

Abstract
Background: Carotid webs are luminal, shelf-like protrusions at the carotid bulb. Considered to be a variant of fibromuscular dysplasia, carotid webs have been observed principally in African American females. The association between carotid webs and recurrent ischemic strokes continues to be established as patients without traditional stroke risk factors are found to have carotid webs as the only possible cause of symptomatic deficits. The majority of patients undergo endarterectomy; few stent placements are reported. We present the case of an African American female who underwent stent placement for treatment and secondary prevention of stroke attributed to a carotid web.
Case Report: A 33-year-old African American female presented with acute onset left hemiparesis and left facial droop. Alteplase was administered; multiphase head and neck computed tomography angiography revealed an occlusion of the right middle cerebral artery with a web at the carotid bulb. Aspiration catheter thrombectomy achieved a Thrombolysis in Cerebral Infarction (TICI) score of 3. She was placed on 2 antiplatelet agents, and 3 weeks later she underwent stent placement. Follow-up digital subtraction angiography at 3 months showed obliteration of the right carotid artery web and satisfactory integration of the stent into the vessel wall. She was reassessed at 1 year and reported no neurologic symptoms.
Conclusion: Although carotid webs are most commonly treated with endarterectomy, they may be amenable to stent therapy with favorable clinical outcomes as shown with this patient.
Keywords: Carotid web, fibromuscular dysplasia, stents, stroke
INTRODUCTION
A carotid web is a thin, shelf-like luminal protrusion of the intimal layer of the internal carotid artery (ICA) that is usually visualized at the bulb by computed tomography angiography (CTA). The literature proposes a developmental etiology for carotid web formation1,2 as opposed to fibromuscular dysplasia (FMD) that is believed to develop as a result of mural ischemia.3 Because carotid webs are a rare pathologic finding, more is yet to be elucidated regarding their pathophysiology, prevalence, thrombus formation risk, and appropriate intervention. Compagne et al4 reported that 2.5% of patients in the MR CLEAN trial had an identifiable carotid bifurcation. Other studies suggest a prevalence of 21.2%-37% in patients diagnosed with cryptogenic stroke.5,6 A study conducted by Joux et al revealed a high prevalence of carotid bulb diaphragms in a young Afro-Caribbean population, underscoring the relevance of a high index of suspicion for carotid webs in the setting of recurrent strokes in African Americans.7
Carotid webs are thought to be a variant of FMD, and carotid web histopathology shows intimal thickening and hyperplasia of the fibromuscular layer.2,8,9 Grossly, a carotid web can be identified on imaging as an intraluminal protrusion at the posterior wall of the carotid bifurcation that may contribute to turbulent flow and thrombus formation; however, this defect does not cause intraluminal narrowing as is the case with FMD.1 In contrast to carotid webs, FMD has been classically described as a “string of beads” on angiography because of the kinked appearance the artery displays.3
Recurrent strokes in the absence of traditional stroke risk factors have been previously associated with carotid webs, highlighting the need for an established therapeutic course.1,10 Treatment of carotid webs has generally been with endarterectomy,2 although Choi et al reported a case series in 2015 in which they used endovascular stent placement in patients who had failed treatment with antiplatelet agents.1 Additionally, a report by Elmokadem et al from 2016 showed carotid artery web stenting to be an effective treatment modality for secondary prevention of stroke.11
A thorough literature review revealed that to date only 22 patients with a diagnosis of carotid web have been reported as undergoing stent placement as definitive treatment for carotid web disease.2,11-13 With the intent to add to the body of literature and to propose stent placement as a therapeutic option for this rare pathology, we present an African American female patient who was successfully treated with stent placement for her carotid web.
CASE REPORT
A 33-year-old female with no significant medical history (no hypertension, coronary artery disease, hyperlipidemia, diabetes, smoking, or other pertinent stroke risk factors) or recent trauma presented to an outside emergency department with left hemiparesis and left facial droop. Her National Institutes of Health Stroke Scale (NIHSS) score was 9. The patient was treated with alteplase and transferred to our facility for further evaluation and treatment. Multiphase head and neck CTA revealed an occlusion of the second segment (M2) of the right middle cerebral artery, as well as a web at the bulb of the right ICA (Figure 1). Digital subtraction angiography (DSA) of the right common carotid artery (CCA) showed a filling defect with turbulent flow at the bifurcation (Figure 2).
Figure 1.
