

Abstract
Background
This is an updated version of a review that was originally published in the Cochrane Database of Systematic Reviews in 2004, Issue 2. People with cancer, their families and carers have a high prevalence of psychological stress which may be minimised by effective communication and support from their attending healthcare professionals (HCPs). Research suggests communication skills do not reliably improve with experience, therefore, considerable effort is dedicated to courses that may improve communication skills for HCPs involved in cancer care. A variety of communication skills training (CST) courses have been proposed and are in practice. We conducted this review to determine whether CST works and which types of CST, if any, are the most effective.
Objectives
To assess whether CST is effective in improving the communication skills of HCPs involved in cancer care, and in improving patient health status and satisfaction.
Search methods
We searched the following electronic databases: Cochrane Central Register of Controlled Trials (CENTRAL) Issue 2, 2012, MEDLINE, EMBASE, PsycInfo and CINAHL to February 2012. The original search was conducted in November 2001. In addition, we handsearched the reference lists of relevant articles and relevant conference proceedings for additional studies.
Selection criteria
The original review was a narrative review that included randomised controlled trials (RCTs) and controlled before‐and‐after studies. In this updated version, we limited our criteria to RCTs evaluating 'CST' compared with 'no CST' or other CST in HCPs working in cancer care. Primary outcomes were changes in HCP communication skills measured in interactions with real and/or simulated patients with cancer, using objective scales. We excluded studies whose focus was communication skills in encounters related to informed consent for research.
Data collection and analysis
Two review authors independently assessed trials and extracted data to a pre‐designed data collection form. We pooled data using the random‐effects model and, for continuous data, we used standardised mean differences (SMDs).
Main results
We included 15 RCTs (42 records), conducted mainly in outpatient settings. Eleven studies compared CST with no CST intervention, three studies compared the effect of a follow‐up CST intervention after initial CST training, and one study compared two types of CST. The types of CST courses evaluated in these trials were diverse. Study participants included oncologists (six studies), residents (one study) other doctors (one study), nurses (six studies) and a mixed team of HCPs (one study). Overall, 1147 HCPs participated (536 doctors, 522 nurses and 80 mixed HCPs).
Ten studies contributed data to the meta‐analyses. HCPs in the CST group were statistically significantly more likely to use open questions in the post‐intervention interviews than the control group (five studies, 679 participant interviews; P = 0.04, I² = 65%) and more likely to show empathy towards patients (six studies, 727 participant interviews; P = 0.004, I² = 0%); we considered this evidence to be of moderate and high quality, respectively. Doctors and nurses did not perform statistically significantly differently for any HCP outcomes.There were no statistically significant differences in the other HCP communication skills except for the subgroup of participant interviews with simulated patients, where the intervention group was significantly less likely to present 'facts only' compared with the control group (four studies, 344 participant interviews; P = 0.01, I² = 70%).
There were no significant differences between the groups with regard to outcomes assessing HCP 'burnout', patient satisfaction or patient perception of the HCPs communication skills. Patients in the control group experienced a greater reduction in mean anxiety scores in a meta‐analyses of two studies (169 participant interviews; P = 0.02; I² = 8%); we considered this evidence to be of a very low quality.
Authors' conclusions
Various CST courses appear to be effective in improving some types of HCP communication skills related to information gathering and supportive skills. We were unable to determine whether the effects of CST are sustained over time, whether consolidation sessions are necessary, and which types of CST programs are most likely to work. We found no evidence to support a beneficial effect of CST on HCP 'burnout', patients' mental or physical health, and patient satisfaction.
Keywords: Humans; Communication; Caregivers; Caregivers/education; Caregivers/psychology; Health Personnel; Health Personnel/education; Medical Oncology; Medical Oncology/education; Neoplasms; Neoplasms/psychology; Neoplasms/therapy; Oncology Nursing; Oncology Nursing/education; Professional‐Patient Relations; Randomized Controlled Trials as Topic; Stress, Psychological; Stress, Psychological/prevention & control
Are courses aimed at improving the way doctors and nurses communicate with patients with cancer helpful?
People with cancer, and those who care for them, often suffer from psychological stress which may be reduced by effective communication and support from their attending doctor, nurse or other healthcare professional (HCP). Research suggests communication skills do not reliably improve with experience, therefore, considerable effort is dedicated to courses to improve communication skills for HCPs involved in cancer care. Many different types of communication skills training (CST) courses have been proposed and are in practice. We conducted this review to determine whether CST works and which types of CST, if any, are the most effective.
We found 15 studies to include in this review. All of these studies except one were conducted in nurses and doctors. To measure the impact of CST, some studies used encounters with real patients and some used role‐players (simulated patients). We found that CST significantly improved some of the communication skills used by healthcare workers, including using 'open questions' in the interview to gather information and showing empathy as a way of supporting their patients. Other communication skills evaluated showed no significant differences between the HCPs who received the training and those who did not. We did not find evidence to suggest any benefits of CST to patients' mental and physical health, patient satisfaction levels or quality of life, however, few studies addressed these outcomes. Furthermore, it is not clear whether the improvement in HCP communication skills is sustained over time and which types of CST are best.
Summary of findings
Summary of findings for the main comparison.
| Communication skills training compared with no communication skills training for improving healthcare professionals (HCP) communication with cancer patients | ||||
|
Patient or population: healthcare professionals working with patients with cancer Settings: outpatient or primary care Intervention: A communications skills training program Comparison: No communication skill training | ||||
| Outcomes | Relative effect: (P value) | No of participant interviews (studies) | Quality of the evidence (GRADE) | Comments |
| HCP showed 'empathy' | Favoured the intervention (P = 0.004) |
727 (6 studies) |
⊕⊕⊕⊕ high | These data were consistent and did not display statistical heterogeneity (I² = 0%). |
| HCP used 'open questions' | Favoured the intervention (P = 0.04) |
679 (5 studies) | ⊕⊕⊕⊝ moderate | We downgraded the quality of the evidence due to the statistical heterogeneity of the studies (I² = 65%). |
| HCP 'gave facts only' (simulated patients only) | Favoured the control group (P = 0.01) |
406 (4 studies) | ⊕⊕⊕⊝ moderate | We downgraded the quality of this evidence due to the clinical and statistical heterogeneity of the studies (I² = 70%).This effect was not evident in the subgroup of 'real patients'. Tests for subgroup differences were statistically significant. |
| Patient satisfaction with communication | Not significantly different P = 0.36 |
429 (2 studies) | ⊕⊕⊝⊝ low | We downgraded the quality of the evidence due to clinical and statistical heterogeneity (I² = 74%) and the fact that only two studies contributed data. |
| Patient anxiety: State trait Anxiety Inventory | Favoured the control group (P = 0.02) |
169 (2 studies) |
⊕⊝⊝⊝ very low | We downgraded the quality of the evidence due to the clinical heterogeneity of the studies and the fact that only two studies contributed data. In addition, one of these studies reported baseline differences in anxiety between the two groups (significantly higher in the control group) and it was not clear from the report whether the results were adjusted for this difference. |
| GRADE Working Group grades of evidence: High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||
Background
This is an updated version of a review that was originally published in the Cochrane Database of Systematic Reviews in 2003, Issue 2. Good communication between health professionals and patients is essential for high quality health care. Effective communication benefits the well‐being of patients and health professionals, influencing the rate of patient recovery, effective pain control, adherence to treatment regimens, and psychological functioning (Fallowfield 1990; Gattellari 2001; Stewart 1989; Stewart 1996; Vogel 2009). Cancer sufferers have a high prevalence of psychological stress and need emotional and social support. Hence, it is important that from the start there is adequate communication about the diagnosis, prognosis and treatment alternatives (Hack 2011). Furthermore, treatment of psychological stress may have a positive effect on quality of life (Girgis 2009).
Conversely, ineffective communication can leave patients feeling anxious, uncertain and generally dissatisfied with their care (Hagerty 2005) and has been linked to a lack of compliance with recommended treatment regimens (Turnberg 1997). Avoiding disclosing cancer as the diagnosis has been linked to higher rates of depression and anxiety and lower use of coping skills (Donovan‐Kicken 2011). Complaints about health professionals made by patients frequently focus, not on a lack of clinical competence per se, but rather on a perceived failure of communication and an inability to adequately convey a sense of care (Moore 2011; Lussier 2005). Communication issues are an important factor in litigation (Levinson 1997).
Ineffective communication is also linked to increased stress, lack of job satisfaction and emotional burnout amongst healthcare professionals (Fallowfield 1995; Ramirez 1995). Self‐awareness, reflection and learning about communication skills may have benefits for health professionals, and prevent burnout.
Most patients with cancer prefer a patient‐centred or collaborative approach (Dowsett 2000; Hubbard 2008; Tariman 2010); however, there is a minority who prefer a more task‐centred approach. Furthermore, patient preferences regarding the communication of bad news have been found to be culturally dependent (Fujimori 2009).This makes it imperative that health professionals understand the needs of the individual patient (Dowsett 2000; Sepucha 2010). The type of relationship that occurs in reality can be very different from that preferred by patients and doctors (Tariman 2010; Taylor 2011) and the literature suggests that patients with cancer continue to have unmet communication needs (Hack 2005). Taylor 2011 reported that a majority of clinicians liked to include emotional issues during their interviews with patients with cancer, however, clinical interviews tend to be predominated by biomedical discussion with only a minimal time dedicated to psychosocial issues (Hack 2011; Vail 2011).
The ability to communicate effectively is a pre‐condition of qualification for most healthcare professionals (HCPs) (ACGME 2009; CanMEDS 2011; GMC 2009). As communication skills do not reliably improve with experience alone (Cantwell 1997), communication skills training (CST) is mandatory in many training programs, therefore, considerable effort and expense is being dedicated to CST.
Description of the intervention
CST courses/workshops generally focus on communication between HCPs and patients during the formal assessment procedure (interview), and include emphasis on skills for building a relationship, providing structure to the interview, initiating the session, gathering information, explaining, planning and closure (Silverman 2005). Building a relationship may be particularly relevant with patients with cancer where promoting a greater disclosure of individual concerns and feelings may enable optimum care. Breaking bad news and shared decision‐making have been other focuses of CST for HCPs involved in cancer care (Fallowfield 2004; Paul 2009).
Most approaches to teaching communication in health care incorporate cognitive, affective and behavioural components, with the general aim of promoting greater self‐awareness in the HCP. CST based on acquiring skills may be more effective than programmes based on attitudes or specific tasks (Kurtz 2005) and is considered to be more effective if experiential. The essential components that facilitate learning have been highlighted in guidelines (Gysels 2004; Stiefel 2010) and include the following.
Systematic delineation and definition of the essential skills (verbal, non‐verbal and paralinguistic). Skills that are effective in communication with patients with cancer are defined (e.g. the use of open questions, incorporating a psychosocial assessment, demonstrating empathy). Pitfalls include leading questions, focusing only on the physical and failing to explore the more psychological issues and premature reassurance. However, some claim that the evidence base for this definition of essential skills is still weak (Cegala 2002; Paul 2009).
Observation of learners: through the use of learning techniques such as role‐play, participants are then given the opportunity to practice their communication skills using facilitating behaviours and avoiding blocking behaviours in a 'safe’ environment. Often, role‐playing is aided by the use of simulated patients trained to represent someone with cancer, and who can provide a range of cues and responses to communication in the role‐play, thus providing a safe opportunity for healthcare professionals to practice communication skills without distressing patients (Aspegren 1999; Kruijver 2001; Nestel 2007).
Well‐intentioned, descriptive feedback, which may be verbal or written.
Video or audio‐recordings and review permitting self‐reflection.
Repeated practice.
Active small group or one‐to‐one 'learner‐centred' learning.
Facilitators with training and experience (Bylund 2009).
CST has been delivered in a variety of ways, for example, via sessions integrated into degree or diploma studies (e.g. Wilkinson 1999) or three to five day workshops using actors as simulated patients (Fallowfield 1990; Heaven 1996; Razavi 2000). The optimal length for CST is under debate. Gysels 2004 argues that longer courses are more effective.
There is a wide variety of models and approaches to trials of communication skills training and interpreting the data is often hampered by poor methodological quality (Fallowfield 2004). The original 2004 version of this Cochrane review concluded, based on three randomised controlled trials, that there was some evidence that courses on CST for HCPs working with patients with cancer may be effective in improving HCP communication skills (Fellowes 2003). Since then, other reviewers have reached the same conclusions in different ways (Barth 2011; Bylund 2010; Kissane 2012). Whilst some have suggested that these positive effects can be maintained over time, others have concluded that a strong evidence base for a significant effect on trial outcomes is lacking (Alvarez 2006), particularly for an effect on patient outcomes (Uitterhoeve 2010).
Why it is important to do this review
There has been much research in this area since the original Cochrane review was published, including the conduct of several randomised controlled trials (RCTs), which were scant at the time of the original review. Other more recent reviews in the field have included a variety of studies with different study designs, however, none have conducted meta‐analyses of the results from RCTs. By undertaking this systematic review and keeping it up‐to‐date we aimed to critically evaluate all RCTs that have investigated the effectiveness of CST for HCPs working in cancer care, in order to enable evidence‐based teaching and practice in this important and expanding area. Furthermore, we hoped that a review and meta‐analysis of data from such RCTs would provide stronger evidence of any potential benefits that CST may have on HCP behaviour and provide guidance on the optimal methodology and length of training, as well as how to ensure that these newly acquired skills are transferred to the work‐place.
Objectives
To assess whether communication skills training is effective in changing behaviour of HCPs working in cancer care and in improving patient health status and satisfaction.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs), including cluster‐randomised studies.
Types of participants
Types of healthcare professionals (HCPs): All qualified HCPs (medical, nursing and allied health professionals) within all hospital, hospice and ambulatory care settings, working in cancer care. If a study included other non‐professionals, the percentage of professionals in the sample was > 60%. If a study also included HCPs working in non‐cancer care, the percentage of HCP working in cancer care was > 60%. Training of intermediaries (e.g. interpreters, advocates, self‐help groups) was not considered.
Types of patients: Men and women with a diagnosis of cancer, at any stage of treatment. If a study included patients with other diagnoses, patients with cancer made up > 60% of the study sample. We included studies that assessed interviews in both real and simulated patients (for definition see Appendix 1).
Types of encounters: Consultations and interviews where cancer patient care is the main aim. We excluded trials that studied encounters where the aim was to improve the quality of informed consent or to disclose information for informed patient consent to participate in a RCT.
Types of interventions
We included only studies in which the intervention group had communication skills training (e.g. study days, teaching pack, distance learning, workshops; and including any mode of training such as audiotape feedback, videotape recording of interviews, role‐play, group discussion, didactic teaching), and in which the control group received nothing beyond the usual, or received an alternative training to the intervention group. We included all types and approaches to teaching, any length of training and any focus of communication between professionals and patients with cancer within the context of patient care. We excluded studies whose focus was communication skills in encounters related to informed consent for research. This specific type of CST is under discussion as the subject of a separate Cochrane review.
Types of outcome measures
We included outcomes that measured changes in HCP behaviour or skills, other HCP outcomes and patient‐related outcomes at any time after the intervention. We anticipated that many of these outcomes would be measured by validated study‐specific observational rating scales and potentially subject to a high degree of inter‐trial methodological heterogeneity. Studies that only reported outcomes of changes in attitudes/knowledge on the part of the HCPs or patients without examining resulting changes in behaviour of HCPs were excluded from the review, as self‐perceived improvements have been shown to be over‐optimistic (Chant 2002).
Primary outcomes
HCP communication skills
Information gathering skills, such as open questions, leading questions, facilitation, clarifying and summarising
Discovering the patients perspective such as eliciting concerns
Explaining and planning skills such as giving the appropriate information, checking understanding, and negotiating procedures and future arrangements
Supportive, building relationship skills such as empathy, responding to emotions/psychological utterances; and offering support
Undesirable outcomes, including blocking behaviours such as interruptions and false reassurances, and providing facts only
Secondary outcomes
Other HCP outcomes
Burnout
Patient‐rated outcomes
-
Patient health status
Anxiety level/psychological distress
Quality of life
-
Patient Perception
Perception of HCP's communication skills: clarification, assessment of concerns, information, support, trust
Satisfaction
Outcomes of 'significant other'
-
Perception of significant other
Perception of HCP's communication skills: clarification, assessment of concerns, information, support, trust
Satisfaction
Search methods for identification of studies
Electronic searches
For the original review, the following databases were searched.
CENTRAL (The Cochrane Library, 2001, Issue 3)
MEDLINE (1966 to November 2001)
EMBASE (1980 to November 2001)
PsycInfo (1887 to November 2001)
CINAHL (1982 to November 2001)
AMED (1985 to October 2001)
SIGLE (Start to March 2002) (Grey literature database held by British Library)
Dissertation Abstracts International (1861 to March 2002)
Evidence‐Based Medical Reviews (1991 to March/April 2001)
For the updated review, the search strategy was modified by Jane Hayes (JH) of the Cochrane Gynaecological Cancer Review group (CGCRG), who extended the searches of CENTRAL, MEDLINE, EMBASE, PsycInfo and CINAHL to Febuary 2012. In addition, JH searched the Database of Reviews of Effects (DARE) in The Cochrane Library in September 2011. No language restrictions were applied. (See Appendix 2, Appendix 3, Appendix 4 for search strategies).
Searching other resources
We handsearched the reference lists of relevant studies that we identified from the electronic searches and the conference abstracts of the annual International Psycho‐Oncology Society meetings.
Data collection and analysis
Selection of studies
For the original review, two of three review authors, Deborah Fellowes (DF), Susie Wilkinson (SW) and Philippa Moore (PM) independently applied inclusion criteria to each identified study. For the update, PM and Solange Rivera Mercado (SRM) or Monica Grez Artigues(MGA) independently evaluated identified studies for inclusion. Disagreements were resolved by discussion between all three review authors. We identified potentially eligible studies from the search abstracts and retrieved the full text of the articles if the review criteria were met, or if the abstract contained insufficient information to assess the review criteria.
Data extraction and management
For the original data extraction, two review authors recorded the methodology (including study design, participants, sample size, intervention, length of follow‐up and outcomes), quality and results of the included studies on a standardised data extraction form. For the updated review, we designed a new data extraction form to include some specific outcomes and a 'Risk of bias' assessment. Two review authors extracted data independently (PM and SRM or MGA) and resolved any disagreement by discussion. We entered the data into Review Manager software (RevMan 2011) and checked for accuracy.
Assessment of risk of bias in included studies
The quality of eligible studies was assessed independently by three review authors (DF, SW, PM) for the original review, and by two review authors (PM, SRM) for the updated review. For included studies, we assessed the risk of bias as follows.
Selection bias: random sequence generation and allocation concealment.
Detection bias: blinding of outcome assessment.
Attrition bias: incomplete outcome data.
Reporting bias: selective reporting of outcomes.
Other possible sources of bias.
For further details see Appendix 5. Results are summarised in a 'Risk of bias' graph (Figure 1) and a 'Risk of bias' summary.
Figure 1.
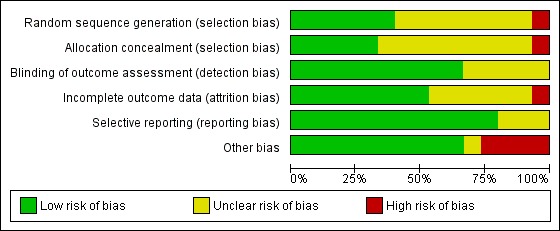
'Risk of bias' graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Measures of treatment effect
Tools for assessing communication were diverse and usually consisted of validated questionnaires and scales. Data for all outcomes were continuous. We had planned to measure the mean difference (MD) between treatment arms, however most trials measured the same outcome using different scales, and so we used the standardised mean difference (SMD) for all meta‐analyses.
Unit of analysis issues
The units of analyses included the HCPs, their patients and significant others, and their encounters/conversations/interviews. Two review authors (PM and SRM or MG) reviewed unit of analysis issues according to Higgins 2011 and differences were resolved by discussion. These included reports where there were multiple observations for the same outcome, e.g. several interviews involving the same HCP for the same outcome at different time points. When there were multiple time points for observation, we considered the data from the time point closest to the end of intervention as the post‐intervention measurement. This ranged from immediately post‐intervention to three months post‐intervention. We also analysed the longest follow‐up measurement for each study which ranged from two to 12 months.
Dealing with missing data
For included studies we noted the level of attrition. Studies with greater than 20% attrition were considered at moderate to high risk of bias. For all outcomes, we attempted to carry out analyses on an intention‐to‐treat basis. We did not impute missing outcome data. If data were missing or only imputed data were reported, we attempted to contact trial authors to request the missing data.
Assessment of heterogeneity
We assessed the heterogeneity between studies by visual inspection of forest plots, by estimation of the percentage heterogeneity between trials (the I² statistic) (Higgins 2003), and by a formal statistical test of the significance of the heterogeneity (Deeks 2001). We considered a P value of less than 0.10 and an I² > 50% to represent substantial heterogeneity.
Assessment of reporting biases
We intended to examine funnel plots corresponding to meta‐analysis of the primary outcome to assess the potential for small study effects such as publication bias if a sufficient number of studies were identified, however, there were fewer than 10 studies in all meta‐analyses.
Data synthesis
We used the random‐effects model with inverse variance weighting for all meta‐analyses (DerSimonian 1986) and pooled the standardised mean differences (SMDs), presenting these results with the corresponding 95% confidence intervals (CIs).
Subgroup analysis and investigation of heterogeneity
To investigate heterogeneity, we carried out subgroup analyses of the primary outcomes according to staff group (e.g. doctors and nurses), patient type (e.g. real or simulated) and type of comparison (e.g. CST versus no‐CST or CST with follow‐up versus CST alone). We had intended to carry out subgroup analyses according to the type of CST e.g. didactic teaching, distance learning, role‐play workshops, however this was not possible due to the wide variety of interventions included. We will attempt subgroup analyses in future versions of this review.
Sensitivity analysis
We performed sensitivity analysis for the primary outcomes to investigate heterogeneity between studies. Three studies compared a CST intervention with no CST after giving preliminary CST to all HCP participants (intervention and control groups). Where any of these three studies contributed to meta‐analyses, we performed sensitivity analyses by excluding these data and compared the results.
Results
Description of studies
Results of the search
For the original review, we identified 51 potentially relevant articles, of which we included three studies (Fallowfield 2002; Razavi 1993; Razavi 2002) and excluded 48 studies (Figure 2). For the updated review, we retrieved a total of 5472 articles; 4948 were either duplicates or were excluded on title. Of the remainder, we identified 119 records for classification. On retrieval of the full text of these records, we included 39 records (pertaining to 15 studies) and excluded 80 records (pertaining to 70 studies; see Figure 3).
Figure 2.
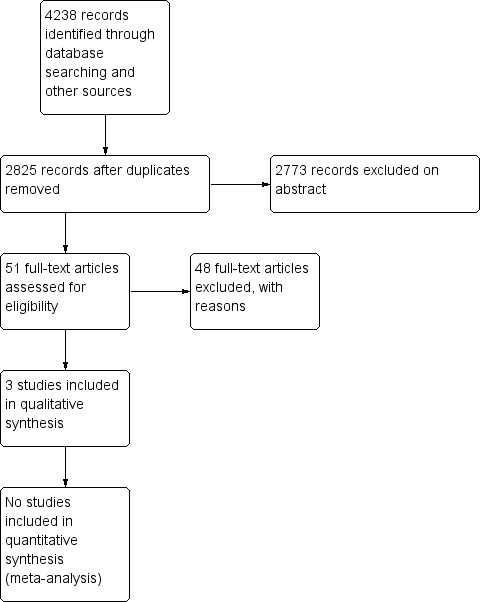
Study flow diagram of original searches (November 2001and November 2003)
Figure 3.
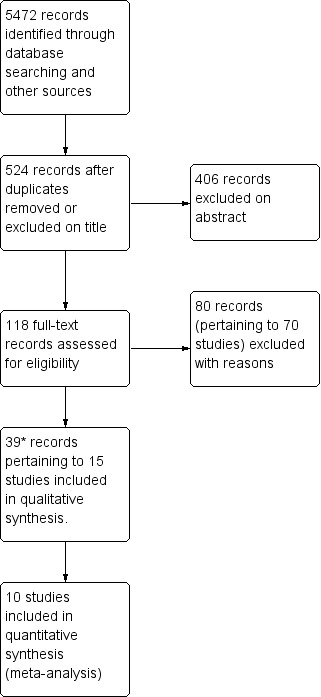
Study flow diagram of updated searches to 28 February 2012.
*Therefore, 15 studies and 42 records in total (updated search results plus original results)
Included studies
Of the 42 records included (3+39) from all the searches to date, we identified 15 trials in total (nine of which had multiple publications, including the original three included studies). Fourteen trials were published in full and one (Fujimori 2011) was available as a conference abstract only.
Ten studies (Butow 2008; Fujimori 2011; Gibon 2011; Goelz 2009; Kruijver 2001; Lienard 2010; Razavi 1993; Razavi 2002; van Weert 2011; Wilkinson 2008) investigated the effect of CST in the intervention group compared with a control group with no intervention.
One study (Fallowfield 2002) compared two interventions in four comparative groups: CST or no training, and the provision of individual feedback or no feedback.
Three studies assessed the effect of a follow‐up intervention after initial training: six bi‐monthly consolidation workshops of three hours in length (Razavi 2003), four half‐day supervision sessions spread over four weeks (Heaven 2006) and CD‐ROM (Tulsky 2011).
One study compared different durations of CST (Stewart 2007).
Overall, the communication skills of 1147 healthcare professional (HCP) participants were reported in these studies and 2105 patient encounters were analysed. Patients with cancer were from various cancer care settings (59% women; mean age 60 years) and the studies enrolled the following HCPs.
