

Abstract
A multistage model of drug addiction in which individuals’ motivations for use change as they develop problems is widely accepted (Koob and Volkow, 2010); however, the evidence for this model comes mostly from animal work and cross-sectional studies. We used longitudinal data to test whether positive and negative reinforcement associated with alcohol consumption differed as a function of alcohol dependence (AD). Specifically, we tested whether: 1) positive reinforcement is more strongly associated with alcohol consumption than is negative reinforcement among individuals without AD; 2) negative reinforcement is more strongly associated with AD than is positive reinforcement; and 3) in the presence of AD, the association between positive reinforcement and alcohol consumption becomes weaker, while the association with negative reinforcement becomes stronger. We included assessments between ages 18 and 30 from participants who indicated they ever had a drink (N=2556, 51.6% female), from the Collaborative Study on the Genetics of Alcoholism Prospective Study. Results from generalized estimating equations indicated that positive reinforcement, but not negative reinforcement was associated with alcohol consumption among individuals without AD. Both positive and negative reinforcement were associated with AD, but the association was stronger with negative reinforcement. Results from the multilevel growth model indicated that, the association between negative reinforcement and alcohol consumption became stronger with the presence of AD, whereas the association between positive reinforcement and alcohol consumption did not differ as a function of AD. We provided empirical evidence that positive and negative reinforcement are differentially associated with alcohol consumption as a function of AD.
Keywords: alcohol use disorder, multistage model of drug addiction, drinking motives, alcohol expectancy, longitudinal analysis
Alcohol use disorders represent significant public health concerns due to their prevalence (14% past year and 29% lifetime) and serious personal and societal costs (Grant et al., 2015). Alcohol consumption is widespread among adolescents and adults in the United States, with 22.7% of adolescents (age 12–17) and 70.1% of adults (age 18 or older) reporting they consumed alcohol in the past year (SAMHSA, 2016). Because only a fraction of those who consume alcohol progress to develop alcohol use disorders, understanding the factors that may contribute to pathways from alcohol consumption to alcohol use disorders is important for tailoring prevention and intervention efforts.
There are different pathways of risk for alcohol consumption and misuse. Some people drink alcohol in order to enhance positive emotions and social performance, whereas others use alcohol to cope with emotional and physical stress (Cooper, Frone, Russell, & Mudar, 1995; Kuntsche, E., Knibbe, R., Gmel, G., & Engels, 2005). A variety of concepts have been used by researchers to describe individuals’ experiences with alcohol use, including concepts related to why individuals drink (i.e., drinking motives) (Cooper et al., 1995), as well as individuals’ thoughts and beliefs about alcohol use (i.e., alcohol expectancies) (Brown, Goldman, Inn & Anderson, 1980). This is further complicated by the fact that what these concepts reflect may differ as a function of individuals’ drinking experiences (e.g., before versus after drinking is initiated). For example, for individuals who have initiated drinking, alcohol expectancies may reflect their past experiences of positive and/or negative reinforcement effects of alcohol use, which also contribute to individuals’ motivations to drink. Thus, drinking motives and alcohol expectancies are closely related (although conceptually distinct) concepts (Anthenien, Lembo, & Neighbors, 2017; Cooper et al., 1995), particularly among drinkers.
Positive and negative reinforcement, either measured as drinking motives or alcohol expectancies, have been associated with alcohol use and misuse (Brown et al., 1980; Cooper et al., 1995; Kuntsche et al., 2005). Positive reinforcement generally refers to the pleasant feelings and social enhancement effects that alcohol provides, while negative reinforcement encompasses relief from negative affective states like stress or anxiety. Some studies suggest differential effects of positive and negative reinforcement across different alcohol use outcomes. Positive reinforcement of alcohol intake is generally associated with greater frequency and quantity of alcohol consumption, whereas negative reinforcement is more predictive of subsequent drinking related problems and alcohol use disorders (Grotmol et al., 2010; Jester, Steinberg, Heitzeg, & Zucker, 2015). Understanding how positive and negative reinforcement of alcohol intake may differentially influence alcohol use behaviors as individuals develop alcohol use disorder is important.
One of the theoretical models useful for understanding the potentially different roles of positive and negative reinforcement in the pathways of risk for substance use disorders is the multistage model of addiction proposed by Koob and Volkow (2010). This model proposed that the progression from occasional and limited drug use to addiction involves three stages: binge/intoxication, withdrawal/negative affect, and preoccupation/anticipation. Grounded in a psychiatric-motivational framework surrounding positive and negative reinforcement for drug taking, Koob and Volkow (2010) posited that earlier stages of addiction primarily involve impulsivity and later stages are dominated by both impulsivity and compulsivity. Impulse control disorders are characterized by failure to suppress an urge or resist a temptation such as seeking pleasure or gratification and thus are largely associated with positive reinforcement (Koob, 2013). In contrast, compulsive disorders are characterized by the relief from negative affective states, such as stress and anxiety, by committing the compulsive behavior, and they are, thus, associated with negative reinforcement (Kwako & Koob, 2017). According to this model, as individuals move from earlier to later stages of addiction there is a shift from positive reinforcement to negative reinforcement associated with drug use. Applying the multistage model of addiction to alcohol use behaviors, it can be expected that positive reinforcement of alcohol intake, such as the taste of alcohol or pleasant feelings that alcohol provide, would be more important in influencing earlier stages of drinking, such as occasional or moderate use. In contrast, in later stages such as alcohol dependence, it is expected that negative reinforcement, such as relief from negative affective states like stress or anxiety, would be more important in influencing drinking behavior.
Although the multistage model of drug addiction was mainly based on evidence from animal models and neurophysiological studies on humans (Koob and Volkow 2010), the model has also been supported in behavioral studies in humans. A review by Kuntsche and colleagues (2005) indicated that positive reinforcement, such as social and personal enhancements, were generally associated with moderate and heavy drinking, whereas negative reinforcement, such as relaxation from tension and conforming to peer pressure, was associated with alcohol-related problems, including alcohol dependence, among adolescents and young adults. Several longitudinal studies have also provided evidence that drinking motives and expectancies related to positive and negative reinforcement differentially predicted subsequent alcohol outcomes (Grotmol et al., 2010; Jester, Steinberg, Heitzeg, & Zucker, 2015; Mackinnon, Kehayes, Clar, Sherry, & Stewart, 2014; Osberg, Insana, Eggert, & Billingsley, 2011; Watkins, Franz, DiLillo, Gratz, & Messman-Moore, 2015). For example, Anderson, Briggs, and White (2013) found that positive reinforcement assessed in late adolescence or early adulthood was generally associated with quantity of drinking in adulthood, and negative reinforcement was predictive of subsequent drinking related problems but not levels of alcohol consumption. In addition, human experimental studies on individuals’ subjective response to alcohol showed that self-reported stimulation effects of alcohol were more strongly associated with alcohol craving among nonalcohol-dependent heavy drinkers than among individuals who were alcohol dependent, providing evidence for diminished positive reinforcement in alcohol dependence (Bujarski, Hutchison, Prause, & Ray, 2017; Bujarski & Ray, 2014). Other studies showed continued heightened alcohol stimulation and reward sensitivity in heavy drinkers with increasing alcohol use disorder symptoms over time, compared to light drinkers (King, Hasin, O’Connor, McNamara, & Caro, 2016; King, McNamara, Hasin, & Cao, 2014).
