and decrease the complications from inaccurate knee injection, these medications should be delivered directly into the intra-articular space and not into extra-articular area, the anterior fat pad and extra-synovial tissue layers. These complications might contribute to the incidence of local tissue damage such as skin hypopigmentation, atrophy of subcutaneous fat and muscle.4,5 From the previous studies, There are several anecdotal evidences and still controversy about the best injection technique, the most popular injection method, and route for the precision of landmark-guided injection of the knee in symptomatic osteoarthritis knee without an effusion.4,6,8, 9, 10, 11. A systematic review7 showed the superolateral approach with the leg in extension has highest accuracy of about 91% compared to the lateral midpatellar, the anterolateral, and the anteromedial approach (85%, 67%, and 72% respectively). Therefore, the development of injection technique is important.
In this study, We proposed a new modified anterolateral injection,12 modified from standard anterolateral technique compare with standard superolateral technique.13 We did not use the medial approach in our study because most of knee osteoarthritis have narrow medial and patellofemoral joint space, may be damage to chondral cartilage and led to pain.
The primary aim of this study was to compare the accuracy rate between the new modified anterolateral injection versus standard superolateral injection technique. Furthermore, the pain was evaluated in both techniques. We hypothesized that the new modified anterolateral injection should yield more accuracy rate of injection than the standard superolateral injection.
Material and Methods
Inclusion and exclusion criteria
This study was conducted with the formal approval of the human ethical committee of Thammasat University No.MTU-EC-OT-1-054/57. The inclusion criteria in this study were symptomatic knee arthritis without effusion whose confirm by clinical and radiographic evidence (included all grade of knee osteoarthritis by the Kellgren-Lawrence grading scale) with not response to adequate oral medications. While the exclusion criteria were the patients with the contraindications of intra-articular knee injection; infection, patients with bleeding disorder (ie, coagulopathy), hypersensitivity to knee injection agents. (ie, corticosteroid and hyaluronic acid).
Consecutive series of patients who met the inclusion criteria were recruited between May 2014 to May 2015. One-hundred and thirty-two knees were including in this prospective study. No patients were excluded. All were informed consent about the knee injection procedure and imaging process. Patients who agreed with the informed consent were consecutively included in the study.
Injection techniques
Before injection, Meticulous aseptic technique is performed. The point of entry was cleansed with povidone solution. Needle gauge No.25 was use in both techniques to decrease pain from injection (2007 WN Robert). Both techniques use one needle, for air and medical agent injection, and two syringe, first for air injection and medical agent respectively.
The standard anterolateral injection technique is injected from the anterolateral route in about 90-degree knee flexion and advanced the needle obliquely toward the intercondylar notch of the knee.17 For the new modified anterolateral injection technique, the patient was in supine or sitting position with knee flexion in 90°. The landmark was the intersection between 2 imaginary lines; the horizontal line from lower border the patella and the vertical line from Gerdy tubercle. The direction of needle tip is 10° parallel to posterior tibial slope, avoid cartilage and meniscus injury, and the needle tip was aimed toward the lateral tibial plateau, not into the intercondylar notch, avoid damage to structure in the intercondylar notch (eg.fatpad, ligamentum mucosum, anterior and posterior cruciate ligament)(Fig. 1). The needle was passed until it gently touches the cartilage of lateral femoral condyle and then move backward 1 mm. This technique also has the stopper to confirm the end point of injection that might be better than the intercondylar notch direction which has no the end point. After that the 10 ml volume of air without resistant was injected into joint which using the same technique as epidural injection. Backflow technique12 was observed to confirm that the needle tip was in the intra-articular space. If the backflow was not detected, the 10 ml volume of air was injected repeatedly. Once backflow was detected, medical agents were injected respectively. After injection, clearly audible squishing sounds were observed to confirm accurate of injection placement.14
Fig. 1.

The modified anterolateral approach of intra-articular injection of the right knee: the patient was in supine or sitting position with knee flexion in 90°. The landmark was the intersection between 2 imaginary lines; the horizontal line from lower border the patella and the vertical line from Gerdy tubercle. Backflow technique was observed to confirm that the needle tip was in the intra-articular space. If the backflow was not detected, the 10 ml volume of air was injected repeatedly. Once backflow was detected, medical agents were injected respectively.
