

Abstract
Background
Maternal pushing during the second stage of labour is an important and indispensable contributor to the involuntary expulsive force developed by uterine contraction. There is no consensus on an ideal strategy to facilitate these expulsive efforts and there are contradictory results about the influence on the mother and fetus.
Objectives
To evaluate the benefits and possible disadvantages of different kinds of techniques regarding maternal pushing/breathing during the expulsive stage of labour on maternal and fetal outcomes.
Search methods
We searched Cochrane Pregnancy and Childbirth's Trials Register (19 September 2016) and reference lists of retrieved studies.
Selection criteria
Randomised controlled trials (RCTs) and quasi‐RCTs assessing the effects of pushing/bearing down techniques (type and/or timing) performed during the second stage of labour on maternal and neonatal outcomes. Cluster‐RCTs were eligible for inclusion, but none were identified. Studies using a cross‐over design and those published in abstract form only were not eligible for inclusion in this review.
Data collection and analysis
Two review authors independently assessed trials for inclusion, extracted data and assessed risk of bias. Data were checked for accuracy.
Main results
In this updated review, we included 21 studies in total, eight (884 women) comparing spontaneous pushing versus directed pushing, with or without epidural analgesia and 13 (2879 women) comparing delayed pushing versus immediate pushing with epidural analgesia. Our GRADE assessments of evidence ranged from moderate to very low quality; the main reasons for downgrading were study design limitations and imprecision of effect estimates. Overall, the included studies varied in their risk of bias; most were judged to be at unclear risk of bias.
Comparison 1: types of pushing: spontaneous pushing versus directed pushing
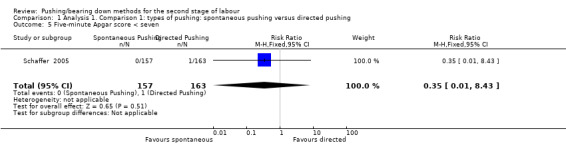
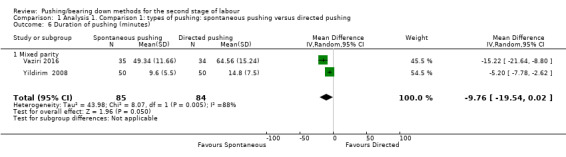
There was no clear difference in the duration of the second stage of labour (mean difference (MD) 10.26 minutes; 95% confidence interval (CI) ‐1.12 to 21.64 minutes, six studies, 667 women, random‐effects, I² = 81%) (very low‐quality evidence). There was no clear difference in 3rd or 4th degree perineal laceration (risk ratio (RR) 0.87; 95% CI 0.45 to 1.66, one study, 320 women) (low‐quality evidence), episiotomy (average RR 1.05; 95% CI 0.60 to 1.85, two studies, 420 women, random‐effects, I² = 81%), duration of pushing (MD ‐9.76 minutes, 95% CI ‐19.54 to 0.02; two studies; 169 women; I² = 88%) (very low‐quality evidence), or rate of spontaneous vaginal delivery (RR 1.01, 95% CI 0.97 to 1.05; five studies; 688 women; I² = 2%) (moderate‐quality evidence). For primary neonatal outcomes such as five‐minute Apgar score less than seven, there was no clear difference between groups (RR 0.35; 95% CI 0.01 to 8.43, one study, 320 infants) (very low‐quality evidence), and the number of admissions to neonatal intensive care (RR 1.08; 95% CI 0.30 to 3.79, two studies, 393 infants) (very low‐quality evidence) also showed no clear difference between spontaneous and directed pushing. No data were available on hypoxic ischaemic encephalopathy.
Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural)
For the primary maternal outcomes, delayed pushing was associated with an increase of 56 minutes in the duration of the second stage of labour (MD 56.40, 95% CI 42.05 to 70.76; 11 studies; 3049 women; I² = 91%) (very low‐quality evidence), but no clear difference in third or 4th degree perineal laceration (RR 0.94; 95% CI 0.78 to 1.14, seven studies. 2775 women) (moderate‐quality evidence) or episiotomy (RR 0.95; 95% CI 0.87 to 1.04, five studies, 2320 women). Delayed pushing was also associated with a 19‐minute decrease in the duration of pushing (MD ‐19.05, 95% CI ‐32.27 to ‐5.83; 11 studies; 2932 women; I² = 95%) (very low‐quality evidence) and an increase in spontaneous vaginal delivery (RR 1.07; 95% CI 1.02 to 1.11, 12 studies, 3114 women) (moderate‐quality evidence).
For the primary neonatal outcomes, there was no clear difference between groups in admission to neonatal intensive care (RR 0.98; 95% CI 0.67 to 1.41, three studies, n = 2197) (low‐quality evidence) and five‐minute Apgar score less than seven (RR 0.15; 95% CI 0.01 to 3.00; three studies; 413 infants) (very low‐quality evidence). There were no data on hypoxic ischaemic encephalopathy. Delayed pushing was associated with a greater incidence of low umbilical cord blood pH (RR 2.24; 95% CI 1.37 to 3.68, 4 studies, 2145 infants) and increased the cost of intrapartum care by CDN$ 68.22 (MD 68.22, 95% CI 55.37, 81.07, one study, 1862 women).
Authors' conclusions
This updated review is based on 21 included studies of moderate to very low quality of evidence (with evidence mainly downgraded due to study design limitations and imprecision of effect estimates).
Timing of pushing with epidural is consistent in that delayed pushing leads to a shortening of the actual time pushing and increase of spontaneous vaginal delivery at the expense of an overall longer duration of the second stage of labour and an increased risk of a low umbilical cord pH (based only on one study). Nevertheless, there was no clear difference in serious perineal laceration and episiotomy, and in other neonatal outcomes (admission to neonatal intensive care, five‐minute Apgar score less than seven and delivery room resuscitation) between delayed and immediate pushing.
Therefore, for the type of pushing, with or without epidural, there is no conclusive evidence to support or refute any specific style as part of routine clinical practice, and in the absence of strong evidence supporting a specific method or timing of pushing, the woman's preference and comfort and clinical context should guide decisions.
Further properly well‐designed RCTs, addressing clinically important maternal and neonatal outcomes are required to add evidence‐based information to the current knowledge. Such trials will provide more complete data to be incorporated into a future update of this review.
Keywords: Adult; Female; Humans; Infant, Newborn; Pregnancy; Analgesia, Epidural; Analgesia, Epidural/methods; Analgesia, Obstetrical; Analgesia, Obstetrical/methods; Breath Holding; Delivery, Obstetric; Delivery, Obstetric/methods; Intensive Care Units, Neonatal; Intensive Care Units, Neonatal/statistics & numerical data; Labor Stage, Second; Labor Stage, Second/physiology; Perineum; Perineum/injuries; Publication Bias; Randomized Controlled Trials as Topic; Respiration; Time Factors; Uterine Contraction; Uterine Contraction/physiology; Valsalva Maneuver
Plain language summary
Pushing methods for the second stage of labour
What is the issue?
During the second stage of labour a common technique is to encourage women to take a deep breath at the beginning of a contraction then hold it and bear down throughout the contraction (this is known as directed pushing). In spontaneous pushing, women are free to follow their own instincts and generally push three to five times per contraction. Delayed pushing involves instructing women to avoid pushing until there is an irresistible urge to push or when the presenting part of the baby has descended to the perineum.
Why is this important?
We need to know the benefits and possible disadvantages of different kinds of techniques regarding maternal pushing/breathing during the expulsive stage of labour on maternal and fetal outcomes.
What evidence did we find?
We searched for evidence on (search date 19 September 2016) and identified eight trials (884 women) comparing the types of pushing: spontaneous pushing versus directed pushing with or without epidural analgesia and 13 trials (2879 women) comparing timing of pushing: delayed pushing versus immediate pushing with epidural analgesia. The quality of the evidence in this updated review ranges from moderate to very low quality.
Comparison 1: Spontaneous pushing versus directed pushing
For types of pushing (spontaneous pushing versus directed pushing) there was no clear difference in the duration of the second stage (very low‐quality evidence), perineal laceration (low‐quality evidence), episiotomy, time spent pushing (very low‐quality evidence), or number of women with a spontaneous vaginal birth (moderate‐quality evidence) between the women who spontaneously pushed and the women who were directed. Outcomes relating to the baby (such as five‐minute Apgar score less than seven (very low‐quality evidence), admission to neonatal intensive care (very low‐quality evidence)) were not clearly different. None of the studies reported on the outcome of babies with hypoxic ischaemic encephalopathy.
Comparison 2: Delayed pushing versus immediate pushing (women with epidural)
For the timing of pushing: delayed pushing versus immediate pushing (all women with epidural) ‐ delayed pushing was associated with an increase in the duration of the second stage by about 56 minutes (very low‐quality evidence). There were no clear differences between the two groups in the number of women with perineal laceration (moderate‐quality evidence) and episiotomy. Delayed pushing reduced the duration of pushing by about 19 minutes (very low‐quality of evidence), and slightly increased the number of women with a spontaneous vaginal birth (moderate‐quality evidence). There were no clear differences between the delayed and immediate pushing groups in terms of important outcomes for the baby: Apgar score less than seven at five minutes (very low‐quality evidence), admission to neonatal intensive care (low‐quality evidence). None of the studies reported on the outcome of babies with brain damage due to lack of oxygen to the brain. Futhermore, delayed pushing was associated with an increased incidence of low umbilical cord pH and increased the cost of intrapartum care by CDN$ 68.22.
What does this mean?
We are unable to say whether spontaneous pushing or directed pushing coaching methods are best. Until further high‐quality studies are available, women should be encouraged to push and bear down according to their comfort and preference.
Delaying pushing for women with epidural reduces the time spent pushing when giving birth, and increases the likelihood of a spontaneous vaginal birth. However, it increases the duration of the second stage. The possible effects on important neonatal outcomes and maternal perineal injury (serious tears) is still unclear. Therefore, the evidence is still insufficient and inconclusive to support any indication of specific timing of pushing as well as for the type of pushing once there is no conclusive evidence to indicate an adequate style of pushing to be used in the clinical practice.
Further properly well‐designed randomised controlled trials are required to produce more evidence‐based information. These trials should address clinically important maternal and neonatal outcomes and will provide more complete data to be incorporated into a future update of this review.
Summary of findings
Summary of findings for the main comparison. Spontaneous pushing compared to directed pushing for the second stage of labour (types of pushing).
| Spontaneous pushing compared to directed pushing for the second stage of labour (types of pushing) | ||||||
| Patient or population: women in the second stage of labour Settings: labour ward. Trials conducted in Turkey, Iran, UK, US and Hong Kong Intervention: types of pushing: spontaneous pushing versus directed pushing | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with directed pushing | Risk with spontaneous pushing | |||||
| Duration of second stage (minutes) | The mean duration of second stage (minutes) was 0 | MD 10.26 higher (1.12 lower to 21.64 higher) | ‐ | 667 (6 RCTs) | ⊕⊝⊝⊝ VERY LOW 1 2 3 | |
| Perineal laceration (3rd or 4th degree) | Study population | RR 0.87 (0.45 to 1.66) | 320 (1 RCT) | ⊕⊕⊝⊝ LOW 3 4 | ||
| 110 per 1000 | 96 per 1000 (50 to 183) | |||||
| Admission to neonatal intensive care | Study population | RR 1.08 (0.30 to 3.79) | 393 (2 RCTs) | ⊕⊝⊝⊝ VERY LOW 1 5 | ||
| 20 per 1000 | 21 per 1000 (6 to 75) | |||||
| Hypoxic ischaemic encephalopathy | Study population | ‐ | (0 study) | ‐ | Outcome not reported in the included studies under this comparison. | |
| see comment | see comment | |||||
| 5‐minute Apgar score < 7 | Study population | RR 0.35 (0.01 to 8.43) | 320 (1 RCT) | ⊕⊝⊝⊝ VERY LOW 4 5 | ||
| 6 per 1000 | 2 per 1000 (0 to 52) | |||||
| Duration of pushing (minutes) | The mean duration of pushing (minutes) was 0 | MD 9.76 lower (19.54 lower to 0.02 higher) | ‐ | 169 (2 RCTs) | ⊕⊝⊝⊝ VERY LOW 2 6 7 | |
| Spontaneous vaginal delivery | Study population | RR 1.01 (0.97 to 1.05) | 688 (5 RCTs) | ⊕⊕⊕⊝ MODERATE 8 9 | ||
| 922 per 1000 | 932 per 1000 (895 to 969) | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; OR: Odds ratio; | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1 Most studies contributing data had design limitations, with more than 40% of weight from studies with serious design limitations. (‐2)
2 Statistical Heterogeneity (I2>60%). Variation in size of effect. (‐1)
3 Wide confidence intervals crossing the line of no effect. (‐1)
4 One study with design limitations. (‐1)
5 Wide confidence intervals crossing the line of no effect and few events. (‐2)
6 One study contributing >40% of data had serious design limitations. One other study had design limitations. (‐2)
7 Wide confidence intervals just crossing the line of no effect and small sample size. (‐2)
8 Study contributing most data (46.9%) has design limitations, other studies have design limitations or serious design limitations. (‐1)
9 Although confidence intervals cross the line of no effect, the effect estimate is precise. (not downgraded)
Summary of findings 2. Delayed pushing compared to immediate pushing (all women with epidural) for the second stage of labour (timing of pushing).
| Delayed pushing compared to immediate pushing (all women with epidural) for the second stage of labour (timing of pushing) | ||||||
| Patient or population: women in the second stage of labour with epidural in situ Settings: labour wards in hospital settings. Trials were carried out in Ireland, US, UK, Canada Intervention: timing of pushing: delayed pushing versus immediate pushing (women with epidural only) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with immediate pushing (all women with epidural) | Risk with delayed pushing | |||||
| Duration of second stage (minutes) | The mean duration of second stage (minutes) was 0 | MD 56.40 higher (42.05 higher to 70.76 higher) | ‐ | 3049 (11 RCTs) | ⊕⊝⊝⊝ VERY LOW 1 2 | 1 trial contributing data for multiparous women, 1 trial included both nulliparous and multiparous women. |
| Perineal laceration (3rd or 4th degree) | Study population | RR 0.94 (0.78 to 1.14) | 2775 (7 RCTs) | ⊕⊕⊕⊝ MODERATE 1 3 | 1 of the studies contributing data reported all lacerations (i.e. did not specify 3rd or 4th degree) | |
| 122 per 1000 | 115 per 1000 (95 to 139) | |||||
| Admission to neonatal intensive care | Study population | RR 0.98 (0.67 to 1.41) | 2197 (3 RCTs) | ⊕⊕⊝⊝ LOW 4 5 | ||
| 49 per 1000 | 48 per 1000 (33 to 69) | |||||
| Hypoxic ischaemic encephalopathy | Study population | ‐ | (0 study) | ‐ | Outcome not reported in the included studies under this comparison. | |
| see comment | see comment | |||||
| 5‐minute Apgar score < 7 | Study population | RR 0.15 (0.01 to 3.00) | 413 (3 RCTs) | ⊕⊝⊝⊝ VERY LOW 6 7 | Only 1 trial contributing data. | |
| 10 per 1000 | 2 per 1000 (0 to 31) | |||||
| Duration of pushing (minutes) | The mean duration of pushing (minutes) was 0 | MD 19.05 lower (32.27 lower to 5.83 lower) | ‐ | 2932 (11 RCTs) | ⊕⊝⊝⊝ VERY LOW 1 2 | 1 trial contributing data for multiparous women, 1 trial included both nulliparous and multiparous women. |
| Spontaneous vaginal delivery | Study population | RR 1.07 (1.03 to 1.11) | 3114 (12 RCTs) | ⊕⊕⊕⊝ MODERATE 1 | ||
| 713 per 1000 | 762 per 1000 (734 to 791) | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; OR: Odds ratio; | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1 All studies have design limitations, two studies contributing <40% have serious design limitations. (‐1)
2 Heterogeneity (I2>60%). Considerable variation in size of effect. (‐2)
3 Although confidence intervals cross the line of no effect, the effect estimate is precise. (not downgraded)
4 All studies have design limitations. (‐1)
5 Wide confidence intervals crossing the line of no effect. (‐1)
6 One study contributing data has design limitations. (‐1)
7 Wide confidence intervals crossing the line of no effect and very few events. (‐2)
Background
Description of the condition
The pattern of breathing that helps women during vaginal labour, especially during the second stage, is a controversial topic in the literature (Beynon 1957; Bloom 2006). Breathing, which is normally an unconscious act, becomes a voluntary and controlled activity induced by the physiological mechanisms of labour.
During the second stage of labour, the fetal presentation comes down and a compression occurs in both the bladder and rectum, generating a reflex which causes a strong urge to bear down, or 'push'. Therefore, the combination of involuntary intrauterine contractions and voluntary expulsive effort, through the abdominal and respiratory muscles, will help fetus delivery (Cunningham 2005). Arbitrarily directing women on how to push or bear down (both terms used) once the cervix is fully dilated is still a common practice (Buhimschi 2002; Thompson 1995).
Description of the intervention
A common technique is to encourage women to use a closed‐glottis pushing (holding breath while pushing) duration of 10 seconds or more, once the cervix has reached 10 cm dilation (Roberts 2002; Yeates 1984). In this procedure, women are coached to take a deep breath at the beginning of a contraction, then hold the breath as long and hard as possible and bear down towards the vagina throughout the contraction (Parnell 1993).
The process of taking a deep breath and holding it with a closed‐glottis is called the Valsalva Maneuver (VM). Several physiological findings oppose the use of the VM of 10 seconds or more, as this type of directed pushing can negatively affect fetal acid‐base balance, Apgar scores and cerebral oxygenation. It can also interfere with the length of the second stage of labour, increase maternal fatigue, cause damage to the maternal pelvic floor structures and impair bladder function (Aldrich 1995; Barnett 1982; Caldeyro‐Barcia 1981; Mayberry 1999; Schaffer 2005; Yildirim 2008).
In contrast, some authors argue that breathing control interventions should not be imposed during the expulsive stage, and that rather than follow direct instructions for the VM, women should be free to follow their own instincts in response to the physiology of this stage in labour (Beynon 1957; Caldeyro‐Barcia 1981; Minato 2001; Roberts 1996). This approach is known as ‘spontaneous or involuntary pushing’ and most of the respiratory effort to help in this type of bearing down occurs with an open glottis (with only about 25% of the breaths carried out using the VM, or closed glottis, and only for a maximum duration of four to six seconds) (Aderhold 1991; Hanson 2009; Roberts 1987). Additionally, women who use spontaneous pushing begin at a resting respiratory volume, push three to five times per contraction and take several breaths between each bearing down effort (Roberts 1987; Yeates 1984). Spontaneous pushing occurs as a result of optimal obstetric conditions for fetal descent which includes fetal station of at least +1 and fetal position (approaching occipito anterior position). This condition evokes the Ferguson's reflex, through increased oxytocin release, which augments maternal bearing down efforts by making them more effective and less fatiguing (Roberts 2002).
The same uncertainty occurs in relation to the second‐stage labour care of women with epidural anaesthesia. The usual practice is to begin encouraging the mother to bear down when the cervix is fully dilated, known as 'early, active or immediate pushing' (Hansen 2002; Maresh 1983; Simpson 2005). However, it has been found that women who have epidural analgesia, for relieving the pain of labour and childbirth, show a weak desire to push due to a diminution of the bearing down reflex (Bates 1985; Thorp 1996). As a result, this interferes with the normal mechanisms of labour and leads to an increase in instrumental deliveries.
Since the 1980s, trials have proposed a 'delayed pushing' method in labours where epidural analgesia is used (Fraser 2000a; Lai 2009;Vause 1998). This method involves instructing women to avoid pushing either until there is an irresistible urge to push, or when the presenting part has descended to the perineum, and is also known as the 'passive descent or labouring down method' (Maresh 1983; Mayberry 1999). This method is associated with a number of benefits in terms of less maternal fatigue, perineal injury, fetal acidosis and a reduction in instrumental deliveries despite an increase in the length of the second stage (Albers 2007; Hansen 2002).
How the intervention might work
It has been suggested that spontaneous pushing allows a slower and controlled descent of the fetus and therefore a gradual stretching of the perineal muscles. This type of pushing may lead to less pressure on the anterior vaginal wall and on the cervical ligaments and connective tissue that support the vaginal walls, as it does not start until the fetus has already started to descend. When the expulsive effort begins before the desire to push, this effort causes a downward pressure on the vaginal wall, the bladder and the support structure in front of the fetal head, which may obstruct the descent of the fetus and contribute to a greater biomechanical misalignment (Beynon 1957; Knauth 1986; Roberts 2007). Thus spontaneous pushing tends to show better maternal perineal results in the short and long term (Schaffer 2005). In addition, spontaneous pushing provides less fatigue and better umbilical cord gasometrics values (Chang 2011; Yildirim 2008).
Those that propose delayed pushing suggest that delay in the onset of pushing would allow spontaneous descent and rotation of the fetal head, thereby maximising the efficiency of pushing efforts and reducing the risk of the parturient fatigue and instrumental delivery (Fraser 2000b; Minato 2001). Delayed pushing aims to reduce the adverse effects of epidural analgesia and facilitate the second stage of labour in those conditions (Hansen 2002; Roberts 2002).
Why it is important to do this review
The involuntary urge to bear down may occur before or after the recognition of complete cervical dilatation. Therefore, the time when the woman should begin to push will have a significant effect on both mother and fetus. However, there is no consensus in the literature about the optimal time for the woman to begin pushing or bearing down.
There are no data to support a policy of directed maternal pushing. Despite several publications showing the adverse maternal and fetal effects from the use of the sustained VM, this choice of method is still common practice worldwide, and the scientific evidence base supporting the recommendation of breathing control for the expulsive stage is scant.
This review will concentrate on all eligible studies using spontaneous versus directed pushing and delayed versus early pushing for bearing down during the second stage of labour, with and without analgesia.
Objectives
The objectives of this review are to determine the benefits and possible disadvantages of different kinds of techniques regarding maternal pushing/breathing during the expulsive stage of labour on maternal and fetal outcomes.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs) and quasi‐RCTs comparing different instructions regarding maternal pushing in the second stage of labour. Cluster‐RCTs were eligible for inclusion, but none were identified.
Studies using a cross‐over design and those published in abstract form only were not eligible for inclusion.
Types of participants
Low‐risk pregnant women during the second stage of labour with all of the following:
nulliparous or multiparous;
between 37 and 42 weeks' gestation;
vertex presentation;
alive fetus;
with or without epidural analgesia;
singleton pregnancy;
absence of intrapartal complications.
Types of interventions
Any kind of breathing/pushing techniques performed during the second stage of labour. We considered the following comparisons.
Timing of pushing: to compare pushing which begins as soon as full dilatation has been determined versus pushing which begins after the urge to push is felt.
Type of pushing: to compare pushing techniques that involve the Valsalva Maneuver (VM) versus all other pushing techniques.
Types of outcome measures
Primary outcomes
Maternal outcomes
Duration of the second stage of labour (as defined by trial author)
Perineal laceration (3rd or 4th degree)
Episiotomy
Neonatal outcomes
Admission to neonatal intensive care
Hypoxic ischaemic encephalopathy
Apgar scores (less than seven at five minutes)
Secondary outcomes
Maternal outcomes
Duration of pushing
Oxytocin use in second stage after randomisation
Mode of delivery (spontaneous vaginal delivery, instrumental delivery, rotational or midpelvic or posterior forceps, caesarean delivery)
Maternal hypertension (as defined by trial author)
Postpartum haemorrhage (as defined by trial author)
Maternal report of severe pain in second stage labour
Fatigue after delivery
Maternal satisfaction
Long‐term outcomes
Perineal pain (as defined by trial author)
Dyspareunia
Urinary incontinence (as defined by trial author)
Detrusor overactivity
Fecal incontinence (as defined by trial author)
Pelvic floor prolapse (as defined by trial author)
Neonatal outcomes
Low umbilical cord blood pH (arterial less than 7.2 and venous less than 7.3)
Delivery room resuscitation
Total care costs (as defined by trial author)
Search methods for identification of studies
The following methods section of this review is based on a standard template used by Cochrane Pregnancy and Childbirth.
Electronic searches
We searched Cochrane Pregnancy and Childbirth’s Trials Register by contacting their Information Specialist (19 September 2016).
The Register is a database containing over 22,000 reports of controlled trials in the field of pregnancy and childbirth. For full search methods used to populate Pregnancy and Childbirth’s Trials Register including the detailed search strategies for CENTRAL, MEDLINE, Embase and CINAHL; the list of handsearched journals and conference proceedings, and the list of journals reviewed via the current awareness service, please follow this link to the editorial information about the Cochrane Pregnancy and Childbirth in the Cochrane Library and select the ‘Specialized Register ’ section from the options on the left side of the screen.
Briefly, Cochrane Pregnancy and Childbirth’s Trials Register is maintained by their Information Specialist and contains trials identified from:
monthly searches of the Cochrane Central Register of Controlled Trials (CENTRAL);
weekly searches of MEDLINE (Ovid);
weekly searches of Embase (Ovid);
monthly searches of CINAHL (EBSCO);
handsearches of 30 journals and the proceedings of major conferences;
weekly current awareness alerts for a further 44 journals plus monthly BioMed Central email alerts.
