

Abstract
One of the most understudied health disparity populations in the U.S. is the Deaf community – a sociolinguistic minority group of at least 500,000 individuals who communicate using American Sign Language. Research within this population is lacking, in part, due to researchers’ use of methodologies that are inaccessible to Deaf sign language users. Traditional qualitative methods were developed to collect and analyze participants’ spoken language. There is, therefore, a paradigm shift that must occur in order to move from an auditory data schema to one that prioritizes the collection and analysis of visual data. To effectively navigate this shift when working with Deaf sign language users, there are unique linguistic and sociopolitical considerations that should be taken into account. The current article explores these considerations and outlines an emerging method of conducting qualitative analysis that, we argue, has the potential to enhance qualitative researchers’ work regardless of the population of focus.
Keywords: Deaf, health disparities, cultural competence, social equality
Traditionally, qualitative analysis is conducted using the following approach: (1) an encounter or interview between a researcher and research participant(s) is audiotaped; (2) the audiotape is transcribed into written form by a research assistant or transcriptionist; (3) written transcripts are uploaded into qualitative analysis software; and (4) this software is used as a tool to assign qualitative codes and themes to specific portions of text. Although this method has proved successful for qualitative researchers across a number of disciplines, without some level of adaptation, it cannot be directly applied to qualitative research in which data are collected from and/or by Deaf sign language users. Rather, there are unique linguistic and sociopolitical considerations that one should take into account when working with this group. The current article explores these considerations and outlines our team’s emerging method of conducting qualitative analysis that, we argue, has the potential to enhance qualitative researchers’ work regardless of the population of focus.
Deaf Sign Language Users
In the United States, one of the most understudied populations is the Deaf community – a sociolinguistic minority group of at least 500,000 individuals who communicate using American Sign Language (ASL; Mitchell, Young, Bachleda, & Karchmer, 2006). ASL is fully distinct from English – i.e., it is not “English on the hands” – and over the past several decades, ASL has become recognized as a formal language with its own syntax, morphology, and structure (Stokoe, 2005). ASL is a natural form of language, self-expression, and communication of information among Deaf individuals in the United States. Much like spoken languages, sign languages develop according to surrounding macro- and microsystems. As a result, there are over 138 documented sign languages across the world (Simons & Fennig, 2017). Despite the fact that sign language is considered a natural language for Deaf individuals (Stokoe, 2005), historical and recent attempts to discredit sign language in favor of spoken language have occurred frequently (Ruben, 2005; Stokoe, 2005).
Health and Health Literacy of the Deaf Population
Recent findings collected using an ASL public health survey identified striking disparities in obesity, domestic violence, and suicide compared to the general population (Barnett, Klein, et al., 2011; Barnett, McKee, Smith, & Pearson, 2011). One contributing factor to these health disparities could be low levels of health literacy documented in the Deaf community – a common predictor of health outcomes. Deaf people’s median English reading level falls at approximately the fourth grade (Gallaudet Research Institute, 2003), and many present with low health literacy due to reduced incidental learning throughout the lifespan - e.g., inability to communicate with hearing parents, overhear family conversations, or understand spoken health information on TV/radio/PSAs (Pollard & Barnett, 2009; Pollard, Dean, O’Hearn, & Haynes, 2009).
Further research on the these disparities in health and health literacy is lacking due, in part, to researchers’ use of recruitment, sampling, and data collection procedures that are inaccessible to Deaf sign language users - e.g., random-digit-dial surveys, use of written materials in research protocols (Livermore, Whalen, Prenovitz, Aggarwal, & Bardos, 2011). Perhaps a more dire barrier to Deaf people’s research engagement is the disconnect between the biomedical research community and the Deaf community (McKee, Schlehofer, & Thew, 2013).
Specifically, many researchers follow a “medical model” of deafness, aiming to “cure” or “fix” hearing loss. Conversely, most Deaf people do not view themselves as disabled or as needing to be fixed, but as members of a rich culture with shared experience, history, art, and literature (Bauman, 2004; Ladd, 2003; H. Lane, 1992). This disconnect underlies a long history of mistreatment of Deaf people in the research world, including the eugenics movement that spanned the late 19th century through the 20th century. The eugenics movement historically included the sterilization of Deaf people to reduce “social burdens” and increase the health of the human species through “better breeding,” but has now evolved to Deaf people’s fears about the elimination of deafness through present-day medical technologies and genetic engineering (H. Lane, 2005; McKee et al., 2013). This shared history underlies a common feeling of mistrust toward researchers and resistance to enroll in health research.
As many of these barriers are experienced by Deaf people residing both within and outside of the United States, the remainder of our discussion will attempt to be inclusive of the international population of Deaf sign language users.
Applying Traditional Qualitative Methods to Deaf Health Research
Sign language is a visual-tactile language. This means that researchers need to adjust their framework from one that emphasizes the collection and analysis of auditory data to the collection and analysis of visual data. For data collection, such a paradigm shift means that interviews and focus groups are videotaped rather than audiotaped. While such methodological adaptions for data collection and recording appear relatively straightforward, considerations for and adjustments to the data analysis process are relatively more complex.
You may wonder, Why not just transcribe sign language videotapes into written form? The primary reason is that sign languages do not have a standardized written form (Arnold, 2016; Ruben, 2005; Stokoe, 2005). There have been numerous undertakings to create written forms of sign languages since Roche-Ambroise Auguste Bebian in 1825’s “Mimiographie” (Arnold, 2016). For instance, in 1965, Stokoe developed one of the more well-known ASL notation systems and, in recent years, SignWriting, Si5s, and ASL-phabet have also emerged as proposed writing systems. However, no written forms of any sign language have been widely adopted by the Deaf population.