Taken together, these studies consistently support the notion that positive and negative reinforcement are differentially associated with drinking at different stages of alcohol addiction. However, most of the previous studies were cross-sectional, and the existing longitudinal studies tended to focus on examining how positive and negative reinforcement assessed at one time point predicted subsequent alcohol use outcomes. Such study designs do not provide evidence regarding whether the influence of positive and negative reinforcement changes in influencing drinking as an individual progresses from casual drinking to problematic drinking, which is a key proposition of the multistage model. In the present study, we used longitudinal data with repeated and concurrent measures of positive and negative reinforcement and alcohol use outcomes from late adolescence to young adulthood to examine changes in the salience of positive and negative reinforcement associated with alcohol consumption as a function of whether or not individuals met criteria for AD. Informed by the multistage model of addiction (Koob & Volkow, 2010), we examined the following three hypotheses.
Hypothesis 1:
Positive reinforcement is more strongly associated with frequency of alcohol consumption than is negative reinforcement among individuals without AD.
Hypothesis 2:
Negative reinforcement is more strongly associated with AD than is positive reinforcement.
Hypothesis 3:
With the presence of AD, the association between positive reinforcement and alcohol consumption will become weaker and the association between negative reinforcement and alcohol consumption will become stronger.
Given that rates of alcohol consumption and AD vary across race/ethnicity (Grant et al., 2015; SAMHSA, 2015) and that pathways of risk to alcohol problems may differ among individuals of different racial/ethnic backgrounds (Akins, Smith, Mosher, 2010; Su & Supple, 2014), we explored whether the patterns of associations between positive and negative reinforcement and alcohol use outcomes differ across race/ethnicity. In addition, drinking patterns also differ across sex (Grant et al., 2015; SAMHSA, 2015) and researchers have suggested that there may be sex differences in the physiological, psychological, and social factors influencing alcohol use outcomes (Schutle, Rarno, & Brown, 2009). Thus, we also explored whether the patterns of associations between positive and negative reinforcement and alcohol use outcomes differ across sex. Examination of potential differences across sex and race/ethnicity was exploratory, and thus no specific hypotheses were proposed.
Method
Sample
We used data from the Prospective Study sample of the Collaborative Study on the Genetics of Alcoholism (COGA), which has the goal of identifying genetic influences on alcohol dependence and related psychiatric outcomes (Begleiter et al. 1995). COGA recruited families with alcohol dependent probands based on both the Diagnostic and Statistical Manual of Mental Disorders, third edition, revised (DSM-III-R) (American Psychiatric Association 1987) and Feighner criteria (Feighner et al. 1972), from inpatient and outpatient alcohol treatment centers across six study sites in the United States. Population-based comparison families were also recruited. The Institutional Review Boards of all participating institutions approved the study, and written consents were obtained from all participants. Information about the design of the COGA study is described in more detail in previously published papers (Begleiter et al. 1995; Foroud et al. 2000; Reich et al., 1998).
The Prospective Study is a part of the COGA study launched in 2004 with the goal to examine how genetic risk unfolds across development and in conjunction with the environment. Offspring who were aged between 12 and 22 and had at least one parent who had previously completed an interview were recruited (Bucholz et al., 2017). Participants completed an assessment at enrollment and were followed up biennially. For the purpose of the current study, we included assessments between ages 18 and 30 if 1) the participant indicated he/she ever had a drink of alcohol at the assessment, and 2) the participant completed the Alcohol Expectancy Questionnaire (AEQ) (Brown, Christiansen, & Goldman, 1987; Brown, Goldman, Inn, & Andersen, 1980) at the assessment. We focused on assessments between ages 18 and 30 because this is a developmental period during which risk for AD peaks and stabilizes. In addition, prevalence for AD was very low for ages younger than 18 and the sample sizes were too small for ages older than 30. These resulted in an analytic sample of 6,884 assessments from 2,556 participants (51.6% female) with each individual having up to 6 assessments throughout the included age range. Of the whole analytic sample, 26.8% completed one assessment, 23.0% completed 2 assessments, 20.4% completed 3 assessments, and 29.8% completed 4 or more assessments. The resulting sample consisted of 0.59% of Native Americans, 0.2% of Asians, 0.35% of Pacific Islanders, 26.81% of African Americans, 66.34% of European Americans, and 5.71% of unknown self-identified racial identity.
Measures
Alcohol use outcomes.
Alcohol consumption at each assessment was measured by a question adapted from the Semi-Structured Assessment for the Genetics of Alcoholism (SSAGA-IV) (Bucholz et al., 1994) that assessed participants’ frequency of drinking: “On how many days did you drink any beverages containing alcohol during the last 12 months?” The responses included 13 categories ranging from 0 (Never) to 12 (Every day). Because the categories were not in equal intervals, we converted the responses into number of drinking days per year by taking the midpoint of each category. For example, the categories “Every day” and “2 days per week (100–149 days)” were converted into 365 and 124.5 days per year, respectively. Those who reported not drinking during the past year skipped the question, and their answers were recoded into zero. Alcohol dependence (AD) was measured at each assessment as part of the SSAGA-IV interview. AD status was determined based on the diagnostic criteria for AD according to the Diagnostic and Statistical Manual of Mental Disorders 4th edition (DSM-IV, American Psychiatric Association, 2000). AD was coded into a binary variable (0= absence of AD and 1= presence of AD) that indicates whether or not participants met the clinical diagnosis for AD in the past 12 months.
Positive and negative reinforcement of alcohol use.
Participants completed two subscales adapted from the Alcohol Expectancy Questionnaire (AEQ) (Brown et al., 1980; Brown et al., 1987) at each assessment. Individuals were asked to respond to statements about the effects of alcohol with respect to their “own personal thoughts, feelings, and beliefs about alcohol now”. Positive reinforcement was measured by the “Physical and Social Pleasure” subscale consisted of 9 items regarding positive affective, social, or physical states anticipated from drinking, such as “drinking makes me feel good” and “some alcohol has a pleasant, cleansing, tingly taste”. Negative reinforcement was measured by the “Relaxation and Tension Reduction” subscale consisted of 9 items related to alleviations of negative affective or physical states by using alcohol, such as “if I am tense or anxious, having a few drinks makes me feel better” and “alcohol decreases muscular tension.” A list of all the items included in these measures is presented in the Appendix. Response options for each item ranged from 1 (disagree strongly) to 5 (agree strongly). Sum score was created for each scale. Cronbach’s alphas ranged from .85 to .89 and from .87 to .92 across ages for positive and negative reinforcement, respectively.
