

Abstract
BACKGROUND:
Hepatitis B infection is a universal health problem. Worldwide, 5% of health-care-related injections continued unsafe. Dentist considers being at high-risk group for cross infection. Therefore, their knowledge and practice towards Hepatitis B virus (HBV) positive patients should be at an optimal level.
AIM:
The current study is aimed to evaluate and comparison of the knowledge, attitude and practice of Saudi dental students and interns towards HBV infection.
METHODS:
A self-explanatory questionnaire comprising of 16 questions was designed to assess and compare students’ knowledge, attitude and risk perception regarding hepatitis B infection among dental students across Saudi Arabia.
RESULTS:
The response rate was 91.6% the overall knowledge of the participants was poor. The attitude was fair, with the female show a significant difference in attitude and practice (P-value < 0.05). The overall practice was good, 78.1% was vaccinated against HBV, and 73.2% stated that they regularly use personal protection equipment. The higher levels show a good attitude and practice compared with the lower levels; the difference was significant (P value < 0.05).
CONCLUSION:
The overall knowledge was below average, continuous health education courses are mandatory.
Keywords: Hepatitis B infection, Dental students, Dental interns, Survey, Cross infection, Prevention
Introduction
Hepatitis B infection is a universal health problem, caused by the hepatitis B virus (HBV), which is a DNA virus. The infection usually begins as subclinical or asymptomatic, except for some cases where acute symptoms are seen. Although it’s a vaccine-preventable, can cause chronic infection and increase the risk of death from cirrhosis and liver cancer. Hepatitis B infection is endemic in tropical, under-developed and developing countries. Statistical data revealed that around two billion people around the world had been infected with HBV, and around 350 million people are known to be a chronic carrier for the virus. The case fatality rate is approximately one per cent [1]. According to WHO, the highest prevalence is in the Western Pacific region and the African region (6.2% and 6.1% respectively). Whereas, the WHO region of America is the least infected with a prevalence of 0.7% [2]. Saudi Ministry of Health (MOH) Statistical data have revealed that viral hepatitis is considered as second most common viral infection after chickenpox, with a high incidence rate of 19.8 per 100 thousand individuals [3]. In Saudi Arabia, the prevalence of HBV among blood donor found to be between 1.5% and 2.6% within the adult population [4].
The peak incidence of the HBV infection found to be in young adults, and most HBV infections are acquired through unprotected sex or needles sharing used by drug abusers [5]. Because of the highly sensitive virologic screening of donor blood, the risk of acquiring HBV infection from a blood transfusion is one in 2,300,000 [6]. Worldwide, 5% of health-care-related injections continued to be unsafe [7]. This carries the risk of cross-infection in health care facilities. HBsAg is considered as a diagnostic marker for the primary infection because it is the first serological marker to appear in serum. Serological markers like anti-HBc, HBeAg and anti-HBe are used to evaluate the different state of the disease. Presence of Antibody to HBsAg (anti-HBsAg) in the serum is suggestive of withdrawal of HBsAg.
Transmission of infectious disease can occur easily in dental clinics [8]. Infections can be transmitted in the dental clinic through infected needles, direct blood contact, oral saliva, and indirect contact with contaminated instruments, operatory equipment, or environmental surfaces [9]. This can be prevented by the standard precaution that has been adopted by the U.S. Centers for Disease Control and Prevention (CDC) in 1996. This precaution should be applied by the dentist and dental team to overcome the risk of cross infection. Wearing of gloves by a dentist and dental assistant has been recommended as an essential component of cross-infection control [10], [11]. Hands are a major source of infection [11], and potentially infected blood may be retained beneath the fingernails for up to five days [12] unless there is meticulous mechanical cleansing. Serological studies in diverse parts of the world have found a higher prevalence of HBV infection with a higher possibility for transmission, among dentists, compared to the general population [13], [14].
Dental knowledge and attitude are the cornerstones in the prevention of diseases transmission. Several studies have been done to assess the level of students and dental practitioners. Keeping this in mind, the objective of this study was to evaluate the knowledge, attitude and practice behaviour of dental students and interns regarding infection control in central and Sothern Western areas in Kingdom of Saudi Arabia.
Material and Methods
The present cross-sectional survey was conducted from 15 June 2017 to 26 December 2017. A total of 789 dental students were randomly selected from the various dental cross across Saudi Arabia. A self-explanatory questionnaire comprising of 16 questions was designed to assess and compare students’ knowledge, attitude and risk perception regarding hepatitis B infection among dental students across Saudi Arabia. The questionnaire was prepared in English language considering the language in which courses are taught to the student. English of the questionnaire was checked by the language expert. Face validity and content validity was assessed and evaluated by the expert in the field of research.
