

Abstract
Respiratory disorders are responsible for considerable morbidity and mortality in children. Spirometry is a useful investigation for diagnosing and monitoring a variety of paediatric respiratory diseases, but it is underused by primary care physicians and paediatricians treating children with respiratory disease. We now have a better understanding of respiratory physiology in children, and newer computerised spirometry equipment is available with updated regional reference values for the paediatric age group. This review evaluates the current literature for indications, test procedures, quality assessment, and interpretation of spirometry results in children. Spirometry may be useful for asthma, cystic fibrosis, congenital or acquired airway malformations and many other respiratory diseases in children. The technique for performing spirometry in children is crucial and is discussed in detail. Most children, including preschool children, can perform acceptable spirometry. Steps for interpreting spirometry results include identification of common errors during the test by applying acceptability and repeatability criteria and then comparing test parameters with reference standards. Spirometry results depict only the pattern of ventilation, which may be normal, obstructive, restrictive, or mixed. The diagnosis should be based on both clinical features and spirometry results. There is a need to encourage primary care physicians and paediatricians treating respiratory diseases in children to use spirometry after adequate training.
Keywords: spirometry, preschool children, forced vital capacity, forced expiratory volume in one second
Introduction
Respiratory diseases account for the majority of all paediatric hospital visits and hospitalisations all over the world, with significant morbidity and mortality. Spirometry is a procedure that measures the rate of changing lung volumes during forced breathing manoeuvres and it is used to diagnose, manage, and monitor patients with a variety of respiratory diseases. Children have a dynamic developmental phase during which lung volume size and airway size change with increasing age. Spirometry parameters are influenced by weight, height, age, sex, environmental factors, ethnicity, prematurity, patient cooperation and effort, and technical factors.1,2 Spirometry is frequently used in adults while managing respiratory conditions. Although it is not difficult to perform spirometry in children in the primary care office setting,3,4 it is frequently underused in the paediatric age group. Dombkowski et al.5 conducted a survey to assess the use of spirometry by physicians in paediatric primary care who were treating children with asthma and found that only half of them were using spirometry and nearly half did not interpret the spirometry results correctly.
In the past, spirometry was considered difficult to perform in children of preschool age (2–6 years) as they are not able to perform voluntary breathing manoeuvres as efficiently as older children and adults. However, in the current era with the availability of better spirometry equipment with incentives and modified criteria for acceptability and repeatability, it is possible to perform reliable spirometry tests even in preschool children by trained personnel.6–9 A variety of methods other than spirometry have also been adopted to assess lung function in infants and young children, such as the interrupter technique, the forced oscillation technique,10 gas washout techniques, tidal breathing techniques, and the rapid thoracoabdominal compression manoeuvre.11 Some of these manoeuvres may require sedation and are usually performed in advanced respiratory laboratories. These will not be discussed in this review.
Spirometry has been found to be safe with regard to inducing cardiac arrhythmias in both children and adults.12 It is therefore prudent for primary care physicians and paediatricians who treat respiratory diseases in children to consider the role of spirometry in this age group and the issues of underutilisation and incorrect interpretation of spirometry tests.
This review aims to summarise the current literature regarding indications, test procedure, quality assessment, and interpretation of spirometry results in children.
Search methodology
For the purpose of this review, PubMed was searched using the keywords ‘spirometry’ OR ‘pulmonary function test’ OR ‘lung function test’ with filters activated: English language, child; birth to 18 years, and field; Title. The search was last performed on 19 November 2012. A total of 273 articles were found by the search. The title and abstract of these articles were screened and full texts of relevant articles were obtained. The references of selected articles were also screened to find other relevant articles.
Types of spirometer
A variety of spirometers are available on the market. The basic handheld spirometers provide forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) values that can be compared manually with available predicted normal values. The next generation of spirometers provide graphs (usually volume-time curves) visually with or without printouts. The most recent electronic spirometers calculate the percentage of the predicted normal values based on reference values already programmed after entering patient details and performing the test. Most of these recent spirometers have built-in printers and can also be connected to a computer. When selecting a spirometer it is desirable that the equipment fulfils American Thoracic Society/European Respiratory Society (ATS/ERS) recommendations for spirometry (which are regularly updated).13,14 As the volume of air is affected by the environment, the spirometry parameters should be presented at body temperature and ambient pressure saturated with water vapour (BTPS). The calibration, maintenance, and infection control measures (e.g. use of disposal mouthpiece or use of filters) should be implemented in accordance with the recommendations of the manufacturer of the equipment.13 Many newer generation spirometers do not require calibration daily or after a certain number of tests, as used to be the case. The respiratory technician or physician performing the spirometry tests requires training. It is suggested that at least five tests a week (20/month) are required to maintain competency in a person with initial competency.13
Indications for spirometry in children
Spirometry is commonly indicated for children with chronic cough, persistent wheezing,15 and for the diagnosis and monitoring of asthma16,17 and cystic fibrosis.18,19 It must be included as a necessary component in reviewing asthma control and disease activity in cystic fibrosis in children as well as in adults. It is also frequently used to measure lung function in a number of diseases that affect the lungs including haematological disorders such as transfusion-dependent thalassaemia major20 and sickle cell anaemia,21 haemato-oncology conditions,22 connective tissue disorders, ataxia telangiectasia,23 and chest deformities such as pectus excavatum. Spirometry is helpful in ascertaining preoperative lung function in flaccid neuromuscular scoliosis (e.g. muscular dystrophy, spinal muscular atrophy, and cerebral palsy).24 Constant et al.15 used field spirometry as a measure to screen schoolchildren for respiratory diseases. The role of spirometry during an acute exacerbation of asthma in children is not well established. In a study by Schneider et al.,25 many children presenting to the emergency department with an acute moderate to severe exacerbation of asthma were unable to perform acceptable spirometry tests, whereas in a study by Langhan et al.,26 most children performed acceptable spirometry tests during an acute exacerbation. In both studies, correlation was not good between clinical severity and spirometry measurements.25,26 Uchida reported three cases of double aortic arch in children who were initially misdiagnosed as having asthma and a correct diagnosis was made based on spirometry findings.27 Many research studies on asthma and cystic fibrosis in children had spirometry parameters (especially FEV1, FVC, and FEV1/FVC) as one of the primary or secondary outcomes since these parameters are objective and less prone to bias. Brouwer et al.28 assessed the usefulness of home spirometry in children with non-specific lower respiratory tract symptoms to diagnose or exclude asthma and found that it had a limited role with a sensitivity and specificity of 50% and 72%, respectively, for peak expiratory flow (PEF) variation and a sensitivity and specificity of 45% and 92%, respectively, for FEV1 variation.