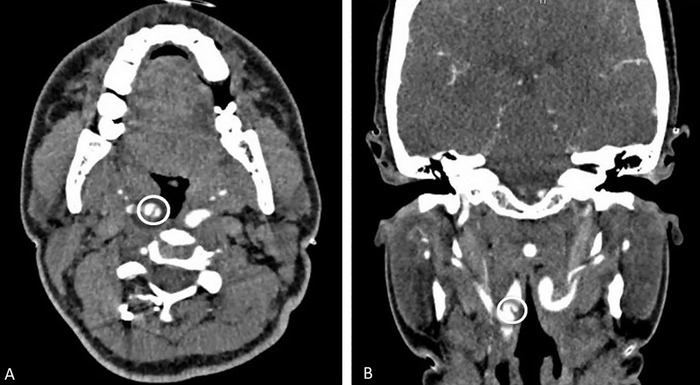
Computed tomography angiogram (A) axial and (B) coronal views show the right internal carotid web near the bifurcation (circles).
Figure 2.
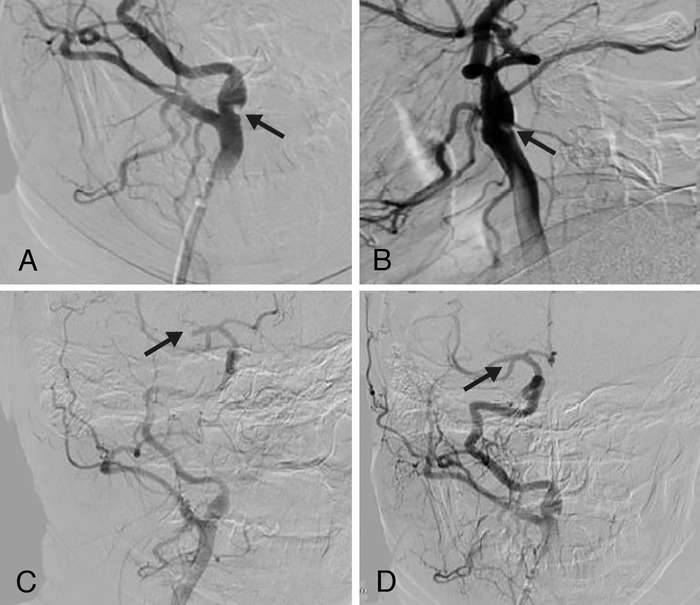
Digital subtraction angiography of injections of the right common carotid artery at the time of presentation in (A) anteroposterior view (B) and lateral view show the carotid web at the bifurcation with a filling defect and turbulent flow at the bifurcation, and (C, D) anteroposterior views show the right middle cerebral artery second segment occlusion with successful mechanical thrombectomy (arrows).
The patient successfully underwent aspiration catheter thrombectomy of the right M2 under conscious sedation to achieve a Thrombolysis in Cerebral Infarction (TICI) score of 3 (Figure 2). Twenty-four hours after alteplase administration, the patient was placed on daily aspirin (81 mg) and clopidogrel (Plavix, 75 mg) for secondary stroke prevention.
After a discussion of endarterectomy vs stenting, the patient agreed to endovascular treatment, and 3 weeks later (once antiplatelet agents were at therapeutic levels), the patient underwent elective right carotid artery stent placement to treat the carotid web. DSA showed obliteration of the right carotid artery web (Figure 3). The patient tolerated the procedure well and was discharged on daily dual antiplatelet agents (aspirin 81 mg and clopidogrel 75 mg) and atorvastatin (10 mg daily).
Figure 3.
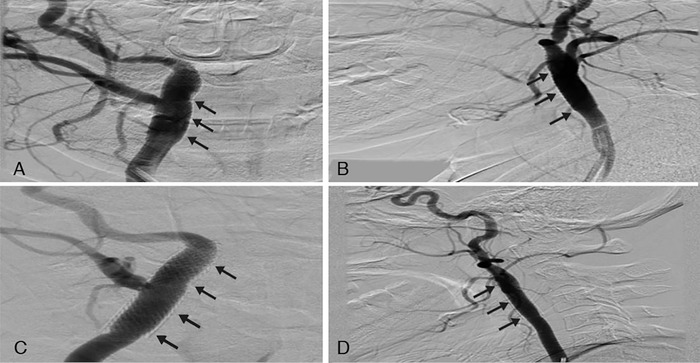
Digital subtraction angiography of injections of the right common carotid artery after stent placement in the (A) anteroposterior view and (B) lateral view 3 weeks after the stroke and in the (C) anteroposterior view and (D) lateral view at 3-month follow-up after stent placement show complete obliteration of the right carotid artery web (arrows).
The patient was reassessed at 2 weeks, at 3 months, and at 1 year. She reported no neurologic symptoms since she was first treated. The patient was advised to stop one antiplatelet agent (clopidogrel) 3 months posttreatment (after DSA showed good stent integration to the carotid wall) and to continue aspirin and the statin for life.
