

Abstract
Introduction The cochlear anatomy varies in each individual, and that has an impact on decisions regarding the insertion of electrodes. The measurement of the cochlear size is the routine examination required to choose the proper cochlear implant (CI) electrodes.
Objective To acquire normative data on the size of the cochlea (length, width, height, scala timpani [ST] height, cochlear duct length [CDL]) of CI candidates in Medan, Indonesia.
Methods This descriptive study was conducted based on high-resolution computed tomography (HRCT) temporal bone data and on HRCT temporal data manipulated to reconstruct three-dimensional (3D) multiplanar images with OsiriX MD DICOM Viewer version 9.5.1 (Pixmeo SARL, Bernex, Geneva, Switzerland) viewer of 18 patients (36 ears) who were CI candidates in Medan, Indonesia, in order to determine cochlear length (A), cochlear width, cochlear height, ST height and CDL, calculated through a simple mathematical function.
Results The average cochlear length (A) was 8.75 mm (standard deviation [SD] = 0.31 mm); the average cochlear width was 6.53 mm (SD = 0.35 mm); the average cochlear height was 3.26 mm (SD = 0.24 mm) and the average ST height at the basal cochlea was 1.00 mm (SD = 0.1 mm); and 0.71 mm (SD = 0.1 mm) at the half turn of cochlea. The average total CDL was 32.45 mm (SD = 1.31 mm; range: 30.01–34.83 mm).
Conclusion The cochlear size varies in each individual; therefore, the temporal bone measurement of CI candidates using HRCT is essential: for the selection of suitable implant electrodes; to minimize cochlear damages at the insertion of the electrode arrays; and to maximize the hearing improvements.
Keywords: cochlea, cochlear implant, computed tomography, temporal bone
Introduction
Congenital sensorineural hearing loss is generally bilateral, and most of the cases present severe to profound hearing loss. 1 2 3 Hearing rehabilitation with a cochlear implant (CI) for electrical stimulation of the auditory nerve is a standard therapy for severe to profound congenital hearing loss that has received little or no benefit from hearing aids. 1 2
Bony cochlear or vestibular malformations occur in ∼ 20 to 25% of the patients with congenital hearing loss, which is indicated by a computed tomography (CT) of the temporal bone. Although the human cochlea reaches adult size before birth, it is known that the size of the cochlea varies between individuals, and that the cochlea differs significantly in shape, size and spiral characteristics. 4 5 6 7 8 9 10 11 12 13 14 15 Currently, because of the variations among individuals, and in order to preserve the residual hearing, CIs tend to have dimensions designed for each individual cochlear size. Detailed quantified information about the variation of each individual cochlea is required to enable the design of the appropriate CI electrode for each individual. 6 8
A high-resolution computed tomography (HRCT) of the temporal bone is routinely performed before CI surgery. The HRCT can evaluate inner ear abnormalities, facilitate surgical planning, and define the features of the cochlear nerve, as well as identify the presence of malformations or ossifications that may limit the access to the scala timpani (ST). 16 17 18 Preoperative prediction of the design of the CI electrode may help reduce the risk of intraoperative cochlear trauma in patients who need to preserve acoustic hearing for electroacoustic stimulation, or in patients with anomalies or malformations. Indications for cochlear implantation have been expanded to include not only deafness, but also severe hearing impairment with unsatisfactory speech perception through the use of hearing aids. 18 19 20
Knowing about individual cochlear variations is essential for the greatest possible electrode insertion with a minimal risk of injury. The implant may stimulate the rest of the spiral ganglion located in the cochlear apex. In some cases, the depth of the insertion can also be adjusted for residual hearing, especially in patients with severe to profound hearing loss at high and low frequencies, whose hearing is preserved to be given electroacoustic stimulation. Therefore, the measurement of the length of the cochlea is important to predict the proper insertion depth for each individual, to select the appropriate electrode, and for the planning of surgical techniques prior to CI surgery. 18 19
The purpose of the present study is to establish normative data on the size of the cochlea (cochlear length, width, height, ST height, cochlear duct length [CDL]) from HRCT temporal bone data of CI candidates in Medan, Indonesia.
Methods
In the present study, we included the HRCT temporal bone data of 18 patients (36 ears) aged between 2 and 17 years old, consisting of 11 men and 7 women, who presented congenital sensorineural hearing loss and had been screened for cochlear anomaly or malformation as CI candidates in Medan, Indonesia, between October 2012 and September 2017. We excluded HRCT temporal bone data that could not be evaluated after multiplanar reconstruction. The Health Research Ethical Committee granted approval for the study.
