

Ultrasound-guided (USG) brachiocephalic vein (BCV) cannulation has regained interest because of the superficial location and lack of bone overlying the vein. This is useful as it facilitates visualisation of the entire path of the needle during cannulation. The supraclavicular approach to BCV is unique in that the catheter dressing usually tightly adheres and inconspicuously drapes over the shoulder in a manner that it does not transverse the pectoralis muscle; therefore, it is less likely to limit upper-extremity movement compared with the infraclavicular subclavian approach.[1] This technique is especially useful in patients where the internal jugular vein (IJV) vessel lumen is small (eg., volume deficient patient), patients with history of multiple cannulations, and in whom subclavian puncture is contraindicated.[1,2] Though there is resurgence of this technique, there is debate about exact target site of USG BCV cannulation.
Here, we describe three different sites of USG BCV cannulation through supraclavicular fossa: Method 1 – cannulation through lateral wall of IJV near venous confluence; Method 2 – cannulation at venous confluence of three vessels, IJV, subclavian vein (SCV), and BCV also known as the “Pirogoff” confluence;[2] and Method 3 – cannulation of BCV.
We place the linear USG probe (M-Turbo, Fujifilm Sonosite, Inc., Bothell, WA, USA) in the left supraclavicular fossa parallel to medial end of clavicle. The probe is tilted caudally to obtain in-plane view of BCV and venous confluence of three vessels. Doppler power is used to differentiate subclavian and other artery from vein. The needle is inserted in-plane to probe from lateral to medial direction in all three methods. But methods 2 and 3 require insertion of needle oblique to probe for better alignment and needle visualisation to achieve target.
The tip of needle is kept above the imaginary line passing horizontally through centre of Pirogoff's angle between IJV and SCV to prevent inadvertent puncture of pleura as shown in Figure 1. There is danger zone situated below imaginary line, because there are chances of pleural puncture. Three different sites of needle puncture are shown in Figure 1.
Figure 1.
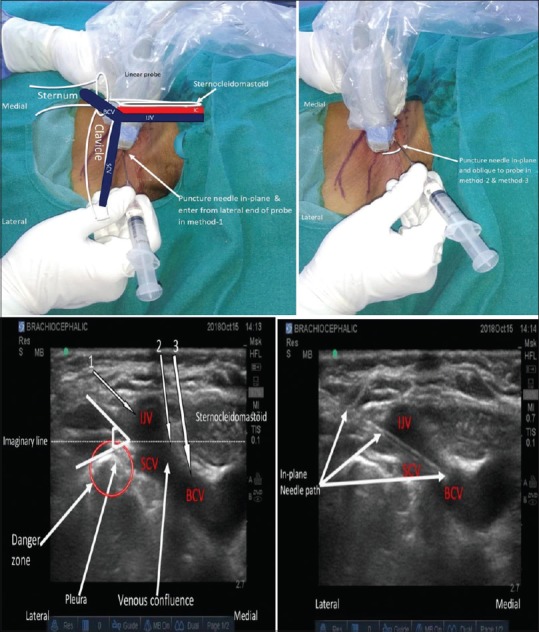
Surface anatomy and sono-anatomy of BCV
Breschan et al.[3] stated that the USG-guided cannulation of right BCV is technically more difficult due to the shorter course, sharp angle and caudal turn of the vein. This may be of greater importance in smaller patients, especially as the left BCV is apparently larger than the right in preterm babies.[4] The incidence of contamination during BCV cannulation was lowered as compared to internal jugular, subclavian or femoral central lines.[5]
In our experience of routinely cannulating USG-guided BCV in paediatric patients and adult patients scheduled for emergency and elective surgeries, we have realised that method 1 is technically easier, while methods 2 and 3 may have lesser chances of pleural puncture. In all cases however, the needle entry point should be tried to be kept above the horizontal imaginary line described earlier. We have done around 50 cannulations till date and have not encountered any adverse events (pneumo- or haemothorax) in any of these. Further studies are required to compare all the three techniques amongst themselves and with other techniques.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Thompson ME. Ultrasound-guided cannulation of the brachiocephalic vein in infants and children is useful and stable. Turk J Anaesthesiol Reanim. 2017;45:153–7. doi: 10.5152/TJAR.2017.67535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Saini V, Sardana DK, Samra T, Sethi S. Trouble shooting a small sized IJV. Indian J Crit Care Med. 2017;21:335–6. doi: 10.4103/ijccm.IJCCM_398_16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Breschan C, Platzer M, Jost R, Stettner H, Beyer AS, Feigl G, et al. Consecutive, prospective case series of a new method for ultrasound-guided supraclavicular approach to the brachiocephalic vein in children. Br J Anaesth. 2011;106:732–7. doi: 10.1093/bja/aer031. [DOI] [PubMed] [Google Scholar]
- 4.Eifinger F, Briskn B, Roth B, Koebke J. Topographical anatomy of the central venous system in extremely low-birth weight neonates less than 1000 grams and the effect of central venous catheter placement. Clin Anat. 2011;24:711–6. doi: 10.1002/ca.21204. [DOI] [PubMed] [Google Scholar]
- 5.Jordan JR, Moore EE, Haenel J, Burlew CC. Ultrasound-guided supraclavicular access to the innominate vein for central venous cannulation. J Trauma Acute Care Surg. 2014;76:1328–31. doi: 10.1097/TA.0000000000000209. [DOI] [PubMed] [Google Scholar]