

Abstract
Background
We here present the first case report of takotsubo cardiomyopathy that developed during rewarming of a patient with severe accidental hypothermia with extracorporeal membrane oxygenation.
Case
A 74‐year‐old woman was found unresponsive outdoors and suffered cardiopulmonary arrest during transfer to our hospital. On arrival, she was still in cardiopulmonary arrest. Veno‐arterial extracorporeal membrane oxygenation was initiated for resuscitation and rewarming. After admission to the intensive care unit, her blood pressure suddenly dropped, and coronary angiography on day 2 indicated intact coronary arteries. Left ventriculography showed typical takotsubo‐like dysfunction in the end‐systolic phase, which led to the diagnosis of takotsubo cardiomyopathy. Left ventricular wall motion gradually improved, and echocardiography on day 6 revealed that abnormalities in the left ventricular wall motion had almost disappeared.
Conclusion
Takotsubo cardiomyopathy might arise during rewarming of patients with severe accidental hypothermia.
Keywords: Accidental hypothermia, cardiopulmonary arrest, extracorporeal membrane oxygenation, rewarming, takotsubo cardiomyopathy
Background
Takotsubo cardiomyopathy is defined as a transient cardiac dysfunction that is commonly triggered by physical or emotional stress.1 Wall‐motion abnormalities of takotsubo cardiomyopathy are typically characterized by apical systolic dysfunction and hyperdynamic basal contraction; therefore, it can be complicated by heart failure. The underlying pathophysiology remains uncertain; however, excess catecholamine release is considered as a trigger for takotsubo cardiomyopathy.1
Accidental hypothermia is defined as an unintentional drop of the core body temperature below 35°C.2 The risk of cardiac arrest substantially increases when the core temperature drops below 28°C.2 Rewarming of patients with severe accidental hypothermia is associated with complications, such as cardiovascular collapse, often termed as rewarming shock. This condition is defined as a decline in the cardiac output that results in a sudden drop in the arterial blood pressure.3 Here, we report the first case of a patient who developed takotsubo cardiomyopathy during rewarming for severe accidental hypothermia with extracorporeal membrane oxygenation (ECMO).
Case presentation
A 74‐year‐old woman was found unresponsive outdoors, and the ambient temperature on the arrival of emergency medical services to the scene was −1.7°C. At that time, she was in shock, with a body temperature of 24.6°C. During her transfer to our hospital, she suffered cardiopulmonary arrest (CPA). On arrival, she was still in CPA, and her cardiac rhythm was ventricular fibrillation. Veno‐arterial ECMO was initiated for resuscitation and rewarming, and she became responsive to commands after a few minutes. Rewarming was aimed at increasing her body temperature to 36°C as rapidly as possible with the inclusion of a heater‐cooler device with ECMO. Whole‐body computed tomography scan with contrast enhancement showed no abnormalities that could explain the cause of CPA. She was admitted to the intensive care unit (ICU), and the return of spontaneous circulation was achieved at the time of admission without adrenaline and defibrillation. The left ventricular (LV) ejection fraction was approximately 60% estimated visually.
Her blood pressure suddenly dropped 1 h after the ICU admission, and echocardiography showed severe diffuse hypokinesis of the LV wall and apical akinesis. Coronary angiography undertaken on day 2 indicated that coronary arteries were intact (Fig. 1A,B). Left ventriculography showed typical takotsubo‐like dysfunction in the end‐systolic phase and hyperdynamic basal contraction, and apical akinesis (Fig. 1C,D) as well as a T‐wave inversion in multiple leads on the electrocardiogram (Fig. 2). Based on these findings, she was diagnosed with takotsubo cardiomyopathy. Left ventricular wall motion gradually improved, and she was taken off ECMO on day 3 (Fig. 3) and extubated on day 5. Echocardiography on day 6 showed that abnormalities in the LV wall motion had almost disappeared.
Figure 1.
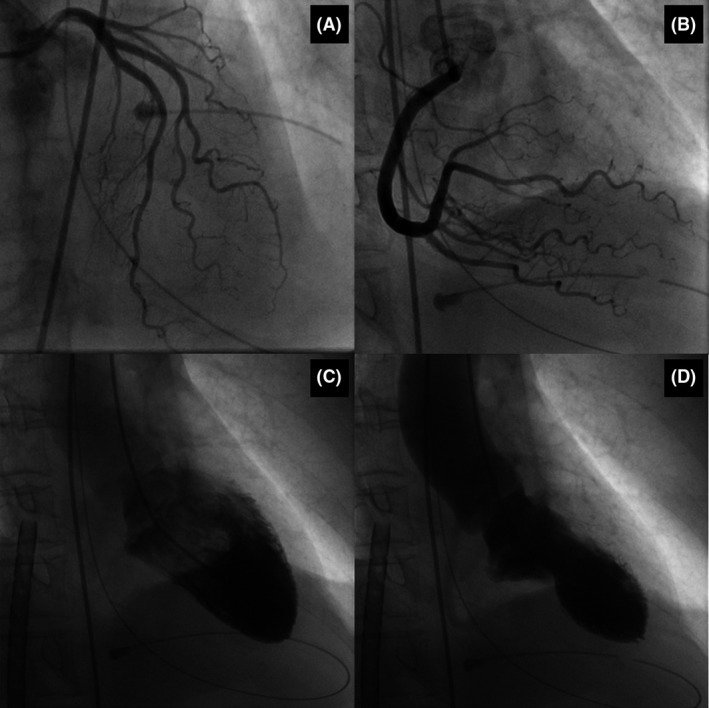
Coronary angiogram and left ventriculogram of a 74‐year‐old woman who suffered cardiopulmonary arrest due to severe accidental hypothermia. Left (A) and right (B) coronary arteries show the absence of coronary artery disease. The left ventriculogram shows hyperdynamic basal contraction in the presence of akinesis of the apical segments (C, D).