Statistical Analysis
To evaluate Hypothesis 1, that positive reinforcement is more strongly associated with alcohol consumption than is negative reinforcement among individuals without AD, we fit a generalized estimating equation (GEE) model with logarithm link and Poisson distribution with frequency of alcohol consumption as the outcome variable and positive and negative reinforcement as predictors (N =1824, 53.1% female). Individuals diagnosed with AD at the time of assessment were excluded from this set of analyses. To test Hypothesis 2, that negative reinforcement is more strongly associated with AD than positive reinforcement, we fit a GEE model with logit link and binomial distribution that predicted AD by positive and negative reinforcement. All participants were included in this analysis (N = 2556, 51.6% female). For both models, linear and quadratic effects of age were included as covariates to take into account the non-linear trajectory of alcohol use between age 18 and 30, as previously described (Dick et al., 2014; Li et al., 2017). Age was centered at 21, where alcohol consumption started to stabilize (Dick et al., 2014; Li et al., 2017). In addition to age, sex and self-reported racial identity were included as covariates to control for the baseline differences in alcohol consumption and AD by sex and race. For race, two dummy variables were created from self-reported racial identity to represent African Americans (AA) or other races, respectively, with European Americans (EA) as the reference group. Native Americans, Asians, Pacific Islanders, and unknown racial identification were combined into other races. First-degree autoregressive covariance structure was used in all models to incorporate repeated assessments within individuals. Parameters were estimated by the GEE estimator in SAS software version 9.4 (SAS Institute, Cary, NC) using the GENMOD procedure with the REPEATED option.
To test Hypothesis 3, regarding within-individual changes in the associations between positive and negative reinforcement and alcohol consumption as a function of AD, we fit a multilevel growth model with alcohol consumption as the outcome variable. In this model, we disentangled between-person and within-person variations following the approaches described by Curran and Bauer (2011). Specifically, we created person-level means of positive and negative reinforcement (to represent between-person variance) and included them as timeinvariant, between-person covariates. We created person-mean centered variables for positive and negative reinforcement (to reflect within-person variance) and included them as time-varying, within-person predictors, along with AD, and the 2-way interactions between them. Because AD was coded binary, parameters for the 2-way interaction effects represent changes in the associations between positive/negative reinforcement and alcohol consumption as a function of the presence of AD. As in the previous models, linear and quadratic effects of age were included as time-varying covariates, and sex and self-reported race were included as timeinvariant covariates. Random effects of the intercept, linear and quadratic slopes of age, and all time-varying predictors were examined, with non-significant random effects constrained to zero to yield a parsimonious final analytic model. The alcohol consumption variable was rescaled (divided by 100) for the purpose of model convergence. Parameters were estimated using maximum likelihood estimation with robust standard errors in Mplus, which is robust to nonnormality of variables and non-independence of observations (Muthén & Muthén, 1998–2012).
To examine potential differences in the patterns of associations across sex and racial groups, we conducted analyses as described above separately for males and females, as well as separately for EA and AA, the two largest racial groups included in the sample. In analyses conducted separately across sex groups, sex was excluded from the model. Similarly, self-reported racial identity was removed from the analytic models when conducting analyses separately for EA and AA.
Results
Descriptive Statistics
Table 1 provides descriptive statistics of alcohol use outcomes and positive and negative reinforcement by age. Both frequency of alcohol consumption and proportions of AD diagnosis generally increased until early 20’s then tapered off or decreased afterwards. There were 417 (16.3%) individuals with at least one assessment with AD; among them, 114 individuals had AD at all available assessments. The average age at the onset of AD was 22.09 years (SD = 2.76). Of the sample, 2,043 (79.9%) participants reported engagement in binge drinking in the past year at least at one assessment. Means and standard deviations of positive and negative reinforcement mostly remained stable across age.
Table 1:
Descriptive Statistics of Alcohol Consumption, Alcohol Dependence, Positive and Negative Reinforcement by Age at Assessment
| Age | N | Alcohol Consumption |
AD Diagnosis |
Mean (SD) Positive Reinforcement |
Mean (SD) Negative Reinforcement |
|---|---|---|---|---|---|
| 18 | 702 | 40.0 | 4.5% | 28.6 (7.8) | 26.0 (8.2) |
| 19 | 710 | 55.0 | 7.7% | 28.9 (8.0) | 25.9 (8.7) |
| 20 | 798 | 54.5 | 9.0% | 29.0 (7.8) | 26.0 (8.4) |
| 21 | 865 | 67.0 | 8.2% | 29.5 (7.6) | 26.3 (8.2) |
| 22 | 763 | 71.5 | 10.1% | 29.6 (7.4) | 25.9 (8.0) |
| 23 | 663 | 70.4 | 12.0% | 29.5 (7.5) | 25.9 (8.3) |
| 24 | 604 | 70.9 | 14.4% | 29.9 (7.4) | 26.2 (8.2) |
| 25 | 480 | 73.0 | 12.8% | 29.8 (7.7) | 26.0 (8.2) |
| 26 | 402 | 76.4 | 15.0% | 30.5 (7.1) | 26.7 (8.1) |
| 27 | 335 | 73.1 | 14.8% | 30.3 (7.5) | 26.3 (8.4) |
| 28 | 244 | 79.2 | 20.6% | 30.2 (7.7) | 27.2 (8.3) |
| 29 | 191 | 74.6 | 9.7% | 30.2 (8.0) | 26.0 (8.7) |
| 30 | 127 | 63.7 | 11.3% | 29.7 (8.1) | 26.7 (8.8) |
Note. N represents the number of individuals who completed assessments at each age. Values for alcohol consumption represent the number of days participants consumed alcohol during the past 12 months.
Missing Data and Attrition
Individuals who met AD criteria at one or more assessments tended to have completed fewer numbers of assessments (M = 2.5, SD = 1.3) than individuals who did not meet AD criteria at any assessment (M = 3.0, SD = 1.3). Individuals’ frequency of alcohol consumption at their first assessment was not significantly correlated with the number of assessments completed (r = - .04, p = .08).
Hypotheses 1 and 2: Differential Associations between Positive/Negative Reinforcement and Alcohol Use Outcomes
Table 2 summarizes parameter estimates from the GEE model predicting frequency of alcohol consumption among participants without AD. Consistent with Hypothesis 1, positive reinforcement was more strongly associated with more frequent alcohol consumption than was negative reinforcement, as indicated by the larger regression coefficient for positive reinforcement. Tests of the parameters indicated that positive reinforcement, but not negative reinforcement, was significantly associated with frequency of alcohol consumption. Table 3 summarizes parameter estimates from the GEE model predicting AD by positive and negative reinforcement, which tests Hypothesis 2. Results indicated that both positive and negative reinforcement were significantly associated with AD. However, we only observed a slight difference in regression coefficients for positive and negative reinforcement, which did not provide clear support for Hypothesis 2.
Table 2:
Parameter Estimates from GEE Model of Alcohol Consumption predicted by Positive and Negative Reinforcement
| b | SE | 95% CI | Z | p | |
|---|---|---|---|---|---|
| Intercept | 2.294 | 0.096 | [2.11, 2.48] | 24.02 | <.0001 |
| Sex | 0.308 | 0.040 | [0.23, 0.39] | 7.77 | <.0001 |
| Race-AA | −0.247 | 0.050 | [−0.34, −0.15] | −4.98 | <.0001 |
| Race-other | −0.111 | 0.069 | [−0.25, 0.02] | −1.62 | 0.1056 |
| Age linear | 0.090 | 0.009 | [0.07, 0.11] | 10.64 | <.0001 |
| Age quad. | −0.010 | 0.001 | [−0.01, −0.01] | −6.89 | <.0001 |
| Positive | 0.052 | 0.004 | [0.05, 0.06] | 14.39 | <.0001 |
| Negative | 0.002 | 0.003 | [0.00, 0.01] | 0.68 | 0.4988 |
Note. Only participants without AD were included in this analysis. Sex was coded 1 = male, 0 = female. AA = African American; other = other race. European American was the reference group for race. Quad. = quadratic. Positive = positive reinforcement. Negative = negative reinforcement. Z = b/SE. CI = confidence intervals.