The temporal bone data obtained through HRCT was used to perform a three-dimensional (3D) multiplanar reconstruction with OsiriX MD DICOM Viewer version 9.5.1 (Pixmeo SARL, Bernex, Geneva, Switzerland) viewer to obtain cochlear length (A), cochlear width, cochlear height, and ST height. A view of the basal turn of the cochlea was developed in a double oblique coronal reformatted image, as shown in Fig. 1 . In one view, the round window, the oval window, the basal turn of the cochlea, the vestibule and the anterior branches of the lateral and superior semicircular canals can be seen. The view was developed to provide the largest distance from the round window through the mid modiolar axis to the lateral wall, which was measured as cochlear length, and the perpendicular distance, which was measured as cochlear width. 8 11 21 22
Fig. 1.
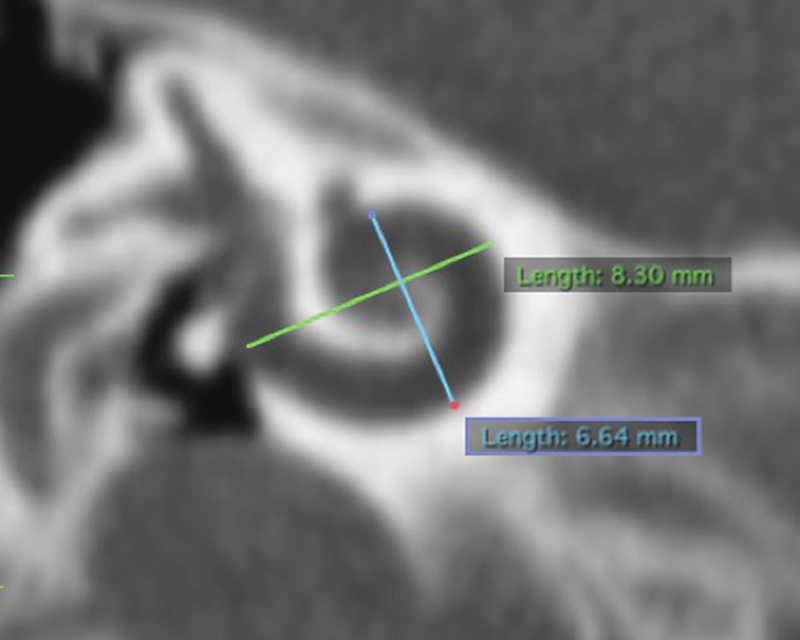
A double-oblique coronal reformatted image. Distance A (cochlear length) of 8.30 mm, and perpendicular distance (cochlear width) of 6.64 mm.
The cochlear height [ Fig. 2 ] was obtained from an axial image reconstructed from a temporal HRCT and was defined as the length between the tip of the cochlea and the orthogonal projection passing through the middle of the canal to the cochlear base. 8 23
Fig. 2.
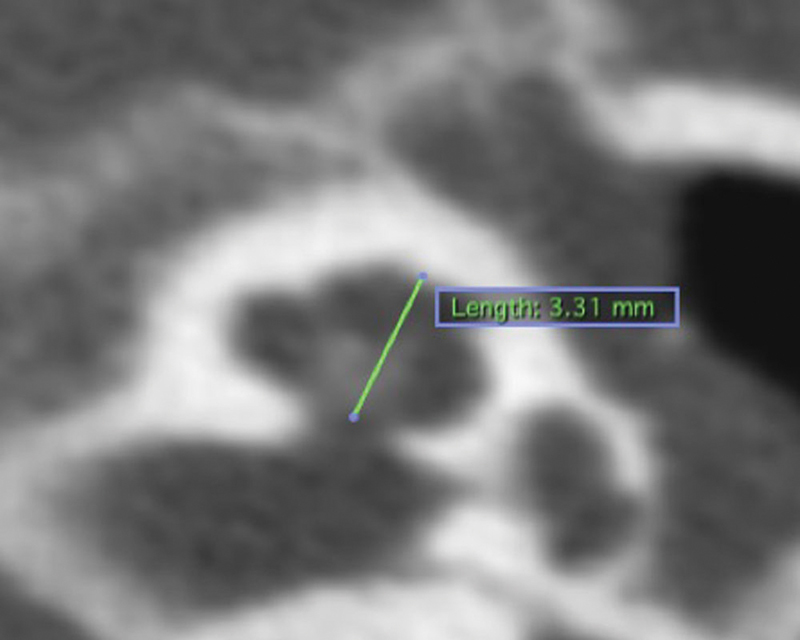
Axial computed tomography of the left ear shows an example of the measurement of the cochlear height (3.31 mm).
The ST height was measured at two locations: at the base of the cochlea and at the half-turn of the cochlea, which provided the center height of the ST, as shown in Fig. 3 . 24
Fig. 3.