Figure 2.
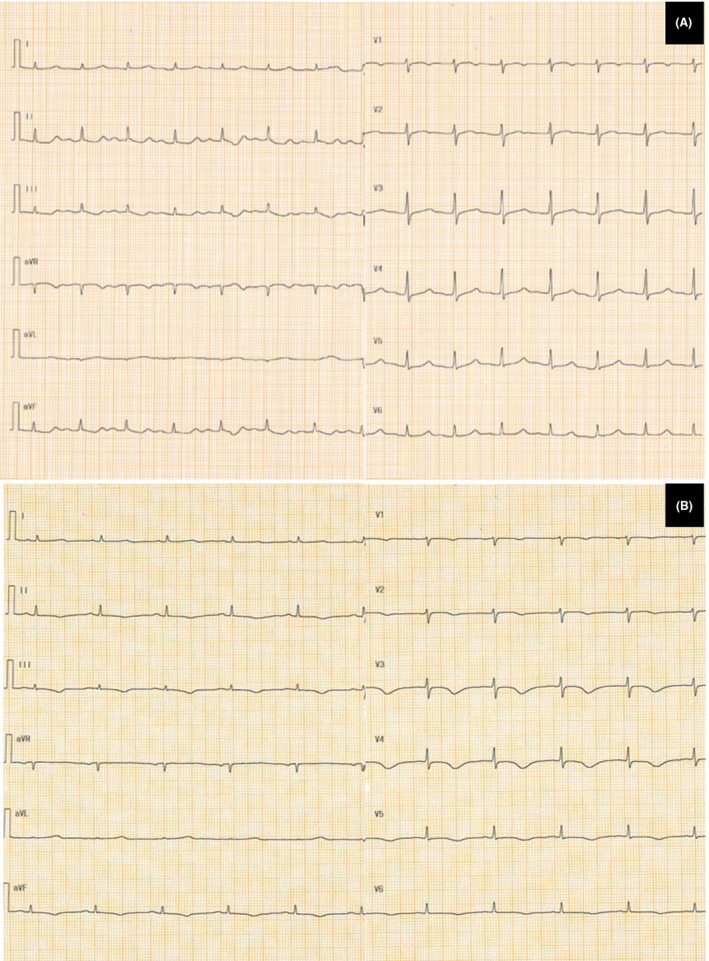
Electrocardiogram on admission (A) and day 2 (B) of a 74‐year‐old woman who suffered cardiopulmonary arrest due to severe accidental hypothermia. A new T‐wave inversion in multiple leads appears on day 2.
Figure 3.
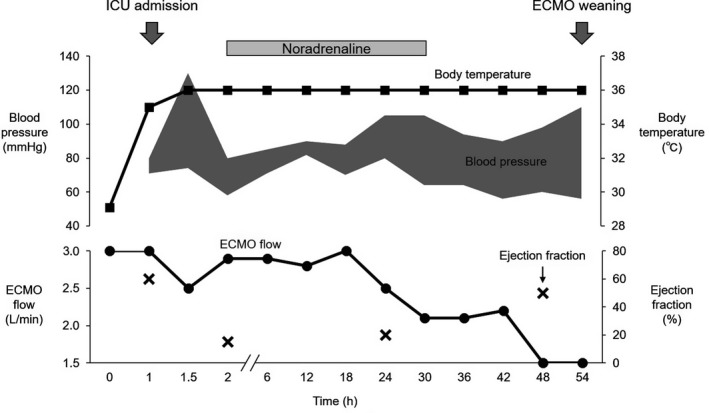
Clinical course from admission to extracorporeal membrane oxygenation (ECMO) weaning of a 74‐year‐old woman who suffered cardiopulmonary arrest due to severe accidental hypothermia. ICU, intensive care unit.
She was discharged from the ICU on day 8. She confessed having ingested several sleeping pills. Therefore, she was moved to the psychiatric ward to receive psychological treatment on day 12 and was discharged on day 43 without neurological deficits.
