

Abstract
1. Background
The Experimental Tobacco Marketplace (ETM) is a digital storefront in which participants can purchase tobacco products using an account balance that reflects their typical tobacco product purchasing. The ETM is also an ideal resource to investigate the harm-reduction potential of alternative nicotine products such as e-cigarettes. In a series of experiments, we explored the effects of harm-reduction narratives that encouraged e-cigarette substitution of conventional cigarettes in the ETM. These narratives incorporated different cognitive biases in order to determine which strategy is most effective.
2. Methods
In both experiments, participants, recruited from Amazon Mechanical Turk, read a narrative about a friend that either falls ill or faces financial difficulties and then made purchases in the ETM. Some of these narratives specifically incorporated different cognitive biases including trusting authority. Across ETM trials, the price of conventional cigarettes increased while the price of the alternative products, including e-cigarettes, remained constant.
3. Results
Across both experiments, a general pattern emerged supporting the effectiveness of narratives in increasing e-cigarette purchasing. Importantly, from a harm-reduction perspective, this increase in e-cigarette substitution frequently corresponded with a decrease in conventional cigarette purchasing.
4. Conclusions
Narratives can decrease conventional cigarette and increase e-cigarette purchasing in an ETM that mimics real-world marketplaces. Invoking different cognitive biases may bolster this effect. Narratives can be a valuable harm-reduction tool because they are cost-effective, can be widely disseminated, and can be personalized to individuals.
Keywords: narratives, harm-reduction, demand, behavioral economics, experimental tobacco marketplace
1.1. Introduction
Smoking-related illnesses inflict a massive toll on the American economy, approximating over $300 billion each year in health care and lost productivity (Xu et al., 2015) and is still the largest cause of preventable death (CDC, 2014). Most smoking interventions, including public health interventions such as the CDC’s “Tips from Former Smokers” narrative campaign (CDCTobaccoFree, 2018), promote complete nicotine cessation; however, harm-reduction methods are increasingly considered (Abrams et al., 2018; Phillips, 2009). Harm-reduction methods target reductions in the exposure to toxicants from tobacco products by altering smoking behavior or adopting alternative nicotine products (Phillips, 2009) while not necessarily eliminating all nicotine use.
A growing body of evidence suggests that for some, substituting electronic nicotine delivery systems (e-cigarettes or ENDS; e.g., e-liquid, disposables) may be a viable harm-reduction method (Brown et al., 2014; Kalkhoran and Glantz, 2016; Notley et al., 2018; Selya et al., 2017; Warner, 2018). ENDS may be particularly capable as harm-reduction substitutes, compared to nicotine replacement therapy (NRT), because ENDS better approximate the secondary reinforcers associated with conventional cigarettes (e.g., smoking motion and inhalation; Hartmann-Boyce et al. 2018) and indeed some research suggests that ENDS are more effective substitutes (Johnson et al. 2017) though we noted that the long-term consequences of exclusive ENDS (Callahan-Lyon 2014) or cigarette dual-use (Lee et al. 2014) are still unclear and that any consumption of conventional cigarettes can still lead to detrimental health outcomes (Hackshaw et al. 2018). Substitution refers to an increase in the purchasing of a fixed price product as the price of an alternative product increases (Hursh and Bauman, 1987; Reed et al., 2013). Research indicates that ENDS can function as a substitute for conventional cigarettes among smokers (Bickel et al., 2018; Grace et al., 2015; Pope et al., 2018).
The traditional definitions of substitution do not require declines in the purchasing of the increasing-price product (Kroon, 2007)a decrease in conventional cigarettes should be observed if ENDS substitution is to have a harm-reducing effect. Second, evaluating the effectiveness of interventions on increasing the substitutability of ENDS should not be restricted to changes in the rate of change in consumption but should include changes in consumption at the lowest alternative product price, an index we have termed the initial intensity of substitution (DeHart et al. 2018). In fact, an individual could report an important change in the initial intensity of substitution and consequently reduce the slope of substitution to 0. Research investigating the substitutability of ENDS does suggest that encouraging ENDS substitution may subsequently reduce conventional cigarette purchasing (Berry et al., 2018; Soneji et al., 2018).
One method of encouraging behavioral change (e.g., increasing ENDS substitution) is with narratives. Narratives are informative stories that present information in a persuasive and understandable form. Narrative Theory asserts that humans are particularly prepared to be influenced by the decisions and experiences of others through narratives (Bickel et al., 2017). Narratives have frequently been found more effective than information alone at disseminating information (Nummenmaa et al., 2014) and producing behavioral change (Winterbottom et al., 2008). The persuasiveness of narratives is especially potent when the narrative is personalized to the reader such as matching demographic characteristics between the reader and subject of the narrative (Hirsh et al., 2012).
Narratives have been found more effective at encouraging real-world health-related behavioral change than information alone including increasing the likelihood that an individual will participate in mammogram (Kreuter et al., 2010), cervical (Murphy et al., 2015), and colon cancer (Dillard et al., 2010) screenings, scheduling vaccinations (Frank et al., 2015), and safer sex practices (Kiene and Barta, 2003). Narrative interventions are also amenable to in-laboratory demonstrations. For example, when presented with a narrative about a friend contracting a sexually transmitted infection (STI), Quisenberry and colleagues (2015) found that participants were less likely to engage in unprotected sex with an individual with an STI.
One strength of narratives is that they can be disseminated widely through public-health campaigns. The “Tips From Former Smokers” campaign, in which former cigarette smokers shared written and video-recorded narratives about the negative health consequences of smoking as well as the health gains from quitting, is one example of a widely disseminated narrative intervention (CDCTobaccoFree, 2018). Neff and colleagues (Neff et al., 2016) found evidence to suggest that these narratives were effective at increasing both quit attempts and quit successes over the course of the campaign.
Another strength of narratives is their ability to incorporate different cognitive biases in order to improve their effectiveness. Cognitive biases, or decision-making heuristics (Tversky and Kahneman, 1974), serve as information-processing shortcuts (Gigerenzer and Goldstein, 2011) which simplify decisions allowing for faster and more efficient decision-making. Cognitive biases are typically ascribed to decrease the quality but increase the ease of decisionmaking (e.g., irrationality; Denes-Raj and Epstein, 1994). Conversely, cognitive biases could be incorporated into narratives to improve decision-making (Rothman et al., 2006). Salmon and colleagues have repeatedly found that encouraging participants to engage in social proof cognitive biases (e.g., portraying a choice as the choice of the majority) improved healthy food selections (Salmon et al., 2015, 2014). Cognitive biases could be incorporated into harm-reduction narratives in a similar fashion.
The Experimental Tobacco Marketplace (Bickel et al., 2018; Quisenberry et al., 2017, 2016) is acutely positioned to investigate the effectiveness narratives and to identify which cognitive biases are most effective at producing behavioral change and particularly engendering greater ENDS substitution in an experimental context. The ETM assesses demand and substitution and promotes ecological validity by giving participants an account balance (i.e., budget) derived from their real-world tobacco consumption and allows them to purchase a wide range of products. One product (typically the participant’s preferred conventional cigarette) is selected as the price manipulated product, with its price increasing across trials while the remaining product prices are fixed. The ETM has proven valuable in investigating the substitutability of ENDS (Bickel et al., 2018; Heckman et al., 2017; Quisenberry et al., 2017, 2016) under a variety of conditions. For example, Heckman et al. (2017) found that ENDS substitution was a stronger substitute for conventional cigarettes than NRT products in conventional cigarette smokers and that NRT product substitution decreased when ENDS products were simultaneously available in the ETM.
