

Abstract
Damage control surgery (DCS) consists of three steps: an abbreviated initial operation, resuscitation in the ICU, and a planned reoperation. Although DCS for lung and heart injury have been established, there is no concept of DCS for the chest wall. We experienced a successful case, in which a DCS of chest wall lifting procedure and internal pneumatic stabilization were performed on the flail chest accompanied by a remarkable destruction of chest wall. As a result, the patient's abnormal breathing improved. Surgical fixations using KANI plate were performed at a later date. We suggest that the chest wall lifting procedure may be suitable as a DCS for thoracic cage destruction from severe chest wall injury.
Keywords: Damage control surgery, Thoracic wall destruction, Rib fracture, Surgical stabilization
Introduction
Damage control surgery (DCS) consists of three steps; an abbreviated initial operation, resuscitation in the ICU, and a planned reoperation. Although DCS has been established as a treatment for lung and heart injuries, there has been no concept of DCS for the chest wall. We experienced a successful case, in which a DCS of chest wall lifting procedure and internal pneumatic stabilization were performed on a destructive flail chest that was accompanied by a remarkable collapse of the chest wall.
Case
A previously healthy 58-year-old man sustained an injury due to a hit by a combine harvester that hurtled down a slope onto his chest. After he was diagnosed with left flail chest and tension pneumothorax in prehospital, a tracheal intubation and chest drain were performed, and he was transported to our trauma center by medical helicopter. The chest X-ray revealed a collapsed left lung on arrival (Fig. 1), and then another chest drain was further inserted from the left anterior chest. With palpation, the partial chest wall was defected; therefore, heart beating was directly palpable during the procedure. All left ribs were fractured, and flail segments were composed of the left 3rd to 10th ribs. The chest CT scan revealed that the rib cage of the left anterior chest was partially defected, as the fifth rib dropped into the thoracic cavity (Fig. 2a). Since the fractured rib edges were just about to pierce the heart, these fractures conferred a risk of cardiac penetration. The left lung was markedly collapsed, even after application of the thoracic drain, and bilateral pneumothorax and mediastinal emphysis were observed (Fig. 2b). ST elevation at V2–V6 in the ECG, and elevation of myocardial enzymes, including CK (1018 U/L), CK–MB (10.8 U/L), and TNI (0.84 ng/mL) were observed as markers of cardiac injury due to the fractured fifth rib. The therapeutic strategy for a flail chest generally involves stabilization of the flail segments using positive pressure ventilation under tracheal intubation. However, in this case, since the deformity of the chest wall was extremely severe and diagnosed as “chest wall destruction,” it was necessary to improve the physiological abnormalities, such as the withdrawal from ventilation failure and avoidance of cardiac damage due to fractured ribs. Therefore, the chest wall lifting technique as a resuscitative surgery was performed in the emergency room. This procedure provided a temporary reconstruction of the chest wall. The chest wall was rebuilt by raising the dorsal end of the fifth rib fracture into the skin with a thread, to promptly improve the physiological abnormality. After the temporary chest wall stabilization was performed, we continued respiratory management in the ICU. On day 12 after the surgical stabilization using a rib fixation plate (KANI®, USCI, Tokyo, Japan; Fig. 3), the patient could be weaned off from the ventilator. The subsequent clinical course of the patient was uneventful, the patient (injury severity score, ISS 30) was discharged on day 69 of admission.
Fig. 1.
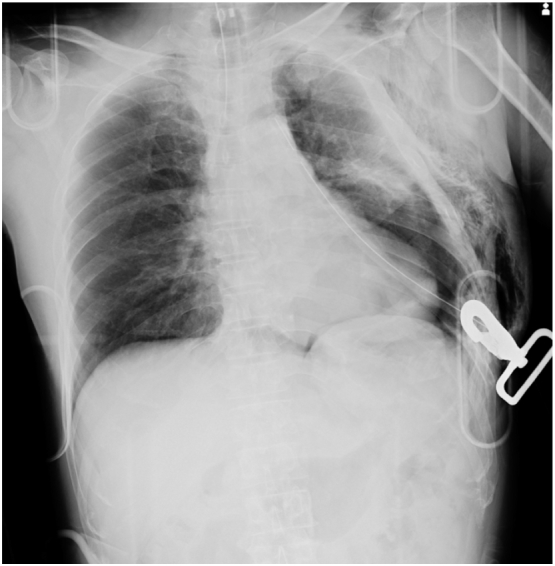
Chest X-ray findings showed remaining pneumothorax after insertion of the chest drain, left rib cage deformity, and left lung contusion.
Fig. 2.

(a) Sagittal chest CT findings revealed that all left ribs were fractured, and the fractured ribs between third and tenth formed the flail segment. The rib cage of the left anterior chest was defected, as the fifth rib dropped into the thoracic cavity (see arrow). (b) Axial chest CT findings showed that the bilateral lung markedly collapsed, even after the additional insertion of the chest drain, and mediastinal emphysema was recognized.
Fig. 3.

