

Abstract
AIM:
To safely perform angioplasties in acute coronary syndromes with low contrast volume using Cordis 6F diagnostic catheters and to perform mechanical bench tests on the diagnostic and guide catheters in a radial path model.
METHODS:
In 191 patients (242 lesions/268 stents) with acute coronary syndromes angioplasty were performed with cordis 6F diagnostic catheters.
RESULTS:
The lesions were present at left anterior descending (121), Left main (5), left circumflex (51), ramus (5) and right coronary artery (60). In 72% of cases, Iodixanol was used. All contrast injections were given by hand. Regular follow-up of the patients was performed at 30 days. The procedures were performed in the femoral route only. Pre-dilatation was performed in 43 cases. Successful revascularization of the target lesion was achieved in all cases. The mean contrast volume used per patient was 28 ml (± 8 ml). Mild reversible contrast-induced nephropathy (CIN) was observed in two patients. Cardiogenic shock was seen in 7 cases, and one death was observed. Pushability and trackability tests showed good force transmission and hysteresis in diagnostic catheters compared to guide catheters.
CONCLUSIONS:
Angioplasty with stenting could be performed safely in patients using cordis 6F diagnostic catheters using a low volume of contrast in acute coronary syndromes. Low contrast volume usage would result in a lower incidence of contrast-induced nephropathy and cardiac failures.
Keywords: Low contrast volume, Acute coronary syndromes, Diagnostic catheter, Contrast-induced nephropathy, Angioplasty with stenting
Introduction
Angioplasties in acute coronary syndromes (ACS) are challenging, and these procedures are associated with higher morbidity and mortality than elective procedures. Longer procedural times, higher contrast usage, deranged renal parameters and bleeding risk commonly add to the complications in addition to the primary cardiac problems. Hence, minimising these will greatly improve the outcome of the procedure. Contrast-induced nephropathies, as well as contrast related problems, add to complications gambit. Contrast-induced nephropathy is common, and the incidence is about 7 to 10% in primary angioplasties and about 5 to 10% in routine angioplasties [1], [2], [3]. Long-term kidney injuries are frequent in patients with contrast-induced nephropathy [4], [5], [6]. Contrast media are known to have direct cytotoxicity on human kidney cells in vitro evaluation [7].
Some studies [8], [9], [10], [11] have shown higher contrast requirement in radial procedures, or at least it is equal volumes in femoral and radial [11]. Also, the radial routes are known to have increased radiation dosage to patients and the physicians [12], [13]. Contrast agents are also associated with thrombotic and bleeding manifestations, which was observed in various studies [14], [15], [16], [17], [18]. They are well known to induce platelet degranulation [19]. Also, they can induce renal apoptosis and thereby cause chronic renal failure [20]. This is a report of angioplasty in 191 cases with acute coronary syndromes, which were performed with minimal contrast volume to achieve a higher clinical success of the patients using 6F Cordis diagnostic catheters.
Methods
In the initial part of the study, diagnostic catheters were used to perform angioplasty when guide catheters failed to engage in the same patients [21]. Subsequently, when the technique was improved in high-risk patients with acute coronary syndromes, the angioplasty procedures were performed with Cordis 6F Infiniti diagnostic catheters itself.
Angioplasty and stents
In 191 patients’ angioplasty with stenting was performed by this technique using 6F diagnostic (Cordis) catheters, and 268 stents were deployed from June 2016 to May 2017. During this period 265 angioplasties were performed in total. The lesions (242) included left anterior descending (121), Left main (5), left circumflex (51), ramus (5) and right coronary artery (60) lesions, and in total 268 stents were used. A variety of coronary stents from various standard companies were used in the procedures. Cardiogenic shock was seen in seven cases. The aim was to reduce contrast-induced nephropathy as well as hemodynamic problems and cardio-renal syndromes. In 72% of cases, Iodixanol was used. All injections were given by hand only. Regular follow-up of the patients was performed at 30 days. All the procedures were performed through the femoral route only. All procedures were performed in Siemens Axiom Artis cardiac catheterisation lab, and the images were acquired at a frame rate of 15 frames/s. Pressure tracings were monitored during the procedure though there was mild dampening the pressure tracings were visible (Figure 1).
Figure 1.

Pressure tracings show the pressure waveforms during angioplasty using a diagnostic catheter. Panel A showed the pressure tracings when a left anterior descending artery lesion was wired. Panel B showed pressure tracings when the stent was being deployed. Panel C showed the pressure tracings from right coronary when a different stent was used for right coronary lesion
Pre-dilatation was performed in 43 cases with 57 lesions using 74 balloons (semi-compliant 2 mm x 10 mm and lesser sizes) and in 4 cases, 2.5 x 10 mm and in two patients 3 x 10 mm. In 5 cases short balloons (1.25 x 6 mm or 1.5 x 6 mm) were used with wires to cross the lesions though inflations were not given. For the procedures pre-dominantly floppy wires (Allstar or run through) or balanced middle-weight (BMW) wires were used.
Smaller balloon sizes were chosen to minimise the risk of coronary dissections and severe coronary spasms, which would deem further procedure difficult. The stent deployments were usually at 14 to 16 atm (Figure 2).
Figure 2.
