

Abstract
Laparoscopic surgery has spread worldwide and become a standard procedure among many abdominal surgical fields. The incidence of postoperative adhesion, which is a typical postoperative complication, is considered low compared with that after laparotomy. However, once complications develop, such as adhesion-induced intestinal obstruction and chronic abdominal pain, the low-invasiveness of laparoscopic surgery can decrease markedly. While we have previously used a sheet-type anti-adhesion barrier, it requires a specific technique in many cases when it is applied in the abdominal cavity. In this study, we used a spray-type anti-adhesion barrier, which is considered simple to apply, as an adhesion-preventing absorbable barrier following laparoscopic surgery.
INTRODUCTION
It is reported that adhesions occur in more than 90% of patients who undergo abdominal surgery, and small bowel obstruction that can be caused by this is one of postoperative complications. Postoperative intestinal obstruction may damage its minimally invasiveness in laparoscopic surgery and its prevention is important. However, in laparoscopic surgery, there are cases where techniques and ingenuity are necessary to use anti-adhesion agents in precise parts. In this report, we report the experience of using spray type adhesion prevention absorbable barrier which is easy to use regardless of the site [1–6].
PROCEDURE
The adhesion-proof absorbable barrier is used around the peritoneal exfoliation or injured area caused by the surgical procedure just before the end of laparoscopic surgery. Used in the intestinal motility section, mesenteric detachment section, blood vascular dissection part or skin incision section to prevent adhesion. For the operation of the left side colon, it is used in the processing section of the descending colon peeling section or the lower mesenteric vascular area, and in the case of operation on the right colon, it is used for the vessel processing section of the ascending colon peeling section and the superior mesenteric vascular region. In case of rectal surgery, it is used in the pelvis which is largely peritoneal defect on the rectum detachment side.
The spray-type anti-adhesion barrier (Ad Spray type L®(TERUMO Corp, Tokyo, Japan)) consists of a dissolution kit and a Sprayer Kit (Fig. 1a), and the kit is assembled after combining the two drugs. The regulator is then connected to a compressed air supply for use (Fig. 1b). The nozzle is 334 mm long, and the angle of the tip is adjustable from 0-90 degrees, and the rotation of the shaft is 360 degrees. However, while it is difficult to secure the working space by fine-tuning the angle and rotation of the tip, it is possible to easily apply the spray to the desired part. In addition, since gelation after application requires about 10 seconds, some degree of viscosity is obtained, and it is useful to maintain the adhesion barrier at the area of the curvature and the damaged peritoneal portion of the abdominal wall side. We apply the barrier to the port insertion area from within the peritoneal cavity (Fig. 2a) and the peeling surface at the small incision. In particular, the peeling surface is widely used, such as the pelvic floor at the time of milestone surgery, and it is difficult to use the sheet type anti-adhesion barrier in the Hartmann operation (Fig. 2b). In order for the barrier to remain in the target region, this preparation must remain viscous after application. The area of the coating is similar to the sheet type.
Figure 1:
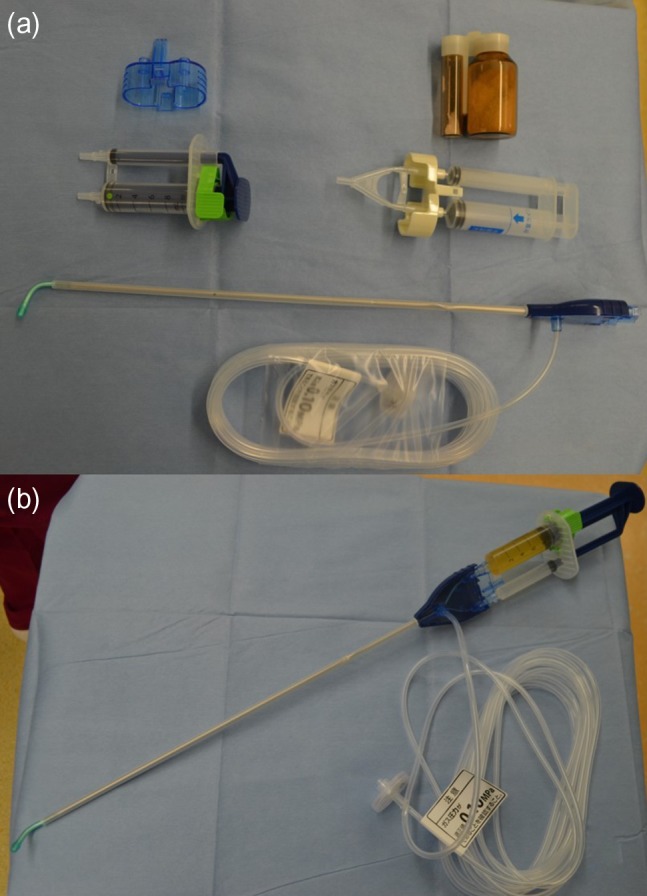
A spray-type anti-adhesion barrier kit. (a) Before assembly. (b) After assembly.