Contraindications to spirometry
Although there is no absolute contraindication for spirometry, the following conditions are considered relative contraindications: presence of respiratory tract infection (e.g. influenza), haemoptysis of unknown origin, pneumothorax, aneurysm, uncontrolled hypertension, recent thoracic, abdominal or eye surgery, nausea, vomiting or pain, and confusion or dementia.14
How to perform the spirometry test
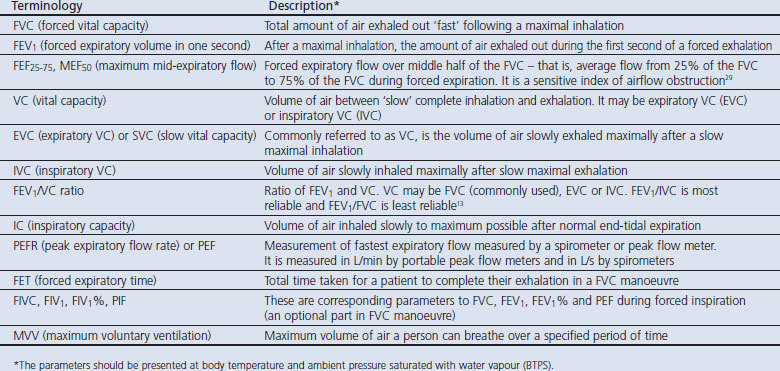
The various terminologies related to spirometry are described in Table 1. The spirometry test technique is similar in adults and children aged >6 years. The person performing the test should have the ability to identify common errors and to interpret the results of spirometry.13 Appropriate equipment should be selected and prepared as needed (e.g. calibrated if required). The procedure should be explained to the patient in a friendly way. Patients should be asked if they have recently taken any medications such as bronchodilators or β-blockers, when they last had a meal (as heavy meals can affect performance of the test, possibly causing some restriction), and they should be advised not to wear tight or restrictive clothes that could interfere with the test. The patient's weight and height should be measured and entered into software along with the name, ID, age, sex, and race. The position of the patient for the test may be sitting (preferred) or standing. To perform a manoeuvre, a new disposable mouthpiece is attached to the spirometer and a nose clip is used or the patient is asked to pinch his/her nose. The next step is selection of the appropriate test manoeuvre (FVC, vital capacity (VC) or maximum voluntary ventilation (MVV)) from the spirometer and the test is performed accordingly. The FVC manoeuvre is most useful and is usually the only one performed.
Table 1. Terminology in relation to spirometry with explanations.
FVC test manoeuvre
The patient is asked for 2–3 tidal breaths in and out (optional) and to inhale deeply (inhale fast and deep) with the lips sealed tightly around the mouthpiece. The patient is then asked to blow air through the mouthpiece as fast as possible (to blast air from the lungs) and to continue to blow until no air is left to exhale. During instructions to children, some phrases may be used such as “sucking on a straw” for a deep inspiration, “blowing out birthday candles” for a forceful expiration, and “keep blowing and keep blowing” for complete exhalation until no air is left. The optional part of the FVC manoeuvre is inhalation as fast and completely as possible at the end of forced expiration if one requires FIVC, FIV1, FIV1%, and PIF parameters. The test should be repeated at least three times and checked for acceptability and repeatability as shown below. If the results are not acceptable, the test may be repeated a maximum of eight times before abandoning it.
In preschool children (2–6 years of age), nearly 82.6% (214/259) of children aged 3–6 years, 75% of children aged 2–5 years, and 55% (196/355) of children aged 3–5 years were able to perform technically acceptable and reproducible spirometry manoeuvres in studies by Eigen et al.,29 Aurora et al.,6 and Crenesse et al.,30 respectively. The test may be performed in a similar way in preschool children to that described above, with the same minimum number of attempts (i.e. three), but the maximum number is not recommended in this age group.