In a demonstration of the effects of narratives on purchasing in the ETM, DeHart et al. (2018) presented cigarette smokers with one of four narratives about a hypothetical friend falling ill. In the Positive condition, the participant’s friend discovers that they only had the flu, in Negative condition, the friend discovers that their illness is due to smoking, the Negative-Regret condition, the friend explicitly expressed regret for having started smoking and in the Negative-Change condition, the friend switches to ENDS and recovers. After participants read their assigned narrative, they made hypothetical purchases in the ETM in which the price of their preferred conventional cigarette increased trials (e.g., 7 trials, price per cigarette increased from $0.13 to $4.00). The price of alternative products, including ENDS, remained constant across trials (e.g., $7.99 per disposable ENDS). ENDS products were the best substitute across all four groups; however, participants who read the Negative-Change condition substituted ENDS more regardless of prior ENDS use and importantly purchased fewer conventional cigarettes in the ETM compared to the other three narrative groups.
The purpose of this series of experiments is to extend our previous work demonstrating that narratives can change purchasing in the ETM by incorporating specific cognitive biases in the public health narratives. As stated previously, targeting cognitive biases have the potential to increase the effectiveness of narratives. In Experiment 1, we compared substitution of ENDS for conventional cigarettes in the ETM between narratives that incorporated cognitive biases of authority or social proof to a narrative adapted from the CDC “Tips for Former Smokers” campaign (CDCTobaccoFree, 2018). By using narratives adapted directly from the CDC, the narratives presented in Experiment 1 are ecologically valid and better reflect narratives that participants could encounter in real-life. In the authority narrative, a doctor describes the possible health-benefits of ENDS substitution and invokes scientific authority and in the social proof narrative, a second friend addresses the social stigma associated with ENDS use and provides a second testimonial as to their effectiveness. These specific cognitive biases were chosen because they are narrative adaptations that could be easily implemented, are reported as common inhibitors of ENDS acquisition (Coleman et al., 2016) and reflect comments made by previous participants (DeHart et al. 2018) as to why they would not adopt ENDS products. We hypothesized that the authority and social proof narratives would result in similar increases of ENDS purchasing in the ETM.
In Experiment 2, we extended the results of (DeHart et al. 2018) by comparing ENDS substitution in the ETM between narratives that highlighted the health benefits of switching to ENDS to narratives that highlighted the financial benefits of switching. The financial narrative exploits the loss aversion cognitive bias (Kahneman et al. 1991) in that participants may prefer to avoid a monetary loss over a health gain. We hypothesized that highlighting the health versus the financial benefits of ENDS substitution would have similar effects on ENDS purchasing in the ETM.
2. Experiment 1
Experiment 1 presented participants with narratives designed to invoke the cognitive biases of trust in authority and social proof and presented them with opportunities to purchase nicotine products in the ETM.
2.1. Methods
2.1.1. Procedure
2.1.2. Demographics and Tobacco Product Use
One hundred and fifty-seven participants (104 males, 53 females; determined by a priori power-analysis, conducted in G*Power to observe a medium effect size of 0.25 at 80% power; (Faul et al., 2009) were recruited through Amazon Mechanical Turk (Mturk) and paid $7.50 to complete an approximately one-hour online survey administered through Qualtrics survey software. Data were collected in November 2017. In order to qualify, participants had to report having previously completed at least 50 Mturk assignments with a 95% approval rating and smoke a minimum of 10 cigarettes a day. Experience with ENDS was not a determinant of participation and both ENDS users and naive-ENDS users could participate. Participants first completed a series of demographic questions and reported nicotine product use in a Timeline Followback (TLFB; Sobell and Sobell, 1992), the Fagerstrom Test for Cigarette Dependence (FTCD; Fagerstrom, 2012) and reported their perceived risk of different nicotine products both before and after reading their assigned narrative (Mooney et al., 2006). The perceived risk questionnaire asked participants (on a scale of 1 to 10 with 1 indicating a very low risk of disease and 10 indicating a very high risk of disease) to rate how likely both conventional cigarettes and ENDS products were to cause different health ailments including lung cancer, emphysema, and stroke. Participants were also asked to compare the risk of developing these diseases through ENDS use compared to conventional cigarettes on a 5-point scale (1 indicated much lower in risk and 5 indicated much higher in risk). The Virginia Tech Institutional Review Board approved all procedures and protocols and consent was implied with the submission of the online survey.
2.1.3. Experimental Tobacco Marketplace
In the ETM, participants made hypothetical purchases of nicotine products constrained by a budget (M = $26.57, SD = $21.37) based on their typical number of nicotine products and type of nicotine products used per day. Participants could not purchase more products than their budget allowed (Quisenberry et al., 2016). The prices of the nicotine products for calculation of the budget and for some of the conditions when purchasing products within the ETM were based on prior studies (DeHart et al., n.d.; Quisenberry et al., 2017, 2016). The description of the nicotine products included the approximate nicotine concentration (as labeled by product package) and the approximate single-cigarette equivalent nicotine content. Conventional cigarettes were labeled as 1 mg of nicotine per individual cigarette (approximate nicotine yield; Jarvis et al. 2001).
Participants completed seven ETM trials. For each trial, the price of a single conventional cigarette increased sequentially ($0.13, $0.25, $0.50, $1.00, $2.00, $4.00, $8.00) while prices of the other nicotine products were held constant (single disposable ENDS = $7.99, 2 mL of e-liquid = $0.75, single piece of nicotine gum = $0.80, single nicotine lozenge = $0.60, single pouch of chew = $0.20, and single pouch of snus = $0.20). A participant’s budget was individually determined based on their self-reported tobacco product use (using the prices listed above) during the previous five days. In line with previous research (DeHart et al. 2018), Participants were instructed to purchase as many products as they wished to consume over a five-day period and assume both that no other nicotine products were available and that they would keep any unspent budget.
2.2.4. Narratives
Prior to the ETM, participants were randomly assigned one of four brief narratives (see Supplemental Material): Center for Disease Control (CDC; n = 39), e-cigarette without biases (E-cigaretteControl; n = 39), e-cigarette with authority bias (E-cigaretteAuthority; n = 40), and e-cigarette with social proof (E-cigaretteSocial Proof; n = 39). The CDC narrative was obtained from the CDC “Tips from Former Smokers” campaign website (CDCTobaccoFree, 2018), and describes a woman who quits smoking after a Chronic Obstructive Pulmonary Disease (COPD) diagnosis. The three personalized ENDSnarratives depicted an identical scenario but the narrative was about a friend of the reader. The characteristics of the friend were personalized to match some of the reported demographics of the reader including smoking behavior, gender and age. In the E-cigaretteControl narrative, the subject permanently switches to ENDS after the COPD diagnosis and makes a recovery. In the E-cigaretteAuthority narrative, the subject permanently switches to ENDS after the physician (authority bias) recommends switching. In the E-cigaretteSocial Proof narrative, the subject permanently switches to ENDS after a second friend encourages the principal friend to switch by addressing the stigma of using ENDS (stigma and social proof biases). Participants also answered questions about narrative transportiveness (e.g., how well the participant could imagine and believe the event of the narrative; Green and Brock, 2000).