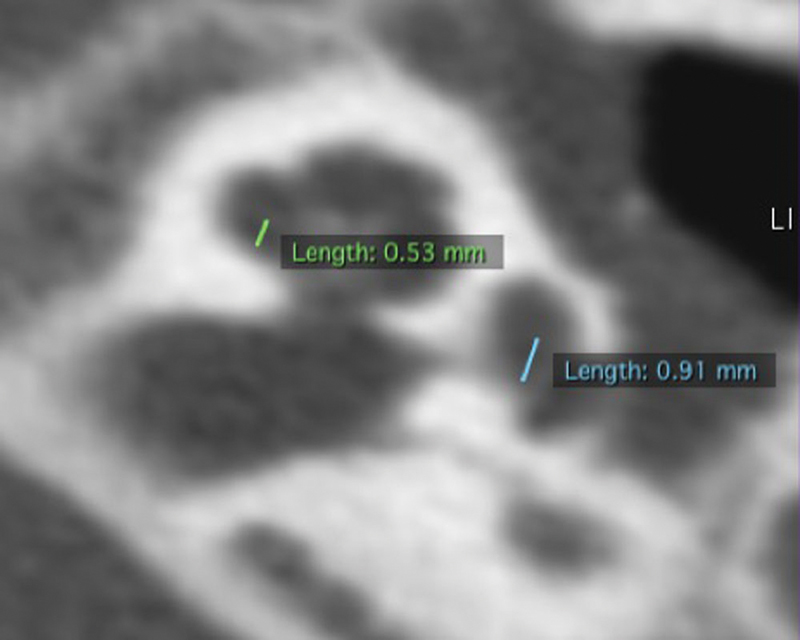
Measurements of the height of the scala timpani on axial computed tomography image (0.91 mm at the basal turn, and 0.53 mm at half-turn).
The CDL is the length of the scala media measured from the middle of the round window to 1 turn of the cochlea (360°), using the formula 2.43A – 2.43. The formulas used to measure additional turns were: 1.5 turns (540°): 3A – 3.02; 2 turns (720°): 3.65A – 3.63; 2.5 turns, or helicotrema (900°): 4.16A – 3.98. 25 26
Results
The mean value of the cochlear length (A) was 8.75 mm (standard deviation [SD] = 0.31 mm), the mean cochlear width was 6.53 mm (SD = 0.35 mm), and the mean cochlear height was 3.26 mm (SD = 0.24 mm), as shown in Table 1 and in the box plots in Fig. 4 (A) . The mean ST height at the basal cochlea was 1.00 mm (SD = 0.1 mm) and 0.71 mm (SD = 0.1 mm) at the half turn of the cochlea (180°), as shown in Table 2 and in the box plots in Fig. 4 (B) . The mean length of the cochlear duct was: 18.85 mm (SD = 0.76 mm) at 1 turn of the cochlea (360°); 23.25 mm (SD = 0.94 mm) at 1.5 turns (540°); 28.33 mm (SD = 1.15 mm) at 2 turns (720°); and 32.45 mm (SD = 1.31 mm; range: 30.01–34.83 mm) at 2.5 turns (900°), as shown in Table 3 and in the box plots in Fig. 4 (C) .
Table 1. Cochlear length, cochlear width and cochlear height.
| Cochlear length (mm) | Cochlear width (mm) | Cochlear height (mm) | |
|---|---|---|---|
| Mean | 8.75 | 6.53 | 3.26 |
| Median | 8.83 | 6.51 | 3.26 |
| Standard deviation | 0.31 | 0.35 | 0.24 |
| Minimum | 8.17 | 5.73 | 2.80 |
| Maximum | 9.33 | 7.50 | 3.72 |
Fig. 4.
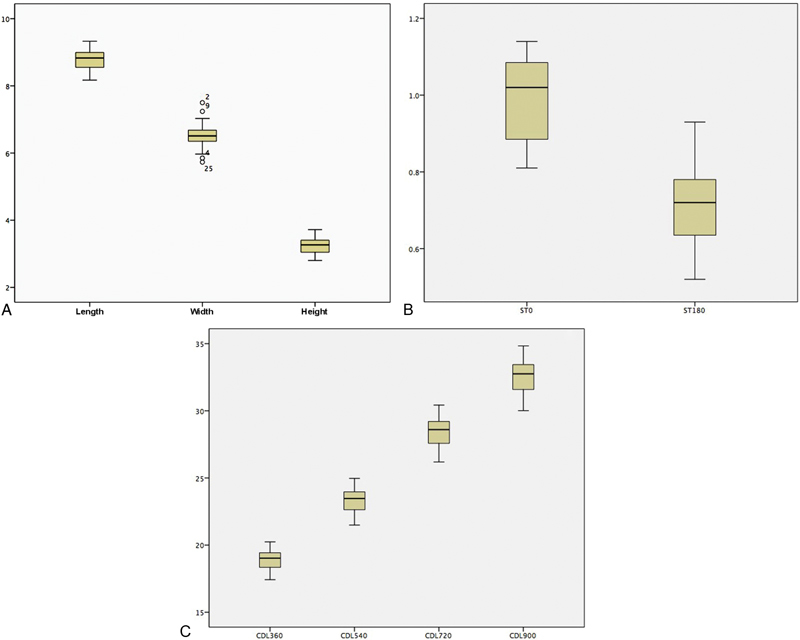
( A ) Box-plots of the cochlear length, width and height. ( B ) Scala timpani height: ST0 = scala timpani height at basal turn, ST180 = scala timpani height at half-turn. ( C ) Cochlear duct length at 360°, 540°, 720° and 900° of cochlear turn.