As such, there is no process of written transcription for ASL that is equivalent to transcription from the spoken form of a language to the written form of that same language (e.g., spoken Spanish to written Spanish). Rather, beginning with sign language and ending with written language requires a process of translation between languages and modalities (one entirely visual/gestural with no print base, and one that is sound/print based) (Temple & Young, 2004). For the purposes of the current discussion, we use the term translation to refer to the process of “transforming research data (e.g., audiotaped interviews or documents) from one language into another” (Wong & Poon, 2010).
The process of translation is often applied in cross-cultural qualitative research when there is a language incompatibility between members of the research team and members of the target study population (e.g., Clark, Birkhead, Fernandez, & Egger, 2017). In such situations, researchers use translation as a practical tool to shape the data into a form that they can more easily understand and explore. Applied to empirical work with Deaf sign language users, a researcher whose first or primary language is English might reason: The data must be translated from ASL to written English so that I can understand what the participant is saying and analyze the data.
Such a utilitarian approach to transforming data is commonly observed within the field of Deaf qualitative health research, but is unexpected given the value that qualitative researchers generally place on the accurately capturing the content, structure, and underlying meanings of participants’ utterances (Shklarov, 2007). In addition to exploring these linguistic considerations below, we also discuss the sociopolitical implications of translating participant data between languages prior to data analysis – especially when the translation occurs from the language of an oppressed minority group (e.g., the Deaf community) to the language of the majority (e.g., the general hearing population).
Linguistic Considerations
Translation accuracy.
When translating a participant’s original message into a second language prior to qualitative data analysis, maintaining conceptual equivalence (i.e., technical and conceptual accuracy) is essential (Squires, 2009). Any omissions, oversights, misinterpretations, or additions that occur when translating research data between languages will likely “compromise the researcher’s ability to uncover certain descriptive nuances, contradictions, or paradoxes” (Wong & Poon, 2010), subsequently leading to results and conclusions that are inaccurate or invalid. Yet, translators are human. Humans err. Creating a “perfect translation” is extremely challenging, no matter how skilled, diligent, or meticulous the translation team.
The translation from a sign language into written form involves one of two possible forms of interpretation: simultaneous or consecutive interpreting. Simultaneous interpreting refers to when an interpreter begins interpreting while another person is speaking; consecutive interpreting refers to a practice when an interpreter waits until a complete thought is expressed, in order to understand the entire concept, before beginning interpretation. Research indicates that consecutive interpreting is more accurate than simultaneous interpreting; however, both forms leave room for error (Russell, 2000).
For example, achieving conceptual equivalence is especially challenging when a translation is conducted after data collection has already occurred, as there may not be an opportunity to receive feedback from participants about the accuracy of the intended message – a bi-directional check-in process that occurs fairly regularly in interactions between Deaf consumers and sign language interpreters. Moreover, a one-to-one translation may not be possible depending upon the languages one is translating between. Similar to translating between many spoken languages, certain signs, phrases, or idioms in ASL do not have sufficient counterparts in English, and vice-versa. Additionally, the structure of the participant’s language use may be altered during the translation process (Squires, 2009), a concern quite relevant for transformations between visual/signed and spoken/written modalities.
These linguistic considerations have significant implications for qualitative approaches that emphasize the importance of both the content and the structure of participants’ utterances. Together, the potential for translation error and the inherent alterations to the original message when translation occurs prior to data analysis increase the likelihood that “the investigator will not adequately capture the essence of the phenomenon in the translated language” (Squires, 2009).
Translation bias.
Just as translators are vulnerable to translation error, they are also susceptible to bias. Investigators who ascribe to the social-constructionist or feminist models of qualitative research consider the influence of the translator on the resulting translated product (Bjork Bramberg & Dahlberg, 2013; Temple, 2002), recognizing the translator as a “producer of research data who shapes the analysis” (Squires, 2009):
…As translation is a specific form of interpretation, the social positions, lived experiences, and epistemological stances of the translators have significant influence on data collection and data transformation. (Wong & Poon, 2010)
Adopting this theoretical stance, therefore, raises a number of questions. How do the translator’s identity, experiences, attitudes, and belief systems play a role in their understanding of the original message? How does this context influence their selection of vocabulary and grammatical structures? And, most importantly, when translation occurs prior to qualitative data analysis, whose data are we truly analyzing – the participant’s, the translator’s, or a fusion of both?
Given these questions, a social-constructionist or feminist stance challenges the appropriateness of hiring translators for qualitative research who may not be expert in, immersed in, or members of the culture of the population of focus, as accurate translations require both language proficiency and cultural knowledge (Larkin, Dierckx de Casterle, & Schotsmans, 2007). A related consideration “implicitly familiar to many translators is the problem of adequacy of cultural representation claimed by bilingual members of the culture” (Shklarov, 2007, p. 531). In other words, being a fluent bilingual may not be sufficient to translate material through a representative cultural lens. For example, even when translators possess both linguistic and cultural expertise, the adequacy of cultural representation might also be challenged by systematic differences between monolingual and bilingual members of a particular cultural group (e.g., age, level of education, level of acculturation to the majority group, age of exposure to sign language as a first or second language) (Shklarov, 2007).