2.1.5. Analyses
All measures and participant data were included in the analyses. The number of nicotine products purchased in each ETM trial was converted to mg of nicotine purchased. The exponentiated demand equation was fitted to the cigarette purchase results (Koffarnus et al., 2015):
| (1) |
where Q is the mg of nicotine purchased at a given price, C is the price of the cigarette, Q0 represents demand intensity or the model fit y-intercept, k is a constant and is the range of the function in logarithmic units (set to 2.79 in these analyses), and α represents demand elasticity or the decrease in purchasing as price increases. Demand curves were fitted using the “beezdemand” package in R (Kaplan, 2018).
To measure substitution, a linear regression line was fitted to alternative nicotine product purchases as a function of conventional cigarette price converted to the proportion of the smallest price. The y-intercept term represents the purchasing of the alternative at zero conventional cigarette cost (e.g., initial intensity of substitution). The regression slope represents one facet of substitutability of that alternative, with positive slopes indicating greater purchasing associated with increases in conventional cigarette price. Model fit parameters for both conventional cigarettes and their alternatives were compared using the estimated marginal means differences (MD) between the parameter estimates using the “emmeans” package in R (Lenth, 2018). Estimated marginal means are means adjusted for additional model covariates. False discovery rate adjustments were used for all pairwise comparisons.
Changes in perceived conventional and ENDS risk perception were analyzed using false-discovery rate adjusted pairwise comparisons (e.g., multiple test adjusted t-tests) on the group mean differences (MD). Omnibus test results (e.g., ANOVA, GEE) are not reported because the direction of the change in risk perception can differ by group, making main effects and interaction terms less interpretable.
2.2. Results
2.2.1. Demographics
Participant demographics are reported in Table 1, and did not meaningfully differ between groups. Pairwise comparisons reveal a change in conventional cigarette risk perception for the CDC group (MD = 4.72, p < .001, d = 0.33) but not the ENDS narrative groups (E-cigaretteControl MD = −0.32, p = .89, d = 0.02; E-cigaretteAuthority MD = 2.15, p = .51, d = 0.13; E-cigaretteSocial Proof MD = 2.97, p = .16, d = 0.18). Pairwise comparisons did reveal a change in e-cigarette risk perception for the E-cigaretteAuthority (MD = −7.63, p < .001, d = 0.35) and E-cigaretteSocial Proof (MD = −7.18, p < .001, d = 0.33) narrative groups indicating that these participants rated ENDS as less risky after reading their assigned narrative.
Table 1.
Experiment 1 Participant Demographics
| CDC | E-cigaretteControl | E-cigaretteAuthority | E-cigaretteSocial Proof | Total | |
|---|---|---|---|---|---|
| Demographics | |||||
| Age | 33.05(7.79) | 36.68(9.62) | 39.20(13.16) | 37.58(13.81) | 36.62(11.48) |
| Education (years) | 13.23(2.34) | 13.78(2.50) | 13.81(2.69) | 13.73(2.18) | 13.63(2.53) |
| Employment Status (employed) | 80% | 78% | 83% | 73% | 79% |
| Gender (Male) | 63% | 75% | 68% | 60% | 66% |
| Yearly Income | $45,967 ($33,278) |
$42,986 ($25,056) |
$36,210 ($22,112) |
$43,277 ($33,248) |
$42,122 ($28,816) |
| Race (Caucasian) | 85% | 73% | 78% | 75% | 78% |
| Relationship Status (married or cohabitating) | 40% | 40% | 38% | 38% | 39% |
| Fagerström | 11.29(1.35) | 11.05(1.39) | 10.95(1.48) | 10.71(1.35) | 11.01(1.40) |
| Daily Nicotine Product Use | |||||
| Chew (single pouch) | 0.32(1.13) | 0.26(1.62) | 0.20(0.91) | 0.18(0.73) | 0.24(1.14) |
| Conventional Cigarettes (single) | 16.90(4.86) | 16.87(8.10) | 17.78(7.18) | 17.82(10.23) | 17.34(7.72) |
| Disposable ENDS (single) | 0.07(0.26) | 0.11(0.45) | 0.05(0.22) | 0.16(0.72) | 0.10(0.45) |
| mL of E-liquid (1 mL) | 0.32(1.13) | 0.26(1.62) | 0.20(0.91) | 0.18(0.73) | 0.24(1.14) |
| Nicotine Gum (single) | 0.00(0.00) | 0.05(0.32) | 0.05(0.32) | 0.00(0.00) | 0.03(0.23) |
| Nicotine Lozenge (single) | 0.00(0.00) | 0.00(0.00) | 0.00(0.00) | 0.03(0.16) | 0.00(0.08) |
| Snus (single pouch) | 0.00(0.00) | 0.00(0.00) | 0.00(0.00) | 0.00(0.00) | 0.00(0.00) |
2.2.2. ETM
The effects of the narratives on conventional cigarette purchasing between groups were analyzed by comparing Q0 and α (derived from Equation 1; Koffarnus et al., 2015) using linear regression (Figure 1, Table 2). Equation 1 fit participant data well (mean of individual model fits R2 = 0.98; see Table S1 for additional model fit parameters). Cigarette demand intensity (Qo) was significantly lower in the E-cigaretteAuthority narrative group (b = −56.38, p < .05, d = 0.49). Cigarette demand elasticity (α) was significantly higher in all three e-cigarette narrative groups compared to the CDC narrative (E-cigaretteControl b = 0.46, p < .05, d = 0.93; E-cigaretteAuthority b = 0.33, p < .05, d = 0.56; E-cigaretteSocial Proof b = 0.31, p < .05, d = 0.55), after controlling for Fagerstrom scores (b = −0.17, p < .05), indicating that purchasing of cigarettes decreased more rapidly as a function of price in these groups compared to the CDC group.
Figure 1.
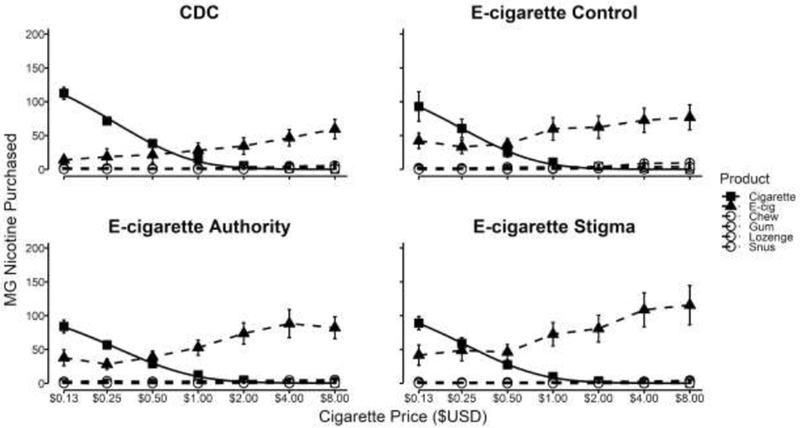
Experiment 1 ETM results for each narrative group. Solid black lines depict the Equation 1 model fit to mg of nicotine purchased at each cigarette price point. x-axis is scaled in log units.
