

Abstract
Aim:
This study aims to compare efficacy and safety between mesotherapy (intralesional injection) and 5% topical minoxidil solution in male androgenic alopecia (AGA) by dermoscopic evaluation.
Methodology:
In a randomized active controlled trial, we enrolled 49 clinically diagnosed males of AGA and randomly allotted them into two groups – mesotherapy (A) (25) and minoxidil (B) (24). Males in Group A were given total 8 sessions of intralesional mesosolution with microneedling procedure while Group B males were prescribed topical solution of minoxidil 5% twice daily for 4 months. Results were evaluated at baseline and then monthly for 4 months with clinical photographs, dermoscopy, trichoscan, 7-point standard assessment tool, and patient-self assessment scores.
Results:
Grade II was the most common presentation in our study. All dermoscopic parameters such as variation of hair shaft diameter, follicular units with single and multiple hairs, yellow dots, and perifollicular halo did not show any significant difference between the groups at all time points except at 1st month where the difference in variation of hair shaft diameter between the two group was 0.04. We observed a significant increase (P = 0.01) in the variation of hair shaft diameter between pre- and post-treatment in mesotherapy group compared to minoxidil group. The rest of parameters failed to show any significant difference within the group in mesotherapy and minoxidil.
Conclusion:
In our study, we observed a significant increase in the variation of hair shaft diameter between pre- and post-treatment in Group A compared to B. Other dermoscopic, trichoscan, and subjective measurement tool failed to show significant difference between two groups. Our observation suggests that there is no significant improvement of mesotherapy in male AGA over minoxidil.
Key words: Androgenic alopecia, mesotherapy, trichoscopy
INTRODUCTION
The term “androgenetic alopecia” (AGA) was coined by Orentreich in 1960. Pattern or AGA is a genetically predetermined disorder due to excessive response to androgens which is characterized by progressive miniaturization of the hair follicles on scalp at any time after puberty, in a characteristic distribution in both males and females. In males, hair loss is more prominent in the frontotemporal regions, while in women, the frontal hairline is typically spared with widening of the central partition of the scalp in a Christmas tree pattern. More easy visibility of pattern baldness in males makes them more susceptible to psychological stress. It is the most common type of nonscarring alopecia in men.[1]
Pathophysiology includes shortening hair cycle, increasing telogen shedding as well as increasing the duration of the lag phase or catagen.[1,2]
There are many invasive, semiinvasive, and noninvasive methods available for hair evaluation. Recently, trichoscopy has emerged as a novel, easy, accurate, and handy OPD tool to identify, differentiate, evaluate the condition, and monitor the therapy.[3]
Mesotherapy is a Greek word which means treating (“therapy”) the middle layer of skin (“mesoderm”). It involves microinjections of multiple conventional medications, vitamins, pharmaceuticals, and other ingredients into the mesoderm.
Minoxidil discovered originally as an antihypertensive agent increases vasculature of hair follicles through its direct vasodilatory action and prolongs the anagen phase of hair cycle.[3,4]
Till now, though many studies have been conducted with different therapies and evaluated by various methods, we could not find any study about mesotherapy in male AGA which is evaluated by dermoscopy. Hence, we conducted a study to compare efficacy and safety between mesotherapy with microneedling and topical minoxidil 5% solution in male AGA with dermoscopic evaluation.
METHODOLOGY
A randomized active controlled trial was undertaken at outpatient clinic of Department of Dermatology between January 2017 and May 2018 after obtaining prior human ethics approval and prospectively registering in Clinical trial registry of India. Following the checklist of CONSORT, a total of 65 males between 18 and 35 years of age with clinically diagnosed mild to moderate AGA (Grades II–V), according to Norwood–Hamilton classification, were enrolled in the study after taking a written informed consent. Sample size was calculated as 70 using Nmaster software taking Power-80 (Nmaster software 2.0 uses STATA, EpiInfo, nQuery and others for sample size calculation. It is from Department of biostatitics, CMC, Vellore.). About 16 males were lost to follow-up because of prolonged follow-up period and delayed improvement in the hair loss. The rest 49 males were randomly allocated into microneedling procedure combined with mesosolution Group A (n = 25) and minoxidil Group B (n = 24). We excluded males who were on any allopathic treatment for hair loss within last 6 months, having other scalp dermatoses, prior major illness or hospitalization, thyroid disease, systemic illness, anemia, taking psychiatric medications, and those refusing for consent for enrolling into the study and long follow-up.
Detailed clinical record was prepared on a predesigned pro forma, and all the patients were subjected to detailed history. Nature of the disease, various treatment options, and prognosis of each treatment modality were explained to the patient before enrolling them.
Routine investigations such as complete blood count, renal and liver function test, random blood sugar, viral markers such as HIV, hepatitis B surface antigen, hepatitis C, and thyroid function test were carried out before commencing the treatment to rule out infection, thyroid disorder, anemia, and systemic illness.
Therapy group
Mesotherapy
Patients were enrolled for mesotherapy group after performing intradermal allergy testing with mesosolution. After applying topical anesthesia, intradermal injections of mesosolution were given combined with microneedling. Any adverse events were noted during the procedure, and if no complications appeared, patient was allowed to go home.
Mesohair solution contained 56 ingredients including 24 amino acids, 13 vitamins, 4 coenzymes, 4 nucleic acids, 5 minerals, and 2 reducing agents. The active ingredient was decapeptide 4, acetyl decapeptide, and copper tripeptide [Figure 1].