Search results are screened by two people and the full text of all relevant trial reports identified through the searching activities described above is reviewed. Based on the intervention described, each trial report is assigned a number that corresponds to a specific Pregnancy and Childbirth review topic (or topics), and is then added to the Register. The Information Specialist searches the Register for each review using this topic number rather than keywords. This results in a more specific search set which has been fully accounted for in the relevant review sections (Included studies; Excluded studies; Ongoing studies).
Searching other resources
We searched the reference lists of retrieved studies.
We did not apply any language or date restrictions.
Data collection and analysis
For methods used in the previous version of this review, seeLemos 2015.
For this update, the following methods were used for assessing the seven reports that were identified as a result of the updated search plus the one report in the ongoing studies section of Lemos 2015.
The following methods section of this review is based on a standard template used by Cochrane Pregnancy and Childbirth.
Selection of studies
Two review authors (A Lemos and A Dornelas de Andrade) independently assessed for inclusion all the potential studies that were identified as a result of the search strategy. We resolved any disagreement through discussion and when required, we consulted a third review author (MMR Amorim).
Data extraction and management
We designed a form to extract data. For eligible studies, at least two review authors extracted the data using the agreed form. We resolved differences and discrepancies by discussion and when necessary we consulted a third review author. We entered data into Review Manager software (RevMan 2014) and checked them for accuracy. There was no blinding of authorship or results.
When information regarding any of the above was unclear, we attempted to contact authors of the original reports to provide further details.
Assessment of risk of bias in included studies
Two review authors independently assessed risk of bias for each study using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
(1) Sequence generation (checking for possible selection bias)
We described for each included study whether the method used to generate the allocation sequence was reported in sufficient detail to allow an assessment of whether it should produce comparable groups.
We assessed the method as:
low risk of bias (any truly random process, e.g. random number table; computer random number generator);
high risk of bias (any non‐random process, e.g. odd or even date of birth; hospital or clinic record number);
unclear risk of bias.
(2) Allocation concealment (checking for possible selection bias)
We described for each included study the method used to conceal allocation to interventions prior to assignment and assessed whether intervention allocation could have been foreseen in advance of, or during recruitment, or changed after assignment.
We assessed the methods as:
low risk of bias (e.g. telephone or central randomisation; consecutively numbered sealed opaque envelopes);
high risk of bias (open random allocation; unsealed or non‐opaque envelopes, alternation; date of birth);
unclear risk of bias.
(3) Blinding (checking for possible performance bias)
(3.1) Blinding of participants and personnel
We described for each included study the methods used, if any, to blind study participants and personnel from knowledge of which intervention a participant received. We considered that studies were at low risk of bias if they were blinded, or if we judged that the lack of blinding would be unlikely to affect results. We assessed blinding separately for different outcomes or classes of outcomes.
We assessed the methods as:
low, high or unclear risk of bias for participants;
low, high or unclear risk of bias for personnel.
(3.2) Blinding of outcome assessment (checking for possible detection bias)
We described for each included study the methods used, if any, to blind outcome assessors from knowledge of which intervention a participant received. We assessed blinding separately for different outcomes or classes of outcomes.
We assessed methods used to blind outcome assessment as:
low, high or unclear risk of bias.
(4) Incomplete outcome data (checking for possible attrition bias due to the amount, nature and handling of incomplete outcome data)
We described for each included study, and for each outcome or class of outcomes, the completeness of data including attrition and exclusions from the analysis. We stated whether attrition and exclusions were reported and the numbers included in the analysis at each stage (compared with the total randomised participants), reasons for attrition or exclusion where reported, and whether missing data were balanced across groups or were related to outcomes. Where sufficient information was reported, or could be supplied by the trial authors, we re‐included missing data in the analyses which we undertook.
We assessed methods as:
low risk of bias (20% or less missing data);
high risk of bias (e.g. more than 20% missing data; numbers or reasons for missing data imbalanced across groups; ‘as treated’ analysis done with substantial departure of intervention received from that assigned at randomisation);
unclear risk of bias.
(5) Selective reporting bias
We described for each included study how we investigated the possibility of selective outcome reporting bias and what we found.
We assessed the methods as:
low risk of bias (where it is clear that all of the study’s pre‐specified outcomes and all expected outcomes of interest to the review have been reported);
high risk of bias (where not all the study’s pre‐specified outcomes have been reported; one or more reported primary outcomes were not pre‐specified; outcomes of interest are reported incompletely and so cannot be used; study fails to include results of a key outcome that would have been expected to have been reported);
unclear risk of bias.
(6) Other bias (checking for bias due to problems not covered by (1) to (5) above)
We described for each included study any important concerns we have about other possible sources of bias.
We assessed whether each study was free of other problems that could put it at risk of bias:
low risk of other bias;
high risk of other bias;
unclear whether there is risk of other bias.
(7) Overall risk of bias
We made explicit judgements about whether studies were at high risk of bias, according to the criteria given in the Handbook (Higgins 2011). With reference to (1) to (6) above, we assessed the likely magnitude and direction of the bias and whether we considered it was likely to impact on the findings. We explored the impact of the level of bias through undertaking sensitivity analyses ‐ seeSensitivity analysis.
Assessment of the quality of the evidence using the GRADE approach
For this update, we assessed the quality of the evidence using the GRADE approach as outlined in the GRADE handbook in order to assess the quality of the body of evidence relating to the outcomes listed below for the main comparisons: types of pushing: spontaneous pushing versus directed pushing (with or without epidural analgesia) and timing of pushing: delayed pushing versus immediate pushing (all women with epidural).
The following outcomes were included in the 'Summary of findings´ tables' (Table 1; Table 2):
Duration of second stage (minutes)
Perineal laceration (3rd or 4th degree)
Admission to neonatal intensive care
Hypoxic ischaemic encephalopathy
Five‐minute Apgar score less than seven
Duration of pushing (minutes)
Spontaneous vaginal delivery
We used the GRADEpro Guideline Development Tool to import data from Review Manager 5.3 (RevMan 2014) in order to create ’Summary of findings’ tables. A summary of the intervention effect and a measure of quality for each of the above outcomes was produced using the GRADE approach. The GRADE approach uses five considerations (study limitations, consistency of effect, imprecision, indirectness and publication bias) to assess the quality of the body of evidence for each outcome. The evidence can be downgraded from 'high quality' by one level for serious (or by two levels for very serious) limitations, depending on assessments for risk of bias, indirectness of evidence, serious inconsistency, imprecision of effect estimates or potential publication bias.
Measures of treatment effect
Dichotomous data
For dichotomous data, we present results as summary risk ratio with 95% confidence intervals.
Continuous data
For continuous data, we used the mean difference if outcomes were measured in the same way between trials. We planned to use the standardised mean difference to combine trials that measured the same outcome, but used different methods. For the studies that reported medians and ranges for continuous data, we estimated means and standard deviations through the method proposed by Hozo (Hozo 2005).
Unit of analysis issues
Cluster‐randomised trials
We did not identify any cluster‐randomised trials for inclusion in this version of the review. If we identify any cluster‐randomised trials in future updates, we will include cluster‐randomised trials in the analyses along with individually‐randomised trials. We will adjust their sample sizes using the methods described in the Handbook [Section 16.3.4 or 16.3.6] using an estimate of the intracluster correlation co‐efficient (ICC) derived from the trial (if possible), from a similar trial or from a study of a similar population. If we use ICCs from other sources, we will report this and conduct sensitivity analyses to investigate the effect of variation in the ICC. If we identify both cluster‐randomised trials and individually‐randomised trials, we plan to synthesise the relevant information. We will consider it reasonable to combine the results from both if there is little heterogeneity between the study designs and the interaction between the effect of intervention and the choice of randomisation unit is considered to be unlikely.
We will also acknowledge heterogeneity in the randomisation unit and perform a sensitivity analysis to investigate the effects of the randomisation unit.
Cross‐over trials
Cross‐over trials are not eligible for inclusion because we consider this is not an adequate study design to verify the efficacy of this kind of intervention. There is no time for a trustful washout period, hence this period would be contaminated by the other intervention and the results would not be reliable.
Dealing with missing data
For included studies, we noted the levels of attrition. We explored the impact of including studies with high levels of missing data in the overall assessment of treatment effect by using sensitivity analysis.
For all outcomes, we carried out analyses, as far as possible, on an intention‐to‐treat basis, i.e. we attempted to include all participants randomised to each group in the analyses, and all participants were analysed in the group to which they were allocated, regardless of whether or not they received the allocated intervention. The denominator for each outcome in each trial was the number randomised minus any participants whose outcomes were known to be missing.
Assessment of heterogeneity
We assessed statistical heterogeneity in each meta‐analysis using the T², I² and Chi² statistics. We regarded heterogeneity as substantial if an I² was greater than 30% and either a T² was greater than zero, or there was a low P value (less than 0.10) in the Chi² test for heterogeneity. We used a random‐effects meta‐analysis as an overall summary, if this was considered appropriate.
Assessment of reporting biases
If there were 10 or more studies in the meta‐analysis, we planned to investigate reporting biases (such as publication bias) using funnel plots. We planned to assess funnel plot asymmetry visually. If asymmetry was suggested by a visual assessment, we planned to perform exploratory analyses to investigate it.
Where we suspected reporting bias, we contacted study authors, whenever possible, to ask them to provide missing outcome data. Where this was not possible, and the missing data were thought to introduce serious bias, we have explored the impact of including such studies in the overall assessment of results by sensitivity analysis.
Data synthesis
We carried out statistical analysis using the Review Manager software (RevMan 2014). We used fixed‐effect meta‐analysis for combining data where it was reasonable to assume that studies were estimating the same underlying treatment effect: i.e. where trials examined the same intervention, and we judged that the trials’ populations and methods were sufficiently similar. If there was clinical heterogeneity sufficient to expect that the underlying treatment effects differed between trials, or if substantial statistical heterogeneity was detected, we used random‐effects meta‐analysis to produce an overall summary, if an average treatment effect across trials was considered clinically meaningful. The random‐effects summary was treated as the average range of possible treatment effects and we discuss the clinical implications of treatment effects differing between trials. If the average treatment effect was not clinically meaningful, we did not combine trials.
Where we used random‐effects analyses, the results are presented as the average treatment effect with 95% confidence intervals, and the estimates of T² and I².
Subgroup analysis and investigation of heterogeneity
When we identified substantial heterogeneity, we investigated it using subgroup analyses and sensitivity analyses. We considered whether an overall summary was meaningful, and if it was, we used random‐effects analysis to produce it.
We planned to carry out subgroup analysis by use of epidural analgesia in situ or not (including discontinuation of epidural analgesia) for the maternal and neonatal primary outcomes, but this was not possible.
We also carried a subgroup analysis by parity (nulliparous (primigravida) and multiparous with or without epidural analgesia) for three maternal outcomes (duration of the second stage of labour, duration of pushing, and spontaneous vaginal delivery).
For fixed‐effect inverse variance meta‐analyses, we assessed differences between subgroups by interaction tests. For random‐effects and fixed‐effect meta‐analyses using methods other than inverse variance, we assessed differences between subgroups by inspection of the subgroups’ confidence intervals; non‐overlapping confidence intervals indicate a statistically significant difference in treatment effect between the subgroups.
Sensitivity analysis
We planned to carry out a sensitivity analysis to explore the effects of fixed‐effect or random‐effects analyses for outcomes with statistical heterogeneity, but instead used random‐effects analysis where we identified substantial heterogeneity. We carried out sensitivity analyses to explore the effect of trial quality (excluding quasi‐RCTs, and trials assessed to be at high risk of bias for random sequence generation or allocation concealment) for the primary outcome, duration of the second stage of labour, and for the secondary outcome, duration of pushing because of the high heterogeneity found. Lam 2010, Maresh 1983 and Yildirim 2008 were excluded for being at high risk of selection bias.
We performed other sensitivity analyses to explore the effect of possible errors in the estimates of the mean and standard deviations of the trials that reported the continuous data in median and range (Fitzpatrick 2002; Fraser 2000b; Plunkett 2003; Vause 1998) (excluding trials reporting median and ranges) for the primary outcome, duration of the second stage and the secondary outcome duration of pushing.
In future updates, if we include cluster‐randomised trials in meta‐analysis with individually‐randomised trials, we will carry out a sensitivity analysis in order to investigate the effect of the randomisation unit.
Results
Description of studies
Results of the search
The search of the Cochrane Pregnancy and Childbirth Group's Trials Register retrieved 64 trial reports and we identified a further four reports from reference lists of retrieved studies (Chang 2011; Gleeson 1991; Lai 2009; Yeates 1984) (see: Figure 1). We included 21 studies (42 reports) and excluded 22 studies (24 reports). Two trials are ongoing (Cahill 2014; Hauspurg 2014).
1.
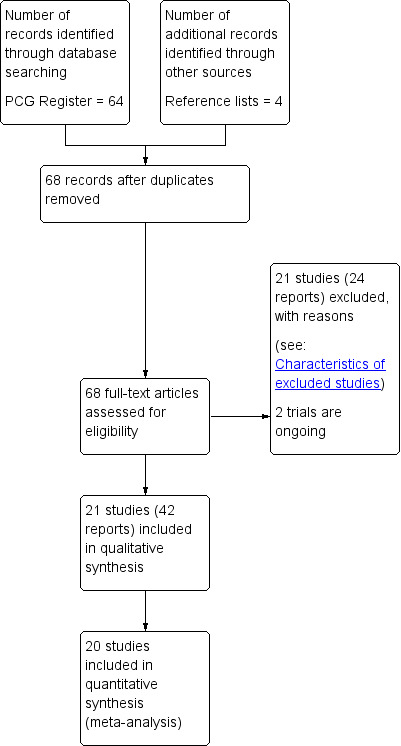
Study flow diagram.
Included studies
This updated review now has 21 included studies.
Eight trials (Jahdi 2011; Knauth 1986; Lam 2010; Low 2013; Schaffer 2005; Thomson 1993;Vaziri 2016; Yildirim 2008) compared the types of pushing and 13 trials (Buxton 1988; Fitzpatrick 2002; Fraser 2000b; Gillesby 2010; Goodfellow 1979; Hansen 2002; Kelly 2010; Maresh 1983; Mayberry 1999; Plunkett 2003; Ravindran 1981; Simpson 2005; Vause 1998) compared the timing of pushing.
One included trial (Ravindran 1981) did not contribute data to our analysis because it did not report on the outcomes of interest in this review.
Some of the included studies assessed the types of pushing, whilst others evaluated the timing of pushing. Consequently, we carried out two separate comparisons.
Comparison 1: Types of pushing: spontaneous pushing versus directed pushing (with or without epidural analgesia)
Comparison 2: Timing of pushing: delayed pushing versus immediate pushing (all women with epidural)
Comparison 1: Types of pushing: spontaneous pushing versus directed pushing (with or without epidural analgesia)
For the eight trials comparing the types of pushing, the women involved (884 women) were low‐risk nulliparous (Knauth 1986; Lam 2010; Low 2013; Schaffer 2005; Vaziri 2016), or primiparous (Jahdi 2011; Thomson 1993; Yildirim 2008), and multiparous (Jahdi 2011), with a singleton fetus in cephalic presentation between 39 and 40 weeks of gestation.
The women's age ranged between 18 and 40 years old and there was no use of epidural analgesia during labour in seven trials (Jahdi 2011; Knauth 1986; Lam 2010; Schaffer 2005; Thomson 1993; Vaziri 2016; Yildirim 2008). One trial (Low 2013) used epidural, but not all women made use of this option.
The studies were conducted in different countries: United States of America (USA) (Knauth 1986; Low 2013; Schaffer 2005), Turkey (Yildirim 2008), England (Thomson 1993), Iran (Jahdi 2011; Vaziri 2016) and Hong Kong (Lam 2010).
Seven trials compared spontaneous pushing with direct Valsalva/closed glottis type pushing (Jahdi 2011; Lam 2010; Low 2013; Schaffer 2005; Thomson 1993;Vaziri 2016; Yildirim 2008). One trial (Knauth 1986) compared Valsalva pushing with slow exhalation through pursed lips (see Characteristics of included studies). There were no specific instructions for spontaneous pushing regarding timing and duration of pushing, and the women were encouraged to follow their body sensations and do what comes naturally.
The timing of pushing was reported in three studies (Lam 2010; Schaffer 2005; Yildirim 2008) and this varied between studies. Four studies (Jahdi 2011; Lam 2010; Schaffer 2005; Vaziri 2016) started pushing with the onset of the second stage of labour for the directed group, and for the spontaneous group when the urge to push was felt. One study (Yildirim 2008), started pushing at full dilation and also with the fetal head at least 1+ level in the pelvis for both groups. The other three trials (Knauth 1986; Low 2013; Thomson 1993) did not mention the timing.
The randomisation was done at full dilation in three studies (Jahdi 2011; Lam 2010; Schaffer 2005) and at 6 cm of dilation in one study (Thomson 1993), whereas three trials (Knauth 1986; Vaziri 2016; Yildirim 2008), did not report this information. One trial (Low 2013) randomised the groups during the prenatal visit.
The posture used for labouring down varied among the studies: free option as the women desire (Schaffer 2005), lithotomy (Yildirim 2008), and birthing chair or sitting (Knauth 1986), while the other three trials did not mention the posture used (Lam 2010; Low 2013; Thomson 1993). For one study (Jahdi 2011), besides the method of pushing used, they also included different postures for each arm of the trial. The group coached to a directed pushing assumed the supine position (Jahdi 2011), while the group selected to do the spontaneous pushing used an upright position (standing, sitting and squatting). The last study (Vaziri 2016) also included different postures for each arm of the trial. The spontaneous pushing group used the lateral position and the directed group used the supine position.
Only two trials (Schaffer 2005; Yildirim 2008) reported that they had used oxytocin, but the dosage was not described. One trial (Schaffer 2005), had used oxytocin after randomisation, and in the other trial (Yildirim 2008), it is not clear when it was used.
The intervention was conducted by certified nurse‐midwives (Low 2013; Schaffer 2005), midwives (Jahdi 2011; Lam 2010; Low 2013; Thomson 1993), nurse, obstetrician, or family medicine physician (Low 2013), and certified childbirth educators (Knauth 1986). Two trials did not mention this aspect of the methods (Vaziri 2016; Yildirim 2008). Three trials (Knauth 1986; Low 2013; Schaffer 2005), included training for the team responsible for the intervention in the labour ward, while the others five trials (Jahdi 2011; Lam 2010; Thomson 1993; Vaziri 2016; Yildirim 2008), did not mention any training sessions.
In one study (Low 2013), the spontaneous group received a video that provided instructions on the breathing technique, but in the remainder of the trials it is not stated that the women receive prenatal education about how to push.
One study (Schaffer 2005), derived two reports, one published in 2006 (Bloom 2006) showed the obstetrical outcomes, and the other one, published in 2005 (Schaffer 2005b), was a three‐month follow‐up to determine the effect of a direct pushing on the urogynaecologic measures and pelvic floor structure and function.
Low 2013 compared the effect of spontaneous pushing (either with or without prenatal perineal massage) with directed pushing (with and without prenatal massage) and involved four groups. Therefore, we considered the two groups (spontaneous versus directed without perineal massage). This study published another report with one‐year follow‐up on the presence or not of fecal incontinence (Brincat 2009), and a secondary analysis based on audio tapes designated women into spontaneous pushing or directed pushing groups based on the actual pushing method which was not used in the results.
Comparison 2: Timing of pushing: delayed pushing versus immediate pushing (all women with epidural analgesia)
The 12 trials comparing timing of pushing and that contributed to the data analysis involved 2879 women. The sample was nulliparous (Fraser 2000b; Gillesby 2010; Goodfellow 1979; Kelly 2010; Maresh 1983; Mayberry 1999; Plunkett 2003; Simpson 2005; Vause 1998), primiparous (Fitzpatrick 2002), or nulliparous and multiparous (Buxton 1988; Hansen 2002), with a singleton fetus in cephalic presentation, between 36 and 42 weeks of gestation. The age ranged between 17 to 40 years old.
The studies were from different countries: USA (Buxton 1988; Gillesby 2010; Hansen 2002; Kelly 2010; Mayberry 1999; Plunkett 2003; Simpson 2005), England (Goodfellow 1979; Vause 1998), Ireland (Fitzpatrick 2002), Malaysia (Maresh 1983), and there was one multicentre trial (Fraser 2000b) involving three countries: USA, Canada and Switzerland that resulted in two reports, one aimed to determine the efficacy of delayed pushing for nulliparous with epidural analgesia on the risk of difficult delivery (Fraser 2000a), and the other aimed to estimate the economic efficiency of this policy of delayed pushing with the same sample (Petrou 2000).
All the trials had used epidural analgesia and compared an immediate pushing technique versus delayed pushing. The immediate group began pushing after the cervix was identified as being completely dilated and the time for the delayed group to start pushing varied among the studies. The delay for the onset of pushing was until the woman experienced an irresistible urge to push, or to one, two or three hours (see Characteristics of included studies). The randomisation process was conducted upon diagnosis of full dilation in five studies (Fitzpatrick 2002; Fraser 2000b; Gillesby 2010; Goodfellow 1979; Simpson 2005), before complete dilation in two studies (Kelly 2010; Mayberry 1999), and either the first or within the first hour of the start of the second stage (Vause 1998); the other four trials (Buxton 1988; Hansen 2002; Maresh 1983; Plunkett 2003) did not report this information.
In relation to the type of pushing used, eight studies (Buxton 1988; Fitzpatrick 2002; Fraser 2000b; Goodfellow 1979; Gillesby 2010; Maresh 1983; Plunkett 2003; Vause 1998), did not report this. Three trials provided this information. One trial used a closed glottis (Hansen 2002), two used both closed and open glottis (Kelly 2010), or breath holding no longer than six to eight seconds (Mayberry 1999). One trial (Simpson 2005), divided the type of pushing according to the group, whilst the immediate group bore down with a Valsalva type pushing; the delayed group used an open‐glottis breath.
All the trials comparing timing of pushing used analgesia. Different doses and schemes of epidural analgesia were used, but only six trials described the epidural dosage used (0.125% or 0.12 mg to 0.25 mg or 4 mL to 10 mL of 0.25% and occasionally 0.35% or 0.5%) of bupivacaine and 2 ug/mL of fentanyl to a rate of 6 mL/hr to 12 mL/hr (Fraser 2000b; Goodfellow 1979; Kelly 2010; Mayberry 1999; Plunkett 2003; Simpson 2005), while the others six studies did not report the dosage (Buxton 1988; Fitzpatrick 2002; Gillesby 2010; Hansen 2002; Maresh 1983; Vause 1998).
The description of oxytocin used among trials was confusing. Nine trials (Buxton 1988; Fitzpatrick 2002; Fraser 2000b; Gillesby 2010; Goodfellow 1979; Kelly 2010; Maresh 1983; Simpson 2005; Vause 1998) reported oxytocin use. Five trials (Buxton 1988; Fitzpatrick 2002; Fraser 2000b; Simpson 2005; Vause 1998) reported the time this medication was used (first and/or second stage), but this was not clear in the other two trials (Kelly 2010; Maresh 1983). One trial (Goodfellow 1979), used oxytocin only in the treatment group, and an other trial (Simpson 2005) reported oxytocin use for all women in both groups. In one trial (Gillesby 2010), we contacted the authors and they provided this information, stating that oxytocin was either used in the first or second stage.
The posture used during labouring down was described in only five trials and varied between studies: no limit to changing position (Gillesby 2010; Kelly 2010), sitting or lateral position for the intervention group (Buxton 1988; Simpson 2005), lateral or decubitos position for both groups (Hansen 2002). The other seven studies (Fitzpatrick 2002; Fraser 2000b; Goodfellow 1979; Maresh 1983; Mayberry 1999; Plunkett 2003; Vause 1998), did not mention the posture used by the women. The intervention was conducted by nurse or physician (Gillesby 2010; Hansen 2002; Maresh 1983; Mayberry 1999; Simpson 2005; Vause 1998), and midwives (Fitzpatrick 2002; Goodfellow 1979), and four trials did not describe who assisted the woman at the labour (Buxton 1988; Fraser 2000b; Kelly 2010; Plunkett 2003). Only one trial (Kelly 2010), referred to training of the health team responsible for the pushing orientation.
None of the women in the included studies had received prenatal education about how to push.
Excluded studies
We excluded 22 trials (24 reports). Ten studies were not randomised controlled trials (RCTs) (Barnett 1982; Caldeyro Barcia 1990; Chang 2011; Gleeson 1991; Haseeb 2014; Lai 2009; Martinez Lopez 1984; Mc Queen 1977; Parnell 1993; Yeates 1984), and four were trial registrations for trials that do not appear to have been completed (Liston 1987; Mulvey 2008; Snyder 1996; Spiby 1990). Two were published in abstract form only (Boulvain 1998; Pickrell 1989), two trials used different interventions to those considered in this review (Matsuo 2009; Phipps 2009), one trial compared different positions and did not report the pushing method used in the groups (Moraloglu 2016), another trial (Aviram 2016), aimed to determine the effect of a dental support device on the course of labour and delivery (it did not report the type of pushing used), and in the Walker 2012 study, the same intervention was used in both study arms.
Risk of bias in included studies
For a summary of the risk of bias for the included studies, see Figure 2 and Figure 3.
2.
