

Abstract
BACKGROUND:
The prevalence of malocclusion varies from one region to another and among different age groups and ethnicities. According to the World Health Organization, malocclusion is the third most common abnormal dental condition.
AIM:
This study aims to establish the prevalence of malocclusion among schoolchildren in the Holy City of Makkah, Saudi Arabia.
METHODS:
A cross-sectional study was conducted among 400 Saudi schoolchildren, 12-15 years of age, of both genders, randomly selected from 15 schools in different regions of Makkah. Molar and canine relationships were examined, in addition to traits such as crowding, spacing, overjet, overbite, cross-bite, scissor bite, and maxillary diastema.
RESULTS:
The most prevalent molar relationship was Class I (52.3%), followed by Class II (25%), and Class III (20.5%). Crowding was the most prevalent malocclusion trait (74%), and scissor bite was the least common (2.5%). A statistically significant difference was found between males and females in most of the recorded criteria (P < 0.005).
CONCLUSION:
Among schoolchildren in Makkah, Class I molar relationship was the most prevalent type of occlusion, and the most prevalent malocclusion trait was crowding.
Keywords: Malocclusion, Holy City of Makkah, Schoolchildren
Introduction
Malocclusion occurs when the dental arches are misaligned, incorrectly related to each other, or when there is an irregularity in teeth position beyond the normal limits [1]. It is usually a developmental condition rather than a pathological one ]2[. There are many etiological factors associated with malocclusion, including an abnormal number of teeth, jaw size and form, habits such as nail biting or thumb sucking, and premature loss of or prolonged retention of deciduous teeth [3].
Dental caries and periodontal diseases may result from malocclusion [4], and due to an unpleasant dentofacial appearance, psychosocial problems may develop [5]. Malocclusion may also have unfavourable effects on oral functions, including mastication, swallowing, and speech [6]. Furthermore, if malocclusion remains untreated, it may increase the incidence of temporomandibular joint disorders [7].
Previous studies have shown that the prevalence of malocclusion varies widely among several populations around the world; these variations may be due to differences in age, ethnicity, or size of the studied populations [8].
A study in the northern border region of Saudi Arabia was conducted on 500 Saudi adolescents (male and female) showed a considerable prevalence of malocclusion [9]. Another study in the southern region of Saudi Arabia including only males but with a large cross-section of different ethnicities also showed a high prevalence of malocclusion, and the most common malocclusion trait was crowding [2]. In the central region, specifically in Riyadh, two studies have reported the predominance of Class I molar and canine relationships among Saudi children (12-16 years of age), and crowding was again the most common malocclusion trait [10], [11]. Another study was conducted in the eastern region of Saudi Arabia, on 330 female patients. They were categorised into an adolescent group (12-17 years) and an adult group (18-35 years). The study revealed that adolescents had more spacing problems and discrepancies involving overjet and overbite than did adults [12].
When reviewing the available literature for similar studies conducted in regions outside of Saudi Arabia, we found one study that showed 70% of adolescent Kuwaitis had moderate-to-severe malocclusion [13]. Another study in Turkey showed that only 3.5% of 1,507 patients had normal occlusion [14].
Because malocclusion can affect a patient’s function and appearance, it is better if it is identified and treated at early stages to avoid further complications [15] and to increase the probability of a favourable prognosis [16]. Unfortunately, few studies have examined the prevalence of malocclusion in the western region of Saudi Arabia [17], [18]. Further studies in the western region would form a complete database to aid in planning appropriate orthodontic treatment services among all regions of Saudi Arabia and help to assess the resources needed to overcome the increasing number of malocclusion cases.
Thus, this study aimed to assess the prevalence of malocclusion among schoolchildren in the Holy City of Makkah, which is in the western region of Saudi Arabia.
Methods
Subjects
The study was conducted in the Holy City of Makkah, Saudi Arabia, and included 400 Saudi schoolchildren (200 females and 200 males who were born and lived in Holy City of Makkah, Saudi Arabia) aged 12-15 years. The sample was selected from ten intermediate schools, which were randomly chosen from different regions of the city (two schools from each region): the east, west, north, south, and centre of the city. Students with missing teeth due to previous extraction, previous orthodontic treatment, maxillofacial surgeries, or syndromes were excluded from the study.
