

Watch a video presentation of this article
Watch the interview with the author
Abbreviations.
- AFP
alpha‐fetoprotein
- ALT
alanine aminotransferase
- HBeAg
hepatitis B e antigen
- HBV
hepatitis B virus
- HCC
hepatocellular carcinoma
- TDF
tenofovir disoproxil fumarate
- ULN
upper limit of normal
Worldwide, most individuals with chronic hepatitis B virus (HBV) acquire their infections around the time of birth or during early childhood. In countries where HBV is endemic, perinatal transmission remains the most important cause of chronic infection because of high rates of infection in pregnant women. However, perinatal transmission also occurs in nonendemic countries, including the United States, mostly in children who have HBV‐infected mothers but do not receive appropriate HBV immunoprophylaxis at birth. Pediatric subjects who should be tested for hepatitis B are shown in Table 1.1
Table 1.
Pediatric Subjects Who Should Be Tested for HBV
| • Adolescents who engage in high‐risk behaviors, including those who use intravenous or intranasal drugs, those who have unprotected sex with an infected partner or more than one partner, men who have sex with men, and those with a history of sexually transmitted disease. |
| • All internationally adopted children. |
| • Immigrants from high‐prevalence areas (regions in which hepatitis B surface antigen prevalence is >2%), including all of Africa and Asia, the Cape Verde islands, most of Eastern and Mediterranean Europe, the Caribbean, and parts of South America. |
| • Children living in communities where HBV is endemic (including children born to immigrant parents from endemic areas). |
| • Household contacts of individuals with HBV infection. |
| • Infants born to women with HBV infection (HBeAg‐positive or ‐negative). Infants who received hepatitis B immunoglobulin and hepatitis B vaccine at birth, followed by two additional immunizations, should be tested for anti‐HBs and HBsAg at 9 to 18 months of age; this is important because about 5% of such infants develop chronic HBV infection even after optimal immunoprophylaxis. Those who have not been immunized should be tested as soon as identified. |
The natural history of chronic HBV infection in children is variable, depending upon age, mode of acquisition, and ethnicity. Children from endemic countries in whom HBV is acquired perinatally are usually hepatitis B e antigen (HBeAg)‐positive with high levels of viral replication.2 Rates of spontaneous seroconversion are <2% per year in children <3 years of age and 4% to 5% after age 3. The frequency of spontaneous HBeAg seroconversion increases during puberty. By contrast, children in nonendemic countries are less likely to have acquired the infection perinatally and frequently clear HBeAg and HBV DNA during the first two decades of life.3 Children tend to have higher alanine aminotransferase (ALT) levels early in life. The risk of hepatocellular carcinoma (HCC) is related to the duration of infection, the degree of histologic injury, and the replicative state of the virus (HBV DNA levels). The risk is higher in patients who are HBeAg‐positive for extended periods or have basal core promoter mutants, and this risk is increased further in the presence of cirrhosis. Hepatocellular carcinoma in children with HBV infection has been described in both Asian4 and Western5 populations. Importantly, HCC has been described in children who had undergone early HBeAg seroconversion, indicating that there is still a risk for HCC even after viral replication decreases.
Although inflammatory changes are often mild in liver biopsies from children with chronic hepatitis B, fibrosis may be significant. Nonetheless, cirrhosis is an infrequent complication of HBV infection during childhood. One of the largest studies included 292 consecutive children who were HBsAg‐positive and had elevated serum ALT levels.6 Cirrhosis was found in 10 patients (3%) at a mean age of 4.0 ± 3.3 years. No child developed cirrhosis during follow‐up (range, 1‐10 years).
Management of children with chronic HBV infection involves education, surveillance for HCC, and, in some cases, antiviral therapies. Figure 1 demonstrates the recommended management of children in the primary care setting. Some children with chronic HBV infection require treatment in order to prevent serious sequelae, such as cirrhosis and HCC, in young adult life. The approach to selection of children for treatment is outlined in Fig. 2.7 ALT levels less than 1.5 to 2 times the upper limit of normal generally indicate that the patient is in the immune‐tolerant phase of HBV infection. Such children are typically not candidates for treatment, because treatment with any of the currently available drugs does not result in higher rates of HBeAg seroconversion compared with no treatment. Children with ALT values more than 10 times the upper limit of normal may be in the process of spontaneous HBeAg seroconversion and should be observed for several months before treatment is begun.
Figure 1.