Table 3:
Parameter Estimates from GEE Model of Alcohol Dependence Predicted by Positive and Negative Reinforcement
| b (OR) | SE | 95% CI | 95% CI in OR | Z | p | |
|---|---|---|---|---|---|---|
| Intercept | −5.23 (0.01) | 0.302 | [−5.82, −4.64] | [0.00, 0.01] | −17.30 | <.0001 |
| Sex | 0.35 (1.41) | 0.113 | [0.12, 0.57] | [1.13, 1.77] | 3.06 | 0.0022 |
| Race-AA | −0.32 (0.73) | 0.144 | [−0.60, −0.03] | [0.55, 0.97] | −2.19 | 0.0283 |
| Race-other | 0.07 (1.07) | 0.180 | [−0.28, 0.42] | [0.75, 1.53] | 0.38 | 0.7027 |
| Age linear | 0.18 (1.19) | 0.024 | [0.13, 0.22] | [1.14, 1.25] | 7.32 | <.0001 |
| Age quad. | −0.02 (0.98) | 0.004 | [−0.02, −0.01] | [0.98, 0.99] | −4.17 | <.0001 |
| Positive | 0.04 (1.04) | 0.011 | [0.02, 0.06] | [1.02, 1.06] | 3.62 | 0.0003 |
| Negative | 0.06 (1.06) | 0.009 | [0.04, 0.08] | [1.04, 1.08] | 6.41 | <.0001 |
Note. This analysis was conducted with the whole sample. Sex was coded 1 = male, 0 = female. AA = African American; other = other race. European American was the reference group for race. Quad. = quadratic. Positive = positive reinforcement. Negative = negative reinforcement. Z = b/SE. OR = odds ratios. CI = confidence intervals.
Hypothesis 3: Changes in Positive and Negative Reinforcement Associated with Alcohol Consumption as a Function of AD
Table 4 summarizes parameter estimates from the multilevel growth model where we disentangled between-person and within-person variations and predicted frequency of alcohol consumption from positive/negative reinforcement, AD, and the two 2-way interactions between them. Random slopes were retained for linear and quadratic effects of age, AD, and the interaction effect between negative reinforcement and AD because preliminary analysis indicated that they were statistically significant. Results indicated that, at the between-person level, positive reinforcement was associated with more frequent alcohol consumption, but negative reinforcement was not associated. At the within-person level, positive reinforcement was also associated with more frequent alcohol consumption. Contrary to our hypothesis, this association did not vary as a function of AD, as indicated by the non-significant interaction effect between positive reinforcement and AD. Consistent with our hypothesis, there was a significant interaction effect between negative reinforcement and AD. Specifically, the parameter estimate of the main effect of negative reinforcement indicated a positive association with alcohol consumption when AD diagnosis was absent. The positive parameter for the interaction between negative reinforcement and AD indicated that the within-person association between negative reinforcement and alcohol consumption became stronger with the presence of alcohol dependence. Figure 1 illustrates the within-person associations between positive and negative reinforcement and alcohol consumption as a function of AD. As shown in Figure 1, the association between positive reinforcement and alcohol consumption did not significantly vary as a function of AD diagnosis. In contrast, the association between negative reinforcement and alcohol consumption increased as a function of individuals’ presence of AD.
Table 4:
Parameter Estimates from Multilevel Growth Model Predicting Alcohol Consumption From Interactions Between Positive and Negative Reinforcement and Alcohol Dependence
| b | SE | CI | t | p | |
|---|---|---|---|---|---|
| Intercept | −.444 | .052 | [−.530, −.359] | −8.553 | < .001 |
| Sex | .168 | .022 | [.131,.204] | 7.560 | < .001 |
| Race-AA | −.090 | .024 | [−.131, −.050] | −3.698 | < .001 |
| Race-other | −.069 | .040 | [−.135, −.003] | −1.709 | .087 |
| Positive-btw | .037 | .003 | [.032,.042] | 12.255 | < .001 |
| Negative-btw | −.003 | .003 | [−.008,.001] | −1.142 | .254 |
| Age linear | .049 | .004 | [.042,.057] | 11.314 | < .001 |
| Age quad. | −.005 | .001 | [−.007, −.004] | −6.644 | < .001 |
| Positive-within | .012 | .002 | [.009,.016] | 5.511 | < .001 |
| Negative-within | .004 | .002 | [.001, .007] | 1.952 | .051 |
| AD | .371 | .044 | [.298,.443] | 8.412 | < .001 |
| Positive-within *AD | .001 | .012 | [−.019,.021] | .091 | .928 |
| Negative-within*AD | .038 | .013 | [.017,.060] | 2.932 | .003 |
Note. This analysis was conducted with the whole sample. Sex was coded 1 = male, 0 = female. AA = African American; other = other race. European American was the reference group for race. Quad. = quadratic. Positive/Negative-btw = person-level means of positive/negative reinforcement. Positive/Negative-within = person-mean centered variables for positive and negative reinforcement. AD = alcohol dependence. CI = confidence intervals.
Figure 1: Within-person Associations Between Positive and Negative Reinforcement and Alcohol Consumption as a Function of Alcohol Dependence.
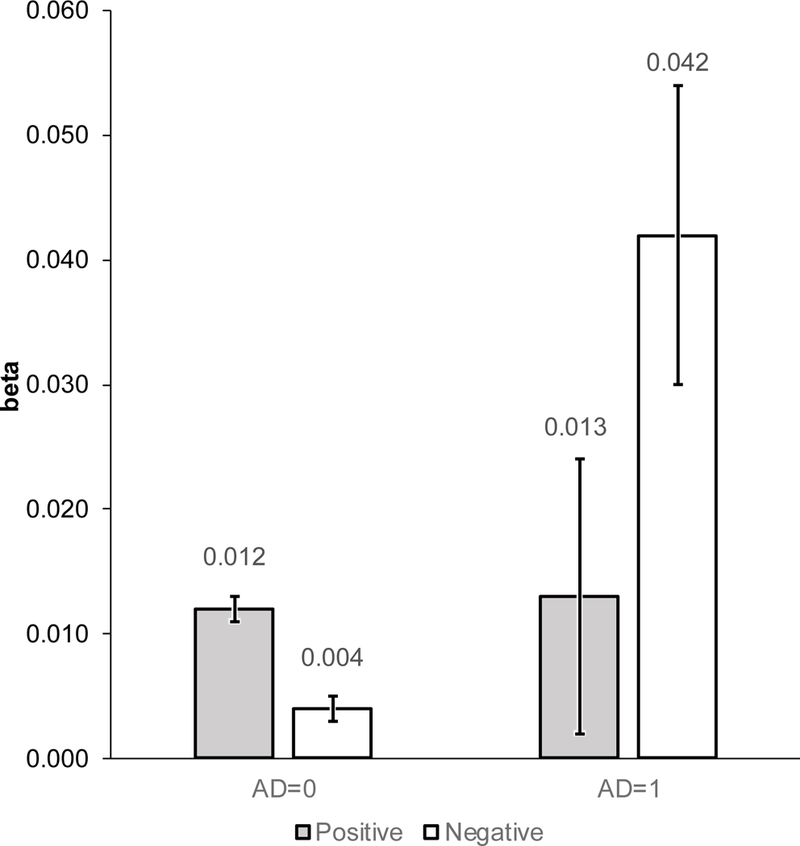
Note. Values on the Y-axis represent parameter estimates for the effects of positive and negative reinforcement on alcohol consumption as a function of alcohol dependence. The error bars show the 95% confidence intervals for the parameter estimates.