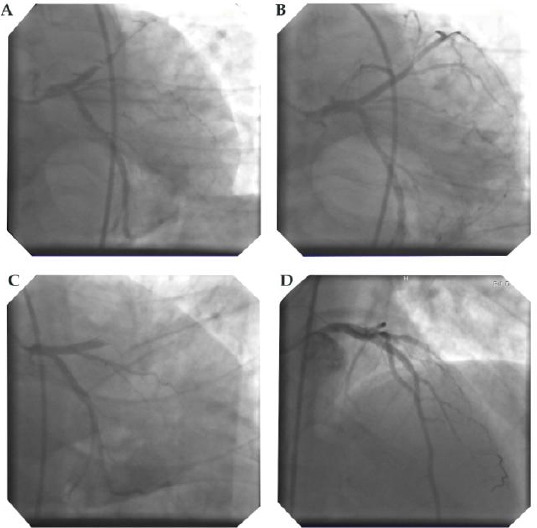
Shows angioplasties and proximal left anterior artery stent deployments. Panels A and B show stenting to proximal LAD with near total occlusion and Panels C and D show stenting to proximal LAD with complete occlusion
Two inflations were given for 5 to 7 seconds with a time interval of about 5 to 10 seconds of deflation, which is the user routine in all the cases. High-pressure deployments (> 16 atm.) were used in only 6 cases. Post-dilatation with the semi-compliant balloons was used in 5 cases only.
In cases with difficulty in wire crossing, balloon-assisted wire crossing was performed, wherein the balloon and wire were taken to the tip, and with gentle manipulation, the wire crosses the lesion. The length of the stents varied from 8mm to 28 mm and the diameter of the stent varied from 2.25 mm to 4.0mm. IVUS and OCT were not performed in these cases. Five patients underwent coronary artery bypass grafting in the past, and stenting was performed in the native vessels (Figure 3). Buddy wires were used in four cases for deployment of the stents.
Figure 3.
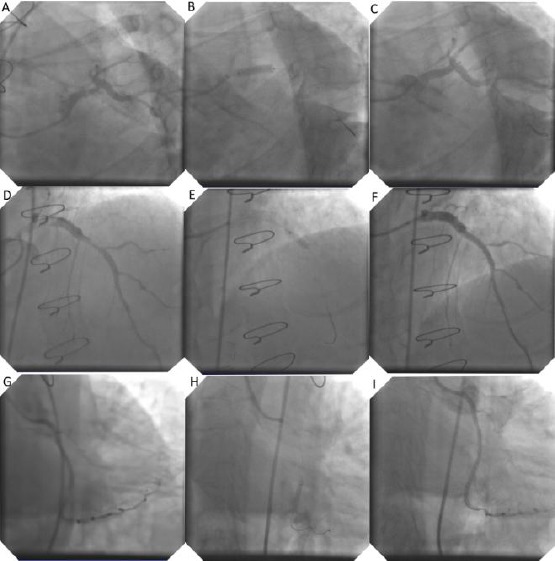
Stenting in patients who underwent coronary artery bypass grafting in the past. Panels A to C show stenting from LMCA to proximal LAD, Panels D to F show stenting in proximal LAD and panels G to I show stenting in proximal LCA
Medications
Aspirin, clopidogrel, tirofiban and low molecular weight heparin were used in appropriate doses in all patients. Ticagrelor was not used in any of the cases in the first two days of angioplasty, and in four patients at discharge ticagrelor was added after stopping clopidogrel.
Tirofiban was given to all patients, and the dosage was titrated based on the creatinine values. Immediately after stenting a bolus of 10ml tirofiban (Conc. 5 mg/100 ml) was given for one stent forcibly by hand, and if further stents are required extra bolus of 5ml was given through intracoronary route in the diagnostic catheter. When the creatinine levels were > 3 mg/dl, tirofiban was given at 1 to 1.5 ml/hr. Infusion for 14 hours. At normal creatinine values, the standard flow rate of tirofiban was 4 ml/hr. for 18 hours (conc. 5 mg/100 ml). In frail patients, the infusion rate was 3.5 ml/hr for 18 hours. For 18 hours. If there was any minor bleeding Tirofiban was stopped for 1 to 2 hours and restarted at 2.5 to 3 ml/hr. When the creatinine was 2 to 3 mg/dl, the infusion rate was 1.5 to 2 ml/hr for 12 to 14 hours. For 12 to 14 hours. The concentration of the tirofiban solution used for bolus and infusion was 5 mg/100ml.
Contrast-induced nephropathy was defined as a rise in creatinine of 0.5 mg/dl from the baseline or increase in creatinine up to 25% from baseline values. N-acetyl cysteine was started orally immediately after completion of the procedure in patients with elevated creatinine. Blood sugars were controlled predominantly by rapid-acting insulin injections and if required insulin infusion. At discharge, the patients were started with adequate doses of (rapid-acting + long-acting, mix) insulin along with diabetic medications. All patients were followed up to 30 days after discharge.
Bench testing through the radial path
Bench testing of the diagnostic and guide catheters was performed. A radial path was created based on anatomy with suitable angles and dimensions. The radial path creation is shown in Figure 4. The path starts with 4 mm and gradually increases in width and joins the aortic arch. The insertion sheath was 6F with 10 cm length instead of the standard 7cm. Details of indexation of the catheters for pushability and trackability parameters are shown in supplementary figures 1. The average length of the radial path is about 81 cm, and that of the femoral path is 56 cm.
Figure 4.
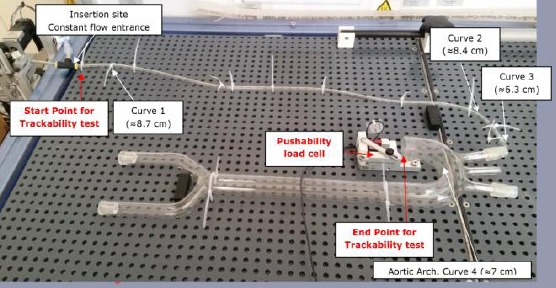
Radial and Femoral paths used in the bench testing evaluation
Results
The baseline characteristics, contrast requirement, and CIN
Table 1 summarises the baseline and patient characteristics. All parameters were approximated to the nearest integer. Successful revascularisation of the target lesion was achieved in all cases. The mean contrast requirement in this retrospective series per patient was 28ml (± 8 ml), and one death was seen. Contrast-induced nephropathy was observed in two patients. Patient 1 had CIN had risen in creatinine from 1.7 to 2.3 mg/dl and returned to near baseline 1.9 mg/dl. This patient had accelerated hypertension and gastritis and vomiting. However, the urine output was good. Patient 2 had an increase in creatinine from 1.1 to 1.5 mg/dl. Patient 2 was 72 years old and had heart failure and moderate left ventricular dysfunction and was on diuretics.