Figure 1.

Derma roller and mesosolution
Follow-up
This procedure was repeated weekly for 1 month followed by fortnightly for 2nd month and then every monthly for 2 months. Hence, in total, eight sessions were carried out.
Postoperative advice
Patients were advised not to wash, comb, or itch their scalp for 3 days after the procedure. They were asked to restrain from heavy exercise, apply oil or dye, and going out bareheaded in pollution for 3 days.
Minoxidil
Patient under minoxidil Group B was prescribed application of 2–3 ml of 5% minoxidil solution twice daily on the bald areas of scalp. They were explained the side effects such as initial hair loss for 1–2 months, headache, redness, and irritation. They were also reassured about the lag period of about 2–3 months for the improvement.
Evaluation method
All the enrolled males were evaluated before starting therapy and then monthly till 4 months. Gross photographs were taken under adequate illumination, identical settings, lighting, and position. Measuring tape was used to determine three fixed point on the scalp for future dermoscopic evaluation. Landmarks for each frontal region were the intersecting point between lines passing through ipsilateral tragus and lateral point of eyebrows and the intersection of two imaginary line crossing both the ears and glabella for vertex region. A Heine Delta 20 Plus videodermoscope (Germany) with polarized light that is attached with digital camera (Canon EOS 550 D Camera, Tokyo, Japan) was used for trichoscopy and trichoscan was performed on the same dermoscopic pictures through computer-based software [Figure 2]. Measuring tape was used to determine three fixed point on the scalp for future dermoscopic evaluation. Two subjective evaluating methods such as standard 7-point analysis scales and patient self-assessment score were used [Tables 1 and 2]. The data analyzed were from frontal region between the two groups. Dermoscopic and trichoscan readings in vertex region of the same patient was considered as control.
Figure 2.
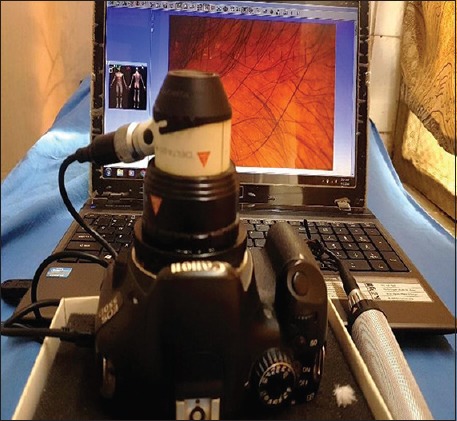
Heine 20 × dermoscope with trichoscan
Table 1.
Standard 7-point rating scale
| Score | |
|---|---|
| Slightly increased | +1 |
| Moderately increased | +2 |
| Greatly increased | +3 |
| No change | 0 |
| Slightly decreased | −1 |
| Moderately decreased | −2 |
| Greatly decreased | −3 |
Table 2.
Patients self-assessment tool
| Score | |
|---|---|
| No improvement | 0 |
| 1%-25% improvement | 1 |
| 26%-50% improvement | 2 |
| 51%-75% improvement | 3 |
| 76%-100% improvement | 4 |
Direct dermoscopy showed parameters such as variation in hair shaft diameters, number of follicular units with one and more than one hair follicles, number of yellow dots (YD), white dots, and perifollicular halo. Kodak A4 print of dermoscopic pictures was used to count the primary parameters manually [Figure 3]
Trichoscan performed provided total hair count, hair density, percentage of anagen hairs, catagen hairs, ratio of vellus hairs, and terminal hairs over an area of 1.195 cm2. Trichoscopic parameters were evaluated by two observers.
Figure 3.

Kodak A4 print with dermoscopic picture
Statistical analysis
The data collected were analyzed in Graphpad instat software, Inc (California, version 3.06). Parameters in-between the two groups were compared using Mann–Whitney test (nonparametric) at all 5 time points. Difference in the parameters within the group at different time points was compared using paired t-test (parametric distribution) and Kruskal–Wallis test (nonparametric distribution). P < 0.05 was considered as statistical significant.
OBSERVATION AND RESULTS
Out of 65 enrolled males, 17 dropped the treatment. We randomly recruited the remaining 49 males into two therapeutic groups – mesotherapy (25) and minoxidil (24).
Grade II (Norwood–Hamilton classification) was the most common (63%) grade of presentation followed by Grade III (27%) in our study [Graph 1]. Demographic details of participants of our study are mentioned in Table 3.
Graph 1.
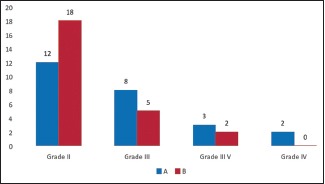
Distribution of patients (n) based on grades of androgenic alopecia
Table 3.
Demographic details of the study group
| Parameters | Group 1 | Group 2 |
|---|---|---|
| Age (years) | ||
| 18-25 | 17 | 15 |
| 26-30 | 5 | 6 |
| 31-35 | 3 | 3 |
| Duration of illness (years) | 3.4 | 3 |
| Positive family history of early hair loss | 8 | 10 |
Values mentioned in the table are mean
The treatment result were analyzed at time points 0, 1st, 2nd, 3rd and 4th month with the help of dermoscope and trichoscan.