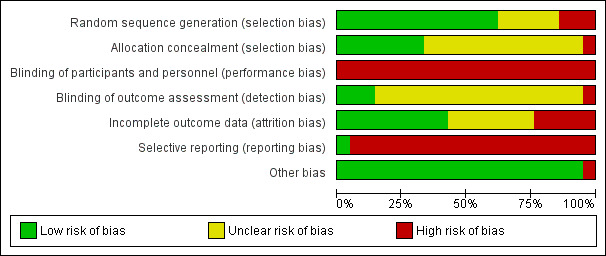
'Risk of bias' graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
3.
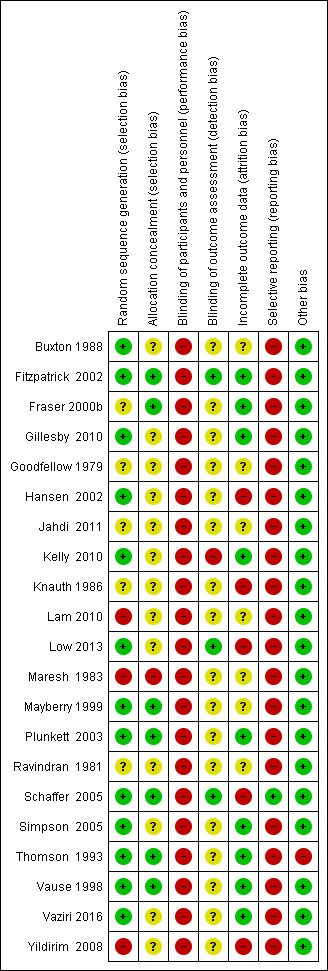
'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Sequence generation
Comparison 1: Types of pushing: spontaneous pushing versus directed pushing (with or without epidural analgesia)
We considered that the randomisation process was adequate in only four trials (Low 2013; Schaffer 2005; Thomson 1993; Vaziri 2016). Two trials (Lam 2010; Yildirim 2008) were considered to be at a high risk of bias as only envelopes were described as being used for randomisation. We classified two trials (Jahdi 2011; Knauth 1986) as unclear as there was no information on the method used for random generation.
Comparison 2: Timing of pushing: delayed pushing versus immediate pushing (all women with epidural analgesia)
The randomisation sequence generation was adequate for nine trials (Buxton 1988; Fitzpatrick 2002; Gillesby 2010; Hansen 2002; Kelly 2010; Mayberry 1999; Plunkett 2003; Simpson 2005; Vause 1998). One trial (Maresh 1983), was assessed as having a high risk of bias because we considered the method used to be inadequate (odd and even hospital numbers) (Maresh 1983).
One trial (Fraser 2000b), despite reporting "randomisation was centralized", it was not clear how the sequence generation was done and therefore, it was classified as unclear risk of bias. Similarly, Goodfellow 1979 only reported that women were 'randomly allocated' and no further information was provided so this study was also assessed as having an unclear risk of selection bias.
Allocation concealment
Comparison 1: Types of pushing: spontaneous pushing versus directed pushing (with or without epidural analgesia)
For the seven trials comparing the types of pushing, adequate allocation concealment was described in only two trials (Schaffer 2005; Thomson 1993), and in the other six studies (Jahdi 2011; Knauth 1986; Lam 2010; Low 2013; Vaziri 2016Yildirim 2008), concealment of allocation was not described (unclear risk of selection bias).
Comparison 2: Timing of pushing: delayed pushing versus immediate pushing (all women with epidural analgesia)
For the trials comparing the timing of pushing, there was description of an adequate allocation concealment in five studies (Fitzpatrick 2002; Fraser 2000b; Mayberry 1999; Plunkett 2003; Vause 1998). For six trials (Buxton 1988; Gillesby 2010; Goodfellow 1979; Hansen 2002; Kelly 2010; Simpson 2005), it was 'unclear' if there was adequate allocation concealment, and one trial (Maresh 1983), we rated as high risk of bias as it was a quasi‐randomisation trial.
Blinding
Blinding of the participants and personnel
None of the trials included in this review blinded the participants and personnel and all trials were rated as 'high risk' of performance bias.
Blinding of the outcome assessors
Comparison 1: Types of pushing: spontaneous pushing versus directed pushing (with or without epidural analgesia)
Two studies reported that outcome assessors were blinded (Low 2013; Schaffer 2005). All the others studies did not mention whether the outcome assessors were blinded and were thus considered to be at an unclear risk of detection bias (Jahdi 2011; Knauth 1986; Lam 2010; Thomson 1993; Vaziri 2016; Yildirim 2008).
Comparison 2: Timing of pushing: delayed pushing versus immediate pushing (all women with epidural analgesia)
Of the 12 trials included, 10 (Buxton 1988; Fraser 2000b; Gillesby 2010; Goodfellow 1979; Hansen 2002; Maresh 1983; Mayberry 1999; Plunkett 2003; Simpson 2005; Vause 1998) did not mention blinding of the outcome assessors, and we considered them 'unclear' for this domain. The other two trials (Fitzpatrick 2002; Kelly 2010), described that the investigators were blinded for the assessment of specific outcomes. Fitzpatrick 2002 was assessed as of low risk because most outcomes were blinded to assessors; in Kelly 2010, most outcomes were not blinded, and so this trial was assessed as of high risk of bias.
Incomplete outcome data
Comparison 1: Types of pushing: spontaneous pushing versus directed pushing (with or without epidural analgesia)
For the trials comparing types of pushing, only two trials (Thomson 1993; Vaziri 2016) were at a low risk of attrition bias. Four trials were at high risk of bias (Knauth 1986; Low 2013; Schaffer 2005; Yildirim 2008). In one trial (Jahdi 2011), it was not clear if there were losses or changes between groups, and in the other trial (Lam 2010), it was not clear how many women were lost after randomisation.
One trial (Low 2013), had an 41% of attrition bias for the 12‐month follow‐up.
Comparison 2: Timing of pushing: delayed pushing versus immediate pushing (all women with epidural analgesia)
Seven trials (Fitzpatrick 2002; Fraser 2000b; Gillesby 2010; Kelly 2010; Plunkett 2003; Simpson 2005; Vause 1998), were classified as low risk for this bias and two of them carried out intention‐to‐treat analysis (Gillesby 2010; Kelly 2010).
Four trials (Buxton 1988; Goodfellow 1979; Maresh 1983; Mayberry 1999), did not describe losses or dropouts, therefore it is not clear if there was bias or not and they were classified as unclear risk of bias.
One trial (Hansen 2002), had almost 20% of losses and was thus categorised as high risk of bias.
Selective reporting
Comparison 1: Types of pushing: spontaneous pushing versus directed pushing (with or without epidural analgesia)
We classified one study (Schaffer 2005) as low risk of bias for selective reporting. The other six studies (Jahdi 2011; Knauth 1986; Lam 2010; Thomson 1993; Vaziri 2016; Yildirim 2008), we rated as high risk because they did not report important outcomes, also some of the outcomes of interest in this review were reported incompletely such that some of the data could not be entered in the meta‐analysis.
One trial (Low 2013) was assessed as being at high risk of reporting bias. The study aimed to test the effect of spontaneous pushing on incontinence outcomes at one year after the birth of the woman's first birth. Birth data (including perineal lacerations and episiotomy) were reported for the study population overall but data were not reported by treatment group. A table reporting 'obstetric characteristics by treatment condition' is restricted to the following outcomes: epidural; second stage length; delivery method (vaginal/caesarean section).
Comparison 2: Timing of pushing: delayed pushing versus immediate pushing (all women with epidural analgesia)
There was a high risk of bias for all 12 trials (Buxton 1988; Fitzpatrick 2002; Fraser 2000b; Gillesby 2010; Goodfellow 1979; Hansen 2002; Kelly 2010; Maresh 1983; Mayberry 1999; Plunkett 2003; Simpson 2005; Vause 1998), comparing timing of pushing because most of the outcomes of interest in the review were reported incompletely and as a result, data could not be entered in the meta‐analysis. In addition, other important outcomes were not reported.
Other potential sources of bias
No other potential sources of bias was found for almost all of studies. Only one study (Thomson 1993), from Comparison 1 (types of pushing: spontaneous pushing versus directed pushing ‐ with or without epidural analgesia) reported that the main author from the study was present for all second stages "to ensure reliability of group allocation" and therefore this could be an interference.
Effects of interventions
Comparison 1: Types of pushing: spontaneous pushing versus directed pushing (with or without epidural analgesia)
Selected outcomes have been downgraded using the GRADE approach. See Table 1 for further details.
Primary outcomes
Maternal outcomes
1. Duration of the second stage (minutes)
Data from six trials (Lam 2010; Low 2013; Schaffer 2005; Thomson 1993; Vaziri 2016; Yildirim 2008) of nulliparous women, showed no clear difference in the duration of the second stage (mean difference (MD) 10.26 minutes; 95% confidence interval (CI) ‐1.12 to 21.64; six studies, 667 women, random‐effects: I² = 81%; very low‐quality evidence;Analysis 1.1) between spontaneous and directed pushing. The overall result comes from a meta‐analysis with substantial heterogeneity. This outcome was downgraded to very low‐quality of evidence because of very serious study limitations, high heterogeneity and wide confidence intervals crossing the line of no effect (see Table 1).
1.1. Analysis.
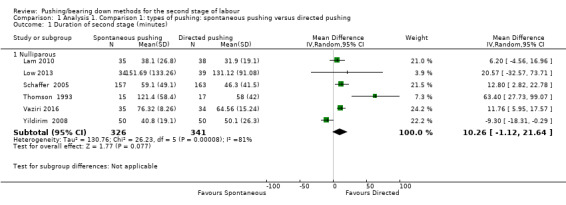
Comparison 1 Analysis 1. Comparison 1: types of pushing: spontaneous pushing versus directed pushing, Outcome 1 Duration of second stage (minutes).
A sensitivity analysis was performed for this outcome. Lam 2010 and Yildirim 2008 were excluded for inadequate random sequence generation. These results are documented below (Analysis 1.17).
1.17. Analysis.
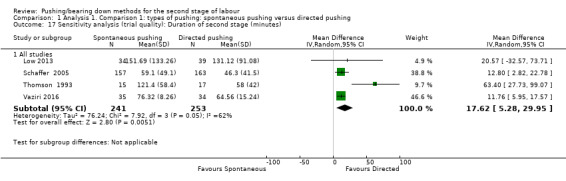
Comparison 1 Analysis 1. Comparison 1: types of pushing: spontaneous pushing versus directed pushing, Outcome 17 Sensitivity analysis (trial quality): Duration of second stage (minutes).
2. Perineal laceration (3rd and 4th degree)
The overall evidence from one study (Schaffer 2005), involving 320 women, shows that there is no clear difference in the risk of perineal trauma (3rd and 4th degree tears) between the use of spontaneous pushing compared to directed pushing (risk ratio (RR) 0.87; 95% CI 0.45 to 1.66; one study; 320 women;low‐quality evidence; Analysis 1.2).
1.2. Analysis.
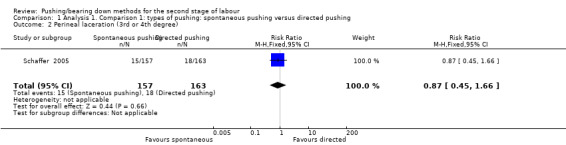
Comparison 1 Analysis 1. Comparison 1: types of pushing: spontaneous pushing versus directed pushing, Outcome 2 Perineal laceration (3rd or 4th degree).
3. Episiotomy
Two studies contributed to this analysis (Schaffer 2005; Yildirim 2008); the final result showed no clear difference in the risk of episiotomy between groups (average RR 1.05; 95% CI 0.60 to 1.85; 420 women; random‐effects; I² = 81%; Analysis 1.3).
1.3. Analysis.
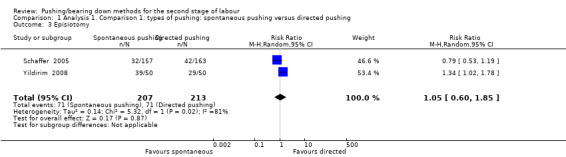
Comparison 1 Analysis 1. Comparison 1: types of pushing: spontaneous pushing versus directed pushing, Outcome 3 Episiotomy.
Neonatal outcomes
1. Admission to neonatal intensive care
Two studies (Lam 2010; Schaffer 2005), reported this outcome and there was no difference between groups (RR 1.08, 95% CI 0.30 to 3.79; 393 infants; I² = 0%;very low‐quality evidence;Analysis 1.4).
1.4. Analysis.
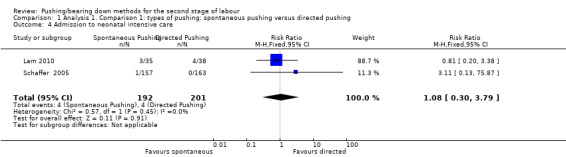
Comparison 1 Analysis 1. Comparison 1: types of pushing: spontaneous pushing versus directed pushing, Outcome 4 Admission to neonatal intensive care.
2. Hypoxic ischaemic encephalopathy
None of the included studies reported on this outcome.
3. Five‐minute Apgar score less than seven
Only one trial (Schaffer 2005), reported this outcome as a binary variable and there was no difference between groups (RR 0.35; 95% CI 0.01 to 8.43; 320 infants; very low‐quality evidence;Analysis 1.5). Data were also reported in another trial (Yildirim 2008), but as mean and standard deviation, which could not be incorporated into our meta‐analysis.
1.5. Analysis.
Comparison 1 Analysis 1. Comparison 1: types of pushing: spontaneous pushing versus directed pushing, Outcome 5 Five‐minute Apgar score < seven.
Secondary outcomes
Maternal outcomes
1. Duration of pushing (outcome not pre‐specified in our published protocol)
Two trials (Vaziri 2016; Yildirim 2008), reported this outcome and the result showed no clear difference between groups (MD ‐9.76 minutes; 95% CI ‐19.54 to 0.02, two studies, 169 women; random‐effects; I² = 88%; T² = 43.98; P < 0.005; Analysis 1.6). This outcome was downgraded to very low‐quality of evidence because of serious study limitations, serious imprecision (null effect) and serious inconsistency (Table 1).
1.6. Analysis.
Comparison 1 Analysis 1. Comparison 1: types of pushing: spontaneous pushing versus directed pushing, Outcome 6 Duration of pushing (minutes).
A sensitivity analysis was performed for this outcome, excluding Yildirim 2008, because of inadequate random sequence generation. These results are documented below (Analysis 1.18).
1.18. Analysis.
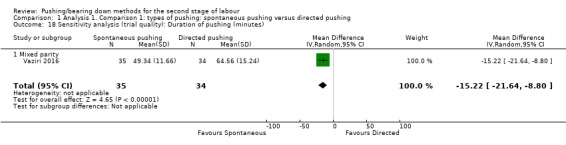
Comparison 1 Analysis 1. Comparison 1: types of pushing: spontaneous pushing versus directed pushing, Outcome 18 Sensitivity analysis (trial quality): Duration of pushing (minutes).
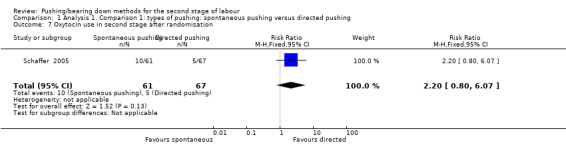
2. Oxytocin use in the second stage after randomisation
Only one study (Schaffer 2005), reported this outcome and there was no clear difference between the pushing groups in the risk of this outcome (RR 2.20, 95% CI 0.80 to 6.07; 128 women; Analysis 1.7).
1.7. Analysis.
Comparison 1 Analysis 1. Comparison 1: types of pushing: spontaneous pushing versus directed pushing, Outcome 7 Oxytocin use in second stage after randomisation.
3. Spontaneous vaginal delivery
Five trials (Schaffer 2005; Jahdi 2011; Lam 2010; Low 2013; Thomson 1993), reported this outcome and there was no clear difference in the risk of spontaneous vaginal delivery between groups (RR 1.01; 95% CI 0.97 to 1.05; five studies; 688 women; moderate‐quality evidence;Analysis 1.8).
1.8. Analysis.

Comparison 1 Analysis 1. Comparison 1: types of pushing: spontaneous pushing versus directed pushing, Outcome 8 Spontaneous vaginal delivery.
4. Instrumental delivery
Two studies (Lam 2010; Schaffer 2005) reported this outcome. There was no clear difference in the risk of instrumental delivery between spontaneous pushing and directed pushing groups (average RR 0.56; 95% CI 0.06 to 5.10; 393 women; random‐effects; I² = 57%; Analysis 1.9).
1.9. Analysis.
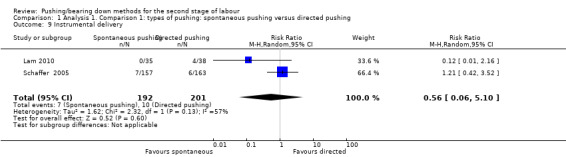
Comparison 1 Analysis 1. Comparison 1: types of pushing: spontaneous pushing versus directed pushing, Outcome 9 Instrumental delivery.
5.Rotational or midpelvic or posterior forceps
No studies provided data for this analysis.
6. Caesarean delivery
Three trials (Jahdi 2011; Low 2013; Schaffer 2005), reported this outcome and showed no clear difference in the risk of caesarean delivery between groups (average RR 0.79; 95% CI 0.14 to 4.39; 583 women; random‐effects; I² = 64%; Analysis 1.10).
1.10. Analysis.
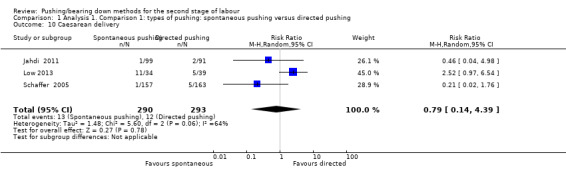
Comparison 1 Analysis 1. Comparison 1: types of pushing: spontaneous pushing versus directed pushing, Outcome 10 Caesarean delivery.
7. Maternal hypertension
No trials reported maternal hypertension as an outcome.
8. Postpartum haemorrhage
No trials report postpartum haemorrhage as a binary variable. Only two trials (Lam 2010; Thomson 1993) reported "estimated blood loss" but data were expressed as a continuous variable and so could not be combined in meta‐analysis.
9. Maternal report of severe pain in second stage
Maternal report of severe pain in second stage was not reported by these trials.
10. Fatigue after delivery (outcome not pre‐specified in our published protocol)
Two trials (Lam 2010; Vaziri 2016), measured this outcome using a visual analogue scale (VAS). There was no clear difference between groups (standardised mean difference (SMD) ‐1.14, 95% CI ‐3.29 to 1.02; random‐effects; 142 women; I² = 97%; Analysis 1.11).
1.11. Analysis.
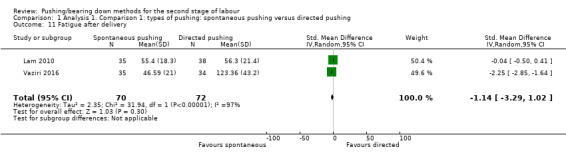
Comparison 1 Analysis 1. Comparison 1: types of pushing: spontaneous pushing versus directed pushing, Outcome 11 Fatigue after delivery.
11. Maternal satisfaction (outcome not pre‐specified in our published protocol)
Only one trial (Thomson 1993), reported this outcome (measured using a VAS) and reported there was no clear difference (MD 0.91; 95% CI ‐1.30 to 3.12; 31 women; Analysis 1.12).
1.12. Analysis.
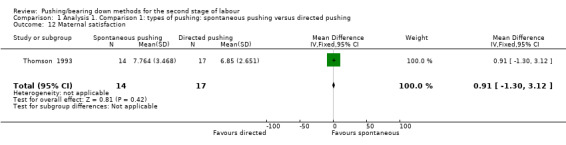
Comparison 1 Analysis 1. Comparison 1: types of pushing: spontaneous pushing versus directed pushing, Outcome 12 Maternal satisfaction.
12. Perineal pain
No trials reported data for perineal pain.
13. Dyspareunia
No trials reported data for dyspareunia.
14. Urinary incontinence
Urodynamic stress incontinence was reported by one trial (Schaffer 2005). The results showed no clear difference in urinary incontinence between groups (RR 0.70, 95% CI 0.29 to 1.69; 128 women; Analysis 1.14).
1.14. Analysis.

Comparison 1 Analysis 1. Comparison 1: types of pushing: spontaneous pushing versus directed pushing, Outcome 14 Urinary stress incontinence.
One trial (Low 2013), reported urinary incontinence 12 months postpartum through the Leakage Index Questionnaire with potential index scores ranged from zero to eight, with larger numbers indicating greater severity of incontinence. The results showed no difference (P = 0.57) between the groups (directed group: mean and SD 2.17 + 2.5 and spontaneous group: mean and SD 1.20 + 1.76).
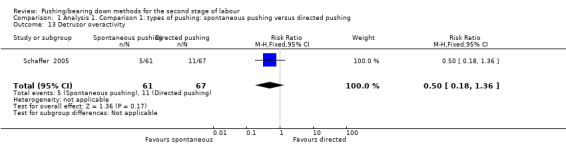
15. Detrusor overactivity (outcome not pre‐specified in our published protocol)
Detrusor overactivity measured by urodynamic testing was reported by one trial (Schaffer 2005); results showed no clear difference in the risk of detrusor overactivity between groups ((RR 0.50, 95% CI 0.18 to 1.36; 128 women; Analysis 1.13).
1.13. Analysis.
Comparison 1 Analysis 1. Comparison 1: types of pushing: spontaneous pushing versus directed pushing, Outcome 13 Detrusor overactivity.
16. Fecal incontinence
Fecal incontinence was reported in a secondary analysis of one study (Low 2013), but the data were analysed only by the presence or not of fecal incontinence one year postpartum, independent of the types of pushing groups. Therefore, there were no available data by each group to inform a meta‐analysis. The results only reported that "the women in the “spontaneous pushing” group were equally likely to have fecal incontinence at 1 year (5%) as those in the other 2 groups (6%) (P=0.985) ".
17. Pelvic floor prolapse
Pelvic floor prolapse was not reported by the trials in this review.
Neonatal outcomes
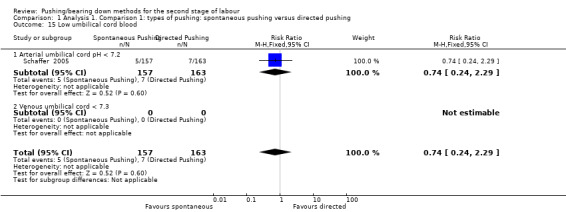
1. Low umbilical cord blood pH
Only one trial (Schaffer 2005) reported this outcome as a binary variable. There was no clear difference between the spontaneous group and the directed pushing group for the risk of umbilical arterial cord pH less than 7.1 (RR 0.74, 95% CI 0.24 to 2.29; 320 women; Analysis 1.15).
1.15. Analysis.
Comparison 1 Analysis 1. Comparison 1: types of pushing: spontaneous pushing versus directed pushing, Outcome 15 Low umbilical cord blood.
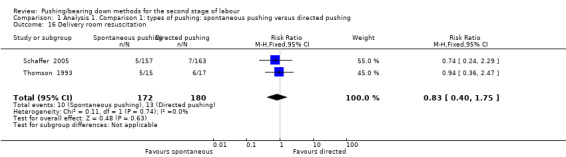
2. Delivery room resuscitation (outcome not pre‐specified in our published protocol)
Only two trials (Schaffer 2005; Thomson 1993) reported delivery room resuscitation and there was no clear difference between the groups (RR 0.83, 95% CI 0.40 to 1.75; 352 women; I² = 0%; Analysis 1.16).
1.16. Analysis.
Comparison 1 Analysis 1. Comparison 1: types of pushing: spontaneous pushing versus directed pushing, Outcome 16 Delivery room resuscitation.
3. Total care costs (outcome not pre‐specified in our published protocol)
For this comparison, none of the included studies reported this outcome.
Sensitivity analysis for comparison 1
Trial quality
Duration of second stage: When we carried out a sensitivity analysis, excluding the quasi‐randomised trials (Lam 2010; Yildirim 2008), there was an increase in the effect size favouring the direct group with a reduced pushing time of about 17 minutes (MD 17.62, 95% CI 5.28 to 29.95; random‐effects; four studies; 494 women; I² = 62%; T² = 76.24; P < 0.05; Analysis 1.17).
Duration of pushing: When we carried out a sensitivity analysis, excluding the quasi‐randomised trial (Yildirim 2008), results showed that the group who pushed spontaneously spent less time (about 15 minutes) on pushing, but results were based on findings from a single trial with a small sample size (MD: ‐15.22 minutes; 95% CI ‐21.64 to ‐8.80; random‐effects; one study; 69 women; Analysis 1.18).
Comparison 2: Timing of pushing: delayed pushing versus immediate pushing (all women with epidural analgesia)
Selected outcomes have been downgraded using the GRADE approach. See Table 2 for further details.
Primary outcomes
Maternal outcomes
1. Duration of the second stage (minutes)
There was an increase in the duration of the second stage of 56.40 minutes with the use of a delayed pushing in labour with epidural analgesia, based on data from 10 trials (Buxton 1988; Fitzpatrick 2002; Fraser 2000b; Gillesby 2010; Kelly 2010; Maresh 1983; Mayberry 1999; Plunkett 2003; Simpson 2005; Vause 1998) (MD 56.40, 95% CI 42.05 to 70.76; 11 trials; 3049 women; random‐effects; I² = 91%; T² = 524.61; very low‐quality evidence; Analysis 2.1).
2.1. Analysis.

Comparison 2 Analysis 2. Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural), Outcome 1 Duration of second stage (minutes).