Table 2.
Experiment 1 Regression and GEE Results
| b(std. error) | t-value | |
|---|---|---|
| Cigarette Demand - Intensity (Q0) | ||
| Intercept | 1.04 (106.15) | 0.01 |
| E-cigarette Control Narrative | −31.58 (31.45) | −1.01 |
| E-cigarette Authority Narrative | −56.38 (30.21) | −2.02* |
| E-cigarette Social Proof Narrative | −26.61 (3.06) | −0.86 |
| Fagerstrom Score | 13.18 (7.65) | 1.72 |
| Narrative Transportiveness | 0.77 (1.01) | 0.76 |
| Change in Cigarette Risk Perception | −1.70 (1.25) | −1.36 |
| Cigarette Demand - Elasticity(lnα) | ||
| Intercept | −3.74(0.61) | −6.11*** |
| E-cigarette Control Narrative | 0.46(0.18) | 2.56* |
| E-cigarette Authority Narrative | 0.36(0.17) | 2.21* |
| E-cigarette Social Proof Narrative | 0.38(0.18) | 2.34* |
| Fagerstrom Score | −0.17(0.04) | −3.93*** |
| Narrative Transportiveness | −0.00(0.01) | −0.09 |
| Change in Cigarette Risk Perception | 0.01(0.01) | 1.27 |
| ENDS Initial Intensity of Substitution | ||
| Intercept | −16.70(22.13) | −0.75 |
| E-cigarette Control Narrative | 14.83(6.68) | 2.33* |
| E-cigarette Authority Narrative | 14.38(6.23) | 2.31* |
| E-cigarette Social Proof Narrative | 16.37(6.47) | 2.53* |
| Fagerstrom Score | −0.62(1.57) | −0.39 |
| Narrative Transportiveness | 0.53(0.21) | 2.51* |
| Change in ENDS Risk Perception | −0.45(0.19) | −2.32* |
| Prior ENDS Use | 6.43(3.09) | 2.08* |
| ENDS Substitution Slope (sgrtslope) | ||
| Intercept | −2.19(4.61) | −0.47 |
| E-cigarette Control Narrative | −0.27(1.33) | −0.20 |
| E-cigarette Authority Narrative | 0.84(1.3) | 0.64 |
| E-cigarette Social Proof Narrative | 2.30(1.32) | 1.74 |
| Fagerström Score | 0.54(0.33) | 1.63 |
| Narrative Transportiveness | 0.01(0.04) | 0.16 |
| Change in ENDS Risk Perception | −0.00(0.03) | −0.08 |
| Prior ENDS Use | 0.51(0.35) | 1.48 |
p < .05
p < .01
p < .001
The effects of the narratives on ENDS substitution between groups were analyzed by comparing the regression model fit intercepts (initial intensity of substitution) and slopes (Figure 1, Table 2). Participants in all three ENDS narratives purchased more ENDS at the lowest conventional cigarette price compared to the CDC narrative (E-cigaretteControl b = 14.83, p < .05, d = 0.45; E-cigaretteAuthority b = 14.38, p < .05, d = 0.71; E-cigaretteSocialProof b = 16.37, p < .05, d = 0.71). Transportiveness of narratives (b = 0.53, p < .05) and prior ENDS experience (b = 6.43, p < .05) also predicted ENDS purchasing across the four narrative groups, with higher levels of transportiveness and greater ENDS experience predicting greater ENDS purchasing. Importantly, change in ENDS risk perception predicted initial ENDS purchasing across the four narrative groups (b = 0.45, p < .05) with greater decreases in ENDS risk perception resulting in greater ENDS purchasing.
To demonstrate the importance of the availability of a viable substitute for reducing conventional cigarette smoking, a final regression model was conducted. Conventional cigarette demand intensity was lower in participants with greater ENDS initial intensity of substitution (b = −1.26, p < .01) and greater substitution of ENDS as the price of conventional cigarettes increases (b = −8.40, p < .001).
2.3. Experiment 1 Discussion
The results of Experiment 1 demonstrate that narratives designed to engender ENDS substitution can reduce conventional cigarette purchasing by increasing the substitutability of ENDS, even when controlling for covariates such as nicotine dependence (e.g., FTCD) and prior ENDS use. The narrative invoking authority was the only narrative effective at reducing conventional cigarette demand intensity whereas all three ENDS narratives decreased conventional cigarette demand elasticity and increased the initial intensity of ENDS substitution compared to the CDC narrative. Importantly, a reduction in the perceived risk of ENDS provides one possible mechanism for these differences. Participants who reported a decrease in ENDS risk perception after reading their narrative were more likely to purchase ENDS in the ETM compared to those who showed no change in ENDS risk perception. Significant changes in risk perception pre-post were only observed with the E-cigaretteAuthority and E-cigaretteSocial Proof narratives, suggesting these may have the greatest translational potential. These results, interpreted as a whole, would suggest that the most effective method of promoting harm-reduction behaviors is through the engagement of both health professionals (to reduce the perception of harm) and peers (to both reduce the perception of harm and increase social acceptance). Indeed, the number of smokers who discuss switching to ENDS with their doctor is low (e.g., 15%; (Kollath-Cattano et al., 2016) and many physicians do not recommend ENDS for smoking cessation (Ofei-Dodoo et al., 2017) despite some evidence that switching could be beneficial (Brown et al., 2014; Kalkhoran and Glantz, 2016; Notley et al., 2018; Selya et al., 2017).
3. Experiment 2
The purpose of Experiment 2 was to determine which strategy is more effective in decreasing demand for conventional cigarettes and increasing the substitutability of ENDS: appealing to health or financial benefits of substituting ENDS.
3.1. Methods
The methods of Experiment 2 were identical to Experiment 1 with a few exceptions including recruitment and power analyses. Participants that completed Experiment 1 could not participate in Experiment 2. First, the narratives in Experiment 2 described either the health (HealthControl; n = 40) or financial (FinancesControl; n = 40) consequences of smoking conventional cigarettes, as well as the health (HealthE-cigarette; n = 38) or financial (FinancesE-cigarette; n = 39) benefits of switching to ENDS. Participants also completed a financial health survey (Bureau, 2017). Finally, an additional ETM trial was employed where conventional cigarettes were priced at $0.06 in order to provide a larger range of conventional cigarette prices.
One-hundred and twenty-eight participants completed Experiment 2. Participant demographics were nearly identical to Experiment 1 and are fully reported in the Supplemental Material (Table S2). Analyses are also identical to Experiment 1. For the regression analysis, the HealthControl served as the reference group. The groups compared in subsequent pairwise comparisons are explicitly stated.