Table 2. Scala timpani height at basal turn (0°) and half-turn of the cochlea (180°).
| Scala timpani height/0° (mm) | Scala timpani height/180° (mm) | |
|---|---|---|
| Mean | 1.00 | 0.71 |
| Median | 1.02 | 0.72 |
| Standard deviation | 0.10 | 0.10 |
| Minimum | 0.81 | 0.52 |
| Maximum | 1.14 | 0.93 |
Table 3. Cochlear duct length at 1 turn of the cochlea (360°), 1.5 turns of the cochlea (540°), 2 turns of the cochlea (720°), and 2.5 turns of the cochlea (900°).
| Cochlear duct length 360° (mm) | Cochlear duct length 540° (mm) | Cochlear duct length 720° (mm) | Cochlear duct length 900° (mm) | |
|---|---|---|---|---|
| Mean | 18.85 | 23.25 | 28.33 | 32.45 |
| Median | 19.02 | 23.47 | 28.59 | 32.75 |
| Standard deviation | 0.76 | 0.94 | 1.15 | 1.31 |
| Minimum | 17.42 | 21.49 | 26.19 | 30.01 |
| Maximum | 20.24 | 24.97 | 30.42 | 34.83 |
Notes: 360° = 1 turn of the cochlea; 540° = 1.5 turns of the cochlea; 720° = 2 turns of the cochlea; 900° = 2.5 turns turn of the cochlea.
Discussion
Important advances have been made in the insertion of electrodes into the cochlea during cochlear implantation, and they are especially focused on minimizing trauma during insertion and preserving the residual hearing. This result can be achieved with appropriate cochlear electrodes and less traumatic surgical techniques. 7
There are extensive individual variations in cochlear size, which may influence its final position relatively to the cochlea place or the frequency map and final pitch discrimination. 27 These variations have implications for the cochlear electrode insertion as well as for the design of the electrode array. 6 7 19 There are various methods to measure the size of the cochlea. Advances in imaging technology with HRCT and 3D reconstructions can now reliably detect and quantify variations in the human cochlear anatomy. 8 11 17 28 29
Cochlear length measurements are important to estimate the depth of individual electrode insertion and to an appropriate electrode selection, as well as for the planning of surgical techniques prior to the CI surgery. A 3D multiplanar reconstruction analysis of the HRCT data enables a linear reconstruction of length measurements. In some cases, this will be helpful to choose the optimal electrode length before the CI surgery, to minimize intracochlear trauma, and to enable a proper electrode fitting. For electroacoustic stimulation (EAS) surgery, an appropriate prediction of the length of the electrode should be obtained in order to avoid trauma of the apical structures and to obtain good hearing performance. 18
Escude et al 11 developed a method for quantitative determination of the size of the cochlea using reconstructed images from routine HRCTs of the temporal bone. The full basal turn of the cochlea was visualized, and calculations of the length of the outer wall of the basal turn could be made. Measurements based on CT images have been shown to be in accordance with measurements based on histological preparations. 30
We have found that the mean cochlear length was 8.75 mm (SD = 0.31 mm), the mean cochlear width was 6.53 mm (SD = 0.35 mm), and the mean cochlear height was 3.26 mm (SD = 0.24 mm). A previous study by Escude et al 11 found that the mean cochlear length (A) was 9.23 mm (SD = 0.53 mm), and that the mean cochlear width was 6.99 mm (SD = 0.37 mm), which are greater than those found in the present study. A study by Pelliccia et al 21 has also found that the mean cochlear length in patients with severe to profound bilateral sensorineural deafness was 9.06 mm (SD = 0.7 mm), and that the mean cochlear width was 6.92 mm (range: 4.8mm–8.5mm). Gao et al 31 measured the cochlear length in Chinese people and found that the mean cochlear length among males was 9.04mm (SD = 0.3 mm), and 8.80 mm (SD = 0.4 mm) among females. The cochlear width in men was 6.7 mm (SD = 0.34 mm), and 6.38 mm (SD = 0.29 mm) in women, which are similar to the results of the present study. Grover et al, 32 who conducted a study with children < 6 years of age in Jaipur, India, found that the mean cochlear length (A) was 8.12 mm (range: 7.7mm–9.2mm), which is lower than the results of the present study. Both studies revealed that the cochlear length was smaller in the Asian population. Avci et al 8 , in Hannover, Germany, found an average cochlear length of 9.2 mm, average cochlea width of 7.0 mm and average cochlear height of 4.4 mm in 16 fresh-frozen human temporal bones without any evidence of malformation, which were then scanned using micro-CT and measured by reconstructing the micro-CT. The values found by Avci et al are greater than the results of the present study. Similarly, a research by Shin et al 14 in South Korea obtained a mean cochlear height of 3.8 mm (SD = 0.2 mm) on a micro-CT image of 39 temporal bones of corpses. A study by Hassan et al 33 described the measurements of cochlear anatomy in Sudanese people, and found that the average left cochlear height was 3.6 mm (SD = 0.4 mm), and that the average right cochlear height was 3.5 mm (SD = 0.4 mm).