As per described in methodology, here, we have described the result using five parameters in dermoscopy and eight parameters in trichoscan. We also have included two subjective scores – standard 7-point rating tool and patients self-assessment score which was based on physician and patients interpretation, respectively.
Table 4 and 5 show the comparison of median values of dermoscopic and trichoscan parameters between Groups A and B at all time periods. Table 6 demonstrates the intragroup comparison of dermoscopic parameters between 0 and 4th month in both the groups.
Table 4.
Result analysis using dermoscopic parameters between mesotherapy and minoxidil group (intergroup)
| Months | Variation in hair shaft diameter (%) |
FU with single hair |
FU with multiple hairs |
Number of yellow dots |
Number of perifollicular halo |
|||||
|---|---|---|---|---|---|---|---|---|---|---|
| A | B | A | B | A | B | A | B | A# | B# | |
| 0 | 29 (15) | 30 (15) | 55 (26) | 57 (22) | 9 (5) | 13 (12) | 30 (73) | 30 (44) | 8 (14) | 3 (5) |
| P | 0.91 | 0.50 | 0.23 | 0.81 | 0.46 | |||||
| 1 | 37 (13) | 31 (17) | 59 (22) | 57 (23) | 9 (7) | 12 (18) | 28 (48) | 31 (47) | 11 (9) | 4 (1) |
| P | 0.04* | 0.56 | 0.114 | 0.23 | 0.39 | |||||
| 2 | 35 (16) | 32 (18) | 57 (20) | 57 (17) | 6 (7) | 10 (12) | 24 (17) | 38 (50) | 13 (15) | 0 (3) |
| P | 0.43 | 0.68 | 0.38 | 0.15 | 0.09 | |||||
| 3 | 34 (18) | 37 (16) | 55 (20) | 61 (15) | 6 (11) | 10 (10) | 29 (47) | 34 (51) | 0 (10) | 3 (6) |
| P | 0.78 | 0.22 | 0.522 | 0.37 | 0.80 | |||||
| 4 | 40 (19) | 33 (26) | 55 (23) | 58 (26) | 8 (7) | 10 (9) | 28 (28) | 41 (72) | 12 (15) | 5 (3) |
| P | 0.28 | 0.45 | 0.18 | 0.29 | 0.19 | |||||
Values mentioned in the table are in median (IQR). P values are calculated using Mann-Whitney test while comparing the values between Group A and B. *P<0.05 was considered significant. #Here, sample size for A-25, B-24 for all parameters except for perifollicular halo. As we found perifollicular halo only in 6 patients in both the groups, sample size is 6 in each group. FU – Follicular unit; IQR – Interquartile range
Table 5.
Result analysis using trichoscan parameters between mesotherapy and minoxidil group (inter group)
| Months | Total hair count |
Hair density/cm2 |
Anagen hairs |
Telogen hairs |
Vellus hairs density |
Terminal hair density |
Ratio vellus hairs |
Ratio terminal hairs |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| A | B | A | B | A | B | A | B | A | B | A | B | A | B | A | B | |
| 0 | 279 (112) | 297 (75) | 233 (92) | 254 (74) | 73 (12) | 75 (8) | 28 (13) | 26 (7) | 105 (52) | 100 (34) | 140 (46) | 146 (65) | 45 (15) | 40 (14) | 57 (15) | 62 (15) |
| P | 0.96 | 0.78 | 0.5 | 0.29 | 0.26 | 0.5 | 0.24 | 0.45 | ||||||||
| 1 | 261 (146) | 302 (55) | 212 (123) | 252 (46) | 72 (14) | 77 (8) | 28 (14) | 23 (8) | 115 (43) | 107 (51) | 132 (44) | 139 (50) | 48 (20) | 40 (15) | 53 (19) | 61 (14) |
| P | 0.89 | 0.67 | 0.19 | 0.16 | 0.49 | 0.19 | 0.24 | 0.25 | ||||||||
| 2 | 266 (48) | 293 (95) | 222 (35) | 245 (79) | 70 (14) | 74 (10) | 31 (14) | 28 (9) | 96 (39) | 114 (50) | 118 (44) | 118 (71) | 43 (10) | 44 (25) | 58 (11) | 57 (26) |
| P | 0.17 | 0.05 | 0.16 | 0.12 | 0.66 | 0.36 | 0.29 | 0.28 | ||||||||
| P | 283 (54) | 283 (110) | 234 (37) | 237 (93) | 71 (19) | 73 (12) | 33 (19) | 28 (13) | 113 (47) | 83 (28) | 110 (46) | 138 (84) | 47 (13) | 42 (22) | 54 (13) | 58 (20) |
| P | 0.84 | 0.5 | 0.96 | 0.06 | 0.78 | 0.22 | 0.34 | 0.25 | ||||||||
| 4 | 278 (114) | 285 (48) | 231 (94) | 238 (39) | 70 (11) | 72 (12) | 31 (13) | 29 (13) | 104 (46) | 90 (47) | 109 (61) | 131 (66) | 49 (22) | 40 (17) | 54 (23) | 61 (16) |
| P | 0.98 | 0.42 | 0.94 | 0.69 | 0.26 | 0.1 | 0.54 | 0.34 | ||||||||
Values mentioned in the table are in median (IQR). P values are calculated using Mann-Whitney test comparing the values between Group A and B. P<0.05 was considered significant. Sample size of A-25 and B-24. IQR – Interquartile range
Table 6.