Subgroup analysis by parity also demonstrated this increase among nulliparous (MD 56.12, 95% CI 39.29 to 72.96; 10 trials; 2885 women; random‐effects; I² = 92%; T² = 627.33; P < 0.00001) (Fraser 2000b; Gillesby 2010; Kelly 2010; Maresh 1983; Mayberry 1999; Plunkett 2003; Simpson 2005; Vause 1998; Fitzpatrick 2002; Hansen 2002); and multiparous women (MD 38.80 minutes; 95% CI 29.16 to 48.44; one trial; 123 women ‐ Hansen 2002). This larger effect in the nulliparous subgroup was supported by the interaction test when we performed the test for subgroup differences (Test for subgroups differences: Chi² = 8.19; df = 2; P = 0.02). However, since there is only one study included in both the multiparous and mixed parity subgroups, this result should be interpreted with caution.
A sensitivity analysis was performed for this outcome, excluding the quasi randomised trial, Maresh 1983, from the analysis (see below and Analysis 2.19).
2.19. Analysis.
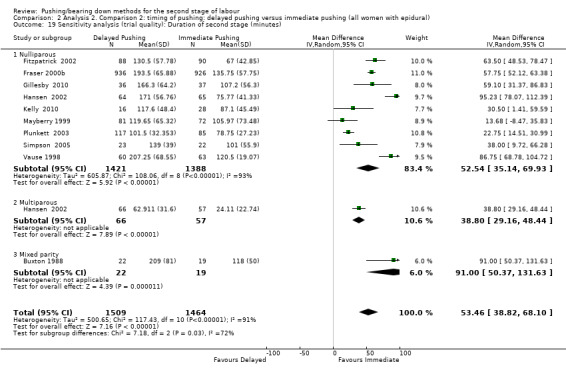
Comparison 2 Analysis 2. Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural), Outcome 19 Sensitivity analysis (trial quality): Duration of second stage (minutes).
We carried out another sensitivity analysis excluding the trials (Fitzpatrick 2002; Fraser 2000b; Plunkett 2003; Vause 1998) where we used a statistical method (Hozo 2005) to estimate means and standard deviations, because these trials reported data as medians and ranges. See below for sensitivity analysis of this outcome (Analysis 2.21).
2.21. Analysis.
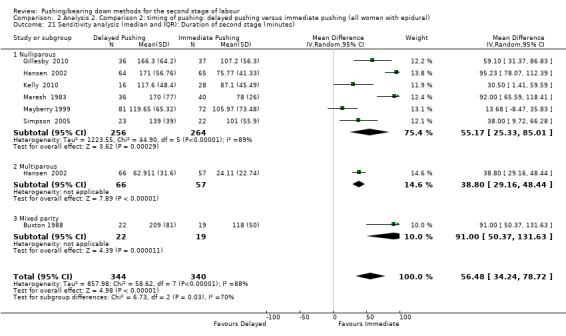
Comparison 2 Analysis 2. Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural), Outcome 21 Sensitivity analysis (median and IQR): Duration of second stage (minutes).
Perineal laceration (3rd and 4th degree)
For seven trials (Fitzpatrick 2002; Fraser 2000b; Gillesby 2010; Hansen 2002; Kelly 2010; Mayberry 1999; Plunkett 2003), there was no clear difference in the risk of perineal laceration (3rd and 4th degree) between the use of delayed pushing compared with immediate pushing (RR 0.94, 95% CI 0.78 to 1.14; seven studies; 2775 women; I² = 0%; moderate‐quality evidence; Analysis 2.2). (Six of the seven studies included in this analysis reported 3rd and 4th degree tears; in one study trialists reported the total number of women with "lacerations" and did not provide separate data for women with more serious trauma (Hansen 2002); temporarily removing this study from the analysis did not cause any substantial change in the results; data not shown.)
2.2. Analysis.
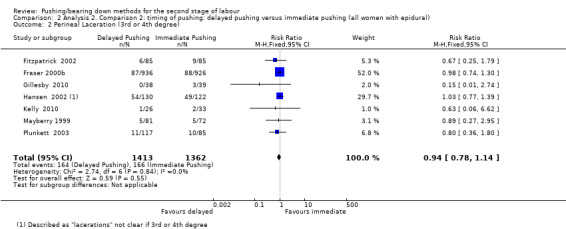
Comparison 2 Analysis 2. Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural), Outcome 2 Perineal Laceration (3rd or 4th degree).
3. Episiotomy
There was no clear difference between groups (RR 0.95; 95% CI 0.87 to 1.04; Analysis 2.3) from five trials (2320 women) (Fitzpatrick 2002;Fraser 2000b; Gillesby 2010; Maresh 1983; Vause 1998).
2.3. Analysis.
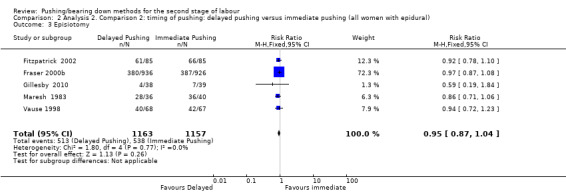
Comparison 2 Analysis 2. Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural), Outcome 3 Episiotomy.
Neonatal outcomes
1. Admission to neonatal intensive care
Three trials (Fraser 2000b; Plunkett 2003; Vause 1998) assessed this outcome; there was no clear difference between groups in admission to neonatal intensive care (RR 0.98, 95% CI 0.67 to 1.41; three studies; 2197 women; I² = 0%; low‐quality evidence; Analysis 2.4).
2.4. Analysis.
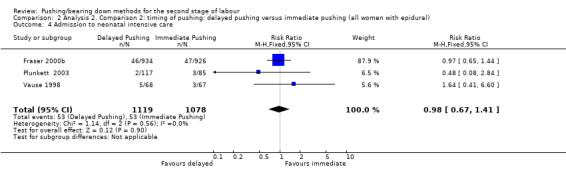
Comparison 2 Analysis 2. Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural), Outcome 4 Admission to neonatal intensive care.
2. Hypoxic ischaemic encephalopathy
None of the included studies reported on this outcome.
3. Five‐minute Apgar score less than seven
Despite three trials (Maresh 1983; Plunkett 2003; Vause 1998) providing data for this meta‐analysis, data from two of the studies (Maresh 1983; Vause 1998), were non‐estimable because the number of events was zero for both groups. The final result was therefore from one trial (Plunkett 2003), and there was no clear difference in the risk of a five‐minute Apgar score less than seven between delayed pushing and immediate pushing (RR 0.15, 95% CI 0.01 to 3.00; three studies; 413 infants; I² = 0%; very low‐quality evidence; Analysis 2.5). Five trials (Gillesby 2010; Hansen 2002; Kelly 2010; Mayberry 1999; Simpson 2005), reported this outcome as means and standard deviations. Wherever possible, we contacted the study authors by e‐mail to get these missing data, with success for one author (Gillesby 2010), who informed us that there were no five‐minute Apgar scores less than seven in both groups.
2.5. Analysis.
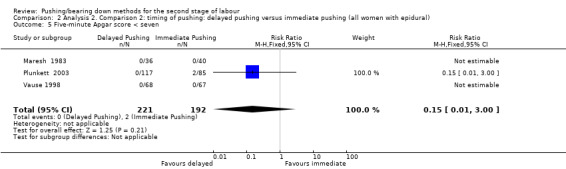
Comparison 2 Analysis 2. Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural), Outcome 5 Five‐minute Apgar score < seven.
Secondary outcomes
Maternal outcomes
1. Duration of pushing (outcome not pre‐specified in our published protocol)
Eleven trials (Buxton 1988; Fitzpatrick 2002; Fraser 2000b; Gillesby 2010; Goodfellow 1979; Hansen 2002; Kelly 2010; Maresh 1983; Vause 1998; Plunkett 2003; Simpson 2005), contributed to this analysis. Compared to spontaneous pushing, delayed pushing was associated with a reduction of 19.05 minutes in the duration of pushing (MD ‐19.05, 95% CI ‐32.27 to ‐5.83; random‐effects; 11 studies; 2932 women; I² = 95%; very low‐quality evidence;Analysis 2.6).
2.6. Analysis.

Comparison 2 Analysis 2. Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural), Outcome 6 Duration of pushing (minutes).
The subgroup analysis shows a slightly larger effect among nulliparous women (MD ‐21.30, 95% CI ‐36.87 to ‐5.73; random‐effects; 10 studies; 2768 women; I² = 96%) (Fitzpatrick 2002; Fraser 2000b; Gillesby 2010; Goodfellow 1979; Hansen 2002; Kelly 2010; Maresh 1983; Plunkett 2003; Simpson 2005; Vause 1998), and less effect for multiparous women (MD ‐11.35, 95% CI ‐18.19 to ‐4.51; random‐effects; one trial; 123 women; (Hansen 2002). Despite the apparent difference between the subgroups, this is not supported by the subgroup interaction test (Chi2 = 1.86; df = 2; P = 0.39).
A sensitivity analysis was performed for this outcome, excluding the quasi‐randomised trial, Maresh 1983, from the analysis (see below and Analysis 2.20).
2.20. Analysis.
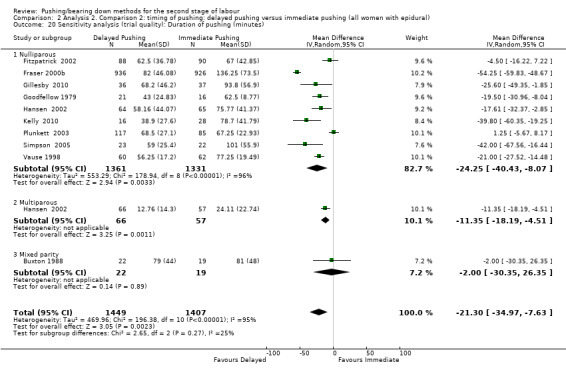
Comparison 2 Analysis 2. Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural), Outcome 20 Sensitivity analysis (trial quality): Duration of pushing (minutes).
We carried out another sensitivity analysis excluding the trials (Fitzpatrick 2002; Fraser 2000b; Goodfellow 1979; Plunkett 2003; Vause 1998) where we used a statistical method (Hozo 2005) to estimate means and standard deviations, because these trials reported data as medians and ranges. See below for sensitivity analysis of this outcome (Analysis 2.22).
2.22. Analysis.
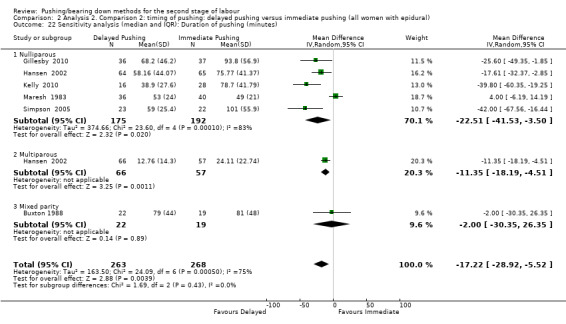
Comparison 2 Analysis 2. Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural), Outcome 22 Sensitivity analysis (median and IQR): Duration of pushing (minutes).
2. Oxytocin use in the second stage after randomisation
Only two studies (Buxton 1988; Vause 1998), could contribute to the meta‐analysis because they specified the time of use of oxytocin (second stage). There was no clear difference between delayed and immediate pushing groups in the risk of oxytocin use in the second stage (RR 1.00, 95% CI 0.79 to 1.27; two studies; 177 women; I² = 0; Analysis 2.7).
2.7. Analysis.
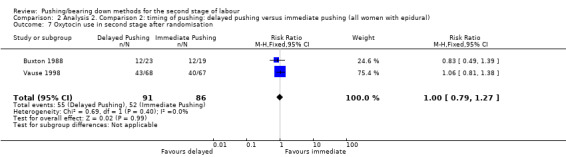
Comparison 2 Analysis 2. Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural), Outcome 7 Oxytocin use in second stage after randomisation.
3. Spontaneous vaginal delivery
The overall result of this outcome from 12 trials (Buxton 1988; Fitzpatrick 2002; Fraser 2000b; Gillesby 2010; Goodfellow 1979; Hansen 2002; Kelly 2010; Maresh 1983; Mayberry 1999; Plunkett 2003; Simpson 2005; Vause 1998), showed a slight increase in spontaneous vaginal delivery in delayed pushing group (RR 1.07; 95% CI 1.03 to 1.11; 12 studies; 3114 women; I² = 0%; moderate‐quality evidence; Analysis 2.8) compared to the immediate pushing group.
2.8. Analysis.
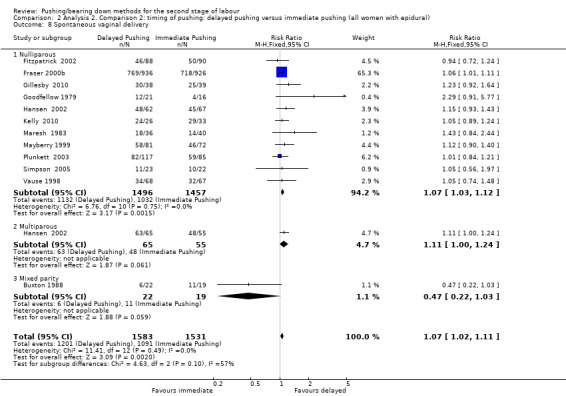
Comparison 2 Analysis 2. Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural), Outcome 8 Spontaneous vaginal delivery.
The same results were found in the subgroup analysis for nulliparous women (RR 1.07, 95% CI 1.03 to 1.12; 11 studies; 2953 women; I² = 0%), from 11 trials (Fitzpatrick 2002; Fraser 2000b; Gillesby 2010; Goodfellow 1979; Hansen 2002; Kelly 2010; Mayberry 1999; Mayberry 1999; Plunkett 2003; Simpson 2005; Vause 1998). There was no apparent difference for the multiparous subgroup (RR 1.11; 95% CI 1.00 to 1.24; P = 0.06; 120 women) from one trial (Hansen 2002). The interaction test for subgroup differences suggests that there is no difference between these subgroups (test for subgroups differences: Chi² = 0.48; df = 2; P = 0.79).
4. Instrumental delivery
Overall, 10 studies (Buxton 1988; Fitzpatrick 2002; Fraser 2000b; Gillesby 2010; Goodfellow 1979; Hansen 2002; Maresh 1983; Mayberry 1999; Plunkett 2003; Vause 1998), contributed to this analysis. No clear difference was found between the spontaneous pushing and the directed pushing groups (average RR 0.89; 95% CI 0.74 to 1.07; random‐effects; 10 studies; 3007 women; I² = 46%; Analysis 2.9).
2.9. Analysis.

Comparison 2 Analysis 2. Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural), Outcome 9 Instrumental delivery.
5.Rotational or midpelvic or posterior forceps
Overall, five studies (Buxton 1988; Fraser 2000b; Goodfellow 1979; Maresh 1983; Vause 1998) contributed data to this analysis. There was no clear difference between groups (RR 0.82, 95% CI 0.61 to 1.10; five studies; 2151 women; I² = 0%; Analysis 2.10)
2.10. Analysis.
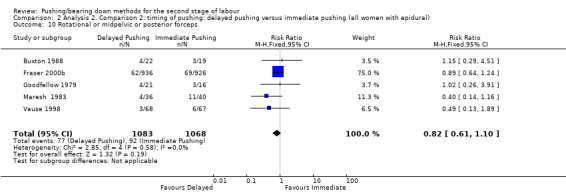
Comparison 2 Analysis 2. Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural), Outcome 10 Rotational or midpelvic or posterior forceps.
6. Caesarean delivery
There was no clear difference between groups in terms of the risk of caesarean section (RR 0.83, 95% CI 0.65 to 1.05; nine studies; 2783 women; I² = 0%; Analysis 2.11) with data from nine trials (Buxton 1988; Fitzpatrick 2002; Fraser 2000b; Gillesby 2010; Kelly 2010; Maresh 1983; Mayberry 1999; Plunkett 2003; Vause 1998).
2.11. Analysis.
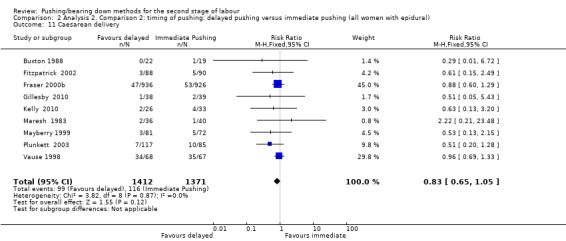
Comparison 2 Analysis 2. Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural), Outcome 11 Caesarean delivery.
7. Maternal hypertension
No trials reported maternal hypertension as an outcome.
8. Postpartum haemorrhage
There was no clear difference in postpartum haemorrhage between groups (RR 1.04, 95% CI 0.86 to 1.26; three studies; 2199 women; I² = 0%; Analysis 2.12).
2.12. Analysis.
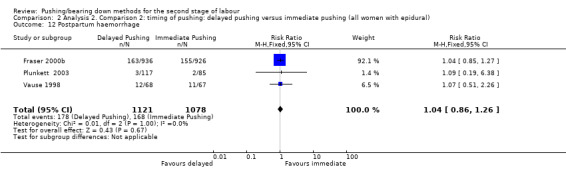
Comparison 2 Analysis 2. Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural), Outcome 12 Postpartum haemorrhage.
The results come from three trials (Fraser 2000b; Plunkett 2003; Vause 1998) that reported this outcome as a binary variable. One trial (Fraser 2000b), measured postpartum haemorrhage as an estimated blood loss greater than 500 mL, Plunkett 2003 did not specify the amount of blood loss they considered to be postpartum haemorrhage, and Vause 1998 considered blood loss at delivery > 500 mL.
9. Maternal report of severe pain in second stage
Maternal report of severe pain in second stage was not reported by these trials.
10. Fatigue after delivery (outcome not pre‐specified in our published protocol)
Only one trial (Gillesby 2010), reported this outcome (measured using a VAS) and reported no clear difference between groups (MD ‐6.40; 95% CI ‐21.00 to 8.20; 73 women; Analysis 2.13).
2.13. Analysis.
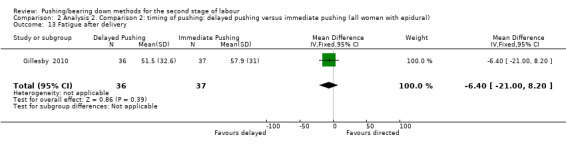
Comparison 2 Analysis 2. Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural), Outcome 13 Fatigue after delivery.
11. Maternal satisfaction (outcome not pre‐specified in our published protocol)
Maternal satisfaction with delivery (measured using a VAS) was reported by only one trial (Gillesby 2010); there was no clear difference (MD 0.40; 95% CI ‐7.34 to 8.14; Analysis 2.14). Another trial also measured maternal satisfaction with the second stage and reported the following result: "maternal satisfaction was similar between groups (median 80 min for both groups)".
2.14. Analysis.
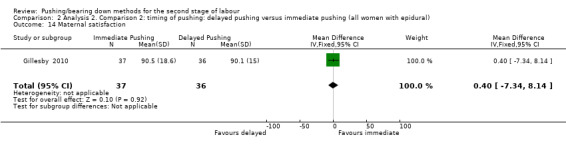
Comparison 2 Analysis 2. Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural), Outcome 14 Maternal satisfaction.
12. Perineal pain
No trials reported data for perineal pain.
13. Dyspareunia
There was no clear difference in the risk of dyspareunia (RR 1.15; 95% CI 0.63 to 2.10; one study; 162 women; Analysis 2.15) reported only by one trial (Fitzpatrick 2002).
2.15. Analysis.
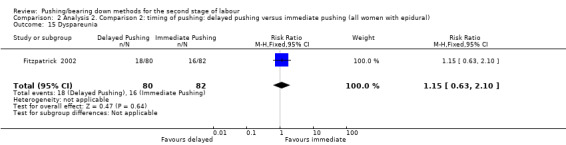
Comparison 2 Analysis 2. Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural), Outcome 15 Dyspareunia.
14. Urinary incontinence
Urinary incontinence was not reported by the trials included for this comparison.
15. Detrusor overactivity (outcome not pre‐specified in our published protocol)
Detrusor overactivity was not reported by the included trials for this comparison.
16. Fecal incontinence
Fecal incontinence was reported by one trial (Fitzpatrick 2002) and it showed no clear difference in the risk of this outcome (RR 1.47; 95% CI 0.94 to 2.29; one study; 178 women; Analysis 2.16). This outcome was documented using a modified continence score which a score of zero implying complete continence and a score of 20 implying complete incontinence.
2.16. Analysis.

Comparison 2 Analysis 2. Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural), Outcome 16 Fecal incontinence.
17. Pelvic floor prolapse
Pelvic floor prolapse was not reported by the trials in this review.
Neonatal outcomes
1. Low umbilical cord blood pH
Four trials (Buxton 1988; Fraser 2000b; Plunkett 2003; Vause 1998) reported data on umbilical cord blood pH. The risk of a low umbilical cord blood pH was higher with the use of delayed compared to immediate pushing (RR 2.24, 95% CI 1.37 to 3.68; four studies; 2145 women; I² = 0%; Analysis 2.17). These results came mainly from one trial (Fraser 2000b), which show data from abnormal pH values that considered low values of venous pH less than 7.15 or an arterial pH less than 7.10.
2.17. Analysis.
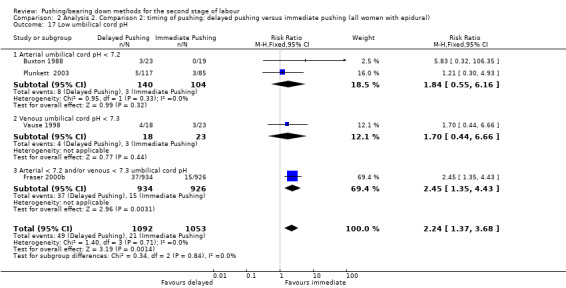
Comparison 2 Analysis 2. Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural), Outcome 17 Low umbilical cord pH.
Three trials (Hansen 2002; Maresh 1983; Simpson 2005) reported this outcome by mean and standard deviation and two trials (Fitzpatrick 2002) by median and ranges.
2. Delivery room resuscitation (outcome not pre‐specified in our published protocol)
For this comparison, none of the included studies reported this outcome.
3. Total care costs (outcome not pre‐specified in our published protocol)
Only one trial (Fraser 2000b) reported this outcome. There was an increase of about 80.00 CND$ in the total costs of hospital care (intrapartum and postnatal) (MD 81.35 CND$, 95% CI ‐80.27 to 242.97; Analysis 2.18) for the use of delayed pushing. A breakdown of the costs by care period (intrapartum/postnatal), showed that there was no difference between groups in the costs of postnatal care (MD 13.13 CND$, 95% CI ‐145.27 to 171.53; Analysis 2.18), but there was an increase in cost of intrapartum care for the delayed group (MD 68.22 CND$; 95% CI 55.37 to 81.07; Analysis 2.18).
2.18. Analysis.
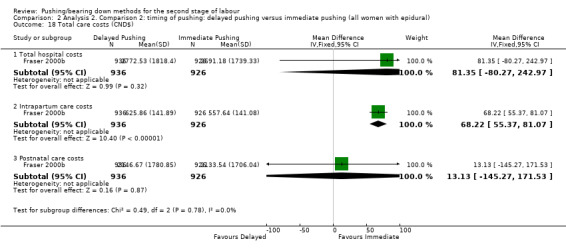
Comparison 2 Analysis 2. Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural), Outcome 18 Total care costs (CND$).
Sensitivity analysis for comparison 2
Trial quality
Duration of second stage: We found high heterogeneity in the overall result meta‐analysis (random‐effects; I² = 91%, T² = 524.61, P < 0.00001; Analysis 2.1), but our sensitivity analysis excluding the inadequately randomised trials did not change the overall result and heterogeneity remained high (MD 53.46, 95% CI 38.82 to 68.10; 10 studies; 2973 women; I2 = 91%) (only one study Maresh 1983 was considered to be quasi‐randomised). The exclusion of Maresh 1983 in the nulliparous subgroup meta‐analysis did not alter the result either (MD 52.54, 95% CI 35.14 to 69.93; 9 studies; 2809 women; I² = 93%; Analysis 2.19).
Duration of pushing: There was a high heterogeneity for the overall result (random‐effects; I² = 95%; T² = 483.92; P < 0.00001; Analysis 2.6). After the sensitivity analysis, excluding one trial (Maresh 1983), with a compromised randomisation process, there was a slight increase in the overall effect size (MD ‐21.30 minutes, 95% CI ‐34.97 to ‐7.63; random‐effects; 10 studies; 2856 women; I² = 95%; Analysis 2.20), and in the nulliparous group (MD ‐24.25 minutes, 95% CI ‐40.43 to ‐8.07; random‐effects; 9 studies; 2692 women; I² = 96%; Analysis 2.20) although high heterogeneity remained in both these analyses.
Trials reporting median and interquartile ranges
Duration of second stage: We also carried out a sensitivity analysis excluding the trials that reported the data as medians and ranges (Fitzpatrick 2002; Fraser 2000b; Plunkett 2003; Vause 1998), where we had to use a statistical method (Hozo 2005) to convert to mean and standard deviation. The results from this sensitivity analysis slightly lowered the heterogeneity and did not change the direction of the overall result (MD 56.48, 95% CI 34.24 to 78.72; random‐effects; seven studies; 684 women; I² = 88%; Analysis 2.21), and the nulliparous group result (MD 55.17, 95% CI 25.33 to 85.01; random‐effects; six studies; 520 women; I² = 89%; Analysis 2.21).