For the standard superolateral injection technique, the patient is positioned supine on the examination table, with the legs extended. The patella and soft sport were palpated. The landmark was the intersection of 2 imaginary lines; horizontal line from the superior border of the patella, and another line intersecting the lateral border of the patella. The needle is aimed parallel to the anterior femoral cortex.
Air and medical agents were injected into knee joint respectively (Fig. 2).
Fig. 2.

The standard superolateral route of intra-articular injection of the left knee: the patient is positioned supine on the examination table, with the legs extended. The patella and soft sport were palpated. The landmark was the intersection of 2 imaginary lines; horizontal line from the superior border of the patella, and another line intersecting the lateral border of the patella. Backflow technique was observed to confirm that the needle tip was in the intra-articular space. If the backflow was not detected, the 10 ml volume of air was injected repeatedly. Once backflow was detected, medical agents were injected respectively.
The injection is performed by a single orthopaedic doctor whom have more than 15 years’ experience in the orthopaedic field. The VAS scale of injection is evaluated immediately after complete injection by the independent evaluator.
Evaluation of accuracy rate of intra-articular knee injection
The mini air-arthrography15 was use to evaluate the accuracy of knee injection technique; Post-injection anterior-posterior and lateral radiographs were taken immediately. In the case of extraarticular or uncertain positioning of the air the procedure was repeated. The accurate and inaccurate knee injection were demonstrated in Fig. 3 and Fig. 4.
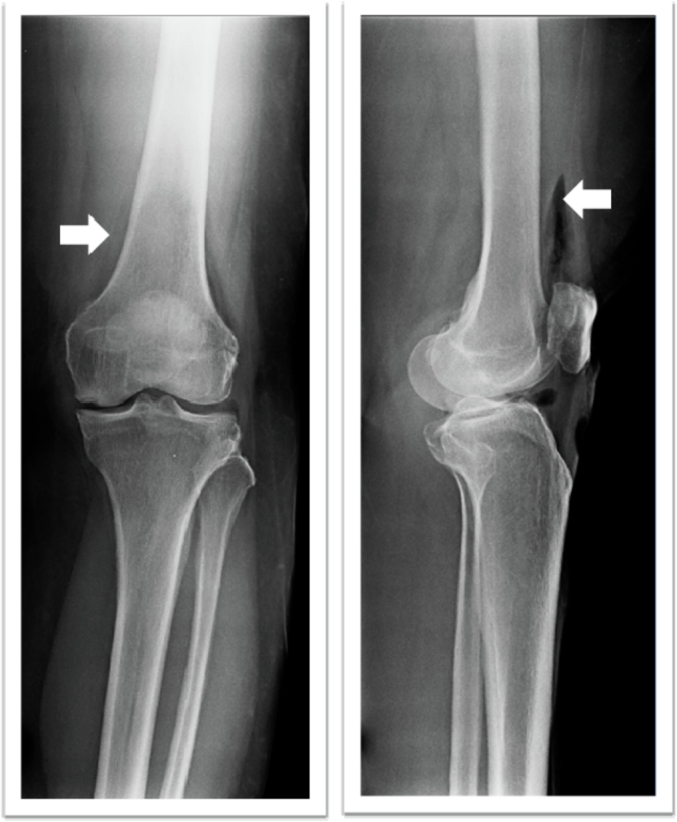
Fig. 3.

The inaccurate/extra-articular knee injection; Anterior-posterior and lateral radiographs of a post-injection knee. The air is distributed in the soft tissue outside the joint (arrow).
Fig. 4.
The Accurate/intra-articular knee injection; Anterior-posterior and lateral radiographs of the post-knee injection. The air is contained in the suprapatellar pouch (white arrow).
Statistical analysis
Sample size was calculated for a paired design determined that at least 130 knees per technique were required to detect a difference in accuracy of >10% with 80% power. Quantitative data were expressed as the means ± SD and qualitative data as numbers and percent. The accuracy of injection and pain visual analog scale of both techniques were compared by using the paired Student’s t-test. A value of p < 0.05 was considered to indicate statistical significance. Statistical analysis of the results was conducted using SPSS for Windows, version 10.0.