Intragroup comparison of dermoscopic parameters before and after treatment in both the groups
| 0 month | 4th month | P | |
|---|---|---|---|
| Variation in hair shaft diameter | |||
| A | 29 (15) | 40 (19) | 0.01* |
| B | 30 (15) | 33 (26) | 0.61 |
| FU with single hair | |||
| A | 55 (26) | 55 (23) | 0.52 |
| B | 57 (22) | 58 (26) | 0.53 |
| FU with multiple hairs | |||
| A | 9 (5) | 8 (7) | 0.62^ |
| B | 13 (12) | 10 (9) | 0.47 |
| Number of yellow dots | |||
| A | 30 (73) | 28 (28) | 0.57^ |
| B | 30 (44) | 41 (72) | 0.41^ |
| Number of perifollicular halo | |||
| A | 8 (14) | 12 (15) | 0.74^ |
| B | 3 (5) | 5 (3) | 0.96^ |
Values mentioned here are median (IQR). P values are calculated with the help of paired t-test (parametric distribution) and Mann-Whitney’s test (^nonparametric distribution). *P<0.05 was considered significant. FU – Follicular unit; IQR – Interquartile range
In dermoscopic evaluation, the difference in the median values of variation in hair shaft diameter (except at 1st month), follicular units with single as well as multiple hairs, number of YD, and perifollicular halo was not significant between both the groups at all time points. The difference in variation of hair shaft diameter was significant between both the groups at the end of 1 month (P = 0.04) [Table 4 and Graph 2]. We found a significant increase (P = 0.01) in the variation of hair shaft diameter between pre- and post-treatment in mesotherapy group. Other four dermoscopic parameters failed to show any significant difference between pre- and post-treatment in both the groups [Table 6]. We found appearance of multiple black dots few days after mesotherapy procedure which later disappeared [Figures 4-6].
Graph 2.
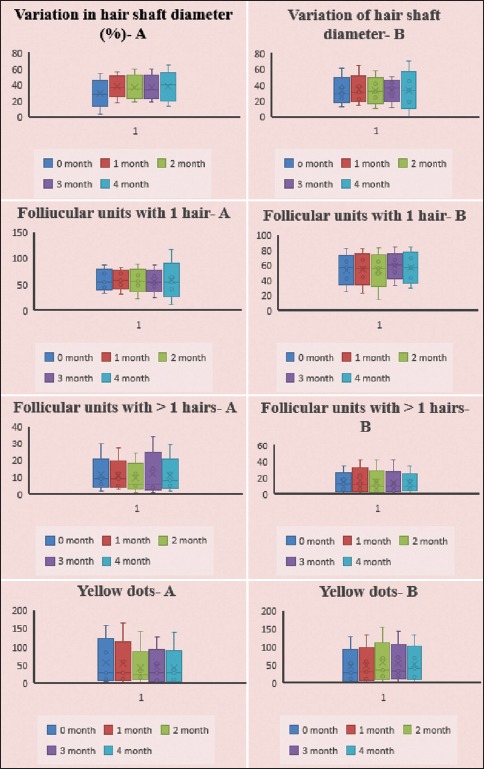
Demonstrates the distribution of 50% data of four dermoscopic parameters (represented inside the box) in both the Groups (A and B) at all time periods. Here, the partition line (__) inside the box represents the median value. (⊥) indicates the minimum and maximum values of data. Variation in hair shaft diameter (%) - A. Variation of hair shaft diameter - B. Follicular units with 1 hair - A. Follicular units with 1 hair - B. Follicular units with >1 hairs - A. Follicular units with >1 hairs - B. Yellow dots - A. Yellow dots - B
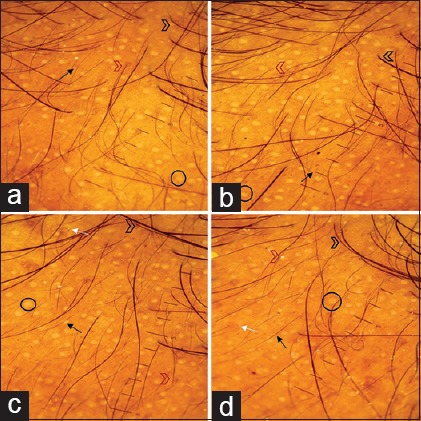
Figure 4.
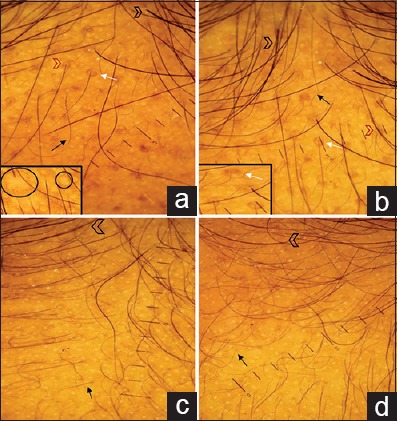
Dermoscopy as a monitoring tool in mesotherapy. (a and b) Dermoscopy findings after improvement. (a) Pretreatment. (b) Posttreatment. There is an increase in the number of hairs with treatment. While there is no change in the number of follicular units with single and multiple hairs and perifollicular halo. (c and d) Dermoscopy findings after slight improvement. (c) Pretreatment. (d) Posttreatment. There is minimal change in the number of hairs and follicular units with single hairs. Thin hairs (black arrow), thick hairs (arrow head), variation in hair shaft diameter is >20% varying size and shape of yellow dots (black circle) in interfollicular area and around the miniaturized hair follicle, predominance of follicular units with single hairs, follicular units with >1 hairs (red arrow head), perifollicular halo (white arrows)
Figure 6.