Doctors (eight studies): Butow 2008 = 30 oncologists; Fallowfield 2002 = 160 oncologists; Fujimori 2011 = 30 oncologists; Goelz 2009 = 41 mainly haematology/oncology doctors; Lienard 2010 = 113 residents; Razavi 2003 = 63 physicians (62% oncologists); Stewart 2007 = 51 doctors (18 oncologists, 17 family physicians and 16 surgeons); Tulsky 2011 = 48 oncologists.
Nurses (six studies): Heaven 2006 = 61 nurses; Kruijver 2001 = 53 nurses; van Weert 2011 = 48 nurses; Razavi 1993 = 72 nurses; Razavi 2002 = 116 nurses; Wilkinson 2008 = 172 nurses.
Other HCPs: one trial studied the effect of CST on radiotherapy teams which included a mixed group of 80 doctors, nurses, physicists and secretaries (Gibon 2011).
The majority of the trials were conducted in Europe, with the exception of Stewart 2007 (Canada), Butow 2008 (Australia); Fujimori 2011 (Japan) and Tulsky 2011 (USA). The average age of the HCP participants (13 studies) was 39 years and the number of HCPs in the studies ranged from 30 to 172 (mean, 75). Women comprised approximately 50% of participants in the trials involving doctors and approximately 90% of those involving nurses. Their experience working with patients with cancer ranged from < two years to 24 years. With regard to previous CST, one study reported that 47% of the participants had received > 50 hours of CST prior to the trial (Heaven 2006); two studies reported that participants had received no previous CST (Goelz 2009; Wilkinson 2008). Fujimori 2011 reported no data relating to participant characteristics and we were unsuccessful in contacting the authors for more details.
Most studies were conducted in the hospital outpatient setting except for two studies that involved professionals working in the community (primary care and hospices) (Heaven 2006; Wilkinson 2008) and four that involved HCPs working in an inpatient setting (Kruijver 2001; Lienard 2010; Razavi 2002; van Weert 2011).
Type of intervention
The objective of most trials was to train the professionals in general communication skills (Fallowfield 2002; Fujimori 2011; Gibon 2011; Heaven 2006; Razavi 1993; Razavi 2002; Stewart 2007; van Weert 2011; Wilkinson 2008). Two trials aimed to train professionals specifically to detect and respond to patients emotions (Butow 2008;Tulsky 2011). Two trials trained HCPs in giving bad news (Lienard 2010; Razavi 2003) and Goelz 2009 trained HCPs in addressing the transition to palliative care. Kruijver 2001 concentrated on CST for nurses' admission interviews.
Most trials specified the use of learner‐centred, experiential, adult education methods by experienced facilitators (10 trials: Butow 2008; Fallowfield 2002; Goelz 2009; Heaven 2006; Lienard 2010; Razavi 2003; Stewart 2007; Tulsky 2011; van Weert 2011; Wilkinson 2008). Co‐teaching was stated in four studies (Goelz 2009; Heaven 2006; Kruijver 2001; Razavi 1993). CST was taught in small groups (range three to 15 participants) in 12 trials (Butow 2008; Fallowfield 2002; Goelz 2009; Heaven 2006; Kruijver 2001; Lienard 2010; Razavi 1993; Razavi 2002; Razavi 2003; Stewart 2007; van Weert 2011; Wilkinson 2008). All small‐group studies used role‐play, although it was often unclear if the cases used were pre‐defined or true cases of the participants, and if the role‐play was between participants or with simulated patients. In all studies, real patients were only used for the assessment interviews, and not during training.
Most interventions included written material (10 trials; Butow 2008; Fallowfield 2002; Goelz 2009; Kruijver 2001; Razavi 1993; Razavi 2002; Razavi 2003; Stewart 2007; van Weert 2011; Wilkinson 2008) and short didactic lectures (eight trials; Butow 2008; Goelz 2009; Kruijver 2001; Lienard 2010; Razavi 1993; Razavi 2002; Razavi 2003; Wilkinson 2008). Six trials specified the use of role‐modelling (Butow 2008; Heaven 2006; Kruijver 2001; Stewart 2007; Tulsky 2011; Wilkinson 2008); and 10 trials specified the use of video material (Butow 2008; Goelz 2009; Fallowfield 2002; Heaven 2006; Kruijver 2001; Razavi 1993; Stewart 2007; Tulsky 2011; van Weert 2011;Wilkinson 2008). Two trials described e‐learning: 1.5 hour video conferences as follow‐up after the CST (Butow 2008) and use of a CD‐ROM as follow‐up after a communication skills lecture (Tulsky 2011). The type of learning in Fujimori 2011 was not specified.
The participants received feedback from their tutors either verbally (Butow 2008; Goelz 2009; Heaven 2006; Kruijver 2001;Lienard 2010; Razavi 1993; Razavi 2002; Razavi 2003; Stewart 2007; Tulsky 2011; van Weert 2011;Wilkinson 2008) or in writing (Fallowfield 2002). In addition, Butow 2008 described feedback from the simulated patients, and Goelz 2009 from the participants' peers. No study stated whether the feedback was structured using a check‐list.
Duration of intervention
One trial had very short on‐site training with no follow‐up: Stewart 2007 (six hours). Four trials included on‐site training that lasted 24 hours or less with no follow‐up intervention (two2 days: Fujimori 2011; 24 hours: Razavi 1993; 24 hours over three days:Fallowfield 2002 and Wilkinson 2008).
Seven trials included on‐site training of less than 24 hours but with follow‐up sessions, including:
three‐day course followed by four three‐hour weekly sessions with one‐to‐one supervision (Heaven 2006);
1.5‐day course followed by four 1.5‐hour monthly video conferences (Butow 2008);
one day course with a follow‐up meeting at six weeks (van Weert 2011);
19‐hour course followed by six three‐hour consolidation workshops (Razavi 2003);
18‐hour course with a follow‐up meeting at two months (Kruijver 2001);
11‐hour course followed by one‐to‐one coaching at 12 weeks (Goelz 2009);
1‐hour lecture followed by the use of a CD‐ROM for one month (Tulsky 2011).
Three trials had longer on‐site training: 38 hours (Gibon 2011), 40 hours (Lienard 2010) and 105 hours (Razavi 2002).
Some on‐site training was on consecutive days (Fallowfield 2002: three‐day residential course; Wilkinson 2008: three days; Fujimori 2011: two days); other on‐site training was spread over a longer period of time (Kruijver 2001; Lienard 2010; Razavi 1993; Razavi 2002; Razavi 2003), ranging from weekly for three weeks (Razavi 2003) to bimonthly over an eight‐month period (Lienard 2010).
Measurement of Outcomes
Primary Outcomes
Most studies measured outcomes before and after the CST (or no CST). Changes in HCP behaviour were measured in interviews involving simulated and/or real patients as follows.
simulated patients only: five trials (Fujimori 2011; Gibon 2011; Goelz 2009; Razavi 1993; Stewart 2007);
real patients only: four trials (Fallowfield 2002; Heaven 2006; Tulsky 2011; van Weert 2011);
real and simulated patients: five trials (Butow 2008; Kruijver 2001; Lienard 2010; Razavi 2002; Razavi 2003).
One trial measured HCP behaviour in interviews with simulated patients only when real patients were not available, however, the data were analysed together (Wilkinson 2008). It is not clear whether the patients in the study by Fujimori 2011 were simulated or real, or how many patient encounters were evaluated. Without counting Fujimori 2011, investigators reported on a total of 1,761 tapes of simulated patient encounters and 1,932 tapes of real patient encounters.
The number of real patient interviews per HCP, assessed at each assessment point, ranged from one (Razavi 2002; Razavi 2003) to six (Kruijver 2001). Interviews were mostly assessed using audio recording (Gibon 2011; Heaven 2006; Lienard 2010; Razavi 2002; Razavi 2003; Stewart 2007; Tulsky 2011) or video recording (Butow 2008; Fallowfield 2002; Goelz 2009; Kruijver 2001; Razavi 1993; Razavi 2002; Razavi 2003; Wilkinson 2008). The Fujimori 2011 abstract does not describe how participants were assessed.
HCP communication skills were evaluated using a variety of scales (see Table 9). Almost every trial used its own unique scale; only two scales were used in more than one study: the Cancer Research Campaign Workshop Evaluation Manual (CRCWEM) (Booth 1991) (Razavi 1993; Razavi 2002; Razavi 2003); and LaComm, a French Communication Analysis Software (LaComm; Gibon 2010) (Gibon 2011; Lienard 2010). Most studies mention that their scale had been validated. The scales had an average of 25 variables (range six to 84). Most studies used more than one rater, and the inter‐rater reliability was considered acceptable by the authors and ranged from 0.49 to 0.94.
Table 1.
Scales used to measure HCP communication skills
| Abbreviation | Name of scale | Studies included in review that used scale | Validation reference (if any) |
| Com‐on | COMmunication challenges in ONcology | Goelz 2009 | Stubenrauch 2012 |
| CRCWEM | Cancer Research Campaign Workshop Evaluation Manual | Razavi 1993; Razavi 2002; Razavi 2003 | Booth 1991 |
| CSRS | Communication Skills Rating Scale | Wilkinson 2008 | Wilkinson 1991 |
| HPSD | Harvard Third Psychosociological Dictionary | Razavi 2002 | |
| LaComm | LaComm | Gibon 2011; Lienard 2010; Razavi 2002 |
Gibon 2010 http://www.lacomm.be/index.php |
| MIARS | Medical Interview Aural Rating Scale | Heaven 2006 | Heaven 2001 |
| MIPS | Medical Interaction Process System | Fallowfield 2002 | Ford 2000 |
| MRID | Martindale Regressive Imagery Dictionary | Razavi 2002 | |
| PCCM | Patient Centred Communication Measure | Stewart 2007 | Brown 1995 |
| QUOTE | Quality of Care through Patient's Eyes | van Weert 2011 | van Weert 2009 |
| RIAS | Roter Interaction Analysis System | Kruijver 2001 |
http://www.riasworks.com/background.html Roter 2002; Ong 1998 |
All the trials included measurement of outcomes relating to HCPs' supportive/building relationship skills (Table 10). One study measured supportive skills only for HCPs outcomes (Tulsky 2011). Other frequently measured outcomes related to:
Table 2.
Types of HCP communication skills *
| Outcome | Definition | Examples |
| Information gathering skills | ||
| Open questioning techniques | Questions or statements designed to introduce an area of inquiry without unduly shaping or focusing the content of the response. | "How are you doing?"; "Tell me how you've been getting on since we last met..." |
| Half‐open questioning techniques | Questions that limit the response to a more precise field. | "What makes your headaches better or worse?" |
| Closed questioning technique | Questions for which a specific often one‐word answer such as yes or no is expected, limiting the response to a narrow field set by the questioner. | "Do you have nausea?"; "How many days have you had the headaches for?" |
| Eliciting concerns | A combination of open and closed questions to make a precise assessment of the patients perspective. | "Tell me more about it from the beginning..."; "What worries you the most?"; "What do you think might be happening?" |
| Clarifying/summarising | Checking out statements that are vague or need amplification and summarising (the deliberate step of making an explicit verbal summary to verify ones understanding of what the patient said). | "Could you explain what you mean by light headed?" "Can I just see if I have got it right? You have had headaches before, but over the last two week you have had a different sort of pain . . . " |
| Explanation and Planning | ||
| Giving appropriate information | The correct amount and type of information (procedural, medical , psychological) to address patient needs and facilitate understanding. | ''There are three important things I want to explain today. First I want to tell you what I think is wrong, second what tests we should do, and third what treatment options are available.'' |
| Checking understanding | Checking patients understanding by direct questions or asking the patient to restate in own words | "Do you understand what I mean?"; |
| Negotiating | Negotiating procedure or future arrangements by taking into account the patient's concerns. | ''Do you mind if I examine you today? Would you prefer it if your husband came with you?'' |
| Supportive or relationship building skills | ||
| Acknowledging concerns | Verbalising the thoughts and concerns expressed by the patient, and express acceptance. | "I can see that you are worried by all this"; "I sense that you feel uneasy about having to come to see me ‐ that's ok, many people feel that way when they first come here." |
| Showing empathy | Verbalising the feelings and emotions expressed by the patient. | ''I can sense how angry you have been feeling about your illness. I can understand that it must be frightening to think the pain will come back.'' |
| Reassurance | To reassure appropriately about a potential discomfort or uncertainty without providing false reassurance. | ''I will do my best to help you.'' |
*Adapted from Silverman 2005 and LaComm.
information gathering e.g. open questions (10 studies: Butow 2008; Fallowfield 2002; Gibon 2011; Heaven 2006; Kruijver 2001; Lienard 2010; Razavi 1993; Razavi 2002; Razavi 2003; Wilkinson 2008); clarifying or summarising (seven studies: Fallowfield 2002; Gibon 2011; Goelz 2009; Kruijver 2001; Razavi 1993; Razavi 2002; Razavi 2003) and eliciting concerns (eight studies: Butow 2008; Goelz 2009; Heaven 2006; Kruijver 2001; Razavi 1993; Razavi 2002; Razavi 2003; Stewart 2007);
explaining and planning e.g. appropriate information giving (nine studies: (Fallowfield 2002; Fujimori 2011; Goelz 2009; Lienard 2010; Razavi 2002; Razavi 2003; Stewart 2007; van Weert 2011: Wilkinson 2008) and negotiating (seven studies: Butow 2008; Gibon 2011; Heaven 2006; Lienard 2010; Razavi 1993; Razavi 2003; Stewart 2007).
Secondary Outcomes
Other HCP outcomes that were measured in these studies included:
HCP health status (six trials: Butow 2008; Kruijver 2001; Lienard 2010; Razavi 1993; Razavi 2002; Razavi 2003);
HCP perception of the interview (three trials: Fallowfield 2002; Razavi 2002; Razavi 2003);
HCP perception of their behaviour change (eight trials: Fallowfield 2002; Fujimori 2011; Gibon 2011; Kruijver 2001; Razavi 2002; Razavi 2003; Tulsky 2011; Wilkinson 2008);
HCP perception of their attitude change (eight trials: Butow 2008; Fallowfield 2002; Kruijver 2001; Lienard 2010; Razavi 1993; Razavi 2002; Razavi 2003; Wilkinson 2008).
We considered HCP perceptions to be very subjective outcomes and so excluded these from our review.
Patient outcomes were measured in 11 trials (Butow 2008; Fallowfield 2002; Fujimori 2011; Kruijver 2001; Lienard 2010; Razavi 2002; Razavi 2003; Stewart 2007; Tulsky 2011; van Weert 2011; Wilkinson 2008) including:
patients' perception of the interview (nine trials: Fallowfield 2002; Fujimori 2011; Kruijver 2001; Lienard 2010; Razavi 2002; Razavi 2003; Stewart 2007; Tulsky 2011; Wilkinson 2008);
patient health status (seven trials: Butow 2008; Fujimori 2011; Kruijver 2001; Razavi 2003; Stewart 2007; Wilkinson 2008);
objective measure of patients communication (five trials: Kruijver 2001; Lienard 2010; Razavi 2002; Razavi 2003; van Weert 2011).
Two trials measured HCP communication with 'significant others' (Goelz 2009; Razavi 2003); one trial measured the satisfaction of 'significant others' (Razavi 2003).
All secondary outcomes except the objective measurement of patient communication were measured with questionnaires, most of which were developed locally and it was not always stated whether they had been previously validated (see Table 11 and Table 12). The following validated questionnaires were used:
Table 3.
Scales used for other HCP outcomes
| Abbreviation | Name of scale | Studies included in review that used scale | Validation reference (if any) |
| MBI | Masslach Burnout inventory | Butow 2008; Kruijver 2001;Lienard 2010 | Schaulell 1993 |
| NSS | Nursing Stress Scale | Razavi 1993; Razavi 2002 | Gray‐Toft 1981 |
| PPSB | Physician Psychosocial Belief questionnaire; | Fallowfield 2002 | Ashworth 1984 |
| SDAQ | Semantic Differential Attitude Questionnaire | Razavi 1993; Razavi 2002 | Silberfarb 1980 |
Table 4.
Scales for measuring patient outcomes
| Abbreviation | Name of scale | Studies included in review that used scale | Validation reference (if any) |
| BSI | Brief Symptom Inventory | Stewart 2007 | Derogatis 1977 |
| CDIS | Cancer Diagnostic Interview Scale | Stewart 2007 | Roberts 1994 |
| EORTC QLQ‐C30: | European Organisation for Research and Treatment of Cancer, Quality of Life Questionnaire‐Core 30; (hjemster) Aaronson 1993 | Butow 2008; Kruijver 2001 | Aaronson 1993; Hjermstad 1995 |
| GHQ‐12 | General health Questionnaire | Wilkinson 2008 | Williams 1988 |
| HADS | Hospital Anxiety and Depression Scale | Butow 2008; Razavi 2003 | Snaith 1986; Julian 2011 |
| PIQ | Perception of Interview Questionnaire | Razavi 2003 | |
| PPPC | Patients perception of patient centeredness | Stewart 2007 | Henbest 1990 |
| PSCQ | Patient Satisfaction with Communication Questionnaire | Fallowfield 2002; Wilkinson 2008 | Ware 1983 |
| PSIAQ | Patient Satisfaction with Interview Assessment Questionnaire | Razavi 2002 | |
| PSQ‐C | Patient Satisfaction Questionnaire (PSQ‐C) | Kruijver 2001 | Blanchard 1986 |
| SCNS | Supportive Care needs survey (Boyes) | Butow 2008 | Samson‐Fisher 2000 |
| STAI‐S | State Trait Anxiety Inventory‐State | Razavi 2003; Wilkinson 2008 |
Speilberger 1983 http://www.theaaceonline.com/stai.pdf Julian 2011 |
| Single item ( Feel better?) | Stewart 2007 | Henbest 1990 |
HCP health status: Maslach Burnout Inventory (MBI) (used by Butow 2008; Kruijver 2001; Lienard 2010; Razavi 2003);
patients' perception of or satisfaction with the interview (used by Fallowfield 2002; Butow 2008; Razavi 2002; Razavi 2003; Stewart 2007; Wilkinson 2008);
-
patient health status:
General Health Questionnaire 12 or GHQ12 (used by Fallowfield 2002; Wilkinson 2008);
European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire‐30 or QLQ‐C30 (used by Butow 2008; Kruijver 2001);
Hospital Anxiety and Depression Scale (HADS) (used by Butow 2008; Razavi 2002; Razavi 2003);
Speilberger's State Trait Anxiety Inventory (STAI‐S) (used by Razavi 2003; Wilkinson 2008).
Timing of the measurement of outcomes
Most studies measured communication skills prior to the intervention (within one to four weeks) and after a post‐intervention period (between one week and six months). Two studies had a further measurement at 12 and 15 months post‐intervention respectively (Butow 2008; Fallowfield 2002). Three studies evaluated the effects of follow‐up CST interventions conducted between one and six months after the preliminary CST intervention (Heaven 2006; Razavi 2003; Tulsky 2011).
Excluded studies
We excluded 118 studies in total, 48 of which were excluded in the original review (November 2001 and November 2003 searches) (see Figure 2). From the updated search, we excluded 80 full text records (pertaining to 70 studies). Of the 118 studies excluded, 97 of these studies were either not RCTs, or were not intervention studies of communication skills training. We excluded the remaining 21 RCTs for the following reasons:
CST for patients not HCPs (de Bie 2011; Clark 2009; Shields 2010; Street 2010; Smith 2010; Rosenbloom 2007);
CST in HCPs who did not work specifically in cancer care (Brown 1999; Hainsworth 1996; Roter 1995; Szmuilowicz 2010; Wetzel 2011);
intervention was not CST (Cort 2009);
CST was aimed at facilitating recruitment of patients to trials (Wuensch 2011);
CST was only measured in the intervention group not the control group (Fukui 2008);
HCP behaviour change was not measured or was self‐assessed (Bernard 2010; Brown 2012; Claxton 2011; Hundley 2008; Ke 2008; Pelayo 2011; Rask 2009).
Risk of bias in included studies
We considered studies to be at a low risk of overall bias if we assessed the individual 'risk of bias' criteria as 'low risk' in 3/6 criteria. As a result, we considered 12 of the 15 included RCTs to be at a low risk of overall bias (see Characteristics of included studies and Figure 1).
Randomisation was computer‐generated in four trials (Goelz 2009; Lienard 2010; Tulsky 2011; Wilkinson 2008); by random number tables in two trials (Butow 2008; Stewart 2007); and was not described in nine trials. Allocation concealment was described in six trials (Butow 2008; Goelz 2009; Lienard 2010; Razavi 1993; Stewart 2007; Tulsky 2011) and unclear (not described) in nine trials.
Blinding of participants was not possible in these trials, however, outcome assessment was clearly stated as blinded in nine of the 15 trials. Most studies pre‐specified their outcomes and reported their pre‐specified primary outcomes. The following studies stated measuring some patient outcomes, however, did not report these results: Fallowfield 2002; Razavi 2002 and Razavi 2003. Loss to follow‐up in relation to the primary outcomes was unclear in seven trials and considered 'low risk' in eight trials with attrition rates ranging from 0% to 20%.
Three studies reported differences between the study groups in baseline characteristics of the HCPs (Gibon 2011; Goelz 2009; Wilkinson 2008) or patients (Razavi 2003). In two studies that measured outcomes at several points in time, it was unclear which participant interviews were included in their analyses (Lienard 2010; van Weert 2011). In Fujimori 2011, the study methods provided in the abstract were very limited, therefore, we considered all 'risk of bias' criteria to be 'unclear'. We expect that these study methods will be clearly described when this study is published in full.
Effects of interventions
See: Table 1
CST compared to no CST
A. HCP outcomes
A.1. Communication skills
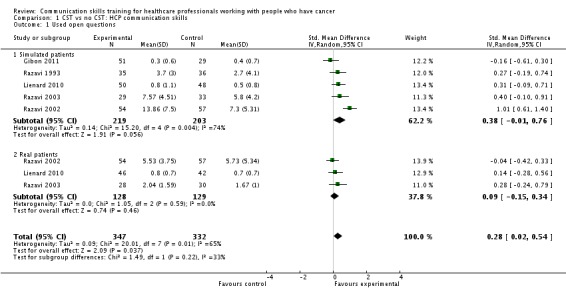
Six studies (Gibon 2011; Lienard 2010; Razavi 1993; Razavi 2002; Razavi 2003; Tulsky 2011) contributed data to these meta‐analyses: four of these studies contributed data to the 'simulated patients' subgroup and four contributed data to the 'real patients' subgroup. HCPs in these studies included 233 doctors (three studies: Lienard 2010; Razavi 2003; Tulsky 2011), 188 nurses (Razavi 1993; Razavi 2002), and one mixed group/radiotherapy team of 80 HCPs (Gibon 2011). At the post‐intervention assessment, HCPs in the intervention group were statistically significantly more likely than the control group to:
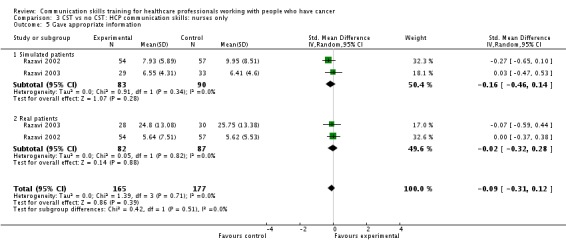
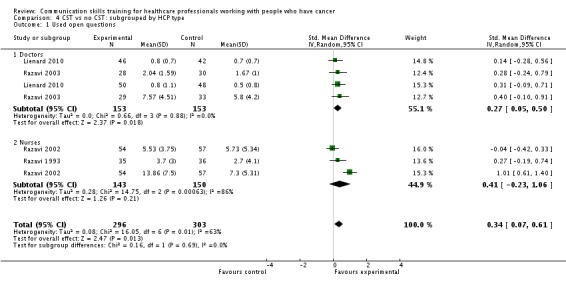
use open questions (five studies, 679 participant interviews; standardised mean difference (SMD) 0.28, 95% confidence interval (CI) 0.02 to 0.54; Analysis 1.1; P = 0.04, I² = 65%);
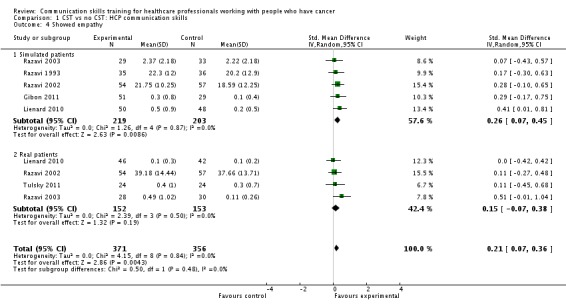
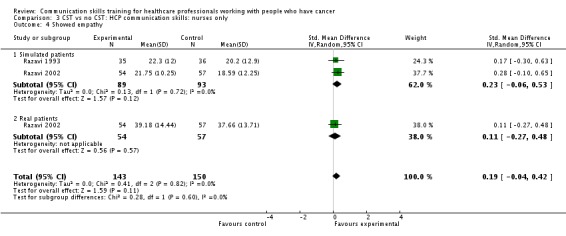
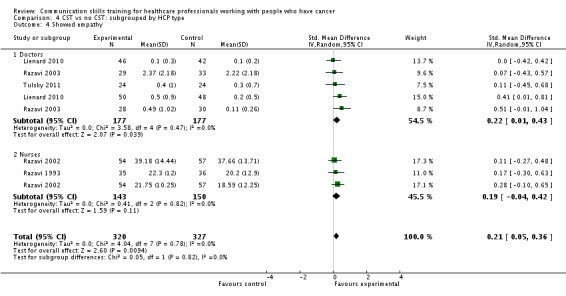
show empathy (six studies, 727 participant interviews; SMD 0.21, 95% CI 0.07 to 0.36; Analysis 1.4; P = 0.004, I² = 0%).