Applied to the Deaf population, this line of reasoning might suggest that only native Deaf signers with equivalent English literacy should translate for research purposes, especially when the translation process occurs prior to data analysis. For example, if a researcher hires a hearing translator who is fluent in both ASL and written/spoken English, the resulting linguistic message is translated through a framework defined by the translator’s hearing experience and hearing culture. This in-group versus out-group issue becomes even more salient when the translator belongs to the majority group yet is performing translations on a member of an oppressed minority group, explored in more detail below.
Yet, even working with Deaf translators may present challenges, as noted above, as Deaf individuals who are bilingual ASL-English users may be inherently different from Deaf individuals who are monolingual users of ASL (e.g., more highly educated, more acculturated into the hearing majority; Grosjean, 2010) and, therefore, may unknowingly impart their own biases during the translation process. Additionally, Deaf translators who are members of majority groups may unknowingly make assumptions or misinterpret the original messages of Deaf participants with intersectional identities (e.g., Deaf People of Color, Deaf LGBTQI, DeafBlind) if methods to account for these biases are not built into the research process.
Sociopolitical Considerations
Qualitative researchers who use translation in their work must weigh the validity of their research findings against issues of translation accuracy and bias; yet, perhaps more importantly, they must also consider the sociopolitical implications of their decision to translate linguistic data, especially if this translation occurs prior to analysis of the participant’s original message (Santos, Black, & Sandelowski, 2015). Translation is a “social practice imbued with power” (Wong & Poon, 2010), particularly when study participants are members of an oppressed minority group and the researcher belongs to the majority society (e.g., Kyoon-Achan et al., 2018). Translating participants’ original utterances into the majority language may be perceived as a form of paternalism, in which the researcher is “naming and speaking for people seen as ‘other’” (Temple & Young, 2004). Members of the Deaf community are intimately familiar with such paternalism – hearing individuals’ well-meaning, but unsolicited, attempts to speak for them, help them, take care of them, and cure them (Hoffmeister & Harvey, 1996; Temple & Young, 2004), all enabling practices that have historically inhibited Deaf people’s development of empowerment and self-efficacy (Ladd, 2003; H. Lane, 1992).
By performing translations in order to more easily conduct data analysis in the majority language, the researcher renders the source language invisible and simultaneously reinforces the power of the majority language:
For its [Deaf] community of users there has been a close link between the denial of the language, and experiences of oppression and social control by those who would prefer deaf children and adults to speak. In quite literally writing out the source language, methodological expediency continues to reinforce the political invisibility of the language and its users. (Temple & Young, 2004)
Deaf people’s long and arduous history of language oppression is one of the core communal experiences that defines Deaf culture; therefore, to disregard or suppress sign language within the research process itself will likely reinforce Deaf people’s pre-existing feelings of mistrust towards medical professionals and biomedical researchers.
These sociopolitical considerations again raise concerns about potential for translator bias. When the translator is a member of the majority society – in our case, a hearing individual– it is entirely possible that the translator could subconsciously transform research data in such a way that would “reinforce social marginalization while giving a false impression of pluralism and good will” (Wong & Poon, 2010).
Applied to data collected from Deaf sign language users, these linguistic and sociopolitical considerations raise enough concern to justify the adaptation of traditional qualitative analysis methods for this unique population of focus. Below, we propose a paradigm shift in how cross-cultural qualitative research is conducted by outlining our research team’s method of qualitative data collection, analysis, and dissemination. Taking into account the concerns outlined above, our team designed a method that defers translation from ASL to English until after data analysis and interpretation have already occurred, with this translation occurring primarily for the purpose of preparing written English dissemination products to share with the general public and scientific community (e.g., research briefs, journal articles).
The method we describe is our team’s emerging best practice, which has evolved from the knowledge, experience, and unique areas of expertise of our team members. We are a relatively young team – having only come together approximately two years prior to the submission of this manuscript. Although we believe that this emerging method has the potential to benefit qualitative health research across a number of disciplines and with a wide range of populations of focus, we do not assert that this is the only way or the best way to conduct qualitative health research in the Deaf community. Rather, it is the method that we have found to be most effective and culturally-congruent based on our team’s experiences thus far.
Reforming Qualitative Methods for Deaf Health Research
How much easier it would be in cross-language research if we could understand how the participants’ own words and nuances without the need for third-party translation. Unfortunately, that is not possible. (Esposito, 2001)
Here, we argue that such a method is not only possible, but potentially more streamlined, valid, and linguistically- and culturally-congruent than research that involves translation of participant’s qualitative data prior to data analysis and interpretation.
Step 1: Formation of the Research Team
Social science researchers need to reconceptualize how cross-cultural research can be conducted despite the constraints of limited resources. Finding co-investigators or research assistants from the communities of the research interests is a viable solution. (Wong & Poon, 2010)
To work toward our objective of conducting Deaf-congruent qualitative data collection, analysis, and dissemination, we first began by cultivating a Deaf-majority research team. Six out of eight of our team members are Deaf; seven of eight are fluent in ASL.
Our principal investigator is a hearing psychologist who conducts clinical research within the Deaf community. As a hearing individual conducting Deaf-engaged research, she believes that her primary role is to provide administrative guidance and consultation on scientific methodology throughout the research process. She co-leads the team with a Deaf co-investigator, a university lecturer of Language Studies. Their collaboration began prior to the initiation of any research procedures – during the grant writing phase – to ensure that the proposed research activities would align with the priorities of the Deaf community. This collaborative leadership team is supported by another Deaf co-investigator, as well as a hearing research coordinator.