Dermoscopy as a monitoring tool in minoxidil. (a and b) Dermoscopic findings after improvement. (a) Pretreatment. (b) Posttreatment. There is an increase in the number of hairs with treatment while there is no change in the number of follicular units with single and multiple hairs and yellow dots. (c and d) Dermoscopic findings after slight improvement. (c) Pretreatment. (d) Posttreatment. There is no major change in the number of hairs, yellow dots, and perifollicular halo. Light yellow dots of varying size are seen. Thin hairs (black arrow) thick hairs (arrow head), variation in hair shaft diameter is >20%, yellow dots (black circle) predominance of follicular units with single hairs, follicular units with >1 hairs (red arrow head), perifollicular halo (white arrows)
Figure 5.
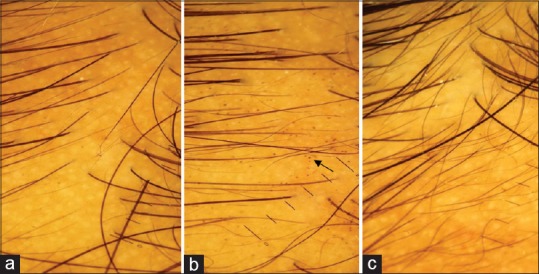
Appearance of black dots postmesotherapy procedure. (a) Baseline, (b) 1st month, (c) posttreatment. Appearance of black dots (black arrow) at 1st month postmesotherapy procedure is due to microhemorrhage due to multiple trauma which later disappears
There was no statistical difference between the median values of trichoscan parameters between both the groups at all time periods [Table 5].
[Graph 2] represents the distribution of data of dermoscopic parameters throughout the study period in both Group A and Group B.
Based on the standard 7-point scale, we did not observe any statistically significant difference in the number of males experiencing mild and moderate improvement in hair growth between Groups A and B [Table 7].
Table 7.
Standard 7-point rating scale at the end of treatment
| A (25) | B (24) | P | |
|---|---|---|---|
| Slightly increased (+1) | 20 | 22 | 0.94 (nonsignificant) |
| Moderately increased (+2) | 5 | 2 | |
| Greatly increased (+3) | 0 | 0 | |
| No change (0) | 0 | 0 | |
| Slightly decreased (−1) | 0 | 0 | |
| Moderately decreased (−2) | 0 | 0 | |
| Greatly decreased (−3) | 0 | 0 |
Values mentioned here are the number of patients attaining the score at the end of 4th month in both groups
Twenty-three males under mesotherapy group experienced up to 25% improvement in hair loss and hair growth while 2 males noticed hair growth of about 25%–50%. Whereas all the males applying minoxidil solution felt improvement only up to 25% in hair loss and hair growth [Table 8]. In few males (4) having AGA involving vertex area, mesotherapy was more effective than frontal region (standard 7-point tool reaching moderately increased and patient self-assessment scale reaching 26%–50% improvement) [Figures 7 and 8].
Table 8.
Patients self-assessment tool at the end of treatment
| A (25) | B (24) | P | |
|---|---|---|---|
| No improvement (0) | 0 | 0 | 0.82 (nonsignificant) |
| 1%-25% improvement (1) | 23 | 24 | |
| 26%-50% improvement (2) | 2 | 0 | |
| 51%-75% improvement (3) | 0 | 0 | |
| 76%-100% improvement (4) | 0 | 0 |
Values mentioned here are the number of patients attaining the score at the end of 4th month in both groups
Figure 7.
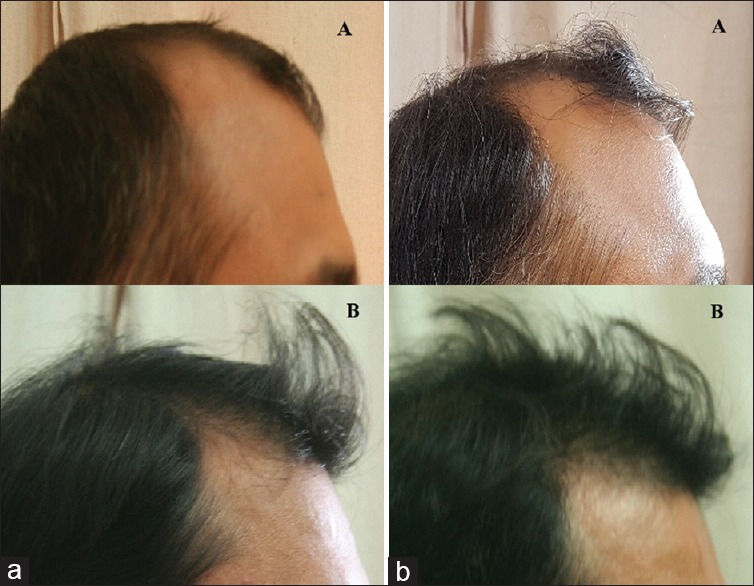
Clinical photographs over frontal region of both the groups. (a) Pretreatment: (A) mesotherapy, (B) minoxidil. (b) Posttreatment: (A) mesotherapy, (B) minoxidil
Figure 8.