Analysis 1.1.
Comparison 1 CST vs no CST: HCP communication skills, Outcome 1 Used open questions.
Analysis 1.4.
Comparison 1 CST vs no CST: HCP communication skills, Outcome 4 Showed empathy.
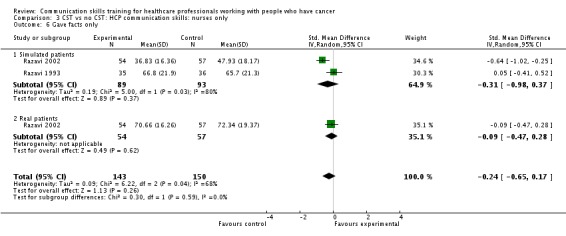
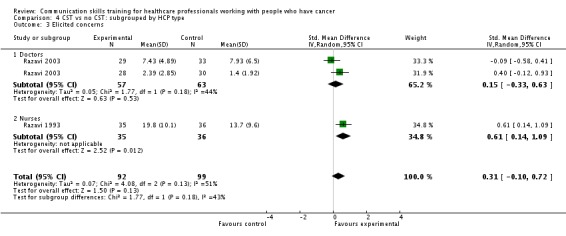
There were no statistically significant differences between the intervention and control groups with regard to the following HCP outcomes: clarifying and/or summarising, eliciting concerns, giving appropriate information, giving facts only and negotiation. However, in the subgroup of 'simulated' patients only, HCPs in the intervention group were also:
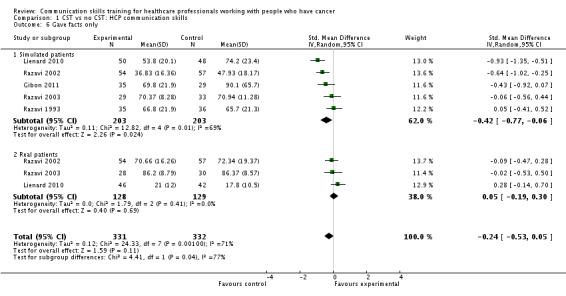
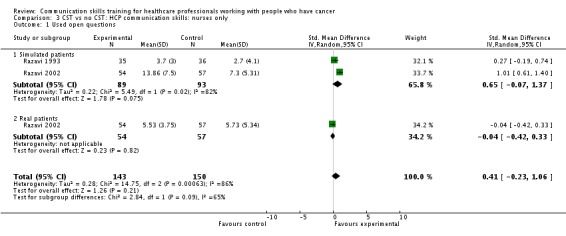
significantly less likely to 'give facts only' (five studies, 406 participant interviews; SMD ‐0.42, 95% CI ‐0.77 to ‐0.06; Analysis 1.6; P = 0.02, I² = 69%). P = 0.04 for subgroup differences.
Analysis 1.6.
Comparison 1 CST vs no CST: HCP communication skills, Outcome 6 Gave facts only.
Other HCP communication skills that were evaluated in some studies but that were either not included in our 'Types of outcome measures', or that gave insufficient data for inclusion in meta‐analyses (e.g. only gave P values), included the following.
Emotional depth: Gibon 2011 and Kruijver 2001 reported significantly greater emotional depth in the intervention groups compared with the control groups, P = 0.03 and P = 0.05, respectively.
Empathy: Butow 2008 found less empathy in intervention group compared with the control group at six months post‐intervention (P = 0.024).
Checking that the patient understands: Kruijver 2001 reported significantly less checking of patient understanding in the CST group than in the control group; whereas Fallowfield 2002 and Goelz 2009 reported no significant difference between the groups.
Emotional support: Fujimori 2011 reported an 'improvement' in emotional support scores in the intervention group compared with the control group. It is not stated whether this improvement was statistically significant.
Appropriate information: There was less appropriate information giving in the CST groups than the control groups in Kruijver 2001 (P < 0.05), Lienard 2010 (P < 0.001) and van Weert 2011 (P < 0.01). Fujimori 2011 reported an 'improvement' in information‐giving skills in the CST group compared with the control group.
Team orientated focus: Gibon 2011 reported greater team orientated focus in favour of the intervention group (P = 0.023).
Blocking behaviours: No significant effect of CST was found by Butow 2008 (P = 0.66), Heaven 2006 and Razavi 1993; whereas, Wilkinson 2008 found significantly less blocking behaviour in the intervention group (P = 0.001).
Global score: Wilkinson 2008 and Goelz 2009 reported significantly better global communication scores for the CST groups than the control groups (P < 0.001 and P = 0.007, respectively).
Doctors only
Three studies enrolling doctors contributed data to these subgroup analyses (Lienard 2010; Razavi 2003; Tulsky 2011); the results were consistent with the main findings. At the post‐intervention assessment, doctors in the intervention group were statistically significantly more likely than those in the control group to:
use open questions (two studies, 306 participant interviews; SMD 0.27, 95% CI 0.05 to 0.50; Analysis 2.1; P = 0.02, I² = 0%);
show empathy (two studies, 354 participant interviews; SMD 0.22, 95% CI 0.01 to 0.43; Analysis 2.4; P = 0.04, I² = 0%).
Analysis 2.1.
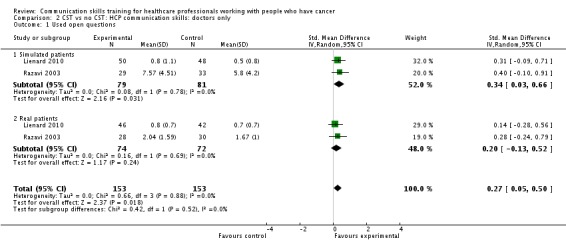
Comparison 2 CST vs no CST: HCP communication skills: doctors only, Outcome 1 Used open questions.
Analysis 2.4.
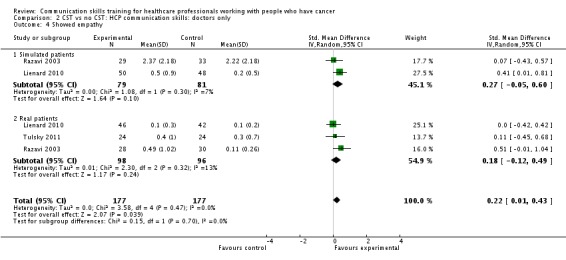
Comparison 2 CST vs no CST: HCP communication skills: doctors only, Outcome 4 Showed empathy.
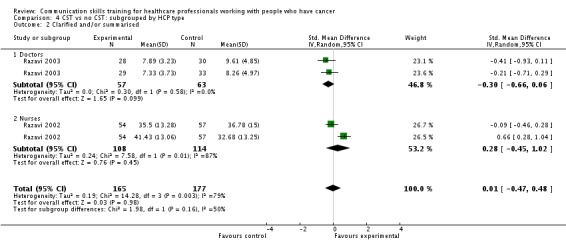
There were no statistically significant differences between the intervention and control groups in the meta‐analyses of the following outcomes: clarifying and summarising, eliciting concerns, giving appropriate information and giving facts only.
Nurses only
Only two studies contributed data to these subgroup analyses (Razavi 1993; Razavi 2002). At the post‐intervention assessment, there were no statistically significant differences between the intervention and control groups in any of the meta‐analyses (Analysis 3.1; Analysis 3.4; Analysis 3.5; Analysis 3.6).
Analysis 3.1.
Comparison 3 CST vs no CST: HCP communication skills: nurses only, Outcome 1 Used open questions.
Analysis 3.4.
Comparison 3 CST vs no CST: HCP communication skills: nurses only, Outcome 4 Showed empathy.
Analysis 3.5.
Comparison 3 CST vs no CST: HCP communication skills: nurses only, Outcome 5 Gave appropriate information.
Analysis 3.6.
Comparison 3 CST vs no CST: HCP communication skills: nurses only, Outcome 6 Gave facts only.
Sensitivity analyses
We performed sensitivity analyses of our primary HCP outcomes to exclude studies that evaluated follow‐up interventions, i.e. Razavi 2003 and Tulsky 2011. We noted the following effects:
Analysis 1.1: the use of 'open questions' became no longer statistically significant (four studies, participant interviews; SMD 0.26; 95% CI ‐0.08 to 0.60; P = 0.13; I² = 75%);
Analysis 1.4: showing 'empathy' remained statistically significant when these two studies were excluded (four studies, participant interviews; 0.21 95% CI 0.04 to 0.38; P = 0.010; I² = 0%);
the results of the other primary analyses either remained either very similar to the original analyses, or they contained insufficient studies for meta‐analyses to be performed.
We also performed subgroup analyses to determine whether there were significant differences in primary outcomes between nurses and doctors participating in these trials (Analysis 4.1; Analysis 4.2; Analysis 4.3; Analysis 4.4; Analysis 4.5; Analysis 4.6), however, tests for subgroup differences were not significant.
Analysis 4.1.
Comparison 4 CST vs no CST: subgrouped by HCP type, Outcome 1 Used open questions.
Analysis 4.2.
Comparison 4 CST vs no CST: subgrouped by HCP type, Outcome 2 Clarified and/or summarised.
Analysis 4.3.
Comparison 4 CST vs no CST: subgrouped by HCP type, Outcome 3 Elicited concerns.
Analysis 4.4.
Comparison 4 CST vs no CST: subgrouped by HCP type, Outcome 4 Showed empathy.
Analysis 4.5.
Comparison 4 CST vs no CST: subgrouped by HCP type, Outcome 5 Gave appropriate information.
Analysis 4.6.
Comparison 4 CST vs no CST: subgrouped by HCP type, Outcome 6 Gave facts only.
A.2. Other HCP outcomes
Two studies (Kruijver 2001; Razavi 2003) contributed data to meta‐analyses relating to HCP 'burnout'. Kruijver 2001 enrolled nurses and Razavi 2003 enrolled doctors (62% were oncologists). Burnout was measured using the Maslach Burnout Inventory (MBI). For the outcome 'emotional exhaustion' there was no statistically significant difference in mean scores between the intervention and control groups (106 participant interviews: SMD ‐0.25, 95% CI ‐0.67 to 0.18; Analysis 5.1; P = 0.25, I² = 16%). Butow 2008 also reported 'burnout' and found no significant effect of CST on this outcome, however did not report these data in a usable form for this meta‐analysis. For the outcome 'personal accomplishment' there was no statistically significant difference between the intervention and control groups (91 participant interviews; SMD 0.26, 95% CI ‐0.24 to 0.76; Analysis 5.2; P = 0.30, I² = 25%).
Analysis 5.1.
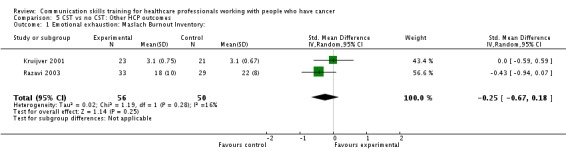
Comparison 5 CST vs no CST: Other HCP outcomes, Outcome 1 Emotional exhaustion: Maslach Burnout Inventory:.
Analysis 5.2.
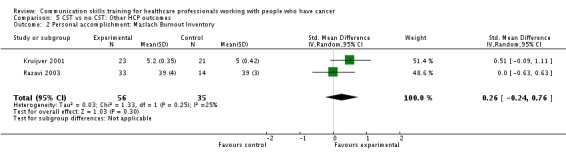
Comparison 5 CST vs no CST: Other HCP outcomes, Outcome 2 Personal accomplishment: Maslach Burnout Inventory.
B. Patient outcomes
Two studies (Razavi 2003; Wilkinson 2008) evaluated 'patient anxiety' using the Spielberger State of Anxiety Inventory (STAI‐S). Anxiety scores decreased in both groups in both studies after all the interviews, however, the mean reduction in anxiety scores (pre‐ and post‐interview) was significantly greater in the control group (169 participant interviews; SMD 0.40; 95% CI 0.07 to 0.72; Analysis 6.2; P = 0.02; I² = 8%).
Analysis 6.2.
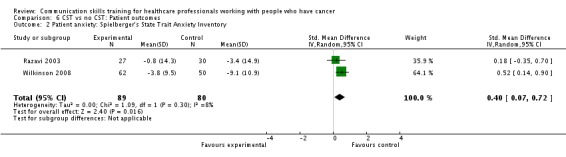
Comparison 6 CST vs no CST: Patient outcomes, Outcome 2 Patient anxiety: Spielberger's State Trait Anxiety Inventory.
Wilkinson 2008 evaluated patient 'psychiatric morbidity', assessed by the GHQ 12 questionnaire, and found it to be significantly lower in the intervention group than the control group (one study, 127 participant interviews; SMD ‐0.36, 95% CI ‐0.71 to ‐0.01; Analysis 6.1; P = 0.05), however, this study reported significantly greater baseline anxiety in the control group.
Analysis 6.1.
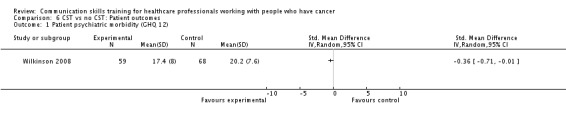
Comparison 6 CST vs no CST: Patient outcomes, Outcome 1 Patient psychiatric morbidity (GHQ 12).
Two studies contributed data to each of the outcomes 'patient perception of HCP communication skills' (Analysis 6.3; Razavi 2002; Razavi 2003) and 'patient satisfaction with communication' (Analysis 6.4; Fallowfield 2002; Wilkinson 2008). There were no statistically significant differences in either of these outcomes between the groups.
Analysis 6.3.
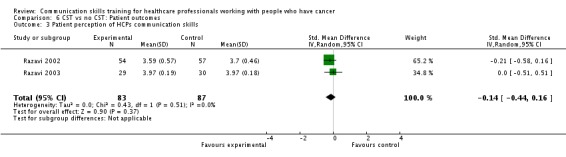
Comparison 6 CST vs no CST: Patient outcomes, Outcome 3 Patient perception of HCPs communication skills.
Analysis 6.4.
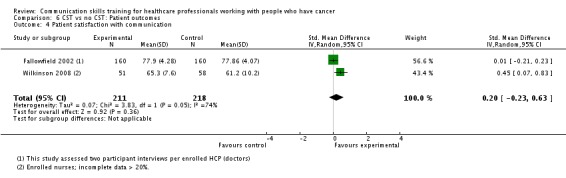
Comparison 6 CST vs no CST: Patient outcomes, Outcome 4 Patient satisfaction with communication.
Patient outcomes that were either not included in our 'Types of outcome measures', or that gave insufficient data for inclusion in meta‐analyses (e.g. only gave P values), included the following.
Patient trust: Tulsky 2011 reported significantly greater patient trust in the intervention group (P = 0.036).
Quality of life: Kruijver 2001 found statistically significant improvement in only 1/30 items; and Butow 2008 found no statistically significant differences.
Recall of information: van Weert 2011 reported a 'marginally significant' improvement in patient recall following HCP CST.
Anxiety: Butow 2008 reported a statistically significant reduction in patient anxiety (telephone interviews) one week after the consultation in the intervention group (P = 0.021). This change was not maintained in telephone interviews three months later.
Depression: Butow 2008 found no statistically significant difference in patient depression (telephone interviews) at one week after the consultation in the intervention group.
Distress: Fujimori 2011 reported that distress scores were 'significantly decreased' in the intervention group compared with the control group.
Satisfaction: Fujimori 2011 reported 'no significant difference' in satisfaction between patients of the intervention group and the control group.
C. 'Significant other' outcomes
One study (Razavi 2003) reported no statistically significant differences in relatives' anxiety or satisfaction between intervention and control groups, however the data given were insufficient for meta‐analysis. Goelz 2009 found statistically significant improvements in some HCP behaviour in relation to relatives in simulated interviews (P < 0.001).
D. Effect of CST over time
Two trials studied the effect of CST up to one year after the intervention. Butow 2008 reported that clinically significant improvements in doctors communication skills at six months were maintained at 12 months in the group that received CST, however these improvements were not statistically significant. Doctors in the intervention group scored lower on responding to distress than the control group at 12 months.
Fallowfield 2002 evaluated all participants at three months post‐intervention, and evaluated the intervention group only at 15 months post‐intervention. For the intervention group doctors, most statistically significant benefits of CST (appropriate questions and responses) displayed at three months were maintained at 15 months, however, there was a drop off in empathy scores (P < 0.001). At 15 months post‐intervention, the investigators also noted a significant improvement in the HCPs' summarising of information for the patients (P = 0.038), and that they interrupted less (P < 0.001) than at the three‐month assessment.
Follow‐up CST compared with no follow‐up CST
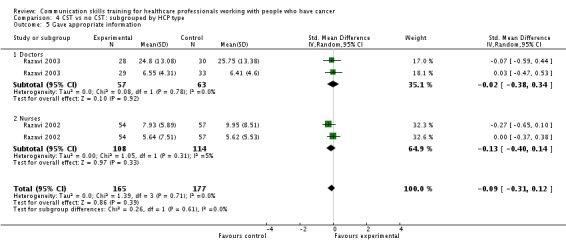
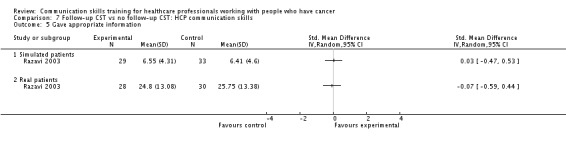
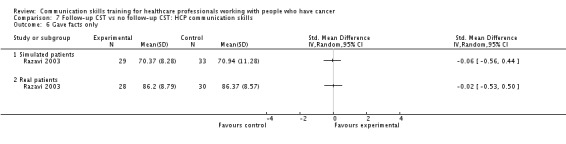
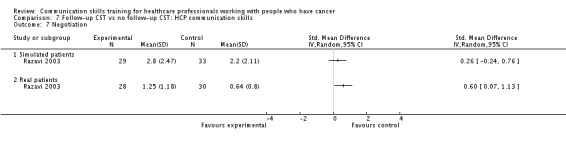
Three trials studied the effect of follow‐up interventions (Heaven 2006; Razavi 2003; Tulsky 2011), however, they reported little data that we could use in our meta‐analyses, most of which (Analysis 7.1; Analysis 7.2; Analysis 7.3; Analysis 7.4; Analysis 7.5; Analysis 7.6; Analysis 7.7) contain data from only one study (Razavi 2003). However, meta‐analysis of two studies was possible for the outcome 'empathy'. We found no significant difference between the intervention and control groups with regard to this outcome (two studies, 168 participant interviews; SMD 0.23, 95% CI ‐0.07 to 0.54; P = 0.14; I² = 0%) (Analysis 7.4).
Analysis 7.1.
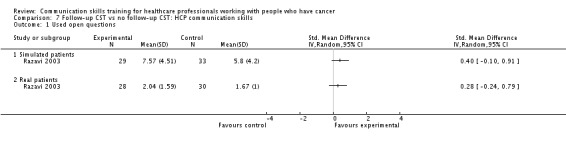
Comparison 7 Follow‐up CST vs no follow‐up CST: HCP communication skills, Outcome 1 Used open questions.
Analysis 7.2.
Comparison 7 Follow‐up CST vs no follow‐up CST: HCP communication skills, Outcome 2 Clarified and/or summarised.
Analysis 7.3.
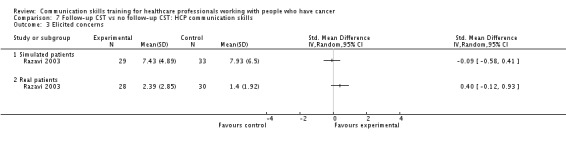
Comparison 7 Follow‐up CST vs no follow‐up CST: HCP communication skills, Outcome 3 Elicited concerns.
Analysis 7.4.
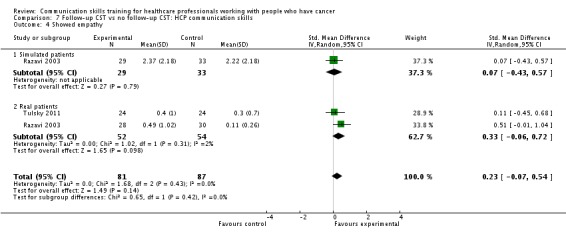
Comparison 7 Follow‐up CST vs no follow‐up CST: HCP communication skills, Outcome 4 Showed empathy.
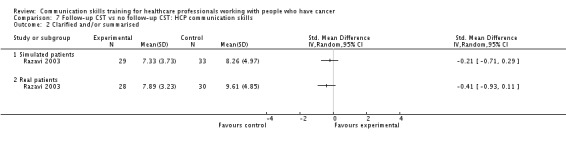
Analysis 7.5.
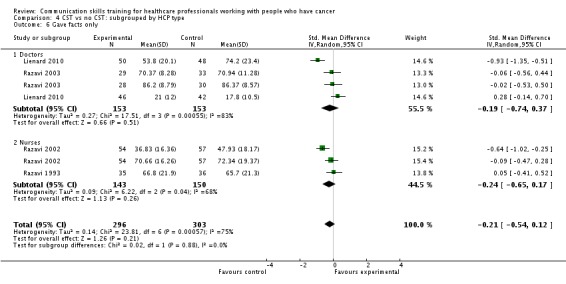
Comparison 7 Follow‐up CST vs no follow‐up CST: HCP communication skills, Outcome 5 Gave appropriate information.
Analysis 7.6.
Comparison 7 Follow‐up CST vs no follow‐up CST: HCP communication skills, Outcome 6 Gave facts only.
Analysis 7.7.
Comparison 7 Follow‐up CST vs no follow‐up CST: HCP communication skills, Outcome 7 Negotiation.
Individually, these studies reported the following.
Razavi 2003 reported some statistically significant improvements in doctors' communication skills after a single 2.5‐day CST workshop followed by six, bimonthly, three‐hour consolidation workshops compared with a single 2.5‐day CST workshop only. These significant improvements included: open questions in simulated interviews (P = 0.014); checking understanding ( P = < 0.01); and empathic statements in real patient interviews (P = 0.009) and in interviews where a relative was present. In addition, patients interviewed by doctors who received the follow‐up CST perceived that their doctor had a better understanding of their disease than patients of doctors who received no follow‐up CST (P = 0.04). The follow‐up CST had no significant effect on patient satisfaction or anxiety levels, except in interviews with relatives, where the patients, but not the relatives, were reported to be more globally satisfied (P = 0.024).
Tulsky 2011 reported a statistically significant improvement in oncologists communication skills in interviews with real patients after a CST lecture and the use of a follow‐up CD‐ROM, compared with a control group who had received a CST lecture only: Empathic statements (P = 0.024) and 'response to empathic opportunity' (P = 0.03) were improved in the intervention group. Patient trust also improved (P = 0.036).
Heaven 2006 failed to show any difference in nurses' communication skills in real patient encounters after receiving a three‐day CST course followed by four half‐day supervision sessions spread over four weeks, compared with the three‐day CST course only.
Comparison of different types of CST
One trial with 51 participants (18 oncologists, 17 family physicians and 16 surgeons) compared a six‐hour student‐centred, experiential CST, to a two‐hour small‐group discussion commenced with a video (Stewart 2007). No statistically significant differences were found between the groups in HCP behaviour outcomes in the post‐intervention simulated interviews, however, in the subgroup analysis of family physicians, those who participated in the six‐hour course showed better scores in offering support (P = 0.02), information sharing (P = 0.05), and exploring and validating whole person issues (P = 0.02 and P = 0.05, respectively) compared with those who participated in the two‐hour course. In the subgroup of surgeons, patient satisfaction and perception of well‐being improved after the six‐hour course (P = 0.02 and P=0.03 respectively). Overall, there was no significant effect on the patients' psychological distress; however, using a single validated question, more patients "felt better" with HCPs who had undergone the six‐hour training course than with HCP participants of the two‐hour course (P = 0.02).
Feedback compared to no feedback
Only one study reported this comparison (Fallowfield 2002) and found no significant differences between HCP communication skills in groups receiving 'feedback' or 'no feedback'.
Discussion
Summary of main results
We performed meta‐analyses of seven HCP communication skill outcomes (using open questions, clarifying/summarising, eliciting concerns, showing empathy, giving appropriate information, giving facts only and negotiating), two 'other' HCP outcomes relating to 'burnout '(emotional exhaustion, personal accomplishment) and four patient outcomes (psychiatric morbidity, anxiety, perception of HCP communication, satisfaction with HCP communication). Overall, 10 studies contributed data to the meta‐analyses.
HCPs in the intervention groups were statistically significantly more likely to use open questions in the post‐intervention interviews than the control group (five studies, 679 participant interviews; P = 0.04, I² = 65%); they were also statistically significantly more likely to show empathy towards their patients (six studies, 727 participant interviews; P = 0.004, I² = 0%). We considered these findings to be of a moderate and high quality, respectively (see Table 1). In subgroup analyses according to staff type, these benefits of CST remained statistically significant when 'doctors only' were included in the meta‐analyses, but not for 'nurses only', however, doctors and nurses did not perform statistically significantly differently for any HCP outcomes.
There were no statistically significant differences in the other HCP communication skills except for the subgroup of participant interviews with simulated patients, where the intervention group was significantly less likely to present simulated patients with 'facts only' compared with the control group (four studies, 344 participant interviews; P = 0.01, I² = 70%). Tests for subgroup differences (between real and simulated patients) were significant.
HCP 'burnout' was assessed post‐intervention in three studies using the Maslach Burnout Inventory. Two studies could be included in a meta‐analysis: one was conducted in nurses, the other in doctors (mainly oncologists). There were no statistically significant differences between the intervention and control groups with regard to 'emotional exhaustion' (106 participant interviews; P = 0.25, I² = 16%) or 'personal accomplishment' (91 participant interviews; P = 0.30, I² = 25%) when we combined these data. We consider this evidence to be of a low quality.