Duration of pushing: We carried out another sensitivity analysis excluding the trials (Fitzpatrick 2002; Fraser 2000b; Goodfellow 1979; Plunkett 2003; Vause 1998) where we used a statistical method (Hozo 2005) to calculate mean and standard deviation, because these trials reported data as median and ranges. The results from this sensitivity analysis slightly reduced the effect size although heterogeneity remained high (MD ‐17.22, 95% CI ‐28.92 to ‐5.52; random‐effects; six studies; 531 women; I² = 75%; Analysis 2.22). The same was true for the nulliparous group (MD ‐22.51, 95% CI ‐41.53 to ‐3.50; random‐effects; five studies; 367 women; I² = 83%; Analysis 2.22).
Discussion
Summary of main results
Comparison 1: types of pushing: spontaneous pushing versus directed pushing (with or without epidural analgesia)
Spontaneous pushing compared with directed pushing did not reduce the duration of the second stage of labour when all trials were included, although there was high heterogeneity for this outcome; when inadequately randomised trials were excluded the duration of second stage of the directed group decreased by 17 minutes; however, there remained high heterogeneity between trials and results should be interpreted with caution.
The posture used in the trials could have influenced the results of the duration of second stage and the duration of pushing. There was no consensus in the trials about the posture adopted. One study divided the groups according to posture, allowing the spontaneous group to have upright position, while the directed pushing group remained in the supine posture for the bearing down (Vaziri 2016). The posture used by the spontaneous group in this trial could have influenced the results, as there is evidence that lateral postures may shorten the second stage of labour (Gupta 2012).
There is no evidence that spontaneous pushing reduces serious perineal laceration and episiotomy, These results come from two studies that controlled the posture, which means that this variable probably did not interfere with the results. Urinary incontinence and overactive bladder results were not different between spontaneous and directed types of pushing. There is no difference between groups for the risk of caesarean and instrumental deliveries, and no evidence that spontaneous pushing increases spontaneous vaginal delivery. The included trials did not report on maternal self‐report of severe pain in the second stage of labour, maternal hypertension, postpartum haemorrhage, perineal pain, dyspareunia, fecal incontinence and pelvic floor prolapse; evidence on these outcomes is needed. Consequently, the possibility of these maternal adverse effects (particularly in relation to damage to the pelvic floor) remains unknown.
There was no difference in the use of oxytocin during the second stage of labour between the directed or spontaneous pushing groups, but this is based on evidence from one small trial (involving 100 women; Schaffer 2005). Similarly, there was no difference between groups in terms of fatigue after delivery, or maternal satisfaction (again, from one small trial involving 31 women, Thomson 1993).
We found no evidence to show that spontaneous or directed pushing was associated with adverse effects on neonatal outcomes. There were no differences between spontaneous and directed pushing groups for admission to neonatal intensive care, five‐minute Apgar score less than seven, low umbilical cord blood pH and delivery room resuscitation. The incidence of hypoxic ischaemic encephalopathy was not reported in the included studies.
Comparison 2: Timing of pushing: delayed pushing versus immediate pushing (all women with epidural analgesia)
Delayed pushing was associated with an increase in the duration of the second stage of labour by about 56 minutes overall. Despite the high heterogeneity found in this analysis, it is notable that all of the subgroup results are in the same direction, which gives some confidence that the effect is likely to be consistent in direction, if not in size.
The use of a delayed pushing in labours with epidural analgesia reduces the duration of pushing by about 19 minutes, which was also seen in the subgroup of nulliparous and multiparous. Despite the primiparous subgroup showing no difference, the interaction test does not suggest strong evidence of a differential effect between subgroups. Nevertheless, the decrease in the duration of pushing did not impact on the outcomes of fatigue after delivery and maternal satisfaction; there was no difference between the delayed and immediate groups.
There was no evidence that delayed pushing reduces third and fourth degree perineal laceration and episiotomy. Moreover, most of the trials reported the posture used by the women. As this variable might have an influence on the risk of perineal trauma, it could be a confounder in these results.
Whilst there was a 7% increase in spontaneous vaginal delivery for the delayed pushing group and even though the subgroups analysis showed no effect for primiparous and multiparous, this observation should be interpreted with caution as it is derived from few studies and the interaction test shows no evidence of any difference between the subgroups.
There was no difference in caesarean and instrumental deliveries, and midpelvic forceps. Despite the non significant results for these outcomes, the overall effects favour the delayed pushing group and the confidence interval upper limit from all these analyses barely overlaps 1.0. Therefore, it seems that delayed pushing tends to reduce caesarean instrumental and midpelvic forceps deliveries.
Some outcomes, such as maternal hypertension, maternal report of severe pain in the second stage of labour, perineal pain, urinary incontinence, detrusor overactivity and pelvic floor prolapse were not reported by the trials and the evidence remains inconclusive for these outcomes. Consequently, the risk of these maternal adverse effects (particularly in relation to damage to the pelvic floor), remains unknown. There were no differences between the delayed and immediate pushing groups in relation to the incidence of postpartum haemorrhage, or the use of oxytocin during the second stage.
The risk of a low umbilical cord blood pH was doubled with delayed pushing, although this result is mainly from one study, suggesting an adverse effect on the fetus. No trials reported hypoxic ischaemic encephalopathy or delivery room resuscitation, and admission to neonatal Intensive unit care was no different between delayed and immediate pushing groups. There was also no difference between groups for five‐minute Apgar score less than seven, however the result comes from just one trial and because of the selective outcome reporting (incomplete data), this finding should not be considered to be truly representative.
Compared to a policy of immediate pushing, delayed pushing did not result in an increase in the total cost of care or the cost of postnatal care. However, delayed pushing was associated with an increase in intrapartum costs by about CND$ 68.22.
Overall completeness and applicability of evidence
The evidence in this review was provided from trials conducted in various countries, but mainly from the USA and Europe. There were no trials from Latin America. The results came exclusively from low‐risk pregnancies of different parities with a singleton fetus in a term gestation in women aged between 18 and 40 years old. Therefore, it is hard to generalise this evidence to high‐risk pregnancies, adolescent pregnant women or to those women with preterm labour. Recruitment to all trials occurred in a hospital setting and mostly there was no prenatal education to teach women about spontaneous pushing, with the exception of one trial that mentioned the method.
Basically, spontaneous pushing with no use of epidural consisted of no instructions about the way (timing and type) that the pregnant women should push, followed by words of encouragement during the process. The protocol of delayed pushing established among the trials was different between the included studies, which makes it difficult to make more precise recommendations. Overall, the trials delayed 'pushing' for one to two hours or until the fetal head was visible at the perineum. This evidence is based on labours in which epidural analgesia was used and therefore may not generalise to labours which do not use epidural analgesia.
It is still not clear what the effects are of delayed pushing versus a spontaneous type of pushing plus the use of an epidural, as most of the trials did not report this method, or used a closed‐glottis pushing. Nevertheless, spontaneous pushing used without epidural analgesia tends to reduce the duration of pushing and increase the duration of the second stage of labour with no effect on pain and fatigue after delivery.
It seems that delayed pushing with epidural analgesia tends to reduce instrumental and caesarean deliveries, despite the evidence found here, which did not reach statistical significance. In the same way, some effect of delayed pushing on reducing rotational or midforceps could not be excluded. However, the use of delayed pushing increased the rate of spontaneous vaginal delivery.
As delayed pushing increases the duration of the second stage of labour and as the largest trial (Fraser 2000b), showed an increase in the abnormal pH umbilical cord values, it is important to explore this possible effect in other trials, as other parameters such as Apgar scores, delivery room resuscitation and neonatal admission to intensive care unit were either no different and/or not described in most of the trials. It is important to mention that although the duration of the second stage of labour seems to increase with delayed pushing, the length of pushing is reduced for this group, indicating a possible "compensatory" effect, once women spend less time pushing. If a longer duration of the second stage, but a reduced length of pushing are beneficial or considered important by the women, it is a point that needs to be investigated in other studies.
Quality of the evidence
For the trials comparing types of pushing: spontaneous pushing versus directed pushing (with or without epidural analgesia), most of the available evidence shows a balance between high and low risk of bias for randomisation and allocation concealment. Selective outcome reporting and attrition bias may affect the reliability of our findings because most of the studies were at high or unclear risk of bias for these domains. Lack of blinding for the women may not cause a bias for objective outcomes, and for this intervention it was impossible to blind the women in this type of study. However, for the outcome assessors, lack of blinding may be a potential source of bias, particularly for the subjective outcomes, as in most of the trials it was not clear whether the outcome assessors were blinded. The global quality of evidence for the seven outcomes (duration of second stage, perineal laceration, hypoxic ischaemic encephalopathy, Apgar scores at five minutes less than seven, admission to neonatal intensive care, duration of pushing, and spontaneous vaginal delivery) listed in the GRADE evaluation was moderate tovery low due mainly due to study limitation bias, inconsistency and imprecision.
Current evidence for the trials comparing timing of pushing: delayed pushing versus immediate pushing (all women with epidural analgesia) comes from studies where the randomisation process was often adequate, but the allocation concealment was often rated to be at unclear or high risk, resulting in bias which may overestimate the final result. Although the non‐blinded design for the patients was present in all trials, the primary outcomes pre‐specified in this review were objective and are less susceptible to bias from lack of blinding compared to subjective outcomes. Since it was not clear whether the outcome assessors were blinded in most of the trials, we are not sure to what extent this could affect some outcomes, such as length of pushing, fatigue after delivery, and maternal satisfaction. According to the GRADE assessment, outcomes for this comparison were graded from moderate to very low quality with downgrading due to inconsistency, imprecision and study limitations.
It is also important to note that selective outcome reporting was present in all but one of the trials. For some trials, we were unable to obtain data for some important outcomes, or data were reported in such a way that they were unsuitable for meta‐analysis.
Potential biases in the review process
We followed the methods set out in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011), in order to try to reduce potential biases in the review process. The evidence for this review came from a detailed search process, which included published and unpublished papers and no language restrictions. It is possible that potentially eligible studies conducted in journals not easy to access have been published and could not be identified by this search strategy. Futhermore, we need to consider the 'lag bias' (studies that have been done, but not yet published). Any additional information about potentially eligible trials to be included in this review will be welcome and should be sent to the contact person for this review.
For Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural analgesia), some studies reported continuous variables as medians and ranges for the duration of the second stage of labour (Fitzpatrick 2002; Fraser 2000b; Plunkett 2003; Vause 1998), and for duration of pushing (Fitzpatrick 2002; Fraser 2000b; Goodfellow 1979; Plunkett 2003; Vause 1998), we used a statistical method (Hozo 2005), to estimate means and standard deviations, which can cause an overestimation or underestimation of the overall effect. However, we carried out sensitivity analyses (excluding the studies with the mean calculated by the statistical method) and the direction of the overall result for both outcomes: duration of the second stage and duration of pushing did not change, but there was a decrease in the heterogeneity, which might explain part of the high heterogeneity found before.
For the outcome instrumental delivery (Figure 4), from the trials comparing timing of pushing: delayed pushing to immediate pushing (all women with epidural analgesia), it seems that there was little evidence of potential publication bias, which could be seen from the funnel plots. However, for the outcome duration of the second stage (Figure 5), the studies are concentrated in the upper part of the graph showing different results, which may indicate a possible reporting bias from the lack of studies in the bottom part, and large trials showing minimum effect. There is also an asymmetry for the outcome duration of pushing (Figure 6), and spontaneous vaginal delivery (Figure 7), which could also reflect a reporting bias.
4.
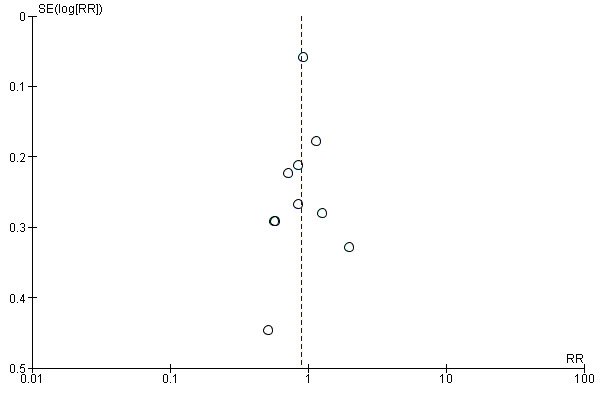
Funnel plot of comparison 2: Delayed pushing versus immediate pushing (all women with epidural), outcome: 2.10 Instrumental delivery.
5.
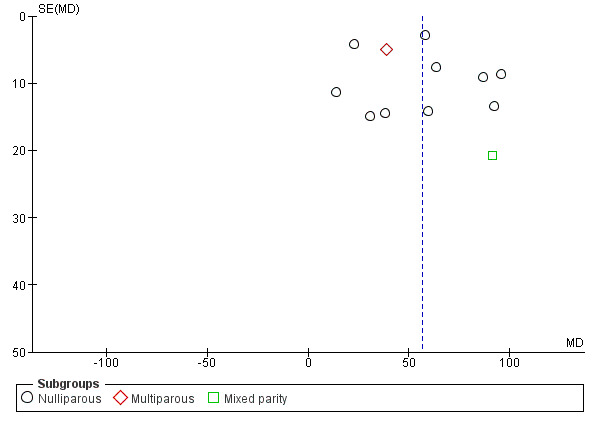
Funnel plot of comparison 2: Delayed pushing versus immediate pushing (all women with epidural), outcome: 2.1 Duration of second stage.
6.
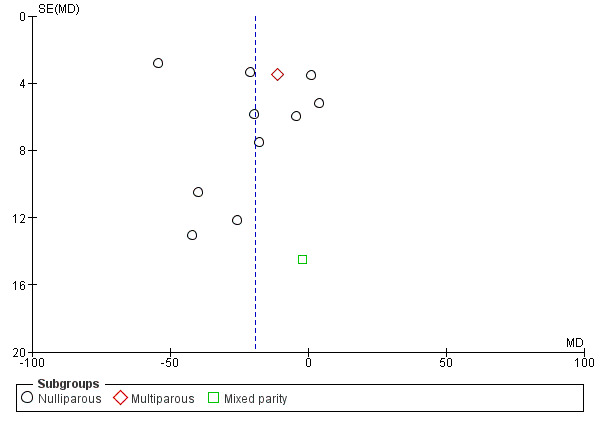
Funnel plot of comparison 2: Delayed pushing versus immediate pushing (all women with epidural), outcome: 2.7 Duration of Pushing.
7.
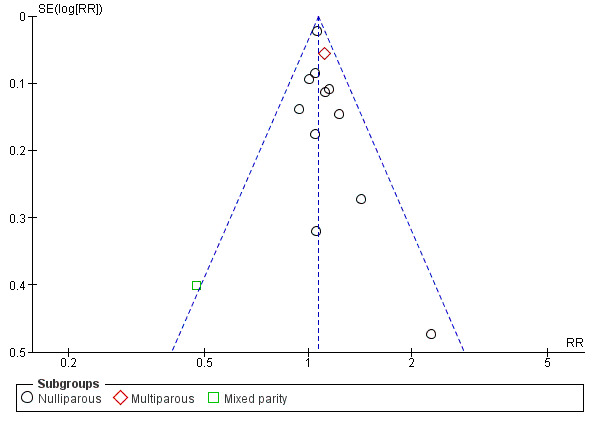
Funnel plot of comparison 2: Delayed pushing versus immediate pushing (all women with epidural), outcome: 2.9 Spontaneous vaginal delivery.
Agreements and disagreements with other studies or reviews
Comparison 1: Types of pushing: spontaneous pushing versus directed pushing (with or without epidural analgesia)
The new finding from this review is that spontaneous pushing may decrease the duration of pushing by about 10 minutes, although there was no clear difference in the duration of the second stage between spontaneous pushing and directed pushing, while another systematic review that included only three studies (Prins 2011), found a shorter duration of labour in women who used directed pushing. The other maternal and neonatal major findings are consistent with those of this previous systematic review (Prins 2011).
Comparison 2: Timing of pushing: delayed pushing versus immediate pushing (all women with epidural analgesia)
The evidence from this systematic review showed that delayed pushing increases the duration of the second stage of labour and decreases the duration of pushing. These results are consistent with the findings from four other reviews (Brancato 2008; Menez‐Orieux 2005; Roberts 2004; Tuuli 2012). The only review (Roberts 2002) that did not find a difference in the pushing time, did not include studies where data were reported as median and ranges.
This review did not find any difference in perineal laceration and episiotomy, which is consistent with the results of three other meta‐analyses (Brancato 2008; Menez‐Orieux 2005; Roberts 2004). The same consistent result from three reviews (Brancato 2008; Roberts 2002; Tuuli 2012) that showed no difference for caesarean delivery was noted in this review.
For the three reviews (Menez‐Orieux 2005; Roberts 2004; Tuuli 2012) that assessed neonatal outcomes, the evidence was not clear about the effects on these outcomes. One review (Tuuli 2012), highlighted the results of a large study (Fraser 2000b) that found a significantly higher rate of abnormal pH with delayed pushing, which corroborates our results.
This review showed a slight increase in spontaneous vaginal birth with the use of delayed pushing and this finding was consistent with the results from the previous reviews. Three reviews (Brancato 2008; Menez‐Orieux 2005; Roberts 2004) found the delayed pushing group was more likely to have spontaneous vaginal delivery. In two reviews (Menez‐Orieux 2005; Roberts 2002), it is not clear which studies were included in the meta‐analysis and the other review (Brancato 2008), included only seven studies, which differs from our review that included 13 studies for this comparison. The fourth review (Tuuli 2012), only noted this outcome increase in the delayed pushing group when lower quality studies were included.
There was no clear difference in the risk of instrumental delivery between groups found in this review. Two reviews (Brancato 2008; Menez‐Orieux 2005), found a lower risk of instrumental delivery for the delayed pushing group and one review (Roberts 2004), found a decrease in instrumental delivery only when the subgroup of rotational or midpelvic instrumental (RR 0.69; 95% CI 0.55 to 0.87) was considered. However, their analysis considered data from the Fraser study (Fraser 2000b), which included midpelvic forceps, midpelvic vacuum and manual rotation and included one trial that showed no difference (Mc Queen 1977). This trial (Mc Queen 1977) was excluded from our review (see (Excluded studies). In contrast, our analysis considered Fraser 2000b data only for midpelvic forceps and also included another trial (Maresh 1983) not included in Roberts 2004 review.
Authors' conclusions
Implications for practice.
For the type of pushing, with or without epidural, based on available evidence it is not clear whether spontaneous or directed pushing achieves optimal outcomes for women and babies. Until further high‐quality studies are available, women should be encouraged to push and bear down according to their comfort and preference.
The maternal and neonatal benefits and adverse effects of delayed and immediate pushing with epidural are not well‐established.
Waiting for the urge to push with an epidural does shorten the duration of pushing and increases spontaneous vaginal delivery, but lengthens the second stage and doubles the risk of low umbilical cord pH (based on data from one study). Nevertheless, there was no difference between delayed and immediate pushing in terms of caesarean and instrumental deliveries, perineal laceration and episiotomy, or other neonatal outcomes (admission to neonatal intensive care, five‐minute Apgar score less than seven, and delivery room resuscitation). Futhermore, adverse effects in relation to maternal pelvic floor are still unclear.
Therefore, in the absence of strong evidence supporting any specific method or timing of pushing, decisions should be guided by the woman's preference and the clinical scenario.
Implications for research.
Further well‐designed trials are required to assess the benefits, adverse effects and risks of pushing/bearing down during the second stage of labour. Future trials should be adequately powered to address clinically important maternal outcomes, particularly for perineal trauma (perineal laceration and episiotomy), oxytocin use in the second stage of labour after randomisation, spontaneous vaginal delivery, instrumental delivery, rotational or midpelvic or posterior forceps, caesarean delivery, maternal hypertension, postpartum haemorrhage, fatigue after delivery, maternal satisfaction, and maternal report of severe pain in the second stage. Furthermore, short‐term and long‐term evidence for maternal pelvic outcomes such as perineal pain, dyspareunia, urinary and fecal incontinence, detrusor overactivity, and pelvic floor prolapse should also be addressed. Women's experiences and preferences should also be measured.
Clinically important neonatal outcomes, including admission to neonatal intensive care, hypoxic ischaemic encephalopathy and the need for resuscitation should be assessed, as well as the total care costs. It is important that future trials capture data for neonatal outcomes, five‐minute Apgar score less than seven, and low umbilical cord pH, should be expressed as a binary variable to enable inclusion of the data in this review's meta‐analysis.
What's new
| Date | Event | Description |
|---|---|---|
| 19 September 2016 | New search has been performed | Search updated. For this update, we have added one new included study (Vaziri 2016), three new excluded studies (Aviram 2016; Haseeb 2014; Moraloglu 2016) and one ongoing study (Cahill 2014). This updated review is now comprised of 21 included studies, 21 excluded studies and two other studies that are ongoing. For this update we have used the GRADE approach to assess the quality of the body of evidence include Table 1 and Table 2. |
| 19 September 2016 | New citation required but conclusions have not changed | The overall conclusions remain unchanged. |
Acknowledgements
We would like to thank Erica Gillesby and Amy Dempsey for providing us with additional information and unpublished data relating to their trial (Gillesby 2010).
This project was supported by the National Institute for Health Research, via Cochrane Infrastructure funding to Cochrane Pregnancy and Childbirth. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS or the Department of Health.