Clinical photographs over vertex region of both the groups. (a) Pretreatment: (A) mesotherapy, (B) minoxidil. (b) Posttreatment: (A) mesotherapy, (B) minoxidil
Side effects of mesotherapy and minoxidil group are mentioned in Table 9.
Table 9.
Adverse drug reaction associated with study group
| ADR | Mesotherapy (%) | Minoxidil (%) |
|---|---|---|
| Headache | 3 (13) | 4 (17) |
| Redness | 21 (88) | 2 (8) |
| Hair loss | 1 (4) | 8 (33) |
| Swelling | 2 (8) | 0 |
| Anaphylaxis, allergy | 0 | 0 |
| Exfoliation of skin | 0 | 7 (29) |
| Hypertrichosis | 0 | 0 |
Values mentioned in the table are frequency (percentage). ADR – Adverse drug reaction
DISCUSSION
Alopecia induced by androgens in genetically predisposed individuals is termed as AGA. During the era of Shakespeare, the only option of AGA was to live with it as its pathogenesis was not clearly understood. The importance of treating this condition is growing because of the emphasis that modern society lays on “looking good.” It has always been recognized as having significant psychological effects on affected patients. Now, we have a deeper understanding of the genetics, molecular basis, and pathophysiology of AGA which has given the way for effective treatment modalities.[1,2]
Similar to one Indian study, the most common grade of AGA we came across was Grade II (61%) based on Norwood–Hamilton classification of AGA [Graph 1].[5,6]
Availability of noninvasive, easy, handy, and accurate OPD assessment tools like dermoscope is a boon for a dermatologist to monitor therapeutic effects.[3] Trichoscopy is a terminology used for dermoscopic examination of hair and scalp. It helps to visualize the hair shaft, scalp epidermis, and follicular openings with higher magnification and accuracy. Seleit et al. defined the dermoscopic features of AGA like variation in hair shaft diameter or anisotrihosis (>20%), YD, and peripilar sign.[7] Predominance of pilosebaceous units with single hairs over frontal area of the scalp compared to occiput has been described by Rakowska et al.[8] As dermoscopic diagnostic criteria for males are yet not described in literature, we have used the above parameters for evaluation of therapy. Parameters such as variation in hair shaft diameter, YD, and new tiny hairs can be used to identify the disease severity and assess the therapeutic response.
Trichoscan is a computer-based software which combines standard epiluminescence microscopy with automatic digital image analysis for the measurement of all important hair parameters in situ. The major drawback with trichoscan is that it lacks the sensitivity to identify fine vellus hairs with diameter <16 μm.[9]
Treating AGA has always been challenging in both the gender. There are only two US Food and Drug Administration-approved drugs for male pattern hair loss – topical minoxidil 5% solution and oral finasteride (5 alpha II reductase inhibitor) 1 mg daily dose. Most of the treatment options available provide only temporary hair growth. Hence, there was always a need to find other solution for hair loss.[10,11]
Minoxidil is an antihypertensive drug which opens ATP-sensitive potassium channels in cell membranes, leading to a vasodilatation. It also increases the expression of vascular endothelial growth factor in the dermal papillae and activates prostaglandin synthase-1, an enzyme that stimulates hair growth. Topical 5% and 2% minoxidil solution prevents progression of AGA in adult males and females, respectively.[12]
The term “mesotherapy” which means therapy in the meso (= mesoderm or middle layer of skin) is a vanished older therapeutic option for many skin diseases. It was previously used by ancient European ladies to beautify their skin. After that, its use in many dermatological conditions has been tried. It consists of injecting conventional herbal and allopathic medications in the dermal layer of the skin. Improvement in AGA with mesotherapy is because of direct inoculation of mesosolution into the scalp, and multiple trauma induced by the injection increases the local release of cytokines and growth factors.[4,13]
There is a very limited literature available on mesotherapy of scalp disorders. One Egyptian study observed significant increase in patient self-assessment score as well as increase in anagen hair count by trichogram in mesotherapy group compared to topical minoxidil group in females with AGA. However, we did not observe any significant difference (P = 0.82) in patient self-assessment score between Groups A and B in males. We could not find literature of mesotherapy in male AGA. Hence, comparing the results of our study and the above-mentioned study, it can be interpreted that mesotherapy may not be equally effective in males as compared to females [Table 8].[4]
Dhurat et al. in their study found that 18 and 22 males out of 50 achieved marked and moderate improvement, respectively, based on 7-point evaluation score in microneedling group while none of the patients in minoxidil group reached up to this improvement.[14] In contrast to this, we observed moderate improvement in 5 males of mesotherapy group and 2 males of minoxidil group [Table 7].[14]
Dermoscopy as a therapeutic evaluation
We have included five dermoscopic parameters for evaluation [Tables 4, 6 and Figures 4-6].
