

Abstract
Background This article measures the life quality, clinical, and functional outcomes of a patient who had undergone reconstruction of the radioscaphocapitate ligament (RSL), using brachioradialis tendon in the treatment of ulnar translation of the carpus.
Case Description We present a 36-year-old man with ulnar translation in his left, nondominant wrist, after fall accident. Reconstruction of the RSL was performed. One year later, the patient experienced good evaluation. Wrist flexion was 70 degrees, extension was 60 degrees, radial deviation was 20 degrees, and ulnar deviation was 30 degrees. Forearm pronation was 85 degrees and supination was 90 degrees and digit motion was full. Disabilities of the Arm, Shoulder and Hand score of 5, Visual Analog Scale of 0, and grip strength of 82% were obtained compared with the unaffected side. Wrist radiographic aspects showed radiocarpal joint congruency. The period of fixator treatment was 8 weeks. Good stability and joint congruency of the radiocarpal joint were obtained. Good radiographic, clinical, and functional results were obtained improving the quality of life of the patient.
Literature Review The treatment of ulnar translation is difficult and complicated. There is no consensus to the overall management. As there is still a lack of long-term results, the indications for surgery, various surgical options, and the type of intervention have been a matter of controversy in the literature. Would radiocarpal joint be stable when reconstruction of the RSL using brachioradialis tendon was obtained? Is it possible to reduce an ulnar translation with this technique?
Clinical Relevance We would like to suggest that the radiocarpal ligament reconstruction will improve the outcome. We believe that this technique will make the wrist more stable and functional. We agree that the best time to perform the corrections is early. The authors prefer to first reconstruct the RSL and then the radiocarpal ligament suture or radioscapholunate arthrodesis.
Keywords: ulnar translation, forearm deformity, wrist deformity, ligament reconstruction, radiocarpal ligaments
Ulnar translation of the carpus is an uncommon traumatic disorder associated with injuries to the radioscaphocapitate (RSL) and radiolunate ligaments. Diagnosis is often delayed because of lack of radiographic findings, and it is often done following chronic failure (instability) of the joint and elevated wrist pain. Treatment of acute translocation usually involves stabilization and ligament suture using cast immobilization. Ligament healing generally requires 8 weeks, but may not occur in that period, especially when underdiagnosed. This type of reconstruction is appropriate in cases with early recognition and for the treatment of traumatic, pure, and isolated ulnar translation of the carpus. It is not ideal for ulnar translation in patients with rheumatoid arthritis or preexisting osteoarthritis. Treatment of chronic lesions may require scapholunate arthrodesis, especially in patients with signs of posttraumatic osteoarthritis. In this case report, we stabilized the radiocarpal joint by RSL reconstruction using a brachioradialis (BR) tendon graft. This novel procedure offers clinically significant procedural and functional advantages.
Case Report
A 36-year-old man presented with an ulnar translation deformity in his left, nondominant forearm. Wrist flexion was limited to 40 degrees, while extension was limited to 10 degrees. Wrist radiographs appeared normal, the diagnosis was ulnar translation with a bruised wrist, and the patient was immobilized with a plaster splint for 2 weeks. Twenty-four months later, the patient complained of persistent wrist pain. Radiographs revealed ulnar translation of the radiocarpal joint without associated fracture or intercarpal injury. On reviewing the initial evaluation, ulnar translocation was evident on the radiographs obtained on the day of injury. A preoperative radiograph of the wrist is shown in Fig. 1 . The patient's Disabilities of the Arm, Shoulder and Hand (DASH) score was 42, and the Visual Analog Scale (VAS) pain score was 7. Grip strength was 45% of that achieved by the unaffected wrist. Before surgery, radiographs of the nonaffected wrist ( Fig. 2 ) were used to plan the reconstruction procedure.
Fig. 1.

Preoperative radiographs of the affected wrist.
Fig. 2.

Preoperative radiograph of the unaffected wrist.
During reconstruction of the radioscaphocapitate, the BR muscle tendon was harvested and elevated from its insertion on the radial styloid process to the proximal myotendinous transition. Dissection of the BR tendon graft is shown in Fig. 3 . A FiberLoop wire suture (Arthrex Inc., Naples, FL) was applied to the proximal end of the BR tendon. An oblique tunnel was made in the radius at the insertion of the BR to the scaphoid cavity using a drill under fluoroscopic guidance. The tendon was passed through the tunnel in the distal radius using a guidewire. The graft was attached (reattached) to the palmar face of the scaphoid bone with a single specific suture anchor (Arthrex Inc.). A capitate tunnel was prepared, and the tendon graft was passed through the capitate tunnel in a palmar to dorsal direction using a guidewire. A schematic drawing of the technique is shown in Fig. 4 . The tendon graft was attached to the third metacarpal using another specific anchor. Radial and ulnar deviations were tested, and the position of the carpal bones was corrected to ensure joint stability. Fig. 5 shows intraoperative wrist fluoroscopy of the joint before and after applying traction to the tendon graft. To protect the ligament reconstruction, the wrist was fixed for 8 weeks in the neutral position with external bridging using two pins in the radius and two in the third metacarpal ( Fig. 6 ).
Fig. 3.