The questionnaire was comprised of four main domains: 1) Demography, course year of the participants, 2) Knowledge, 3) Attitude and 4) Practice of the participants towards hepatitis B infection. A pilot test was performed on 20 participants to evaluate the efficacy of the questionnaire. Only Saudi national students were selected for the survey any other nationalities were excluded.
The sample size was calculated depending on the following formula:
Where:
Z = Z value (1.96 for 95% confidence level)
p = percentage of picking a choice expressed as a decimal (0.5)
This was found to be 50% for the present study which was expressed as 0.50.
e = confidence interval, expressed as decimal (0.05)
n = total population of the region
By using the above formula, the minimum sample size was calculated to be 403.
Ethical clearance was obtained from the Institutional Ethics Committee (IEC), after a comprehensive review of the proposal. The importance of the study was explained verbally to the participants and written informed consent was obtained before the commencement of the study. Every attempt was made to maintain the confidentiality of the participants. The questionnaire was distributed among the participants during their Lecture and clinical hours; meanwhile, the research coordinates were around to answer any queries related to the questionnaire.
All the hypotheses were formulated using two-tailed alternatives against each null hypothesis (hypothesis of no difference). The entire data is statistically analysed using the Statistical Package for Social Sciences (SPSS version 21.0, IBM Corporation, USA) for MS Windows. Chi-square test was executed to compare the descriptive data. P values < 0.05 were taken as statistically significant.
Results
Out of total 789, 723 participants completed the questionnaire with a response rate of 91.63%. Among participants; 400 (55.3%) were female, and 323 (44.7%) were male. Out of the total; 19.8% (143) were interned, and 80.2% (580) was an undergraduate student. Among undergraduates; 20.6% (149), 30.6% (221), 29% (210) belonged to 4th, 5th and 6th year respectively. The age was range between (18-26) years with a mean age of 21.6 ± 4.7 years (Table 1).
Table 1.
Demographic characteristic
| Variables | Number (n) | Frequency (%) |
|---|---|---|
| Gender | ||
| Male | 323 | (44.7%). |
| Female | 400 | (55.3%) |
| Age | ||
| 18-22 | 346 | (48%) |
| 23-26 | 377 | (52%) |
| Year of Study | ||
| 4th year | 149 | (20.6%) |
| 5th year | 221 | (30.6%) |
| 6th year | 210 | (29.0%) |
| Intern | 143 | (19.8%) |
| Total | 723 | (100%) |
Considering the knowledge score only 55 (7.6%) participant have a good level of knowledge, and about two-thirds have below the average of knowledge 64.7% (Figure 1). Regarding the knowledge, although about half of students and interns (53.8%) know that the chance for HBV transmission is more than that of HIV, while only 28.2% know the duration of HBV incubation period and only 13.6% know that most of the patients have no prominent symptoms. On the other hand, only about one-fifth of the participant was aware of how the virus is spread.
Figure 1.
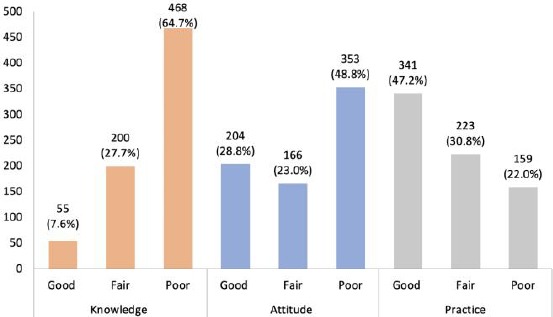
Overall distribution of Knowledge, Attitude, and Practice about HBV among total (n = 723) participants
Given the vaccination for HBV, two third of the participants (66.3%) know that a vaccine against HBV infection is available, but only half of them know the interval for the vaccination. On the other hand, about one third (29.9%) know that post-exposure vaccination is available. Regarding how to test for the HBV infection, 35.8% of them know that HBsAg is the confirmation test for active HBV infection.
Overall the participants presented a positive level of attitude towards HBV positive patients. Most of them consider that dentist have an ethical obligation to treat HBV patient, minority report that they don’t have this obligation (8.3%). About half of them consider that HBV patient should be treated in a separate clinic. While 52.1% of participants confirmed that they go for a periodic Abs test for HBV, 57% have a strong worry about getting infected while treating a patient. Despite that, two third (64%) of participants stated that they would be able to treat patients more confidentially if they are immunised.