Ethics
Ethical approval was obtained from the institutional review board of Umm Al Qura University Faculty of Dentistry and written informed consent was provided by the participants’ parents before the examination and after explaining the purpose and style of the study.
Training, Calibration, and Standardization
To standardise examinations, dentists independently examined 10 patients at baseline and discussed outcomes. Following this initial review, the dentists attended a lecture given by an orthodontist on objective diagnostic criteria. Finally, 2 weeks after the baseline examination, the dentists were calibrated by independently examining another 10 patients and comparing the results (Kappa = 0.88).
Clinical examinations and data collection
Clinical examinations were carried out in each school by the examiners using a disposable mouth mirror, ruler (numbering started with zero), and light source. Severely decayed teeth, periodontally affected teeth should be mentioned; the following traits were recorded:
- The molar relationship between right and left sides recorded according to Angle’s Classification:
Class I: Mesiobuccal cusp of the maxillary first molar occludes with the mesiobuccal groove of the mandibular first molar in maximum intercuspation.
Class II: Mesiobuccal cusp of the maxillary first molar occludes mesial to the mesiobuccal groove of the mandibular first molar in maximum intercuspation.
Class III: Mesiobuccal cusp of the maxillary first molar occludes distal to the mesiobuccal groove of the mandibular first molar in maximum intercuspation [19].
- The canine relationship between right and left sides, according to Angle’s Classification:
Class I: Maxillary canine cusp tip occludes with the embrasure between the mandibular canine and first premolar.
Class II: Maxillary canine cusp tip occludes mesial to the embrasure between the mandibular canine and first premolar.
Class III: Maxillary canine cusp tip occludes distal to the embrasure between the mandibular canine and first premolar [19].
- Crowding/spacing: This is the malalignment of teeth. Crowding was measured as a negative value, while spacing was measured as a positive value.
- Overjet: This is the horizontal distance from the labial surface of the mandibular incisors to the labial surface of the maxillary incisors. It was considered positive when the upper incisors overlapped with the lower, zero when they were edge to edge, and negative when the lower incisors overlapped with the upper incisors [20]. If the overjet was between 2 and 5 mm, it was considered normal based on examiner clinical experience; greater than 5 mm was considered increased, and less than 2 mm was considered decreased.
- Overbite: This is the vertical measurement of anterior maxillary teeth covering the mandibular anterior teeth in the normal occlusal position of the jaws [20]. If the overbite was one third, it was recorded as normal and more than two-thirds were considered a deep bite. If an overbite is zero, it would be edge-to-edge; in the case of no contact between the maxillary and the mandibular anterior teeth, it would be considered an open bite.
- Anterior cross-bite: This is defined as a palatal positioning of the anterior maxillary teeth to the mandibular anterior teeth [21].
- Posterior cross-bite: This is a transversal relationship between the upper and lower jaws, where the upper buccal cusps occlude the fossa of the lower teeth [22].
- Scissor bite: A scissor bite occurs “if the lingual cusp of the upper tooth occludes buccally to the buccal cusp of the corresponding lower tooth” [23].
- Maxillary diastema: This is defined as space/gap between the maxillary central incisors, which is normally present in the primary and mixed dentition and closed after the complete proper eruption of permanent maxillary canines [24].
Statistical analyses
Primary outcomes included molar and canine relationships. Secondary measures included spacing or crowding, overbite, overjet, scissor bite, and maxillary midline diastema. We calculated descriptive statistics for the demographics and occlusion status for all participants. We reported means and standard deviations for continuous measures and numbers and percentages for categorical measures. Further, the Chi-square test (level of significance = 0.05) was used to compare any differences between male and female students about occlusion classification. Stata statistical software version 14 (StataCorp) was used to analyse the data.
Results
Four hundred Saudi intermediate schoolchildren met the selected criteria (200 males and 200 females); the average age was 13.5 ± 0.9 years.
The most prevalent molar relationship was Class I (52.3%), which was higher in females (P < 0.05), followed by Class II (25%), and Class III (20.5%). Of the study subjects, 2.3% had severely destructed first molars due to dental caries. Therefore, their Angel’s Classification could not be determined (NA) (Figures 1 and 2).
Figure 1.
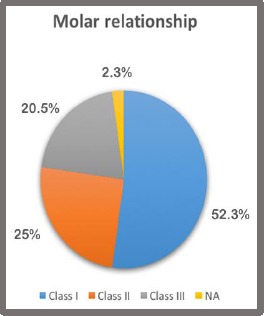
The Prevalence of Molar Relationship (NA = Not applicable: missing tooth)
Figure 2.