Several radiological studies have analyzed the correlation of CDL with the diameter of the basal cochlea, termed the “A” value, the length of the scala media measured from the middle of the round window to the opposite point in the basal turn through the mid-modiolar axis. 11 26 Johnston et al 26 determined that the CDLs (from the measurement of the “A” value) can help estimate the full insertion after the cochlear implantation, while a previous study by Escudé et al 11 established a relationship between the CDL and the diameter of the basal cochlea; the study involved radiologists with extensive experience to perform image reconstructions and measurements.
The marker for the round window niche, as described by Erixon et al 6 and Biedron et al, 10 is used to measure the dimensions of the cochlea. The midpoint of the round window niche is used as the starting point of the cochlea, and the cochlear length is the line drawn from the center point of the round window niche to the opposite point through the central axis of the cochlea (mid-modiolar axis). 11 14 34
Approximately 25% of the patients with congenital sensorineural hearing loss or mixed hearing loss showed malformations of the bony inner ear, which was indicated by temporal CT images, with significantly smaller cochlear height when compared to patients with normal hearing. 35 36 The cochlear height plays a role in diagnosing sensorineural hearing loss in patients with hypoplasia or hyperplasia. 33 35
Tarabishi et al, 36 who conducted a study in Egypt, revealed that the cochlear height was an important measurement in determining subclassification and diagnosing hypoplasia and small cochleae (dwarf cochleae). The authors defined dwarf cochleae in Egyptians as morphologically normal cochleae with less than 2.5 turns, patent ducts, and a significantly reduced cochlear height detected through HRCT, which required a special modification in the surgery regarding the length of the electrode and the location of the cochleostomy during the cochlear implantation.
Manufacturers of CIs have proposed electrode arrays with a softer mechanical profile and a smaller diameter to minimize insertion trauma and ensure the proper placement of the electrodes. To determine this optimal length and the diameter of the electrode arrays, it is important to evaluate the cochlear volume by measuring the diameter of the ST in order to determine the maximum possible diameter of the electrode arrays along the cochlea. 24
In the present study, the mean value of the ST height in the basal cochlea was 1.00 mm (SD = 0.10 mm), and the mean value of the ST height in the half-turn of the cochlea was 0.71 mm (SD = 0.10 mm). This value is lower than the results of previous studies by Wysocki, 9 who found that the height of the ST in the basal cochlea was 1.3 mm, and that near the apex, the height of the ST decreased by 0.25 mm. Similarly, Biedron et al 10 obtained a mean value of the ST height in the basal cochlea of 1.22 mm (range: 0.96–1.48 mm), and of 1.08 mm in the half-turn of the cochlea (range: 0.87–1.28 mm) on histological examinations of 28 human cochlear specimens without any evidence of labyrinth malformations. Similarly, Braun et al, 37 measured the height of the ST in the temporal bone of a cadaver of a 54-year-old female with absence of hearing loss, malformation or bacterial and viral contamination, and afterwards performed a micro-CT reconstruction. The measurements obtained of the ST height in the basal cochlea were 1.39 mm, and 1.15 mm in the half turn of the cochlea, which were higher than the results of the present study.
The CDL is defined as the length of the scala media measured from the middle of the round window to the helicotrema. Measuring the CDL is very important in the CI preoperative stage. With the availability of variable length electrodes, patient-customized electrodes and reports of incomplete insertions of the longer electrodes, measuring the CDL before performing a CI is essential in order to select the appropriate electrode length. 25 34 38 Alexiades et al 34 reported that a single linear measurement of a CT image is believed to predict the effective total CDL. Johnston et al 26 stated that the CDL (determined by the calculation of the value of A, the length of the cochlear basal turn) can help to estimate full insertion after CIs.