With regard to patient outcomes, two studies contributed data to the outcome 'patient anxiety'. Meta‐analysis showed a significantly greater reduction in anxiety scores in the control group (169 participant interviews; P = 0.02). In a study of 172 nurses, psychiatric morbidity was found to be statistically significantly lower in the intervention group than the control group (P = 0.05). There were no statistically significant differences in 'patient perception of HCPs communication skills' (two studies, 170 participant interviews) and 'patient satisfaction with communication' (two studies, 429 participant interviews) in meta‐analyses of these outcomes. We consider this evidence to be of a low to very low quality.
Overall completeness and applicability of evidence
These meta‐analyses offer limited evidence that communications skills training of HCPs working in cancer care has a beneficial effect on some HCP communication skills when assessed up to six months after the training course or workshop. The types of skills that showed statistically significant improvement in our meta‐analyses were related to information gathering (open questions) and supportive or relationship‐building skills (empathy).These benefits probably apply to both doctors and nurses as tests for subgroup differences were not statistically significant.
There was a statistically significant difference in the outcome 'give facts only' when we subgrouped studies by the type of patient (real or simulated); HCPs in the simulated patient subgroup were statistically significantly less likely to 'give facts only' compared with controls. As this did not hold true for 'real' patients, it suggests that CST may not always translate into clinically meaningful results. This is supported by the findings of two studies that measured HCP behaviour with identical scales in both real and simulated patients, and reported that the benefits were less when measured in real patients (Kruijver 2001; Razavi 2002).
The types of CST, length of training and time spread were diverse and it was not possible to draw conclusions as to the relative efficacy of the different programs. These results, therefore, are not necessarily applicable to all types of CST. In future versions of this review, it may be desirable to subgroup our results according to intervention type; this was not possible for the current version due to the small number of contributing studies. Furthermore, longer‐term follow‐up is necessary to ascertain whether these skills are retained. In the 15 included studies, the longest follow‐up occurred in Butow 2008 and Fallowfield 2002, at 12 and 15 months post‐intervention, respectively. These studies give conflicting results and we were unable to combine these data in a meta‐analysis.
Three trials (Heaven 2006; Razavi 2003; Tulsky 2011) studied the effects of follow‐up interventions on HCP communication skills and reported some positive effects on the maintenance of behaviour change in clinical practice, however, the longest follow‐up period was six months, and meta‐analyses including these studies were not possible except for the outcome 'empathy', for which we found no statistically significant difference. The efficacy of follow‐up CST is inconclusive based on the available evidence.
Few studies reported patient health‐related outcomes and those that did had little usable data. Evidence for a beneficial effect on patients' psychological and physical health is lacking and further research is needed in this regard. All trials were performed in developed countries and, thus, the results may not be widely applicable to less‐developed regions.
Quality of the evidence
We graded the review evidence according to guidelines from the Cochrane Handbook for Systematic Reviews of Interventions, that supports the GRADE approach, defining the quality of the body of evidence as the extent to which one can be confident that an estimate of effect or association is close to the quantity of specific interest (Higgins 2011). Downgrading of evidence can occur if there are limitations in the design and implementation of available studies, the data are heterogeneous or imprecise reflected by wide confidence intervals, the evidence is indirect or there is a high probability of publication bias.
We consider the evidence related to two primary outcomes, 'empathy' and 'open questions' to be of a high and moderate quality, respectively (see Table 1 for reasons). We downgraded the evidence relating to 'open questions' due to the substantial heterogeneity amongst studies included in the meta‐analysis of this outcome.
The quality of evidence for the other primary outcomes and secondary outcomes is low to very low. This is due to a number of factors including the small numbers of studies with usable data for various meta‐analyses. In addition, the included studies displayed considerable heterogeneity in terms of the types of CST, the types of patients (real or simulated), the outcomes assessed, the measurement tools used to evaluate outcomes, and other variables.
Potential biases in the review process
For the protocol and original 2002 review, we defined 'Types of outcomes' simply as 'changes in behaviour or skills measured using objective and validated scales'. However, for the update, we defined primary and secondary outcomes more clearly. By so doing, we may have introduced bias into the review. In addition, by choosing to extract data and perform meta‐analyses, thereby possibly limiting the review findings to a handful of outcomes, rather than present the data of the 15 studies in a narrative review, we may have introduced bias. Several studies reported other HCP behavioural outcomes (i.e. that were not included in our list of outcomes) and we hope that by presenting these additional data, we have been able to present the wide range of evidence (and quality of evidence) available to inform opinion.
Some trials reported statistically significant effects (both positive and negative) of various HCP communication outcomes but were limited by the inadequate reporting of data such that the data could not be used in meta‐analyses. Types of limited reporting included only giving P values, percentages, or means without numbers assessed or standard deviations. The fact that useable data for these outcomes were not available, may have inherently biased the review. For example, three studies (Kruijver 2001; Lienard 2010; van Weert 2011) individually reported statistically significantly less 'appropriate information giving' in their intervention groups than the control groups, suggesting that CST may negatively impact this outcome, but there were no accompanying extractable data to support the reports. Our meta‐analysis of this outcome included data from only two studies and we found no significant difference between the two groups, although the point‐estimate favoured the control group (Analysis 1.5).
Analysis 1.5.
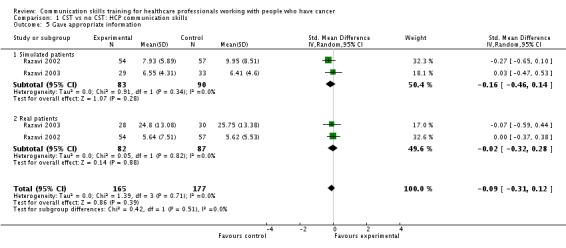
Comparison 1 CST vs no CST: HCP communication skills, Outcome 5 Gave appropriate information.
In some studies, outcomes consisted of phrases, or aspects of scales that we had not included as outcomes for this review. Almost every trial used its own unique scale with an average of 25 variables (range, six to 84); with only two scales used in more than one study. We used standardised mean differences to adjust for these different scales and random‐effects methods for all meta‐analyses, to minimise potential biases.
Lastly, by including data from the studies of follow‐up interventions (three studies) in our meta‐analyses of 'CST versus no CST', we may have introduced bias into our meta‐analyses. All HCPs in these studies received preliminary CST and then subsequently randomised to receive a follow‐up CST intervention. We performed sensitivity analyses to determine what effect including these studies had on our overall results and reported these findings.
Agreements and disagreements with other studies or reviews
Previous reviews Barth 2011; Paul 2009; Uitterhoeve 2010 have consistently concluded that CST leads to better HCP communication behaviours. Barth 2011 included 13 studies (three non‐randomised) and extracted effect sizes for the outcomes HCP behaviour, HCP attitudes and patient outcomes. It is not clear to us how they combined the several aspects of HCP behaviour into a single effect size as the included studies reported diverse behaviour outcomes, however, they report a low to moderate effect of CST on HCP behaviour. Thus, our findings seem to agree. Barth 2011 also performed subgroup analysis to assess the effect of the duration of the CST course on HCP behaviour and reported a trend toward shorter courses being less successful than longer ones; this finding supports the conclusions of Gysels 2004, but we were unable to corroborate these findings.
HCP attitude change is a very subjective outcome and, although CST has been reported in other reviews to have a positive effect on this outcome (Barth 2011), we have not included it in our review. Barth 2011 suggests that the inability to show profound results following CST workshops may be due to the high pre‐intervention competencies in the participants taking part in the CST. This is a good point. Most of our included studies were conducted in oncologists and cancer care nurses with experience ranging from two to 24 years.
We agree with the findings of other reviews (Barth 2011; Paul 2009; Uitterhoeve 2010), that CST in HCPs appears to have little effect on patient outcomes, however high‐quality data for patient outcomes are scarce. The Kissane 2012 review expressed uncertainty as to whether the skills acquired from CST are maintained in the long term; we agree that the long‐term benefits of CST are not clearly established. Our findings support the recommendations for the development of standardised outcome measures for future research in the consensus statement of European experts (Stiefel 2010).
Authors' conclusions
Communication skills training for HCPs working in cancer care using learner‐centred, experiential education methods by experienced facilitators, can result in improvements of some communication skills, particularly gathering information skills and empathy. Whilst improving these information‐gathering and supportive skills, CST courses should also aim to ensure appropriate information‐giving skills in HCP participants. CST appears to have little measurable benefit to the patient and it is unclear whether the skills acquired by HCPs are retained in the long term. In addition, it is unclear what type, duration and intensity of CST is most effective, and whether consolidation workshops may improve the impact of CST.
The original version of this review called for further research and the number of randomised trials has since increased dramatically. However the diversity of studies, particularly in the scales used to measured HCP communication skills, has limited the conclusions of this updated review. We recommend that RCTs use standard validated scales, and that (limited) core study outcomes (both for HCP outcomes and patient outcomes) are identified and pre‐specified. Several validated scales to measure HCP communication now exist (Table 9) but investigators should ensure that their outcomes permit comparability between studies. It may be preferable to use real patients for measurement of HCP communication in studies of CST interventions to ensure clinically meaningful results. Trials should include clear reporting of trial methods and study outcomes, and data should be reported in full e.g. continuous data as means with standard deviations and the number analysed per outcome.
Other Important questions remain unanswered.
The optimal length of training/course structure
The long‐term efficacy of communication skills training
The role of e‐learning
Compulsory rather than voluntary training
The role of consolidation courses
Acknowledgements
We thank the following people for their assistance:
Clare Jess and Gail Quinn, the Managing Editors of the Cochrane Gynecological Cancer Review Group (CGCRG) for their editorial support.
Jane Hayes of the CGCRG in Bath, UK, who conducted the updated searches.Susie Wilkinson (SW) and Deborah Fellows (DF) for their contributions as co‐authors of the original published review. SW wrote the original protocol and DF conducted the original search and wrote the first draft of the original review.
Gabriel Rada and the Unidad de Medicina Basada en Evidencia, P. Universidad Catolica de Chile for statistical advice and constant support.
James Tulsky, Tanja Goeltz and Alexander Wuensch for allowing us pre‐publication access to their trial articles.
The Librarians at the Royal United Hospital in Bath, UK, who assisted us by obtaining several articles for this review.
Chrysi Leliopoulou and Heather Dickinson for their assistance with the original version of this review.
Appendices
Appendix 1. Definition of a simulated patient
A simulated patient (SP) in health education is an individual who is trained to act as a real patient in order to simulate a set of symptoms or problems. An individual SP is typically selected on the basis of gender, body habitus, previous surgeries, past medical history and sometimes level of education and/or language. She/he is matched to a case requirement and trained to reliably portray (and often to accurately recall) details of what was said and done in a medical encounter. SPs may also be trained to provide accurate, written and objective reports by means of checklists. In addition, SPs can be trained to provide patient‐centered, subjective rating and descriptive evaluation of examinee behavior. This can provide a basis for constructive verbal or written post‐encounter feedback to the student by the SP (Adamo 2003).
Appendix 2. CENTRAL search strategy
CENTRAL
#1 MeSH descriptor Medical Oncology explode all trees #2 MeSH descriptor Oncologic Nursing, this term only #3 MeSH descriptor Neoplasms explode all trees #4 MeSH descriptor Palliative Care, this term only #5 (terminal* or palliat* or cancer* or oncol* or hospice*) #6 (#1 OR #2 OR #3 OR #4 OR #5) #7 MeSH descriptor Education, Medical, Continuing, this term only #8 MeSH descriptor Education, Nursing, Continuing, this term only #9 MeSH descriptor Programmed Instruction as Topic explode all trees #10 (train* or educat* or workshop* or module* or teach* or curricul* or learn*) #11 (#7 OR #8 OR #9 OR #10) #12 MeSH descriptor Communication explode all trees #13 communicat* or interview* #14 (#12 OR #13) #15 evaluat* or assess* or critique* or measure* or outcome* or effect* or change* or result* or trial* or prospective* or followup or follow‐up #16 (#6 AND #11 AND #14 AND #15)
Appendix 3. MEDLINE search strategy
MEDLINE Ovid
1 exp Medical Oncology/ 2 Oncologic Nursing/ 3 exp Neoplasms/ 4 Palliative Care/ 5 (terminal* or palliat* or cancer* or oncol* or hospice*).mp. 6 1 or 2 or 3 or 4 or 5 7 Education, Medical, Continuing/ 8 Education, Nursing, Continuing/ 9 exp Programmed Instruction as Topic/ 10 (train* or educat* or workshop* or module* or teach* or curricul* or learn*).mp. 11 7 or 8 or 9 or 10 12 exp Communication/ 13 (communicat* or interview*).mp. 14 12 or 13 15 (evaluat* or assess* or critique* or measure* or outcome* or effect* or change* or result* or trial* or prospective* or followup or follow‐up).mp. 16 6 and 11 and 14 and 15 17 randomized controlled trial.pt. 18 controlled clinical trial.pt. 19 randomized.ab. 20 placebo.ab. 21 clinical trials as topic.sh. 22 randomly.ab. 23 trial.ti. 24 17 or 18 or 19 or 20 or 21 or 22 or 23 25 16 and 24
key: mp=title, original title, abstract, name of substance word, subject heading word, unique identifier
Appendix 4. EMBASE search strategy
EMBASE Ovid
1 exp oncology/ 2 exp oncology nursing/ 3 exp neoplasm/ 4 exp palliative therapy/ 5 (terminal* or palliat* or cancer* or oncol* or hospice*).mp. 6 1 or 2 or 3 or 4 or 5 7 exp medical education/ 8 exp nursing education/ 9 exp continuing education/ 10 (train* or educat* or workshop* or module* or teach* or curricul* or learn*).mp. 11 7 or 8 or 9 or 10 12 exp interpersonal communication/ 13 (communicat* or interview*).mp. 14 12 or 13 15 (evaluat* or assess* or critique* or measure* or outcome* or effect* or change* or result* or trial* or prospective* or followup or follow‐up).mp. 16 6 and 11 and 14 and 15 17 crossover procedure/ 18 double blind procedure/ 19 randomized controlled trial/ 20 single blind procedure/ 21 random*.mp. 22 factorial*.mp. 23 (crossover* or cross over* or cross‐over*).mp. 24 placebo*.mp. 25 (doubl* adj blind*).mp. 26 (singl* adj blind*).mp. 27 assign*.mp. 28 allocat*.mp. 29 volunteer*.mp. 30 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 31 16 and 30
key: mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer, drug manufacturer
Appendix 5. Assessment of the Risk of Bias for Included studies
We assessed the risk of bias as follows:
(1) Method of randomisation
Methodological quality of randomisation was classified as follows:
Low risk of bias(any truly random process, e.g. random number table;computer random number generator),
High risk of bias (any non‐random process, e.g. odd or even date of birth;hospital or clinic record number) or,
Unclear risk of bias (no details provided).
(2) Allocation concealment
Low risk of bias e.g. telephone or central randomisation; consecutively numbered sealed opaque envelopes);
High risk of bias (open random allocation; unsealed or non‐opaque envelopes, alternation; date of birth);
Unclear risk of bias.
(3) Blinding
In studies of communication skills training, both the participants and the providers of the training would be aware of study arm allocation, therefore it was not possible to assess 'performance bias'. However, the outcome assessment could be blinded, therefore we assessed blinding of outcome assessment (Protection against 'detection bias') as:
low, high or unclear risk of bias.
(4) Incomplete outcome data
We described for each included study, and for each outcome or class of outcomes, the completeness of data including attrition and exclusions from the analysis. We stated whether attrition and exclusions were reported and the numbers included in the analysis at each stage (compared with the total randomised participants), reasons for attrition or exclusion where reported, and whether missing data were balanced across groups or were related to outcomes.
We assessed methods as:
low risk of bias (e.g. less than 20% missing outcome data; missing outcome data balanced across groups);
high risk of bias (e.g. numbers or reasons for missing data imbalanced across groups; ‘as treated’ analysis done with substantial departure of intervention received from that assigned at randomisation);
unclear risk of bias.
5) Selective reporting
We described for each included study how we investigated the possibility of selective outcome reporting bias and what we found. We assessed the methods as:
low risk of bias (where it was clear that all of the study’s pre‐specified outcomes and all expected outcomes of interest to the review had been reported);
high risk of bias (where not all the study’s pre‐specified outcomes were reported; one or more reported primary outcomes were not prespecified; outcomes of interest were reported incompletely and so could not be used; study failed to include results of a key outcome that would have been expected to have been reported);
unclear risk of bias.
(6) Other bias (checking for bias due to problems not covered by 1 to 5 above)
We described for each included study any important concerns we had about other possible sources of bias. We assessed whether each study was free of other problems that could put it at risk of bias, as follows:
low risk of other bias;
high risk of other bias;
unclear whether there is risk of other bias.
Appendix 6. Search results for the original review
For the original 2001 review, 48 studies identified by the search were classified as follows:
Included (2)
Excluded (46)
The included studies were Fallowfield 2002 and Razavi 1993.
The 46 excluded studies that had warranted further consideration were excluded for methodological reasons. Most (27) were excluded as they measured changes in attitudes and/or knowledge, rather than skills (Anderson 1982; Baile 1997; Baile 1999; Berman 1983; Bird 1993; Cantwell 1997; Cowan 1997; Craytor 1978; Delvaux 1997; Dixon 2001; Durgahee 1997; Fallowfield 1998; Fallowfield 2001; Ferrell 1998a; Girgis 1997; Gordon 1995; Hainsworth 1996 ; Hall 1999 ; Hallenbeck 1999; Hulsman 1997; Linder 1999; Lloyd‐Williams 1996; Parle 1997; Razavi 1991; Smith 1991; Von Gunten 1998; Wong 2001). Many of these studies would also have been excluded for not having a separate control group. A further 14 studies were excluded as they had no separate control group, although they were longitudinal (Booth 1996; Charlton 1993; Faulkner 1984; Faulkner 1992; Glimelius 1995; Heaven 1996; Heaven 1996b; Maguire 1996a; Maguire 1996b; Matrone 1990; Razavi 2000; Rutter 1996; Wilkinson 1998; Wilkinson 1999). Five were excluded due to the subjective nature of their evaluation of communication skills (largely based on perceived improvement by the participant) (Andrew 1998; de Rond 2000; Ferrell 1998b; La Monica 1987; Shorr 2000) Only one of this latter group included a separate control group of non‐trained staff (de Rond 2000).
In November 2003, three further studies were added to the review; one was included (Razavi 2002) and the remaining two were excluded (Finset 2003; Libert 2003). Therefore, in total, three studies were included and 48 were excluded.
Data and analyses
Comparison 1.
CST vs no CST: HCP communication skills
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Used open questions | 5 | 679 | Std. Mean Difference (IV, Random, 95% CI) | 0.28 [0.02, 0.54] |
| 1.1 Simulated patients | 5 | 422 | Std. Mean Difference (IV, Random, 95% CI) | 0.38 [‐0.01, 0.76] |
| 1.2 Real patients | 3 | 257 | Std. Mean Difference (IV, Random, 95% CI) | 0.09 [‐0.15, 0.34] |
| 2 Clarified and/or summarised | 3 | 422 | Std. Mean Difference (IV, Random, 95% CI) | 0.09 [‐0.30, 0.49] |
| 2.1 Simulated patients | 3 | 253 | Std. Mean Difference (IV, Random, 95% CI) | 0.32 [‐0.18, 0.81] |
| 2.2 Real patients | 2 | 169 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.20 [‐0.50, 0.11] |
| 3 Elicited concerns | 2 | 191 | Std. Mean Difference (IV, Random, 95% CI) | 0.31 [‐0.10, 0.72] |
| 3.1 Simulated patients | 2 | 133 | Std. Mean Difference (IV, Random, 95% CI) | 0.27 [‐0.42, 0.95] |
| 3.2 Real patients | 1 | 58 | Std. Mean Difference (IV, Random, 95% CI) | 0.40 [‐0.12, 0.93] |
| 4 Showed empathy | 6 | 727 | Std. Mean Difference (IV, Random, 95% CI) | 0.21 [0.07, 0.36] |
| 4.1 Simulated patients | 5 | 422 | Std. Mean Difference (IV, Random, 95% CI) | 0.26 [0.07, 0.45] |
| 4.2 Real patients | 4 | 305 | Std. Mean Difference (IV, Random, 95% CI) | 0.15 [‐0.07, 0.38] |
| 5 Gave appropriate information | 2 | 342 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.09 [‐0.31, 0.12] |
| 5.1 Simulated patients | 2 | 173 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.16 [‐0.46, 0.14] |
| 5.2 Real patients | 2 | 169 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.02 [‐0.32, 0.28] |
| 6 Gave facts only | 5 | 663 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.24 [‐0.53, 0.05] |
| 6.1 Simulated patients | 5 | 406 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.42 [‐0.77, ‐0.06] |
| 6.2 Real patients | 3 | 257 | Std. Mean Difference (IV, Random, 95% CI) | 0.05 [‐0.19, 0.30] |
| 7 Negotiation | 3 | 386 | Std. Mean Difference (IV, Random, 95% CI) | 0.16 [‐0.08, 0.41] |
| 7.1 Simulated patients | 3 | 240 | Std. Mean Difference (IV, Random, 95% CI) | 0.13 [‐0.12, 0.39] |
| 7.2 Real patients | 2 | 146 | Std. Mean Difference (IV, Random, 95% CI) | 0.23 [‐0.45, 0.92] |
Analysis 1.2.
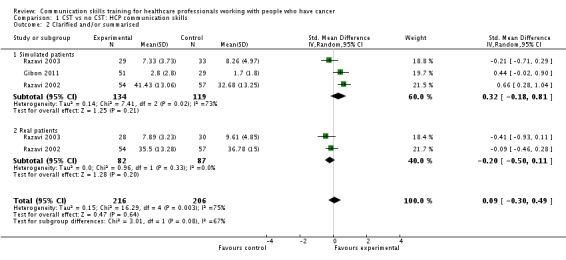
Comparison 1 CST vs no CST: HCP communication skills, Outcome 2 Clarified and/or summarised.
Analysis 1.3.
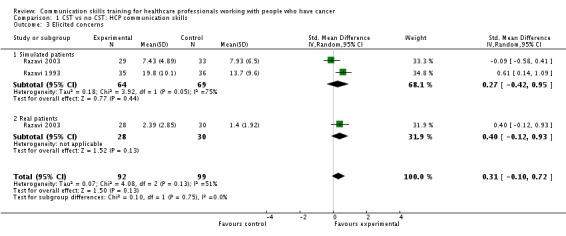
Comparison 1 CST vs no CST: HCP communication skills, Outcome 3 Elicited concerns.
Analysis 1.7.
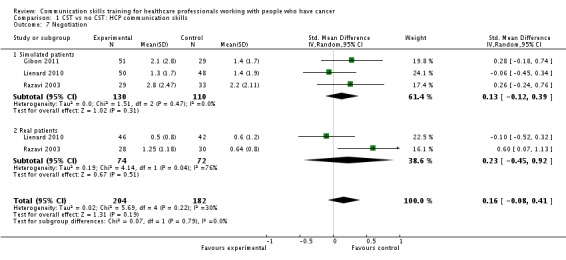
Comparison 1 CST vs no CST: HCP communication skills, Outcome 7 Negotiation.
Comparison 2.
CST vs no CST: HCP communication skills: doctors only
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Used open questions | 2 | 306 | Std. Mean Difference (IV, Random, 95% CI) | 0.27 [0.05, 0.50] |
| 1.1 Simulated patients | 2 | 160 | Std. Mean Difference (IV, Random, 95% CI) | 0.34 [0.03, 0.66] |
| 1.2 Real patients | 2 | 146 | Std. Mean Difference (IV, Random, 95% CI) | 0.20 [‐0.13, 0.52] |
| 2 Clarified and/or summarised | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2.1 Simulated patients | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 Real patients | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 Elicited concerns | 1 | 120 | Std. Mean Difference (IV, Random, 95% CI) | 0.15 [‐0.33, 0.63] |
| 3.1 Simulated patients | 1 | 62 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.09 [‐0.58, 0.41] |
| 3.2 Real patients | 1 | 58 | Std. Mean Difference (IV, Random, 95% CI) | 0.40 [‐0.12, 0.93] |
| 4 Showed empathy | 3 | 354 | Std. Mean Difference (IV, Random, 95% CI) | 0.22 [0.01, 0.43] |
| 4.1 Simulated patients | 2 | 160 | Std. Mean Difference (IV, Random, 95% CI) | 0.27 [‐0.05, 0.60] |
| 4.2 Real patients | 3 | 194 | Std. Mean Difference (IV, Random, 95% CI) | 0.18 [‐0.12, 0.49] |
| 5 Gave appropriate information | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 5.1 Simulated patients | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.2 Real patients | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 Gave facts only | 2 | 306 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.19 [‐0.74, 0.37] |
| 6.1 Simulated patients | 2 | 160 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.50 [‐1.36, 0.35] |
| 6.2 Real patients | 2 | 146 | Std. Mean Difference (IV, Random, 95% CI) | 0.16 [‐0.17, 0.49] |
Analysis 2.2.
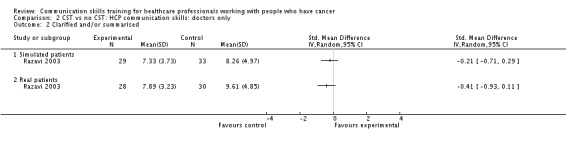
Comparison 2 CST vs no CST: HCP communication skills: doctors only, Outcome 2 Clarified and/or summarised.
Analysis 2.3.