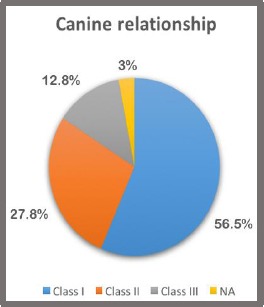
The Prevalence of Canine Relationship (NA = Not applicable: missing tooth)
The prevalence of canine relationship was 56.5%, 27.8%, and 12.8% for Classes I, II, and III, respectively, with a higher prevalence of Class I in females (P <.05) (Table 1).
Table 1.
Prevalence of Molar and Canine Relationships, by gender
| Gender | P-Value | ||||
|---|---|---|---|---|---|
| Male | Female | ||||
| No. | % | No. | % | ||
| Molar Relationship | |||||
| Class I | 81 | 40.5 | 128 | 64 | < 0.001 |
| Class II | 65 | 32.5 | 35 | 17.5 | |
| Class III | 48 | 24 | 34 | 17 | |
| NA (Not applicable: missing tooth) | 6 | 3 | 3 | 1.5 | |
| Canine Relationship | |||||
| Class I | 96 | 48 | 130 | 65 | 0.002 |
| Class II | 67 | 33.5 | 44 | 22 | |
| Class III | 31 | 15.5 | 20 | 10 | |
| NA (Not applicable: missing tooth) | 6 | 3 | 6 | 3 | |
Crowding was the most prevalent malocclusion trait among the study sample (74%), but it was observed in males more than in females (P < 0.05). The next most prevalent trait was two-third overbite (33.5%), which was relatively comparable between the genders.
Of all study subjects, 71.3% had a normal overjet measurement (2-5 mm); 22.3% had a cross-bite; spacing was recorded in 21.5% of them, all the three of the previously mentioned traits were more prevalent in females (P < 0.05).
Maxillary diastema was found in 22% of the cases. The least common trait was Scissor bite (2.5%), and only 3.8% of the subjects had a deep bite. The prevalence of open bite and the prevalence of an edge-to-edge incisal relationship were 3.3% and 4.5%, respectively. There was a statistically significant difference between males and females in all of the measured malocclusion traits (P < 0.05) except for overjet and maxillary midline diastema, both of which revealed no statistically significant difference (P > 0.05) (Table 2).
Table 2.
Prevalence of Different Malocclusion
| Gender | Total | P-Value | |||||
|---|---|---|---|---|---|---|---|
| Male | Female | ||||||
| No. | % | No. | % | No. | % | ||
| Is there spacing or crowding? | |||||||
| Normal | 1 | 0.5 | 17 | 8.5 | 18 | 4.5 | < 0.001 |
| Crowding | 161 | 80.5 | 135 | 67.5 | 296 | 74 | |
| Spacing | 38 | 19 | 48 | 24 | 86 | 21.5 | |
| Is there an overbite? | |||||||
| Normal | 105 | 52.5 | 115 | 57.5 | 220 | 55 | 0.021 |
| Two-Thirds | 74 | 37 | 60 | 30 | 134 | 33.5 | |
| Deep Bite | 3 | 1.5 | 12 | 6 | 15 | 3.8 | |
| Open Bite | 5 | 2.5 | 8 | 4 | 13 | 3.3 | |
| Edge to Edge | 13 | 6.5 | 5 | 2.5 | 18 | 4.5 | |
| Is there a cross-bite? | |||||||
| No | 165 | 82.5 | 146 | 73 | 311 | 77.8 | 0.022 |
| Yes | 35 | 17.5 | 54 | 27 | 89 | 22.3 | |
| Overjet Category | |||||||
| Normal 2-5 mm | 133 | 66.5 | 152 | 76 | 285 | 71.3 | 0.077 |
| Reduced <2 mm | 47 | 23.5 | 30 | 15 | 77 | 19.3 | |
| Increased >5 mm | 20 | 10 | 18 | 9 | 38 | 9.5 | |
| Is there a scissor bite? | |||||||
| No | 200 | 100 | 190 | 95 | 390 | 97.5 | 0.001 |
| Yes | 0 | 0 | 10 | 5 | 10 | 2.5 | |
| Is there a maxillary midline diastema? | |||||||
| No | 151 | 75.5 | 161 | 80.5 | 312 | 78 | 0.227 |
| Yes | 49 | 24.5 | 39 | 19.5 | 88 | 22 | |
*P-values for comparing male vs female using chi-square test.