3.2. Results
3.2.1. Cigarette and ENDS Risk Perception
Pairwise comparisons identified significant changes in conventional cigarette risk perception in the HealthControl (MD = 4.67, p < .001, d = 0.28) and HealthE-cigarette (MD = 2.53, p < .001, d = 0.14) groups, meaning that participants in these groups perceived the risk of conventional cigarettes as higher after reading their assigned narrative. No significant changes in conventional cigarette risk perception were reported in the FinancesControl (MD = 0,87, p = .92, d = 0.04) or FinancesE-cigarette (MD = 1.33, p = .35, d = 0.08) narrative groups. Pairwise comparisons also identified significant changes in ENDS risk perception in the HealthControl (MD = 2.63, p < .05, d = 0.12), HealthE-cigarette (MD = −6.82, p< .001, d = 0.38), and FinancesE-cigarette (MD = −2.21 ,p< .05, d = 0.11) groups but not the FinancesControl (MD = −2.10,p = 0.10, d = 0.08) group. These findings indicate that ENDS risk perception decreased in the HealthE-cigarette and FinancesE-cigarette groups but increased in the HealthControl group.
3.2.2. ETM
The effects of the narratives on conventional cigarette purchasing between groups were analyzed by comparing Qo and a (derived from Equation 1; Koffarnus et al., 2015) using linear regression (Figure 2, Table 3). Equation 1 fit participant data well (meanf?2 = 0.91; see Table S1 for additional model fit parameters). Conventional cigarette demand intensity (Qo) was significantly lower in the HealthE-cigarette (b = −156,74, p < .001, d = 0.92) and FinancesE-cigarette (b = −142.33,p< .001, d = 0.80) narrative groups compared to the HealthControl meaning that participants in these groups purchased fewer conventional cigarettes compared to the HealthControl group. Importantly, pairwise comparisons also revealed that demand intensity for conventional cigarettes was lower in the HealthE-cigarette (MD = −119.33,p< .01, d = 0.80) and FinancesE-cigarette (MD = −107.54,p< .01, d = 0.67) narrative groups compared to the FinancesControl. No difference in demand intensity was found between the HealthControl and FinancesControl groups (MD = 39.56, p = 0.43, d = 0.19). No significant differences in conventional cigarette demand elasticity (a) between groups was found and no other covariates (e.g., Narrative Transportiveness) predicted demand intensity or elasticity.
Figure 2.
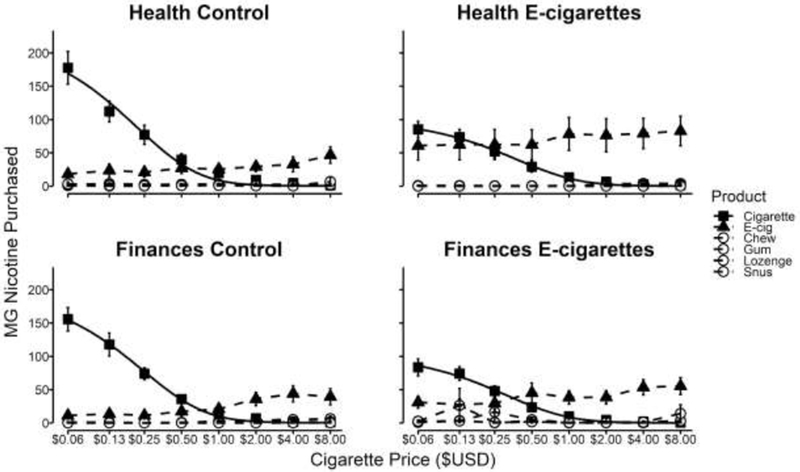
Experiment 2 ETM results for each narrative group. Solid black lines depict the Equation 1 model fit to mg of nicotine purchased at each cigarette price point. x-axis is scaled in log units.
Table 3.
Experiment 2 Regression and GEE Results
| b(std. error) | t-value | |
|---|---|---|
| Cigarette Demand - Intensity (Q0) | ||
| Intercept | 299.15(137.77) | 2.17* |
| Finances Control | −46.62(46.62) | −1.01 |
| Health w/ E-cigarettes | −156.74(43.82) | −3.58*** |
| Finances w/ E-cigarettes | −142.33(45.68) | −3.12** |
| Fagerström Score | −1.37(10.68) | −0.13 |
| Narrative Transportiveness | −0.08(1.48) | −0.06 |
| Change in Cigarette Risk Perception | 0.65(2.71) | 0.24 |
| Cigarette Demand - Elasticity(lnα) | ||
| Intercept | −5.23(0.90) | −5.82*** |
| Finances Control | −0.19(0.30) | −0.65 |
| Health w/ E-cigarehes | 0.44(0.29) | 1.54 |
| Finances w/ E-cigarehes | 0.45(0.30) | 1.51 |
| Fagerstrom Score | −0.08(0.07) | −1.08 |
| Narrative Transportiveness | 0.01(0.01) | 0.96 |
| Change in Cigarette Risk Perception | −0.01(0.02) | −0.42 |
| ENDS Initial Intensity of Substitution | ||
| Intercept | 38.47(15.25) | 2.52* |
| Finances Control | 3.46(21.39) | 0.16 |
| Health w/ E-cigarehes | 40.93(21.39) | 2.03* |
| Finances w/ E-cigarehes | 12.56(21.39) | 0.59 |
| Fagerstrom Score | −9.51(5.44) | −1.75 |
| Narrative Transportiveness | 0.59(0.73) | 0.80 |
| Change in ENDS Risk Perception | −0.47(0.79) | −0.59 |
| Prior ENDS Use | 0.14(0.18) | 0.80 |
| ENDS Substitution Slope (sgrtslope) | ||
| Intercept | 2.45(1.68) | 1.45 |
| Finances Control | 0.13(0.52) | 0.25 |
| Health w/ E-cigarettes | 0.16(0.56) | 0.29 |
| Finances w/ E-cigarettes | 0.56(0.56) | 1.02 |
| Fagerstrom Score | −0.02(0.13) | −0.17 |
| Narrative Transportiveness | −0.01(0.02) | −0.31 |
| Change in ENDS Risk Perception | −0.03(0.02) | −1.17 |
| Prior ENDS Use | 0.52(0.16) | 3.14** |
p < .05
p < .01
p < .001
The effects of the narratives on ENDS substitution between groups were analyzed by comparing the regression model fit intercepts (initial intensity of substitution) and slopes (Figure 2, Table 3). Only participants in the HealthE-cigarette group purchased more ENDS compared to the HealthControl group at the lowest conventional cigarette price (b = 40.93, p < .05, d = 0.44). Further pairwise comparisons did not reveal additional differences. Regarding the regression model slope, only prior ENDS use predicted increases in ENDS substitution as the price of conventional cigarettes increased (b = 0.51, p < .01). Again, pairwise comparisons did not reveal any additional differences. No additional significant predictors of ENDS initial intensity of demand and slope were identified.
To demonstrate the importance of the availability of a viable substitute for reducing conventional cigarette smoking, a final regression model was conducted. Conventional cigarette demand intensity was not predicted by the initial intensity of ENDS substitution or the slope of ENDS substitution, but conventional cigarette demand elasticity was predicted by ENDS initial intensity of substitution (b = −0.001, p < .01) but not the slope of ENDS substitution (b = −0.00, p = .56).