Dissection of the brachioradialis tendon graft.
Fig. 4.
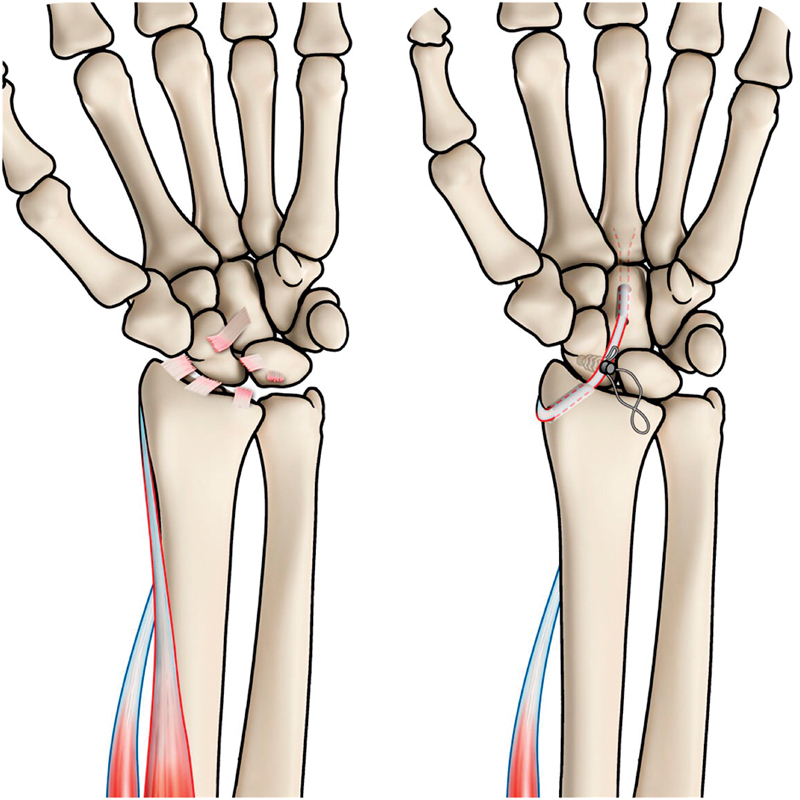
Schematic illustration of the surgical procedure.
Fig. 5.
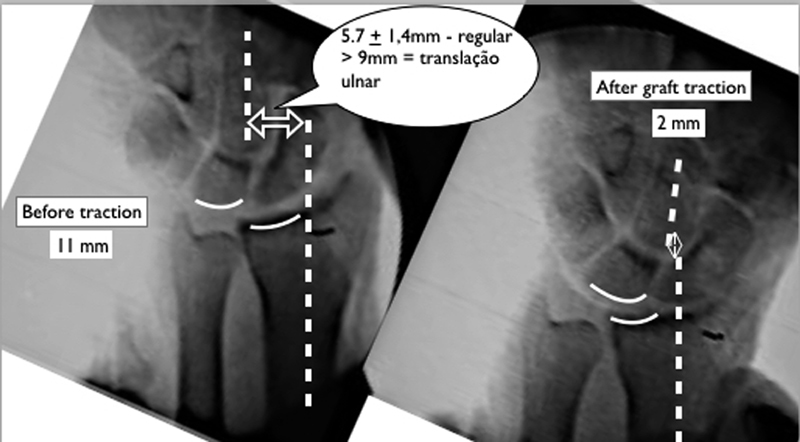
Intraoperative comparative wrist fluoroscopy before and after applying traction to the tendon graft.
Fig. 6.

External fixator bridging to protect the ligament reconstruction.
On follow-up 1 year after surgery, the patient exhibited good wrist, forearm, and elbow range of motion, with 70 degree flexion, 60 degree extension, 20 degree radial deviation, 30 degree ulnar deviation, 85 degree pronation, and 90 degree supination. The postoperative clinical evaluation is summarized in Fig. 7 . The patient had normal movement of digits, a DASH score of 5, VAS of 0, and grip strength of 82% compared with the unaffected wrist. Wrist radiography showed articular congruency of the distal radioulnar joint (DRUJ) and radiocarpal joint. Eight weeks of fixator treatment resulted in good stability and congruency of the DRUJ and radiocarpal joints. The radiographic, clinical, and functional results were consistent with improvement in the patient's daily quality of life. Postoperative wrist radiographs obtained 1 year after surgery are shown in Fig. 8 .
Fig. 7.
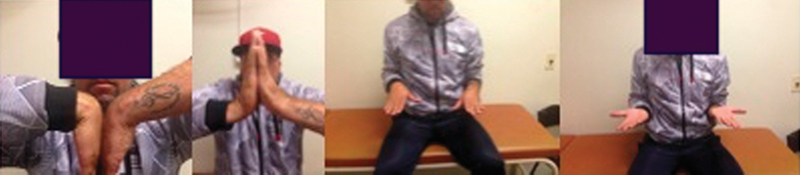
Postoperative clinical status 1 year after surgery.
Fig. 8.