Figure 2:
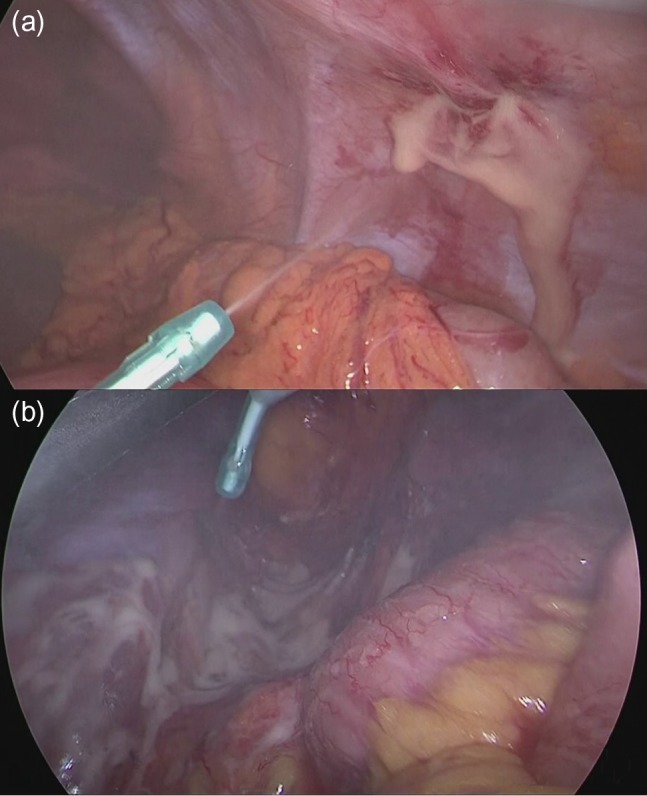
(a) Apply the barrier to the port insertion area. (b) Spraying the peeled surface of pelvic cavity in the Hartmann operation.
DISCUSSION
There are small bowel obstructions as one of the major postoperative complications, and it is reported that 75% of small bowel obstruction is caused by postoperative adhesion. Although laparoscopic surgery is said to have less postoperative adhesions, it is reported that 2.5% of laparoscopic surgery causes small bowel obstruction. In laparoscopic surgery, countermeasures are also necessary. In the case of using adhesion-prohibiting absorbable barrier in the peritoneal lesion in the peritoneal cavity in laparoscopic surgery, in the case of conventional sheet type adhesion-prohibiting absorbable barrier, techniques may be required at the time of affixing, and its insertion and pasting Devices have been reported.
The sheet-type anti-adhesion barrier may require a novel technique when it is attached, as sticking of the device has been reported during insertion1-3. It was considered that application of the adhesion spray during laparoscopic surgery was easy and useful. However, there is the restriction that it is necessary to use it within 60 minutes after combination of the agents, which takes time and requires preparation compared with the sheet type. Moreover, it is not possible for use in patients who are allergic to the corn and have glycogenosis in response to the raw material. Furthermore, its application requires some experience and time for preparation compared with the use of the sheet type, which could be disadvantageous. Additional accumulation of cases, including evaluation of the prevention of adhesion after use of the adhesion-preventing absorbable barrier, may be necessary.
CONFLICT OF INTEREST STATEMENT
None declared.
REFERENCES
- 1. Becker JM, Dayton MT, Fazio VW, Beck DE, Stryker SJ, Wexner SD, et al. Prevention of postoperative abdominal adhesions by a sodium hyaluronate-based bioresorbable membrane: a prospective, randomized, double-blind multicenter study. J Am Coll Surg 1996;183:297–306. [PubMed] [Google Scholar]
- 2. Menzies D, Ellis H. Intestinal obstruction from adhesions—how big is the problem? Ann R Coll Surg Engl 1990;72:60–3. [PMC free article] [PubMed] [Google Scholar]
- 3. Taylor GW, Jayne DG, Brown SR, Thorpe H, Brown JM, Dewberry SC, et al. Adhesions and incisional hernias following laparoscopic versus open surgery for colorectal cancer in the CLASICC trial. Br J Surg 2010;97:70–8. [DOI] [PubMed] [Google Scholar]
- 4. Koketsu S, Sameshima S, Okuyama T, Yamagata Y, Takeshita E, Tagaya N, et al. An effective new method for the placement of an anti-adhesion barrier film using an introducer in laparoscopic surgery. Tech Coloiproctol 2015;19:551–3. [DOI] [PubMed] [Google Scholar]
- 5. Nakase Y, Nakamura K, Sougawa A, Nagata T, Mochizuki S, Kitai S, et al. novel procedure for introducing large sheet-type surgical material with a self-expanding origami structure using a slim trocar (chevron pleats procedure). Surg Endosc 2017;31:3749–54. [DOI] [PubMed] [Google Scholar]
- 6. Nakagawa H, Yoshimura K, Nishimura K, Hachisuga T. Novel technique for adhesion barrier insertion by using cut-off surgical glove fingers in laparoscopic surgery. J Obstet Gynaecol Res 2017;43:909–12. [DOI] [PubMed] [Google Scholar]