Meanwhile, 67.8% gave a solid knowledge about universal precaution protocol; about 73.2% stated that they use personal protection equipment (gloves and facemask) during clinical work. About one-third of them confirm that they have the professional knowledge to safely work with HBV patient. The score shows 48.8% of the participant to have a below average of attitude. Only 28.2% show a good level of attitude towards HBV (Figure 1).
When considering practice only one fifth do not receive vaccination for HBV. Almost half of the participants show a high level of practice at 47.2%. About one fifth (22%) show a low level of practice (Figure 1).
In comparing the knowledge of female to male, the female participants revealed slightly better knowledge than male participants, 7.4% of male show a good level of knowledge in comparison with 7.8% of female participants. 69.3% and 61.0% of male and female respectively show below the average of knowledge. The difference was slightly significant (P value = 0.047) (Table 2). While considering the attitude and practice, there was a significant difference between male and female participants with a P value of less than 0.001 for attitude and 0.012 for practice (Table 2).
Table 2.
Knowledge, attitude, practice according to gender and year
| Variable | Group | Below Average | Average | Good | P value | |
|---|---|---|---|---|---|---|
| Knowledge | Gender | Female | 61.0% | 31.3% | 7.8% | 0.047** |
| Male | 69.3% | 23.2% | 7.4% | |||
| Year | 4th year | 62.9% | 29.0% | 8.1% | ||
| 5th year | 67.1% | 25.5% | 7.4% | 0.843* | ||
| 6th year | 63.8% | 30.0% | 6.2% | |||
| Intern | 64.7% | 27.7% | 7.6% | |||
| Attitude | Gender | Female | 42.0% | 26.3% | 31.8% | <0.001*** |
| Male | 57.3% | 18.9% | 23.8% | |||
| Year | 4th year | 51.4% | 22.4% | 26.2% | ||
| 5th year | 44.1% | 30.5% | 25.4% | <0.001*** | ||
| 6th year | 42.3% | 19.5% | 38.3% | |||
| Intern | 44.3% | 11.2% | 44.6% | |||
| Practice | Gender | Female | 18.8% | 29.5% | 51.7% | 0.012** |
| Male | 26.0% | 32.5% | 41.5% | |||
| Year | 4th year | 20.0% | 38.1% | 41.9% | 0.166* | |
| 5th year | 22.2% | 29.0% | 48.9% | |||
| 6th year | 23.8% | 30.1% | 46.2% | |||
| Intern | 22.8% | 24.2% | 53.0% | |||
No significant difference;
Significant;
Highly Significant.
When the comparison was made based on the year of study, the knowledge level was slightly better in the fourth-year students as compared to fifth and sixth-year students, with no statistic difference (P-value = 0.843). Knowledge for interns was comparable to lower level students. The attitude and practice of the student improved generally by achieving higher levels and the difference were significant for the attitude (P-value < 0.001) (Table 2).
Discussion
The result of this study reveals a higher number of female participants than male. The result also revealed that the knowledge of the dental student and the intern regarding HBV infection is generally below average. According to a study by Gayathri et al. [15] in India, and a study was done by Al-Shamiri et al., [16] in Saudi Arabia, the overall awareness of the student was fairly satisfying, which is consistent with our study results. There is a slight significant difference between the female and male in knowledge. Although one might expect that knowledge level will upgrade by year, but for this sample, the level of knowledge is higher for the lower levels compared with senior one. This could be because the junior levels study the general pathology and microbiology within their present courses. Interns showed better knowledge as compared to higher level students, but slightly lower when compared with lower level students. Improved knowledge with interns could be due to their preparation for higher studies and licensing examination.
Although most of the intern shows a low level of knowledge, they show the highest level of attitude and a good level of practice, which may indicate that they get familiar with cross-infection control measures to the level it is done routinely and that the infection control measurement is restricted. On the other hand, this brings to light the need for reinforcement of the knowledge through special courses or continuing education program. Overall, there is upgrading in the attitude score and the practice score, which may be explained by a firm regulation of infection control measurement by the infection control committees.
When considering the attitude of the students, higher level shows a good attitude comparing to low levels; the difference was significant (P value < 0.001). This might be explained by their less exposure to the clinical work compared with the higher levels. With their good level of attitude, the higher level shows the high level of good practice among the other group, although the difference was not significant. The female showed a better attitude than their male counterpart (P-value < 0.001). This was convenient with the result of the study done by Al-Shamiri et al., [16].