Discussion
The present case highlights two important clinical issues: (i) takotsubo cardiomyopathy can develop during rewarming of patients with severe accidental hypothermia, (ii) ECMO is an effective life‐saving approach for severe LV dysfunction from takotsubo cardiomyopathy that might develop during rewarming. Hypothermia‐induced takotsubo cardiomyopathy has been previously reported, but diabetic ketoacidosis was a coexisting condition in those patients.4, 5
Hypotension, or rewarming shock, can occur during or after rewarming in patients with severe accidental hypothermia.6 The pathophysiology of rewarming shock is poorly understood; however, studies have shown that peripheral vasodilation and severe cardiac dysfunction are causes of rewarming shock.7, 8 Our experience in the present case raises the possibility that cardiac dysfunction, which was previously attributed to rewarming shock, is associated with takotsubo cardiomyopathy.
In a cold environment, catecholamines are released from the adrenal medulla and reach peripheral sympathetic nerve endings.9 Catecholamine secretion from the sympathicoadrenal medullary system is associated with metabolic and cardiovascular responses that are critical for heat production and heat loss prevention.10 Urinary catecholamine levels have been reported to be significantly increased in fatalities due to hypothermia compared with those due to other causes.9 Although the exact factors involved in the pathogenic mechanism underlying takotsubo cardiomyopathy remain unclear, excessive catecholamine secretion and sympathetic hyperexcitation have been proposed as the most likely factors. In the present case, the patient's circulation rapidly improved with ECMO, suggesting that takotsubo cardiomyopathy was induced by the rapid dissemination of increased catecholamines released during hypothermia.
Extracorporeal membrane oxygenation is a safe and efficient rewarming strategy in patients with severe hypothermia11 and is also useful for circulatory support for refractory CPA or severe cardiogenic shock, such as takotsubo cardiomyopathy.12 Therefore, it can be an effective life‐saving treatment approach for takotsubo cardiomyopathy during rewarming of patients suffering from severe hypothermia, as shown in the present patient.
Conclusion
In severe accidental hypothermia, takotsubo cardiomyopathy could occur during rewarming because of the rapid dissemination of increased catecholamines during hypothermia, and ECMO should be considered as an effective life‐saving rewarming strategy in such patients.
Disclosure
Approval of the research protocol: N/A.
Informed consent: The patient provided informed consent for publication of this case report.
Registry and the registration no. of the study/trial: N/A.
Animal studies: N/A.
Conflicts of interest: None.
Funding Information
No funding information provided.
References
- 1. Yoshikawa T. Takotsubo cardiomyopathy, a new concept of cardiomyopathy: clinical features and pathophysiology. Int. J. Cardiol. 2015; 182: 297–303. [DOI] [PubMed] [Google Scholar]
- 2. Brown DJ, Brugger H, Boyd J et al Accidental hypothermia. N. Engl. J. Med. 2012; 367: 1930–8. [DOI] [PubMed] [Google Scholar]
- 3. Dietrichs ES, Haheim B, Kondratiev T et al Effects of hypothermia and rewarming on cardiovascular autonomic control in vivo. J. Appl. Physiol. 2018; 124: 850–9. [DOI] [PubMed] [Google Scholar]
- 4. Katayama Y, Hifumi T, Inoue J et al A case of Takotsubo cardiomyopathy induced by accidental hypothermia and diabetic ketoacidosis. BMJ Case Rep. 2013; 2013: bcr2012008143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Davin L, Legrand V, Legrand D. A frozen heart. Eur. Heart J. 2009; 30: 1827. [DOI] [PubMed] [Google Scholar]
- 6. Tveita T. Rewarming from hypothermia Newer aspects on the pathophysiology of rewarming shock. Int. J. Circumpolar Health 2000; 59: 260–6. [PubMed] [Google Scholar]
- 7. Lloyd EL. Accidental hypothermia. Resuscitation 1996; 32: 111–24. [DOI] [PubMed] [Google Scholar]
- 8. Wold RM, Kondratiev T, Tveita T. Myocardial calcium overload during graded hypothermia and after rewarming in an in vivo rat model. Acta Physiol. (Oxf) 2013; 207: 460–9. [DOI] [PubMed] [Google Scholar]
- 9. Palmiere C, Teresinski G, Hejna P et al Diagnostic performance of urinary metanephrines for the postmortem diagnosis of hypothermia. Forensic Sci. Med. Pathol. 2014; 10: 518–25. [DOI] [PubMed] [Google Scholar]
- 10. Hanhela R, Hollmen A, Huttunen P et al Plasma catecholamines, corticosterone, glucose and fatty acids concentrations and mean arterial pressure and body temperature in haemorrhagic hypovolaemia, hypothermia and a combination of these in the rabbit. Acta Physiol. Scand. 1990; 139: 441–9. [DOI] [PubMed] [Google Scholar]
- 11. Paal P, Gordon L, Strapazzon G et al Accidental hypothermia‐an update: the content of this review is endorsed by the International Commission for Mountain Emergency Medicine (ICAR MEDCOM). Scand. J. Trauma Resusc. Emerg. Med. 2016; 24: 111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Bonacchi M, Maiani M, Harmelin G et al Intractable cardiogenic shock in stress cardiomyopathy with left ventricular outflow tract obstruction: is extra‐corporeal life support the best treatment? Eur. J. Heart Fail. 2009; 11: 721–7. [DOI] [PubMed] [Google Scholar]