3.3. Experiment 2 Discussion
The results of Experiment 2 further the findings of Experiment 1 (DeHart et al., n.d.), that narratives encouraging ENDS substitution can both decrease conventional cigarette purchasing and increase ENDS substitution. Both the HealthE-cigarette and FinancesE-cigarette groups purchased fewer conventional cigarettes, but only the HealthE-cigarette group purchased more ENDS compared to the other groups, suggesting that highlighting the financial consequences of smoking reduces conventional cigarette purchasing but does not increase substitution of an alternative. In practice, such an outcome could be preferred (e.g., decrease in smoking without the need for a substitute) and future financial narratives should explore the efficacy of targeting cigarette smoking without promoting a substitute. Importantly, DeHart et al. (2018) demonstrated that health narratives are most effective when promoting a substitute. These divergent findings should be explored further. Highlighting the combined health and financial benefits may have a compounding effect and further reduce conventional cigarette purchasing while subsequently increasing ENDS substitution. Unlike Experiment 1, changes in conventional cigarettes and ENDS risk perception did not predict purchasing in the ETM. One explanation is that these narratives did not directly address risk perception to the same extent as the narratives in Experiment 1.
4. General Discussion
The purpose of these experiments was to evaluate the effectiveness of narratives in promoting behavior change (e.g., increasing the substitutability of ENDS) in the ETM and to identify specific cognitive biases that can be incorporated to improve their effectiveness. Three aspects will be discussed: 1) key findings from Experiment 1, 2) key findings from Experiment 2, and 3) overarching patterns.
The results of Experiment 1 suggest that both authority and social proof heuristics can improve the effectiveness of narratives; however, only the E-cigaretteAuthority narrative produced a significant decrease in conventional cigarette demand intensity though all three ENDS narratives increased demand elasticity as well as the initial intensity of substitution for ENDS. Reducing the perceived risk of ENDS may provide one method for increasing their substitutability. In Experiment 1, we found that participants who reported a decrease in the perceived risk of ENDS substituted more ENDS. These results suggest that multiple sources of influence can alter cigarette consumption and ENDS substitution.
The results of Experiment 2 demonstrate that highlighting the financial savings of substituting ENDS can decrease conventional cigarette demand intensity though no effect was seen on ENDS substitution. Research has demonstrated links between successful smoking cessation and finances (Kendzor et al., 2018; Widome et al., 2015) and this is a common tactic used in public-health narrative interventions. A combination of highlighting the health and financial benefits could have an additive effect, resulting in even larger decreases in conventional cigarette demand and increases in ENDS substitution. In future research, we will explore the effects of combining the different effective cognitive biases on purchasing in the ETM.
Overall, the results of both Experiments 1 and 2 indicate that narratives that target harm-reduction outcomes can successfully reduce conventional cigarette smoking and that targeting different cognitive biases and mechanisms can have similar outcomes. This flexibility is important, as different narratives may be more appropriate for different groups, environments, and modes of dissemination. Importantly, as the ability of technology to customize information exposure grows, understanding what narrative strategies are most effective for different conditions becomes vital.
One important finding from both experiments is the general absence in purchasing of any alternative tobacco product besides ENDS even no narratives that did not promote ENDS use. This finding has important public health implications as narrative driven decreases in conventional cigarette demand (intensity and/or elasticity) frequently, though not always, corresponded with increases in ENDS substitution (initial intensity of substitution and/or slope of substitution). While the CDC narrative in Experiment 1 produced lower conventional cigarette purchasing compared to the HealthControl (QoMD = −78.44, p < .05) narrative from Experiment 2, presenting a viable substitute reduced conventional cigarette purchasing even further. This finding is especially revealing as participants were not required to spend their account balance meaning that they would rather purchase a substitute than save the extra money. While the evidence on the effectiveness of ENDS as a harm-reduction tool is still preliminary (Notley et al., 2018; Warner, 2018; Warner and Mendez, 2018), our results demonstrate that promoting a viable substitute (e.g., ENDS, nicotine gum) could better reduce conventional cigarette consumption compared to presenting the consequences of smoking alone (e.g. CDC, HealthControl and FinancesControl narrative groups). Of course, any amount of tobacco consumption can have negative health impacts on individuals (Hackshaw et al. 2018); however, for many, ENDS present a possible alternative that could reduce (though not eliminate) the consequences of nicotine consumption (Lightwood & Glantz 2016).
One limitation is that a large proportion of our participants were naive ENDS users (85% in Experiment 1 and 87% in Experiment 2). Typically, assessing demand requires experience with the reinforcing effects of an outcome. Naive ENDS users may be unfamiliar with how many disposable ENDS or mL of e-liquid are required to effectively replace conventional cigarettes despite the ETM providing comparable units. As a result, ENDS purchasing was based on expectations of the product and not actual experience. The uptake in purchasing of hypothetical ENDS in naive users, however, is still valuable because an increase in purchasing of ENDS in the ETM may reflect an increase in the participant’s willingness to sample ENDS, which could result in greater ENDS uptake and less conventional cigarette consumption (Tucker et al., 2018). A second limitation and point of future study is to test if narratives are more effective in individuals that already are motivated to quit, are currently experiencing a tobacco-related disease, or are currently treatment seeking for tobacco use compared to cigarette smokers not experiencing these conditions. Conceivably, t narratives could serve as a catalyst for individuals that are strongly considering or are already in the process of reducing their conventional cigarette consumption. A final limitation of the present work is that the ETM was only administered after the narrative presentation. Despite similarities in demographics and tobacco consumption between the four conditions, our conclusions are limited by the implementation of a between-group design. Future research should investigate the effects of narrative in the ETM by asking participants to complete the ETM both before and after narrative presentation.
5. Conclusions
The combined results of both experiments advocate for a holistic approach to behavior change and smoking reduction. Narratives that addressed the health and financial benefits of ENDS substitution, and authority and peer influence all impacted conventional cigarette purchasing and ENDS substitution. In sum, public-health narratives can provide an effective tool for rapid and widespread information dissemination.
Supplementary Material
Highlights.
Substituting e-cigarettes for cigarettes may minimize health losses
Public health narratives are one effective strategy for encouraging substitution
The Experimental Tobacco Marketplace (ETM) is a tool to study narrative effectiveness
Narratives decreased cigarette, and increased e-cigarette purchasing in the ETM
Narratives are a promising intervention in the ETM with translational potential
Acknowledgments
Funding
This work was supported by the Fralin Biomedical Research Institute at VTC and by NIH Grant No. R01DA034755. This work was also supported by NIDA/NIH grant R01DA042535 and FDA Center for Tobacco Products (CTP). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH or the Food and Drug Administration.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
- William Brady DeHart - None
- Alexandra M. Mellis - None
- Brent A. Kaplan - Principal for BEAM Diagnostics, Inc.
- Derek A. Pope - None
- W. K. Bickel is a principal of HealthSim, LLC; Notifius, LLC; BEAM Diagnostics, Inc.; and a partner for Red 5 Group, LLC. In addition, he serves on the scientific advisory board for Sober Grid, Inc.; Ria Health; US WorldMeds, LLC; and is a consultant for Alkermes, Inc.