Variation in hair shaft diameter is an important major diagnostic criterion for AGA as mentioned by Rakowska et al. They represent miniaturized hair follicles on the bald patch.[7,8] This was a consistent finding in all the males with AGA in our study. We noted a nonsignificant difference in the variation of hair shaft diameter between Groups A and B at all time points except in 1st month (P = 0.04). This suggests that appearance of new hairs was faster after mesotherapy as compared to minoxidil [Table 4]. In our study, the variation in hair shaft diameter increased significantly posttreatment in mesotherapy group (P = 0.01) and nonsignificantly (P = 0.61) in minoxidil group which may be due to the growth of new thin hairs which are sometimes not perceived by naked eyes but only visualized under dermoscope [Table 6]. These new fine hairs correspond to early anagen stage and accelerated hair cycle.[8] This marks the superiority of dermoscope in identifying newly grown tiny thin hairs as an early response marker over clinical observation. Ganjoo and Thappa in their study on intralesional corticosteroid in alopecia areata have mentioned that appearance of new vellus hairs is indicator of remission of the disease. This finding in follow-up visits can encourage the patient to continue treatment[15]
Normally, healthy scalp consists of follicular units with 1–4 hairs arising. However, in AGA, follicular units with single hairs predominate in the frontal area (>2:1) compared to vertex.[7,8] In our study, we observed nonsignificant difference (P = 0.45) in the number of follicular units with single hairs between the two groups after the completion of therapy [Tables 4 and 6]
YD corresponds to active sebaceous glands which produces intraepidermal sebum lagoons after the advanced miniaturized hair follicles. Rudnicka et al. have mentioned that YD vary in size, color, and shape.[7,8,16] Interestingly, in our study on Indian males, we also observed light yellow color dots of irregular size and number with individual variation. Few of them were present near a miniaturized hair follicle. We observed a nonsignificant difference (P = 0.29) in the number of YD at the end of treatment between mesotherapy and minoxidil group [Tables 4 and 6]. This suggests that YD did not show any significant reduction in both the groups. Ganjoo and Thappa similarly demonstrated that YD responded last in their study of alopecia areata[15]
Perifollicular discoloration/halo/peripilar sign is another important dermoscopic finding in AGA which corresponds to lymphocytic infiltrate around hair follicle. It is observed in early stage of AGA and is not specific for AGA as it also sometimes found in telogen effluvium.[8,16] We did not observe any significant difference in the number of perifollicular halo between groups and within the group (P = 0.96) [Tables 4 and 6].
Dermoscopy combined with trichoscan as a therapeutic evaluation
In our study, we did not observe any significant difference in trichoscan parameters between the two groups and also within the same group before and after treatment. We observed nonignificant decrease in median of total hair count, hair density, anagen hairs, vellus hair density, terminal hair density, and ratio terminal hairs [Table 5]. Low sensitivity can be responsible for this result. With the help of trichogram, Mohamed and Hala et al. in their study described anagen hair to increase and telogen hairs to decrease significantly with mesotherapy which is different from our finding.[4] Saraogi and Dhurat in their study have concluded that anagen/telogen hair detection was not optimal with an overestimation of total hair density in trichoscan. She also stated that vellus hair percentage did not correlate well with the clinical severity of the hair loss.[3,9]
Therapeutic safety
Sufficient literature regarding the efficacy and safety profile of mesotherapy for hair loss are lacking. Few studies have reported the development of noncicatricial alopecia and abscess after use of mesotherapy on scalp.[17,18] Fortunately, in our study, we did not come upon any major adverse events except few mild side effects [Table 9]. Those males undergoing mesotherapy commonly complained of erythema (88%) postprocedure which persisted for 1–2 h. This may be due to multiple microinjury following microneedling and injecting mesosolution. Patients applying minoxidil solution commonly complained of headache (17%) and erythema due to its vasodilatory action. This indicates safety of mesotherapy for AGA in our study.
Furthermore, as minoxidil initially regulates the hair cycle and sheds more telogen, patient complains of hair loss (33%) in the initial months [Table 9]. Similarly, DeVillez observed worsening of frontotemporal baldness in his study group even after application on twice daily minoxidil.[19] About 11 males of minoxidil group discontinued the treatment because of delay of therapeutic effect within 2 months. Similar observation was noted by Mapar and Omidian.[20] No any systemic side effects were noted in the study group.
Few limitations of our study include smaller sample size, patient losing to follow-up due to delayed treatment, and shorter duration of follow-up.
CONCLUSION
Our study has demonstrated the role of trichoscopy in increasing the accuracy for diagnosing hair disorders, determining the disease stage, and identifying early response markers to treatment as well as to detect failure to treatment. Variation in hair shaft diameter increases earlier than other dermoscopic parameters and its increase represents new growth of thin hairs which indicates a positive response to treatment. Thus, it is a very important parameter for therapeutic monitoring. Other four dermoscopic and trichoscan parameters as well as subjective assessment tools did not show significant improvement of mesotherapy over minoxidil in male AGA.