The remainder of our research team is comprised of four Deaf Community Advisors – laypersons from the Deaf community who are active members of the research team. The primary role of our Deaf Community Advisors is to guide the design of study methodology in such a way as to represent the diverse experiences, perspectives, and needs of the Deaf community. To achieve this goal, we attempted to attract a diverse cohort of Deaf community members to these positions. We started with a set of essential job qualifications – ASL fluency, expertise in Deaf cultural norms and access barriers, and ability to use a computer. Beyond these qualifications, we were mindful of creating a team diverse with respect to race/ethnicity, gender, sexual orientation, level of education, educational background (i.e., Deaf residential school, mainstream school), and socioeconomic status. In addition to these diversity factors, our selection process was also attuned to how each Deaf Community Advisor contributes a different, complementary skill set to the team – in our case, filmmaking, script writing, community outreach and networking, acting, writing, etc.
Similar to other community-engaged research teams, some of our Deaf Community Advisors had prior experience in research settings, while others had none:
In some cases, the researchers work with community members to develop a capacity-building strategy in which community members receive training on research theories and methodology; in turn, these members contribute to the project by taking on research activities such as recruitment of participants, interviews, translation, and data analysis. (Wong & Poon, 2010)
This strategy directly applies to the complementary expertise and the cross-training experiences that occur within our research team. The principal investigator provides formal training and guidance regarding research ethics, strict procedures for protecting privacy and maintaining confidentiality in a small community context, study methodology, and study-specific content knowledge. The co-investigators and Deaf Community Advisors provide the necessary linguistic and cultural expertise for development of appropriate study methodology, conduct of conceptually-accurate analysis and interpretation of data, and leveraging of effective strategies for disseminating findings back to the community.
When issues arise due to incongruences between culture and traditional empirical approaches, our team attempts to openly discuss and collaboratively decide how to manage these issues. For example, during the first phase of our current study, we conducted community forums where we invited Deaf community members to share their positive and negative experiences interacting with the research world. After these forums, many of the Certified Deaf Interpreters (CDIs) who had facilitated communication during the forums expressed a desire to share their research experiences as well; yet, their Code of Professional Conduct restricted them from stepping out of the interpreter role and stepping into a participant role during the forum. (Note: A CDI is a Deaf individual who demonstrates knowledge and understanding of interpreting, the Deaf community and culture, training/experience in use of gesture, mime, props, drawings, and other tools to enhance communication.)
At the end of the community forums, many of the CDIs approached the research team to ask if they could call us to share their experiences interacting with the research world, or if they could submit video testimonials to our team about their experiences. However, our approved research protocol allowed no such mechanisms for collecting data outside of the forums. This issue required our team to brainstorm about how we could include the valuable perspectives of these individuals, while still remaining within the scope of our approved research methodology. Ultimately, we decided that the most appropriate solution would be to hold an additional focus group during a later phase of our study, open only to CDIs.
This unanticipated modification to study methodology generated extremely rich data, but would not have occurred without the open, collaborative, solution-focused dialogue between the cultural and empirical experts on our research team. This ongoing dialogue informs our approaches to data collection, data analysis/interpretation, and dissemination of findings.
Step 2: Data Collection
There is an overwhelming sense of caution against the intrusion of the translator or distortion of information by the translator’s presence. (Shklarov, 2007)
Within the field of cross-cultural qualitative research, there is general consensus that collecting data directly in the primary language of the participant is preferred, without the presence of an interpreter or translator in the room (Shklarov, 2007). We have seen this sentiment reiterated by focus group participants in one of our studies, who expressed discomfort during past research experiences when interpreters were present during data collection, due to feeling outnumbered and/or intimidated by the number of hearing people in the room. They reported feeling especially unnerved when the interpreters’ presence was merely intended to create an audiotape that could be later used for data analysis by non-signing researchers, or to create a transcript that could be uploaded into qualitative data analysis software that only has the capability of managing text data (Temple & Young, 2004). Wherever possible, a sign-only environment is favored. Thus, our qualitative data collection efforts have included community forums and focus groups conducted directly in sign language. These activities were co-led by our hearing ASL-fluent principal investigator and a Deaf co-investigator.
Unlike traditional qualitative research conducted with hearing participants, interviews and focus groups with signing Deaf participants must be videotaped in order to accurately and fully capture data. Although this adaptation appears relatively simple, there are considerations that must be made in order to capture data in a usable form. Our research team works with a filmmaker who is an ASL-fluent, hearing Child of Deaf Adults (CODA) and who employs Deaf film assistants on his team. The team’s dual expertise in filmmaking and sign language ensures that the visual linguistic data being captured is both within the frame of the shot and in focus – common pitfalls of videographers unfamiliar with filming sign language. Additionally, the presence of the research team members and videography team in the room during data collection is less disconcerting when these individuals share a common cultural background and/or language with the research participants.
Step 3: Uploading Data into Qualitative Analysis Software
Translation, in effect, packages the data into a form that fits the tools we have for handling it. (Temple & Young, 2004)
Upon completion of sign language data collection, many researchers opt to translate sign language data into text. One of the primary motivations for creating text transcripts is that many qualitative analysis tools have historically relied on data mining of text. Fortunately, tools have become available that offer new possibilities for data analysis.
When selecting a qualitative analysis software package, it is critical to select a tool that allows for importing video. Additionally, the software must have the capability to insert qualitative codes directly on the video using timestamps. Qualitative software that advertise these capabilities include ATLAS.ti, ELAN, and Transana, although there are likely other options available as well.