Contributor Information
W. Brady DeHart, Addiction Recovery Research Center, Virginia Tech Carilion Research Institute, Roanoke, VA, USA, 540-526-2236
Alexandra M. Mellis, Graduate Program in Translational Biology, Medicine, and Health, Virginia Tech, Blacksburg, Virginia, USA, 540-526-2136
Brent A. Kaplan, Addiction Recovery Research Center, Virginia Tech Carilion Research Institute, Roanoke, VA, USA, 540-526-2072
Derek A. Pope, Addiction Recovery Research Center, Virginia Tech Carilion Research Institute, Roanoke, VA, USA, 540-526-2017
Warren K. Bickel, Addiction Recovery Research Center, Virginia Tech Carilion Research Institute, Roanoke, Virginia, USA; Department of Psychiatry and Behavioral Medicine, Virginia Tech Carilion School of Medicine, Roanoke, VA, USA; Graduate Program in Translational Biology, Medicine, and Health, Virginia Tech, Blacksburg, Virginia, USA; Department of Psychology, Virginia Tech, Blacksburg, VA, USA; Department of Neuroscience, Virginia Tech, Blacksburg, VA, USA; Faculty of Health Sciences, Virginia Tech, Blacksburg, VA, USA, 540-526-2088
5. References
- Abrams DB, Glasser AM, Villanti AC, Pearson JL, Rose S, Niaura RS, 2018. Managing nicotine without smoke to save lives now: Evidence for harm minimization. Prev. Med. 10.1016/j.ypmed.2018.06.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berry KM, Reynolds LM, Collins JM, Siegel MB, Fetterman JL, Hamburg NM, Bhatnagar A, Benjamin EJ, Stokes A, 2018. E-cigarette initiation and associated changes in smoking cessation and reduction: the Population Assessment of Tobacco and Health Study, 2013-2015. Tob. Control. 10.1136/tobaccocontrol-2017-054108 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bickel WK, Pope DA, Kaplan BA, Brady DeHart W, Koffarnus MN, Stein JS, 2018. Electronic cigarette substitution in the experimental tobacco marketplace: A review. Prev. Med. 10.1016/j.ypmed.2018.04.026 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bickel WK, Stein JS, Moody LN, Snider SE, Mellis AM, Quisenberry AJ, 2017. Toward Narrative Theory: Interventions for Reinforcer Pathology in Health Behavior, in: Impulsivity, Nebraska Symposium on Motivation. Springer, Cham, pp. 227–267. [PubMed] [Google Scholar]
- Brown J, Beard E, Kotz D, Michie S, West R, 2014. Real-world effectiveness of e-cigarettes when used to aid smoking cessation: a cross-sectional population study. Addiction 109, 1531–1540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bureau CFP, 2017. CFPB Financial Well-Being Scale: Scale Development Technical Report. Washington DC: CFPB. [Google Scholar]
- CDCTobaccoFree, 2018. Tips From Former SmokersTM [WWW Document]. Centers for Disease Control and Prevention. URL https://www.cdc.gov/tobacco/campaign/tips/index.html (accessed 7.25.18).
- Coleman BN, Johnson SE, Tessman GK, Tworek C, Alexander J, Dickinson DM, Rath J, Green KM, 2016. “It’s not smoke. It’s not tar. It’s not 4000 chemicals. Case closed”: Exploring attitudes, beliefs, and perceived social norms of e-cigarette use among adult users. Drug Alcohol Depend. 159, 80–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeHart WB, Kaplan BA, Pope DA, Mellis AM, Bickel WK, n.d Using Narratives to Promote Substitution of Electronic Cigarettes for Conventional Cigarettes in an online Experimental Tobacco Marketplace. Under Review. [Google Scholar]
- Denes-Raj V, Epstein S, 1994. Conflict between intuitive and rational processing: when people behave against their better judgment. J. Pers. Soc. Psychol. 66, 819–829. [DOI] [PubMed] [Google Scholar]
- Dillard AJ, Fagerlin A, Dal Cin S, Zikmund-Fisher BJ, Ubel PA, 2010. Narratives that address affective forecasting errors reduce perceived barriers to colorectal cancer screening. Soc. Sci. Med. 71, 45–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fagerstrom K, 2012. Determinants of Tobacco Use and Renaming the FTND to the Fagerstrom Test for Cigarette Dependence. Nicotine Tob. Res. 14, 75–78. [DOI] [PubMed] [Google Scholar]
- Faul F, Erdfelder E, Buchner A, Lang A-G, 2009. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav. Res. Methods 41, 1149–1160. [DOI] [PubMed] [Google Scholar]
- Frank LB, Murphy ST, Chatterjee JS, Moran MB, Baezconde-Garbanati L, 2015. Telling stories, saving lives: creating narrative health messages. Health Commun. 30, 154–163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gigerenzer G, Goldstein DG, 2011. Reasoning the Fast and Frugal Way: Models of Bounded Rationality, in: Heuristics: Oxford University Press. [DOI] [PubMed] [Google Scholar]
- Grace RC, Kivell BM, Laugesen M, 2015. Estimating cross-price elasticity of e-cigarettes using a simulated demand procedure. Nicotine Tob. Res. 17, 592–598. [DOI] [PubMed] [Google Scholar]
- Green MC, Brock TC, 2000. The role of transportation in the persuasiveness of public narratives. J. Pers. Soc. Psychol. 79, 701–721. [DOI] [PubMed] [Google Scholar]
- Heckman BW, Cummings KM, Hirsch AA, Quisenberry AJ, Borland R, O’Connor RJ, Fong GT, Bickel WK, 2017. A Novel Method for Evaluating the Acceptability of Substitutes for Cigarettes: The Experimental Tobacco Marketplace. Tobacco Regulatory Science 3, 266–279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hirsh JB, Kang SK, Bodenhausen GV, 2012. Personalized persuasion: tailoring persuasive appeals to recipients’ personality traits. Psychol. Sci. 23, 578–581. [DOI] [PubMed] [Google Scholar]
- Hursh SR, Bauman RA, 1987. The behavioral analysis of demand. Advances in behavioral economics 1, 117–165. [Google Scholar]
- Kalkhoran S, Glantz SA, 2016. E-cigarettes and smoking cessation in real-world and clinical settings: a systematic review and meta-analysis. Lancet Respir Med 4, 116–128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaplan BA, Gilroy SP, Reed DD, Koffarnus MN, Hursh SR, 2018. The R package beezdemand: Behavioral economic easy demand. Perspectives on Behavioral Science, accepted. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kendzor DE, Businelle MS, Waters AF, Frank SG, Hébert ET, 2018. Financial strain indirectly influences smoking cessation through withdrawal symptom severity. Drug Alcohol Depend. 183, 55–61. [DOI] [PubMed] [Google Scholar]
- Kiene SM, Barta WD, 2003. Personal Narrative as a Medium for STD/HIV Intervention: A Preliminary Study1. J. Appl. Soc. Psychol. 33, 2327–2340. [Google Scholar]
