

Watch a video presentation of this article
The normal color of the liver is brown and the external surface is smooth (Fig. 1). The liver is about 2% of body weight in the adult, which amounts to approximately 1400 g in females and 1800 g in males. The liver receives its blood supply from two sources: 80% is delivered by the portal vein, which drains the spleen and intestines; the remaining 20%, the oxygenated blood, is delivered by the hepatic artery. The portal vein is formed by the union of the splenic and the superior mesenteric veins with the inferior mesenteric vein draining into the splenic vein (Fig. 2). In the majority of cases, the common hepatic artery is a branch of the celiac artery along with the splenic and left gastric arteries (Figs. 3 and 4). Occasionally, the hepatic artery has accessory or replaced vessels supplying the liver. The accessory or replaced right hepatic artery is a branch of the proximal superior mesenteric artery, while the accessory or replaced left hepatic artery is a branch of the left gastric artery (Fig. 3). Multiple anatomic variations, however, may also exist in the anatomy of the hepatic artery.1
Figure 1.
Normal liver.
Figure 2.
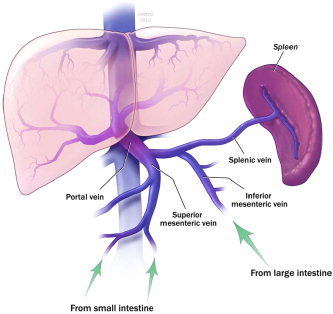
Portal venous drainage.
Figure 3.
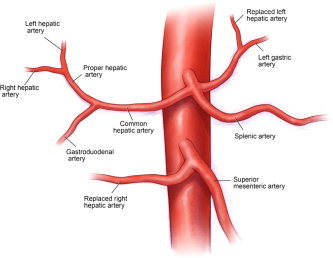
Arterial supply to liver and aberrant arterial anatomy.
Figure 4.
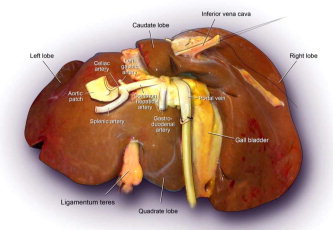
Posterior view of the liver.
Externally, the liver is divided by the falciform ligament into a larger right lobe and a smaller left lobe (Fig. 5). The falciform ligament attaches the liver to the anterior abdominal wall. Its base contains the ligamentum teres, which has a remnant of the vestigial umbilical vein. In cirrhosis, this vein recanalizes as a result of portal hypertension.
Figure 5.
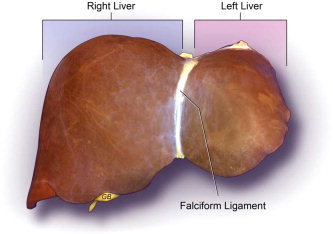
Morphological anatomy of the liver.
Based on Couinaud classification, the liver is divided into eight independent functional segments (Figs. 6 and 7). Each segment has its own portal pedicle consisting of the hepatic arterial branch, portal branch, and the bile duct with a separate hepatic venous branch that provides outflow (Fig. 8). The numbering of segments is in a clockwise manner. Segments II and III, which are known as the anterior and posterior segments of the left lobe, respectively, are also known collectively as the left lateral segment of the liver and the topographic left lobe. Segment IV is the medial segment of the left lobe. Segments II, III, and IV collectively make up the functional left lobe of the liver. The functional right lobe of the liver is made up of segments V and VIII, the anterior segments, and segments VI and VII, the posterior segments. Segment I, the caudate lobe, is located posteriorly.
Figure 6.
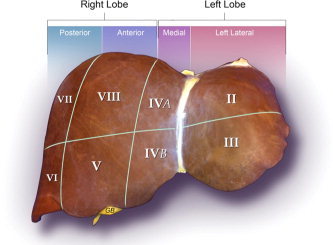
Functional anatomy of the liver.
Figure 7.
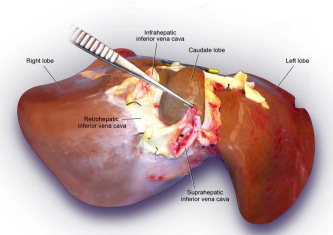
Posterior view of the liver.
Figure 8.