DISCUSSION
Although carotid webs are rare, studies indicate that they pose a significant risk of recurrent strokes in the absence of the typically recognized risk factors such as hypertension, diabetes, and heart disease.9,10 As such, employing the appropriate imaging tools is key to detecting the intimal defect. CTA has proven to be particularly useful for diagnosis.
In a single-institution CTA database, Choi et al a found a carotid web estimated prevalence of 1.2% in the prospective arm and an estimated prevalence of 2.4% in the retrospective cohort.1 However, the ICA lesions in the retrospective arm were not categorized as carotid webs because they could not be identified on the axial view. Notably, >20% of the patients in the retrospective cohort still presented with acute stroke in the area of these small lesions. Compared to CTA, magnetic resonance imaging (MRI) may emerge as a reliable tool to diagnose and characterize carotid webs in more detail, detecting smaller lesions as well as evaluating wall composition, biomechanics, and flow dynamics over time.14
Carotid bulb lesions were evaluated in a study of Afro-Caribbean stroke patients for a 5-year period.6 In this study, 25 patients were identified by CTA as having atypical FMD of the carotid bulb (CaFMD). The radiologic, morphologic, and histopathologic features observed in 7 patients described in the study are compatible with those of carotid webs. The study suggests that CaFMD could be a common pathologic condition in young patients of African descent, namely Afro-Caribbean persons. Of the 25 patients, 7 underwent surgical resection without new neurologic deficits after a 14-month median postoperative follow-up.
Haussen et al identified 24 patients with carotid webs, >90% of whom presented with stroke symptoms. The median age of the cohort was 46 years, >60% were females, and 75% were black.13 Of the 24 patients, 16 were treated by carotid stenting and had no recurrences. The other patients received medical therapy with thrombolysis and antiplatelet therapy only, and 7 of the nonstented patients experienced a recurrence of stroke symptoms. In a 2018 case series of 4 patients, all were diagnosed with carotid webs and treated with stent placement.12 Patients were also given dual antiplatelet agents (ticagrelor and aspirin) prior to the intervention. Three of these patients experienced postprocedure bradycardia, but only one had to be given atropine. Otherwise, no perioperative complications occurred.
Whereas carotid webs have been directly associated with intimal fibrodysplasia, the histopathology of FMD shows dysplasia of the medial layer.3 FMD is typically found incidentally; it is often asymptomatic and can be concurrently detected in the renal arteries in many cases.3,15 Treatment options for FMD include antiplatelet therapy for asymptomatic patients and gradual endoluminal dilation or angioplasty in conjunction with antiplatelet therapy for symptomatic patients. While carotid webs are typically found in the carotid bulb, FMD can commonly be appreciated in the middle and distal extracervical carotid artery.13 Phair et al helped to distinguish carotid webs from FMD when they reported a patient presenting with an M1 occlusion whose CTA and MRI initially showed a filling defect at the right carotid artery bifurcation without a readily identifiable web.16 Upon treatment with endarterectomy, a carotid web was seen, and histopathology showed smooth muscle with extensive myxoid degenerative changes, as opposed to the medial fibroplasia and loose collagen seen in FMD.14
Although no studies compare endarterectomy vs stenting for treatment of a carotid web, we can extrapolate the data from carotid stenosis in which minimal risk is associated with carotid stenting using new stent technologies,17,18 especially if performed after the first week from symptom presentation.19
CONCLUSION
Carotid webs are often the cause of recurrent strokes, especially in African Americans without major stroke risk factors or history of trauma. Although carotid webs have been conventionally treated by endarterectomy, data support the use of stents as a successful treatment option. We add to the current body of literature on this pathology and report a case of a stented carotid web with a favorable clinical outcome.
ACKNOWLEDGMENTS
A portion of this work was presented in October 2017 at the annual meeting for the Congress of Neurological Surgeons in Boston, MA, as well as in January 2018 at the Louisiana Neurosurgical Society in Shreveport, LA, as an abstract presentation.
The authors have no financial or proprietary interest in the subject matter of this article.
This article meets the Accreditation Council for Graduate Medical Education and the American Board of Medical Specialties Maintenance of Certification competencies for Patient Care and Medical Knowledge.