Table 1.
Baseline and the patient characteristics in the study
| Parameter | Value (N = 191) |
|---|---|
| Age, yrs | 58 ± 12 |
| Sex, M (%) | 79 |
| Diabetes, (%) | 82 |
| Hypertension, (%) | 46 |
| Primary PCI, n | 55 |
| Rescue PCI, n | 73 |
| NSTEMI (Post MI or Troponin positive), n | 47 |
| Unstable angina (Troponin negative), n | 16 |
| Baseline chronic renal failure with Cr > 2.0, n | 6 |
| Ticagrelor, n | 4 |
| Groin hematoma, n | 6 |
| Blood Transfusion, n | 2 |
| Antibiotics, n | 10 |
| Mortality, n | 1 |
| Another minor bleeding | 3 |
| Mean Fluoroscopy time, min | 5.3 ± 1.6 |
A reversible insignificant rise in creatinine less than the definition criteria for CIN was seen in 5 more cases. CIN was mild, and none required dialysis. The mean fluoroscopy time in this series of patients was 5.3 ± 1.6 min. Coronary perforations and wire breakages were not seen.
Antibiotics
Need-based higher antibiotics (Imipenem-3 and piperacillin-tazobactam-2 cases) were given in patients associated with sepsis (10 patients). Polymyxin B was used in two patients, and vancomycin in three patients. Oral ciprofloxacin and nitrofurantoin were given to ten patients.
Clinical observations
Cardiogenic shock was seen in 7 cases, which was successfully managed with inotropes, and IABP support was kept as a backup. The details of patients with cardiogenic shock are given in a separate paragraph below (Figure 5).
Figure 5.
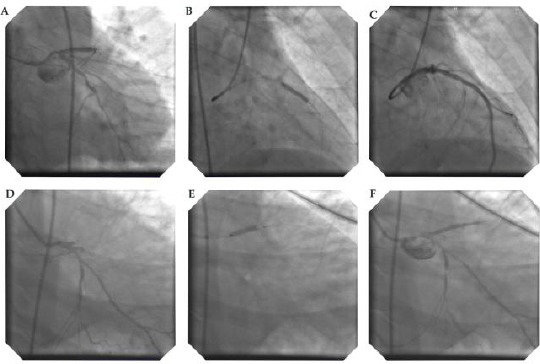
Proximal LAD stenting in patients with cardiogenic shock successfully recovered
Distal vessel spasm was seen in 5 cases, which were managed with a low dose of nitrates. Ventilator support was required in two patients. Mild pulmonary edema/heart failure was seen in 9 cases, which were managed with diuretics and they were managed with oxygen, and in seven cases transiently with non-invasive ventilation. Mild groin hematoma was seen in six cases, and blood transfusion with one unit was required in two patients.
Three patients had high creatinine > 3 mg/dl at baseline (3.1, 3.3 and 3.8 mg/dl). However, after the procedure and N-acetyl cysteine therapy, there was mild fall in creatinine. No mortality was observed in any of these cases.
The radio-opacity of the arteries and the stent was adequate to perform the procedure safely. Reperfusion ventricular tachycardia was seen in three patients, which was managed by DC cardioversion. Ventricular fibrillation was seen in one case, which was successfully reversed with DC cardioversion. Non-sustained ventricular tachycardia was seen in four more cases. Symptomatic transient vasovagal mediated bradycardia and mild hypotension were seen in 7 cases immediately after stenting and revascularisation, which responded to saline infusion, atropine, and vasopressors. Proximal vessel dissections were not seen by the radiological method in any of the cases. This was observed even after occasional sucking of the diagnostic catheters into the coronaries immediately during withdrawal of stent balloon post-stenting.
Hydration
Hydration through normal saline was given only when it is required or when transient hypotension was observed. This was seen in 9 cases where fluids were given due to transient hypotension. However, effective oral fluids were started as early as possible after the procedure. In four cases fluids were given > 1 litre, after insertion of the central venous pressure line. In patients with vasovagal or transient fall in blood pressures, fluids were given.
Cardiogenic shock
Cardiogenic shock was seen in 7 patients (Figure 5). Patient 1 had anterior wall infarction with hypotension, tachycardia (heart rate 140/min) and was thrombolysed, Killip 4. Frusemide infusion was started, and angioplasty was performed with 20 ml contrast and stent was placed to proximal LAD. Patient 2 had severe hypotension, tachycardia and anterior wall MI and stent was placed to proximal LAD with 25 ml contrast. The patient had persistent severe hypotension and decreased urine output. Fluid therapy was given with CVP guidance and inotropes. Urine output improved and the patient recovered. Patient 3 had thrombolysis outside and presented with Killip Class 4 and hypotension and tachycardia. Angioplasty with stenting was done to proximal LAD and the patient recovered. The patient also had septicemia, Polymyxin with imipenem was given for seven days, and the patient recovered. He was on a ventilator for one day.
Patient 4 had hypotension and anterior wall MI. After angioplasty, the patient improved. Patient 5 had inferior wall MI and chronic total occlusion of LAD and culprit RCA was stented and patient improved. Patient 6 had old anterior wall MI and chronic total occlusion (CTO) of proximal LAD, and stenting was done to culprit proximal RCA after multiple pre-dilatation, and the patient improved successfully. This patient had ventricular fibrillation immediately after stenting, which was successfully reversed with DC cardioversion. In the last 2 cases, CTO therapy of the LAD was not attempted in the acute setting. Patient 7 was an 82 yr. The old lady who had acute anterior wall myocardial infarction with the massive left ventricular clot and cardiogenic shock. After successful stenting, the patient developed ventricular tachycardia, which was successfully reversed with a shock. This patient lost sensorium due to embolisation of the clot to the brain, and 12 hours later the patient expired.