Since the dentist considers being at high risk to be infected by HBV [13], vaccination against HBV is an important line in the prevention of cross-infection, despite that about one-fifth of the participants do not receive HBV vaccination, this might be explained by the vaccination being a prerequisite for the clinic work. This was more than the result found by Al-Rabeah A, and Nagpal et al., which revealed that 63.5% and 64% were against hepatitis B virus respectively [17], [18]. According to the study done by Nagpal et al., [18] done at South Indian Dental College, about one third had knowledge about the post-exposure vaccination for HBV. The result of the present study coincides with the finding of above study.
A study by Vlaho Brailo, [19] found that the knowledge of the student increase by going farther in their dental studies, which is partially applicable for this study. He also stated that their knowledge was not consistent with their attitude towards treating and dealing with HBV, and HIV positive patients. This was the reverse of our study result, in which the students have a low level of knowledge and a good attitude towards the patients with HBV, which may indicate a restrict measure by the infection control committees in the dental clinics.
Jain et al., [20] in his survey among Mumbai intern found that most of the intern knows about the HBV transmission and vaccination, but few of them have knowledge about the possibility of post-exposure vaccination. His results were in the same line with this study result. Malhotra et al., [21] in his study stated that the students have suitable knowledge regarding hepatitis B, but still there was a gap in pushing their knowledge into practice. This contradicts the result from the present study; overall the students have an unsatisfactory level of knowledge with an acceptable level of attitude.
Finally, since the cross infection can be barred by infection control measurements, which is an important part of health professions, [22] most of the participants (73.2%) stated that they use personal protection equipment during clinical work. This result was less than that by Nagpal et al., [18] where 85.8% of the participants were aware of the preventive measurement about HBV.
In conclusion, this study showed that despite the low level of knowledge (the knowledge need to be improved), the attitude and practice was acceptable for the participants. This indicates that more obligatory courses regarding HBV infection, transmission and vaccination should be incorporated in the curriculum of the dental colleges. The obtain of HBV vaccination before clinical work and the boosting doses in the right intervals, besides reporting any sharp object stick should be closely monitored by infection control committees.
Footnotes
Funding: This research did not receive any financial support
Competing Interests: The authors have declared that no competing interests exist
References
- 1.Te HS, Jensen DM. Epidemiology of hepatitis B and C viruses:a global overview. Clinics in Liver Disease. 2010;14:2010. doi: 10.1016/j.cld.2009.11.009. https://doi.org/10.1016/j.cld.2009.11.009 PMid:20123436. [DOI] [PubMed] [Google Scholar]
- 2.World Health Organization. Global Hepatitis Report. 2017 [Google Scholar]
- 3.Saudi Ministry of Health. A Review of Health Situation. The annual health statistics book. 2009 [Google Scholar]
- 4.Abdo AA, Sanai FM, Al-Faleh FZ. Epidemiology of viral hepatitis in Saudi Arabia:are we off the hook? Saudi Journal of Gastroenterology. 2012;18:349–57. doi: 10.4103/1319-3767.103425. https://doi.org/10.4103/1319-3767.103425 PMid:23150019 PMCid:PMC3530988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Leggat PA, Kedjarune U, Smith DR. Occupational health problems in modern dentistry:a review. Industrial Health. 2007;45:611–21. doi: 10.2486/indhealth.45.611. https://doi.org/10.2486/indhealth.45.611 PMid:18057804. [DOI] [PubMed] [Google Scholar]
- 6.Garner JS and The Hospital Infection Control Practices Advisory Committee. Guideline for isolation precautions in hospitals. Infection Control and Hospital Epidemiology. 1996;17:53–80. doi: 10.1086/647190. https://doi.org/10.2307/30142367. [DOI] [PubMed] [Google Scholar]