Sex and Racial Differences in Patterns of Associations
We also conducted analyses to examine whether there are differences across sex and racial groups in the associations between positive and negative reinforcement and alcohol use outcomes. Results supporting Hypothesis 1 were observed across sex and race. That is, positive reinforcement was more strongly associated with alcohol consumption than was negative reinforcement among individuals without AD; this pattern of associations was observed for males and females, and for EAs and AAs (see Supplemental Table 1). For Hypothesis 2, no clear evidence was observed across sex and race/ethnicity. For males, females, and EAs, consistent with the results observed in the whole sample, both positive and negative reinforcement were associated with AD, with the association only being slightly stronger for negative reinforcement among males and EAs. However, for AAs, negative reinforcement, but not positive reinforcement, was significantly associated with AD, providing stronger support for Hypothesis 2 compared to results for EAs (see Supplemental Table 2). Results supporting Hypothesis 3 were observed across sex and for EAs. Consistent with the results observed in the whole sample, the association between positive reinforcement and alcohol consumption did not change, whereas the association between negative reinforcement and alcohol consumption increased, with the presence of AD. However, for AAs, results indicated no significant interaction between both positive and negative reinforcement and AD in relation to alcohol consumption (see Supplemental Table 3).
Discussion
This study used a longitudinal design and applied the multistage model of drug addiction (Koob & Volkow, 2010) to alcohol use to test for potential changes in positive and negative reinforcement associated with alcohol consumption as a function of AD. Our results indicated that positive reinforcement was associated with alcohol consumption regardless of the status of AD. In contrast, negative reinforcement was more salient in relation to alcohol consumption with the presence of AD.
Positive and Negative Reinforcement Associated with Alcohol Consumption as a Function of Alcohol Dependence
Our Hypothesis 1, which tested the relative importance of positive and negative reinforcement associated with alcohol consumption, was supported. Our results indicated that positive reinforcement, but not negative reinforcement, was associated with frequency of alcohol consumption among individuals without AD. Results indicated that both positive and negative reinforcement were uniquely associated with higher risk of having an AD diagnosis, with the association being slightly stronger for negative reinforcement than for positive reinforcement. Thus, our findings did not provide clear support for Hypothesis 2 that negative reinforcement would be more strongly associated with AD than positive reinforcement. This finding is consistent with the impulsivity-compulsivity cycle of motivation of drug use proposed in the multistage model of drug addiction (Koob & Volkow, 2010). That is, while positive reinforcement plays a more important role in influencing substance involvement during earlier stages of addiction, both positive and negative reinforcement are important in influencing drug use in later stages of addiction. Our findings are also in line with prior studies that showed associations between positive reinforcement and moderate drinking and associations between negative reinforcement and alcohol-related problems such as AD (Kuntsche et al., 2005). Thus, our findings build upon prior research to provide further support for the notion that positive and negative reinforcement have differential importance in influencing alcohol use outcomes that may represent different stages of alcohol addiction.
Importantly, our results indicated that with the presence of AD, the association between positive reinforcement and alcohol consumption remained similar, whereas the association between negative reinforcement and alcohol consumption increased. That is, positive reinforcement is important in the association with alcohol consumption regardless of the status of AD. In addition, negative reinforcement becomes increasingly important in the presence of AD. This result provided initial support for the proposition of the multistage model of addiction regarding the increasing salience of negative reinforcement as individuals progress from earlier to later stages of addiction. We note that mean levels of negative reinforcement remained stable among individuals who did not develop AD in our sample, indicating that the change in negative reinforcement associated with alcohol consumption as a function of AD was not confounded by a general developmental change in negative reinforcement as a function of age. This finding extends the extant literature on the potential differential importance of positive and negative reinforcement across alcohol use outcomes by providing empirical evidence of within-individual change in the relationship between negative reinforcement and alcohol consumption as a function of AD status. Although our results did not support the hypothesis that the influence of positive reinforcement on alcohol consumption would decrease with the presence of AD, they are consistent with prior findings that alcohol stimulation and reward sensitivity continue to influence drinking as individuals progress in developing alcohol use disorder (King et al., 2014; King et al., 2016). These results are interesting, particularly in view of the tremendous challenges for AD intervention and treatment, which may be because once individuals become alcohol dependent, both positive and negative reinforcing factors are operating. Our findings imply that both positive and negative reinforcement need to be targeted for individuals with AD.
Taken together, our results demonstrated differential importance of positive and negative reinforcement in influencing alcohol consumption and AD, as well as increasing salience of negative reinforcement associated with alcohol consumption in the presence of AD. Understanding how reasons for drinking differ across the addiction cycle could provide useful information for tailoring prevention and intervention efforts. For example, programs that target reducing alcohol consumption among adolescents who engage in moderate or heavy drinking but have not developed AD may be more effective by focusing on adolescents’ anticipated positive reinforcement of alcohol intake, for example, by providing alternative ways to gain similar positive reinforcement instead of alcohol consumption (Goldstein, Wall, Wekerie, & Krank, 2013). On the other hand, programs that target reducing alcohol consumption among alcohol-dependent individuals may need to target positive and negative reinforcement simultaneously in order to be effective, for example, by providing training and support on coping with emotional stress and physical tension that may trigger self-medication (Berking et al., 2011) in addition to providing alternative outlets for positive reinforcement (Goldstein et al., 2013). Understanding individuals’ positive and negative reinforcement profiles can also provide important information for personalized medicine. There is preliminary evidence for effectiveness of tailoring pharmacotherapies to AD patients based on their positive and negative reinforcement tendencies (Mann et al., 2018; Roos, Mann, & Witkiewitz, 2017). For example, acamprosate has been found to be particularly effective for treating patients whose alcohol use disorder is maintained by drinking to relieve negative affect (Roos et al., 2017).
Sex and Racial/Ethnic Differences
We explored potential sex and racial differences in the pattern of associations between positive/negative reinforcement and alcohol use outcomes. Overall, we observed similar patterns of associations between positive/negative reinforcement and alcohol consumption and AD across males and females, and across EA and AA subsamples that are consistent with findings from analyses conducted with the full sample as reported above. One exception was that, the hypothesis that the association between negative reinforcement and alcohol consumption became stronger in the presence of AD was supported in the EA subsample but not in the AA subsample. For AAs, results indicated that the association between negative reinforcement and alcohol consumption did not change with the presence of AD, although the direction of the interaction effect between negative reinforcement and AD observed was consistent with that observed for EAs and the full sample. This finding is consistent with previous findings that negative emotion is associated with alcohol use disorder for Whites but not for Blacks (Akins et al., 2010), further suggesting that pathways of risk to alcohol problems may differ across racial groups.