Results
One hundred and twenty-two knees were enrolled in the study. 66 knees were modified anterolateral group same as superolateral group. Accuracy rate of injection and pain from injection were documented. The accuracy rate of intra-articular knee injection was significantly greater with the modified anterolateral injection technique than the standard superolateral injection technique, 89% and 58% respectively with P = 0.000. In part of pain from injection, the pain visual analog scale was not significantly difference two techniques, 2.61 in modified technique and 2.65 in standard injection with P = 0.917. No adverse events were occurred in both groups. The summary of results was demonstrated in Table 1.
Table 1.
Summary of accuracy rate, pain and complications.
| Outcome | Injection technique |
|
|---|---|---|
| Modified anterolateral (N = 66) | Standard superolateral | |
| Accuracy rate | 89%* | 58%* |
| Pain VAS, (mean SD) | 2.61 (2.21) | 2.65 (2.76) |
| Complications | NA | NA |
*significantly different, P < 0.05 (comparison between Modified anterolateral and standard superolateral).
Discussion
This study demonstrated that the modified anterolateral approach of intra-articular knee injection was significantly greater accurate than the standard superolateral approach (89% vs. 58%). This approach should be one of a useful alternative landmark guided approach for intra-articular knee injection in patient with the symptomatic osteoarthritis knee without joint effusion.
The results of this study demonstrate the accuracy of the modified anterolateral approach for intra-articular knee injection, which is the important factor for successful treatment. The modified anterolateral approach for intra-articular knee injection overcomes the obstacle factors that affect to accurate of intra-articular knee injection. Firstly, the patient with obesity, this approach was reproducible and more comfortable because there was less soft tissue in anterolateral side of knee. Second, the patient with limited range of motion (eg. flexion contracture, limit flexion), it’s easily to make a knee injection in knee 90-degree flexion. The third, patient with marked narrowing joint space (eg. patellofemoral, medial tibiofemoral joint), this approach avoids to damage to articular or osteophyte because this approach didn’t penetrate the needle in the joint articular space but into intra-articular knee space. For these reasons, it’s important to use the modified anterolateral technique.
Intra-articular knee injection is the one of useful modality in conservative treatment.16 To achieve the maximal potential treatment, various medial agents should be delivered into the joint. Injection technique is one of the most important factor for accuracy of intra-articular knee injection especially in symptomatic osteoarthritis knee with no effusion.6 From previous studies about intra-articular knee injection in the symptomatic knee osteoarthritis without effusion, there are limited evidences and still controversy about injection technique and approach for the precision of landmark-guided injection(4, 6–11). The Backflow technique have benefit to prove of the intra-articular placement of needle during injection that have accuracy about 96.97%.12 A study reveals the high accurate in the full-flexion anterolateral injection in the dry osteoarthritis knee17 but the osteoarthritic knee patients may have more pain in the fully flexed of the knee so that we used the 90-degree knee flexion during the injection.
The weakness of this study including; 1. the lack of comparison with other approach of knee injection technique, 2. Relatively low number of participants may lead to low power of the accuracy, 3. We study of the short term follow up study (only immediate result of injections) so do not have the results of the follow-up period, and 4. no randomized double blind that may lead to some bias of the results. For further studies, the large number of cases should be considered to increase the accuracy of the study and the other approach of knee injection technique should be compared.
Conclusion
Our proposed technique, the modified anterolateral approach for intra-articular knee injection yield the favorable accuracy rate of injection and reliable approach of landmark-guided injection in symptomatic osteoarthritis knee without effusion.
Abbreviations
- OA
Osteoarthritis
- MAL
Modified anterolateral
- SL
Standard superolateral
- VAS
Visual Analog Scale
Ethics approval
This study was conducted with the formal approval of the human ethical committee of Thammasat University No.MTU-EC-OT-1-054/57. The consent was informed with written documents to all of participants before injections.
Conflict of Interest
None of the authors have relevant conflicts of interest to declare.
Funding Statement
No funding was obtained for this study.
Acknowledgements
We would like to thank Orthopaedics Department, Faculty of Medicine, Thammasat University and Thammasat Hospital for kindly support.