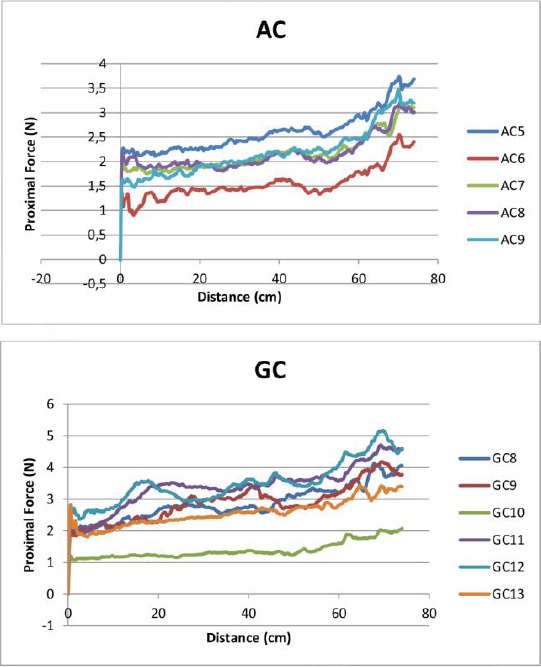
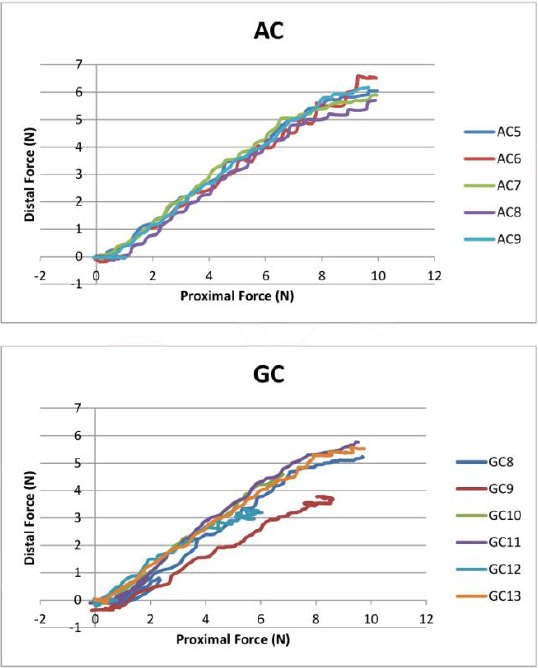
Radial path pushability and trackability
The possibility parameters of the radial track are shown in figure 6 and Supplementary Figure 2. The diagnostic and guide catheters show similar pushability parameters. The mean ratio of distal to distal force transmission in the femoral approach was 0.28 (± 0.13) for diagnostic, and 0.51 (± 0.11) for guide catheters. The mean ratio of distal/proximal force transmission in the radial track was 0.63 (± 0.07) for angiographic catheters and 0.58 (± 0.06) for guide catheters. The force transmission curve was better with diagnostic catheters. The trackability of the catheters is good up to the 74 cm, and after that the trackability was restricted (Figure 7/supplementary Figure 3). The bench testing in the femoral paths showed a force transmission ratio of 0.28 and 0.51 for diagnostic and guided catheters respectively [21].
Figure 6.
Trackability testing for diagnostic and guide catheters in a radial path
Figure 7.
Pushability testing for diagnostic and guide catheters in a radial path
Discussion
This is a series of angioplasties performed with performed with Cordis 6F diagnostic catheters using limited contrast. Bench evaluation of the catheters showed balanced force-displacement curves, compared to guide catheters. Contrast usage is minimised during the procedure, as the inner lumen of the diagnostic catheters is smaller. All types of coronary stents could be taken through the diagnostic catheters, and stent balloon could be easily withdrawn into the catheters. The bio-vascular scaffold was not used in this series of cases. The mean fluoroscopy time for the procedure was significantly lesser, which was about 5.3 min. In the previous study involving 34 patients in emergency setting [21], the Cordis 6F diagnostic catheters were used for angioplasty and stenting when difficulty in engagement in the coronary ostium was encountered, and the bench testing of catheters was performed in the femoral route. In this study, the 6F diagnostic catheters were used regularly for angioplasty, and bench testing of catheters was conducted through the radial path.
In the past, an IVUS guided study in stable coronary disorders has shown a lesser contrast requirement [22]. However, in acute coronary syndromes, IVUS alone strategy is difficult as the clot is unstable and the available time is limited. Routine hydration to all patients was not given though adequate oral fluids intake was ensured. Hydration is often recommended; however, since the contrast usage was less, it was used only when required [23]. Frequent hydration has its downside that it could worsen heart failure [24], and in the setting of anticoagulation, this can result in acute lung injury/ARDS. In a few patients’ intravenous fluids tend to cause rigors.
Clinical implications
The significant reduction in contrast load and fluoroscopy times [25] translate into lesser renal, respiratory injuries and coagulation abnormalities. Even in patients with mild CIN, oliguria was not seen. While renal injury by contrast, is well known, the worsening of congestive heart failure in the setting of anticoagulation can cause acute lung injuries. These lung injuries could cause ARDS or significant oxygen desaturations which would lead to the development of unnecessary arteriovenous shunts and eventually diversion of about 15 to 20% of the cardiac output [26].
This in the setting of acute coronary syndromes could worsen the ischemia or arrhythmias could result. Also, the contrast media by its action on the platelets can cause coagulation abnormalities which could be thrombotic or even bleeding [14], [15], [17], [18], [19], and it can injure the endothelium [27] resulting in the increase in inflammatory markers [28]. Even infection control is modulated by contrast media volumes [29], and a significant number of cases can have coexisting septicemia. These interactions make patient management difficult. Hence, a reduction in contrast media volume would give good clinical results.