(a) Chest wall 3D-CT after the temporary chest wall stabilization on admission. (b) Chest 3D-CT 5 months after the surgical procedure, using a rib fixation plate (the 5-7th ribs).
Discussion
DCS is a widely acceptable strategy for severe abdominal trauma. Although the principles of damage control for abdominal injuries have been successfully applied to vascular and orthopedic trauma, several factors have hindered the wider application to thoracic injury. The first has been the concern that cardiac tamponade or hypoventilation may result from packing the pleural space. Second, a clear definition is lacking [1]. On the other hand, Gonçalves et al. indicated that situations involving DCS in the chest wall could be divided into the control of parietal bleeding and the temporary closure of the chest wall. The temporary closure (abbreviated thoracotomy) has been reported in two situations, including a thoracic packing for coagulopathy and a restriction of heartbeats due to wall closing [2,3]. However, there has been no concept of DCS for the chest wall, especially unstable thoracic cage injuries. A flail chest is a severe and critical physiological injury, that must be improved immediately in the emergency department. Therefore, chest wall stabilization against a flail chest can include the concept of damage control.
In our case, the flail chest was resistant to treatment, despite tracheal intubation, and the temporary surgical chest wall fixation led to respiration stabilization on CT findings and improved the patient's clinical course. Furthermore, the temporary chest wall fixation improved respiration and prevented cardiac penetration. This result indicates that the inclusion of damage control improves physiological conditions. Therefore, we suggest that the chest wall lifting technique provides an abbreviated surgery for chest wall destruction.
In addition, surgical rib fixation with a claw-type titanium plate was performed for flail chest 12 days after admission. This surgical fixation technique could be applied in a short time, and it is simple, convenient, and less invasive. Also, Tanaka et al. proved that this plate could be applied without any pleural injury and preserved intercostal muscle function [4]. On the other hand, the disadvantage of this plate is the appearance of artifacts in CT scan. As a result, the patient could be shortly weaned off from the ventilator. It was suggested that this operation might be an effective technique that can progress granulation formation, and adhesion of the surgical site progressed without thoracotomy. In a previous study, the surgical fixation group had shorter mechanical ventilation time compared with the conservative treatment group [5]. This finding suggest that the operation should have been performed earlier.
Caragounis et al. suggested that the final outcome of surgery cannot be assessed before 1 year post-operatively, because patients with multiple rib fractures and flail chest show a gradual improvement in symptoms, quality of life, mobility, disability, and lung function over one year post surgery [6]. In our case, long term observation was also necessary to prove the effectiveness of this procedure.
Conclusion
We propose that the three steps treatment technique that consists of chest wall lift, intensive care, and surgical procedures using a rib fixation plate is a suitable “damage control surgery” for patients with chest wall destruction and a severe flail chest (Table 1).
Table 1.
Damage control surgery for unstable thoracic cage injuries.

Acknowledgments
Acknowledgments
There are no sources of funding to declare.
Conflicts of interest statement
There are no conflicts of interests to declare by any of listed authors.
References
- 1.O'Connor J.V., DuBose J.J., Scalea T.M. Damage-control thoracic surgery: management and outcomes. J. Trauma Acute Care Surg. 2014;77(5):660–665. doi: 10.1097/TA.0000000000000451. [DOI] [PubMed] [Google Scholar]
- 2.Gonçalves R., Saad R., Jr. Thoracic damage control surgery. Rev. Col. Bras. Cir. 2016;43(5):374–381. doi: 10.1590/0100-69912016005017. [DOI] [PubMed] [Google Scholar]
- 3.Vargo D.J., Battistella F.D. Abbreviated thoracotomy and temporary chest closure: an application of damage control after thoracic trauma. Arch. Surg. 2001;136(1):21–24. doi: 10.1001/archsurg.136.1.21. [DOI] [PubMed] [Google Scholar]
- 4.Tanaka H., Yukioka T., Yamaguti Y. Surgical stabilization of internal pneumatic stabilization? A prospective randomized study of management of severe flail chest patients. J. Trauma. 2002;52:727–732. doi: 10.1097/00005373-200204000-00020. [DOI] [PubMed] [Google Scholar]
- 5.Schuurmans J., Goslings J.C., Schepers T. Operative management versus non-operative management of rib fractures in flail chest injuries: a systematic review. Eur. J. Trauma Emerg. Surg. 2017;43(2):163–168. doi: 10.1007/s00068-016-0721-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Caragounis E.C., Fagevik Olsen M., Pazooki D., Granhed H. Surgical treatment of multiple rib fractures and flail chest in trauma: a one-year follow-up study. World J Emerg Surg. 2016;11:27. doi: 10.1186/s13017-016-0085-2. [DOI] [PMC free article] [PubMed] [Google Scholar]