During the test it is essential to ensure that the child is cooperative and follows the instructions, that there is a tight seal around the mouthpiece, the mouthpiece is not obstructed, inhalation is complete, the start is fast and forceful, there is no pause, no other breath or cough during exhalation, no exhalation through the nose, and the blow is continued until exhalation is complete, as suggested by a plateau on the volume-time graph. Use of computer-generated incentive graphics may be helpful to encourage preschool children to perform spirometry.31 Incentives may be flow-driven, volume-driven, or both flow- and volume-driven; the latter two are considered to be better than the first one when performing spirometry in children.32 Incentives are not always necessary as spirometry may be possible in young children even without them.33
Although no systematic differences in FEV1 or FVC measurements in children with and without nose clips have been described,34 the use of a nose clip is recommended while performing spirometry to avoid part of the blow through the nose. Use of bacterial filters in children was not found to produce any clinically significant changes in spirometry measurements.35
VC/IVC test manoeuvre
The VC test should be selected on the spirometer if available. These are not forceful manoeuvres and should be performed in a relaxed manner. For expiratory vital capacity (EVC) or VC, after several tidal breaths, as much air as possible should be inspired slowly into the lungs and then as much air as possible should be expired slowly. For inspiratory vital capacity (IVC), after several tidal breaths, as much air as possible should be expired slowly and then as much air as possible should be inspired slowly. For inspiratory capacity (IC), after several tidal breaths, the patient should inspire slowly and completely from end tidal expiration to total lung capacity. The spirometer will measure IC in the EVC manoeuvre also. There should be a maximum of four manoeuvres for the VC/IVC test. If both VC and FVC manoeuvres are performed at the same setting, the VC test should be performed before the FVC test because FVC may produce fatigue and air trapping in severe airway obstruction resulting in false measurements in the VC test.13
MVV test manoeuvre
MVV does not provide additional information if FEV1 measurements are available. To perform the MVV test, a few tidal breaths should be taken followed by forced inhalation and exhalation as rapidly (at a rate of at least 30/min) and deeply as possible for at least 12 s or more.
How to interpret spirometry results
The steps for interpreting spirometry results include: (1) assessing the tests for acceptability and repeatability; (2) identifying the spirometry pattern (normal, obstructive, restrictive, or mixed); (3) grading the severity of the pattern identified; (4) diagnosing and treating the condition or investigating further.
Assessment of acceptability and repeatability of tests
There are usually two types of graphs in spirometry — flow-volume curve and volume-time curve — and both are useful for optimum quality control. The flow-volume curve is particularly useful for evaluating the initial part of the FVC manoeuvre and the volume-time curve is useful for assessing the later part of the FVC manoeuvre. Before assessing spirograms, any errors or artifacts in the spirometry procedure should be detected by looking at the shape of the flow-volume curve. The errors may include hesitation in test, premature finish (defined as flow ceasing at more than 10% of peak flow), premature finish and restart (more than one breathing attempt), poor effort, and cough (Figure 1). Individual spirograms are acceptable if they are free from errors or artifacts, have good starts, and satisfactory expiration in accordance with ATS/ERS standards (Table 2).14
Figure 1. Errors in spirometry test identified by flow-volume curves: (A) poor patient effort; (B) cough; (C) premature finish and restart.