To upload video of an individual interview or other data collection effort that requires only one camera angle is relatively simple. However, additional considerations must be made for data collected from focus groups or community forums, in which multiple video streams are recorded in order to capture all participants simultaneously. In our work, when multiple video streams are available, our filmmaker creates a “master” video that integrates all camera angles, including one enlarged view of primary signer, as well as a running time stamp (see Figure 1 below; Note: portions of the image are blurred to protect participant identities). Integrating all camera angles into a single video streamlines the data analysis process, yet our team still has access to the original, individual videos for situations when we may need more in-depth, or zoomed-in, analysis to fully comprehend a participant’s statements.
Figure 1.
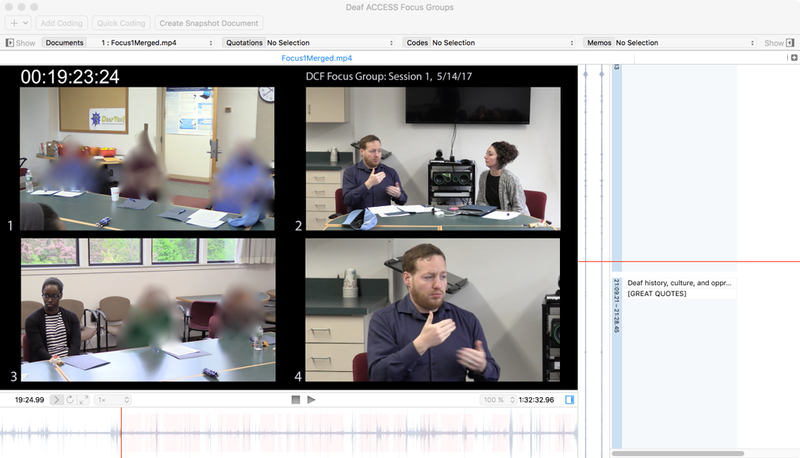
Screenshot of focus group qualitative data in ATLAS
Step 4: Data Analysis and Interpretation
The situation where the researcher is fluent in the language of communities she is working with is rare. It offers opportunities in terms of research methods that are not open to other researchers in cross language research…However, it is increasingly recognized that the insider/outsider boundaries cannot be as easily drawn. (Temple & Young, 2004)
Now that video data is uploaded into the appropriate data analysis software, our team is ready to create our qualitative code book and begin tagging codes onto the master video. As noted in the quote above, our research team faces a unique situation in which the primary investigator is ASL-fluent, but an out-group member – a member of the majority hearing community. While this has allowed her to be involved directly in data collection with Deaf participants, there are implications for the data analysis process that our team has had to consider. Specifically, the potential influence of the principal investigator’s majority culture bias on the interpretation of Deaf participants’ utterances. Additionally, the Deaf community members on our team may bring their own biases and preconceptions into data collection and analysis – e.g., unconsciously misinterpreting experiences of Deaf participants with intersectional identities, minimizing findings that may not be flattering to the Deaf community, or overlooking themes that represent commonplace experiences for Deaf people and may, therefore, be taken for granted during the data analysis process.
To try to avoid introducing such biases into the interpretation of our findings, our team applies a collaborative approach to analyzing data. We develop the qualitative code book and conduct coding together as a group - “Mutuality of the process is key: openly negotiating meanings with the participants and academic audiences, as a way of sharing power, can help prevent misunderstandings” (Shklarov, 2007). Sometimes the team unanimously agrees about how to classify a participant’s statement; sometimes the team disagrees. In instances of disagreement, there is a group dialogue about the particular inconsistency, with increased credence given to the Deaf members of the team in recognition that they are the team’s experts at interpreting sign language data in a Deaf cultural context.
Step 5: Dissemination of Findings to the Deaf Community
How will your research help us? It won’t! We’ve been trying so hard and struggling for such a long time…It will help your job and you will get paid, but how will that help us? You want us to share our experiences and use it to your personal benefit, but will not help us at all! (Anonymous Deaf community forum attendee)
As can be seen in the quote above, the topic of dissemination was of utmost importance to attendees at the Deaf community forums hosted by our research team. Participants reported feeling tired of researchers entering their community, asking them to provide data, and then disappearing, never to be heard from again and failing to give back to the community in any meaningful or tangible way. To ignore these mounting complaints of the Deaf community would only result in a subsequent loss of our ability to engage Deaf people in future research endeavors – both as collaborators and as participants. Accordingly, once our data is analyzed and interpreted, our team has made it a priority to first disseminate a summary of findings back to our participants and to the Deaf community.
To facilitate this objective, our research team is fortunate to be housed within the Systems and Psychosocial Advances Research Center (SPARC) at UMass Medical School, a research center that prioritizes community-engaged research and the dissemination of research findings back to key stakeholders and the lay community (http://www.umassmed.edu/sparc/). SPARC’s ongoing dissemination activities include a number of open-access products intended for use by general audiences – Psychiatry Information Briefs, Research in the Works, and Tip Sheets, to name a few. The goal of each of these products is to keep the community informed of SPARC’s work, including research findings that are relevant to their own health and wellbeing.
To adapt this dissemination process for Deaf ASL users, when our research team has created a SPARC dissemination product thus far, we have filmed a parallel ASL version. Both the ASL and written English versions are disseminated via our research team’s Facebook page and website, with the goal of keeping the Deaf community apprised of our progress throughout each research study and aware of any results that might impact their lives (see Figure 2).
Figure 2.