Discussion
The goal of this study was to determine the prevalence of malocclusion among school-aged children in the Holy City of Makkah. Four-hundred Saudi schoolchildren were examined, and their occlusion status was recorded. Their ages ranged from 12 to 15 years; this is the preferred age range for orthodontic intervention if malocclusion is found because it is the stage of late-mixed or early-permanent dentition. The subjects were randomly selected from five regions to represent Makkah’s population: the north, south, east, west, and centre of the city.
Several studies have been published regarding the prevalence of malocclusion in different populations. However, due to the wide variation in ethnicities and endogenous traits, diverse methods, and differences in sample size, it is difficult to compare the findings.
The present study revealed that the Class I molar relationship was the most prevalent type of occlusion (52.3%), followed by Class II (25%), and Class III (20.5%), which is in agreement with findings by Meer et al., in the southern region of Saudi Arabia [2]; both reported a high prevalence of crowding and a lower prevalence of spacing. The high prevalence of molar Class I, followed by Class II, and Class III found in the present study is similar to that found in studies conducted in Kuwait, Turkey, Jordan, and the northern border region of Saudi Arabia [8], [9], [13], [14]. However, in Riyadh, Asiry reported that Class I was the most prevalent, followed by Class III, then Class II; the same molar-relationship sequence was found in Dammam [10], [12]. The Class I canine relationship was more frequently observed in this study (56.5%) than Class II (27.8%) and Class III (12.8%). Dissimilar findings were reported in Kuwait by Behbehani, who found that the Class II canine relationship was more common than other types [13].
Crowding was the most prevalent malocclusion trait in the current study; it was recorded in 74% of the examined subjects, while in the northern border region of Saudi Arabia, Riyadh, and Aseer, it was much less prevalent (47.2%, 45.4%, and 43.8%, respectively) [2], [9], [10]. However, in Dammam City, crowding was evaluated for both arches: a prevalence of 73.4% was found for the maxillary arch and 67.8% for the mandibular arch [12]. Spacing problems were found in 21.5% of subjects in the present study; this finding is comparable to the findings in Riyadh (20.4%), Asser (16.7%), the northern border region of Saudi Arabia (27.2%), Turkey (12.5%), Jordan (26.7%), and Colombia (25.9%) [2], [8], [9], [11], [14], [15].
We found that 55% of the study subjects had a normal overbite, which is comparable to the findings in the northern border region of Saudi Arabia (64.4%) and Turkey (53.5%) [9], [14]. A deep bite was found in 3.8%, which is higher than the 1.7% found in Kuwait [13] and less than the 8.8% found in Riyadh [11]. An open bite was found in 3.3%, which is comparable to the northern border region of Saudi Arabia (4.6%) and less than that in Colombia (9%) [9], [24]. The prevalence of edge-to-edge was 4.5%, which is less than that observed in Turkey (12.1%) [14].
We found that 71.3% had a normal overjet (2-5 mm), which is comparable to the findings in Riyadh (75.4%). A reduced overjet (< 2 mm) was found in 19.3%, which is more than that found in the northern border region of Saudi Arabia (11.4%). An increased overjet (> 5 mm) was found in 9.5%, which is low in comparison to the findings in Jordan (24.7%) and Turkey (41.7%) [8], [9], [11], [14].
The prevalence of cross-bite was 22.3%, which is slightly high if compared to the findings in Asser (12.6%), Riyadh (17.3%), and the northern border region of Saudi Arabia (14.2%) [2], [9], [10]. Scissor bite was less prevalent than cross-bite, as its percentage was 2.5% in the present study. However, in Riyadh, there were no incidences of Scissor bite (0%) [10].
In this study, maxillary midline diastema was found in 22% of the study subjects, which is higher than that found in Jordan (6.9%), Turkey (4.5%), and Colombia (7%) [8], [14], [25]. A statistically significant difference (P < 0.005) was found between genders in this study among most of the malocclusion traits, which is in agreement with Celikoglu et al., who reported statistically significant differences between males and females with regard to the prevalence of crowding, cross-bite, overjet, and overbite categories [14]. However, Asiry reported different results in Riyadh, as there was no statistically significant difference between the genders among any of the malocclusion traits [10]. The disagreement in these findings could be due to differences in sample size, gender distribution, or registration method, or it could be due to different features of Makkah’s population about other regions of Saudi Arabia or other countries.