Also, technically, large stents up to 4.5 mm and long stents of about 40 mm size can be used through these catheters. Left main lesions were performed and in left circumflex lesions a slight rotation to align coaxial to the vessel may be required.
Bernoulli’s theory, Poiseuille’s equation, and Reynolds number
The reduced volume of contrast is well explained by the diameter of the catheter and flow properties. The internal volume of the diagnostic catheter is 1.69 cu mm, and the internal volume of the guide catheter is 2.79 cu mm. The inner lumen of the diagnostic catheter is 1.4 mm, and the inner lumen of the guide catheter is 1.8 mm. When the stent or balloon is inside the coronaries the volume required to visualise the coronaries is still reduced. This is due to more force required to generate the rate of flow, which results in less contrast volume in the lesser space required to opacify the coronaries. This is further explainable by a derivative of Bernoulli’s Theorem [30], which is the Poiseuille’s equation [31]. Also, when the lumen of the catheter is narrow the volume of contrast wastage at the distal tip is reduced. This is due to better control of Reynold’s number or the laminar flow properties at the head of the contrast stream in thinner diagnostic catheters than in large lumen guide catheters. Reynold’s number is directly proportional to the diameter of the vessel [32]. This results in more turbulent flow at the tip and higher wastage of contrast in guide catheters. The coefficient of friction is higher in diagnostic catheters than in large lumen guide catheters especially when coated with hydrophilic material. All these reasons explain the usage of low contrast volume in angioplasties performed with diagnostic catheters.
Contrast-induced nephropathy is a major concern during these procedures, and it significantly influences the clinical outcome. Also, pulmonary oedema or congestive cardiac failures are often worsened by contrast volume and pulmonary haemorrhages, the need for ventilation and the duration of the ventilation if required are influenced by renal failure.
Couette flow and dynamic catheter sizes on bending
The diameter of the catheter sizes though fixed in the resting stages dynamically changes with the bending of the catheter [33]. The diagnostic has a tapering tip, near 90° angles at rest and on engagement. The guide has a wider angle (about 110°), which increases engagement (Figure 8). The dynamic diameter is directly proportional to the small bending, and the catheter diameter is less in diagnostic after the engagement. The guide retains the catheter thickness as it has wider bending radius.
Figure 8.
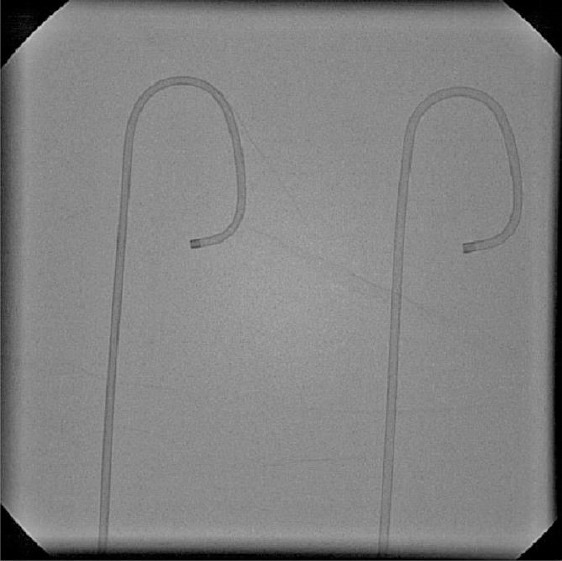
Comparison of the 6F Judkin’s left diagnostic (left) and guide catheter (right) by radiological screening. The tapering tip in the diagnostic catheter is seen
Couette flow represents the flow of fluid between two surfaces, and it can be variably differentiated and applied in different flow patterns with or without gradients in the flow [34]. The blood flow velocity and volume in the coronaries during angioplasty is dependent on the catheter engagement angle, Sine (90° Vs. 110°); the effective radius [(effective R2 = R2 LMCA – R2 catheter)], i.e. the difference radius of LMCA and radius of distal end of the catheter; and inversely proportional to the distal tip-length of the catheter after the distal end.
Radial vs Femoral Observations
This lesser ratio of distal to proximal force in the femoral is desirable for better torque control (δπ) of the catheter, which is inversely proportional to time (δt). The trackability of the catheters was good in the radial track with a unique restriction at 74 cm out of the total 81 cm. This correlates anatomically with the brachiocephalic trunk joining the aortic arch. Also, the angular momentum and velocity applying the right-hand thumb rule were directed towards the left shoulder. In the femoral path, which is shorter, the trackability of the catheters was good up to the end of the path, which is near the coronary ostium. These parameters indirectly correlate with the duration of the procedure and contrast usage.
Radial vs Femoral procedures – Angular momentum and velocity
The lesser trackability of catheters in the radial path is due to angular momentum, and angular velocities are directed away from the main axis of torque at the subclavian to brachiocephalic bend. The vector for these parameters follows the right- hand thumb rule, which is directed away from the main axis [35]. This would clinically translate to a slightly lesser control of catheters in the radial path. Large forces or torque are transmitted through the radial compared to the femoral due to thinner radial path compared to femoral. Hence, manual control of catheters tends to be slightly difficult in the radial path.
Frictional energy loss
The frictional energy loss is directly proportional to the lumen diameter of the catheter. In the diagnostic catheter since the lumen is smaller the loss of energy is more, and this limits the flow of contrast. Some latest catheters especially the newer generation guide catheters show improvements in tribology, frequently with hydrophilic coatings. This reduces the frictional energy loss. However, this could lead to additional contrast usage.