Screenshot of ASL research brief disseminated via Facebook
Step 6: Dissemination of Findings to the Scientific Community
The decision to delay translation into English for as long as possible may be based on a political recognition of the ontological importance for people of their first language and the implications of colluding, through early translation, with the invisibility of some languages and their users. (Temple & Young, 2004)
The final stage of our team’s qualitative research process is to prepare our findings for publication in a peer-reviewed, scientific journal. Our team attempts to delay translating data from the source sign language into text as long as possible in this process. We employ this approach in order to respond to concerns raised by the linguistic and sociopolitical considerations outlined at the beginning of this article.
When it comes time to translate from sign language to text, we generally do so only for salient participant statements that we intend to include as direct quotes in our written English publications – not the entirety of our dataset. The translations are guided by the Deaf members of our team – specifically, our Deaf Community Advisors – who serve not only as linguistic experts, but also cultural brokers, as the data transforms from ASL to written English:
If we acknowledge the final product of translation as a distinct creation, then it is important for the research team to develop an understanding of what has been changed, gained, or lost through the process of translation. This can be achieved through open dialogue, in which translators are not regarded as mechanistic task performers but as research associates who participate in data analysis and interpretation. (Wong & Poon, 2010)
A prime example of this phenomenon (i.e., open dialogue about what has been changed, gained, or lost through the process of translation) occurred during our team’s attempts to translate the quote located under Step 5 of the current manuscript. When we first attempted to translate this participant’s statement from sign language to English, our team recognized that the participant was not using a standard form of ASL that any of us could readily understand, but rather a contact language that had developed from this individual’s combined knowledge of ASL and a formal sign language from another country. We then reviewed video footage of the CDI’s real-time interpretation of the participant’s statement – a CDI who fortunately happened to be a bilingual user of the same two sign languages used by the participant. We initially created a translation of the CDI’s interpretation, but upon repeated comparison with the original statement and ongoing team dialogue, we realized that the CDI had introduced a significant portion of new content that could not be attributed to the data originally provided by the participant. Without this open dialogue during the translation process, our team could have potentially accepted a translation that included content not provided by the research participant.
The Deaf Community Advisors’ role becomes even more critical in ensuring the accuracy and appropriateness of this translation process given the role confusion that can arise when the leaders of the research team (i.e., the principal investigator and co-investigators) also serve as translators of their own dataset:
The double role of a bilingual researcher-translator can carry even greater power than the role of a neutral translator, because the former is associated with a perceived air of a ‘monopoly’ on interpreting his or her own research findings. The position of power might result in situations of mistrust, especially when the meanings of central concepts are arguable. (Shklarov, 2007)
By establishing a Deaf-community-engaged team at the outset of our work, emphasizing open dialogue, and utilizing collaborative decision-making, our research team leaders attempt to navigate around such pitfalls.
Limitations of Our Qualitative Method
Above, we intentionally describe our attempts to develop an ideal method of qualitative data collection, analysis, and dissemination, as we are aware that there are remaining considerations for and limitations to our approach. For example, the use of video data raises additional concerns about anonymity and confidentiality. A researcher cannot “scrub” identifying information from a videotape as one can redact a written transcript. To blur a participant’s facial features to the point of anonymity would result in the loss of data present in facial expressions (i.e., facial grammar and other non-manual markers or non-manual signals) – one of the distinct advantages of our method. Such confidentiality concerns substantially increase the researcher’s responsibility to store video data with more-than-adequate protections – e.g., password-protected digital video files stored on secure servers or password-protected hard drives, physical video materials stored in locked drawers in locked offices, etc.
We also recognize that additional challenges can arise when individuals from small, close-knit communities collect data from within their own community. In our case, the presence of other in-group members may reduce the depth of Deaf participants’ personal disclosure due to inherent lack of anonymity and fear of confidentiality breaches. Or, the presence of a Deaf research team member who has multiple roles in the community (e.g., advocacy, leadership) may unconsciously prompt participants to respond in a certain way that would not have occurred with a researcher who was previously unknown to the community.
Our approach thus far is also potentially limited by the involvement of a hearing researcher in the data collection process. Our community forums and focus groups have been co-led by our hearing ASL-fluent principal investigator and Deaf co-investigator. While this approach was selected to model the potential of Deaf-hearing collaboration in the research world, our decision may have influenced the data being collected. For example:
To function in a predominantly hearing society, Deaf people make enormous adaptations to be understood and to understand. These often include modifying their BSL [British Sign Language] to include a range of English grammar constructions (and in some cases with added vocalizations) in order for hearing signers to understand better…Therefore, whilst from the hearing researcher/translator perspective, doing away with mediated communication (through an interpreter) might give rise to more direct, comfortable, and elaborated data, from the Deaf respondents’ perspective it might equally give rise to constrained expression to someone with whom a different kind of signing is required, including in some cases a collusion with a modality that is constructed as politically more powerful and for some inherently oppressive. (Temple & Young, 2004)
Additionally, our method is not fully conducted in the source language, given that qualitative codes must still rely on written words or phrases. Although available software has the capability to handle video data, it does not yet have the capability for a video-based code book. Therefore, our team must enter qualitative codes in written English. Sometimes, our team finds it difficult to assign a suitable English phrase to the ASL code that we would prefer to use. Sometimes we attempt to use ASL-gloss for coding; however, we are nonetheless limited to using a text-based coding language by our available software.
Given these complex considerations, our research team will seek to continue to modify our approach to better reflect an “emancipatory epistemological position that can only be fulfilled by the Deaf research/translator who shares the common culture of those researched” (Ladd, 2003, as cited in Temple & Young, 2004) – i.e., qualitative health research conducted via Deaf community-engaged methods.