Strengths and Limitations
Several strengths of this study are notable. Utilizing a longitudinal data set that covered the developmental period from late adolescence to young adulthood, we provided empirical evidence for increasing salience of negative reinforcement associated with alcohol consumption as a function of the presence of AD. The age period included in our study is characterized by heightened risk of alcohol problems (SAMHSA, 2016) due to environmental changes that facilitate risky alcohol use (Bachman, Wadsworth, O’Malley, Johnston, & Schulenberg, 2013; Borsari, Murphy & Barnett 2007; White, Kraus, & Swartzwelder, 2006; White et al. 2006). Such characteristics of the data allowed tests of hypotheses regarding differential importance of positive and negative reinforcement in relation to alcohol consumption and AD. More importantly, repeated assessments of alcohol use outcomes and positive and negative reinforcement within individuals allowed an explicit test of the hypothesis regarding within-individual changes in the importance of positive and negative reinforcement in influencing drinking as a function of AD. To our knowledge, this is the first study to examine within- individual changes in the role of positive and negative reinforcement in relation to alcohol consumption in the absence versus presence of AD. In addition, COGA is a high-risk sample where participants were recruited from families with a history of AD. This resulted in a higher prevalence of alcohol consumption and AD in the sample compared to the general population, as seen in Table 1, allowing us to more reliably estimate parameters to test our hypotheses about the associations between positive and negative reinforcement and alcohol use outcomes.
Our results need to be interpreted in light of several limitations. First, we conceptualized positive and negative reinforcement broadly, and we acknowledge that our measure of positive and negative reinforcement using the Alcohol Expectancy Questionnaire (AEQ) is only one of many ways to assess these broad and complicated constructs. We used AEQ because it was the only measure related to positive and negative reinforcement available in our dataset that were repeatedly and concurrently assessed along with alcohol use outcomes, which was necessary to address our research questions. We acknowledge that although the AEQ subscales were designed to measure positive and negative reinforcement expected from drinking (Brown et al., 1980; Brown et al., 1987), they might not exactly represent the corresponding motives that made a person drink. Cooper (1994) argued that expecting certain effects of alcohol is a necessary, but not sufficient, condition for drinking to achieve the expected effects. Future research is warranted to replicate the current findings using other measures of positive and negative reinforcement such as the Drinking Motives Questionnaire (Cooper, 1994). Second, our measure of negative reinforcement was broad, including aspects of negative reinforcement related to coping with emotional challenges (e.g., to feel less anxious) as well as aspects of negative reinforcement related to reducing undesirable physical states associated with alcohol withdrawal (e.g., to sleep better). Future research is needed to examine the potentially different influences of these different aspects of negative reinforcement and examine whether there would be a change from negative reinforcement associated with coping to that associated with alcohol withdrawal as a function of AD.
Third, our measure of alcohol consumption focused only on frequency of drinking and did not represent the total amounts of alcohol consumed, which would be helpful to understand individuals’ transition to AD. We recognize that there are alternative ways to index alcohol consumption other than frequency of alcohol consumption, and it is possible that results could vary when different alcohol outcomes are studied. As observed from previous studies, alcohol use quantity and frequency may be differentially influenced by alcohol expectancy (Chen, Grube, & Madden, 1994; Heath, Meyer, Jardin, & Martin, 1991; Mooney, Fromme, Kivlahan, & Marlatt, 1987). While we focused on alcohol use frequency in this study, testing our hypotheses using different measures of alcohol consumption would corroborate the change in positive and negative reinforcement identified in the current study.
Furthermore, our analysis was limited in that it did not differentiate participants who had different patterns of shifts in AD status. For example, participants who did not meet AD criteria at one assessment might never had AD or be in remission; participants who met AD criteria at one assessment could be having AD for the first time or be in relapse. Individuals with different patterns of shifts in AD status were likely to be at different stages in the addiction process and the effect of positive and negative reinforcement on alcohol consumption may differ between them. In addition, although our results provide support for the multistage model of addiction, we note that this theoretical model does not take into account potential heterogeneity in pathways of risk to AD. Future research is warranted to examine potential differences in the effects of positive and negative reinforcement associated with alcohol consumption across the addiction process among individuals with heterogeneous pathways of developing AD. Lastly, due to the characteristics of our sample, generalizability of findings from this study may be limited. Our sample is a relatively high-risk sample, with most participants embedded within families with histories of alcoholism. Thus, generalizing results from this study in more general population would require replications in independent epidemiological samples.
Conclusion and Future Directions
Informed by the multistage model of addiction (Koob & Volkow, 2010), the present study examined the role of positive and negative reinforcement in alcohol consumption and AD. Our results based on longitudinal data suggest that positive reinforcement is associated with alcohol consumption regardless of the status of AD, whereas negative reinforcement becomes increasingly important in the presence of AD. These findings demonstrate the utility of positive and negative reinforcement in understanding individuals’ risk of developing AD and suggest that positive and negative reinforcement may be important targets for effective intervention and prevention efforts. In future studies, models for more complicated paths from positive and negative reinforcement to AD can be built upon the results of our study. For example, the changes in positive and negative reinforcement in associating with alcohol use may be mediated or moderated by other factors, such as major depression (Armeli et al., 2014) or traumatic experiences (Berenz et al. 2015; Jester et al., 2015), and our model can be expanded to incorporate those mediating and moderating factors.
Supplementary Material
Acknowledgements:
The Collaborative Study on the Genetics of Alcoholism (COGA), Principal Investigators B. Porjesz, V. Hesselbrock, H. Edenberg, L. Bierut, includes eleven different centers: University of Connecticut (V. Hesselbrock); Indiana University (H.J. Edenberg, J. Nurnberger Jr., T. Foroud); University of Iowa (S. Kuperman, J. Kramer); SUNY Downstate (B. Porjesz); Washington University in St. Louis (L. Bierut, J. Rice, K. Bucholz, A. Agrawal); University of California at San Diego (M. Schuckit); Rutgers University (J. Tischfield, A. Brooks); Department of Biomedical and Health Informatics, The Children’s Hospital of Philadelphia; Department of Genetics, Perelman School of Medicine, University of Pennsylvania, Philadelphia PA (L. Almasy), Virginia Commonwealth University (D. Dick), Icahn School of Medicine at Mount Sinai (A. Goate), and Howard University (R. Taylor). Other COGA collaborators include: L. Bauer (University of Connecticut); J. McClintick, L. Wetherill, X. Xuei, Y. Liu, D. Lai, S. O’Connor, M. Plawecki, S. Lourens (Indiana University); G. Chan (University of Iowa; University of Connecticut); J. Meyers, D. Chorlian, C. Kamarajan, A. Pandey, J. Zhang (SUNY Downstate); J.-C. Wang, M. Kapoor, S. Bertelsen (Icahn School of Medicine at Mount Sinai); A. Anokhin, V. McCutcheon, S. Saccone (Washington University); J. Salvatore, F. Aliev, B. Cho (Virginia Commonwealth University); and Mark Kos University of Texas Rio Grande Valley). A. Parsian and M. Reilly are the NIAAA Staff Collaborators. We continue to be inspired by our memories of Henri Begleiter and Theodore Reich, founding PI and Co-PI of COGA, and also owe a debt of gratitude to other past organizers of COGA, including Ting-Kai Li, P. Michael Conneally, Raymond Crowe, and Wendy Reich, for their critical contributions. This national collaborative study is supported by National Institute of Health Grant U10AA008401 from the National Institute on Alcohol Abuse and Alcoholism (NIAAA) and the National Institute on Drug Abuse (NIDA). This research was also support in part by National Institute of Health grant K02AA018755 (PI: Dick).