5F Guide catheters vs 6F Diagnostic catheters
The 5F guide catheters and the 6F diagnostic catheters have the same lumen dimensions. However, the 6F diagnostic catheters have thick wall compared to 5F guide. Bench testing showed less force to displacement in the 5F guide catheters in the pushability, and distal tip flexion test [21], and the 3-bend test showed large hysteresis (plasticity) [21]. The higher wall thickness in the 6F diagnostic catheters facilitates direct stenting by providing a better backup force (F = ma). Hence, by comparing these parameters, the 6F diagnostic catheters show better performance.
Acute coronary syndromes vs stable coronary artery disease
Angioplasties in acute coronary syndromes unlike routine angioplasty behave differently in mechanics and hemodynamics, and also in the biological and inflammatory response. The outcome is worsened by long procedure times and high contrast overload. As the ventricle is unstable, arrhythmias, cardio-renal syndromes with transient hypotension frequently complicate the procedure. Also, higher contrast load could release inflammatory markers like IL6, TNF-alpha, MCP-1, which could worsen the scenario, especially in cardiogenic shock [28]. Previous studies have shown elevated inflammatory markers in cardiogenic shock and their association with CIN and poor clinical outcomes.
Buddy wires, covered stents and IVUS
Using this technique two wires can be used in the diagnostic catheter during the procedure with a single stent on one wire. The second wire can be used as a buddy wire or in another vessel for stabilisation. Thin or low profile covered stents (5F) are feasible by this technique. Though IVUS was not performed routinely in these cases, it was performed in 2 cases using the latest 3F IVUS catheters in the diagnostic catheters (supplement Figure 4). The OCT catheters (2.7F) have lesser calibre compared to IVUS catheters (3F) and therefore are compatible with this technique.
Air bubble
During the procedure occasionally, a small air bubble could be formed at the proximal valve of the Touhy Borst (Y-connector). This air bubble can be expelled simply by a gentle flush of saline (2-3 ml) through the manifold after keeping the proximal valve of the Touhy open.
Limitations
Bifurcation stenting was not performed in this series. However, in primary angioplasties, provisional stenting is the treatment of choice. OCT and IVUS were not performed in this series, though these imaging catheters could be well taken inside these diagnostic catheters if required as they are 3F or less in diameter. Also, thrombo-suction was not performed in any of these cases. If the thrombus load is high and thrombosuction is contemplated, guide catheters could be used. Of late, this disadvantage could be overcome with the availability of 5F aspiration catheters with an outer luminal diameter of 1.09 mm, which is easily compatible with 6F diagnostic catheters.
Also, in appropriate cases if the cardiologist is not comfortable or when the procedure is likely to be prolonged or long calcific lesions are encountered, guide catheters could be chosen. However, the simplicity and stability of the diagnostic catheters, the improvised speed of the procedure, lesser fluoroscopy and radiation times, and the favorable lower contrast volume with good clinical outcomes in this series may not be underestimated.
The Artist Psychology and KISSS principle
It is a psychology for the artists to make any artistic procedures meticulous, difficult to perform with perfection [36]. This often compromises the simplicity of the procedure. This series shows lesser pre-dilatations, use of femoral route, direct stenting of lesions and lesser contrast usage with good clinical outcomes when used in appropriate cases. This is also following KISSS principle (Keep it simple, swift and safe), which is often highlighted in bifurcation lesion therapy [37].
During this period the author performed the angioplasties with an expert nursing assistant only. There was no training program during this period. The procedural technique and the decision making to restrict acquiring images, and further therapy with medications were at the discretion of the author. These could have influenced the results.
In conclusion, angioplasty with stenting can be performed safely in patients using cordis 6F diagnostic catheters using low volume of contrast in acute coronary syndromes. Large studies are required to validate the results.
Acknowledgement
Thanks to Karim Mouneimne, Vincent Gariety and Virginie Cazaly, Protomed labs, Marseille, France for bench testing of catheters.
Footnotes
Funding: This research did not receive any financial support
Competing Interests: The authors have declared that no competing interests exist
References
- 1.Tsai TT, Patel UD, Chang TI, et al. Contemporary Incidence, Predictors, and Outcomes of Acute Kidney Injury in Patients Undergoing Percutaneous Coronary Interventions:Insights From the NCDR Cath-PCI Registry. J Am Coll Cardiol Intv. 2014;7(1):1–9. doi: 10.1016/j.jcin.2013.06.016. https://doi.org/10.1016/j.jcin.2013.06.016 PMid:24456715 PMCid:PMC4122507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gruberg L, Mehran R, Dangas G, et al. Acute renal failure requiring dialysis after percutaneous coronary interventions. Catheter Cardiovasc Interv. 2001;52:409–416. doi: 10.1002/ccd.1093. https://doi.org/10.1002/ccd.1093 PMid:11285590. [DOI] [PubMed] [Google Scholar]