Postoperative wrist radiography 1 year after surgery.
Discussion
Isolated ulnar translation of the carpus is rarely encountered. The radiographic appearance is unusual and the abnormalities may be subtle. Radiographic findings may be present when less than 50% of the lunate articulates with the radius in a posterior-anterior view, although it is necessary to compare the images of affected and unaffected wrists. Ulnar translation of the carpus may also be evident as an increased distance between the radial styloid and scaphoid or placement in the scaphoid lunate fossa. 1 2 A line drawn through the central axis of the radius and the center of the capitate normally averages 5.7 ± 1.4 mm. Lengths of 9 mm have been associated with the ulnar carpal translation. 3 However, the normal length is quite variable, and a comparison with radiographs of the opposite wrist should be made.
The treatment of forearm deformities is difficult and complicated, and the surgical indications and options vary. Overall, we are pessimistic about the success of immediate ligament repair and radiolunate fusion without considering other options. Radiolunate arthrodesis is recommended for cases with a late diagnosis or after failure of ligament repair. 4 We agree that ligament reconstruction is preferable to ligament repair or radiocarpal fusion. Rutgers et al 1 recommended ligament reconstruction procedures and stressed the importance of early recognition and treatment of traumatic, pure, and isolated ulnar translation of the carpus. In a cadaver study, Maschke et al 2 described treatment for ulnar translation of the carpus using the BR tendon as a graft for reconstruction of the radioscaphocapitate ligament. Aita et al 5 successfully performed ligament reconstruction in the forearm using the BR tendon as a graft for reconstruction of the interosseous membrane.
The reconstruction performed in our patient is appropriate for uncomplicated cases with early recognition but not for patients with rheumatoid arthritis or preexisting osteoarthritis. The choice of a BR tendon graft used in this patient is novel and offers several advantages. The small diameter of the bone tunnels averts complications such as iatrogenic fractures of the radius and capitate. It preserves insertion which we believe helps during the surgical procedure to stress the graft. The tendon graft is adjacent to radiocarpal joint, avoiding an additional surgical site. The function of the donor forearm is not affected by the withdrawal of the tendon graft. In this patient, the radiocarpal joint was stabilized by reconstructing the RSL using the BR tendon. Recurrence of ulnar translation may occur after ligament repair, 1 4 but successful clinical results were achieved with this ligament reconstruction procedure. Complications were noted, but a longer follow-up period is needed as a result of the patient's activities.
Acknowledgment
The authors are grateful for the translation service provided by Sandra Miaguti.
Funding Statement
Funding None.
Conflict of Interest None declared.
Ethical Approval
This case presentation was approved by, and followed the ethical standards of, the Faculdade de Medicina do ABC Ethics Committee on human experimentation (no. 1750176). An informed consent document was provided to the patient, who willingly read and signed it.
References
- 1.Rutgers M, Jupiter J, Ring D. Isolated posttraumatic ulnar translocation of the radiocarpal joint. J Hand Microsurg. 2009;1(02):108–112. doi: 10.1007/s12593-009-0014-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Maschke S D, Means K R, Jr, Parks B G, Graham T J. A radiocarpal ligament reconstruction using brachioradialis for secondary ulnar translation of the carpus following radiocarpal dislocation: a cadaver study. J Hand Surg Am. 2010;35(02):256–261. doi: 10.1016/j.jhsa.2009.10.011. [DOI] [PubMed] [Google Scholar]
- 3.DiBenedetto M R, Lubbers L M, Coleman C R. A standardized measurement of ulnar carpal translocation. J Hand Surg Am. 1990;15(06):1009–1010. doi: 10.1016/0363-5023(90)90035-p. [DOI] [PubMed] [Google Scholar]
- 4.Jebson P J, Adams B D, Meletiou S D. Ulnar translocation instability of the carpus after a dorsal radiocarpal dislocation: a case report. Am J Orthop. 2000;29(06):462–464. [PubMed] [Google Scholar]
- 5.Aita M A, Mallozi R C, Ozaki W, Ikeuti D H, Consoni D AP, Rugiero G M. Ligamentous reconstruction of the interosseous membrane of the forearm in the treatment of instability of the DRUJ. Rev Bras Ortop. 2018;53(02):184–191. doi: 10.1016/j.rboe.2018.02.010. [DOI] [PMC free article] [PubMed] [Google Scholar]