Appendix
Items Included in the Measures of Positive and Negative Reinforcement.
| Positive Reinforcement |
|---|
| 1. Some alcohol has a pleasant, cleansing, tingly taste. |
| 2. Drinking adds a certain warmth to social occasions. |
| 3. Time passes quickly when I am drinking. |
| 4. Drinking makes me feel good. |
| 5. Having a few drinks is a nice way to celebrate special occasions. |
| 6. When I feel “high” from drinking, everything seems to feel better. |
| 7. Drinking is pleasurable because it is enjoyable to join in with people who are enjoying themselves. |
| 8. I like the taste of some alcoholic beverages. |
| 9. Sometimes when I drink alone or with one other person it is easy to feel cozy and romantic. |
|
Negative Reinforcement |
| 1. Alcohol helps me sleep better. |
| 2. Alcohol decreases muscular tension. |
| 3. After a few drinks I am usually in a better mood. |
| 4. If I am tense or anxious, having a few drinks makes me feel better. |
| 5. Alcohol enables me to fall asleep more easily. |
| 6. Alcohol can act as an anesthetic; that is, it can deaden pain. |
| 7. I feel like more of a happy-go-lucky person when I drink. |
| 8. Drinking makes get-togethers more fun. |
| 9. If I am cold, having a few drinks will give me a sense of warmth. |
Note. The measure of negative reinforcement contains some items (e.g., “drinking makes get- togethers more fun”) that may not theoretically map onto the negative reinforcement construct. We note that analyses conducted with these items excluded yielded similar results to those presented in the manuscript.
Footnotes
The authors have no conflicts of interest to declare about this manuscript. None of the original material contained in the manuscript has been submitted for consideration nor will any of it be published elsewhere except in abstract form in connection with scientific meetings.
Contributor Information
Seung Bin Cho, Pusan National University.
Jinni Su, Virginia Commonwealth University.
Sally I-Chun Kuo, Virginia Commonwealth University.
Kathleen K. Bucholz, Washington University at St. Louis
Grace Chan, University of Connecticut.
Howard J. Edenberg, Indiana University
Vivia V. McCutcheon, Washington University at St. Louis
Marc A. Schuckit, University of California at San Diego
John R. Kramer, University of Iowa
Danielle M. Dick, Virginia Commonwealth University
References
- American Psychiatric Association. (1987). DSM-III-R casebook: A learning companion to the diagnostic and statistical manual of mental disorders, rev, Washington, DC: American Psychiatric Press. [Google Scholar]
- American Psychiatric Association (2000). Diagnostic and statistical manual of mental disorders (4th ed, text rev.). Washington, DC: Author. [Google Scholar]
- Anderson KG, Briggs KE, & White HR (2013). Motives to drink or not to drink: Longitudinal relations among personality, motives, and alcohol use across adolescence and early adulthood. Alcoholism: Clinical and Experimental Research, 37, 860–867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anthenien AM, Lembo J, & Neighbors C (2017). Drinking motives and alcohol outcome expectancies as mediators of the association between negative urgency and alcohol consumption. Addictive Behaviors, 66, 101–107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Armeli S, Dranoff E, Tennen H, Austad CS, Fallahi CR, Raskin S, Wood R, & Pearlson G (2014). A longitudinal study of the effects of coping motives, negative affect and drinking level on drinking problems among college students. Anxiety, Stress, & Coping, 27, 527–541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bachman JG, Wadsworth KN, O’Malley PM, Johnston LD, & Schulenberg JE (2013). Smoking, drinking, and drug use in young adulthood: The impacts of new freedoms and new responsibilities Psychology Press [Google Scholar]
- Begleiter H, Reich T, Hesselbrock V, Porjesz B, Li T, Schuckit M, Edenberg HJ, & Rice J (1995). The collaborative study on the genetics of alcoholism. Alcohol Health and Research World, 19, 228–228. [PMC free article] [PubMed] [Google Scholar]
- Berenz EC, Cho SB, Overstreet C, Kendler K, Amstadter AB, & Dick DM (2016). Longitudinal investigation of interpersonal trauma exposure and alcohol use trajectories. Addictive Behaviors, 53, 67–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berking M, Margraf M, Ebert D, Wupperman P, Hofmann SG, & Junghanns K (2011). Deficits in emotion-regulation skills predict alcohol use during and after cognitive–behavioral therapy for alcohol dependence. Journal of Consulting and Clinical Psychology, 79, 307–318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borsari B, Murphy JG, & Barnett NP (2007). Predictors of alcohol use during the first year of college: Implications for prevention. Addictive Behaviors, 32, 2062–2086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown SA, Christiansen BA, & Goldman MS (1987). The alcohol expectancy questionnaire: An instrument for the assessment of adolescent and adult alcohol expectancies. Journal of Studies on Alcohol, 48, 483–491. [DOI] [PubMed] [Google Scholar]
- Brown SA, Goldman MS, Inn A, & Anderson LR (1980). Expectations of reinforcement from alcohol: Their domain and relation to drinking patterns. Journal of Consulting and Clinical Psychology, 48, 419–426. [DOI] [PubMed] [Google Scholar]
- Bucholz KK, Cadoret R, Cloninger CR, Dinwiddie SH, Hesselbrock VM, Nurnberger JI, Reigh T, Schmidt I, & Schuckit MA (1994). A new, semi-structured psychiatric interview for use in genetic linkage studies: A report on the reliability of the SSAGA. Journal of Studies on Alcohol and Drugs, 55, 149–158. [DOI] [PubMed] [Google Scholar]
- Bucholz KK, McCutcheon VV, Agrawal A, Dick DM, Hesselbrock VM, Kramer JR, Kuperman S, Nurnberger JI, Salvatore JE, & Schuckit MA (2017). Comparison of parent, peer, psychiatric, and cannabis use influences across stages of offspring alcohol involvement: Evidence from the COGA prospective study. Alcoholism: Clinical and Experimental Research, 41, 359–368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bujarski S, Hutchison KE, Prause N, & Ray LA (2017). Functional significance of subjective response to alcohol across levels of alcohol exposure. Addiction biology, 22, 235–245. [DOI] [PubMed] [Google Scholar]
- Bujarski S, & Ray LA (2014). Subjective response to alcohol and associated craving in heavy drinkers vs. alcohol dependents: An examination of Koob’s allostatic model in humans. Drug and Alcohol Dependence, 140, 161–167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen M, Grube JW, & Madden PA (1994). Alcohol expectancies and adolescent drinking: Differential prediction of frequency, quantity, and intoxication. Addictive Behaviors, 19, 521–529. [DOI] [PubMed] [Google Scholar]