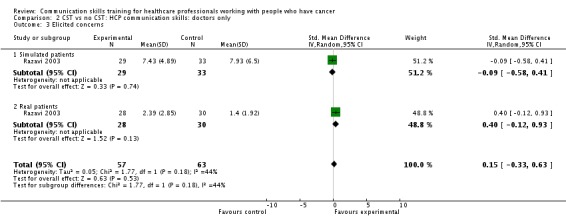
Comparison 2 CST vs no CST: HCP communication skills: doctors only, Outcome 3 Elicited concerns.
Analysis 2.5.
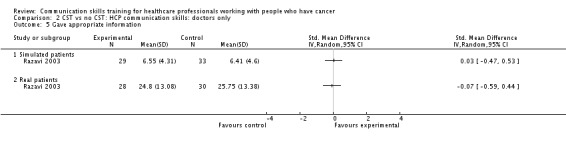
Comparison 2 CST vs no CST: HCP communication skills: doctors only, Outcome 5 Gave appropriate information.
Analysis 2.6.
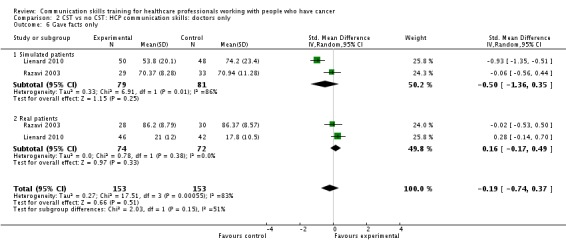
Comparison 2 CST vs no CST: HCP communication skills: doctors only, Outcome 6 Gave facts only.
Comparison 3.
CST vs no CST: HCP communication skills: nurses only
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Used open questions | 2 | 293 | Std. Mean Difference (IV, Random, 95% CI) | 0.41 [‐0.23, 1.06] |
| 1.1 Simulated patients | 2 | 182 | Std. Mean Difference (IV, Random, 95% CI) | 0.65 [‐0.07, 1.37] |
| 1.2 Real patients | 1 | 111 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.04 [‐0.42, 0.33] |
| 2 Clarified and/or summarised | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2.1 Simulated patients | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 Real patients | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 Elicited concerns | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 3.1 Simulated patients | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 Showed empathy | 2 | 293 | Std. Mean Difference (IV, Random, 95% CI) | 0.19 [‐0.04, 0.42] |
| 4.1 Simulated patients | 2 | 182 | Std. Mean Difference (IV, Random, 95% CI) | 0.23 [‐0.06, 0.53] |
| 4.2 Real patients | 1 | 111 | Std. Mean Difference (IV, Random, 95% CI) | 0.11 [‐0.27, 0.48] |
| 5 Gave appropriate information | 2 | 342 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.09 [‐0.31, 0.12] |
| 5.1 Simulated patients | 2 | 173 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.16 [‐0.46, 0.14] |
| 5.2 Real patients | 2 | 169 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.02 [‐0.32, 0.28] |
| 6 Gave facts only | 2 | 293 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.24 [‐0.65, 0.17] |
| 6.1 Simulated patients | 2 | 182 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.31 [‐0.98, 0.37] |
| 6.2 Real patients | 1 | 111 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.09 [‐0.47, 0.28] |
Analysis 3.2.
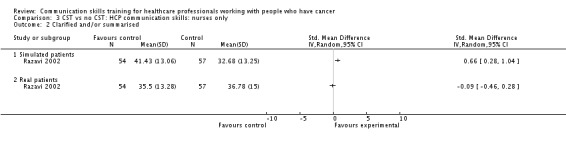
Comparison 3 CST vs no CST: HCP communication skills: nurses only, Outcome 2 Clarified and/or summarised.
Analysis 3.3.
Comparison 3 CST vs no CST: HCP communication skills: nurses only, Outcome 3 Elicited concerns.
Comparison 4.
CST vs no CST: subgrouped by HCP type
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Used open questions | 4 | 599 | Std. Mean Difference (IV, Random, 95% CI) | 0.34 [0.07, 0.61] |
| 1.1 Doctors | 2 | 306 | Std. Mean Difference (IV, Random, 95% CI) | 0.27 [0.05, 0.50] |
| 1.2 Nurses | 2 | 293 | Std. Mean Difference (IV, Random, 95% CI) | 0.41 [‐0.23, 1.06] |
| 2 Clarified and/or summarised | 2 | 342 | Std. Mean Difference (IV, Random, 95% CI) | 0.01 [‐0.47, 0.48] |
| 2.1 Doctors | 1 | 120 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.30 [‐0.66, 0.06] |
| 2.2 Nurses | 1 | 222 | Std. Mean Difference (IV, Random, 95% CI) | 0.28 [‐0.45, 1.02] |
| 3 Elicited concerns | 2 | 191 | Std. Mean Difference (IV, Random, 95% CI) | 0.31 [‐0.10, 0.72] |
| 3.1 Doctors | 1 | 120 | Std. Mean Difference (IV, Random, 95% CI) | 0.15 [‐0.33, 0.63] |
| 3.2 Nurses | 1 | 71 | Std. Mean Difference (IV, Random, 95% CI) | 0.61 [0.14, 1.09] |
| 4 Showed empathy | 5 | 647 | Std. Mean Difference (IV, Random, 95% CI) | 0.21 [0.05, 0.36] |
| 4.1 Doctors | 3 | 354 | Std. Mean Difference (IV, Random, 95% CI) | 0.22 [0.01, 0.43] |
| 4.2 Nurses | 2 | 293 | Std. Mean Difference (IV, Random, 95% CI) | 0.19 [‐0.04, 0.42] |
| 5 Gave appropriate information | 2 | 342 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.09 [‐0.31, 0.12] |
| 5.1 Doctors | 1 | 120 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.02 [‐0.38, 0.34] |
| 5.2 Nurses | 1 | 222 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.13 [‐0.40, 0.14] |
| 6 Gave facts only | 4 | 599 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.21 [‐0.54, 0.12] |
| 6.1 Doctors | 2 | 306 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.19 [‐0.74, 0.37] |
| 6.2 Nurses | 2 | 293 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.24 [‐0.65, 0.17] |
Comparison 5.
CST vs no CST: Other HCP outcomes
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Emotional exhaustion: Maslach Burnout Inventory: | 2 | 106 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.25 [‐0.67, 0.18] |
| 2 Personal accomplishment: Maslach Burnout Inventory | 2 | 91 | Std. Mean Difference (IV, Random, 95% CI) | 0.26 [‐0.24, 0.76] |
Comparison 6.
CST vs no CST: Patient outcomes
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Patient psychiatric morbidity (GHQ 12) | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2 Patient anxiety: Spielberger's State Trait Anxiety Inventory | 2 | 169 | Std. Mean Difference (IV, Random, 95% CI) | 0.40 [0.07, 0.72] |
| 3 Patient perception of HCPs communication skills | 2 | 170 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.14 [‐0.44, 0.16] |
| 4 Patient satisfaction with communication | 2 | 429 | Std. Mean Difference (IV, Random, 95% CI) | 0.20 [‐0.23, 0.63] |
Comparison 7.
Follow‐up CST vs no follow‐up CST: HCP communication skills
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Used open questions | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 1.1 Simulated patients | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 Real patients | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 Clarified and/or summarised | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 2.1 Simulated patients | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 Real patients | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 Elicited concerns | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 3.1 Simulated patients | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 Real patients | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 Showed empathy | 2 | 168 | Std. Mean Difference (IV, Random, 95% CI) | 0.23 [‐0.07, 0.54] |
| 4.1 Simulated patients | 1 | 62 | Std. Mean Difference (IV, Random, 95% CI) | 0.07 [‐0.43, 0.57] |
| 4.2 Real patients | 2 | 106 | Std. Mean Difference (IV, Random, 95% CI) | 0.33 [‐0.06, 0.72] |
| 5 Gave appropriate information | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 5.1 Simulated patients | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.2 Real patients | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 Gave facts only | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 6.1 Simulated patients | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.2 Real patients | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7 Negotiation | 1 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 7.1 Simulated patients | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.2 Real patients | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] |
What's new
Last assessed as up‐to‐date: 19 February 2013.
| Date | Event | Description |
|---|---|---|
| 21 September 2016 | Amended | Contact details updated. |
History
Protocol first published: Issue 3, 2002 Review first published: Issue 2, 2003
| Date | Event | Description |
|---|---|---|
| 1 April 2015 | Amended | Contact details updated. |
| 11 February 2015 | Amended | Contact details updated. |
| 27 March 2014 | Amended | Contact details updated. |
| 19 February 2013 | New search has been performed | Review updated to include 15 RCTs. |
| 18 February 2013 | New citation required but conclusions have not changed | We found more evidence to show that CSTs may be helpful in improving some HCP outcomes. |
| 6 August 2012 | New search has been performed | Out of 119 potentially eligible records identified by the updated searches, we included 12 additional studies (Butow 2008, Gibon 2011, Goelz 2009, Heaven 2006, Kruijver 2001, Razavi 2002, Razavi 2003, Stewart 2007, Lienard 2010, Tulsky 2011, Wilkinson 2008; Fujimori 2011) (33 records) and we identified six records relating to the three previously included studies. Therefore, from the updated search, we included 39 new records relating to 15 studies. We excluded 80 newly identified records (70 studies). |
| 24 February 2012 | New search has been performed | Search updated producing 358 records. |
| 9 September 2011 | New search has been performed | Search updated producing 411 records including 37 duplicates. Three potentially eligible studies identified . |
| 21 January 2011 | New search has been performed | Search updated producing 2,508 records including 43 du plicates .T hirty potentially eligible s tudies/reports identified. |
| 6 May 2008 | Amended | Converted to new review format. |
| 7 December 2003 | New citation required and conclusions have changed | Substantive amendment |
Differences between protocol and review
The original review was a narrative review that included three studies (Fallowfield 2002; Razavi 1993; Razavi 2002). Whereas the protocol and original review included pre‐test/post‐test study designs in the Types of studies for consideration, for the updated review we included only RCTs.
For the protocol and original 2002 review, we defined Types of outcome measures as follows: 'Outcomes were changes in behaviour or skills measured using objective and validated scales.' For the update, we attempted to specify Types of outcome measures more clearly, in accordance with the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Butow 2008
| Methods | RCT. | |
| Participants | 30 medical and radiation oncologists from 6 Australian teaching hospitals: Age = 36.5 to 51 years; years of experience = 7.5 to 24.3 years. 343 cancer patients (60% women) answered questionnaires post‐consultation. |
|
| Interventions | 1.5 day work‐shop with 3 to 6 participants, followed by four 1.5 hour video conferences incorporating role‐play of doctor‐generated scenarios. Work shop included DVD modelling ideal behaviour; role‐play and feedback with an SP using standardised cases and from own experience, booklet summarising evidence, video of own role‐play. Emphasis on how to establish a collaborative framework, and how to respond to anxiety, depression, distress and anger. | |
| Outcomes | HCP (oncologist) outcomes on video of SP interview at baseline, immediately post‐intervention and 6 months post‐intervention (or equivalent timings for control group).
HCP (oncologist) Burnout' measured using MBI* Patient outcomes:
|
|
| Notes | There was a trend for training to be successful in increasing some HCP communication skills, however, no changes were statistically significant. Anxiety was reduced in patients interviewed by oncologists from the intervention group one week later (P = 0.021) No other statistically significant differences were found in patient outcomes. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomised at individual level using random number tables and Excel software. |
| Allocation concealment (selection bias) | Low risk | Allocated centrally by research team. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not described. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No description of total number of HCP measured post‐intervention. Low attrition in HCP and patient questionnaires. |
| Selective reporting (reporting bias) | Low risk | All prespecified outcomes reported. |
| Other bias | Low risk | Baseline characteristics of the two groups were similar. |
Fallowfield 2002
| Methods | RCT. Written feedback followed by course, or course alone, or written feedback alone, or control. |
|
| Participants | 160 medical, surgical and radiation oncologists from 34 cancer centres in the UK; 69% men. 640 cancer patients (60% women) participated in the videotaped consultations (2 video‐tapes per oncologist at baseline and 3 months post‐intervention). 2331 cancer patients answered questionnaires. |
|
| Interventions | Cancer Research UK Communication Skills Program. Intensive 3‐day residential course and/or feedback pack. | |
| Outcomes | HCP (oncologist) outcomes on video of RP interviews at baseline, and 3 months post‐intervention (or equivalent timings for control group).:
Patient outcomes:
|
|
| Notes | CST group had a statistically significant improvement in oncologists' attitudes to psychosocial issues (P = 0.002) and a non‐significant positive effect on patient satisfaction. Follow‐up for 12 months revealed no demonstrable attrition in most of the skills improvement, some new skills, but a decline in expressions of empathy. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not fully described. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Video raters blinded as far as possible for time‐point of assessment and group. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Low risk on HCP behaviour outcomes; 21% attrition for patient outcomes; only intervention group followed up at 12 months. |
| Selective reporting (reporting bias) | Low risk | All prespecified outcomes were described. |
| Other bias | Low risk | Baseline characteristics of two groups were similar. |
Fujimori 2011
| Methods | RCT conducted in Japan. | |
| Participants | 30 oncologists | |
| Interventions | A 2‐day CST workshop (intervention) or 'no CST' (control). | |
| Outcomes | HCP outcomes:
Patient outcomes:
Assessed at baseline, post‐CST or one‐week later. |
|
| Notes | Only the abstract, which contained no data, was available at the time of publication. The abstract reports that skills relating to emotional support and information‐giving were higher in the intervention compared with the control group, patient distress scores were lower, and patient satisfaction scores were similar at the follow‐up assessment. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | 'Randomly assigned'. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not described. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not described. |
| Selective reporting (reporting bias) | Unclear risk | Only a conference abstract available. No data reported. |
| Other bias | Unclear risk | Attempts to contact the authors for data were unsuccessful. |
Gibon 2011
| Methods | RCT. | |
| Participants | 80 participants of 4 radiotherapy teams comprising secretaries (16%), physicists (7.5%), nurses (49%), doctors (27.5 %). | |
| Interventions | 38 hours of CST; not described in detail. | |
| Outcomes | HCP communication skills rated using the scale LaComm* on audio of simulated breast cancer patient (SP) interview at baseline and post‐intervention (or equivalent timings for control group). | |
| Notes | For some communication skill outcomes, course attendees (intervention group) had significantly more appropriate behaviours/skills than those who had not attended; these included a team orientated focus (P = 0.023), empathy (P = 0.037) and emotional words (P = 0.030). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not described. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 83% follow‐up. |
| Selective reporting (reporting bias) | Unclear risk | No details of data extracted using LaComm*. |
| Other bias | High risk | Some differences in baseline characteristics of two groups including work experience in oncology, full‐time occupation, and % of non‐professionals. |
Goelz 2009
| Methods | RCT conducted from June 2007 ‐ Feb 2009. | |
| Participants | 41 doctors (39 from Department of Haematology/Oncology, one from Gynaecology, one from Surgery). | |
| Interventions | CST in the form of COM‐ON‐p(COMmunication challenges in ONcology related to the transition to palliative care training program), including a one hour pre‐assessment with SPs, an 11‐hour training course (main focus practice with SPs using cases of participants) plus a half‐hour individual coaching session two weeks later. The courses were run in groups of 8/9 participants by two experienced facilitators. | |
| Outcomes | HCP (Doctors') communication skills in video‐recorded SP consultations pre‐intervention and five weeks post‐intervention using COM‐ON‐checklist included:
|
|
| Notes | The average overall estimate of effect favoured the intervention group (P=0.0007). There was a statistically significant difference between intervention and control group in all sections in favour of the intervention group including: specific palliative communication skills (P<0.0026); general communication skills (P<0.0078); and involvement of significant others (P<0.0.0051). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation to two groups in blocks of 8 by an 'external statistician'. |
| Allocation concealment (selection bias) | Unclear risk | Allocation by fax. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessors blinded to group allocation. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 100% follow‐up. |
| Selective reporting (reporting bias) | Low risk | All pre‐specified outcomes reported. |
| Other bias | High risk | Doctors in the intervention group had significantly more professional (P = 0.02) experience compared with those in the control group. |
Heaven 2006
| Methods | RCT. | |
| Participants | 61 UK nurses all of who received basic 3‐day CST training prior to randomisation: 68% working in palliative care; mean age 42 years; all but one female; 41% worked in community only, 21% hospital only, 38% hospital and community 366 RP encounters (75% women, mean age 61years) |
|
| Interventions | Four 3‐hour supervision sessions plus feedback on video of interview with RPs. Both intervention and control groups had basic training prior to baseline. |
|
| Outcomes | HCP (nurses') communication skills assessed in audio‐recording of 3‐RP interviews at 1 and 3 months post‐intervention, rated using MIARS:
|
|
| Notes | Some communication behaviours were enhanced in the intervention group after supervision, including psychological exploration (P = 0.039). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Data collectors and judges were blinded to time and group. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 84% follow‐up at 3 months. |
| Selective reporting (reporting bias) | Low risk | All pre‐specified outcomes were reported. |
| Other bias | Low risk | Baseline characteristics of two groups were similar except the control group had more communication skills training (P = 0.037). |
Kruijver 2001
| Methods | RCT. | |
| Participants | 53 nurses from 11 wards in 3 Dutch hospitals: mean age was 32 years, 83% women; mean of 5 years' experience in oncology. 265 recently diagnosed cancer patients admitted for treatment. 106 patient encounters (55% women, mean age 55 years). |
|
| Interventions | Six 3‐hour sessions with 10‐15 participants run by two trainers with experience in clinical patient care. CST included theory, demonstration of skills, and feedback on role‐playing. | |
| Outcomes | HCP (nurses') communication skills assessed on video recordings of SP interviews (one month post‐intervention) and 5 RP admission interviews between 1‐7 months post‐intervention using RIAS*:
Nurses' 'burnout' was measured using MBI. Patients outcomes:
|
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | 53 participants " randomised at ward level". |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Independent rater but blinded status not described. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 83% to 86% follow‐up. |
| Selective reporting (reporting bias) | Low risk | All pre‐specified outcomes were reported. |
| Other bias | Low risk | Baseline characteristics of two groups were similar. |
Lienard 2010
| Methods | RCT. | |
| Participants | 113 Belgian residents who had been, or were, working with cancer patients. 759 hospitalised patients answered questionnaires. 88 patient encounters analysed (56% women;.mean age 55 years). |
|
| Interventions | 40‐hour training programme (17 hours on two‐person interview skills, 10 hours on three‐person interviews, 10 hours on stress management, 3 hours on integration of skills) bimonthly over an 8‐month period. Small groups (maximum 7 participants). Comprised a one‐hour theoretical session, role‐plays of pre‐defined cases, and cases from participants with immediate feedback. | |
| Outcomes | HCP (residents) communication skills were analysed in audiotapes of 1 SP encounter and 1 RP interview during a clinical round pre‐ and post‐intervention or at 8 months (control group) using LaComm*:
Also time spent on the 3 phases of breaking bad news and precision of the delivery of diagnosis. Residents' burnout was measured pre‐ and post‐intervention using MBI. Residents' physiological arousal was measured during the SP interviews. Patient outcomes:
|
|
| Notes | Statistically significant improvement was found in 2 of 12 items of HCP skills with RPs. No effect on empathy or supportive skills in RPs. Significant increase in open questions, empathy, and concise precise diagnoses in SPs, but significant decrease in other information with SP. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Assessor blinded to time assessment and group allocation |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Trained residents took part in an average of 25 hours (62%) of a training program (range 8‐40 hours). 77% follow‐up in RPs; 86% follow‐up in SPs. |
| Selective reporting (reporting bias) | Unclear risk | Subgroup analysis of % training attendance. |
| Other bias | High risk | Selection of interview for HCP communication analysis unclear. Number of patients with cancer : < 40% of patient interviews analysed and numbers are unclear in 'patient satisfaction' outcome. |
Razavi 1993
| Methods | RCT. | |
| Participants | 72 oncology nurses from 4 hospitals in France and Belgium participated. | |
| Interventions | 24‐hour training program taught in 8 weekly, 3‐hour sessions. | |
| Outcomes | HCP (nurses') communication skills in first 5 minutes of video‐taped SP interviews, pre‐ and 2 months post‐training, rated using CRCWEM* (Cancer Research Campaign Workshop Evaluation Manual);
Nurses' attitudes (SDAQ*), occupational stress (NSS*) and self‐perception. |
|
| Notes | Trained group were assessed as 'more in control of the interview' than the untrained group during the follow‐up interview (P = 0.02). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Twelve participants per institution were "randomly assigned" to two groups. |
| Allocation concealment (selection bias) | Low risk | Allocation by sealed envelopes. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Video raters blinded for group; questionnaire assessors not blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Low attrition rates: one drop out, three incomplete data sets out of 72 participants. |
| Selective reporting (reporting bias) | Low risk | All pre‐specified outcomes were reported. |
| Other bias | Low risk | Baseline characteristics of two groups were similar. |
Razavi 2002
| Methods | RCT. | |
| Participants | 115 oncology nurses from 33 hospitals in Belgium. 114 cancer patients during first week of hospitalisation. |
|
| Interventions | 105‐hour communications skills workshop with 10 participants, run by psychologist, taught over 3 months for one week per month. | |
| Outcomes | HCP (nurses') communication skills in video‐taped SP interviews and audio‐taped RP interviews pre‐ and post‐intervention (or equivalent timings for control group), and three months later rated using CRCWEM* (Cancer Research Campaign Workshop Evaluation Manual), plus dictionaries (HPSD* and MRID*) and LACOMM*
Nurses' Stress (NSS*) and Attitudes (SDAQ*). Patient outcomes:
|
|
| Notes | Patients interviewed by trained nurses also used more emotional words associated with 'distress' than did those seen by untrained nurses (P = 0.005). There was a positive training effect on patient satisfaction (P < 0.01). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Randomisation was performed every time there were 20 nurses enrolled. |
| Allocation concealment (selection bias) | High risk | Randomisation was performed every time there were 20 nurses enrolled. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Raters blinded by time and group. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 86% follow‐up for HCP behavioural outcome. |
| Selective reporting (reporting bias) | Low risk | All pre‐specified outcomes were reported. |
| Other bias | Low risk | Baseline characteristics were similar in both groups. |
Razavi 2003
| Methods | RCT of follow‐up consolidation sessions after both groups had basic training. | |
| Participants | 63 physicians (62% oncologists) from Belgium hospitals, age 43+/‐7, 55% men, with average 14 years of experience in oncology and 43% no prior CST. All had participated in a 19‐hour CST workshop (consisting of two, 8‐hour/day sessions and one, 3‐hour evening session). 59 cancer patients, undergoing a 'breaking news' interview (67% women mean age 58 years). 53 cancer patients (65% women mean age 60 years) in encounters with relatives (48% women mean age 57 years). |
|
| Interventions | Six, 3‐hour per evening, bimonthly, consolidation sessions over three months. | |
| Outcomes | HCP (doctors) outcomes:
Patient outcomes:
Significant other outcomes:
|
|
| Notes | There was no effect of consolidation workshops on doctors' ability to detect patient distress. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | 72 participants "randomly assigned". |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Raters blinded for time (pre/post) and group. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 81% follow‐up for SP and RP; and 77% follow‐up for RP interview with significant other. |
| Selective reporting (reporting bias) | Low risk | All pre‐specified outcomes were reported. |
| Other bias | Low risk | Baseline characteristics of the two HCP groups were similar. Baseline scores of patient anxiety were markedly higher in patients seen by the control group. |
Stewart 2007
| Methods | RCT. | |
| Participants | 51 doctors (18 oncologists, 17 family doctors and 16 surgeons) from 3 towns in Canada. 102 cancer patients who attended outpatient clinics of oncologists and surgeons. |
|
| Interventions | 6‐hour intensive CST course including literature, physicians and patients perspectives, video modelling poor and better behaviour, role‐play, video and feedback with SP using standardized cases. Emphasis on exploring patients perspectives. Control group received the standard 2hr small group discussion triggered by video of interview between physician and breast cancer standardised patient. |
|