Table 2. Acceptability and repeatability criteria for spirometry maneuvers in children. Reproduced from Miller et al.14 with permission of the European Respiratory Journal.
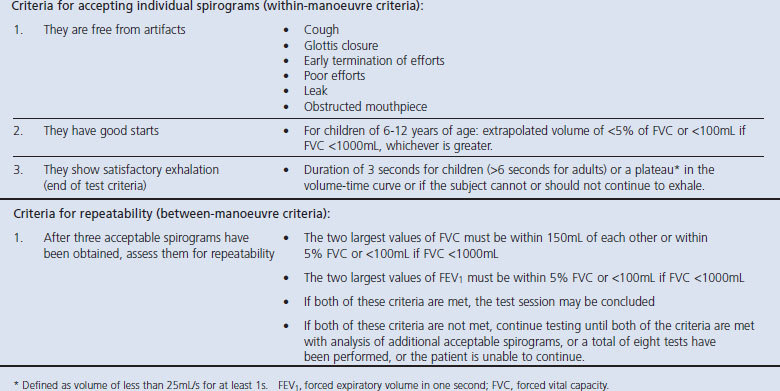
In preschool children, some modifications in the criteria have been suggested in an ATS/ERS statement on pulmonary function testing in preschool children.32 In these children, an extrapolated volume of <80mL or 12.5% of the FVC is acceptable as a good start. The plateau is not defined in preschool children as the criteria for satisfactory expiration (end of test) and the flow-volume curve demonstrating a rapid rise to peak flow and a smooth descending limb is acceptable. For school age children a minimum of three satisfactory spirograms is required but, for preschool children, two acceptable spirograms are sufficient if the second highest FVC and FEV1 are within 100mL or 10% of the highest value, whichever is greater.14,32 Preschool children have a short forced expiratory time. Crenesse et al.30 reported a mean forced expiratory time of 1.7 seconds in preschool children between the age of 3 and 5 years. Therefore, experts suggest that FEV0.5 and FEV0.75 may be used in preschool children.32
Identification of spirometry pattern
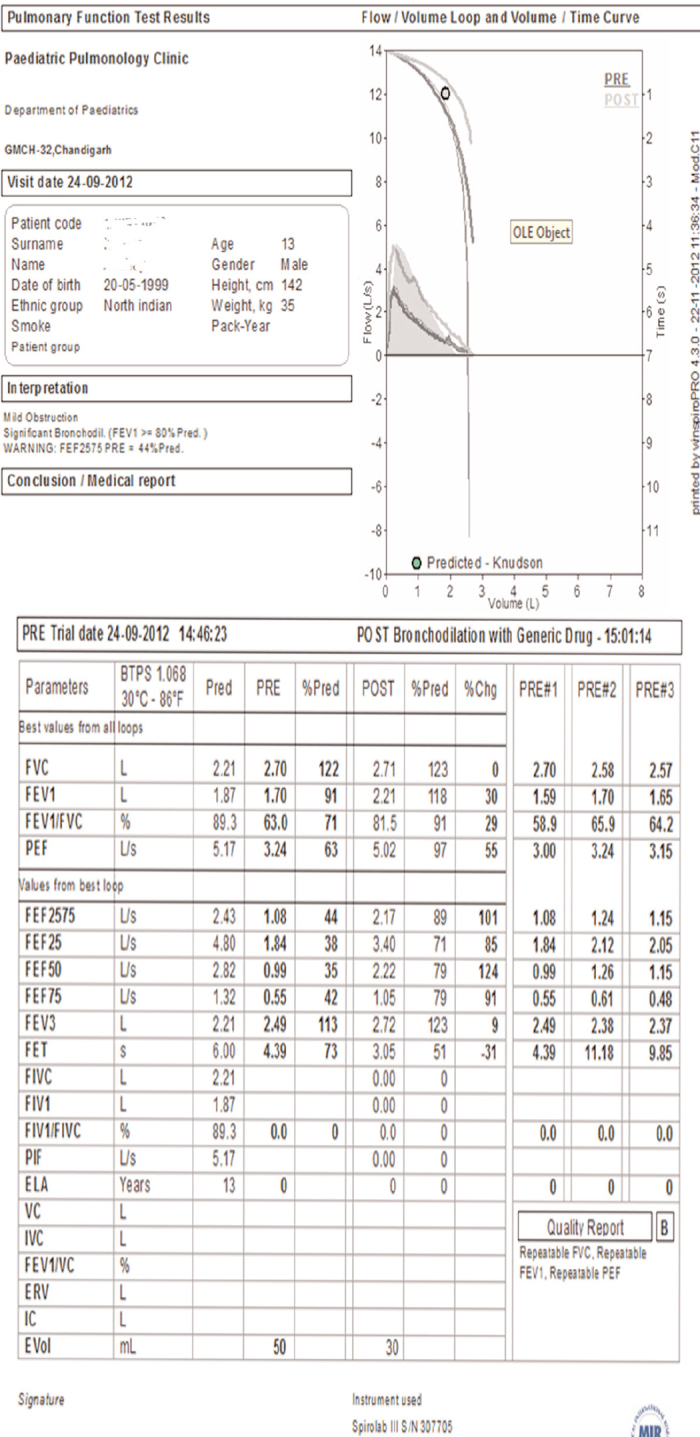
Abnormalities in a spirometry test can be identified by looking at the shape of the curve and comparing the values of test parameters with reference values suitable for age, height, weight, sex, and ethnicity. A sample report together with the interpretation produced by a spirometer (MIR Spirolab III) is shown in Figure 2. The report had two curves (a flow-volume curve and a volume-time curve) for both pre-and post-bronchodilator tests along with numerical values of spirometry parameters with the percentage of predicted and percentage change after the bronchodilator test (Figure 2).
Figure 2. Sample report of spirometry test produced by MIR Spirolab III. Interpretation of the report is: (1) it is acceptable (no artifact, good start and satisfactory exhalation); (2) there is repeatability (two largest forced vital capacity (FVC) measurements within 150mL (2700–2580=120mL) and two largest forced expiratory volume in one second (FEV1) measurements within 5% of FVC (1700–1650/2700=1.8%)); (3) obstructive pattern (FEV1 91%, FEV1/FVC 71%, and FEF25–75 44%); (4) grading of severity mild (FEV1 91%); (5) there is significant bronchodilator response (30% change in FEV1); and (6) diagnosis consistent with asthma.
Normal flow-volume curve looks like a sail which rises sharply to a peak and then descends at an angle of about 45° (Figure 3A). A concave curve indicates mild to moderate airway obstruction (Figure 3B) and an elongated finish like a rat's tail indicates severe obstruction. A normal volume-time curve rises sharply and then reaches a plateau shortly (Figure 3A). A slow gradual rise and no definite plateau indicates moderate to severe airway obstruction. A small flow-volume curve suggests a restrictive pattern (Figure 3C) and a flat FVC flow-volume curve without a peak suggests extrathoracic obstruction (Figure 3D). Younger children have rapid emptying of the larger airways compared with a smaller lung volume that results in a convex shape of the flow-volume curve, and the shape becomes more linear as the child grows.6
Figure 3. Identification of ventilation pattern by spirometry curves: (A) normal flow-volume (in middle) and volume-time (at top) curves: grey shaded area is predicted curve and the blue line is actual tracing; (B) flow-volume curve suggestive of mild to moderate airway obstruction with significant bronchodilatation: grey line is predicted curve, blue line is actual tracing, and blue dotted line is post bronchodilatation curve; (C) flow-volume curve suggestive of restrictive pattern: blue dotted line is predicted curve and the grey line is actual tracing; (D) flow-volume curve suggestive of extrathoracic obstruction: blue dotted line is predicted curve and the grey line is actual tracing.