Further studies are needed in different regions of Saudi Arabia to determine the cause of malocclusion. Studies should examine larger sample sizes and employ additional examination methods such as radiographs and study casts.
In conclusion, this cross-sectional study showed the most prevalent type of occlusion among the Holy City of Makkah to be the Class I molar relationship and revealed normal overjet findings in the majority of cases. Crowding was the most prevalent malocclusion trait, followed by a two-third overbite. A significant difference was detected between males and females in the prevalence of all parameters except for overjet and maxillary midline diastema. These descriptive findings will aid us in understanding the overall picture of malocclusion in these regions and in providing a database that includes the occlusion status among the Saudi population to facilitate the development of appropriate preventive and therapeutic programs. Additionally, they will further increase society’s awareness of malocclusion, its aetiology, complications, and when it is necessary to see an orthodontist. However, this research has some limitations, as it was a cross-sectional study that used only basic examination instruments. Thus, further causality studies that include a larger population and utilise additional examination methods are recommended.
Acknowledgements
First, we thank Allah for giving us the ability to accomplish this work. We want to thank our college, the Faculty of Dentistry at Umm Al Qura University in Makkah, Saudi Arabia, for facilitating and funding this research project. We also thank Dr Hind Hassa Abdulatif, the assistant vice dean for research and graduate studies, for her kind support and guidance, and Jumana Felemban, who helped us with data collection. Finally, we would like to thank Editage (www.editage.com) for English language editing.
Footnotes
Funding: This research did not receive any financial support
Competing Interests: The authors have declared that no competing interests exist
References
- 1.Walther DP, Houston WJB, Jones ML, Oliver RG. Walther and Houston's orthodontic notes. 5th ed. Oxford: Wright; 1994. PMCid:PMC43175. [Google Scholar]
- 2.Meer Z, Sadatullah S, Wahab MA, Mustafa AB, Odusanya SA, Razak PA. Prevalence of malocclusion and its common traits in Saudi males of Aseer region. J Dent Res Rev. 2016;3:99–102. https://doi.org/10.4103/2348-2915.194834. [Google Scholar]
- 3.Dale G. Guidance of occlusion:Serial extraction. In: Graber YM, Swain BF, editors. Orthodontic Current Principles and Technique. St. Louis: CV Mosby Company; 1985. pp. 284–95. PMid:3971422. [Google Scholar]
- 4.Greiger A. Malocclusion as an etiologic factor in periodontal disease:A retrospective essay. Am J Orthod Dentofacial Orthop. 2001;120:112–15. doi: 10.1067/mod.2001.114537. https://doi.org/10.1067/mod.2001.114537 PMid:11500651. [DOI] [PubMed] [Google Scholar]
- 5.Kenealy P, Frude N, Shaw W. An evaluation of the psychological and social effects of malocclusion:Some implications for dental policy making. Social Science &Medicine. 1989;28:583–91. doi: 10.1016/0277-9536(89)90253-0. https://doi.org/10.1016/0277-9536(89)90253-0. [DOI] [PubMed] [Google Scholar]
- 6.Proffit WR, Fields HW., 3rd . Contemporary orthodontics. 3rd ed. St. Louis: CV Mosby; 2000. pp. 185–95. [Google Scholar]
- 7.Housten WJ. Walther's Orthodontic Notes. 4th ed. Oregon: The Stonebridge Publishers; 2000. [Google Scholar]
- 8.Abu Alhaija ES, Al-Khateeb SN, Al-Nimri KS. Prevalence of malocclusion in 13-15 year-old North Jordanian school children. Community Dent Health. 2005;22(4):266–71. PMid:16379166. [PubMed] [Google Scholar]