| Outcomes | HCP (doctors) communication skills in video‐taped SP interviews at baseline and after intervention. Rated using PCCM*:
Patient outcomes (measured only for surgeons and oncologists in both groups):
|
|
| Notes | Training had a positive impact on patients' satisfaction (P = 0.03) and "feeling better" (P = 0.02). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random number table. |
| Allocation concealment (selection bias) | Low risk | Randomized done by project co‐ordinator. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Raters and patients were blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 100% for HCP behaviour outcome; 44.3% patient response rate to patient questionnaire. |
| Selective reporting (reporting bias) | Low risk | Subgroup analysis (family physicians) on selected outcomes. |
| Other bias | Low risk | |
Tulsky 2011
| Methods | Single‐blind RCT. Stratified by site, gender and oncologist speciality. | |
| Participants | 48 oncologists (medical, gynaecological and radiation), all of whom received a one hour lecture on communication skills. 264 patients with advanced cancer (65% women mean age 60 years). |
|
| Interventions | Computerised intervention (interactive CD‐ROM) organised in five 15‐minute modules and included principles of effective communication, recognising and responding to empathic opportunities, conveying prognosis and answering difficult questions. Included tailored feedback from oncologists' own recorded conversations. | |
| Outcomes | HCP (oncologists) outcomes:
Patient outcomes (measured one week after the encounter by telephone survey):
|
|
| Notes | CST aimed to influence a limited number of skills. Median time of training program = 64 minutes (58‐99). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Balanced randomisation in a 1:1 ratio by site, sex and speciality. Statistician performed minimisation method of randomisation to ensure balanced groups. |
| Allocation concealment (selection bias) | Low risk | Statistician revealed the randomisation results only to project co‐ordinator and principal investigators. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Single‐blind. Patients were blinded to their oncologists' group allocation, as were the two audio‐coders. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 21/24 used CD‐ROM in intervention, but all included in evaluation. 4/264 encounters could not be assessed due to technical problems. Overall missing data < 20%. |
| Selective reporting (reporting bias) | Low risk | All pre‐specified outcomes were reported. |
| Other bias | Low risk | Baseline characteristics comparable except for fewer Caucasian doctors in the intervention group (76% vs 92%). Unclear if scales/questionnaires used were validated. |
van Weert 2011
| Methods | RCT conducted in inpatients. | |
| Participants | 48 hospital nurses providing patient education about chemotherapy; 210 older cancer patients receiving chemotherapy (35% women, mean age 72 years) |
|
| Interventions | Individualised web‐based video feedback; a 1‐day CST conducted in groups of 6‐11 nurses focusing on patient education about chemotherapy; observation and feedback of colleagues interviews; and a half‐day follow‐up session and booklet. | |
| Outcomes | HCP (nurses) outcomes:
Patient outcomes:
|
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Independent observers of videos were blinded to group. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No description of the number of nurses who participated in the videos analysed post‐treatment. |
| Selective reporting (reporting bias) | Low risk | All 7 dimensions of communication reported. |
| Other bias | Low risk | Baseline characteristics comparable. |
Wilkinson 2008
| Methods | Multi‐centre RCT. | |
| Participants | 160 nurses (94% women) from hospices (60%) and community (30%) in UK. 312 cancer patients (85% women, mean age 32 years) |
|
| Interventions | A 3‐day course for max. 12 participants run by 2 co‐facilitators. Course included literature, nurses perspectives, video‐modelling ideal behaviour, audio recording with RPs and role‐play with SPs using standardised and participant cases, both with feedback. Emphasis on exploring nurses individual difficulties. | |
| Outcomes | HCP (nurses) outcomes (coded from audio‐tapes of RP admittance interviews and 12 weeks' post‐intervention; rated using CSRS*):
Patient outcomes:
|
|
| Notes | Tendency to improve patient satisfaction and general health. No statistical difference in mean change of patients' anxiety. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation using computer‐generated numbers. |
| Allocation concealment (selection bias) | Low risk | Statistician performed randomisation before the study commenced and kept the results in sealed envelopes in the central research department. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Raters blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 90% follow‐up but missing data stated. |
| Selective reporting (reporting bias) | Low risk | All pre‐specified outcomes described. |
| Other bias | High risk | Higher professional grades in control group. |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Acher 2004 | Not an RCT, no objective behavioural outcome measurement. |
| Ades 2001 | Not an RCT. No CST. |
| Alexander 2006 | Not an RCT. Case‐control study of a course to improve residents' communication skills with patients at end of life. |
| Anderson 1982 | Not an RCT. No controls, post‐CST course measurement only. |
| Andrew 1998 | Not an RCT. Qualitative study of CST in palliative care. |
| Arranz 2005 | Not an RCT. Post‐intervention assessment counselling course for nurses. No objective measurements of skills. |
| Arrighi 2010 | Not an RCT. Exploratory study conducted in patients not HCPs. |
| Back 2005 | Not an RCT. Questionaire survey of bereaved relatives. |
| Back 2007 | Not an RCT. Pre‐post cohort study of a 4‐day residential workshop in oncology fellows with objective measurements of HCP behaviour. |
| Baile 1997 | Not an RCT. Pre‐post cohort study of a 3‐day CST. Only subjective measurement of behavioural change reported. |
| Baile 1999 | Not an RCT. Pre‐post cohort study of a 2.5‐day CST. Only subjective measurement of behavioural change reported. |
| Berman 1983 | Not an RCT. Post‐study subjective measurement of behavioural change of an annual seminar for interns on caring for dying patients. |
| Bernard 2010 | Not an RCT. Case‐control study of a course for medical oncologists and nurses with pre‐post measurements of HCP skills and defence mechanisms. |
| Bird 1993 | Not an RCT. Post‐study subjective measurement of behavioural change of 2.5‐day residential workshop. |
| Booth 1996 | Not a RCT. Pre‐post cohort study of a 6‐session CST course for hospice nurses measuring HCP skills in audio‐taped interviews. |
| Brown 1999 | An RCT of CST in ambulatory care, not in cancer care. No objective measure of HCP skills. |
| Brown 2007 | Not an RCT. A course of communication skills training for oncologists involved in conducting clinical trials in oncology. Training was aimed at improving patient understanding and acceptance of clinical trials. |
| Brown 2011 | Not an RCT. Study of oncologists communication during interviews when recruiting patients for Phase 1 trials. |
| Brown 2012 | HCP communication skills were not assessed. |
| Burgess 2008 | Not an RCT. |
| Bylund 2010 | Not an RCT. Pre‐post study of CST course for oncologists. |
| Bylund 2011a | Not an RCT.Description of implementation of CST curriculum and impressions of participants. |
| Bylund 2011b | Not an RCT. Before‐after assessment of a non‐controlled study of CST for patients. |
| Cantwell 1997 | A qualitative study of junior doctors opinion of undergraduate communication skills in relation to patients with cancer. |
| Caps 2010 | Not an RCT. |
| Chandawarkar 2011 | Not an RCT. Pre‐post assessment using simulated patients of CST for surgical residents. |
| Charlton 1993 | Not an RCT. |
| Clark 2009 | An RCT of patients with cancer receiving patient‐centred care or usual care. |
| Claxton 2011 | An RCT of email education for residents about palliative care. Not specifically communication skills. No objective measurement of skills reported. |
| Connolly 2010 | Not an RCT. Post course measurement of "Sage and Thyme" communication course. No objective measurement of skills reported. |
| Cort 2009 | RCT studying the effect of a course on cognitive behaviour therapy. No objective measurement of behavioural change reported. |
| Cowan 1997 | Not an RCT. Measured changes in attitudes/knowledge, not behaviour. No separate control group. |
| Craytor 1978 | Not an RCT. Measured changes in attitudes/knowledge, not behaviour. No separate control group. |
| Crit 2006 | Not an RCT. |
| de Bie 2011 | Not communication skills training. Trial involved training patients to reduce anxiety prior to colonoscopy. |
| de Rond 2000 | Quasi‐RCT on training nurses about pain management. Only subjective measurement of behavioural change. |
| Del 2009 | Not an RCT. Qualitative study of how experienced doctors give good and bad news. |
| Delvaux 1997 | Not an RCT. Psychological training programme. |
| Dixon 2001 | Not an RCT. Pre‐post study of 12 week distance education for nurses working in breast cancer care. Only subjective measurement of behavioural change reported. |
| Durgahee 1997 | Not an RCT. 5 years experience of reflection through story‐telling for students of palliative care. |
| Fallowfield 1998 | Not an RCT. Cohort of 178 senior oncologists who assisted 1.5 or 3 day CST. Only subjective measurement of behavioural change reported. |
| Fallowfield 2001 | Not an RCT. Cohort of 129 nurses. Only subjective measurement of behavioural change reported. |
| Faulkner 1984 | Not an RCT. Cohort of 8 nurses working in cancer who assisted CST. |
| Faulkner 1992 | Not an RCT. Evaluation of training programmes for communication skills in palliative care. |
| Favre 2007 | Not an RCT. Pre‐post defence mechanism assessment of CST for oncologists. |
| Ferrell 1998a | Not an RCT. Pre‐post assessment of HOPE course for HCP in palliative care. Only subjective measurement of behavioural change reported. |
| Ferrell 1998b | Not an RCT. Pre‐post assessment of HOPE course for HCP in palliative care. Only subjective measurement of behavioural change reported. |
| Fineberg 2005 | Not an RCT. Quasi experimental design with pre‐post assessment of a course on family communication in palliative care for interdisciplinary students. Only subjective measurement of behavioural change reported. |
| Finset 2003 | Not an RCT. Pre‐post assessment of CST for HCP. Only subjective measurement of behavioural change reported. |
| Fujimori 2003 | Not an RCT.Post course assessment of CST for oncologists. Only subjective measurement of behavioural change reported. |
| Fukui 2008 | RCT of CST for nurses in cancer care. No objective measurement of behavioural change reported. Patient outcomes were only measured in the intervention group, not in the control group. |
| Girgis 1997 | Not an RCT. Measured change in attitude/knowledge not skills, not behaviour. |
| Glimelius 1995 | Not an RCT. |
| Gordon 1995 | Not an RCT. Post course assessment of 2.5‐day or 5‐day course of CST. Only subjective measurement of behavioural change reported. |
| Gutheil 2005 | Not an RCT. Patients not HCPs trained in communication skills. |
| Hainsworth 1996 | RCT of a course for nurses on death education. Not specifically for nurses working in cancer care. Only subjective measurement of behavioural change reported. |
| Hall 1999 | Not an RCT. |
| Hallenbeck 1999 | Not an RCT. A questionnaire of interns before and after their rotation in palliative care. |
| Heaven 1996 | Not an RCT. A 10 week CST for hospice nurses with assessment of ability to elicit patient concerns. |
| Heaven 1996b | Not an RCT. A 10‐week CST for hospice nurses with assessment of abiltity to elicit patient concerns. |
| Hellbom 2001 | Not an RCT. Post course assessment of a 4‐session CST course. Only subjective measurement of behavioural change reported. |
| Hietanen 2007 | Not an RCT. Case control study of a course on communication skills training for physicians involved in conducting clinical trials in oncology. Training was aimed at improving patient understanding and acceptance of clinical trials. |
| Hoffman 2002 | Not an RCT. Description of CST course for oncology residents and their views about the course. |
| Hulsman 1997 | Not an RCT. Pre‐post assessment of a computer‐assisted CST for doctors in cancer care. Only subjective measurement of behavioural change reported. |
| Hulsman 2002 | Not an RCT. Pre‐post assessment of a computer assisted CST for doctors in cancer care using videotapes of real patient encounter. |
| Hundley 2008 | An RCT of a course of delivering bad news. Only subjective measurement of behavioural change reported. |
| Jefford 2011 | Not an RCT. Patients received care package. |
| Ke 2008 | An RCT of 50‐minute CST lecture for nurses. Only subjective measurement of behavioural change reported. |
| Kinnane 2011 | Not an RCT. Study conducted in volunteers not HCPs. |
| Kruse 2003 | Not an RCT. Pre‐post assessment of a comparison between 6‐hour and 24‐hour CST programs. |
| La Monica 1987 | Not an RCT. Study of 4‐week session on responding to empathy. |
| Ladouceur 2003 | Not an RCT. Post course assessment of course of breaking bad news. Only subjective measurement of behavioural change reported. |
| Larbig 2009 | Not an RCT. On‐line counselling for patients. |
| Lenzi 2011 | Not an RCT. Pre‐ and post‐assessment of a 3‐day CST workshop in a cohort of 57 Italian oncologists. Only subjective measurement of behavioural change reported. |
| Libert 2003 | Not an RCT. A cohort of physicians were assessed with regard to their communication skills. |
| Linder 1999 | Measured change in attitude/knowledge not skills, not behaviour. |
| Liu 2007 | Not an RCT. Quasi‐experimental study of CST in nurses. |
| Lloyd‐Williams 1996 | Not an RCT. Measured change in attitude/knowledge not skills, not behaviour. |
| Loiselle 2011 | Not an RCT. |
| Macauley 2011 | Not an RCT. |
| Madhavan 2011 | Not an RCT. |
| Maguire 1996a | Not an RCT. Pre‐post assessment of a 3‐5‐day course on key communication skills for HCP in cancer care. Measurement with simulated and real patient encounters. |
| Maguire 1996b | Not an RCT. Similar to Maguire 1996a. |
| Martinez 2009 | Not an RCT, a survey of patient satisfaction with communication/information. |
| Matrone 1990 | Not an RCT. |
| Melo 2011 | Not an RCT. A case‐control study of a course on communication, spiritual advice and death for HCP. Only subjective measurements of behaviour change and measurement of burnout. |
| O'Connor 2011 | Not an RCT. A survey of focus groups including pharmacists, nurses and doctors. |
| Parle 1997 | Not an RCT. Post‐course assessment of a 3‐day workshop on difficult situations. Only subjective assessment of behavioural change reported. |
| Pekmezaris 2011 | Not an RCT. Pre‐post assessment of a course for residents about end of life care. Only subjective measurement of behavioural change are reported. |
| Pelayo 2011 | RCT of on‐line course on palliative care. Only subjective measurement of behavioural change reported. |
| Pieterse 2006 | Not an RCT. Pre‐ and post‐test study of CST for genetic counsellors. |
| Rask 2009 | RCT of a 33‐hour CST course for nurses. No objective measurement of behaviour change reported. Assessment of patient perception of HCP's skills. |
| Razavi 1991 | Not an RCT. Study of a brief psychological training for HCP working with terminal cancer patients. Only subjective measurements of behaviour and attitude change reported. |
| Razavi 2000 | Not an RCT. Study comparing different simulated patients to measure behavioural change after CST. |
| Razavi 2009 | Not an RCT, a summary of research. |
| Rose 2008 | Not an RCT. A review of psycho‐oncology interventions for patients with cancer. |
| Rosenbloom 2007 | RCT of an intervention for patients with cancer comparing nurse assessment of quality of life compared to normal care. |
| Roter 1995 | RCT of CST for primary care physicians. Study not primarily related to cancer care. Assessment using audio‐tapes of encounters with distressed and non‐distressed real and simulated patients. |
| Rushton 2006 | Not an RCT. |
| Rutter 1996 | Not an RCT. |
| Schulman‐Green 2003 | Not an RCT. Qualitative study of how HCP learn about caring for the dying. |
| Shannon 2011 | Not an RCT. Post assessment study of a brief CST for nurses. Only subjective assessment of change reported. |
| Shields 2010 | An RCT of coaching for survivors of breast cancer. |
| Shipman 2008 | Not an RCT. |
| Shorr 2000 | Not an RCT. Cohort study of invention to help HCP discuss end of life issues with patients, not specifically limited to cancer care. |
| Smith 1991 | Not an RCT. Case‐controlled study of a 1‐month CST for residents. Only subjective measurement of change reported. |
| Smith 2010 | An RCT of an intervention comparing a pain/communication session to normal care for patients with cancer. |
| Street 2010 | RCT of CST training (tailored education‐coaching) for patients with cancer. |
| Szmuilowicz 2010 | An RCT of CST in HCPs who did not work specifically in cancer care. |
| Timmermans 2006 | Not an RCT. Pre‐post study of CST training for radiation oncologists. Assessment of oncologists and patient communication in audiotapes of real patient encounters. |
| Ullrich 2011 | Not an RCT. Pre‐post quasi‐RCT of CST for speech therapists. Only subjective measurement of change were reported. |
| Von Gunten 1998 | Not an RCT. Measured change in attitude/knowledge not skills, not behaviour. |
| Wetzel 2011 | RCT of training in stress management for surgeons, not communication training. Not limited to cancer care. |
| Wilkinson 1998 | Not an RCT. Cohort study with pre‐post assessment of 26‐hour CST (including knowledge, attitude and skills training) for nurses. Audiotaped patient encounters measured behavioural change. |
| Wilkinson 1999 | Not an RCT. Long‐term follow‐up of cohort study. |
| Wilkinson 2003 | Not an RCT. Cohort study with pre‐post assessment of 3‐day CST for nurses. Audiotaped patient encounters measured behavioural change. |
| Wong 2001 | Not an RCT. Post‐assessment of a course on death education for nurses. Only subjective measurement of changes reported. |
| Wuensch 2011 | RCT of communication skills training for physicians involved in conducting clinical trials in oncology. Training was aimed at improving patient understanding and acceptance of clinical trials. |
CST: communication skills training HCP: healthcare professional RCT: randomised controlled trial
Contributions of authors
PM and SR sifted and screened the retrieved titles/abstracts. At least two review authors (PM, SR, MA) classified the studies and extracted data from included studies. The original review was written by DF. PM and TL wrote the first draft of the updated review. All four current review authors read and agreed the final version.
Sources of support
Internal sources
No sources of support supplied
External sources
-
National Institute for Health Research (NIHR), UK.
This review received methodological, statistical and editorial support as part of the 10/4001/12 NIHR Cochrane Programme Grant Scheme: Optimising care, diagnosis and treatment pathways to ensure cost effectiveness and best practice in gynaecological cancer: improving evidence for the NHS.
Declarations of interest
None.
Edited (no change to conclusions)
References
References to studies included in this review
- Butow P, Cockburn J, Girgis A, Bowman D, Schofield P, D'Este C, et al. Increasing oncologists' skills in eliciting and responding to emotional cues: evaluation of a communication skills training program. Psycho‐Oncology 2008;17(3):209‐18. [DOI] [PubMed] [Google Scholar]; Girgis A, Cockburn J, Butow P, Bowman D, Schofield P, Stojanovski E, et al. Improving patient emotional functioning and psychological morbidity: Evaluation of a consultation skills training program for oncologists. Patient Education and Counseling 2009;77(3):456‐62. [DOI] [PubMed] [Google Scholar]
- Fallowfield L, Jenkins V, Farewell V, Saul J, Duffy A, Eves R. Efficacy of a Cancer Research UK communication skills training model for oncologists: a randomised controlled study. Lancet 2002;359(9307):650‐6. [DOI] [PubMed] [Google Scholar]; Fallowfield L, Jenkins V, Farewell V, Solis TI. Enduring impact of communication skills training: results of a 12‐month follow‐up. British Journal of Cancer 2003;89:1445‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]; Jenkins V, Fallowfield L. Can communication skills training alter physicians' beliefs and behavior in clinics?. Journal of Clinical Oncology 2002;20:765‐9. [DOI] [PubMed] [Google Scholar]; Shilling V, Jenkins V, Fallowfield L. Factors affecting patient and clinician satisfaction with the clinical consultation: can communication skills training for clinicians improve satisfaction?. Psycho‐Oncology 2003;12:599‐611. [DOI] [PubMed] [Google Scholar]
- Fujimori MS. Effect of communication skills training program for oncologists based on the patient preferences for communicating bad news: A randomized control trial. Psycho‐Oncology Conference: 13th World Congress of Psycho‐Oncology of the International Psycho‐Oncology Society, IPOS Antalya Turkey. Conference Start: 20111016 Conference End: 20111020. 2011:Conference Publication:[var.pagings]. [Google Scholar]
- Gibon A‐SM. Is it possible to improve radiotherapy team communication skills? A randomized study assessing the efficacy of a training program in the context of an encounter with a simulated anxious patient called Mrs Leblanc. Psycho‐Oncology. 2011; Vol. 13th World Congress of the International Psycho‐Oncology Society 16/01/2011 ‐20/01/2011, Antalya, Turkey:[Var. pagings]. [Google Scholar]
- Goeltz TW. The transition from curative to palliative care in oncology‐a special challenge requires special communication skills training. Evaluation of a specific and individualized training concept‐a RCT. Psycho‐Oncology Conference: 11th World Congress of Psycho‐Oncology of the International Psycho‐Oncology Society, IPOS Vienna Austria. Conference Start: 20090621 Conference End: 20090625. 2009:Conference Publication:[var.pagings]. [Google Scholar]; Goelz T, Wuensch A, Stubenrauch S, Ihorst G, Figueiredo M, Bertz H, et al. Specific training program improves oncologists' palliative care communication skills in a randomized controlled trial. Journal of Clinical Oncology 2011;29(25):3402‐7. [DOI] [PubMed] [Google Scholar]; Goelz TW. Psycho‐Oncology; Conference(var.pagings). Conference Publication, 2010; Vol. 19(Suppl 2):S1‐S313. [Google Scholar]
- Heaven C, Clegg J, Maguire P. Transfer of communication skills training from workshop to workplace: the impact of clinical supervision. Patient Education and Counselling 2006;60(3):313‐25. [DOI] [PubMed] [Google Scholar]
- Kruijver IPM, Kerkstra A, Kerssens JJ, Bensing JM, Wiel HBM, Wind RM, et al. Communication between nurses and admitted cancer patients: the impact of a communication training program on nurse and patient outcomes. Chapter 5: Kruijver thesis145‐66. ; Kruijver IPM, Kerkstra A, Kerssens JJ, Holtkamp CCM, Bensing JM, Wiel HBM. Communication between nurses and simulated patients with cancer: evaluation of a communication training programme (including commentary by Heaven C and Payne S). European Journal of Oncology Nursing 2001;5(3):140‐53. [DOI] [PubMed] [Google Scholar]
- Bragard I, Etienne AM, Libert Y, Merckaert I, Lienard A, Meunier J, et al. Efficacy of a communication and stress management training on residents' stress to communicate, self‐efficacy and burnout level: A randomized controlled study [conference abstract]. Psycho‐Oncology: the 11th World Congress of Psycho‐Oncology of the International Psycho‐Oncology Society, IPOS Vienna Austria, 21‐25 June 2009. Conference publication, 2009:var. pagings. [Google Scholar]; Damas AM. Impact of a communication skills training program on residents' bad news disclosure in a simulated consultation: A randomised study. Psycho‐Oncology Conference abstract: 11th World Congress of Psycho‐Oncology of the International Psycho‐Oncology Society, IPOS, Vienna, Austria. 2009. [Google Scholar]; Gibon A‐SM. The efficacy of a communication skills training program on successive sequences of breaking bad news simulated consultation: A randomized controlled study. Psycho‐Oncology Conference: 11th World Congress of Psycho‐Oncology of the International Psycho‐Oncology Society, IPOS Vienna Austria. Conference Start: 20090621 Conference End: 20090625. 2009:Conference Publication:[var.pagings]. [Google Scholar]; Hasoppe SJM. Communication skills training: A study of residents' psychological and physiological variables which facilitate or inhibit the learning of assessment.. Psycho‐Oncology Conference abstract: 11th World Congress of Psycho‐Oncology of the International Psycho‐Oncology Society, IPOS, Vienna, Austria. 2009. [Google Scholar]; Lienard A, Merckaert I, Libert Y, Bragard I, Delvaux N, Etienne M, et al. Is it possible to improve residents breaking bad news skills? A randomised study assessing the efficacy of a communication skills training program. British Journal of Cancer 2010;103(2):171‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]; Lienard A, Merckaert I, Libert Y, Bragard I, Delvaux N, Etienne M, et al. Transfer of communication skills to the workplace during clinical rounds: impact of a program for residents. PLoS ONE: www.plosone.org 2010;5(8):e12426. [DOI] [PMC free article] [PubMed] [Google Scholar]; Lienard AM. Is it possible to improve residents breaking bad news skills? A randomised study assessing the efficacy of a communication skills training program. Psycho‐Oncology Conference: 11th World Congress of Psycho‐Oncology of the International Psycho‐Oncology Society, IPOS Vienna Austria. Conference Start: 20090621 Conference End: 20090625. 2009:Conference Publication:[var.pagings]. [Google Scholar]; Lienard AM. Transfer of communication skills training to workplace: Impact of a program for residents. Psycho‐Oncology Conference: 11th World Congress of Psycho‐Oncology of the International Psycho‐Oncology Society, IPOS Vienna Austria. Conference Start: 20090621 Conference End: 20090625. 2009:Conference Publication:[var.pagings]. [Google Scholar]