Strengths of Our Qualitative Method
We believe that our adapted method of qualitative analysis has a number of advantages over traditional qualitative methods. In terms of practicality, uploading video into qualitative analysis software and directly analyzing themes present within sign language source data removes one full step from the analysis process – transcription into text – which is often time-consuming and costly. In terms of validity, coding a participant’s original utterance is more likely to produce accurate results than coding a second- or third-hand version of the message that has been translated by interpreters or transcriptionists, even when these individuals are quite skilled. Additionally, analyzing video footage allows the research team to code both linguistic data (i.e., sign language, facial grammar and other non-manual linguistic markers) and other non-linguistic visual data (i.e., body language, facial expression). Such subtext is captured more readily with video data than when reviewing audiotapes or reading transcripts.
These advantages are not unique to data collected from Deaf sign language users. For example, sign languages are not the only languages without a standardized writing system. Out of 7,099 living languages, only 3,866 have a developed writing system (Simons & Fennig, 2017) that can be leveraged for transcription to text. Additionally, regardless of the language used for data collection, there is always the possibility that transcriptionists could make errors when creating a text transcript. Qualitative analyses with hearing individuals may also miss important subtextual information if visual or auditory cues are not captured during the transcription process. And, any researcher could benefit from eliminating a tedious, expensive step from their methodological approach. It is, therefore, our opinion that the presented method of collecting and analyzing video qualitative data could potentially benefit researchers conducting studies in a number of disciplines with a wide range of populations of focus.
For research conducted within our population of focus and with members from other sociolinguistic minority populations, our approach is also an attempt to model how to conduct qualitative work in a way that is increasingly sensitive to the unequal power dynamics between researchers and research participants, the unequal power dynamics between the oppressor and the oppressed, and the unequal power dynamics between majority and minority languages, as well as languages without a standardized writing system. Through our work, we are attempting to reform traditional research methodology to more authentically represent the experiences and perspectives of our population of focus; we try to avoid automatic acceptance of traditional methods that would otherwise force our population of focus to adapt to the academic world.
Funding
This work was supported by the National Institute on Deafness and Other Communication Disorders of the National Institutes of Health [Award Number R21DC015580]. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Footnotes
Declaration of Conflicting Interests
The Authors declare that there is no conflict of interest.
Contributor Information
Melissa L. Anderson, Systems and Psychosocial Advances Research Center (SPARC), Department of Psychiatry, University of Massachusetts Medical School, Worcester, MA.
Timothy Riker, Center for Language Studies, Brown University, Providence, RI..
Kurt Gagne, Systems and Psychosocial Advances Research Center (SPARC), Department of Psychiatry, University of Massachusetts Medical School, Worcester, MA..
Stephanie Hakulin, Systems and Psychosocial Advances Research Center (SPARC), Department of Psychiatry, University of Massachusetts Medical School, Worcester, MA..
Todd Higgins, Systems and Psychosocial Advances Research Center (SPARC), Department of Psychiatry, University of Massachusetts Medical School, Worcester, MA..
Jonah Meehan, Systems and Psychosocial Advances Research Center (SPARC), Department of Psychiatry, University of Massachusetts Medical School, Worcester, MA..
Elizabeth Stout, Systems and Psychosocial Advances Research Center (SPARC), Department of Psychiatry, University of Massachusetts Medical School, Worcester, MA..
Emma Pici-D’Ottavio, Systems and Psychosocial Advances Research Center (SPARC), Department of Psychiatry, University of Massachusetts Medical School, Worcester, MA..
Kelsey Cappetta, Systems and Psychosocial Advances Research Center (SPARC), Department of Psychiatry, University of Massachusetts Medical School, Worcester, MA..
Kelly S. Wolf Craig, Systems and Psychosocial Advances Research Center (SPARC), Department of Psychiatry, University of Massachusetts Medical School, Worcester, MA..