The commonly used parameters to interpret spirometry results are FEV1, FVC, and the FEV1/FVC ratio. The FEV1/FVC ratio is the most sensitive and specific indicator for identifying airway obstruction. These parameters are compared with reference values. References values have been published for different countries.36,37 A few countries have reference charts for preschool children.38 If reference values for preschool children are not available, data from healthy young children from the same population may be used as a reference.30 Recently, the ERS Global Lung Function Initiative has published the global multi-ethnic lung function for spirometry for the 3–95 year age range.39
The comparison can be presented as percentage of the predicted value or below the lower limit of normal for a particular population. The use of the lower limit of normal (lower 90% confidence limit) should be preferred if available rather than a percentage of the predicted value for interpreting spirometry results.13,16
Spirometry results may suggest one of the following four types of ventilation patterns: normal, obstructive, restrictive, or mixed pattern.40,41 Normal values of FVC (≥80% of predicted or above the lower limit of normal), FEV1 (≥80% of predicted or above the lower limit of normal), and FEV1/FVC are suggestive of normal spirometry. The obstructive pattern is usually characterised by decreased FEV1 (<80% of predicted or below the lower limit of normal), decreased FEV1/FVC, and normal FVC (FVC may be decreased in severe obstruction).13,42 A value of mid expiratory flow (FEF25–75%) below 60% of predicted also suggests an obstructive pattern.43 FEF25–75% is thought to be less effort-dependent than FEV1 as it does not include high flows in the lung volume and is considered a measurement of small airway patency.44 Studies have evaluated FEV1, FEV1/FVC, and FEF25–75% in children with asthma and found that FEF25–75% is a more sensitive indicator of airway obstruction.43,45,46 The restrictive pattern is suggested by predominantly decreased FVC, normal or decreased FEV1, and normal or increased FEV1/FVC. The proportionate reduction in both FEV1 and FVC is suggestive of a restrictive pattern or poor patient effort. The mixed pattern has a decreased value of all three parameters (i.e. FEV1, FVC, and FEV1/FVC). Standardised residual (z-score or standard deviation score) is an alternative approach to percentage predicted values for spirometry results.14
Normal expiratory flow but decreased inspiratory flow is suggestive of collapsible extrathoracic airway obstruction (e.g. laryngeal paralysis) whereas decreased maximal expiratory flow with normal inspiratory flow suggests collapsible major intrathoracic airway obstruction. If both inspiratory and expiratory flows are decreased, a fixed intrathoracic or extrathoracic airway obstruction is likely.47
Bronchodilator response
The bronchodilator response (BDR) may be used to assess reversibility of the obstructive pattern in spirometry. Before conducting a bronchodilator test it is necessary to ensure that the patient has not used a short-acting β2-agonist or a long-acting β2-agonist in the last 6 hrs and 12 hrs, respectively. The BDR is assessed after 15 mins of 4–5 doses of 100μg salbutamol inhalation using a metered dose inhaler with a spacer. The response to the bronchodilator (>12% improvement in FEV1 or 15–25% improvement in FEF25–75%) suggests reversibility of airway obstruction which is characteristic of asthma.13 A course of oral steroids for two weeks or inhaled steroids for three months can also be used to determine bronchodilator reversibility if asthma is strongly suspected. However, it is important to remember that a negative BDR on an individual test does not exclude the diagnosis of asthma as it is a variable disease. Similarly, BDR with a normal spirometry does not always suggest asthma. A diagnosis of asthma should be based on history, physical examination, and the presence of airway obstruction in spirometry. Galant et al.48 reported that BDR of ≥10% was significantly associated with poor asthma control in children even when the pre-bronchodilator spirometry was normal, which suggests that BDR may be a useful objective tool to assess asthma control in children.
Grading the severity of pattern identified
In children the severity of airway obstruction can be graded according to FEV1 percentage predicted: FEV1 <100% to 80% indicates mild obstruction; FEV1 <80% to 50% indicates moderate obstruction; FEV1 <50% to 30% indicates severe airway obstruction; and FEV1 <30% indicates very severe obstruction. Fuhlbrigge et al.49 observed a significant relationship between FEV1% and asthma symptoms and severe asthma exacerbations requiring oral steroids, emergency department visits, and hospitalisations. Along with other clinical characteristics, FEV1 has been used to classify the severity of persistent asthma in children with mild, moderate, and severe persistent asthma having FEV1 ≥80%, >60% to <80%, and ≤60% of predicted, respectively.50 The spirometry results have been correlated with asthma severity even in preschool children.51
Diagnosis and treatment of the condition or further investigation
It is important to note that spirometry results are not pathognomonic of any particular disease; rather, they provide a pattern of physiological abnormality that can be obstructive, restrictive, or mixed. Spirometry results should not therefore be viewed in isolation, but rather should be considered in conjuction with the differential diagnosis made clinically before performing the test. While making a diagnosis by spirometry, the abovementioned indications for performing the test should be kept in mind. Differential diagnoses of extrathoracic obstructive pattern in children include facial dysmorphism, vocal cord paralysis, and subglottic or tracheal stenosis. Tracheomalacia or bronchomalacia, external compression of the trachea, and foreign body aspiration are some of the conditions that may produce an intrathoracic obstructive pattern in spirometry. Asthma is a typical example of peripheral airway obstruction. Differential diagnoses of a restrictive pattern in spirometry in children include interstitial lung disease, pneumonia and pleural effusion, atelectasis, rib cage or spine malformation (e.g. kyphosis and scoliosis), congestive cardiac failure, connective tissue disorders, and haemato-oncological diseases. Cystic fibrosis may have an obstructive, restrictive, or mixed spirometry pattern. Once a diagnosis is made it must be treated, or further investigations should be done at advanced respiratory laboratories (e.g. lung volume measurements or diffusion capacity estimation for interstitial lung diseases).
Spirometers versus peak flow meters
PEF measured by a peak flow meter rather than by a spirometer is inaccurate and substantially overestimated in the range of 200–400L/min.52,53 Choi et al.54 reported that a peak flow meter underestimated the severity of airflow obstruction in acute asthma. Furthermore, in a study by Sly et al., peak flow meters were inaccurate in detecting changes in lung function in children which were detected by a spirometer.55 Therefore, when available, spirometers should be preferred to peak flow meters for measuring lung function in children.