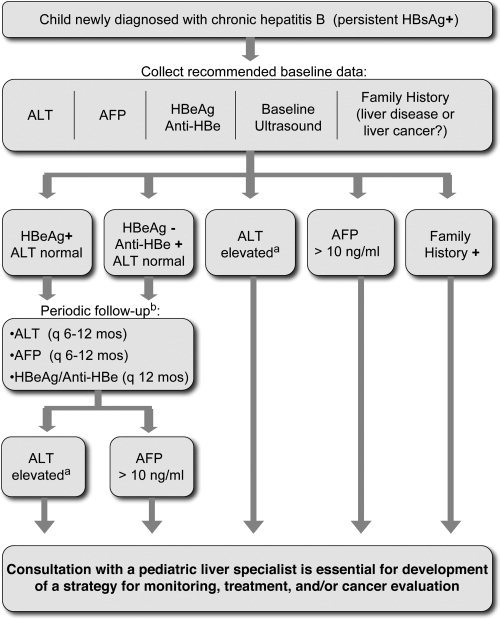
Recommended approach to monitoring children with chronic HBV infection. Abbreviations: AFP, alpha‐fetoprotein; HBsAg, hepatitis B surface antigen. Reprinted with permission from Pediatrics.1 Copyright 2009, American Academy of Pediatrics.
Figure 2.
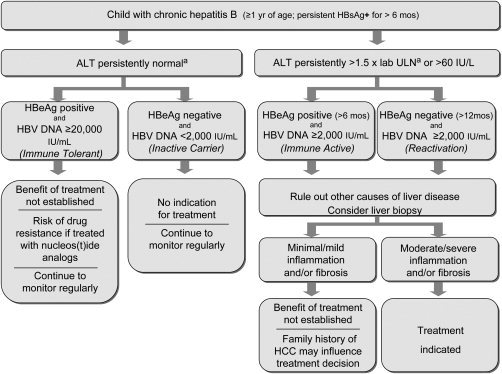
Algorithm for selection of children with chronic HBV infection for treatment. Abbreviations: HBsAg, hepatitis B surface antigen; ULN, upper limit of normal. Reprinted with permission from Hepatology.7 Copyright 2010, American Association for the Study of Liver Diseases.
There are few large trials in children to guide treatment decisions. Almost all children with chronic HBV are HBeAg‐positive, but therapy can also be considered for the few who are HBeAg‐negative, provided that viremia >2000 IU/mL is documented and other diseases are excluded. None of the available treatments is highly efficacious. Therefore, the choice of whether to treat depends on patient‐specific characteristics that predict the efficacy of treatment, including persistently abnormal ALT levels, and active disease on liver biopsy, as well as considerations regarding the likelihood of achieving appropriate therapeutic goals.
The likelihood of response to any of the currently available drugs depends highly upon the degree of elevation of the serum aminotransferases.8, 9, 10
Prolonged treatment with nucleoside or nucleotide analogs in children who are in the immune‐tolerant stage is associated with little benefit but imposes the important risk of viral resistance, both to the agent chosen and to similar drugs. An exception may be those immune‐tolerant children who will be undergoing immunosuppression, such as those who will have chemotherapy, or stem cell or solid organ transplantation. Prophylactic HBV suppression should be considered during these critical periods to avoid activation of hepatitis.
In the United States, only lamivudine and interferon‐α are licensed for use in young children, and adefovir dipivoxil is licensed for use in children >12 years of age. In August 2012, the use of tenofovir disoproxil fumarate (TDF), which had been licensed for treatment of human immunodeficiency virus in children, was expanded to include treatment of chronic hepatitis B in adolescents ≥12 years of age.11 Interferon, lamivudine, and adefovir dipivoxil are no longer first‐line therapy in adults, since much better agents are available, so they are less than ideal for children. Randomized phase III trials of entecavir, peginterferon‐alfa2a, and TDF in children with chronic HBV are underway. A summary of HBV drugs and their use in a pediatric population is given in Table 2.
Table 2.