In the present study, the mean total CDL (2.5 turns) was 32.45 mm (SD = 1.31 mm; range: 30.01–34.83 mm). In a study using a 3D and a histopathological reconstruction, both methods obtained the mean value of the CDL from the midpoint of the round window to the helicotrema ranging between 30 and 31 mm. 14 22 39 Koch et al 22 compared several methods of measuring the CDL. Using the average direct method, the mean value of the CDL was 33.79 mm. The indirect method resulted in a mean value of 31.31 mm, while the 3D reconstruction method resulted in an average CDL of 35.04 mm.
There is a significant variability in the CDL in humans. 8 39 This variability has clinical applications for cochlear implantation because the depth of the electrode insertion may be associated with insertion trauma and postoperative hearing function impairment. In addition, given that variations in length and electrodes tailored to the patients are available, some researchers are seriously concerned with the measurement of the CDL before the cochlear implantation in order to help determine the correct length of the electrode. 38
Deep insertion of an electrode into the cochlear apex provides the maximal range of frequency stimuli, can increase the word recognition score and improve the detection of pitch at low frequencies, a more natural speech perception, 40 41 and the identification of intonation. 42 However, when placing electrodes closer to the apex, physicians should reconsider the risk of cochlear damage if using long electrodes with deep insertion. Given the significant variation in normal cochlear dimensions and with the aim of reducing trauma during the insertion, the electrode selection should be tailored for each individual. 43
In the present research, we found that the minimum total CDL was 30.01 mm, and the maximum total CDL was 34.83 mm. This means that a CDL of 30.01 mm is not appropriate for the implantation of an electrode with a length of 31.5 mm, because the electrode will be kinked at the apex, so it can damage the apical structures. Similarly, for a CDL of 34.83 mm, when an electrode with a length of 24 mm is implanted, it will not cover the apex cochlea. This will cause a loss of stimulus from low frequencies, which plays a role in low pitch and intonation identification. Therefore, the preoperative measurement of the CDL becomes the guideline for the surgeon to choose the proper electrodes, with the aim of obtaining good hearing and auditory perceptions after the cochlear implantation.
Conclusion
Cochlear size varies in each individual; therefore, the measurement of temporal HRCT data of CI candidates is essential for the selection of suitable implant electrodes. A shallow insertion of a cochlear electrode reduces the risk of damage to apical structures, whereas a deep insertion of the array may improve the performance of the CI in cases of loss of residual hearing. With a proper electrode, we aim to obtain good hearing and auditory perceptions after the cochlear implantation.
The data regarding the cochlear duct may provide information to assist the design of individualized cochlear electrode insertion. The CDL should be calculated preoperatively in every patient.
References
- 1.Chi D H, Sabo D L. Philadelphia: Lippincott Williams & Wilkins, a Wolters Kluwer business; 2014. Pediatric audiology and implantable hearing devices; pp. 1507–1522. [Google Scholar]
- 2.Vincenti V, Bacciu A, Guida M et al. Pediatric cochlear implantation: an update. Ital J Pediatr. 2014;40(01):72. doi: 10.1186/s13052-014-0072-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Paludetti G, Conti G, DI Nardo W et al. Infant hearing loss: from diagnosis to therapy Official Report of XXI Conference of Italian Society of Pediatric Otorhinolaryngology. Acta Otorhinolaryngol Ital. 2012;32(06):347–370. [PMC free article] [PubMed] [Google Scholar]
- 4.Xu J, Xu S A, Cohen L T, Clark G M. Cochlear view: postoperative radiography for cochlear implantation. Am J Otol. 2000;21(01):49–56. [PubMed] [Google Scholar]
- 5.Dimopoulos P, Muren C. Anatomic variations of the cochlea and relations to other temporal bone structures. Acta Radiol. 1990;31(05):439–444. [PubMed] [Google Scholar]
- 6.Erixon E, Högstorp H, Wadin K, Rask-Andersen H. Variational anatomy of the human cochlea: implications for cochlear implantation. Otol Neurotol. 2009;30(01):14–22. doi: 10.1097/MAO.0b013e31818a08e8. [DOI] [PubMed] [Google Scholar]