References
- 1.Jackson D.W., Simon T.M., Aberman H.M. Symptomatic articular cartilage degeneration : the impact in the new millennium. Clin Orthop Relat Res. 2001 Oct;(391 Suppl):S14–S25. 2001. [PubMed] [Google Scholar]
- 2.Cross M., Smith E., Hoy D. The global burden of hip and knee osteoarthritis: estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014;73(7):1323–1330. doi: 10.1136/annrheumdis-2013-204763. [DOI] [PubMed] [Google Scholar]
- 3.Litwic A., Edwards M.H., Dennison E.M., Cooper C. Epidemiology and burden of osteoarthritis. Br Med Bull. 2013;105:185–199. doi: 10.1093/bmb/lds038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Jones A., Regan M., Ledingham J., Pattrick M., Manhire A., Doherty M. Importance of placement of intra-articular steroid injections. BMJ. 1993;307(6915):1329–1330. doi: 10.1136/bmj.307.6915.1329. 1993. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Park S.K., Choi Y.S., Kim H.J. Hypopigmentation and subcutaneous fat, muscle atrophy after local corticosteroid injection. Kor J Anesthesiol. 2013;65(6 Suppl):S59–S61. doi: 10.4097/kjae.2013.65.6S.S59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Jackson D.W., Evans N.A., Thomas B.M. Accuracy of needle placement into the intra-articular space of the knee. J Bone Joint Surg Am. 2002;84(9):1522–1527. doi: 10.2106/00004623-200209000-00003. 2002. [DOI] [PubMed] [Google Scholar]
- 7.Hermans J., Bierma-Zeinstra S.M., Bos P.K., Verhaar J.A., Reijman M. The most accurate approach for intra-articular needle placement in the knee joint: a systematic review. Semin Arthritis Rheum. 2011;41(2):106–115. doi: 10.1016/j.semarthrit.2011.02.007. [DOI] [PubMed] [Google Scholar]
- 8.Toda Y., Tsukimura N. A comparison of intra-articular hyaluronan injection accuracy rates between three approaches based on radiographic severity of knee osteoarthritis. Osteoarthritis Cartilage. 2008;16(9):980–985. doi: 10.1016/j.joca.2008.01.003. [DOI] [PubMed] [Google Scholar]
- 9.Daley E.L., Bajaj S., Bisson L.J., Cole B.J. Improving injection accuracy of the elbow, knee, and shoulder: does injection site and imaging make a difference? A systematic review. Am J Sports Med. 2011;39(3):656–662. doi: 10.1177/0363546510390610. [DOI] [PubMed] [Google Scholar]
- 10.KEITH M. SMART. Approaches to Intra-Articular Injections for Dry Knee Osteoarthritis : the accuracy of needle placement may have efficacy and safety implications. J Muscoskel Med. 2012;29(4) [Google Scholar]
- 11.Douglas R.J. Aspiration and injection of the knee joint: approach portal. Knee Surg Relat Res. 2014;26(1):1–6. doi: 10.5792/ksrr.2014.26.1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Luc M., Pham T., Chagnaud C., Lafforgue P., Legre V. Placement of intra-articular injection verified by the backflow technique. Osteoarthritis Cartilage. 2006;14(7):714–716. doi: 10.1016/j.joca.2006.02.013. [DOI] [PubMed] [Google Scholar]
- 13.Maricar N., Parkes M.J., Callaghan M.J., Felson D.T., O’Neill T.W. Where and how to inject the knee--a systematic review. Semin Arthritis Rheum. 2013;43(2):195–203. doi: 10.1016/j.semarthrit.2013.04.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Glattes R.C., Spindler K.P., Blanchard G.M., Rohmiller M.T., McCarty E.C., Block J. A simple, accurate method to confirm placement of intra-articular knee injection. Am J Sports Med. 2004;32(4):1029–1031. doi: 10.1177/0363546503258703. 2004. [DOI] [PubMed] [Google Scholar]
- 15.Bliddal H. Placement of intra-articular injections verified by mini airarthrography. Ann Rheum Dis. 1999;58(10):641–643. doi: 10.1136/ard.58.10.641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ayhan E., Kesmezacar H., Akgun I. Intraarticular injections (corticosteroid, hyaluronic acid, platelet rich plasma) for the knee osteoarthritis. World J Orthoped. 2014;5(3):351–361. doi: 10.5312/wjo.v5.i3.351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hussein M. An accurate full-flexion anterolateral portal for needle placement in the knee joint with dry osteoarthritis. J Am Acad Orthop Surg. 2017 Jul;25(7):e131–e137. doi: 10.5435/JAAOS-D-16-00338. doi: 0.5435/JAAOS-D-16-00338. [DOI] [PubMed] [Google Scholar]