References
- Arnold RA (2016). Sign writing. In Gertz G & Boudreault P (Eds.), The SAGE deaf studies encyclopedia. Thousand Oaks, CA: SAGE Publications Ltd. [Google Scholar]
- Barnett S, Klein JD, Pollard RQ Jr., Samar V, Schlehofer D, Starr M, … Pearson TA (2011). Community participatory research with deaf sign language users to identify health inequities. American Journal of Public Health, 101(12), 2235–2238. doi: 10.2105/AJPH.2011.300247 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barnett S, McKee M, Smith SR, & Pearson TA (2011). Deaf sign language users, health inequities, and public health: opportunity for social justice. Preventing Chronic Disease, 8(2), A45. [PMC free article] [PubMed] [Google Scholar]
- Bauman HD (2004). Audism: exploring the metaphysics of oppression. Journal of Deaf Studies and Deaf Education, 9(2), 239–246. doi: 10.1093/deafed/enh025 [DOI] [PubMed] [Google Scholar]
- Bjork Bramberg E., & Dahlberg K (2013). Interpreters in cross-cultural interviews: a three-way coconstruction of data. Qual Health Res, 23(2), 241–247. doi: 10.1177/1049732312467705 [DOI] [PubMed] [Google Scholar]
- Clark L, Birkhead AS, Fernandez C, & Egger MJ (2017). A Transcription and Translation Protocol for Sensitive Cross-Cultural Team Research. Qual Health Res, 27(12), 1751–1764. doi: 10.1177/1049732317726761 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Esposito N (2001). From meaning to meaning: the influence of translation techniques on non-English focus group research. Qual Health Res, 11(4), 568–579. doi: 10.1177/104973201129119217 [DOI] [PubMed] [Google Scholar]
- Gallaudet Research Institute. (2003). Literacy and deaf students. Retrieved from http://gri.gallaudet.edu/Literacy/-reading
- Grosjean F (2010). Bilingualism, biculturalism, and deafness. International Journal of Bilingual Education and Bilingualism, 13, 133–145. doi: 10.1080/13670050903474051 [DOI] [Google Scholar]
- Hoffmeister R, & Harvey M (1996). Is there a psychology of the hearing? In Glickman NS & Harvey M (Eds.), Culturally affirmative psychotherapy with deaf persons (pp. 73–98). Hillsdale, NJ: Lawrence Erlbaum Associates. [Google Scholar]
- Kyoon-Achan G, Lavoie J, Avery Kinew K, Phillips-Beck W, Ibrahim N, Sinclair S, & Katz A (2018). Innovating for Transformation in First Nations Health Using Community-Based Participatory Research. Qual Health Res, 1049732318756056. doi: 10.1177/1049732318756056 [DOI] [PubMed] [Google Scholar]
- Ladd P (2003). Understanding deaf culture: In search of deafhood. Tonawanda, NY: Multilingual Matters. [Google Scholar]
- Lane H (1992). The mask of benevolence: Disabling the deaf community. New York, NY: Alfred A. Knopf, Inc. [Google Scholar]
- Lane H (2005). Ethnicity, ethics, and the deaf-world. J Deaf Stud Deaf Educ, 10(3), 291–310. doi: 10.1093/deafed/eni030 [DOI] [PubMed] [Google Scholar]
- Larkin PJ, Dierckx de Casterle B, & Schotsmans P (2007). Multilingual translation issues in qualitative research: reflections on a metaphorical process. Qual Health Res, 17(4), 468–476. doi: 10.1177/1049732307299258 [DOI] [PubMed] [Google Scholar]
- Livermore G, Whalen D, Prenovitz S, Aggarwal R, & Bardos M (2011). Disability data in national surveys: Prepared for the Office of Disability, Aging and Long-Term Care Policy. Retrieved from https://aspe.hhs.gov/basic-report/disability-data-national-surveys:
- McKee M, Schlehofer D, & Thew D (2013). Ethical issues in conducting research with deaf populations. Am J Public Health, 103(12), 2174–2178. doi: 10.2105/AJPH.2013.301343 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mitchell R, Young T, Bachleda B, & Karchmer M (2006). How many people use ASL in the United States? Why estimates need updating. Sign Language Studies, 6, 306–335. doi: 10.1353/sls.2006.0019 [DOI] [Google Scholar]
- Pollard RQ, & Barnett S (2009). Health-related vocabulary knowledge among deaf adults. Rehabilitation Psychology, 54(2), 182–185. doi: 10.1037/a0015771 [DOI] [PubMed] [Google Scholar]
- Pollard RQ, Dean RK, O’Hearn A, & Haynes SL (2009). Adapting health education material for deaf audiences. Rehabilitation Psychology, 54(2), 232–238. doi: 10.1037/a0015772 [DOI] [PubMed] [Google Scholar]
- Ruben RJ (2005). Sign language: its history and contribution to the understanding of the biological nature of language. Acta Otolaryngol, 125(5), 464–467. doi: 10.1080/00016480510026287 [DOI] [PubMed] [Google Scholar]
- Russell DL (2000). Interpreting in legal contexts: Consecutive and simultaneous interpreting. (Unpublished doctoral dissertation), University of Calgary, Calgary, Alberta, Canada. [Google Scholar]
- Santos HP Jr., Black AM, & Sandelowski M (2015). Timing of translation in cross-language qualitative research. Qual Health Res, 25(1), 134–144. doi: 10.1177/1049732314549603 [DOI] [PubMed] [Google Scholar]
- Shklarov S (2007). Double vision uncertainty: the bilingual researcher and the ethics of cross-language research. Qual Health Res, 17(4), 529–538. doi: 10.1177/1049732306298263 [DOI] [PubMed] [Google Scholar]
- Simons GF, & Fennig CD (2017). Ethnologue: Languages of the world, 20th edition Retrieved November 20, 2017, from SIL International; Online version: http://www.ethnologue.com/ [Google Scholar]
- Squires A (2009). Methodological challenges in cross-language qualitative research: a research review. Int J Nurs Stud, 46(2), 277–287. doi: 10.1016/j.ijnurstu.2008.08.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stokoe WC Jr. (2005). Sign language structure: an outline of the visual communication systems of the American deaf. 1960. J Deaf Stud Deaf Educ, 10(1), 3–37. doi: 10.1093/deafed/eni001 [DOI] [PubMed] [Google Scholar]
- Temple B (2002). Crossed wires: interpreters, translators, and bilingual workers in cross-language research. Qualitative Health Research, 17(10), 1372–1380. doi: 10.1177/104973230201200610 [DOI] [PubMed] [Google Scholar]
- Temple B, & Young A (2004). Qualitative research and translation dilemmas. Qualitative Research, 4(2), 161–178. doi: 10.1177/1468794104044430 [DOI] [Google Scholar]
- Wong JP, & Poon MK (2010). Bringing translation out of the shadows: translation as an issue of methodological significance in cross-cultural qualitative research. J Transcult Nurs, 21(2), 151–158. doi: 10.1177/1043659609357637 [DOI] [PubMed] [Google Scholar]