Conclusions
Spirometry is a useful investigation for diagnosing and monitoring a number of paediatric respiratory diseases. With the availability of better equipment with incentives for children to aid spirometry performance, most children (including preschool children) can perform acceptable spirometry. Spirometry is underused in children, and there is a need to encourage its use by primary care physicians and paediatricians treating children with respiratory diseases after adequate training.
Acknowledgments
Handling editor Niels Chavannes
Funding None.
Footnotes
The author declares that he has no conflicts of interest in relation to this article.
References
- Kotecha SJ, Watkins WJ, Paranjothy S, Dunstan FD, Henderson AJ, Kotecha S. Effect of late preterm birth on longitudinal lung spirometry in school age children and adolescents. Thorax 2012;67(1):54–61. http://dx.doi.org/10.1136/thoraxjnl-2011-200329 [DOI] [PubMed] [Google Scholar]
- Chhabra SK, Vijayan VK, Rahman M, Mittal V, Singh PD. Regression equations for spirometry in children aged 6 to 17 years in Delhi region. Indian J Chest Dis Allied Sci 2012;54(1):59–63. [PubMed] [Google Scholar]
- Kirkby J, Welsh L, Lum S, et al. The EPICure study: comparison of pediatric spirometry in community and laboratory settings. Pediatr Pulmonol 2008;43(12):1233–41. http://dx.doi.org/10.1002/ppul.20950 [DOI] [PubMed] [Google Scholar]
- Zanconato S, Meneghelli G, Braga R, Zacchello F, Baraldi E. Office spirometry in primary care pediatrics: a pilot study. Pediatrics 2005;116(6):e792–7. http://dx.doi.org/10.1542/peds.2005-0487 [DOI] [PubMed] [Google Scholar]
- Dombkowski KJ, Hassan F, Wasilevich EA, Clark SJ. Spirometry use among pediatric primary care physicians. Pediatrics 2010;126(4):682–7. http://dx.doi.org/10.1542/peds.2010-0362 [DOI] [PubMed] [Google Scholar]
- Aurora P, Stocks J, Oliver C, et al. Quality control for spirometry in preschool children with and without lung disease. Am J Respir Crit Care Med 2004;169:1152–9. http://dx.doi.org/10.1164/rccm.200310-1453OC [DOI] [PubMed] [Google Scholar]
- Nystad W, Samuelsen SO, Nafstad P, Edvardsen E, Stensrud T, Jaakkola JJK. Feasibility of measuring lung function in preschool children. Thorax 2002;57:1021–7. http://dx.doi.org/10.1136/thorax.57.12.1021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Veras TN, Pinto LA. Feasibility of spirometry in preschool children. J Bras Pneumol 2011;37(1):69–74. http://dx.doi.org/10.1590/S1806-37132011000100011 [DOI] [PubMed] [Google Scholar]
- Gaffin JM, Shotola NL, Martin TR, Phipatanakul W. Clinically useful spirometry in preschool-aged children: evaluation of the 2007 American Thoracic Society guidelines. J Asthma 2010;47(7):762–7. http://dx.doi.org/10.3109/02770903.2010.485664 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Komarow HD, Skinner J, Young M, et al. A study of the use of impulse oscillometry in the evaluation of children with asthma: analysis of lung parameters, order effect, and utility compared with spirometry. Pediatr Pulmonol 2012;47(1):18–26. http://dx.doi.org/10.1002/ppul.21507 [DOI] [PMC free article] [PubMed] [Google Scholar]
- American Thoracic Society/European Respiratory Society. ATS/ERS statement: raised volume forced expirations in infants: guidelines for current practice. Am J Respir Crit Care Med 2005;172(11):1463–71. http://dx.doi.org/10.1164/rccm.200408-1141ST [DOI] [PubMed] [Google Scholar]
- Araujo CG, Vianna LC. How often does spirometry testing induce cardiac arrhythmias? Prim Care Respir J 2009;18(3):185–8. http://dx.doi.org/10.4104/pcrj.2009.00023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levy ML, Quanjer PH, Booker R, Cooper BG, Holmes S, Small I; General Practice Airways Group. Diagnostic spirometry in primary care: proposed standards for general practice compliant with American Thoracic Society and European Respiratory Society recommendations: a General Practice Airways Group (GPIAG) document in association with the Association for Respiratory Technology & Physiology (ARTP) and Education for Health. Prim Care Respir J 2009;18(3):130–47. http://dx.doi.org/10.4104/pcrj.2009.00054 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller MR, Hankinson J, Brusasco V, et al. ATS/ERS Task Force. Standardisation of spirometry. Eur Respir J 2005;26(2):319–38. http://dx.doi.org/10.1183/09031936.05.00034805 [DOI] [PubMed] [Google Scholar]
- Constant C, Sampaio I, Negreiro F, et al. Respiratory disease screening in school-aged children using portable spirometry. J Pediatr (Rio J) 2011;87(2):123–30. [DOI] [PubMed] [Google Scholar]
- Holt EW, Tan J, Hosgood HD. The impact of spirometry on pediatric asthma diagnosis and treatment. J Asthma 2006;43(7):489–93. http://dx.doi.org/10.1080/02770900600859040 [DOI] [PubMed] [Google Scholar]