- Delvaux N, Razavi D, Marchal S, et al. The effects of a 24hr psychological training programme on attitudes, communication skills and occupational stress in oncology: a randomised study [abstract]. Quality of Life Research 1993;2:55‐6. [Google Scholar]; Razavi D, Delvaux N, Marchal S, Bredart A, Farvacques C, Paesmans M. The effects of a 24‐h psychological training program on attitudes, communication skills and occupational stress in oncology: a randomised study. European Journal of Cancer 1993;29A(13):1858‐63. [DOI] [PubMed] [Google Scholar]
- Canivet DD. Impact of a communication skills training on nurses communication efficiency: A qualitative analysis of an encounter with Mrs Gudule, a simulated cancer patient anxious about taking morphine. Psycho‐Oncology Conference: 13th World Congress of Psycho‐Oncology of the International Psycho‐Oncology Society, IPOS Antalya Turkey. Conference Start: 20111016 Conference End: 20111020. 2011:Conference Publication:[var.pagings]. [Google Scholar]; Delvaux N, Razavi D, Marchal S, Bredart A, Farvacques C, Slachmuylder JL. Effects of a 105 hours psychological training program on attitudes, communication skills and occupational stress in oncology: a randomised study. British Journal of Cancer 2004;90(1):106‐14. [DOI] [PMC free article] [PubMed] [Google Scholar]; Gibon A‐S, Durieux JF, Merckaert I, Delvaux N, Farvacques C, Libert Y, et al. Development of the Lacomm, a French Medical Communication Analysis Software: A Study Assessing its Sensitivity to Change. Psycho‐Oncology. Conference Publication, 2010; Vol. 19(Suppl 2):S1‐313. [DOI] [PubMed] [Google Scholar]; Razavi D, Delvaux N, Marchal S, Durieux J‐F, Farvacques C, Dubus L, et al. Does training increase the use of more emotionally laden words by nurses when talking with cancer patients? A randomised study. British Journal of Cancer 2002;87:1‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bragard I, Libert Y, Etienne AM, Merckaert I, Delvaux N, Marchal S, et al. Insight on variables leading to burnout in cancer physicians. Journal of Cancer Education: the official journal of the American Association for Cancer 2010;25:109‐15. [DOI] [PubMed] [Google Scholar]; Delvaux N, Merckaert I, Marchal S, Libert Y, Conradt S, Boniver J, et al. Physicians' communication with a cancer patient and a relative: a randomised study assessing the efficacy of consolidation workshops. Cancer 2005;103(11):2397‐411. [DOI] [PubMed] [Google Scholar]; Lienard A, Merckaert I, Libert Y, Delvaux N, Marchal S, Boniver J, et al. Factors that influence cancer patients' and relatives' anxiety following a three‐person medical consultation: impact of a communication skills training program for physicians. Psycho‐Oncology 2008;17(5):488‐96. [DOI] [PubMed] [Google Scholar]; Lienard A, Merckaert I, Libert Y, Delvaux N, Marchal S, Boniver J, et al. Factors that influence cancer patients' anxiety following a medical consultation: impact of a communication skills training programme for physicians. Annals of Oncology: the official journal of the European Society for Medical Oncology / ESMO 2006;17(9):1450‐8. [PUBMED: 16801333] [DOI] [PubMed] [Google Scholar]; Merckaert I, Libert Y, Delvaux N, Marchal S, Boniver J, Etienne AM, et al. Factors influencing physicians' detection of cancer patients' and relatives' distress: can a communication skills training program improve physicians' detection?. Psycho‐Oncology 2008;17(3):260‐9. [DOI] [PubMed] [Google Scholar]; Merckaert I, Libert Y, Delvaux N, Marchal S, Boniver J, Etienne AM, et al. Factors that influence physicians' detection of distress in patients with cancer: can a communication skills training program improve physicians' detection?. Cancer 2005;104(2):411‐21. [DOI] [PubMed] [Google Scholar]; Razavi D, Merckaert I, Marchal S, Libert Y, Conradt S, Boniver J, et al. How to optimise physicians' communication skills in cancer care: results of a randomised study assessing the usefulness of post‐training consolidation workshops. Journal of Clinical Oncology : official journal of the American Society of Clinical Oncology 2003;21(16):3141‐9. [PUBMED: 12915605] [DOI] [PubMed] [Google Scholar]
- Stewart M, Brown JB, Hammerton J, Donner A, Gavin A, Holliday RL, et al. Improving communication between doctors and breast cancer patients. Annals of Family Medicine 2007;5(5):387‐94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koropchak CM, Pollak KI, Arnold RM, Alexander SC, Skinner CS, Olsen MK, et al. Studying communication in oncologist‐patient encounters: the SCOPE Trial. Palliative Medicine 2006;20(8):813‐9. [DOI] [PubMed] [Google Scholar]; Rodriguez KLB. How oncologists and their patients with advanced cancer communicate about health‐related quality of life. Psycho‐Oncology 2010;19(5):490‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]; Skinner CSP. Use of and reactions to a tailored CD‐ROM designed to enhance oncologist‐patient communication: The SCOPE trial intervention. Patient Education and Counseling 2009;77(1):90‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]; Tulsky JA, Arnold RM, Alexander SC, Olsen MK, Jeffreys AS, Rodriguez KL, et al. Enhancing communication between oncologists and patients with a computer‐based training program: a randomized controlled trial. Annals of Internal Medicine Nov 2011;155:593‐601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weert JC, Jansen J, Spreeuwenberg PM, Dulmen S, Bensing JM. Effects of communication skills training and a Question Prompt Sheet to improve communication with older cancer patients: a randomized controlled trial. Critical Reviews in Oncology‐Hematology 2011;80(1):145‐59. [DOI] [PubMed] [Google Scholar]
- Wilkinson S, Perry R, Blanchard K, Linsell L. Effectiveness of a three‐day communication skills course in changing nurses' communication skills with cancer/palliative care patients: a randomised controlled trial. Palliative Medicine 2008;22(4):365‐75. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
- Archer M, Daniel R, Riley J, Wynburne J. Empowering people with cancer. Expert Review of Anticancer Therapy 2004;4(3 Suppl. 1):S51‐7. [DOI] [PubMed] [Google Scholar]
- Ades T, Gansler T, Eyre H. Communicating with patients about quality of life issues. CA: A Cancer Journal for Clinicians 2001;51(4):211‐2. [DOI] [PubMed] [Google Scholar]
- Alexander SC, Keitz SA, Sloane R, Tulsky JA. A controlled trial of a short course to improve residents' communication with patients at the end of life. Academic Medicine 2006;81(11):1008‐12. [DOI] [PubMed] [Google Scholar]
- Anderson JL. Evaluation of a practical approach to teaching about communication with terminal cancer patients. Medical Education 1982;16(4):202‐7. [DOI] [PubMed] [Google Scholar]
- Andrew M. The dilemmas of experiential teaching: toward an interpretive approach. Journal of Continuing Education in Nursing 1998;29(2):73‐8. [DOI] [PubMed] [Google Scholar]
- Arranz P, Ulla SM, Ramos JL, Rincón C, López‐Fando T. Evaluation of a counselling training program for nursing staff. Patient Education & Counseling 2005;56(2):233‐9. [DOI] [PubMed] [Google Scholar]
- Arrighi E, Jovell AJ, Navarro MD. Therapeutic value in oncology. Patients', caregivers' and professionals' perspective [El valor terapeutico en oncologia. La perspectiva de pacientes, familiares y profesionales]. Psicooncologia 2010;2‐3:363‐74. [Google Scholar]
- Back AL. How should physicians communicate the transition to palliative care?. Nature Clinical Practice Oncology 2005;2(3):136‐7. [DOI] [PubMed] [Google Scholar]
- Back AL, Arnold RM, Baile WF, Fryer‐Edwards KA, Alexander SC, Barley GE, et al. Efficacy of communication skills training for giving bad news and discussing transitions to palliative care. Archives of Internal Medicine 2007;167(5):453‐60. [DOI] [PubMed] [Google Scholar]
- Baile WF, Lenzi R, Kudelka AP, Maguire P, Novack D, Goldstein M, et al. Improving physician‐patient communication in cancer care: outcome of a workshop for oncologists. Journal of Cancer Education 1997;12(3):166‐73. [DOI] [PubMed] [Google Scholar]
- Baile WF, Kudelka AP, Beale EA, Glober GA, Myers EG, Greisinger AJ, et al. Communication skills training in oncology. Description and preliminary outcomes of workshops on breaking bad news and managing patient reactions to illness. Cancer 1999;86(5):887‐97. [PubMed] [Google Scholar]
- Berman S, Villarreal S. Use of a seminar as an aid in helping interns care for dying children and their families. Clinical Pediatrics 1983;22(3):175‐9. [DOI] [PubMed] [Google Scholar]
- Bernard M, Roten Y, Despland JN, Stiefel F. Communication skills training and clinicians' defenses in oncology: an exploratory, controlled study. Psycho‐Oncology 2010;19(2):209‐15. [DOI] [PubMed] [Google Scholar]
- Bird J, Hall A, Maguire P, Heavy P. Workshops for consultants on the teaching of communication skills. Medical Education 1993 1993;27:181‐5. [DOI] [PubMed] [Google Scholar]
- Booth K, Maguire PM, Butterworth T, Hillier VF. Perceived professional support and the use of blocking behaviours by hospice nurses. Journal of Advanced Nursing 1996;24(3):522‐7. [DOI] [PubMed] [Google Scholar]
- Brown JB, Boles M, Mullooly JP, Levinson W. Effect of clinician communication skills training on patient satisfaction. A randomized, controlled trial. Annals of Internal Medicine 1999;131(11):822‐9. [DOI] [PubMed] [Google Scholar]
- Brown RF, Butow PN, Boyle F, Tattersall MH. Seeking informed consent to cancer clinical trials; evaluating the efficacy of doctor communication skills training. Psycho‐Oncology 2007;16(6):507‐16. [DOI] [PubMed] [Google Scholar]
- Brown R, Bylund CL, Siminoff LA, Slovin SF. Seeking informed consent to Phase I cancer clinical trials: Identifying oncologists' communication strategies. Psycho‐Oncology 2011;4:361‐8. [DOI] [PubMed] [Google Scholar]
- Bernhard J, Butow P, Aldridge J, Juraskove I, Ribi K, Brown R. Communication about standard treatment options and clinical trials: can we teach doctors new skills to improve patient outcomes?. Psycho‐Oncology 2011;epub www.wileyonlinelibrary.com:DOI: 10.1002/pon.2044. [DOI] [PubMed] [Google Scholar]; Bernhard JB. An international randomized trial of skills training for oncologists concerning communication about standard treatment options and clinical trials with patients with early breast cancer. Psycho‐Oncology Conference: 11th World Congress of Psycho‐Oncology of the International Psycho‐Oncology Society, IPOS Vienna Austria. Conference Start: 20090621 Conference End: 20090625. Conference Publication, 2009:var.pagings. [Google Scholar]; Brown R. Meeting breast cancer patients' decision‐making preferences in oncology consultations: Impact on decision specific outcomes. Psycho‐Oncology Conference: 13th World Congress of Psycho‐Oncology of the International Psycho‐Oncology Society, IPOS Antalya Turkey. Conference Start: 20111016 Conference End: 20111020. Conference Publication:[var.pagings]., 2011. [Google Scholar]; Brown R, Butow P, Wilson‐Genderson M, Bernhard J, Ribi K, Juraskova I. Meeting the decision‐making preferences of patients with breast cancer in oncology consultations: impact on decision‐related outcomes. Journal of Clinical Oncology 2012;30(8):857‐62. [DOI] [PubMed] [Google Scholar]
- Burgess CCB. Promoting early presentation of breast cancer: Development of a psycho‐educational intervention. Chronic Illness 2008;4(1):13‐27. [DOI] [PubMed] [Google Scholar]
- Bylund CL, Brown R, Gueguen JA, Diamond C, Bianculli J, Kissane DW. The implementation and assessment of a comprehensive communication skills training curriculum for oncologists. Psycho‐Oncology 2010;19(6):583‐93. [DOI] [PubMed] [Google Scholar]
- Bylund CL, Brown RF, Bialer PA, Levin TT, Lubrano di Ciccone B, Kissane DW, et al. Developing and implementing an advanced communication training program in oncology at a comprehensive cancer center. Journal of Cancer Education 2011;26(4):604‐11. [DOI] [PubMed] [Google Scholar]
- Bylund CL, Goytia J, D'Agostino A, Bulone L, Horner J, Li Y, et al. Evaluation of a pilot communication skills training intervention for minority cancer patients. Journal of Pyschosocial Oncology 2011;29(4):347‐59. [PMC free article] [PubMed] [Google Scholar]
- Cantwell BM, Ramirez AJ. Doctor‐patient communication: a study of junior house officers. Medical Education 1997;31(1):17‐21. [DOI] [PubMed] [Google Scholar]
- Caps E, Libert Y, Marchal S, Bragard I, Etienne AM. Optimizing team members communication skills in radiation therapy: content and feasibility of a Belgian Inter‐university curriculum. Psycho‐Oncology; conference (var. pagings). 2010; Vol. 19 (Suppl 2):S1‐313. [Google Scholar]
- Chandawarkar RYR. Pretraining and posttraining assessment of residents' performance in the fourth accreditation council for graduate medical education competency: Patient communication skills. Archives of Surgery 2011;146(8):916‐21. [DOI] [PubMed] [Google Scholar]
- Charlton R. Education about death and dying at Otago University Medical School. New Zealand Medical Journal 1993;106(966):447‐9. [PubMed] [Google Scholar]
- Clark P. Reducing psychological distress in the in‐patient oncology treatment setting using FLEX Care: An intervention study. Psycho‐Oncology Conference: 6th Annual Conference of the American Psychosocial Oncology Society, APOS Charlotte, NC United States. Conference Start: 20090205 Conference End: 20090208. 2009:Conference Publication:[var.pagings]. [Google Scholar]
- Claxton R, Marks S, Buranosky R, Rosielle D, Arnold RM. The educational impact of weekly e‐mailed fast facts and concepts. Journal of Palliative Medicine 2011;14(4):475‐81. [DOI] [PubMed] [Google Scholar]
- Connolly M, Perryman J, McKenna Y, Orford J, Thomson L, Shuttleworth J, et al. SAGE & THYME: a model for training health and social care professionals in patient‐focussed support. Patient Education and Counseling 2010;79(1):87‐93. [DOI] [PubMed] [Google Scholar]
- Cort E, Moorey S, Hotopf M, Kapari M, Monroe B, Hansford P, et al. Palliative care nurses' experiences of training in cognitive behaviour therapy and taking part in a randomised controlled trial. International Journal of Palliative Nursing 2009;15(6):290‐8. [DOI] [PubMed] [Google Scholar]
- Cowan DH, Laidlaw JC, Russell ML. A strategy to improve communication between health care professionals and people living with cancer: II. Follow‐up of a workshop on the teaching and assessment of communication skills in Canadian Medical Schools. Journal of Cancer Education 1997;12(3):161‐5. [DOI] [PubMed] [Google Scholar]
- Craytor JK, Brown JK, Morrow GR. Assessing learning needs of nurses who care for persons with cancer. Cancer Nursing 1978 1978;1(3):211‐20. [PubMed] [Google Scholar]
- No authors listed. The critical need to communicate effectively with the children of cancer patients. Journal of Supportive Oncology 2006;4(2):75‐6. [PubMed] [Google Scholar]
- Bie RP, Massuger LF, Lenselink CH, Derksen YH, Prins JB, Bekkers RL. The role of individually targeted information to reduce anxiety before colposcopy: a randomised controlled trial. British Journal of Obstetrics and Gynaecology 2011;118(8):945‐50. [DOI] [PubMed] [Google Scholar]
- Del VA, Bavelas J, Healing S, MacLean G, Kirk P. An experimental investigation of the dilemma of delivering bad news. Patient Education and Counselling 2009;77(3):443‐9. [DOI] [PubMed] [Google Scholar]
- Delvaux N, Razavi D. Psychological training for health‐care professionals in oncology. A way to improve communication skills. Annals of the New York Acadamy of Science 1997;809:336‐49. [DOI] [PubMed] [Google Scholar]
- Rond MEJ, Wit R, Dam FSA, Muller MJ. A pain monitoring program for nurses: effects on communication, assessment and documentation of patients' pain. Journal of Pain & Symptom Management 2000;20(6):424‐39. [DOI] [PubMed] [Google Scholar]
- Dixon H, Hordern A, Borland R. The Breast Cancer Distance Education Program: development and evaluation of a course for specialist breast cancer nurses. Cancer Nursing 2001;24(1):44‐52. [DOI] [PubMed] [Google Scholar]
- Durgahee T. Reflective practice: nursing ethics through story telling. Nursing Ethics: an International Journal for Health Care Professionals 1997;4(2):135‐46. [DOI] [PubMed] [Google Scholar]
- Fallowfield L, Lipkin M, Hall A. Teaching senior oncologists communication skills: results from phase I of a comprehensive longitudinal program in the United Kingdom. Journal of Clinical Oncology 1998;16(5):1961‐8. [DOI] [PubMed] [Google Scholar]
- Fallowfield L, Saul J, Gilligan B. Teaching senior nurses how to teach communication skills in oncology. Cancer Nursing 2001;24(3):185‐91. [PubMed] [Google Scholar]
- Faulkner A, Maguire P. Teaching ward nurses to monitor cancer patients. Clinical Oncology 1984;10(4):383‐9. [PubMed] [Google Scholar]
- Faulkner A. The evaluation of training programmes for communication skills in palliative care. Journal of Cancer Care 1992;1(2):75‐8. [Google Scholar]
- Favre N, Despland JN, Roten Y, Drapeau M, Bernard M, Stiefel F. Psychodynamic aspects of communication skills training: a pilot study. Supportive Care in Cancer 2007;15(3):333‐7. [DOI] [PubMed] [Google Scholar]
- Ferrell BR, Virani R, Grant M. HOPE. Home Care Outreach for Palliative Care Education. Cancer Practice 1998;6(2):79‐85. [DOI] [PubMed] [Google Scholar]
- Ferrell BR, Virani R, Grant M. Improving end‐of‐life care education in home care. Journal of Palliative Medicine 1998;1(1):11‐9. [DOI] [PubMed] [Google Scholar]
- Fineberg IC. Preparing professionals for family conferences in palliative care: Evaluation results of an interdisciplinary approach. Journal of Palliative Medicine 2005;8(4):857‐66. [DOI] [PubMed] [Google Scholar]
- Finset A, Ekeberg O, Eide H, Aspegren K. Long term benefits of communication skills training for cancer doctors. Psycho‐Oncology 2003;12:686‐93. [DOI] [PubMed] [Google Scholar]
- Fujimori M, Oba A, Koike M, Okamura M, Akizuki N, Kamiya M. Communication skills training for Japanese oncologists on how to break bad news. Journal of Cancer Education 2003;18(4):194‐201. [DOI] [PubMed] [Google Scholar]
- Fukui S, Ogawa K, Ohtsuka M, Fukui N. Effect of communication skills training on nurses' detection of patients' distress and related factors after cancer diagnosis: a randomized study. Psycho‐Oncology 2009;18:1156‐64. [DOI] [PubMed] [Google Scholar]; Fukui S, Ogawa K, Ohtsuka M, Fukui N, Fukui S, Ogawa K, et al. A randomized study assessing the efficacy of communication skill training on patients' psychologic distress and coping: nurses' communication with patients just after being diagnosed with cancer. Cancer 2008;113(6):1462‐70. [DOI] [PubMed] [Google Scholar]
- Girgis A, Sanson‐Fisher RW, McCarthy WH. Communicating with patients: surgeons' perceptions of their skills and need for training. Australia and New Zealand Journal of Surgery 1997;67(11):775‐80. [DOI] [PubMed] [Google Scholar]
- Glimelius B, Birgegard G, Hoffman K, Kvale G, Sjödén PO. Information to and communication with cancer patients: Improvements and psychosocial correlates in a comprehensive care program for patients and their relatives. Patient Education & Counselling 1995;25(2):171‐82. [DOI] [PubMed] [Google Scholar]
- Gordon GH, Rust K. Evaluating a faculty development course on medical interviewing. In: Lipkin M, Putnam SM, Lazare A editor(s). The Medical Interview: Clinical Care, Education and Research. Frontiers of Primary Care. New York, NY, USA: Springer‐Verlag, 1995:436‐447. [Google Scholar]
- Gutheil IA, Heyman JC. Communication between older people and their health care agents: results of an intervention. Health & Social Work 2005;30(2):107‐16. [DOI] [PubMed] [Google Scholar]
- Hainsworth DS. The effect of death education on attitudes of hospital nurses toward care of the dying. Oncology Nursing Forum 1996;23(6):963‐7. [PubMed] [Google Scholar]
- Hall P, Weaver L, Hupe D, Seely JF. Community‐based palliative care education: Can it improve care of the terminally ill?. Academic Medicine 1999;74(Suppl 10):S105‐7. [DOI] [PubMed] [Google Scholar]
- Hallenbeck JL, Bergen MR. A medical resident inpatient hospice rotation: experiences with dying and subsequent changes in attitudes and knowledge. Journal of Palliative Medicine 1999;2(2):197‐208. [DOI] [PubMed] [Google Scholar]
- Heaven CM, Maguire GP. Training hospice nurses to elicit patient concerns. Psycho‐Oncology; conference abstract1995; Vol. 4, issue 2. [DOI] [PubMed]
- Heaven CM, Maguire P. Training hospice nurses to elicit patient concerns. Journal of Advanced Nursing 1996;23(2):280‐6. [DOI] [PubMed] [Google Scholar]
- Hellbom M, Brandberg Y, Kurland J, Arving C, Thalén‐Lindström A, Glimelius B, et al. Assessment and treatment of psychosocial problems in cancer patients: an exploratory study of a course for nurses. Patient Education and Counseling 2001;45(2):101‐6. [DOI] [PubMed] [Google Scholar]
- Hietanen PS, Aro AR, Holli KA, Schreck M, Peura A, Joensuu HT. A short communication course for physicians improves the quality of patient information in a clinical trial. Acta Oncologica 2007;46(1):42‐8. [DOI] [PubMed] [Google Scholar]
- Hoffman M, Steinberg M. Development and implementation of a curriculum in communication skills and psycho‐oncology for medical oncology fellows. Journal of Cancer Education 2002;17(4):196‐200. [DOI] [PubMed] [Google Scholar]
- Hulsman RL, Ros WJ, Janssen M, Winnubst JA. INTERACT‐CANCER. The development and evaluation of a computer‐assisted course on communication skills for medical specialists in oncology. Patient Education & Counseling 1997;30(2):129‐41. [DOI] [PubMed] [Google Scholar]
- Hulsman RL, Ros WJ, Winnubst JA, Bensing JM. The effectiveness of a computer‐assisted instruction programme on communication skills of medical specialists in oncology. Medical Education 2002;36(2):125‐34. [DOI] [PubMed] [Google Scholar]
- Hundley G. The effectiveness of "delivering unfavorable news to patients diagnosed with cancer" training program for oncologists in Uzbekistan. Dissertation Abstracts International Section A: Humanities and Social Sciences. Orlando, Florida: University of Central Florida, 2008; Vol. 2156, issue 69:6. ; Hundley G. The effectiveness of "delivering unfavorable news to patients diagnosed with cancer" training program for oncologists in Uzbekistan. PhD dissertation2008; Vol. UMI Number: 3319247:iii‐15.
- Jefford M, Lotfi‐Jam K, Baravelli C, Grogan S, Rogers M, Krishnasamy M, et al. Development and pilot testing of a nurse‐led posttreatment support package for bowel cancer survivors. Cancer Nursing 2011;34(3):E1‐10. [DOI] [PubMed] [Google Scholar]
- Ke LS, Chiu TY, Hu WY, Lo SS, Ke LS, Chiu TY, et al. Effects of educational intervention on nurses' knowledge, attitudes, and behavioral intentions toward supplying artificial nutrition and hydration to terminal cancer patients. Supportive Care in Cancer 2008;16(11):1265‐72. [DOI] [PubMed] [Google Scholar]
- Kinnane NA, Waters T, Aranda S. Evaluation of a pilot 'peer support' training programme for volunteers in a hospital‐based cancer information and support centre. Supportive Care in Cancer 2011;19(1):81‐90. [DOI] [PubMed] [Google Scholar]
- Kruse J, Schmitz N, Woller W, Clar B, Meyer E, Grinschgl A, et al. [Effects of a psychosocial education programme to improve doctor‐patient interaction with cancer patients]. Zeitschrift für Psychosomatische Medizin und Psychotherapie 2003;49(3):232‐45. [DOI] [PubMed] [Google Scholar]
- Ladouceur R, Goulet F, Gagnon R, Boulé R, Girard G, Jacques A, et al. Breaking bad news: impact of a continuing medical education workshop. Journal of Palliative Care 2003;19(4):238‐45. [PubMed] [Google Scholar]
- Monica EL, Madea AR, Oberst MT. Empathy and nursing care outcomes. Scholarly Inquiry for Nursing Practice 1987;1:197‐213. [PubMed] [Google Scholar]
- Larbig WD. Psychosocial online counselling in breast cancer patients. Psycho‐Oncology Conference: 11th World Congress of Psycho‐Oncology of the International Psycho‐Oncology Society, IPOS Vienna Austria. Conference Start: 20090621 Conference End: 20090625. 2009:Conference Publication:[var.pagings].. [Google Scholar]
- Lenzi R, Baile WF, Costantini A, Grassi L, Parker PA. Communication training in oncology: results of intensive communication workshops for Italian oncologists. European Journal of Cancer Care 2011;20:196‐203. [DOI] [PubMed] [Google Scholar]
- Libert Y, Janne P, Razavi D, Merckaert I, Scalliet P, Delvaux N, et al. Impact of medical specialists' locus of control on communication skills in oncological interviews. British Journal of Cancer 2003;88(4):502‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Linder JF, Blais J, Enders SR, Melberg SE, Meyers FJ. Palliative education: a didactic and experiential approach to teaching end‐of‐life care. Journal of Cancer Education 1999;14(3):154‐60. [DOI] [PubMed] [Google Scholar]
- Liu J, Mok E, Wong T, Xue L, Xu B. Evaluation of an integrated communication skills training program for nurses in cancer care in Beijing, China. Nursing Research 2007;56(3):202‐9. [DOI] [PubMed] [Google Scholar]
- Lloyd‐Williams M, Lloyd‐Williams F. Communication skills: the House Officer's perception. Journal of Cancer Care 1996;5(4):151‐3. [Google Scholar]
- Loiselle CG. Training the next generation of researchers in psychosocial oncology: Research priorities and future directions. Psycho‐Oncology: Conference: 11th World Congress of Psycho‐Oncology of the International Psycho‐Oncology Society, IPOS Vienna Austria. Conference Start: 20090621 Conference End: 20090625.. 2009. [Google Scholar]
- Macauley R, Billings JA. Teaching small groups in palliative care. Journal of Palliative Medicine 2011;1:91‐5. [DOI] [PubMed] [Google Scholar]
- Madhavan S, Sanders AE, Chou WYS, Shuster A, Boone KW, Dente MA, et al. Pediatric palliative care and eHealth: Opportunities for patient‐centered care. American Journal of Preventative Medicine 2011;5 (Suppl 2):S208‐216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maguire P, Faulkner A, Booth K, Elliott C, Hillier V. Helping cancer patients disclose their concerns. European Journal of Cancer 1996;32A(1):78‐81. [DOI] [PubMed] [Google Scholar]
- Maguire P, Booth K, Elliott C, Jones B. Helping health professionals involved in cancer care acquire key interviewing skills‐‐the impact of workshops. European Journal of Cancer 1996;32A(9):1486‐9. [DOI] [PubMed] [Google Scholar]
- Martinez LS, Schwartz JS, Freres D, Fraze T, Hornik RC. Patient‐clinician information engagement increases treatment decision satisfaction among cancer patients through feeling of being informed. Patient Education and Counseling 2009;77(3):384‐90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Matrone JS. The effect of a staff development program on nursing case management competencies and patient outcomes in the acute care setting. [PhD thesis]1990; Vol. Boston College, USA.