- 9.Gudipaneni RK, Aldahmeshi RF, Patil SR, Alam MK. The prevalence of malocclusion and the need for orthodontic treatment among adolescents in the northern border region of Saudi Arabia:An epidemiological study. BMC Oral Health. 2018;18:16. doi: 10.1186/s12903-018-0476-8. https://doi.org/10.1186/s12903-018-0476-8 PMid:29390986 PMCid:PMC5796577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Asiry MA. Occlusal status among 12-16 year-old school children in Riyadh, Saudi Arabia. J Int Oral Health. 2015;7(5):20. PMid:26028897 PMCid:PMC4441230. [PMC free article] [PubMed] [Google Scholar]
- 11.Albakri FM, Ingle N, Assery MK. Prevalence of malocclusion among male school children in Riyadh City. Open Access Maced J Med Sci. 2018;6(7):1296. doi: 10.3889/oamjms.2018.207. https://doi.org/10.3889/oamjms.2018.207 PMid:30087740 PMCid:PMC6062270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Albarakati SF, Taher S. Malocclusion traits in Saudi females seeking orthodontic treatment. Pak Oral Dent J. 2010;30:127–132. [Google Scholar]
- 13.Behbehani F, Artun J, Al-Jame B, Kerosuo H. Prevalence and severity of malocclusion in adolescent Kuwaitis. Med Princ Pract. 2005;14:390–5. doi: 10.1159/000088111. https://doi.org/10.1159/000088111 PMid:16220011. [DOI] [PubMed] [Google Scholar]
- 14.Celikoglu M, Akpinar S, Yavuz I. The pattern of malocclusion in a sample of orthodontic patients from Turkey. Med Oral Patol Oral Cir Bucal. 2010;15:e791–6. doi: 10.4317/medoral.15.e791. https://doi.org/10.4317/medoral.15:e791 PMid:20383112. [DOI] [PubMed] [Google Scholar]
- 15.American Dental Association:Adopted 1995, Revised 1997. (n.d.) Retrieved from https://www.ada.org/en/member-center/member-benefits/practice-resources/dental-practice-parameters/malocclusion .
- 16.Baeshen H. The Prevalence of Major Types of Occlusal Anomalies among Saudi Middle School Students. The journal of contemporary dental practice. 2017;18(2):142–146. doi: 10.5005/jp-journals-10024-2005. https://doi.org/10.5005/jp-journals-10024-2005 PMid:28174368. [DOI] [PubMed] [Google Scholar]
- 17.Al-Hummayani FM, Taibah SM. Orthodontic treatment needs in Saudi young adults and manpower requirements. Saudi medical journal. 2018;39(8):822. doi: 10.15537/smj.2018.8.22337. https://doi.org/10.15537/smj.2018.8.22337 PMid:30106421 PMCid:PMC6194985. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Adib K, Joseph BS, Nayla BN. Orthodontic patients:An epidemiologic and analytic study, an observational retrospective study. International Arab Journal of Dentistry. 2010;1:36–43. [Google Scholar]
- 19.Angle EH. Classification of malocclusion. Dental Cosmos. 1899;41:248–64. [Google Scholar]
- 20.Bishara SE. Textbook of orthodontics. 1st ed. Philadelphia: Saunders; 2001. [Google Scholar]
- 21.Tsai HH. Components of anterior crossbite in the primary dentition. J Dent Child. 2001;68(1):27–32. PMid:11324403. [PubMed] [Google Scholar]
- 22.Filho OGS, Montes LAP, Torelly LF. Rapid maxillary expansion in the deciduous and mixed dentition evaluated through posteroanterior cephalometric analysis. Am J Orthod Dentofacial Orthop. 1995;107(3):268–75. doi: 10.1016/s0889-5406(95)70142-7. https://doi.org/10.1016/S0889-5406(95)70142-7. [DOI] [PubMed] [Google Scholar]
- 23.Björk A, Krebs A, Solow B. A method for epidemiological registration of malocclusion. Acta Odontol Scand. 1964;22:28–40. doi: 10.3109/00016356408993963. https://doi.org/10.3109/00016356408993963. [DOI] [PubMed] [Google Scholar]
- 24.Baum AT. The midline diastema. J Oral Med. 1966;21:30–9. PMid:4951230. [PubMed] [Google Scholar]
- 25.Thilander B, Pena L, Infante C, Parada SS, de Mayorga C. Prevalence of malocclusion and orthodontic treatment need in children and adolescents in Bogota, Colombia. An epidemiological study related to different stages of dental development. Eur J Orthodont. 2001;23(2):153–68. doi: 10.1093/ejo/23.2.153. https://doi.org/10.1093/ejo/23.2.153 PMid:11398553. [DOI] [PubMed] [Google Scholar]