- Dundas I, Mckenzie S. Spirometry in the diagnosis of asthma in children. Curr Opin Pulm Med 2006;12(1):28–33. http://dx.doi.org/10.1097/01.mcp.0000199809.42011.58 [DOI] [PubMed] [Google Scholar]
- Sanders DB, Rosenfeld M, Mayer-Hamblett N, Stamey D, Redding GJ. Reproducibility of spirometry during cystic fibrosis pulmonary exacerbations. Pediatr Pulmonol 2008;43(11):1142–6. http://dx.doi.org/10.1002/ppul.20924 [DOI] [PubMed] [Google Scholar]
- Vilozni D, Bentur L, Efrati O, et al. Spirometry in early childhood in cystic fibrosis patients. Chest 2007;131(2):356–61. http://dx.doi.org/10.1378/chest.06-1351 [DOI] [PubMed] [Google Scholar]
- Alyasin S, Moghtaderi M, Amin R, Kashef S, Karimi M. Pulmonary function test in transfusion-dependent β-thalassemia major patients: a pilot study. Pediatr Hematol Oncol 2011;28(4):329–33. http://dx.doi.org/10.3109/08880018.2010.543449 [DOI] [PubMed] [Google Scholar]
- Ahmad FA, Macias CG, Allen JY. The use of incentive spirometry in pediatric patients with sickle cell disease to reduce the incidence of acute chest syndrome. J Pediatr Hematol Oncol 2011;33(6):415–20. http://dx.doi.org/10.1097/MPH.0b013e31821ed4ce [DOI] [PubMed] [Google Scholar]
- Efrati O, Toren A, Duskin H, et al. Spirometry follow-up in young children with hemato-oncologic diseases. Med Sci Monit 2010;16(3):MT28–33. [PubMed] [Google Scholar]
- Vilozni D, Berkun Y, Levi Y, Weiss B, Jacobson JM, Efrati O. The feasibility and validity of forced spirometry in ataxia telangiectasia. Pediatr Pulmonol 2010;45(10):1030–6. http://dx.doi.org/10.1002/ppul.21291 [DOI] [PubMed] [Google Scholar]
- Chong HS, Moon ES, Park JO, et al. Value of preoperative pulmonary function test in flaccid neuromuscular scoliosis surgery. Spine 2011;36(21):E1391–4. http://dx.doi.org/10.1097/BRS.0b013e31820cd489 [DOI] [PubMed] [Google Scholar]
- Schneider WV, Bulloch B, Wilkinson M, Garcia-Filion P, Keahey L, Hostetler M. Utility of portable spirometry in a pediatric emergency department in children with acute exacerbation of asthma. J Asthma 2011;48(3):248–52. http://dx.doi.org/10.3109/02770903.2011.555036 [DOI] [PubMed] [Google Scholar]
- Langhan ML, Spiro DM. Portable spirometry during acute exacerbations of asthma in children. J Asthma 2009;46(2):122–5. http://dx.doi.org/10.1080/02770900802460522 [DOI] [PubMed] [Google Scholar]
- Uchida DA. Late presentation of double aortic arch in school-age children presumed to have asthma: the benefits of spirometry and examination of the flow-volume curve. Respir Care 2009;54(10):1402–4. [PubMed] [Google Scholar]
- Brouwer AF, Visser CA, Duiverman EJ, Roorda RJ, Brand PL. Is home spirometry useful in diagnosing asthma in children with nonspecific respiratory symptoms? Pediatr Pulmonol 2010;45(4):326–32. [DOI] [PubMed] [Google Scholar]
- Eigen H, Bieler H, Grant D, et al. Spirometric pulmonary function in healthy preschool children. Am J Respir Crit Care Med 2001;163(3 Pt 1):619–23. http://dx.doi.org/10.1164/ajrccm.163.3.2002054 [DOI] [PubMed] [Google Scholar]
- Crenesse D, Berlioz M, Bourrier T, Albertini M. Spirometry in children aged 3 to 5 years: reliability of forced expiratory maneuvers. Pediatr Pulmonol 2001;32:56–61. http://dx.doi.org/10.1002/ppul.1089 [DOI] [PubMed] [Google Scholar]
- Vilozni D, Barker M, Jellouschek H, Heimann G, Blau H. An interactive computer-animated system (SpiroGame) facilitates spirometry in preschool children. Am J Respir Crit Care Med 2001;164:2200–05. http://dx.doi.org/10.1164/ajrccm.164.12.2101002 [DOI] [PubMed] [Google Scholar]
- Beydon N, Davis SD, Lombardi E, et al. American Thoracic Society/European Respiratory Society Working Group on Infant and Young Children Pulmonary Function Testing. An official American Thoracic Society/European Respiratory Society statement: pulmonary function testing in preschool children. Am J Respir Crit Care Med 2007;175(12):1304–45. http://dx.doi.org/10.1164/rccm.200605-642ST [DOI] [PubMed] [Google Scholar]
- Gracchi V, Boel M, van der Laag J, van der Ent CK. Spirometry in young children: should computer-animation programs be used during testing? Eur Respir J 2003;21:872–5. http://dx.doi.org/10.1183/09031936.03.00059902 [DOI] [PubMed] [Google Scholar]
- Chavasse R, Johnson P, Francis J, Balfour-Lynn I, Rosenthal M, Bush A. To clip or not to clip? Noseclips for spirometry. Eur Respir J 2003;21(5):876–8. http://dx.doi.org/10.1183/09031936.03.00048303 [DOI] [PubMed] [Google Scholar]
- Kamps AW, Vermeer K, Roorda RJ, Brand PL. Effect of bacterial filters on spirometry measurements. Arch Dis Child 2001;85(4):346–7. http://dx.doi.org/10.1136/adc.85.4.346 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pistelli F, Bottai M, Carrozzi L, et al. Reference equations for spirometry from a general population sample in central Italy. Respir Med 2007;101(4):814–25. http://dx.doi.org/10.1016/j.rmed.2006.06.032 [DOI] [PubMed] [Google Scholar]