Data and analyses
Comparison 1. Analysis 1. Comparison 1: types of pushing: spontaneous pushing versus directed pushing.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Duration of second stage (minutes) | 6 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 Nulliparous | 6 | 667 | Mean Difference (IV, Random, 95% CI) | 10.26 [‐1.12, 21.64] |
| 2 Perineal laceration (3rd or 4th degree) | 1 | 320 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.87 [0.45, 1.66] |
| 3 Episiotomy | 2 | 420 | Risk Ratio (M‐H, Random, 95% CI) | 1.05 [0.60, 1.85] |
| 4 Admission to neonatal intensive care | 2 | 393 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.08 [0.30, 3.79] |
| 5 Five‐minute Apgar score < seven | 1 | 320 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.35 [0.01, 8.43] |
| 6 Duration of pushing (minutes) | 2 | 169 | Mean Difference (IV, Random, 95% CI) | ‐9.76 [‐19.54, 0.02] |
| 6.1 Mixed parity | 2 | 169 | Mean Difference (IV, Random, 95% CI) | ‐9.76 [‐19.54, 0.02] |
| 7 Oxytocin use in second stage after randomisation | 1 | 128 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.20 [0.80, 6.07] |
| 8 Spontaneous vaginal delivery | 5 | 688 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.01 [0.97, 1.05] |
| 9 Instrumental delivery | 2 | 393 | Risk Ratio (M‐H, Random, 95% CI) | 0.56 [0.06, 5.10] |
| 10 Caesarean delivery | 3 | 583 | Risk Ratio (M‐H, Random, 95% CI) | 0.79 [0.14, 4.39] |
| 11 Fatigue after delivery | 2 | 142 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.14 [‐3.29, 1.02] |
| 12 Maternal satisfaction | 1 | 31 | Mean Difference (IV, Fixed, 95% CI) | 0.91 [‐1.30, 3.12] |
| 13 Detrusor overactivity | 1 | 128 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.50 [0.18, 1.36] |
| 14 Urinary stress incontinence | 1 | 128 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.70 [0.29, 1.69] |
| 15 Low umbilical cord blood | 1 | 320 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.74 [0.24, 2.29] |
| 15.1 Arterial umbilical cord pH < 7.2 | 1 | 320 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.74 [0.24, 2.29] |
| 15.2 Venous umbilical cord < 7.3 | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 16 Delivery room resuscitation | 2 | 352 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.83 [0.40, 1.75] |
| 17 Sensitivity analysis (trial quality): Duration of second stage (minutes) | 4 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 17.1 All studies | 4 | 494 | Mean Difference (IV, Random, 95% CI) | 17.62 [5.28, 29.95] |
| 18 Sensitivity analysis (trial quality): Duration of pushing (minutes) | 1 | 69 | Mean Difference (IV, Random, 95% CI) | ‐15.22 [‐21.64, ‐8.80] |
| 18.1 Mixed parity | 1 | 69 | Mean Difference (IV, Random, 95% CI) | ‐15.22 [‐21.64, ‐8.80] |
Comparison 2. Analysis 2. Comparison 2: timing of pushing: delayed pushing versus immediate pushing (all women with epidural).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Duration of second stage (minutes) | 11 | 3049 | Mean Difference (IV, Random, 95% CI) | 56.40 [42.05, 70.76] |
| 1.1 Nulliparous | 10 | 2885 | Mean Difference (IV, Random, 95% CI) | 56.12 [39.29, 72.96] |
| 1.2 Multiparous | 1 | 123 | Mean Difference (IV, Random, 95% CI) | 38.80 [29.16, 48.44] |
| 1.3 Mixed parity | 1 | 41 | Mean Difference (IV, Random, 95% CI) | 91.0 [50.37, 131.63] |
| 2 Perineal Laceration (3rd or 4th degree) | 7 | 2775 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.78, 1.14] |
| 3 Episiotomy | 5 | 2320 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.95 [0.87, 1.04] |
| 4 Admission to neonatal intensive care | 3 | 2197 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.98 [0.67, 1.41] |
| 5 Five‐minute Apgar score < seven | 3 | 413 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.15 [0.01, 3.00] |
| 6 Duration of pushing (minutes) | 11 | 2932 | Mean Difference (IV, Random, 95% CI) | ‐19.05 [‐32.27, ‐5.83] |
| 6.1 Nulliparous | 10 | 2768 | Mean Difference (IV, Random, 95% CI) | ‐21.30 [‐36.87, ‐5.73] |
| 6.2 Multiparous | 1 | 123 | Mean Difference (IV, Random, 95% CI) | ‐11.35 [‐18.19, ‐4.51] |
| 6.3 Mixed parity | 1 | 41 | Mean Difference (IV, Random, 95% CI) | ‐2.0 [‐30.35, 26.35] |
| 7 Oxytocin use in second stage after randomisation | 2 | 177 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.00 [0.79, 1.27] |
| 8 Spontaneous vaginal delivery | 12 | 3114 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.07 [1.02, 1.11] |
| 8.1 Nulliparous | 11 | 2953 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.07 [1.03, 1.12] |
| 8.2 Multiparous | 1 | 120 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.11 [1.00, 1.24] |
| 8.3 Mixed parity | 1 | 41 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.47 [0.22, 1.03] |
| 9 Instrumental delivery | 10 | 3007 | Risk Ratio (M‐H, Random, 95% CI) | 0.89 [0.74, 1.07] |
| 10 Rotational or midpelvic or posterior forceps | 5 | 2151 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.82 [0.61, 1.10] |
| 11 Caesarean delivery | 9 | 2783 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.83 [0.65, 1.05] |
| 12 Postpartum haemorrhage | 3 | 2199 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.04 [0.86, 1.26] |
| 13 Fatigue after delivery | 1 | 73 | Mean Difference (IV, Fixed, 95% CI) | ‐6.40 [‐21.00, 8.20] |
| 14 Maternal satisfaction | 1 | 73 | Mean Difference (IV, Fixed, 95% CI) | 0.40 [‐7.34, 8.14] |
| 15 Dyspareunia | 1 | 162 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.15 [0.63, 2.10] |
| 16 Fecal incontinence | 1 | 178 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.47 [0.94, 2.29] |
| 17 Low umbilical cord pH | 4 | 2145 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.24 [1.37, 3.68] |
| 17.1 Arterial umbilical cord pH < 7.2 | 2 | 244 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.84 [0.55, 6.16] |
| 17.2 Venous umbilical cord pH < 7.3 | 1 | 41 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.70 [0.44, 6.66] |
| 17.3 Arterial < 7.2 and/or venous < 7.3 umbilical cord pH | 1 | 1860 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.45 [1.35, 4.43] |
| 18 Total care costs (CND$) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 18.1 Total hospital costs | 1 | 1862 | Mean Difference (IV, Fixed, 95% CI) | 81.35 [‐80.27, 242.97] |
| 18.2 Intrapartum care costs | 1 | 1862 | Mean Difference (IV, Fixed, 95% CI) | 68.22 [55.37, 81.07] |
| 18.3 Postnatal care costs | 1 | 1862 | Mean Difference (IV, Fixed, 95% CI) | 13.13 [‐145.27, 171.53] |
| 19 Sensitivity analysis (trial quality): Duration of second stage (minutes) | 10 | 2973 | Mean Difference (IV, Random, 95% CI) | 53.46 [38.82, 68.10] |
| 19.1 Nulliparous | 9 | 2809 | Mean Difference (IV, Random, 95% CI) | 52.54 [35.14, 69.93] |
| 19.2 Multiparous | 1 | 123 | Mean Difference (IV, Random, 95% CI) | 38.80 [29.16, 48.44] |
| 19.3 Mixed parity | 1 | 41 | Mean Difference (IV, Random, 95% CI) | 91.0 [50.37, 131.63] |
| 20 Sensitivity analysis (trial quality): Duration of pushing (minutes) | 10 | 2856 | Mean Difference (IV, Random, 95% CI) | ‐21.30 [‐34.97, ‐7.63] |
| 20.1 Nulliparous | 9 | 2692 | Mean Difference (IV, Random, 95% CI) | ‐24.25 [‐40.43, ‐8.07] |
| 20.2 Multiparous | 1 | 123 | Mean Difference (IV, Random, 95% CI) | ‐11.35 [‐18.19, ‐4.51] |
| 20.3 Mixed parity | 1 | 41 | Mean Difference (IV, Random, 95% CI) | ‐2.0 [‐30.35, 26.35] |
| 21 Sensitivity analysis (median and IQR): Duration of second stage (minutes) | 7 | 684 | Mean Difference (IV, Random, 95% CI) | 56.48 [34.24, 78.72] |
| 21.1 Nulliparous | 6 | 520 | Mean Difference (IV, Random, 95% CI) | 55.17 [25.33, 85.01] |
| 21.2 Multiparous | 1 | 123 | Mean Difference (IV, Random, 95% CI) | 38.80 [29.16, 48.44] |
| 21.3 Mixed parity | 1 | 41 | Mean Difference (IV, Random, 95% CI) | 91.0 [50.37, 131.63] |
| 22 Sensitivity analysis (median and IQR): Duration of pushing (minutes) | 6 | 531 | Mean Difference (IV, Random, 95% CI) | ‐17.22 [‐28.92, ‐5.52] |
| 22.1 Nulliparous | 5 | 367 | Mean Difference (IV, Random, 95% CI) | ‐22.51 [‐41.53, ‐3.50] |
| 22.2 Multiparous | 1 | 123 | Mean Difference (IV, Random, 95% CI) | ‐11.35 [‐18.19, ‐4.51] |
| 22.3 Mixed parity | 1 | 41 | Mean Difference (IV, Random, 95% CI) | ‐2.0 [‐30.35, 26.35] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Buxton 1988.
| Methods | RCT | |
| Participants |
Setting: trial conducted in the UK. Inclusion criteria: singleton vertex presentations, age 17 to 35 years old. Exclusion criteria: 4 previous deliveries, obstetric complications or indication for a short second stage and upon diagnosis of full cervical dilation a fetal scalp blood sample was obtained and if any patient with occult fetal acidosis (pH < 7.3; base excess > ‐6.0 mmol/L) was detected, the patient was excluded from the study. 42 women randomised. |
|
| Interventions |
“Pushing group”: commenced organised pushing immediately (19 women). “Delayed pushing group”: remained sitting or in the lateral position for up to 3 hours or until the vertex became visible and organised pushing commenced immediately (23 women). |
|
| Outcomes | Length of second stage, length of pushing, mode of delivery vaginal, caesarean and forceps (rotational and non rotational). | |
| Notes | Trial funding not clear. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐derived random number series. |
| Allocation concealment (selection bias) | Unclear risk | There is no report about allocation concealment or when the randomisation was done. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not mentioned. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | It does not show any fluxogram. It just says: "one women was withdrawn at the onset of 2 stage – occult fetal acidosis". |
| Selective reporting (reporting bias) | High risk | Most of the important outcomes are missing. |
| Other bias | Low risk | No other problems detected that could put the study at a risk of bias. |
Fitzpatrick 2002.
| Methods | RCT | |
| Participants |
Setting: trial conducted in Ireland. Inclusion criteria: primiparae, in either spontaneous or induced labour with a singleton fetus, cephalic presentation between 37 and 42 weeks of gestation and had effective epidural analgesia in situ Exclusion criteria: patients with diabetes, irritable bowel syndrome or other bowel or neurological disorder were excluded from the study. Or if after randomisation the vertex was visible at the introitus. 178 women randomised. |
|
| Interventions |
“Immediate pushing”: pushing right after full dilatation (90 women). “Delayed pushing”: 60 min delay (88 women). |
|
| Outcomes | Length of second stage, length of pushing episiotomy, perineal laceration second degree and third degree, mode of delivery vaginal, caesarean and forceps, dyspareunia at 3 months postpartum, fecal incontinence. | |
| Notes | Labours were managed according to the Active Management protocol, which included early amniotomy and subsequent augmentation with intravenous oxytocin if cervical dilation did not progress at 1 cm per hour. It was stated that the study "was supported by a grant from the Irish Research Board". |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Numbered opaque sealed envelopes containing computer‐generated random allocations in a ratio of 1:1 in balanced blocks of 10. |
| Allocation concealment (selection bias) | Low risk | Upon a diagnosis of full dilation sealed envelopes were opened and the patient was randomised by the attending midwife. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding of participants and key study personnel. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | All the clinical staff who measured the outcomes were blinded to the patient's history. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 1412 approached antenatal. 1030 consented (73%). 650 had epidural. 178 randomised (27%). 90 immediate pushing. 88 delayed pushing. Follow‐up (3 months). 90 immediate pushing. 88 delayed pushing. |
| Selective reporting (reporting bias) | High risk | More than 1 outcome of interest in the review was reported incompletely so that they could not be entered in the meta‐analyses. |
| Other bias | Low risk | No other problems detected that could put the study at a risk of bias. |
Fraser 2000b.
| Methods | RCT | |
| Participants |
Setting: trial conducted in Canada. Inclusion criteria: nulliparous, ≥ 37 weeks' gestation (≥ 259 days' gestation), single fetus with cephalic presentation, spontaneous or induced labour with normal fetal heart status and effective epidural analgesia (pain < 3 cm on a 10 cm VAS) with a standardised continuous‐infusion technique. Exclusion criteria: if women were already pushing spontaneously, if they had fever with a temperature > 38° C, if the pregnancy was complicated by hypertension, a recent haemorrhage, suspicion of fetal malformation, or intrauterine growth restriction, or if any condition was present that necessitated shortening of the second stage of labour. 1862 women randomised. |
|
| Interventions |
“Early pushing group”: was encouraged to commence pushing immediately (926 women). “Delayed pushing group”: was advised to avoid voluntary expulsive efforts for 2 hours unless: 1 ‐ she felt an irresistible urge to push, 2 ‐ the fetal head was visualised during the course of routine (every 15 mins) inspection of the perineum or 3 ‐ a medical indication to shorten the second stage of labour developed (936 women). |
|
| Outcomes | Length of second stage, length of pushing, admission to NICU, mode of delivery vaginal and caesarean. Intrapartum care costs, postnatal care costs and total costs. | |
| Notes | 1 report (Le Ray 2008) did not contribute to the analysis because it was a secondary analysis considering the data from both groups together. It was stated that the work was supported by the Medical Research Council of Canada (who provided salary support for 1 of the trial authors). AstraZeneca R&D Montreal (Montreal, Quebec, Canada) provided medication and salary support for a research fellow (one of the trial authors). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomisation was centralised and stratified according to centre and to the use of oxytocin during the first stage of labour. There is no description of the random sequence generation. This was done when the women were full dilated. |
| Allocation concealment (selection bias) | Low risk | Randomisation was centralised. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding of participants. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not mentioned. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Intention‐to‐treat analysis. |
| Selective reporting (reporting bias) | High risk | Incomplete outcomes to enter in the meta‐analysis. |
| Other bias | Low risk | No other problems detected that could put the study at a risk of bias. |
Gillesby 2010.
| Methods | RCT | |
| Participants |
Setting: trial conducted in the USA. Inclusion criteria: nulliparous women, with continuous standard dose, lumbar epidurals who reached the 2nd stage of labour. Age > 16 years; viable vertex singleton fetus, and fetal age >= 36 weeks, Exclusion criteria: scheduled caesarean delivery, administration of magnesium sulphate therapy, and/or maternal cardiac condition. Maternal weight >= 275 pounds was an additional exclusion criterion. 77 women randomised. |
|
| Interventions |
Immediate pushing: began pushing within 15 mins of the time the cervix was determined to be completely dilated. Instruction was to bear down 3 to 4 times with each contraction, but was not limited (39 women). Delayed pushing: delayed the onset of pushing for 2 hours or until the patient experienced an irresistible urge to push or spontaneous delivery was imminent (38 women). |
|
| Outcomes | Length of second stage, length of pushing, episiotomy, laceration first, second, third and fourth degree, mode of delivery vaginal, caesarean and forceps. | |
| Notes | Funding sources not stated. Authors report no conflict of interest. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation scheme. |
| Allocation concealment (selection bias) | Unclear risk | Randomisation at full dilation but methods for allocation concealment were not mentioned. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding of participants. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not mentioned. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 85 consented. 8 were excluded. 77 were randomised. Intention‐to‐treat analysis. |
| Selective reporting (reporting bias) | High risk | Incomplete outcomes to enter in the meta‐analysis. |
| Other bias | Low risk | No other problems detected that could put the study at a risk of bias. |
Goodfellow 1979.
| Methods | RCT | |
| Participants |
Setting: trial conducted in the UK. Inclusion criteria: normal primagravidae 158 cm or more in height. Exclusion criteria: those with inadequate epidurals or complications such as fetal distress were excluded from allocation. 37 women randomised. |
|
| Interventions |
“Control group”: made expulsive effort without delay and no increase was made in the rate of oxytocin infusion (16 women). “Treatment group”: treated patients lay on their sides without making expulsive efforts. The rate of oxytocin infusion was increased by 4 miliunits per min every 4 mins in the absence of excessive uterine activity to a maximum of 32 mu/mi. When the fetal head became visible or an hour had elapsed expulsive efforts were encouraged (21 women). |
|
| Outcomes | Mode of delivery vaginal, caesarean and forceps. | |
| Notes | Funding sources not specified. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | At the onset of full dilation patients were allocated randomly to treatment or control groups. |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding of participants. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not mentioned. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not mentioned. |
| Selective reporting (reporting bias) | High risk | Missing most of the important outcomes and the study fails to include result from 1 of the key outcomes (length of second stage). |
| Other bias | Low risk | No other problems detected that could put the study at a risk of bias. |
Hansen 2002.
| Methods | RCT | |
| Participants |
Setting: trial conducted in the USA. Inclusion criteria: primigravid and multigravid. Exclusion criteria: refused an epidural, first epidural dose after complete dilation, known fetal anomaly, multiple gestation, nonvertex presentation, gestational age less than 37 weeks or over 42 weeks, and pregnancy complicated by pregnancy‐induced hypertension, heart disease, or insulin‐dependent diabetes. 312 women randomised, data available for 252. |
|
| Interventions |
“Passive fetal descent”: began a period of rest and descend at the time of complete dilatation and continued until the head was seen at the introitus or after 120 mins in primigravidas or 60 mins in multigravidas. These women were encouraged not to push. The introitus was examined in this manner every 30 mins or sooner if signs of imminent delivery occurred (130 women included in the analysis (not clear how many randomised)). “Active pushing”: both the primigravidas and multigravidas in the control group were encouraged to begin pushing as soon as they were found to be completely dilated (122 women included in the analysis (not clear how many randomised)). In both control and experimental group pushing consisted of coached Valsalva Maneuver direct by the nurse or physician during contractions. |
|
| Outcomes | Length of second stage, length of pushing, mode of delivery forceps. | |
| Notes | Reported to be funded by the Deseret Foundation. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer–generated randomised list. |
| Allocation concealment (selection bias) | Unclear risk | Methods for allocation concealment and the onset of the randomisation are not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding of the participants. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not mentioned. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Initial enrolment: 312. Completed the study: 252. Lost: 60. |
| Selective reporting (reporting bias) | High risk | Incomplete outcomes to enter in the meta‐analysis. |
| Other bias | Low risk | No other problems detected that could put the study at a risk of bias. |
Jahdi 2011.
| Methods | RCT | |
| Participants |
Setting: trial conducted in Iran. Inclusion criteria: low‐risk pregnancies with singleton fetus with estimated birthweight of 2500 g to 4000 g, vertex presentation, gestational age between 37 and 42 weeks, parity between 1 and 5, maternal age: 18‐40 years. Exclusion criteria: did not wish to participate, had maternal medical or obstetric complications which would affect the management of the second stage of labour, had a baby with congenital anomalies or when fetal compromise was suspected. 258 women randomised. |
|
| Interventions |
Directed pushing group: women were coached by the midwife to use closed‐glottis pushing 3 to 4 times during each contraction immediately when cervical dilation reached 10 cm and a fetal head plus 1 and to continue pushing using this method with each contraction until birth. The breath was held for 10 seconds. They were limited to bed in supine position (130 women). Physiological pushing group: women commenced pushing only when they felt urge to do so and no specific instructions about the timing and duration of pushing was given. They used upright position including: standing, sitting, and squatting (128 women). In both groups if delivery was not imminent after 120 mins for primiparous and 60 mins for multiparous, the method used was whatever clinical management deemed necessary to facilitate birth. Both groups delivered in a birthing chair in a sitting position. |
|
| Outcomes | Duration of second stage, mode of birth, Apgar scores. | |
| Notes | Funded by the Islamic Azad University, Tehran Medical Branch and Tehran University of Medical Sciences. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomisation occurred upon confirmation of full dilatation of the cervix by block randomisation from a set of 10 envelopes. Does not mention how the sequence generation was done. |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not mentioned. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | There is no report on missing and drops. |
| Selective reporting (reporting bias) | High risk | Important outcomes are missing and incomplete results to put in meta‐analysis. |
| Other bias | Low risk | No other problems detected that could put the study at a risk of bias. |
Kelly 2010.
| Methods | RCT | |
| Participants |
Setting: trial conducted in the USA. Inclusion criteria: spontaneous, elective or medically‐indicated labour induction; reassuring fetal heart rate at enrolment in study, fetal gestational age >= 38 weeks, maternal age 18 to 40 years, and pain scores of <= 3 with a numeric pain scale from 0 to 10. Exclusion criteria: first epidural dose after complete dilation, known fetal anomaly before birth, multiple gestation, non‐vertex presentation, maternal heart disease, administration of magnesium sulphate and poor comprehension of English. 59 women randomised (44 analysed). |
|
| Interventions |
“Immediate pushing”: after dilation of 10 cm was reached, the VAS was completed and women were then directed to begin pushing. Women were instructed to push 3 to 4 times during each contraction by bearing down in a manner similar to the bearing‐down effort used to have a bowel movement. No provider counting during pushing occurred. Both open and closed glottis methods were used, depending on participant's preference and effectiveness of pushing effort as determined by progressive fetal decent (33 women (28 included in analysis). “Delayed pushing”: after dilation of 10 cm was reached, the VAS was completed and women randomised were told to rest for 90 mins or until they felt an uncontrollable urge to push (whichever came first) before they began pushing. Instructions for pushing were provided in the same manner as for the immediate pushing group (26 women (16 included in the analysis). |
|
| Outcomes | Length of second stage, length of pushing perineal laceration third degree and fourth degree, mode of delivery vaginal and caesarean. | |
| Notes | Authors report "no financial relationships related to this article". | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomly assigned by a computerised random‐number generator to 1 of 2 groups before complete dilation. |
| Allocation concealment (selection bias) | Unclear risk | Not mentioned. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding of participants. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Other variables (length of second stage, length of pushing, spontaneous birth, perineal trauma, fetal Apgar) were obtained form existing medical records by unblinded investigators. Blinding was for fetal heart rate tracings (outcome not included in this review). |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 59 consented and randomised. Immediate 33. Delayed 26. 4 exclusion (immediate) ‐ 28. 10 exclusion (delayed) ‐ 16. Intention‐to‐treat analysis. |
| Selective reporting (reporting bias) | High risk | Incomplete results to enter in the meta‐analysis. |
| Other bias | Low risk | No other problems detected that could put the study at a risk of bias. |
Knauth 1986.
| Methods | RCT | |
| Participants |
Setting: trial conducted in the USA. Inclusion criteria: primigravidas between 20 and 30 years, 37‐42 weeks' gestation, who had attended a prepared childbirth program. Exclusion criteria: not mentioned. Not clear how many women were randomised; 94 women recruited, 27 included in the analysis. |
|
| Interventions |
“Breath in holding pushing”: take 2 deep breaths with the onset of each contraction; inhale deeply once more, let out a small amount of air, hold breath, close mouth; raise head, round shoulders, bring chin forward, place hands underneath knees letting legs abduct and relax, keep elbows out and bear down forcefully, consciously tightening the abdominal muscles; while pushing keep pelvis tilted and concentrate on relaxing pelvic floor and leg muscles; push as long and as hard as you can (about 10‐15 seconds); when you can no longer hold your breath, release your breath, inhale again, and repeat technique as long as contraction continues. At the end of the contractions, take 2 deep breaths and relax (10 women included in the analysis). “Exhalation pushing”: with the onset of each contraction begin to take normal, relaxing breaths. Continue until an urge to push is felt. At this point take a normal breath, hold it for a few seconds (2‐3), assume pelvic tilt position, bend head to chest; as you slowly exhale through pursed lips consciously pull in abdominal muscles. Direct effort through area where pressure is felt, usually rectum; continue to exhale slowly in a controlled manner with a crescent effect, increasing the volume exhaled gradually. Practice exhaling into fist as if blowing a trumpet. During this time continue to assume pelvic tilt position, contract abdominal muscles, and relax pelvic floor muscles ‐ keep chin forward and jaw relaxed. At the end of exhalation, quickly inhale, and repeat previous pattern as long as an urge to push is felt. At the end of contraction, take 2 normal breaths, relax (17 women included in the analysis). |
|
| Outcomes | Length of second stage (incomplete). | |
| Notes | Sources of funding not clear. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "subjects were randomly divided into two groups". |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment and the onset of the randomisation process were not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No Blinding of participants. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not mentioned. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 94 recruited. 67 dropped*. 27 stayed. 10 control group. 17 intervention group. |
| Selective reporting (reporting bias) | High risk | Important outcomes are missing and incomplete results. |
| Other bias | Low risk | No other problems detected that could put the study at a risk of bias. |
Lam 2010.
| Methods | RCT | |
| Participants |
Setting: trial conducted in Hong Kong. 396 nulliparous women were enrolled into this study. 73 women completed the study randomly allocated to either the directed pushing group (n = 38) or spontaneous pushing group (n = 35). Inclusion criteria: nulliparous women aged 18‐40 years with a healthy singleton baby (cephalic presentation), at full term, planned vaginal birth and be able to read Chinese or English. Labour could be spontaneous, or induced as a result of either premature rupture of membranes or post dates pregnancy. Exclusion criteria: not wishing to participate, already in established labour, epidural analgesia, maternal complications (medical or obstetric) which could potentially affect management of labour during the second stage. Suspected fetal compromise or having a baby with congenital anomalies. |
|
| Interventions |
“Directed pushing”: when it was confirmed that the cervix was fully dilated and the fetal head station was assessed as being plus 1 below the level of the ischial spines of the pelvis, the midwife suggested the woman commenced pushing using the directed pushing technique regardless of whether she felt an urge to push or not (38 women). “Spontaneous pushing”: when it was confirmed that the cervix was fully dilated and the fetal head station was assessed as being plus 1 below the level of the ischial spines of the pelvis, the midwife suggested the woman commenced pushing only when she felt the urge to do so and gave no specific instructions about the timing and duration of pushing (35 women). In both groups, if midwives or obstetricians were concerned about the maternal and/or fetal well‐being at any time, or delivery was not imminent after 60 mins (prolonged second stage of labour), the woman was reassessed to gauge maternal and fetal condition and adopt whatever clinical management was deemed necessary to facilitate a safe birth. |
|
| Outcomes | Length of second stage, admission to NICU, spontaneous vaginal delivery. | |
| Notes | Funding source not stated. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Randomisation upon full dilation of the cervix. The woman was asked to select 1 envelope from a set of 20. |
| Allocation concealment (selection bias) | Unclear risk | It is not clear who conducted the randomisation. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not mentioned. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | "396 eligible nulliparous women consented to take part in the study... Among these, 97 chose epidural analgesia during the first stage of labour. Another 117 did not continue with the study at different stages. The major reasons for discontinuation included 51 who were admitted in active labour, 17 who had suspected fetal distress, moderate meconium‐stained liquor, or a non‐reassuring cardiotocography during the second stage of labour. Overall, 73 women successfully completed the four fatigue assessment forms." |
| Selective reporting (reporting bias) | High risk | There are incomplete results to put in meta‐analysis. |
| Other bias | Low risk | No other problems detected that could put the study at a risk of bias. |
Low 2013.
| Methods | RCT | |
| Participants |
Setting: trial conducted in the USA. Inclusion criteria: 18 years of age, no history of genitourinary pathology, continent during first 20 weeks of pregnancy by self‐report and continent at 20 weeks' gestation by negative standing stress test. First pregnancy. Exclusion criteria: ability to contract the pelvic floor muscles voluntarily as assessed by manual examination at 20 weeks' gestation. It was reported that 249 women were randomised (but data reported for only 145). |
|
| Interventions | There were 4 groups: 1. Directed group or coached group using a closed glottis Valsalva Maneuver, which was routine care provided at the recruitment hospital (data for 39 women); 2. Spontaneous group with instruction provided prenatally via a standardised training video. This method included instructing the woman to follow her bodily sensations and push as she felt the urge. Directions given to the woman in any form regarding her pushing position, length of pushing or how to hold her breath were discouraged. Statements such as "you are so strong" or "good work" were considered supportive, not directive and were allowed (data for 32 women); 3. prenatal perineal massage initiated in the third trimester with a standardised training regarding its use and then directed pushing during second‐stage labour (data for 34 women); 4. combination of group 2 and 3 treatment, with spontaneous pushing plus perineal massage (data for 40 women). |
|
| Outcomes | Second stage length, delivery method (vaginal and caesarean section). | |
| Notes | This study resulted in another report: a secondary analysis 1‐year follow‐up to assess the fecal incontinence, but this report did not contribute to the analysis because this secondary analysis did not distinguish between the groups. The authors reported no conflict of interest. Reported funding from the Natinal Institute of Nursing Research. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated table. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not described. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | The provider was informed of group assignment of the woman upon admission to labour. The participants were not blinded to the group assignment. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Collection of self‐reports was blinded to the group assignment. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 41% for the follow‐up of 12 months. |
| Selective reporting (reporting bias) | High risk | The purpose of the trial was to test the effect of spontaneous pushing (either with or without prenatal perineal massage) compared to direct pushing on incontinence outcomes in women evaluated 1 year after their first birth. Birth data (including perineal lacerations and episiotomy) were reported for the study population overall but data were not reported by treatment group. A table reporting 'obstetric characteristics by treatment condition' is restricted to the following outcomes: epidural; second stage length; delivery method (vaginal/caesarean section). |
| Other bias | Low risk | No other problems detected that could put the study at a risk of bias. |
Maresh 1983.