REFERENCES
- 1.Choi PM, Singh D, Trivedi A, et al. Carotid webs and recurrent ischemic strokes in the era of CT angiography. AJNR Am J Neuroradiol. 2015. November;36(11): 2134-2139. doi: 10.3174/ajnr.A4431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Martinez-Perez R, Lownie SP, Pandey SK, Boulton MR. Stent placement for carotid web. World Neurosurg. 2017. February;98:879.e9-879.e11. doi: 10.1016/j.wneu.2016.11.050. [DOI] [PubMed] [Google Scholar]
- 3.Stahlfeld KR, Means JR, Didomenico P. Carotid artery fibromuscular dysplasia. Am J Surg. 2007. January;193(1):71-72. [DOI] [PubMed] [Google Scholar]
- 4.Compagne KCJ, van Es ACGM, Berkhemer OA, et al; MR CLEAN Trial Investigators. Prevalence of carotid web in patients with acute intracranial stroke due to intracranial large vessel occlusion. Radiology. 2018. March;286(3):1000-1007. doi: 10.1148/radiol.2017170094. [DOI] [PubMed] [Google Scholar]
- 5.Sajedi PI, Gonzalez JN, Cronin CA, et al. Carotid bulb webs as a cause of “cryptogenic” ischemic stroke. AJNR Am J Neuroradiol. 2017. July;38(7):1399-1404. doi: 10.3174/ajnr.A5208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Joux J, Chausson N, Jeannin S, et al. Carotid-bulb atypical fibromuscular dysplasia in young Afro-Caribbean patients with stroke. Stroke. 2014. December;45(12):3711-3713. doi: 10.1161/STROKEAHA.114.007313. [DOI] [PubMed] [Google Scholar]
- 7.Joux J, Boulanger M, Jeannin S, et al. Association between carotid bulb diaphragm and ischemic stroke in young Afro-Caribbean patients: a population-based case-control study. Stroke. 2016. October;47(10):2641-2644. doi: 10.1161/STROKEAHA.116.013918. [DOI] [PubMed] [Google Scholar]
- 8.Coutinho JM, Derkatch S, Potvin AR, et al. Carotid artery web and ischemic stroke: a case-control study. Neurology. 2017. January;88(1):65-69. doi: 10.1212/WNL.0000000000003464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Fu W, Crockett A, Low G, Patel V. Internal carotid artery web: Doppler ultrasound with CT angiography correlation. J Radiol Case Rep. 2015. May 31;9(5):1-6. doi: 10.3941/jrcr.v9i5.2434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Morgenlander JC, Goldstein LB. Recurrent transient ischemic attacks and stroke in association with an internal carotid artery web. Stroke. 1991. January;22(1):94-98. [DOI] [PubMed] [Google Scholar]
- 11.Elmokadem AH, Ansari SA, Sangha R, Prabhakaran S, Shaibani A, Hurley MC. Neurointerventional management of carotid webs with recurrent and acute cerebral ischemic syndromes. Interv Neuroradiol. 2016. August;22(4):432-437. doi: 10.1177/1591019916633245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Brinjikji W, Agid R, Pereira VM. Carotid stenting for treatment of symptomatic carotid webs: a single-center case series. Interv Neurol. 2018. April;7(5):233-240. doi: 10.1159/000486537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Haussen DC, Grossberg JA, Bouslama M, et al. Carotid web (intimal fibromuscular dysplasia) has high stroke recurrence risk and is amenable to stenting. Stroke. 2017. November;48(11):3134-3137. doi: 10.1161/STROKEAHA.117.019020. [DOI] [PubMed] [Google Scholar]
- 14.Boesen ME, Eswaradass PV, Singh D, et al. MR imaging of carotid webs. Neuroradiology. 2017. April;59(4):361-365. doi: 10.1007/s00234-017-1797-z. [DOI] [PubMed] [Google Scholar]
- 15.Narula N, Kadian-Dodov D, Olin JW. Fibromuscular dysplasia: contemporary concepts and future directions. Prog Cardiovasc Dis. 2018. Mar-Apr;60(6):580-585. doi: 10.1016/j.pcad.2018.03.001. [DOI] [PubMed] [Google Scholar]
- 16.Phair J, Trestman EB, Yean C, Lipsitz E. Endarterectomy for a symptomatic carotid web. Vascular. 2017. October;25(5):553-556. doi: 10.1177/1708538116684940. [DOI] [PubMed] [Google Scholar]
- 17.Brott TG, Hobson RW 2nd, Howard G, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med. 2010. Jul 1;363(1):11-23. doi: 10.1056/NEJMoa0912321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mas JL, Chatellier G, Beyssen B, et al; EVA-3S Investigators. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med. 2006. Oct 19;355(16):1660-1671. [DOI] [PubMed] [Google Scholar]
- 19.Rantner B, Goebel G, Bonati LH, Ringleb PA, Mas JL, Fraedrich G; Carotid Stenting Trialists' Collaboration. The risk of carotid artery stenting compared with carotid endarterectomy is greatest in patients treated within 7 days of symptoms. J Vasc Surg. 2013. March;57(3):619-626.e2; discussion 625-626. doi: 10.1016/j.jvs.2012.08.107. [DOI] [PubMed] [Google Scholar]