- Chhabra SK, Vijayan VK, Rahman M, Mittal V, Singh PD. Regression equations for spirometry in children aged 6 to 17 years in Delhi region. Indian J Chest Dis Allied Sci 2012;54(1):59–63. [PubMed] [Google Scholar]
- Stanojevic S, Wade A, Cole TJ, et al. Asthma UK Spirometry Collaborative Group. Spirometry centile charts for young Caucasian children: the Asthma UK Collaborative Initiative. Am J Respir Crit Care Med 2009;180(6):547–52. http://dx.doi.org/10.1164/rccm.200903-0323OC [DOI] [PubMed] [Google Scholar]
- Quanjer PH, Stanojevic S, Cole TJ, et al. The ERS Global Lung Function Initiative. Multi-ethnic reference values for spirometry for the 3–95 year age range: the global lung function 2012 equations. Eur Respir J 2012;40(6):1324–43. http://dx.doi.org/10.1183/09031936.00080312 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quanjer PH, Tammeling GJ, Cotes JE, Pedersen OF, Peslin R, Yernault JC. Lung volumes and forced ventilatory flows. Report Working Party Standardization of Lung Function Tests, European Community for Steel and Coal. Official Statement of the European Respiratory Society. Eur Respir J 1993;16:5–40. [PubMed] [Google Scholar]
- Barreiro TJ, Perillo I. An approach to interpreting spirometry. Am Fam Physician 2004;69(5):1107–14. [PubMed] [Google Scholar]
- Glady CA, Aaron SD, Lunau M, Clinch J, Dales RE. A spirometry-based algorithm to direct lung function testing in the pulmonary function laboratory. Chest 2003;123(6):1939–46. http://dx.doi.org/10.1378/chest.123.6.1939 [DOI] [PubMed] [Google Scholar]
- Lebecque P, Kiakulanda P, Coates AL. Spirometry in the asthmatic child: is FEF25–75 a more sensitive test than FEV1/FVC? Pediatr Pulmonol 1993;16(1):19–22. http://dx.doi.org/10.1002/ppul.1950160105 [DOI] [PubMed] [Google Scholar]
- Gelb AF, Zamel N. Simplified diagnosis of small-airway obstruction. N Engl J Med 1973;288:395–8. http://dx.doi.org/10.1056/NEJM197302222880805 [DOI] [PubMed] [Google Scholar]
- Valletta EA, Piacentini GL, Del Col G, Boner AL. FEF25–75 as a marker of airway obstruction in asthmatic children during reduced mite exposure at high altitude. J Asthma 1997;34(2):127–31. http://dx.doi.org/10.3109/02770909709075657 [DOI] [PubMed] [Google Scholar]
- Simon MR, Chinchilli VM, Phillips BR, et al.; Childhood Asthma Research and Education Network of the National Heart, Lung, and Blood Institute. Forced expiratory flow between 25% and 75% of vital capacity and FEV1/forced vital capacity ratio in relation to clinical and physiological parameters in asthmatic children with normal FEV1 values. J Allergy Clin Immunol 2010;126(3):527–34. http://dx.doi.org/10.1016/j.jaci.2010.05.016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pellegrino R, Viegi G, Brusasco V, et al. Interpretative strategies for lung function tests. ATS/ERS Task Force Standardization of Lung Function Testing. Eur Respir J 2005;26(5):948–68. http://dx.doi.org/10.1183/09031936.05.00035205 [DOI] [PubMed] [Google Scholar]
- Galant SP, Morphew T, Newcomb RL, Hioe K, Guijon O, Liao O. The relationship of the bronchodilator response phenotype to poor asthma control in children with normal spirometry. J Pediatr 2011;158(6):953–959.e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fuhlbrigge AL, Weiss ST, Kuntz KM, Paltiel AD; CAMP Research Group. Forced expiratory volume in 1 second percentage improves the classification of severity among children with asthma. Pediatrics 2006;118(2):e347–55. http://dx.doi.org/10.1542/peds.2005-2962 [DOI] [PubMed] [Google Scholar]
- Stout JW, Visness CM, Enright P, et al. Classification of asthma severity in children: the contribution of pulmonary function testing. Arch Pediatr Adolesc Med 2006;160(8):844–50. http://dx.doi.org/10.1001/archpedi.160.8.844 [DOI] [PubMed] [Google Scholar]
- Vilozni D, Barak A, Efrati O, et al. The role of computer games in measuring spirometry in healthy and ‘asthmatic’ preschool children. Chest 2005;128:1146–55. http://dx.doi.org/10.1378/chest.128.3.1146 [DOI] [PubMed] [Google Scholar]
- Miller MR, Dickinson SA, Hitchings DJ. The accuracy of portable peak flow meters. Thorax 1992;47:904–9. http://dx.doi.org/10.1136/thx.47.11.904 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sly PD, Burton D, Walker 5, Kano S. Do mini peak flow meters overestimate peak espiratory flow in children? Eur Respir J 1992;5(Suppl 15):105S. [Google Scholar]
- Choi IS, Koh YI, Lim H. Peak expiratory flow rate underestimates severity of airflow obstruction in acute asthma. Korean J Intern Med 2002;17(3):174–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sly PD, Cahill P, Willet K, Burton P. Accuracy of mini peak flow meters in indicating changes in lung function in children with asthma. BMJ 1994;308:572–4. http://dx.doi.org/10.1136/bmj.308.6928.572 [DOI] [PMC free article] [PubMed] [Google Scholar]