| Methods | Quasi‐randomised trial. | |
| Participants |
Setting: trial conducted in UK. Inclusion criteria: at or beyond 37 weeks' gestation and singleton cephalic presentations. Exclusion criteria: no major obstetric complications. 76 women randomised. |
|
| Interventions |
“Early pushing group”: once full dilation of the cervix had been reached they were encouraged to push as soon as they had the desire (40 women). “Delayed pushing group”: continued to lie on their side and if they had the desire to bear down and the head was not visible on parting the labia, 1 epidural top‐up was allowed. Every 15 mins the vulva was inspected to see whether the head was visible. If, after 2 hours, the head was not visible, the labia were parted and a visual assessment of the level of the head was made. If at 2 subsequent 15 min‐inspections there appeared to be no further descent the patient was encouraged to push as soon as she had the desire (36 women). Pushing was managed in the routine labour ward manner. |
|
| Outcomes | Length of second stage, length of pushing, 5‐min Apgar score, mode of delivery vaginal, caesarean and forceps (straight and rotational). | |
| Notes | Funding source not specified. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Quasi‐randomised. According to the last digit of their hospital number: even numbers to group 1 (early pushing) and odd numbers to group 2 (late pushing). |
| Allocation concealment (selection bias) | High risk | No allocation concealment. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding of participants. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not mentioned. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not mentioned. |
| Selective reporting (reporting bias) | High risk | Incomplete results to be entered in the meta‐analysis. |
| Other bias | Low risk | No other problems detected that could put the study at a risk of bias. |
Mayberry 1999.
| Methods | RCT | |
| Participants |
Setting: trial conducted in the USA. Inclusion criteria: nulliparous women, English speaking, with healthy, singleton, and full‐term pregnancies. Exclusion criteria: evidence of fetal complications. 153 women randomised. |
|
| Interventions |
“Non‐delayed pushing group”: commencement of pushing efforts immediately following confirmation of full cervical dilation, regardless of the presence or lack of bearing‐down pressures experienced (72 women). “Delayed pushing group”: commencement of directed pushing efforts (following confirmation of full cervical dilation by the attending labour and delivery nurse, either after 1‐hour rest period or in the presence of involuntary pressure accompanied by the urge to bear down (81 women). Type of pushing: breath holding no longer than 6‐8 seconds, with a documented adequate contraction pattern (minimum of 3 to a maximum of 5 uterine contractions in 10‐min period or a Montevideo score of 95 to 395 mmHg; average of 200 to 250 mmHg) if and change bed positions at least every 20 to 30 mins. |
|
| Outcomes | Length of second stage, perineal laceration third degree, mode of delivery vaginal, caesarean and instrumental. | |
| Notes | Reported to be funded by A School of Nursing Grant. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | “…Using sets of sealed envelopes (containing assignments based on sequences of random numbers).“ The randomisation process occurred before 8 cm dilation. |
| Allocation concealment (selection bias) | Low risk | “…prepared for each site by the research team biostatistician.” |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding of participants. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not mentioned. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not mentioned. |
| Selective reporting (reporting bias) | High risk | Incomplete results to enter in the meta‐analysis. |
| Other bias | Low risk | No other problems detected that could put the study at a risk of bias. |
Plunkett 2003.
| Methods | RCT | |
| Participants |
Setting: trial conducted in the USA. Inclusion criteria: nulliparous women at term with a fetus in a cephalic presentation and who received neuraxial analgesia. Exclusion criteria: women with gestational or pre‐gestational diabetes mellitus or a contraindication to pushing in the second stage were excluded. 202 women randomised. |
|
| Interventions |
“Immediate pushing group”: were encouraged to begin pushing efforts upon reaching complete dilatation (85 women). “Delayed pushing group”: were instructed to wait until they appreciated a strong urge to push, defined as 50 mm or greater on an unmarked 100 mm VAS. The limits of the scale were verbally defined as no urge to push (0 mm) and an overwhelming urge to push (100 mm). If patients did not feel a strong urge to push after 90 mins, they were asked to start pushing without an urge (117 women). |
|
| Outcomes | Umbilical artery pH < 7.1, admission to NICU, mode of delivery vaginal, caesarean, postpartum haemorrhage. | |
| Notes | Reported to be funded by a National Research Service Award from the Agency for Healthcare Research and Quality. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomised assignments were determined through the use of a computer‐generated random numbers table. |
| Allocation concealment (selection bias) | Low risk | Assignments were kept in opaque envelopes until after patient consent was obtained. There is no report when the randomisation process started. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding of participants. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not mentioned. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 202: consented to participate. 117: delayed pushing. 85: pushing immediately. |
| Selective reporting (reporting bias) | High risk | Incomplete results to be entered in the meta‐analysis. |
| Other bias | Low risk | No other problems detected that could put the study at a risk of bias. |
Ravindran 1981.
| Methods | RCT | |
| Participants |
Setting: trial conducted in the USA. The women ranged from 17 to 25 years of age and were primigravidas or secundigravidas. 200 women randomised. |
|
| Interventions |
Group 1: were encourage to bear down with the uterine contractions and deliver the infant spontaneously (100 women). Group 2: were urged not to bear down following administration of spinal anaesthesia (100 women). |
|
| Outcomes | Postlumbar puncture headache. | |
| Notes | This study did not contribute to the analysis. Lumbar puncture was done upon "crowning of the fetal head" with the patient in the sitting position. Sources of funding not specified. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | The patients were randomly assigned to 1 group or the other. |
| Allocation concealment (selection bias) | Unclear risk | Not clear who conducted the randomisation. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not mentioned. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not mentioned. |
| Selective reporting (reporting bias) | High risk | It only shows the results for postlumbar puncture headache. |
| Other bias | Low risk | No other problems detected that could put the study at a risk of bias. |
Schaffer 2005.
| Methods | RCT | |
| Participants |
Setting: trial conducted in USA. Inclusion criteria: nulliparous women, between 36 and 41 weeks, singleton fetus in cephalic presentation, regular uterine contractions with cervical dilatation of at least 4 cm. Exclusion criteria: prior history of urinary incontinence, anal incontinence, pelvic organ prolapsed, any known complication of pregnancy, estimated fetal weight greater than 4000 g/use of oxytocin or epidural analgesia and chorioamnionitis prior to the 2nd stage. 325 women randomised (320 some data, 128 in analysis at 3 months postpartum). |
|
| Interventions |
“Coached pushing”: pushing using a closed glottis ‐ take a deep breath and hold during the peak of a contraction the bear down and push for 10 seconds; repeat this as long as the contraction continues. Coach patient to pull back on both knees and tuck her chin in while the provider or partner supports the legs (not clear, data for 157 for some outcomes, 67 for 3 months postpartum analysis). “Uncoached pushing”: not given specific instructions on pushing technique ‐ “do what comes naturally” or” whatever the patient feels the urge to do while in bed.” (Some data for 163 women, data for 61 at 3 months postpartum.) |
|
| Outcomes | Length of second stage, episiotomy, perineal laceration first, second, third and fourth degree, 5‐min Apgar score, Umbilical artery pH 7.1, admission to NICU, mode of delivery vaginal, caesarean and forceps from 1 report (2005) and Urodynamic results 3 months postpartum: Detrusor overactivity, urinary stress incontinence from the other report (2006). | |
| Notes | This study was the result of the primary outcome to see the difference in the maximal urethral closure pressure between the coached and uncoached group. The sample was calculated to obtain a 3‐month postpartum urodynamic testing of 106 women. So to ensure enough women to their postpartum evaluation, it was estimated that about 3 times the number of women actually required should be recruited to the randomised phase. The study was terminated when the sample size for urethral closure pressure had been obtained. This study resulted in 2 publications: 1 in 2005 with 128 women and the other 1 in 2006 with 320 woman. 1 report (Wai 2011) did not contribute to the analysis because this secondary analysis is from data of both groups (coached and uncoached) together. Sources of funding not specified. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation scheme in blocks of 10 patients. |
| Allocation concealment (selection bias) | Low risk | Assigment was masked to the providers by use of opaque envelopes at the onset of the second stage of labour. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding for the participants and key study personnel. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Blinding for the outcome assessment. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 1534 were screened. 988 consented. 546 declined to participate. 325 stayed. 128 returned for the 3‐month postpartum. 67 coached. 61 uncoached. 97 did not returned (29.84%). Intention‐to‐treat analysis. |
| Selective reporting (reporting bias) | Low risk | No selective reporting. |
| Other bias | Low risk | No other problems detected that could put the study at a risk of bias. |
Simpson 2005.
| Methods | RCT | |
| Participants |
Setting: trial conducted in the USA. Inclusion criteria: nulliparous women at term (> 37 weeks' gestation) in the second stage of labour with a singleton fetus in a vertex presentation who were having an elective induction of labour, and had a reassuring fetal heart rate pattern at the time of enrolment. Exclusion criteria: women with medical or obstetrical complications or a maternal condition that could potentially influence oxygen saturation including history of smoking, asthma, chronic or acute pulmonary, or cardiac disease. 45 women randomised. |
|
| Interventions |
“Immediate pushing group”: use closed‐glottis pushing 3 to 4 times during each contractions immediately when cervical dilation reached 10 cm and to continue pushing using this method with each contraction until birth. The nurse counted to 10 during each pushing effort to assist the woman in holding her breath for at least 10 seconds (22 women). “Delayed pushing group”: women were assisted to a left lateral position at 10 cm where they remained until they felt the urge to push or the second stage had lasted 2 hours (whichever came first). Then they were encouraged by the nurse to bear down with contractions without holding their breath (open‐glottis) for no more than 6‐8 seconds and continue bearing down no more than 3 times with each contraction until birth (23 women). |
|
| Outcomes | Length of second stage, length of pushing. | |
| Notes | Research funded by a grant from the American Nurses Foundation sponsored by GlaxoSmithKline. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer–generated allocation. |
| Allocation concealment (selection bias) | Unclear risk | Not described (randomisation at 10 cm cervical dilation). |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding of participants. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not mentioned. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Eligible: 60. Declined participation: 4. Consented in early labour: 56. Enrolled and randomised: 45. CG: 22/TG: 23. No loss after randomisation. |
| Selective reporting (reporting bias) | High risk | Incomplete results to be entered in the meta‐analysis. |
| Other bias | Low risk | No other problems detected that could put the study at a risk of bias. |
Thomson 1993.
| Methods | RCT | |
| Participants |
Setting: trial conducted in UK. Inclusion criteria: aged 18 or over, primiparous, singleton pregnancy, > 37 weeks, cephalic presentation, no epidural, no maternal condition (obstetric or medical) or fetal condition which would affect the management of the second stage. Exclusion criteria: conception in‐vitro, where the baby was to be adopted or where a “ care order” was to be taken out on the baby after delivery, use of epidural. 32 women randomised. |
|
| Interventions |
“Valsalva group”: take a deep breath, hold it and push for as long as possible (17 women). “Exhalation pushing”: spontaneous pushing activity (15 women). If delivery is not imminent in 90 min please adopt whatever clinical management you and the woman think fit. If you are concerned about maternal and/or fetal well‐being at any time please discontinue the trial and institute normal clinical management for that situation. All women were free to adopt any position they wanted. |
|
| Outcomes | Length of second stage, mode of delivery vaginal, estimated blood loss. | |
| Notes | 1 report did not contribute to the data 1 it was a qualitative analysis. Source of funding not specified. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Table of random numbers. |
| Allocation concealment (selection bias) | Low risk | When the second stage was diagnosed the midwife was given a sealed piece of paper which contained the group of allocation and instructions. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding for the participants or the key study personnel. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not clear if it was blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 32 were recruited. 15 – IG. 17 ‐ CG. |
| Selective reporting (reporting bias) | High risk | The study included few main expected outcomes, but some were reported incompletely to be entered in a meta‐analysis. |
| Other bias | High risk | The main author was present: “in order to ensure reliability of group allocation AMT was present for all the second stages". |
Vause 1998.
| Methods | RCT | |
| Participants |
Setting: trial conducted in UK. Inclusion criteria: nulliparous women in spontaneous or induced labour, with a singleton fetus between 37 and 42 weeks of gestation, and with an effective epidural, were eligible. Exclusion criteria: women with a non vertex presentation, or any complication which might influence second stage management, such as raised blood pressure, heart disease, or a dural tap were excluded. 135 women randomised. |
|
| Interventions |
“Early pushing”: pushing would commence within 1 hour of full dilation, whether the vertex was visible or not (67 women). “Delayed pushing”: women were encouraged to rest without pushing for a maximum of 3 hours from the time of full dilation, unless the vertex was visible ate the introitus earlier (68 women). |
|
| Outcomes | Episiotomy, perineal laceration second degree, 5‐min Apgar score, admission to NICU, oxytocin use in second stage after randomisation, mode of delivery caesarean and forceps (nonrotational and rotational). | |
| Notes | Funding source not specified. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Numbered opaque sealed envelopes containing computer‐generated random allocations in a ratio of 1:1 in balanced blocks of 10. |
| Allocation concealment (selection bias) | Low risk | The randomisation was done either in the first stage or within 1 hour of the start of the second stage. Opaque sealed envelopes. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not mentioned. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 135 participated. 67 early pushing. 68 delayed pushing. |
| Selective reporting (reporting bias) | High risk | Incomplete results to be entered in the meta‐analysis including the key outcome. |
| Other bias | Low risk | No other problems detected that could put the study at a risk of bias. |
Vaziri 2016.
| Methods | RCT | |
| Participants |
Setting: trial conducted in Iran. Inclusion criteria: nulliparous mothers, live fetus with vertex presentation, gestational age of 37‐40 weeks, spontaneous labour. Exclusion criteria: chronic diseases, pregnancy complications (pre‐eclampsia and placental abruption), premature rupture of membranes, caesarean section. 72 women randomised. |
|
| Interventions |
Intervention group: women pushed when they felt the urge to push while being in the lateral position during pushing (36 women). Control group: women pushed from the onset of the second stage using the Valsalva method while being in the supine position, according tho the routine practice in the maternity unit (36 women). |
|
| Outcomes | Maternal outcomes: duration of the second stage, duration of pushing, pain, fatigue and pain severity in the second stage. Fetal outcomes: fetal heart rate patterns (late deceleration, variable deceleration, bradycardia and tachycardia), Apgar score and pH and pO2 of the umbilical cord blood. |
|
| Notes | Research supported by Shiraz University of Medical Sciences. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Stratified and block random sampling. |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 72 were randomised. 34 for the control group (lost of 2 participants). 35 for the intervention group (lost of 1 participant). |
| Selective reporting (reporting bias) | High risk | Incomplete results to be entered in the meta‐analysis. |
| Other bias | Low risk | No other problems detected that could put the study at a risk of bias. |
Yildirim 2008.
| Methods | RCT | |
| Participants |
Setting:trial conducted in Turkey. Researcher went into hospital twice a week during the day shift to recruit women who fitted the inclusion criteria. Inclusion criteria: low‐risk, primiparous, 38‐42 weeks' gestation, single vertex fetus, peso 2.500 e 3999. The study women had no knowledge or preparation about birth and pushing techniques. 100 women randomised. |
|
| Interventions | Pushing began in both groups with full dilatation of the cervix, when uterine contractions became intense, and the fetal head had completed its rotation and descended to at least the + 1 level in the pelvis. “Valsalva pushing”: women were encouraged and supported in using Valsalva‐type pushing in the second stage of labour (50 women). “Spontaneous pushing”: women were encouraged and supported to push spontaneously in the second stage of labour bearing down in response to contractions (50 women). If delivery is not imminent in 90 mins please adopt whatever clinical management you and the woman think fit. If you are concerned about maternal and/or fetal well‐being at any time please discontinue the trial and institute normal clinical management for that situation. |
|
| Outcomes | Length of second stage, length of pushing, episiotomy, 5‐min Apgar scores, umbilical arterial pH. | |
| Notes | All women delivered in the lithotomy position. The authors report 'increase in oxytocin dose' by treatment groups but not the outcome of 'oxytocin use'. The authors state only that there were no differences in oxytocin use between treatment arms. Reported to be supported by the Research Fund of Instanbul University, Turkey. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | The Valsalva and spontaneous groups were randomised using envelopes. The random sequence generation is not described. |
| Allocation concealment (selection bias) | Unclear risk | Randomisation at full dilation. Methods of allocation concealment not clear. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not clear. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 1920 were screened. 174 met the inclusion criteria. 74 declined to participate (13 had unplanned caesarean, 5 refused and 56 was not included because the study observation could not have been completed during the day shift). 100 stayed. |
| Selective reporting (reporting bias) | High risk | Incomplete data; 'use of oxytocin' not reported by treatment arm, only 'increase in oxytocin use'. |
| Other bias | Low risk | No other problems detected that could put the study at a risk of bias. |
min: minute NICU: neonatal intensive care unit RCT: randomised controlled trial VAS: visual analogue scale
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Aviram 2016 | This trial aimed to determine the effect of a dental support device use on the course of labour and delivery. It does not report the type of pushing used. |
| Barnett 1982 | Not a randomised controlled trial. It does not report the randomisation method. It is only describe: "the study continued until 10 women who met both the pregnancy and labour criteria were monitored". |
| Boulvain 1998 | Study only present in abstract form. |
| Caldeyro Barcia 1990 | Not a randomised controlled trial. The 2 groups (spontaneous versus directed) were matched by the investigators. |
| Chang 2011 | Quasi‐experimental study. |
| Gleeson 1991 | Not a randomised controlled trial. |
| Haseeb 2014 | Quasi‐experimental study. |
| Lai 2009 | Not a randomised controlled trial. Women were assigned into 1 of the 2 groups based on their personal choice once full dilation was confirmed. |
| Liston 1987 | Study present in abstract form and registration of a controlled trial. |
| Martinez Lopez 1984 | Not a randomised controlled trial. Randomisation not stated. |
| Matsuo 2009 | Intervention: use of a support dental device compared to non‐use in active pushing phase of second stage. Both groups were coached on Valsalva maneuver during contraction. |
| Mc Queen 1977 | Letter to the editor and uncertain methodology. |
| Moraloglu 2016 | The aim of this study was to compare different positions (squatting versus supine). It does not report the type of pushing used in both groups. |
| Mulvey 2008 | Registration of clinical trial recruiting participants. The intervention was the McRobert's manoeuvre ‐ there is no evidence that the trial was completed. |
| Parnell 1993 | The randomisation was broken and the final analysis did not follow the initial allocation by the randomisation. |
| Phipps 2009 | Different type of intervention. The intervention was antenatal education with Valsalva maneuver and relaxed pelvic floor compared to control with no education. Both groups (intervention and control) pushed spontaneously in second stage according to standard of care from the labour ward. |
| Pickrell 1989 | Study presented in abstract form. |
| Snyder 1996 | Registration of an ongoing trial ‐ there is no evidence that the trial was completed. |
| Spiby 1990 | Registration of an ongoing trial ‐ there is no evidence that the trial was completed. |
| Walker 2012 | The method of pushing was the same in both groups. Most of the women did not feel the urge to push as a consequence of epidural anaesthesia and the push was directed by midwives not allowing any delayed time. |
| Yeates 1984 | Not a randomised controlled trial. |
Characteristics of ongoing studies [ordered by study ID]
Cahill 2014.
| Trial name or title | Optimizing management of the 2nd Stage of labor: multicenter randomized trial (OMSS). |
| Methods | Large, multicentre, randomised clinical trial. |
| Participants |
|
| Interventions | Compare immediate versus delayed pushing in the second stage of labour. |
| Outcomes | Primary: spontaneous vaginal delivery. Secondary:
|
| Starting date | May 2014 |
| Contact information | Alison G. Cahill (cahilla@wudosis.wustl.edu) and Methodius G. Tuuli (tuulim@wudosis.wustl.edu) |
| Notes | NCT02137200 on ClinicalTrials.gov Archive site. |
Hauspurg 2014.
| Trial name or title | Passive descent in obese nulliparous gravidae. |
| Methods | Randomised trial, single‐blind (investigator). |
| Participants | Obese (body mass index greater than or equal to 30), Nulliparous, gestational age of 37 weeks and greater, singleton pregnancy, regional anaesthesia. |
| Interventions | Compare passive descent versus immediate pushing. |
| Outcomes | Primary: spontaneous vaginal delivery. Secondary: rate of infections, third and fourth degree lacerations, postpartum haemorrhage, admission to NICU, umbilical cord pH < 7.1. |
| Starting date | Not provided. |
| Contact information | Alisse Hauspurg ahauspurg@wihri.org |
| Notes |
NICU: neonatal intensive care unit
Differences between protocol and review
We followed the pre‐specified protocol, however after an exhaustive reading and examination of the studies we added four more maternal secondary outcomes (duration of pushing, maternal satisfaction, fatigue after delivery and detrusor overactivity, and one more neonatal secondary outcome (need for resuscitation) because we judged them to be clinically important in contributing to the overall evidence. We also add total care costs as a secondary outcome.
We clarified the maternal secondary outcome "mode of delivery" to include spontaneous vaginal delivery, instrumental delivery, rotational or midpelvic or posterior forceps and caesarean delivery in order to allow for clearer analyses. For the maternal primary outcome "perineal trauma", we separated this outcome into two: perineal lacerations of third or fourth degree and episiotomy to show transparency in the findings.
To provide a better understanding of the available evidence we added one subgroup analysis:
parity (nulliparous, primiparous and multiparous with or without epidural analgesia) for three maternal outcomes: duration of the second stage, duration of pushing and spontaneous vaginal delivery.
We changed our inclusion criteria to include randomised controlled trials using a cluster‐randomised design, but none were identified. We added methods to the Unit of analysis issues section to clarify how we will handle such data in future updates, if appropriate.
We also used a statistical method to estimate means and standard deviations from the studies that showed the results as medians (Hozo 2005) and therefore we had to perform a sensitivity analyses for the outcomes that had used this method. A sensitivity analysis was performed for the outcomes "duration of second stage" and "duration of pushing" from Comparison 2: Timing of pushing: delayed pushing versus immediate pushing (all women with epidural analgesia).
We carried out another sensitivity analysis to explore the effect of trial quality for outcomes "duration of second stage" and "duration of pushing". In the review protocol, only quasi‐randomised trials were excluded. For this update, we excluded any trials which were assessed as being at high risk for random sequence generation and allocation concealment as we felt this criteria was more transparent.
We will carry out a further sensitivity analysis in future updates if cluster‐randomised trials are included in meta‐analysis along with individually‐randomised trials.
We planned to carry out a sensitivity analysis to explore the effects of fixed‐effect or random‐effects analyses for outcomes with statistical heterogeneity but instead used random‐effects analysis where we identified substantial heterogeneity.
Contributions of authors
For the initial (Lemos 2015) version of this review, Andrea Lemos designed the review, wrote the protocol, and is the guarantor for the review. Melania Amorim designed the review and provided a clinical perspective. Armele Dornelas de Andrade designed the search strategies for the additional searching. Ariani Impieri de Souza provided a clinical perspective. José Eulálio Cabral‐Filho provided general advice on the protocol and designed the search strategies for the additional searching. Jailson Correia provided a methodological perspective, wrote the protocol and provided general advice on the protocol.
For this update, Andrea Lemos assessed the new trials eligibility and built the GRADE tables. Melania Amorim provided a clinical perspective. Armele Dornelas de Andrade provided a methodological perspective. Ariani Impieri de Souza provided a clinical perspective. José Eulálio Cabral‐Filho assessed the new trials eligibility and the quality of evidence. Jailson Correia provided a methodological perspective
Sources of support
Internal sources
Universidade Federal de Pernambuco, Physical Therapy Department ‐ Recife‐PE, Brazil.
Instituto de Medicina Integral Prof. Fernando Figueira‐ Recife‐PE, Brazil.
External sources
UNDP‐UNFPA‐UNICEF‐WHO‐World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP), Department of Reproductive Health and Research (RHR), World Health Organization, Switzerland.
Declarations of interest
Andrea Lemos ‐ none known.
Melania MR Amorim ‐ none known.
Armele Dornelas de Andrade ‐ none known.
Ariani I de Souza ‐ none known.
José Eulálio Cabral Filho ‐ none known.
Jailson B Correia ‐ received salary from Instituto de Medicina Integral Professor Fernando Figueira and a research scholarship from Conselho Nacional de Desenvolvimento Científico e Tecnológico.