- 7.Taiwo JO, Aderinokun GA. Assessing cross infection prevention measures at the dental clinic, University College Hospital, Ibadan. The African journal of medical sciences. 2002;31:213–7. Burke FT, Wilson NF, Bogge HJ. Glove wearing by dental surgery assistants. Dental Update. 1993; 20:385-7. [PubMed] [Google Scholar]
- 8.Verrusio AC, Neidle EA, Nash KD, Silverman S, Jr, Horowitz AM, Wagner KS. The dentist and infectious diseases:a national survey of attitudes and behavior. Journal of American Dental Association. 1989;118:684. doi: 10.14219/jada.archive.1989.0082. https://doi.org/10.14219/jada.archive.1989.0082. [DOI] [PubMed] [Google Scholar]
- 9.Rustage KJ, Rothwell PS, Brook IM. Evaluation of a dedicated dental procedure glove for clinical dentistry. British Dental Journal. 1987;103:193–5. doi: 10.1038/sj.bdj.4806240. https://doi.org/10.1038/sj.bdj.4806240. [DOI] [PubMed] [Google Scholar]
- 10.Crawford TJ. State of the art practical infection control in dentistry. Journal of American Dental Association. 1985;110:629–33. doi: 10.1016/s0002-8177(15)30014-3. https://doi.org/10.1016/S0002-8177(15)30014-3. [DOI] [PubMed] [Google Scholar]
- 11.Burke FJT, Wilson NHF, Bogge HFJ. Glove wearing by dental surgery assistants. Dent Update. 1993;20:385–7. [PubMed] [Google Scholar]
- 12.Allen AL, Organ RJ. Occult blood accumulation under the finger nails:a mechanism for the spread of bloodborne infection. Journal of American Dental Association. 1982;105:455–9. doi: 10.14219/jada.archive.1982.0347. https://doi.org/10.14219/jada.archive.1982.0347. [DOI] [PubMed] [Google Scholar]
- 13.Mahboobi N, Agha HF, Mahboobi N, Safari S, Lavanchy D, Alavian SM. Hepatitis B virus infection in dentistry:a forgotten topic. Journal of Viral Hepatitis. 2010;17:307. doi: 10.1111/j.1365-2893.2010.01284.x. https://doi.org/10.1111/j.1365-2893.2010.01284.x PMid:20196802. [DOI] [PubMed] [Google Scholar]
- 14.Martins AM, Barreto SM. Hepatitis B vaccination among dentists surgeons. Revista de Saúde Pública. 2003;37:333–8. doi: 10.1590/s0034-89102003000300011. https://doi.org/10.1590/S0034-89102003000300011 PMid:12792684. [DOI] [PubMed] [Google Scholar]
- 15.Gayathri MM. Knowledge, Awareness and Attitude among Dental Students about Hepatitis B Infection. Journal of Pharmaceutical Sciences and Research. 2016;8(3):168. [Google Scholar]
- 16.Al-Shamiri HM, Al-Shalawi FE, Al-Jumah TM, Al-Harthi MM, Al-Ali EM, Al-Harthi HM. Knowledge, Attitude and Practice of Hepatitis B Virus Infection among Dental Students and Interns in Saudi Arabia. Journal of Clinical and Experimental Dentistry. 2018;10:e54–60. doi: 10.4317/jced.54418. PMid:29670716 PMCid:PMC5899805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Al-Rabeah A, Mohamed AI. Infection control in the private dental sector in Riyadh. Annals of Saudi Medicine. 2002;22:1–2. doi: 10.5144/0256-4947.2002.13. https://doi.org/10.5144/0256-4947.2002.13. [DOI] [PubMed] [Google Scholar]
- 18.Nagpal B, Hegde U. Knowledge, attitude, and practices of hepatitis B infection among dental students. International Journal of Medical Science and Public Health. 2016;5:1123–7. https://doi.org/10.5455/ijmsph.2016.03102015170. [Google Scholar]
- 19.Vlaho B, Pelivan I, Škaricic J, Marko V, Nikša D, Gordana C. Treating Patients with HIV and Hepatitis B and C Infections:Croatian Dental Students'Knowledge, Attitudes, and Risk Perceptions. Journal of Dental Education. 2011;75:1115–21. [PubMed] [Google Scholar]
- 20.Jain R, Oswal KC, Chitguppi R, Dupare R, Puttaswamy B, Gaikwad R. Knowledge, Attitudes and Practices regarding Hepatitis B Infection among Dental Interns in Mumbai, Maharashtra Journal Article. International Journal of Preventive and Clinical Dental Research. 2014;1:51–7. [Google Scholar]
- 21.Malhotra V, Kaura S, Sharma H. Knowledge, attitude and practices about hepatitis B and Infection Control Measures among dental students in Patiala. Journal Dental Allied Science. 2017;6:65–9. https://doi.org/10.4103/2277-4696.219977. [Google Scholar]
- 22.McCarthy GM, MacDonald JK. A comparison of infection control practices of different groups of oral specialists and general dental practitioners. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontics. 1998;85:47–54. doi: 10.1016/s1079-2104(98)90397-3. https://doi.org/10.1016/S1079-2104(98)90397-3. [DOI] [PubMed] [Google Scholar]