- Cooper ML (1994). Motivations for alcohol use among adolescents: Development and validation of a four-factor model. Psychological Assessment, 6, 117–128. [Google Scholar]
- Cooper ML, Frone MR, Russell M, & Mudar P (1995). Drinking to regulate positive and negative emotions: A motivational model of alcohol use. Journal of Personality and Social Psychology, 69, 990–1005. [DOI] [PubMed] [Google Scholar]
- Dick DM, Cho SB, Latendresse SJ, Aliev F, Nurnberger JI, Edenberg HJ, Howard J, Schuckit MA, Hesselbrock VM, Porjesz B, & Bucholz K. (2014). Genetic influences on alcohol use across stages of development: GABRA2 and longitudinal trajectories of drunkenness from adolescence to young adulthood. Addiction Biology, 19, 1055–1064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feighner JP, Robins E, Guze SB, Woodruff RA, Winokur G, & Munoz R (1972). Diagnostic criteria for use in psychiatric research. Archives of General Psychiatry, 26, 57–63. [DOI] [PubMed] [Google Scholar]
- Foroud T, Edenberg HJ, Goate A, Rice J, Flury L, Koller DL, … Bucholz KK. (2000). Alcoholism susceptibility loci: Confirmation studies in a replicate sample and further mapping. Alcoholism: Clinical and Experimental Research, 24, 933–945. [PubMed] [Google Scholar]
- Goldstein AL, Wall A, Wekerle C, & Krank M (2013). The impact of perceived reinforcement from alcohol and involvement in leisure activities on adolescent alcohol use. Journal of Child & Adolescent Substance Abuse, 22, 340–363. [Google Scholar]
- Grant BF, Goldstein RB, Saha TD, Chou SP, Jung J, Zhang H, Pickering RP, Ruan WJ, Smith SM, & Huang B (2015). Epidemiology of DSM-5 alcohol use disorder: Results from the national epidemiologic survey on alcohol and related conditions III. JAMA Psychiatry, 7), 757–766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grotmol KS, Vaglum P, Ekeberg O, Gude T, Aasland OG, & Tyssen R (2010). Alcohol expectancy and hazardous drinking: A 6-year longitudinal and nationwide study of medical doctors. European Addiction Research, 16, 17–22. [DOI] [PubMed] [Google Scholar]
- Heath AC, Meyer J, Jardine R, & Martin N (1991). The inheritance of alcohol consumption patterns in a general population twin sample: II. determinants of consumption frequency and quantity consumed. Journal of Studies on Alcohol, 52, 425–433. [DOI] [PubMed] [Google Scholar]
- Jester JM, Steinberg DB, Heitzeg MM, & Zucker RA (2015). Coping expectancies, not enhancement expectancies, mediate trauma experience effects on problem alcohol use: A prospective study from early childhood to adolescence. Journal of Studies on Alcohol and Drugs, 76, 781–789. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koob G F (2013). Theoretical frameworks and mechanistic aspects of alcohol addiction: alcohol addiction: alcohol addiction as a reward deficit disorder In: Sommer WH and Spanagel R (eds) Behavioral neurobiology of alcohol addiction (series title: Current topics in nehavioral neuroscience, vol 13). Berlin: Springer-Verlag, pp. 3–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koob GF, & Volkow ND (2010). Neurocircuitry of addiction. Neuropsychopharmacology, 35, 217–238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kuntsche E, Knibbe R, Gmel G, & Engels R (2005). Why do young people drink? A review of drinking motives. Clinical Psychology Review, 25, 841–861. [DOI] [PubMed] [Google Scholar]
- Kwako LE, & Koob GF (2017). Neuroclinical Framework for the Role of Stress in Addiction. Chronic Stress, 1, 1–14. doi: 10.1177/2470547017698140 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li JJ, Cho SB, Salvatore JE, Edenberg HJ, Agrawal A, Chorlian DB, … Dick DM. (2017). The impact of peer substance use and polygenic risk on trajectories of heavy episodic drinking across adolescence and emerging adulthood. Alcoholism: Clinical and Experimental Research, 41, 65–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mackinnon SP, Kehayes IL, Clark R, Sherry SB, & Stewart SH (2014). Testing the four-factor model of personality vulnerability to alcohol misuse: A three-wave, one-year longitudinal study. Psychology of Addictive Behaviors, 28, 1000–1012. [DOI] [PubMed] [Google Scholar]
- Mann K, Roos CR, Hoffmann S, Nakovics H, Lemenager T, Heinz A, & Witkiewitz K (2018). Precision medicine in alcohol dependence: A controlled trial testing pharmacotherapy response among reward and relief drinking phenotypes. Neuropsychopharmacology, 43, 891–899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mooney DK, Fromme K, Kivlahan DR, & Marlatt GA (1987). Correlates of alcohol consumption: Sex, age, and expectancies relate differentially to quantity and frequency. Addictive Behaviors, 12, 235–240. [DOI] [PubMed] [Google Scholar]
- Muthén LK and Muthén BO (1998–2012). Mplus User’s Guide. Seventh Edition Los Angeles, CA: Muthen & Muthen [Google Scholar]
- Osberg TM, Insana M, Eggert M, & Billingsley K (2011). Incremental validity of college alcohol beliefs in the prediction of freshman drinking and its consequences: A prospective study. Addictive Behaviors, 36, 333–340. [DOI] [PubMed] [Google Scholar]
- Reich T, Edenberg HJ, Goate A, Williams JT, Rice JP, Van Eerdewegh P, Foroud T, Schuckit MA, &Bucholz K. (1998). Genome-wide search for genes affecting the risk for alcohol dependence. American Journal of Medical Genetics, 81, 207–215. [PubMed] [Google Scholar]
- Roos CR, Mann K, & Witkiewitz K (2017). Reward and relief dimensions of temptation to drink: Construct validity and role in predicting differential benefit from acamprosate and naltrexone. Addiction biology, 22, 1528–1539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- SAMHSA (2016). Center for Behavioral Health Statistics and Quality 2015 National Survey on Drug Use and Health: Detailed Tables. Rockville, MD: Substance Abuse and Mental Health Services Administration. [Google Scholar]
- Watkins LE, Franz MR, DiLillo D, Gratz KL, & Messman-Moore TL (2015). Does drinking to cope explain links between emotion-driven impulse control difficulties and hazardous drinking? A longitudinal test. Psychology of Addictive Behaviors, 29, 875–884. [DOI] [PMC free article] [PubMed] [Google Scholar]
- White AM, Kraus CL, & Swartzwelder HS (2006). Many college freshmen drink at levels far beyond the binge threshold. Alcoholism: Clinical and Experimental Research, 30, 1006–1010. [DOI] [PubMed] [Google Scholar]
- White HR, McMorris BJ, Catalano RF, Fleming CB, Haggerty KP, & Abbott RD (2006) . Increases in alcohol and marijuana use during the transition out of high school into emerging adulthood: The effects of leaving home, going to college, and high school protective factors. Journal of Studies on Alcohol, 67, 810–822. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.