- 3.Marenzi G, Lauri G, Assanelli E, et al. Contrast-induced nephropathy in patients undergoing primary angioplasty for acute myocardial infarction. J Am Coll Cardiol. 2004;44:1780–1785. doi: 10.1016/j.jacc.2004.07.043. https://doi.org/10.1016/j.jacc.2004.07.043 PMid:15519007. [DOI] [PubMed] [Google Scholar]
- 4.Fox CS, Muntner P, Chen AY, et al. Short-term outcomes of acute myocardial infarction in patients with acute kidney injury:a report from the National Cardiovascular Data Registry. Circulation. 2012;125:497–504. doi: 10.1161/CIRCULATIONAHA.111.039909. https://doi.org/10.1161/CIRCULATIONAHA.111.039909 PMid:22179533 PMCid:PMC3411118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Parikh CR, Coca SG, Wang Y, et al. Long-term prognosis of acute kidney injury after acute myocardial infarction. Arch Intern Med. 2008;168:987–995. doi: 10.1001/archinte.168.9.987. https://doi.org/10.1001/archinte.168.9.987 PMid:18474763. [DOI] [PubMed] [Google Scholar]
- 6.Gruberg L, Mintz GS, Mehran R, et al. The prognostic implications of further renal function deterioration within 48 h of interventional coronary procedures in patients with pre-existent chronic renal insufficiency. J Am Coll Cardiol. 2000;36:1542–1548. doi: 10.1016/s0735-1097(00)00917-7. https://doi.org/10.1016/S0735-1097(00)00917-7. [DOI] [PubMed] [Google Scholar]
- 7.Duan S, Zhou X, Liu F, Peng Y, Chen Y, Pei Y, Ling G, Zhou L, Li Y, Pi Y, Tang K. Comparative cytotoxicity of high-osmolar and low-osmolar contrast media on HKCs in vitro. Journal of nephrology. 2006;19(6):717. PMid:17173243. [PubMed] [Google Scholar]
- 8.Samul W, Turowska A, Kwasiborski PJ, et al. Comparison of Safety of Radial and Femoral Approaches for Coronary Catheterization in Interventional Cardiology. Medical Science Monitor:International Medical Journal of Experimental and Clinical Research. 2015;21:1464–1468. doi: 10.12659/MSM.893193. https://doi.org/10.12659/MSM.893193 PMid:25996689 PMCid:PMC4450601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hibbert B, Simard T, Wilson K, et al. Transradial Versus Transfemoral Artery Approach for Coronary Angiography and Percutaneous Coronary Intervention in the Extremely Obese. JACC:Cardiovascular Interventions. 2012;5(8):819–826. doi: 10.1016/j.jcin.2012.04.009. https://doi.org/10.1016/j.jcin.2012.04.009. [DOI] [PubMed] [Google Scholar]
- 10.Michael TT, Alomar M, Papayannis A, et al. A randomized comparison of the transradial and transfemoral approaches for coronary artery bypass graft angiography and intervention:the RADIAL-CABG Trial (RADIAL Versus Femoral Access for Coronary Artery Bypass Graft Angiography and Intervention) JACC Cardiovasc Interv. 2013;6(11):1138–44. doi: 10.1016/j.jcin.2013.08.004. https://doi.org/10.1016/j.jcin.2013.08.004 PMid:24139930. [DOI] [PubMed] [Google Scholar]
- 11.Dmitriy N, Feldman, Rajesh V, Swaminathan, Lisa A, Kaltenbach, et al. Adoption of Radial Access and Comparison of Outcomes to Femoral Access in Percutaneous Coronary Intervention. Circulation. 2013;127:2295–2306. doi: 10.1161/CIRCULATIONAHA.112.000536. https://doi.org/10.1161/CIRCULATIONAHA.112.000536 PMid:23753843. [DOI] [PubMed] [Google Scholar]
- 12.Becher T, Behnes M, Ünsal M, et al. Radiation exposure and contrast agent use related to radial versus femoral arterial access during percutaneous coronary intervention (PCI)—Results of the FERARI study. Cardiovascular Revascularization Medicine. 2016;17(8):505–509. doi: 10.1016/j.carrev.2016.05.008. https://doi.org/10.1016/j.carrev.2016.05.008 PMid:27350417. [DOI] [PubMed] [Google Scholar]
- 13.Zukowski C, Wozniak l, de Souza Filho N, Cordeiro E, Rell A, Leal M, et al. Radial vs. Femoral Artery Access in Elderly Patients Undergoing Percutaneous Coronary Intervention. Revista Brasileira de Cardiologia Invasiva (English Version) 2014;22(2):125–130. https://doi.org/10.1590/0104-1843000000022. [Google Scholar]
- 14.Piessens J, Stammen F, Vrolix M, et al. Effects of an ionic versus a nonionic low osmolar contrast agent on the thrombotic complications of coronary angioplasty. Catheterization and Cardiovascular Diagnosis. 1993;28(2):99–105. doi: 10.1002/ccd.1810280203. https://doi.org/10.1002/ccd.1810280203 PMid:8448808. [DOI] [PubMed] [Google Scholar]
- 15.Hill J, Grabowski E. Relationship of anticoagulation and radiographic contrast agents to thrombosis during coronary angiography and angioplasty:Are there real concerns? Catheterization and Cardiovascular Diagnosis. 1992;25(3):200–208. doi: 10.1002/ccd.1810250306. https://doi.org/10.1002/ccd.1810250306 PMid:1571975. [DOI] [PubMed] [Google Scholar]
- 16.Cui T, Zhao J, Bei W, Li H, Tan N, Wu D, et al. Association between prophylactic hydration volume and risk of contrast-induced nephropathy after emergent percutaneous coronary intervention. Cardiology Journal. 2017;24(6):660–670. doi: 10.5603/CJ.a2017.0048. https://doi.org/10.5603/CJ.a2017.0048 PMid:28394010. [DOI] [PubMed] [Google Scholar]
- 17.Krause W, Press W. Influence of Contrast Media on Blood Coagulation. Investigative Radiology. 1997;32(5):249–259. doi: 10.1097/00004424-199705000-00001. https://doi.org/10.1097/00004424-199705000-00001 PMid:9140744. [DOI] [PubMed] [Google Scholar]