- 7.Erixon E, Liu W, Rask-Andersen H. Anatomic studies of the human cochlea: implications for cochlear implantation. The Registry. 2011;19(01):1–7. [Google Scholar]
- 8.Avci E, Nauwelaers T, Lenarz T, Hamacher V, Kral A. Variations in microanatomy of the human cochlea. J Comp Neurol. 2014;522(14):3245–3261. doi: 10.1002/cne.23594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wysocki J.Dimensions of the human vestibular and tympanic scalae Hear Res 1999135(1-2):39–46. [DOI] [PubMed] [Google Scholar]
- 10.Biedron S, Prescher A, Ilgner J, Westhofen M. The internal dimensions of the cochlear scalae with special reference to cochlear electrode insertion trauma. Otol Neurotol. 2010;31(05):731–737. doi: 10.1097/MAO.0b013e3181d27b5e. [DOI] [PubMed] [Google Scholar]
- 11.Escudé B, James C, Deguine O, Cochard N, Eter E, Fraysse B.The size of the cochlea and predictions of insertion depth angles for cochlear implant electrodes Audiol Neurootol 2006;1101, Suppl0127–33. [DOI] [PubMed] [Google Scholar]
- 12.Hardy M. The length of the organ of Corti in man. Am J Anat. 1938;62(02):291–311. [Google Scholar]
- 13.Rask-Andersen H, Erixon E, Kinnefors A, Löwenheim H, Schrott-Fischer A, Liu W.Anatomy of the human cochlea--implications for cochlear implantation Cochlear Implants Int 201112(Suppl01S8–S13. [DOI] [PubMed] [Google Scholar]
- 14.Shin K J, Lee J Y, Kim J N et al. Quantitative analysis of the cochlea using three-dimensional reconstruction based on microcomputed tomographic images. Anat Rec (Hoboken) 2013;296(07):1083–1088. doi: 10.1002/ar.22714. [DOI] [PubMed] [Google Scholar]
- 15.Verbist B M, Ferrarini L, Briaire J J et al. Anatomic considerations of cochlear morphology and its implications for insertion trauma in cochlear implant surgery. Otol Neurotol. 2009;30(04):471–477. doi: 10.1097/MAO.0b013e3181a32c0d. [DOI] [PubMed] [Google Scholar]
- 16.Kawano A, Seldon H L, Clark G M. Computer-aided three-dimensional reconstruction in human cochlear maps: measurement of the lengths of organ of Corti, outer wall, inner wall, and Rosenthal's canal. Ann Otol Rhinol Laryngol. 1996;105(09):701–709. doi: 10.1177/000348949610500906. [DOI] [PubMed] [Google Scholar]
- 17.Ketten D R, Skinner M W, Wang G, Vannier M W, Gates G A, Neely J G. In vivo measures of cochlear length and insertion depth of nucleus cochlear implant electrode arrays. Ann Otol Rhinol Laryngol Suppl. 1998;175:1–16. [PubMed] [Google Scholar]
- 18.Kisser U, Ertl-Wagner B, Hempel J M et al. High-resolution computed tomography-based length assessments of the cochlea--an accuracy evaluation. Acta Otolaryngol. 2014;134(10):1011–1015. doi: 10.3109/00016489.2014.913313. [DOI] [PubMed] [Google Scholar]
- 19.Thong J F, Low D, Tham A, Liew C, Tan T Y, Yuen H W. Cochlear duct length-one size fits all? Am J Otolaryngol. 2017;38(02):218–221. doi: 10.1016/j.amjoto.2017.01.015. [DOI] [PubMed] [Google Scholar]
- 20.Aschendorff A. Imaging in cochlear implant patients. GMS Curr Top Otorhinolaryngol Head Neck Surg. 2011;10:Doc07. doi: 10.3205/cto000080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Pelliccia P, Venail F, Bonafé A et al. Cochlea size variability and implications in clinical practice. Acta Otorhinolaryngol Ital. 2014;34(01):42–49. [PMC free article] [PubMed] [Google Scholar]
- 22.Koch R W, Ladak H M, Elfarnawany M, Agrawal S K. Measuring Cochlear Duct Length - a historical analysis of methods and results. J Otolaryngol Head Neck Surg. 2017;46(01):19. doi: 10.1186/s40463-017-0194-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Teissier N, Van Den Abbeele T, Sebag G, Elmaleh-Berges M. Computed Tomography measurements of the normal and the pathologic cochlea in children. Pediatr Radiol. 2010;40(03):275–283. doi: 10.1007/s00247-009-1423-2. [DOI] [PubMed] [Google Scholar]
- 24.Gnansia D, Demarcy T, Vandersteen Cet al. Optimal electrode diameter in relation to volume of the cochlea Eur Ann Otorhinolaryngol Head Neck Dis 2016;13301, Suppl01S66–S67. [DOI] [PubMed] [Google Scholar]
- 25.Wimmer W, Gerber N, Dhanasingh A et al. In-vitro microCT validation of preoperative cochlear duct length estimation. CURAC. 2013;1477:143–146. [Google Scholar]