HBV Drugs and Their Use in Pediatrics
| Drug | Age Indication | Pros | Cons | Comments |
|---|---|---|---|---|
| Lamivudine | ≥3 years | Rapidly lowers HBV DNA; well tolerated | High rate of viral resistance | May be used during chemotherapy or other short‐term immunosuppression |
| Interferon‐α | ≥1 year | Limited treatment time (24 weeks); no resistance or cross‐resistance | Side‐effect profile; thrice weekly injections | Replaced by peginterferon‐alfa2a in adult patients |
| Adefovir dipivoxil | ≥12 years | Intermediate resistance rate; well tolerated | Relative low antiviral efficacy; low risk of nephrotoxicity | Largely replaced by TDF in adult patients |
| Entecavir | ≥16 years | Rapidly lowers HBV DNA; low rate of resistance (especially in lamivudine naïve); well tolerated | Phase III trial in children 2‐16 years currently underway | |
| TDF | ≥12 years | Rapidly lowers HBV DNA; low rate of resistance; well tolerated | No difference in HBeAg seroconversion rate; low risk of nephrotoxicity; concern regarding effects on bone mineral density | Phase III trial in children 2‐12 years currently underway |
| Peginterferon‐alfa2a | Not approved for childhood HBV | Open‐label efficacy trial in children currently underway | ||
| Telbivudine | Not approved for childhood HBV | Efficacy trial in children being planned |
Potential conflict of interest: Nothing to report.
References
- 1. Haber BA, Block JM, Jonas MM, Karpen SJ, London WT, McMahon BJ, et al. Recommendations for screening, monitoring, and referral of pediatric chronic hepatitis B. Pediatrics 2009; 124: e1007–e1013. [DOI] [PubMed] [Google Scholar]
- 2. Lok ASF, Lai CL. A longitudinal follow‐up of asymptomatic hepatitis B surface antigen‐positive Chinese children. Hepatology 1988; 8: 1130–1133. [DOI] [PubMed] [Google Scholar]
- 3. Bortolotti F, Cadrobbi P, Crivellaro C, Guido M, Rugge M, Noventa F, et al. Long‐term outcome of chronic type B hepatitis in patients who acquire hepatitis B virus infection in childhood. Gastroenterology 1990; 99: 805–810. [DOI] [PubMed] [Google Scholar]
- 4. Wen W‐H, Chang M‐H, Hsu H‐Y, Ni Y‐H, Chen H‐L. The development of hepatocellular carcinoma among prospectively followed children with chronic hepatitis B virus infection. J Pediatr 2004; 144: 397–399. [DOI] [PubMed] [Google Scholar]
- 5. Pontisso P, Basso G, Perilongo G, Morsica G, Cecchetto G, Ruvoletto MG, et al. Does hepatitis B virus play a role in primary liver cancer in children of Western countries? Cancer Detect Prev 1991; 15: 363–368. [PubMed] [Google Scholar]
- 6. Bortolotti F, Calzia R, Cadrobbi P, Giacchini R, Ciravegna B, Armigliato M, et al. Liver cirrhosis associated with chronic hepatitis B virus infection in childhood. J Pediatr 1986; 108: 224–227. [DOI] [PubMed] [Google Scholar]
- 7. Jonas MM, Block JM, Haber BA, Karpen SJ, London WT, Murray KF, et al. Treatment of children with chronic hepatitis B virus infection in the United States: patient selection and therapeutic options. Hepatology 2010; 52: 2192–2205. [DOI] [PubMed] [Google Scholar]
- 8. Jonas MM, Kelly D, Pollack H, Mizerski J, Sorbel J, Frederick D et al. Safety, efficacy, and pharmacokinetics of adefovir dipivoxil in children and adolescents (age 2 to < 18 years) with chronic hepatitis B. Hepatology 2008; 47: 1863–1871. [DOI] [PubMed] [Google Scholar]
- 9. Jonas MM, Mizerski J, Badia IB, Areias JA, Schwarz KB, Little NR, et al. Clinical trial of lamivudine in children with chronic hepatitis B. New Engl J Med 2002; 346: 1706–1713. [DOI] [PubMed] [Google Scholar]
- 10. Sokal EM, Conjeevaram HS, Roberts EA, Alvarez F, Bern EM, Goyens P, et al. Interferon alfa therapy for chronic hepatitis B in children: a multinational randomized controlled trial. Gastroenterology 1998; 114: 988–995. [DOI] [PubMed] [Google Scholar]
- 11. Murray KF, Szenborn L, Wysocki J, Rossi S, Corsa AC, Dinh P, et al. Randomized, placebo‐controlled trial of tenofovir disoproxil fumarate in adolescents with chronic hepatitis B. Hepatology 2012; 56: 2018–2026. [DOI] [PubMed] [Google Scholar]