Still, further studies with larger sample size and longer follow-up period are required to establish the role of mesotherapy in AGA. Although effective therapeutic options are limited, AGA continues to remain an area where expanding research is adding more information regarding pathogenesis and newer therapeutic options are being developed accordingly.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Kaliyadan F, Nambiar A, Vijayaraghavan S. Androgenetic alopecia: An update. Indian J Dermatol Venereol Leprol. 2013;79:613–25. doi: 10.4103/0378-6323.116730. [DOI] [PubMed] [Google Scholar]
- 2.Sehgal VN, Kak R, Aggarwal A, Srivastava G, Rajput P. Male pattern androgenetic alopecia in an Indian context: A perspective study. J Eur Acad Dermatol Venereol. 2007;21:473–9. doi: 10.1111/j.1468-3083.2006.01920.x. [DOI] [PubMed] [Google Scholar]
- 3.Dhurat R, Saraogi P. Hair evaluation methods: Merits and demerits. Int J Trichology. 2009;1:108–19. doi: 10.4103/0974-7753.58553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mohamed H, Hala M. Comparative study between 2% minoxidil topical spray vs. intradermal injection (Mesotherapy) for treatment of androgenetic alopecia in female patients: A controlled, 4-month randomized trial. Egypt Dermatol Online J. 2010;6:5. [Google Scholar]
- 5.Wang TL, Zhou C, Shen YW, Wang XY, Ding XL, Tian S, et al. Prevalence of androgenetic alopecia in China: A community-based study in six cities. Br J Dermatol. 2010;162:843–7. doi: 10.1111/j.1365-2133.2010.09640.x. [DOI] [PubMed] [Google Scholar]
- 6.Kaufman KD, Girman CJ, Round EM, Johnson-Levonas AO, Shah AK, Rotonda J, et al. Progression of hair loss in men with androgenetic alopecia (male pattern hair loss): Long-term (5-year) controlled observational data in placebo-treated patients. Eur J Dermatol. 2008;18:407–11. doi: 10.1684/ejd.2008.0435. [DOI] [PubMed] [Google Scholar]
- 7.Seleit IA, El-Bakry OA, El-Sherif RM. Dermoscopy in hair disorders. Menoufia Med J. 2014;27:762–5. [Google Scholar]
- 8.Rakowska A, Slowinska M, Kowalska-Oledzka E, Olszewska M, Rudnicka L. Dermoscopy in female androgenic alopecia: Method standardization and diagnostic criteria. Int J Trichology. 2009;1:123–30. doi: 10.4103/0974-7753.58555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Saraogi PP, Dhurat RS. Automated digital image analysis (TrichoScan®) for human hair growth analysis: Ease versus errors. Int J Trichology. 2010;2:5–13. doi: 10.4103/0974-7753.66905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lee WS, Lee HJ, Choi GS, Cheong WK, Chow SK, Gabriel MT, et al. Guidelines for management of androgenetic alopecia based on BASP classification – The Asian consensus committee guideline. J Eur Acad Dermatol Venereol. 2013;27:1026–34. doi: 10.1111/jdv.12034. [DOI] [PubMed] [Google Scholar]
- 11.Tsuboi R, Arano O, Nishikawa T, Yamada H, Katsuoka K. Randomized clinical trial comparing 5% and 1% topical minoxidil for the treatment of androgenetic alopecia in Japanese men. J Dermatol. 2009;36:437–46. doi: 10.1111/j.1346-8138.2009.00673.x. [DOI] [PubMed] [Google Scholar]
- 12.Olsen EA, Dunlap FE, Funicella T, Koperski JA, Swinehart JM, Tschen EH, et al. A randomized clinical trial of 5% topical minoxidil versus 2% topical minoxidil and placebo in the treatment of androgenetic alopecia in men. J Am Acad Dermatol. 2002;47:377–85. doi: 10.1067/mjd.2002.124088. [DOI] [PubMed] [Google Scholar]
- 13.Vedamurthy M. Mesotherapy. Indian J Dermatol Venereol Leprol. 2007;73:60–2. doi: 10.4103/0378-6323.30661. [DOI] [PubMed] [Google Scholar]
- 14.Dhurat R, Sukesh M, Avhad G, Dandale A, Pal A, Pund P, et al. A randomized evaluator blinded study of effect of microneedling in androgenetic alopecia: A pilot study. Int J Trichology. 2013;5:6–11. doi: 10.4103/0974-7753.114700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ganjoo S, Thappa DM. Dermoscopic evaluation of therapeutic response to an intralesional corticosteroid in the treatment of alopecia areata. Indian J Dermatol Venereol Leprol. 2013;79:408–17. doi: 10.4103/0378-6323.110767. [DOI] [PubMed] [Google Scholar]
- 16.Rudnicka L, Olszewska M, Rakowska A, Slowinska M. Trichoscopy update 2011. J Dermatol Case Rep. 2011;5:82–8. doi: 10.3315/jdcr.2011.1083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Duque-Estrada B, Vincenzi C, Misciali C, Tosti A. Alopecia secondary to mesotherapy. J Am Acad Dermatol. 2009;61:707–9. doi: 10.1016/j.jaad.2008.11.896. [DOI] [PubMed] [Google Scholar]
- 18.Kadry R, Hamadah I, Al-Issa A, Field L, Alrabiah F. Multifocal scalp abscess with subcutaneous fat necrosis and scarring alopecia as a complication of scalp mesotherapy. J Drugs Dermatol. 2008;7:72–3. [PubMed] [Google Scholar]
- 19.DeVillez RL. Topical minoxidil for androgenetic alopecia: Optimizing the chance for success by appropriate patient selection. Dermatologica. 1987;175(Suppl 2):50–3. doi: 10.1159/000248903. [DOI] [PubMed] [Google Scholar]
- 20.Mapar MA, Omidian M. Is topical minoxidil solution effective on androgenetic alopecia in routine daily practice? J Dermatolog Treat. 2007;18:268–70. doi: 10.1080/09546630701383727. [DOI] [PubMed] [Google Scholar]