- 26.Johnston J D, Scoffings D, Chung M et al. Computed tomography estimation of cochlear duct length can predict full insertion in cochlear implantation. Otol Neurotol. 2016;37(03):223–228. doi: 10.1097/MAO.0000000000000955. [DOI] [PubMed] [Google Scholar]
- 27.Baskent D, Shannon R V.Speech recognition under conditions of frequency-place compression and expansion J Acoust Soc Am 2003113(4 Pt 1):2064–2076. [DOI] [PubMed] [Google Scholar]
- 28.Skinner M W, Ketten D R, Holden L K et al. CT-derived estimation of cochlear morphology and electrode array position in relation to word recognition in Nucleus-22 recipients. J Assoc Res Otolaryngol. 2002;3(03):332–350. doi: 10.1007/s101620020013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.James C, Albegger K, Battmer R et al. Preservation of residual hearing with cochlear implantation: how and why. Acta Otolaryngol. 2005;125(05):481–491. doi: 10.1080/00016480510026197. [DOI] [PubMed] [Google Scholar]
- 30.Adunka O, Unkelbach M H, Mack M G, Radeloff A, Gstoettner W. Predicting basal cochlear length for electric-acoustic stimulation. Arch Otolaryngol Head Neck Surg. 2005;131(06):488–492. doi: 10.1001/archotol.131.6.488. [DOI] [PubMed] [Google Scholar]
- 31.Gao Z, Tian X, Feng G.Cochlea duct length of Chinese adults for individualized cochlear electrode design. Meeting Abstract 84 th Annual Meeting of the German Society of Oto-Rhino-Laryngology Head and Neck Surgery. Numberg: German Medical Science GMS; 2013
- 32.Grover M, Mishra P, Gupta G, Jangid M.Cochlear duct length: are we giving it adequate importance? Otolaryngol Head Neck Surg 201314902219–225.23629969 [Google Scholar]
- 33.Hassan L A, Ayad C E, Hassan H A, Abdalla E A, Mohamed M E. Normative Sudanese cochlea measurements using high resolution computerized tomography. GARJMMS. 2014;3(06):117–123. [Google Scholar]
- 34.Alexiades G, Dhanasingh A, Jolly C. Method to estimate the complete and two-turn cochlear duct length. Otol Neurotol. 2015;36(05):904–907. doi: 10.1097/MAO.0000000000000620. [DOI] [PubMed] [Google Scholar]
- 35.Purcell D, Johnson J, Fischbein N, Lalwani A K. Establishment of normative cochlear and vestibular measurements to aid in the diagnosis of inner ear malformations. Otolaryngol Head Neck Surg. 2003;128(01):78–87. doi: 10.1067/mhn.2003.51. [DOI] [PubMed] [Google Scholar]
- 36.Tarabishi M N, Sarwat A A, Rabie H M et al. Miniature cochlea: a study of radiological measurements and its implications during the cochlear implant surgery. Egypt J Otolaryngol. 2016;32(03):170–177. [Google Scholar]
- 37.Braun K, Böhnke F, Stark T. Three-dimensional representation of the human cochlea using micro-computed tomography data: presenting an anatomical model for further numerical calculations. Acta Otolaryngol. 2012;132(06):603–613. doi: 10.3109/00016489.2011.653670. [DOI] [PubMed] [Google Scholar]
- 38.Deep N L, Howard B E, Holbert S O, Hoxworth J M, Barrs D M. Measurement of cochlear length using the ‘A’ value for cochlea basal diameter: A feasibility study. Cochlear Implants Int. 2017;18(04):226–229. doi: 10.1080/14670100.2017.1292689. [DOI] [PubMed] [Google Scholar]
- 39.Lee J, Nadol J B, Jr, Eddington D K. Depth of electrode insertion and postoperative performance in humans with cochlear implants: a histopathologic study. Audiol Neurootol. 2010;15(05):323–331. doi: 10.1159/000289571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Hochmair I, Arnold W, Nopp P, Jolly C, Müller J, Roland P. Deep electrode insertion in cochlear implants: apical morphology, electrodes and speech perception results. Acta Otolaryngol. 2003;123(05):612–617. [PubMed] [Google Scholar]
- 41.Hamzavi J, Arnoldner C. Effect of deep insertion of the cochlear implant electrode array on pitch estimation and speech perception. Acta Otolaryngol. 2006;126(11):1182–1187. doi: 10.1080/00016480600672683. [DOI] [PubMed] [Google Scholar]
- 42.Landwehr M, Fürstenberg D, Walger M, von Wedel H, Meister H. Effects of various electrode configurations on music perception, intonation and speaker gender identification. Cochlear Implants Int. 2014;15(01):27–35. doi: 10.1179/1754762813Y.0000000037. [DOI] [PubMed] [Google Scholar]
- 43.Angeli S I, Goncalves S. Predicting depth of electrode insertion by cochlear measurements on computed tomography scans. Laryngoscope. 2016;126(07):1656–1661. doi: 10.1002/lary.25742. [DOI] [PubMed] [Google Scholar]