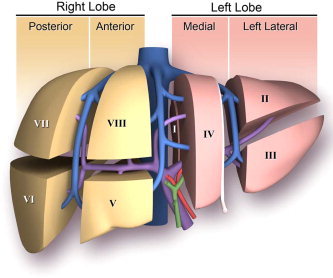
Segmental anatomy of the liver.
The outflow of the liver is provided by the three hepatic veins. The right hepatic vein divides the right lobe of the liver into anterior and posterior segments. The middle hepatic vein divides the liver into the right and left lobes and runs in the same plane with the inferior vena cava and the gallbladder fossa. The left hepatic vein divides the left liver into medial and lateral segments. The portal vein divides the liver into the upper and lower segments (Fig. 8).
The segmental liver anatomy is important to radiologists and surgeons, especially in view of the need for an accurate preoperative localization of focal hepatic lesions.2, 3 Liver resection depends on accurate localization of the hepatic lesions and knowledge of liver anatomy. Liver resection is now practiced widely with reduced morbidity and minimal mortality. Nonanatomic resections encompass wedge resections. Segmentectomies are anatomical resections of segments based on Couinaud classification. Bisegmentectomy includes resection of segments II and III is known as a left lateral segmentectomy. Resection of segment IV is known as a left medial segmentectomy, resection of segments V and VIII is known as a right anterior segmentectomy, and resection of segments VI and VII are known as a right posterior segmentectomy. Resection of segments II, III, and IV is known as the left lobe resection or left hepatectomy. Resection of segments V, VI, VII, VIII is known as right lobe resection or right hepatectomy. Extended right hepatectomy includes segments IV to VIII, while extended left hepatectomy includes segments II, III, IV, V, VIII (Table 1).
Table 1.
Hepatic Anatomy and Resection Nomenclature
| Anatomical Resections | Liver Segments |
|---|---|
| Left lateral segmentectomy | II, III |
| Left medial segmentectomy | IV |
| Right anterior segmentectomy | V, VIII |
| Right posterior segmentectomy | VI, VII |
| Left hepatectomy | II, III, IV |
| Right hepatectomy | V, VI, VII, VIII |
| Extended left hepatectomy | II, III, IV, V, VIII |
| Extended right hepatectomy | IV, V, VI, VII, VIII |
Cirrhosis is an end result of parenchymal degeneration, regeneration, and scarring (Fig. 9). The cirrhotic liver varies in color, size, and appearance, depending on etiology. It might be large and green in diseases with biliary obstruction, such as primary sclerosing cholangitis or yellow and small in advanced alcoholic cirrhosis. It is firm and appears either micro‐ or macronodular as a result of formation of regenerative nodules with surrounding fibrosis in the parenchyma of the liver. Portal hypertension develops because of liver stiffness and increased resistance to flow. As a result, the blood is shunted away from the liver, and new thin dilated vessels form, shunting the blood away from the portal to the systemic circulation. Examples include esophageal, gastric, and rectal varices.4
Figure 9.
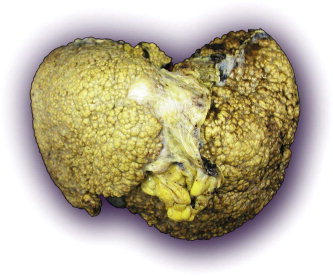
Liver cirrhosis.
Acknowledgements
I thank Raouf E. Nakhleh for revising the paper and Margaret A. McKinney and David T. Smyrk for creating the figures.
Potential conflict of interest: Nothing to report.
References
- 1. Hiatt JR, Gabbay J, Busuttil RW. Surgical anatomy of the hepatic arteries in 1000 cases. Ann Surg 1994; 220: 50–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Soler L, Delingette H, Malandain G, Montagnat J, Ayache N, Koehl C, et al. Fully automatic anatomical, pathological, and functional segmentation from CT scans for hepatic surgery. Comp Aid Surg 2001; 6: 131–142. [DOI] [PubMed] [Google Scholar]
- 3. Liau KH, Blumgart LH, DeMatteo RP. Segment‐oriented approach to liver resection. Surg Clin N Am 2004; 84: 543–561. [DOI] [PubMed] [Google Scholar]
- 4. Garcia‐Tsao G, Bosch J. Management of varices and variceal hemorrhage in cirrhosis. N Engl J Med 2010; 362: 823–832. [DOI] [PubMed] [Google Scholar]