- Melo CG, Oliver D. Can addressing death anxiety reduce health care workers' burnout and improve patient care?. Journal of Palliative Care 2011;27(4):287‐95. [PubMed] [Google Scholar]
- O'Connor M, Fisher C, French L, Halkett G, Jiwa M, Hughes J. Exploring the community pharmacist's role in palliative care: Focusing on the person not just the prescription. Patient Education and Counseling 2011;3:458‐64. [DOI] [PubMed] [Google Scholar]
- Parle M, Maguire P, Heaven C. The development of a training model to improve health professionals' skills, self‐efficacy and outcome expectancies when communicating with cancer patients. Social Science & Medicine 1997;44(2):231‐40. [DOI] [PubMed] [Google Scholar]
- Pekmezaris R, Walia R, Nouryan C, Katinas L, Zeitoun N, Alano G, et al. The Impact of an end‐of‐life communication skills intervention on physicians‐in‐training. Gerontology & Geriatrics Education 2011;32(2):152‐64. [DOI] [PubMed] [Google Scholar]
- Pelayo M, Cebrian D, Areosa A, Agra Y, Izquierdo JV, Buendia F. Effects of online palliative care training on knowledge, attitude and satisfaction of primary care physicians. BMC Family Practice 2011;12:37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pieterse AH, Dulmen AM, Beemer FA, Ausems MG, Bensing JM. Tailoring communication in cancer genetic counseling through individual video‐supported feedback: a controlled pretest‐posttest design. Patient Education and Counseling 2006;60(3):326‐35. [DOI] [PubMed] [Google Scholar]
- Rask MT, Jensen ML, Andersen J, Zachariae R. Effects of an intervention aimed at improving nurse‐patient communication in an oncology outpatient clinic. Cancer Nursing 2009;32(1):E1‐11. [DOI] [PubMed] [Google Scholar]
- Razavi D, Delvaux N, Farvacques C, Robaye E. Brief psychological training for health professionals dealing with cancer patients: a one‐year assessment. General Hospital Psychiatry 1991;13:253‐60. [DOI] [PubMed] [Google Scholar]
- Razavi D, Delvaux N, Marchal S, De CM, Farvacques C, Slachmuylder JL. Testing health care professionals' communication skills: the usefulness of highly emotional standardized role‐playing sessions with simulators. Psycho‐Oncology 2000;9:293‐302. [DOI] [PubMed] [Google Scholar]
- Razavi D. Physicians, team work and the cancer patient: The acquisition of communication skills as a promoter of care quality and as a professional stress antidote. Psycho‐Oncology Conference: 11th World Congress of Psycho‐Oncology of the International Psycho‐Oncology Society, IPOS Vienna Austria. Conference Start: 20090621 Conference End: 20090625. Conference Publication:[var.pagings], 2009. [Google Scholar]
- Rose JH, Radziewicz R, Bowmans KF, O'Toole EE. A coping and communication support intervention tailored to older patients diagnosed with late‐stage cancer. Clinical Interventions in Aging 2008;3(1):77–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosenbloom SK, Victorson DE, Hahn EA, Peterman AH, Cella D. Assessment is not enough: a randomised controlled trial of the effects of HRQL assessment on quality of life and satisfaction in oncology clinical practice. Psycho‐Oncology 2007;16(12):1069‐79. [DOI] [PubMed] [Google Scholar]
- Roter DL, Hall JA, Kern DE, Barker LR, Cole KA, Roca RP. Improving physicians' interviewing skills and reducing patients' emotional distress. A randomized clinical trial. Archives of Internal Medicine 1995;155:1877‐84. [PubMed] [Google Scholar]
- Rushton CH, Reder E, Hall B, Comello K, Sellers DE, Hutton N. Interdisciplinary interventions to improve pediatric palliative care and reduce health care professional suffering. Journal of Palliative Medicine 2006;9(4):922‐33. [DOI] [PubMed] [Google Scholar]
- Rutter DR, Iconomou G, Quine L. Doctor‐patient communication and outcome in cancer patients: An intervention. Psychology & Health 1996;12(1):57‐71. [Google Scholar]
- Schulman‐Green D. How do physicians learn to provide palliative care?. Journal of Palliative Care 2003;19(4):246‐52. [PubMed] [Google Scholar]
- Shannon SE, Long‐Sutehall T, Coombs M. Conversations in end‐of‐life care: Communication tools for critical care practitioners. Nursing in Critical Care 2011;3:124‐30. [DOI] [PubMed] [Google Scholar]
- Shields CG, Ziner KW, Bourff SA, Schilling K, Zhao Q, Monahan P, et al. An intervention to improve communication between breast cancer survivors and their physicians. Journal of Psychosocial Oncology 2010;28(6):610‐29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shipman C, Burt J, Ream E, Beynon T, Richardson A, Addington‐Hall J. Improving district nurses' confidence and knowledge in the principles and practice of palliative care. Journall of Advanced Nursing 2008;63(5):494‐505. [DOI] [PubMed] [Google Scholar]
- Shorr AF, Niven AS, Katz DE, Parker JM, Eliasson AH. Regulatory and educational initiatives fail to promote discussions regarding end‐of‐life care. Journal of Pain & Symptom Management 2000;19(3):165‐73. [DOI] [PubMed] [Google Scholar]
- Smith RC, Osborn G, Hoppe RB, Lyles JS, Egeren LV, Henry R, et al. Efficacy of a one‐month training block in psychosocial medicine for residents: a controlled study. Journal of General Internal Medicine 1991;6:535‐43. [DOI] [PubMed] [Google Scholar]
- Smith MY, DuHamel KN, Egert J, Winkel G. Impact of a brief intervention on patient communication and barriers to pain management: results from a randomized controlled trial. Patient Education and counseling 2010;81(1):79‐86. [DOI] [PubMed] [Google Scholar]
- Street RL, Slee C, Kalauokalani DK, Dean DE, Tancredi DJ, Kravitz RL. Improving physician‐patient communication about cancer pain with a tailored education‐coaching intervention. Patient Education and Counseling 2010;80(1):42‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Szmuilowicz E, el‐Jawahri A, Chiappetta L, Kamdar M, Block S. Improving residents' end‐of‐life communication skills with a short retreat: a randomized controlled trial. Journal of Palliative Medicine 2010;13(4):439‐52. [DOI] [PubMed] [Google Scholar]
- Timmermans LM, Maazen RW, Leer JW, Kraaimaat FW. Palliative or curative treatment intent affects communication in radiation therapy consultations. Psycho‐Oncology 2006;15(8):713‐25. [DOI] [PubMed] [Google Scholar]; Timmermans LM, Maazen RW, Spaendonck KP, Leer JW, Kraaimaat FW. Enhancing patient participation by training radiation oncologists. Patient Education and Counseling 2006;63(1‐2):55‐63. [DOI] [PubMed] [Google Scholar]
- Ullrich P, Wollbruck D, Danker H, Singer S. Evaluation of psycho‐social training for speech therapists in oncology. Impact on general communication skills and empathy. A qualitative pilot study. Journal of Cancer Education 2011;26(2):294‐300. [DOI] [PubMed] [Google Scholar]
- Gunten CF, Martinez J, Neely KJ, Twaddle M, Preodor M. Clinical experience in hospice and palliative medicine for clinicians in practice. Journal of Palliative Medicine 1998;1(3):249‐55. [DOI] [PubMed] [Google Scholar]
- Wetzel CM, George A, Hanna GB, Athanasiou T, Black SA, Kneebone RL, et al. Stress management training for surgeons‐a randomized, controlled, intervention study. Annals of Surgery 2011;253(3):488‐94. [DOI] [PubMed] [Google Scholar]
- Wilkinson S, Roberts A, Aldridge J. Nurse‐patient communication in palliative care: an evaluation of a communication skills programme. Palliative Medicine 1998;12(1):13‐22. [DOI] [PubMed] [Google Scholar]
- Wilkinson S, Bailey K, Aldridge J, Roberts A. A longitudinal evaluation of a communication skills programme. Palliative Medicine 1999;13(4):341‐8. [DOI] [PubMed] [Google Scholar]
- Wilkinson SM Leliopoulou C, Gambles M, Roberts A. Can intensive three‐day programmes improve nurses' communication skills in cancer care?. Psycho‐Oncology 2003;12(8):747‐59. [DOI] [PubMed] [Google Scholar]
- Wong FK, Lee WM, Mok E. Educating nurses to care for the dying in Hong Kong: a problem‐based learning approach. Cancer Nursing 2001;24(2):112‐21. [DOI] [PubMed] [Google Scholar]
- Wuensch A, Goelz T, Bertz H, Wirsching M, Fritzsche K. Disclosing information about randomised controlled trials in oncology: training concept and evaluation of an individualised communication skills training for physicians COM‐ON‐rct. European Journal of Cancer Care 2011;20(5):570‐6. [DOI] [PubMed] [Google Scholar]; Wuensch A, Goelz T, Ihorst G, Terris DD, Bertz H, Bengel J, et al. Effects of individualised communication skills training on physicians' discussion of clinical trials in oncology: results from a randomised controlled trial. Unpublished manuscript2011. [DOI] [PMC free article] [PubMed]; Wuensch AG. Individualised communication skills training for randomized clinical trials and therapy options in oncology. training concept and results of a RCT. Psycho‐Oncology Conference: 11th World Congress of Psycho‐Oncology of the International Psycho‐Oncology Society, IPOS Vienna Austria. Conference Start: 20090621 Conference End: 20090625. 2009:Conference Publication:[var.pagings]. [Google Scholar]
Additional references
- Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et al. The European Organization for Research and Treatment of Cancer QLQ‐C30: A Quality‐of‐Life Instrument for Use in International Clinical Trials in Oncology. Journal of the National Cancer Institute 1993;85(5):365‐76. [DOI] [PubMed] [Google Scholar]
- ACGME (Accreditiation Council for Graduate Medical Education). Common Program Requirements. ACGME 2009. Available from: http://www.acgme.org/acWebsite/dutyHours/dh_dutyhoursCommonPR07012007.pdf.
- Adamo G. Simulated and standardized patients in OSCEs: achievements and challenges 1992‐2003. Medical Teacher 2003;25(3):262‐70. [DOI] [PubMed] [Google Scholar]
- Alvarez MP, Agra Y. Systematic review of educational interventions in palliative care for primary care physicians. Palliative Medicine 2006;20(7):673‐83. [DOI] [PubMed] [Google Scholar]
- Ashworth CD, Williamson P, Montano D. A scale to measure physician beliefs about psychosocial aspects of patient care. Social Science & Medicine 1984;19(11):1235‐8. [DOI] [PubMed] [Google Scholar]
- Aspegren K. BEME guide No. 2: Teaching and learning communication skills in medicine: a review with quality grading of articles. Medical Teaching 1999;21(6):563‐70. [DOI] [PubMed] [Google Scholar]
- Barth JL. Efficacy of communication skills training courses in oncology: A systematic review and meta‐analysis. Annals of Oncology 2011;22(5):1030‐40. [DOI] [PubMed] [Google Scholar]
- Blanchard CG, Ruckdeschel JC, Fletcher BA, Blanchard EB. The impact of oncologists' behaviors on patient satisfaction with morning rounds. Cancer 1986;58(2):387‐93. [DOI] [PubMed] [Google Scholar]
- Booth K, Maguire P. Development of a rating system to assess interaction between cancer patients and health professionals. Report to Cancer Research Campaign 1991, London, United Kingdom:37.
- Brown J Stewart M Tessier S. Assessing Communiction between Patients and doctors: A Manual for scoring Patient Centered Communication. Centre for studies in Family Medicine and Thames Valley Family Practice Research Unit1995; Vol. Working paper Series:95‐102.
- Bylund CL, Brown RF, Lubrano di CB, Diamond C, Eddington J, Kissane DW. Assessing facilitator competence in a comprehensive communication skills training programme. Medical Education 2009;43(4):342‐9. [DOI] [PubMed] [Google Scholar]
- Royal College of Physicians and Surgeons of Canada. CanMEDS: better standards, better physicians, better care. Available at: http://www.royalcollege.ca/public/resources/aboutcanmeds2011.
- Cegala DJ, Lenzmeier Broz S. Physician communication skills training: a review of theoretical backgrounds, objectives and skills. Medical Education 2002;36(11):1004‐16. [DOI] [PubMed] [Google Scholar]
- Chant S, Jenkinson T, Randle J, Russell G. Communication skills: some problems in nursing education and practice. Journal of Clinical Nursing 2002;11:12‐21. [DOI] [PubMed] [Google Scholar]
- Deeks JJ, Altman DG, Bradburn MJ. Statistical methods for examining heterogeneity and combining results from several studies in meta‐analysis. In: Egger M, Davey Smith G, Altman DG editor(s). Systematic Reviews in Health Care: Meta‐Analysis in Context. 2nd Edition. London: BMJ Publication Group, 2001. [Google Scholar]
- Derogatis l. SCL‐90(R): Administration, scoring and procedures manual for the revised version of other instruments of the psychopathology rating scale series. Baltimore: Baltimore Md: Clinical Psychometrics Research Unit, John Hopkins Univsersity of Medicine 1977, 1977. [Google Scholar]
- DerSimonian R, Laird N. Meta‐analysis in clinical trials. Controlled Clinical Trials 1986;7:177‐88. [DOI] [PubMed] [Google Scholar]
- Donovan‐Kicken E, Caughlin JP. Breast cancer patients' topic avoidance and psychological distress: the mediating role of coping. Journal of Health Psychology 2011;16(4):596‐606. [DOI] [PubMed] [Google Scholar]
- Dowsett SM, Saul JL, Butow PN, Dunn SM, Boyer MJ, Findlow R, et al. Communication styles in the cancer consultation: preferences for a patient‐centred approach. Psychooncology 2000;9(2):147‐56. [DOI] [PubMed] [Google Scholar]
- Fallowfield LJ, Hall A, Maguire GP, Baum M. Psychological outcomes of different treatment policies in women with early breast cancer outside a clinical trial. BMJ 1990;301:575‐80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fallowfield, L. Communication skills for oncologists. Clinical Medicine 1995;5(1):99‐103. [Google Scholar]
- Fallowfield L, Jenkins V. Communicating sad, bad, and difficult news in medicine. Lancet 2004;363(9405):24. [DOI] [PubMed] [Google Scholar]
- Ford S, Hall A, Ratcliffe D, Fallowfield L. The Medical Interaction Process System (MIPS): an instrument for analysing interviews of oncologists and patients with cancer. Social Science & Medicine 2000;50(4):553‐66. [DOI] [PubMed] [Google Scholar]
- Fujimori M, Uchitomi Y. Preferences of cancer patients regarding communication of bad news: a systematic literature review. Japanese Journal of Clinical Oncology 2009;39(4):201‐16. [DOI] [PubMed] [Google Scholar]
- Gattellari M, Butow PN, Tattersall MH. Sharing decisions in cancer care. Social Science & Medicine 2001;52(12):1865‐78. [DOI] [PubMed] [Google Scholar]
- Gibon AS, Durieux JF. Development of the Lacomm, a French medical communication analysis software: A study assessing its sensitivity to change. Psycho‐Oncology. http://www.lacomm.be/index.php, 2010; Vol. 19(Suppl.2):Oral Abstracts S133. [Google Scholar]
- Girgis A, Breen S, Stacey F, Lecathelinais C. Impact of two supportive care interventions on anxiety, depression, quality of life, and unmet needs in patients with non localized breast and colorectal cancers. Journal of Clinical Oncology 2009;27(36):6180‐90. [DOI] [PubMed] [Google Scholar]
- General Medical Council. Tomorrow's Doctors. Available from: http://www.gmc‐uk.org/education/undergraduate/tomorrows_doctors_2009.asp.
- Gray‐Toft, P, Anderson J. The Nursing Stress Scale: Development of an instrument. Journal of Behavioral Assessment 1981;3(1):11‐23. [Google Scholar]
- Gysels M, Richardson A, Higginson IJ. Communication training for health professionals who care for patients with cancer: a systematic review of effectiveness (Provisional abstract). Supportive Care in Cancer 2004;12:692‐700. [DOI] [PubMed] [Google Scholar]
- Hack TF, Degner LF, Parker PA. The communication goals and needs of cancer patients: a review. Psycho‐Oncology 2005;14(10):831‐45. [DOI] [PubMed] [Google Scholar]
- Hack TF, Ruether JD, Pickles T, Bultz BD, Chateau D, Degner LF. Behind closed doors II: systematic analysis of prostate cancer patients' primary treatment consultations with radiation oncologists and predictors of satisfaction with communication. Psycho‐Oncology 2011;May 6:Epub ahead of print. [DOI: 10.1002/pon.1984] [DOI] [PubMed] [Google Scholar]
- Hagerty RG, Butow PN, Ellis PM, Dimitry S, Tattersall MH. Communicating prognosis in cancer care: a systematic review of the literature. Annals of Oncology 2005;16(7):1005‐53. [DOI] [PubMed] [Google Scholar]
- Heaven C. The role of clinical supervision in communication skills. Vol. PhD thesis, Manchester: University of Manchester, 2001. [Google Scholar]
- Henbest RJ, Stewart M. Patient‐centredness in the consultation. 2: Does it really make a difference?. Family Practice 1990;7(1):28‐33. [DOI] [PubMed] [Google Scholar]
- Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327:557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 [updated March 2011]. Available from www.cochrane‐handbook.org, 2011. [Google Scholar]
- Hjermstad MJ, Fossa SD, Bjordal K, Kaasa S. Test/retest study of the European Organization for Research and Treatment of Cancer Core Quality‐of‐Life Questionnaire. Journal of Clinical Oncology 1995;13(5):1249‐54. [DOI] [PubMed] [Google Scholar]
- Hubbard G, Kidd L, Donaghy E. Preferences for involvement in treatment decision making of patients with cancer: a review of the literature. European Journal of Oncology Nursing 2008;12(4):299‐318. [DOI] [PubMed] [Google Scholar]
- Julian LJ. Measures of anxiety: State‐Trait Anxiety Inventory (STAI), Beck Anxiety Inventory (BAI), and Hospital Anxiety and Depression Scale‐Anxiety (HADS‐A). Arthritis Care Research 2011;63(Suppl 11):S467‐72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kissane DW, Bylund CL, Banerjee SC, Bialer PA, Levin TT, Maloney EK, et al. Communication skills training for oncology professionals. Journal of Clinical Oncology 2012;30(11):1242‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kurtz S, J Silverman, Draper J. Teaching and Learning Communication Skills in Medicine. Radcliffe Medical Press, 2005. [Google Scholar]
- La Comm, A French Communication Analysis Software. http://www.lacomm.be/Ressources/documents/htmlPosterVenise1.php Accessed 21/09/2012:1‐3.
- Levinson W, Roter DL, Mulhooly JP, Dull V, Frankel R. Physician‐patient communication: the relationship with malpractice claims among primary care physicians and surgeons. JAMA: the Journal of the American Medical Association 1997;277:553‐9. [DOI] [PubMed] [Google Scholar]
- Lussier MT, Richard C. Doctor‐patient communication: complaints and legal actions. Canadian Family Physician 2005;51:37‐9. [PMC free article] [PubMed] [Google Scholar]
- Moore P, Vargas A, Nunez S, Macchiavello S. [A study of hospital complaints and the role of the doctor‐patient communication]. Revista Medica de Chile 2011;139(7):880‐5. [PubMed] [Google Scholar]
- Nestel D, Tierney T. Role‐play for medical students learning about communication: guidelines for maximising benefits. BMC Medical Education 2007;7:3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ong LM, Visser MR, Kruyver IP, Bensing JM, Brink‐Muinen, Stouthard JM, et al. The Roter Interaction Analysis System (RIAS) in oncological consultations: psychometric properties. Psycho‐Oncology 1998;7(5):387‐401. [DOI] [PubMed] [Google Scholar]
- Paul CL, Clinton‐McHarg T, Sanson‐Fisher RW, Douglas H, Webb G. Are we there yet? The state of the evidence base for guidelines on breaking bad news to cancer patients. European Journal of Cancer 2009;45(17):2960‐6. [DOI] [PubMed] [Google Scholar]
- Ramirez AJ, Graham J, Richards MA, Cull A, Gregory WM, Leaning MS, et al. Burnout and psychiatric disorder among cancer clinicians. British Journal of Cancer 1995;71(6):1263‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.1. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2011.
- Roberts CS, Cox CE, Reintgen DS, Baile WF, Gibertini M. Influence of physician communication on newly diagnosed breast patients' psychologic adjustment and decision‐making. Cancer 1994;74(1 Suppl):336‐41. [DOI] [PubMed] [Google Scholar]
- Roter D, Larson S. The Roter interaction analysis system (RIAS): utility and flexibility for analysis of medical interactions. Patient Education and Counselling 2002;46(4):243‐51. [DOI] [PubMed] [Google Scholar]
- Samson‐Fisher R, Grigis A, Boyes A, Bonevski B, Burton L, Cook P. Supportive Care Review Group. The unmet supportive care needs of patients with cancer. Cancer 2000;88:226‐37. [DOI] [PubMed] [Google Scholar]
- Schaulell WB, van Dierendonk. The construct validity of two burnout measures. Journal of Organizational Behaviour 1993;14:631‐47. [Google Scholar]
- Sepucha K, Ozanne EM. How to define and measure concordance between patients' preferences and medical treatments: A systematic review of approaches and recommendations for standardization. Patient Education and Counselling 2010;78(1):12‐23. [DOI] [PubMed] [Google Scholar]
- Silberfarb PM, Levine PM. Psychosocial aspects of neoplastic disease. III. Group support for the oncology nurse. General Hospital Psychiatry 1980;2(3):192‐7. [DOI] [PubMed] [Google Scholar]
- Silverman J, Kurtz S, Draper J. Skills for Communicating with Patients. 2nd Edition. Oxford: Radcliffe Medical Press, 2005. [Google Scholar]
- Snaith RP, Zigmond AS. The hospital anxiety and depression scale. BMJ (Clinical Research and Education) 1986;292(6516):344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spielberger CD, Gorssuch RL, Lushene PR, Vagg PR, Jacobs GA. Manual for the State‐Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press, Inc, 1983. [Google Scholar]
- Stewart MA, Brown JB, Weston WW. Patient‐centred interviewing part III: Five provocative questions. Canadian Family Physician 1989;35:159‐61. [PMC free article] [PubMed] [Google Scholar]
- Stewart MA. Effective physician‐patient communication and health outcomes: a review. Canadian Medical Association Journal 1996;152:1423‐33. [PMC free article] [PubMed] [Google Scholar]
- Stiefel F, Barth J, Bensing J, Fallowfield L, Jost L, Razavi D, et al. Communication skills training in oncology: a position paper based on a consensus meeting among European experts in 2009. Annals of Oncology 2010;21:204‐7. [DOI] [PubMed] [Google Scholar]
- Stubenrauch S, Schneid EM, Wunsch A, Helmes A, Bertz H, Fritzsche K, et al. Development and evaluation of a checklist assessing communication skills of oncologists: the COM‐ON‐Checklist. Journal of Evaluation in Clinical Practice 2012;18(2):225‐30. [DOI] [PubMed] [Google Scholar]
- Tariman JD, Berry DL, Cochrane B, Doorenbos A, Schepp K. Preferred and actual participation roles during health care decision making in persons with cancer: a systematic review. Annals of Oncology 2010;21(6):1145‐51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taylor J. The moral aesthetics of simulated suffering in standardized patient performances. Culture, Medicine and Psychiatry 2011;35(2):134‐62. [DOI] [PubMed] [Google Scholar]
- Turnberg L. Improving communication between doctors and patients. Royal College of Physicians1997.
- Uitterhoeve RJ, Bensing JM, Grol RP, Demulder PHM, Achterberg T. The effect of communication skills training on patient outcomes in cancer care: a systematic review of the literature. European Journal of Cancer Care 2010;19:442‐57. [DOI] [PubMed] [Google Scholar]
- Vail L, Sandhu H, Fisher J, Cooke H, Dale J, Barnett M. Hospital consultants breaking bad news with simulated patients: an analysis of communication using the Roter Interaction Analysis System. Patient Education and Counselling 2011;83(2):185‐94. [DOI] [PubMed] [Google Scholar]
- Weert JC, Jansen J, Bruijn GJ, Noordman J, van DS, Bensing JM. QUOTEchemo: a patient‐centred instrument to measure quality of communication preceding chemotherapy treatment through the patient's eyes. European Journal of Cancer 2009;45(17):2967‐76. [DOI] [PubMed] [Google Scholar]
- Vogel BA, Leonhart R, Helmes AW. Communication matters: the impact of communication and participation in decision making on breast cancer patients' depression and quality of life. Patient Education and Counselling 2009;77(3):391‐7. [DOI] [PubMed] [Google Scholar]
- Ware JE Jr, Snyder MK, Wright WR, Davies AR. Defining and measuring patient satisfaction with medical care. Evaluation and Program Planning 1983;6(3‐4):247‐63. [DOI] [PubMed] [Google Scholar]
- Wilkinson S. Factors influencing nurses’ verbal communication with cancer patients. Vol. PhD Thesis, Manchester: University of Manchester, 1991. [Google Scholar]
- Williams P. A users’ guide to the general health questionnaire. NFER‐Wilson1988; Vol. Windsor.
References to other published versions of this review
- Fellowes D, Wilkinson SM, Moore PM. Communication skills training for health care professionals working with cancer patients, their families and/or carers. Cochrane Database of Systematic Reviews 2003, Issue 2. [DOI: 10.1002/14651858.CD003751] [DOI] [PubMed] [Google Scholar]
- Moore PM, Wilkinson SM, Rivera Mercado S. Communication skills training for health care professionals working with cancer patients, their families and/or carers. Cochrane Database of Systematic Reviews 2004, Issue 2. [DOI: 10.1002/14651858.CD003751.pub2] [DOI] [PubMed] [Google Scholar]