- 18.Brass O, Belleville J, Sabattier V, et al. Effect of ioxaglate—an ionic low osmolar contrast medium—on fibrin polymerization in vitro. Blood Coagulation &Fibrinolysis. 1993;4(5):689–697. https://doi.org/10.1097/00001721-199310000-00004. [PubMed] [Google Scholar]
- 19.Gabriel D, Jones M, Reece N, et al. Platelet and fibrin modification by radiographic contrast media. Circulation Research. 1991;68(3):881–887. doi: 10.1161/01.res.68.3.881. https://doi.org/10.1161/01.RES.68.3.881 PMid:1742873. [DOI] [PubMed] [Google Scholar]
- 20.Deftereos S, Giannopoulos G, Kossyvakis C, et al. Effect of radiographic contrast media on markers of complement activation and apoptosis in patients with chronic coronary artery disease undergoing coronary angiography. J Invasive Cardiol. 2009;21:473–477. PMid:19726822. [PubMed] [Google Scholar]
- 21.Arokiaraj MC. Emergency coronary angioplasty with stenting using Cordis®diagnostic coronary catheters when there is difficulty in engaging guide catheters and bench evaluation of diagnostic and guide catheters. Revista Portuguesa de Cardiologia (English Edition) 2018;37(2):117–125. doi: 10.1016/j.repc.2017.04.007. https://doi.org/10.1016/j.repce.2018.03.011. [DOI] [PubMed] [Google Scholar]
- 22.Mariani J, Guedes C, Soares P, et al. Intravascular Ultrasound Guidance to Minimize the use of Iodine Contrast in Percutaneous Coronary Intervention:The MOZART Randomized Controlled Trial. JACC Cardiovascular interventions. 2014;7(11):1287–1293. doi: 10.1016/j.jcin.2014.05.024. https://doi.org/10.1016/j.jcin.2014.05.024 PMid:25326742 PMCid:PMC4637944. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Maioli M, Toso A, Leoncini M, et al. Effects of Hydration in Contrast-Induced Acute Kidney Injury After Primary Angioplasty:A Randomized, Controlled Trial. Circulation:Cardiovascular Interventions. 2011;4(5):456–462. doi: 10.1161/CIRCINTERVENTIONS.111.961391. https://doi.org/10.1161/CIRCINTERVENTIONS.111.961391 PMid:21972403. [DOI] [PubMed] [Google Scholar]
- 24.Cui T, Zhao J, Bei W, Li H, Tan N, Wu D, Wang K, Guo X, Liu Y, Duan C, Chen S. Association between prophylactic hydration volume and risk of contrast-induced nephropathy after emergent percutaneous coronary intervention. Cardiology journal. 2017;24(6):660–70. doi: 10.5603/CJ.a2017.0048. https://doi.org/10.5603/CJ.a2017.0048 PMid:28394010. [DOI] [PubMed] [Google Scholar]
- 25.Nikolsky E, Pucelikova T, Mehran R, Balter S, Kaufman L, Fahy M, Lansky AJ, Leon MB, Moses JW, Stone GW, Dangas G. An Evaluation of Fluoroscopy Time and Correlation With Outcomes After Percutaneous Coronary Intervention. J Invasive Cardiol. 2007;19(5):208–213. PMid:17476034. [PubMed] [Google Scholar]
- 26.Sarkar M, Niranjan N, Banyal PK. Mechanisms of hypoxemia. Lung India. 2017;34(1):47–60. doi: 10.4103/0970-2113.197116. https://doi.org/10.4103/0970-2113.197116 PMid:28144061 PMCid:PMC5234199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Sawmiller C, Powell R, Quader M, Dudrick S, Sumpio B. The differential effect of contrast agents on endothelial cell and smooth muscle cell growth in vitro. Journal of Vascular Surgery. 1998;27(6):1128–1140. doi: 10.1016/s0741-5214(98)70015-1. https://doi.org/10.1016/S0741-5214(98)70015-1. [DOI] [PubMed] [Google Scholar]
- 28.Laskey WK, Gellman J. Inflammatory markers increase following exposure to radiographic contrast media. Acta Radiol. 2003;44(5):498–503. doi: 10.1080/j.1600-0455.2003.00119.x. https://doi.org/10.1034/j.1600-0455.2003.00119.x. [DOI] [PubMed] [Google Scholar]
- 29.Thorpe P, Zhan X, Agrawal D. Effect of Iodinated Contrast Media on Neutrophil Adhesion to Cultured Endothelial Cells. Journal of Vascular and Interventional Radiology. 1998;9(5):808–816. doi: 10.1016/s1051-0443(98)70396-3. https://doi.org/10.1016/S1051-0443(98)70396-3. [DOI] [PubMed] [Google Scholar]
- 30.Resnick R, Halliday D. Section 18-4, Physics. John Wiley &Sons, Inc; 1960. [Google Scholar]
- 31.Pfitzner J. (1976). “Poiseuille and his law”. Anaesthesia. 1976;31(2):273–5. doi: 10.1111/j.1365-2044.1976.tb11804.x. https://doi.org/10.1111/j.1365-2044.1976.tb11804.x. [DOI] [PubMed] [Google Scholar]
- 32.Fox RW, McDonald AT, Pritchard PJ. Introduction to Fluid Mechanics. 6th ed. Hoboken: John Wiley and Sons; 2004. p. 348. [Google Scholar]
- 33.Pelyhe I, Kertersz A, Bognar E. Flexibility of diagnostic catheters. XIII youth symposium on experimental solid mechanics. Decin, Czech Republic, 29 June to July 2. 2014 PMid:25240876. [Google Scholar]
- 34.Mendiburu AA, Carocci LR, Carvalho JA. Analytical solution for transient one dimensional couette flow considering constant and time dependent pressure gradients. Engenharia Termica. 2009;8(2):92–98. https://doi.org/10.5380/reterm.v8i2.61921. [Google Scholar]
- 35.Watson W. General Physics. New York: Longmans, Green and Co; 1912. p. 33. [Google Scholar]
- 36.Fiebelman JK. The psychology of the artist. 1945;19(2):165–189. [Google Scholar]
- 37.Lassen JF, Holm NR, Banning A, et al. Percutaneous coronary intervention for coronary bifurcation disease:11th consensus document from the European Bifurcation Club. EuroIntervention. 2016;12(1):38–46. doi: 10.4244/EIJV12I1A7. https://doi.org/10.4244/EIJV12I1A7 PMid:27173860. [DOI] [PubMed] [Google Scholar]