- Koffarnus MN, Franck CT, Stein JS, Bickel WK, 2015. A modified exponential behavioral economic demand model to better describe consumption data. Exp. Clin. Psychopharmacol. 23, 504–512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kollath-Cattano C, Thrasher JF, Osman A, Andrews JO, Strayer SM, 2016. Physician Advice for e-Cigarette Use. J. Am. Board Fam. Med. 29, 741–747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kreuter MW, Holmes K, Alcaraz K, Kalesan B, Rath S, Richert M, McQueen A, Caito N, Robinson L, Clark EM, 2010. Comparing narrative and informational videos to increase mammography in low-income African American women. Patient Educ. Couns. 81 Suppl, S6–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kroon GE, 2007. Macroeconomics the Easy Way. Barron’s Educational Series. [Google Scholar]
- Lenth R, 2018. Emmeans: Estimated marginal means, aka least-squares means. R Package Version 1. [Google Scholar]
- Mooney ME, Leventhal AM, Hatsukami DK, 2006. Attitudes and knowledge about nicotine and nicotine replacement therapy. Nicotine Tob. Res. 8, 435–446. [DOI] [PubMed] [Google Scholar]
- Murphy ST, Frank LB, Chatterjee JS, Moran MB, Zhao N, Amezola de Herrera P, Baezconde-Garbanati LA, 2015. Comparing the Relative Efficacy of Narrative vs Nonnarrative Health Messages in Reducing Health Disparities Using a Randomized Trial. Am. J. Public Health 105, 2117–2123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Center for Chronic Disease Prevention and Health Promotion (US) Office on Smoking and Health, 2014. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. Centers for Disease Control and Prevention (US), Atlanta (GA). [PubMed] [Google Scholar]
- Neff LJ, Patel D, Davis K, Ridgeway W, Shafer P, Cox S, 2016. Evaluation of the National Tips From Former Smokers Campaign: the 2014 Longitudinal Cohort. Prev. Chronic Dis. 13, E42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Notley C, Ward E, Dawkins L, Holland R, 2018. The unique contribution of e-cigarettes for tobacco harm reduction in supporting smoking relapse prevention. Harm Reduct. J. 15, 31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nummenmaa L, Saarimäki H, Glerean E, Gotsopoulos A, Jääskeläinen IP, Hari R, Sams M, 2014. Emotional speech synchronizes brains across listeners and engages large-scale dynamic brain networks. Neuroimage 102 Pt 2, 498–509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ofei-Dodoo S, Kellerman R, Nilsen K, Nutting R, Lewis D, 2017. Family Physicians’ Perceptions of Electronic Cigarettes in Tobacco Use Counseling. J. Am. Board Fam. Med. 30, 448–459. [DOI] [PubMed] [Google Scholar]
- Phillips CV, 2009. Debunking the claim that abstinence is usually healthier for smokers than switching to a low-risk alternative, and other observations about anti-tobacco-harm-reduction arguments. Harm Reduct. J. 6, 29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pope DA, Poe L, Stein JS, Kaplan BA, Heckman BW, Epstein LH, Bickel WK, 2018. Experimental tobacco marketplace: substitutability of e-cigarette liquid for cigarettes as a function of nicotine strength. Tob. Control. 10.1136/tobaccocontrol-2017-054024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quisenberry AJ, Eddy CR, Patterson DL, Franck CT, Bickel WK, 2015. Regret Expression and Social Learning Increases Delay to Sexual Gratification. PLoS One 10, e0135977. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quisenberry AJ, Koffarnus MN, Epstein LH, Bickel WK, 2017. The Experimental Tobacco Marketplace II: Substitutability and sex effects in dual electronic cigarette and conventional cigarette users. Drug Alcohol Depend. 178, 551–555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quisenberry AJ, Koffarnus MN, Hatz LE, Epstein LH, Bickel WK, 2016. The Experimental Tobacco Marketplace I: Substitutability as a Function of the Price of Conventional Cigarettes. Nicotine Tob. Res. 18, 1642–1648. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reed DD, Niileksela CR, Kaplan BA, 2013. Behavioral economics: a tutorial for behavior analysts in practice. Behav. Anal. Pract. 6, 34–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rothman AJ, Bartels RD, Wlaschin J, Salovey P, 2006. The Strategic Use of Gain- and Loss-Framed Messages to Promote Healthy Behavior: How Theory Can Inform Practice. J. Commun. 56, S202–S220. [Google Scholar]
- Salmon SJ, De Vet E, Adriaanse MA, Fennis BM, Veltkamp M, De Ridder DTD, 2015. Social proof in the supermarket: Promoting healthy choices under low self-control conditions. Food Qual. Prefer. 45, 113–120. [Google Scholar]
- Salmon SJ, Fennis BM, de Ridder DTD, Adriaanse MA, de Vet E, 2014. Health on impulse: when low self-control promotes healthy food choices. Health Psychol. 33, 103–109. [DOI] [PubMed] [Google Scholar]
- Selya AS, Dierker L, Rose JS, Hedeker D, Mermelstein RJ, 2017. The Role of Nicotine Dependence in E-Cigarettes’ Potential for Smoking Reduction. Nicotine Tob. Res. 10.1093/ntr/ntx160 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sobell LC, Sobell MB, 1992. Timeline Follow-Back, in: Measuring Alcohol Consumption. Humana Press, Totowa, NJ, pp. 41–72. [Google Scholar]
- Soneji SS, Sung H-Y, Primack BA, Pierce JP, Sargent JD, 2018. Quantifying population-level health benefits and harms of e-cigarette use in the United States. PLoS One 13, e0193328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tucker MR, Laugesen M, Bullen C, Grace RC, 2018. Predicting Short-Term Uptake of Electronic Cigarettes: Effects of Nicotine, Subjective Effects, and Simulated Demand. Nicotine Tob. Res. 20, 1265–1271. [DOI] [PubMed] [Google Scholar]
- Tversky A, Kahneman D, 1974. Judgment under Uncertainty: Heuristics and Biases. Science 185, 1124–1131. [DOI] [PubMed] [Google Scholar]
- Warner KE, 2018. How to Think--Not Feel--about Tobacco Harm Reduction. Nicotine Tob. Res. [DOI] [PubMed] [Google Scholar]
- Warner KE, Mendez D, 2018. E-cigarettes: Comparing the Possible Risks of Increasing Smoking Initiation with the Potential Benefits of Increasing Smoking Cessation. Nicotine Tob. Res. 10.1093/ntr/nty062 [DOI] [PubMed] [Google Scholar]
- Widome R, Joseph AM, Hammett P, Van Ryn M, Nelson DB, Nyman JA, Fu SS, 2015. Associations between smoking behaviors and financial stress among low-income smokers. Prev Med Rep 2, 911–915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Winterbottom A, Bekker HL, Conner M, Mooney A, 2008. Does narrative information bias individual’s decision making? A systematic review. Soc. Sci. Med. 67, 2079–2088. [DOI] [PubMed] [Google Scholar]
- Xu X, Bishop EE, Kennedy SM, Simpson SA, Pechacek TF, 2015. Annual healthcare spending attributable to cigarette smoking: an update. Am. J. Prev. Med. 48, 326–333. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.