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
Buxton 1988 {published data only}
- Buxton EJ, Redman CWE, Obhari M. Delayed pushing with lumbar epidural in labour‐ does it increase the incidence of spontaneous delivery?. Journal of Obstetrics and Gynaecology 1988;8:258‐61. [Google Scholar]
- Buxton EJ, Redman CWE, Obhrai M. Delayed pushing in the second stage: effect on fetal acid base status. Proceedings of Silver Jubilee British Congress of Obstetrics and Gynaecology; 1989 July 4‐7; London, UK. 1989:80.
Fitzpatrick 2002 {published data only}
- Fitzpatrick M, Harkin R, McQuillan K, O´Brien C, O´Connell PR, O´Herlihy C. A randomised clinical trial comparing the effects of delayed versus immediate pushing with epidural analgesia on mode of delivery and faecal continence. BJOG: an international journal of obstetrics and gynaecology 2002;109:1359‐65. [DOI] [PubMed] [Google Scholar]
- Fitzpatrick M, O'Brien C, McQuillan K, O'Connell PR, O'Herlihy C. Comparison of immediate and delayed pushing in second stage of labor on anal sphincter integrity and mode of delivery. American Journal of Obstetrics and Gynecology 2000;182(1 Pt 2):S37. [Google Scholar]
Fraser 2000b {published data only}
- Fraser WD, Marcoux S, Douglas J, Goulet C, Krauss I, for the PEOPLE Study Group. Multicentre trial of delayed pushing for women with continuous epidural. Acta Obstetricia et Gynecologica Scandinavica 1997;76 Suppl(167:1):45. [Google Scholar]
- Fraser WD, Marcoux S, Douglas J, Goulet C, Krauss I, for the PEOPLE Study Group. Multicentre trial of delayed pushing for women with continuous epidural. Society of Obstetricians and Gynaecologists of Canada, 54th Annual Meeting; 1988 June; Victoria, Canada. 1998:36.
- Fraser WD, Marcoux S, Krauss I, Douglas J, Goulet C, Boulvain M, for the PEOPLE (Pushing Early or Pushing Late with Epidural) Study Group. Multicenter randomized, controlled trial of delayed pushing for nulliparous women in the second stage of labor with continuous epidural analgesia. American Journal of Gynecology and Obstetrics 2000;182(5):1165‐72. [DOI] [PubMed] [Google Scholar]
- Ray C, Audibert F, Goffinet F, Fraser W. When to stop pushing? Consequences of pushing duration on maternal and neonatal outcomes in nullipara with epidural. American Journal of Obstetrics and Gynecology 2008;199(6 Suppl 1):S37. [DOI] [PubMed] [Google Scholar]
- Ray C, Audibert F, Goffinet F, Fraser W. When to stop pushing? effects of duration of second‐stage expulsion efforts on maternal and neonatal outcomes in nulliparas women with epidural analgesia. American Journal of Obstetrics and Gynecology 2009;201:361.e1‐361.e7. [DOI] [PubMed] [Google Scholar]
- Lin P, Newton W. Does delayed pushing reduce difficult deliveries for nulliparous women with epidural analgesia?. Journal of Family Practice 2000;49(9):783‐4. [PubMed] [Google Scholar]
- Petrou S, Coyle D, Fraser WD, for the PEOPLE (Pushing Early or Pushing Late with Epidural) study group. Cost‐effectiveness of a delayed pushing policy for patients with epidural anesthesia. American Journal of Obstetrics and Gynecology 2000;182(5):1158‐64. [DOI] [PubMed] [Google Scholar]
Gillesby 2010 {published data only}
- Gillesby E, Burns S, Dempsey A, Kirby S, Mogensen K, Naylor K, et al. Comparison of delayed versus immediate pushing during second stage of labor for nulliparous women with epidural anesthesia. Journal of Obstetric, Gynecologic and Neonatal Nursing 2010;39(6):635‐44. [DOI] [PubMed] [Google Scholar]
- Gillesby EJ, Mogensen KD, Burns SM, Kirby S, Naylor KS, Petrella JA, et al. Comparison of delayed versus immediate pushing during second stage of labor for nulliparous women with epidural anesthesia. JOGNN: Journal of Obstetric, Gynecologic & Neonatal Nursing 2010;39 Suppl 1:S87. [DOI] [PubMed] [Google Scholar]
Goodfellow 1979 {published data only}
- Goodfellow CF, Studd C. The reduction of forceps in primigravidae with epidural analgesia‐a controlled trial. British Journal of Clinical Practice 1979;33(10):287‐8. [PubMed] [Google Scholar]
Hansen 2002 {published data only}
- Hansen SL, Clark SL, Foster JC. Active pushing versus passive fetal descent in the second stage of labor: a randomized controlled trial. Obstetric & Gynecology 2002;99(1):29‐34. [DOI] [PubMed] [Google Scholar]
Jahdi 2011 {published data only}
- Jahdi F, Shahnazari M, Kashanian M, Farahani MA, Haghani H. A randomized controlled trial comparing the physiological and direct pushing on the duration of the second stage of labor, the mode of delivery and Apgar score. International Journal of Collaborative Research on Internal Medicine & Public Health 2011;3(2):159‐64. [Google Scholar]
- Jahdi F, Shahnazari M, Kashanian M, Farahani MA, Haghani H. A randomized controlled trial comparing the physiological and directed pushing on the duration of the second stage of labor, the mode of delivery and Apgar score. International Journal of Nursing and Midwifery 2011;3(5):55‐9. [ISSN 2141‐2499] [Google Scholar]
Kelly 2010 {published data only}
- Kelly M, Johnson E, Lee V, Massey L, Purser D, Ring K, et al. Delayed versus immediate pushing in second stage of labor. MCN; American Journal of Maternal Child Nursing 2010;35(2):81‐8. [DOI] [PubMed] [Google Scholar]
Knauth 1986 {published data only}
- Knauth DG, Haloburdo EP. Effect of pushing techniques in birthing chair on length of second stage of labor. Nursing Research 1986;35:49‐51. [PubMed] [Google Scholar]
Lam 2010 {published data only}
- Lam CCO, McDonald SJ. Comparison of pushing techniques used in the second stage of labour for their effect on maternal perception of fatigue in the early postpartum period among Chinese women. Hong Kong Journal of Gynaecology, Obstetrics and Midwifery 2010;10(1):13‐21. [Google Scholar]
- Lam COC. Comparison of Two Pushing Techniques Used in the Second Stage of Labour for Their Effect on Maternal Perception of Fatigue in the Early Postpartum Period: a Randomised Controlled Trial [thesis]. Victoria: La Trobe University, 2006. [Google Scholar]
Low 2013 {published data only}
- Brincat C, Lewicky‐Gaupp C, Patel D, Sampselle C, Miller J, Delancey JO, et al. Fecal incontinence in pregnancy and post partum. International Journal of Gynaecology & Obstetrics 2009;106(3):236‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Low LK, Miller JM, Guo Y, Ashton‐Miller JA, DeLancey JOL, Sampselle CM. Spontaneous pushing to prevent postpartum incontinence: a randomized, controlled trial. International Urogynecology Journal 2013;24(3):453‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Low LK, Miller JM, Sampselle C. Prevention of post partum urinary incontinence using perineal massage, spontaneous pushing and muscle training. Female Pelvic Medicine & Reconstructive Surgery 2010;16(5 Suppl 2):S70. [Google Scholar]
- Low LK, Sampselle C, Miller JM. Spontaneous pushing during 2nd stage labor to reduce risk of incontinence. Female Pelvic Medicine and Reconstructive Surgery 2013; Vol. 19.
Maresh 1983 {published data only}
- Maresh M, Choong KH, Beard RW. Delayed pushing with lumbar epidural analgesia in labour. British Journal of Obstetrics and Gynaecology 1983;90:623‐7. [DOI] [PubMed] [Google Scholar]
Mayberry 1999 {published data only}
- Mayberry LJ, Hammer R, Kelly C, True‐Driver B, De A. Use of delayed pushing with epidural anesthesia: findings from a randomized, controlled trial. Journal of Perinatology 1999;19(1):26‐30. [DOI] [PubMed] [Google Scholar]
Plunkett 2003 {published data only}
- Plunkett B, Lin A, Wong C, Grobman W, Peaceman A. A randomized trial of the management of the second stage of labor in nulliparous patients with continuous epidural analgesia [abstract]. American Journal of Obstetrics and Gynecology 2001;184(1):S119. [DOI] [PubMed] [Google Scholar]
- Plunkett BA, Lin A, Wong CA, Grobman WA, Peaceman AM. Management of the second stage of labor in nulliparas with continuous epidural analgesia. Obstetrics & Gynecology 2003;102(1):109‐14. [DOI] [PubMed] [Google Scholar]
Ravindran 1981 {published data only}
- Ravindran RS, Viegas OJ, Tasch MD, Cline PH, Deaton RL, Brown TR. Bearing down at the time of delivery and the incidence of spinal headache in parturients. Anesthesia and Analgesia 1981;60(7):524‐6. [PubMed] [Google Scholar]
Schaffer 2005 {published data only}
- Bloom SL, Casey BM, Schaffer JI, McIntire DD, Leveno KJ. A randomized trial of coached versus uncoached maternal pushing during the second stage of labor. American Journal of Obstetrics and Gynecology 2006;194(1):10‐3. [DOI] [PubMed] [Google Scholar]
- Schaffer JI, Bloom SL, Casey BM, McIntire DD, Nihira MA, Leveno KJ. A randomized trial of the effects of coached vs uncoached maternal pushing during the second stage of labor on postpartum pelvic floor structure and function. American Journal of Obstetrics and Gynecology 2005;192:1692‐6. [DOI] [PubMed] [Google Scholar]
- Wai CY, McIntire DD, Atnip SD, Schaffer JI, Bloom SL, Leveno KJ. Urodynamic indices and pelvic organ prolapse quantification 3 months after vaginal delivery in primiparous women. International Urogynecology Journal 2011;22:1293‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Simpson 2005 {published data only}
- Simpson KR, James DC. Effects of immediate versus delayed pushing during second‐stage labor on fetal well‐being. Nursing Research 2005;54(3):149‐57. [DOI] [PubMed] [Google Scholar]
Thomson 1993 {published data only}
- Thomson AM. Comparison of 'Pushing' Techniques in the Second Stage of Labour: Pilot Study [MSc thesis]. Manchester, UK: University of Manchester, 1990. [Google Scholar]
- Thomson AM. A pilot study of a randomised controlled trial of pushing techniques in the second stage of labour. Proceedings of 22nd International Congress of Confederation of Midwives; 1991 Oct 7‐12; Kobe, Japan. 1991:76.
- Thomson AM. Maternal behaviour during spontaneous and directed pushing in the second stage of labour. Journal of Advanced Nursing 1995;22:1027‐34. [DOI] [PubMed] [Google Scholar]
- Thomson AM. Pushing techniques in the second stage of labour. Journal of Advanced Nursing 1993;18:171‐7. [DOI] [PubMed] [Google Scholar]
Vause 1998 {published data only}
- Vause S, Congdon HM, Thornton JG. A randomized controlled trial of immediate and delayed pushing in the second stage of labour for nulliparous women with epidural analgesia. British Journal of Obstetrics and Gynaecology 1998;105 Suppl 17:85. [DOI] [PubMed] [Google Scholar]
- Vause S, Congdon HM, Thornton JG. Immediate and delayed pushing in the second stage of labour for nulliparous women with epidural analgesia: a randomised controlled trial. British Journal of Obstetrics and Gynaecology 1998;105:186‐8. [DOI] [PubMed] [Google Scholar]
Vaziri 2016 {published data only}
- Vaziri F, Arzhe N, Asadi N, Pourahmad S, Moshfeghy Z. Spontaneous pushing in lateral position versus valsalva maneuver during second stage of labor on maternal and fetal outcomes: randomized clinical trial. Iranian Red Crescent Medical Journal 2016 in‐press. [DOI] [PMC free article] [PubMed]
Yildirim 2008 {published data only}
- Yildirim G, Beji NK. Effects of pushing techniques in birth on mother and fetus: a randomized study. Birth 2008;35:25‐30. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Aviram 2016 {published data only}
- Aviram A, Ashwal E, Hiersch L, Hadar E, Wiznitzer A, Yogev Y. The effect of intrapartum dental support use among nulliparous during the second stage of labor ‐ a randomized controlled study. Journal of Maternal‐Fetal & Neonatal Medicine 2016;29(6):868‐71. [DOI] [PubMed] [Google Scholar]
Barnett 1982 {published data only}
- Barnett MM, Humenick SS. Infant outcome in relation to second stage labor pushing method. Birth 1982;9:221‐8. [Google Scholar]
Boulvain 1998 {published data only}
- Boulvain M, Irion O, Mentha V. Multicentre randomised controlled trial of delayed pushing for women with continuous epidural analgesia. 21st Conference of the Swiss Society of Gynecology and Obstetrics; 1998; Switzerland. 1998:5.
Caldeyro Barcia 1990 {published data only}
- Caldeyro‐Barcia R. The effects of humanized labour on fetal outcome. Personal communication 1990.
Chang 2011 {published data only}
- Chang S‐C, Chou M‐M, Lin K‐C, Lin L‐C, Lin Y‐l, Kuo S‐C. Effects of a pushing intervention on pain, fatigue and birthing experiences among Taiwanese women during the second stage of labour. Midwifery 2011;27:825‐31. [DOI] [PubMed] [Google Scholar]
Gleeson 1991 {published data only}
- Gleeson NC, Griffith AP. The management of the second stage of labour in primiparae with epidural analgesia. British Journal of Clinical Practice 1991;45(2):90‐1. [PubMed] [Google Scholar]
Haseeb 2014 {published data only}
- Haseeb Y, Alkunaizi A, Al Turki H, Aljama F, Sobhy S. The impact of valsalva's versus spontaneous pushing techniques during second stage of labor on postpartum maternal fatigue and neonatal outcome. Saudi Journal of Medicine and Medical Sciences 2014;2(2):101‐5. [Google Scholar]
Lai 2009 {published data only}
- Lai ML, Lin K, Li HY, Shey K, Gau M. Effects of delayed pushing during the second stage of labor on postpartum fatigue and birth outcomes in nulliparous women. Journal of Nursing Research 2009;17(1):62‐72. [DOI] [PubMed] [Google Scholar]
Liston 1987 {published data only}
- Liston RM. Effect of delayed expulsive efforts on rate of spontaneous delivery with continuous epidural analgesia. Personal communication 1996.
- Liston RM, Writer WDR, Young DC, McNeil K. Delayed maternal pushing does not reduce mid‐forceps rate. Proceedings of 19th Annual Meeting of Society for Obstetric Anesthesia and Perinatology; 1987 May 20‐23; Halifax, Nova Scotia, Canada. 1987:94.
Martinez Lopez 1984 {published data only}
- Martinez‐Lopez V, Fuente P, Iniguez A, Freese UE, Mendez‐Bauer C. Comparison of two methods of bearing down during second stage of labour. Proceedings of 31st Meeting of Society for Gynecologic Investigation; 1984; San Francisco, California, USA. 1984:Abstract no: 76P.
Matsuo 2009 {published data only}
- Matsuo K, Mudd JV, Kopelman JN, Atlas RO. Duration of second stage of labor while wearing a dental support device: a pilot study. Journal of Obstetrics and Gynaecology Research 2009;35(4):672‐8. [DOI] [PubMed] [Google Scholar]
Mc Queen 1977 {published data only}
- Queen J, Myrlea L. Lumbar epidural analgesia in labour. British Medical Journal 1977;1:640‐1. [PMC free article] [PubMed] [Google Scholar]
Moraloglu 2016 {published data only}
Mulvey 2008 {published data only}
- Mulvey SF. McRoberts manoeuvre or pushing study (McMOPS). ClinicalTrials.gov (accessed 7 November 2008).
Parnell 1993 {published data only}
- Parnell C, Langhoff‐Roos J, Iversen R, Damgaard P. Pushing in the expulsive phase of labour. Ugeskrift for Laeger 1993;155:2259‐62. [PubMed] [Google Scholar]
- Parnell C, Langhoff‐Roos J, Iversen R, Damgaard P. Pushing method in the expulsive phase of labor: a randomized trial. Acta Obstetricia et Gynecologica Scandinavica 1993;72:31‐5. [DOI] [PubMed] [Google Scholar]
- Parnell C, Langhoff‐Roos J, Iversen R, Damgaard P. Pushing method in the expulsive phase of labour. Acta Paediatrica 1992;Suppl 384:17. [DOI] [PubMed] [Google Scholar]
Phipps 2009 {published data only}
- Phipps H, Charlton S, Dietz HP. Can antenatal education influence how women push in labour? [abstract]. Journal of Paediatrics and Child Health 2007;43(Suppl 1):A67‐8. [DOI] [PubMed] [Google Scholar]
- Phipps H, Charlton S, Dietz HP. Can antenatal education influence how women push in labour? a pilot randomised controlled trial on maternal antenatal teaching for pushing in second stage of labour (PUSH STUDY). Australian and New Zealand Journal of Obstetrics and Gynaecology 2009;49:274‐8. [DOI] [PubMed] [Google Scholar]
Pickrell 1989 {published data only}
- Pickrell MD, Buxton EJ, Redman CWE, Obhrai M. Epidural analgesia: delayed pushing and augmentation in the second stage do not reduce operative deliveries. Proceedings of Silver Jubilee British Congress of Obstetrics and Gynaecology; 1989 July 4‐7; London, UK. 1989:128.
Snyder 1996 {published data only}
- Snyder S. Trial to compare two management techniques in the second stage of labor: pushing vs non‐pushing. Personal communication 1996.
Spiby 1990 {published data only}
- Spiby H. A randomised controlled trial to evaluate the use of spontaneous bearing down efforts in the second stage of labour. Personal communication 1990.
Walker 2012 {published data only}
- Walker C, Rodríguez T, Herranz A, Espinosa JA, Sánchez E, Espuña‐Pons M. Alternative model of birth to reduce the risk of assisted vaginal delivery and perineal trauma. International Uroginecology Journal 2012;23(9):1249‐56. [DOI] [PubMed] [Google Scholar]
Yeates 1984 {published data only}
- Yeates DA, Roberts JE. A comparison of two bearing‐down techniques during the second stage of labor. Journal of Nurse‐Midwifery 1984;29(1):3‐11. [DOI] [PubMed] [Google Scholar]
References to ongoing studies
Cahill 2014 {published data only}
- NCT02137200. Optimizing management of the 2nd stage of labor: Multicenter randomized trial (OMSS). clinicaltrials.gov/ct2/show/NCT02137200 Date first received: 9 May 2014.
Hauspurg 2014 {published data only}
- Hauspurg A. Passive descent in obese nulliparous gravidae. ClinicalTrials.gov (http://clinicaltrials.gov/) [accessed 24 March 2014] 2014.
Additional references
Aderhold 1991
- Aderhold K, Roberts JE. Phases of second stage labor. Four descriptive case studies. Journal of Nurse‐Midwifery 1991;36:267‐75. [DOI] [PubMed] [Google Scholar]
Albers 2007
- Albers LL, Borders N. Minimizing genital tract trauma and related pain following spontaneous vaginal birth. Journal of Midwifery & Women's Health 2007;52:246‐53. [DOI] [PubMed] [Google Scholar]
Aldrich 1995
- Aldrich CJ, Spencer JAD, Wyatt JS, Delpy DT. The effect of maternal pushing on fetal cerebral oxygenation and blood volume during the second stage of labour. British Journal of Obstetrics and Gynaecology 1995;102:448‐53. [DOI] [PubMed] [Google Scholar]
Bates 1985
- Bates RG, Helms CW, Duncan A, Edmonds DK. Uterine activity in the second stage of labour and the effect of epidural analgesia. British Journal of Obstetrics and Gynaecology 1985;92:1246‐50. [DOI] [PubMed] [Google Scholar]
Beynon 1957
- Beynon C. The normal second stage of labour. A plea for reform in its conduct. Journal of Obstetrics and Gynaecology of the British Commonwealth 1957;64:815‐20. [DOI] [PubMed] [Google Scholar]
Bloom 2006
- Bloom SL, Casey BM, Schaffer JI, McIntire SS, Leveno KJ. A randomized trial of coached versus uncoached maternal pushing during the second stage of labor. American Journal of Obstetrics and Gynecology 2006;194(1):10‐3. [DOI] [PubMed] [Google Scholar]
Brancato 2008
- Brancato RM, Church S, Stone PW. A meta‐analysis of passive descent versus immediate pushing in nulliparous women with epidural analgesia in the second stage of labor. JOGN: Journal of Obstetric, Gynecologic & Neonatal Nursing 2008;37(1):4‐12. [DOI] [PubMed] [Google Scholar]
Brincat 2009
- Brincat C, Lewicky‐Gaupp C, Patel D, Sampselle C, Miller J, Delancey JO, et al. Fecal incontinence in pregnancy and post partum. International Journal of Gynaecology & Obstetrics 2009;106(3):236‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Buhimschi 2002
- Buhimschi CS, Buhimschi IA, Malinow AM. Pushing in labor: performance and not endurance. American Journal of Obstetrics and Gynecology 2002;186:1336‐44. [DOI] [PubMed] [Google Scholar]
Caldeyro‐Barcia 1981
- Caldeyro‐Barcia R, Giussi G, Storch E, Poseiro JJ, Lafaurie N, Kettenhuber K, et al. The bearing‐down efforts and their effects on fetal heart rate, oxygenation and acid base balance. Journal of Perinatal Medicine 1981;9:63‐7. [DOI] [PubMed] [Google Scholar]
Cunningham 2005
- Cunningham FG, Macdonald G. Williams Obstetrics. New York: McGraw‐Hill, 2001. [Google Scholar]
Fraser 2000a
- Fraser WD, Marcoux S, Krauss I, Douglas J, Goulet C, Boulvain M. Multicenter, randomized, controlled trial of delayed pushing for nulliparous women in the second stage of labour with continuous epidural analgesia. American Journal of Obstetrics and Gynecology 2000;182(5):1165‐72. [DOI] [PubMed] [Google Scholar]
Gupta 2012
- Gupta JK, Hofmeyr GJ, Shehmar M. Position in the second stage of labour for women without epidural anaesthesia. Cochrane Database of Systematic Reviews 2012, Issue 5. [DOI: 10.1002/14651858.CD002006.pub3] [DOI] [PubMed] [Google Scholar]
Hansen 2002
- Hansen SL, Clark SL, Foster JC. Active pushing versus passive fetal descent in the second stage of labor: a randomized controlled trial. Obstetrics & Gynecology 2002;99:29‐34. [DOI] [PubMed] [Google Scholar]
Hanson 2009
- Hanson L. Second‐stage labor care. Challenges in spontaneous bearing down. Journal of Perinatal & Neonatal Nursing 2009;23:31‐9. [DOI] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Hozo 2005
- Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of sample. BMC Medical Research Methodology 2005;5:1‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lai 2009
- Lai M, Lin K, Li HY, Shey KS, Gau M. Effects of delayed pushing during the second stage of labor on postpartum fatigue and birth outcomes in nulliparous women. Journal of Nursing Research 2009;17:62‐71. [DOI] [PubMed] [Google Scholar]
Le Ray 2008
- Ray C, Audibert F, Goffinet F, Fraser W. When to stop pushing? Consequences of pushing duration on maternal and neonatal outcomes in nullipara with epidural. American Journal of Obstetrics and Gynecology 2008;199(6 Suppl 1):S37. [DOI] [PubMed] [Google Scholar]
Menez‐Orieux 2005
- Menez‐Orieux C, Linet T, Philippe H‐J, Boog G. Delayed versus immediate pushing in the second stage of labor for nulliparous parturients with epidural analgesia: a meta‐analysis of randomized trials [Poussée retardée versus poussée immédiate lors de la seconde phase du travail chez les nullipares sus anesthesie péridurale]. Journal de Gynecologie, Obstetrique et Biologie de la Reproduction 2005;34(5):440‐7. [DOI] [PubMed] [Google Scholar]
Minato 2001
- Minato JF. Is it time to push? Examining rest in second‐stage labor. AWHONN Lifelines 2001;4:20‐3. [DOI] [PubMed] [Google Scholar]
Petrou 2000
- Petrou S, Coyle D, Fraser WD, for the PEOPLE (Pushing Early or Pushing Late with Epidural) study group. Cost‐effectiveness of a delayed pushing policy for patients with epidural anesthesia. American Journal of Obstetrics and Gynecology 2000;182(5):1158‐64. [DOI] [PubMed] [Google Scholar]
Prins 2011
- Prins M, Boxem J, Lucas C, Hutton E. Effect of spontaneous pushing versus Valsalva pushing in the second stage of labour on mother and fetus: a systematic review of randomised trials. BJOG: an international journal of obstetrics and gynaecology 2011;118(6):662‐70. [DOI] [PubMed] [Google Scholar]
RevMan 2014 [Computer program]
- The Nordic Cochrane Centre: The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre: The Cochrane Collaboration, 2014.
Roberts 2004
- Roberts CL, Torvaldsen S, Cameron CA, Olive E. Delayed versus early pushing in women with epidural analgesia: a systematic review and meta‐analysis. BJOG: an international journal of obstetrics and gynaecology 2004;111:1333‐40. [DOI] [PubMed] [Google Scholar]
Roberts 1987
- Roberts J, Goldstein SA, Gruener JS. A descriptive analysis of involuntary bearing‐down efforts during the expulsive phase of labor. Journal of Obstetric, Gynecologic, and Neonatal Nursing 1987;16:48‐55. [DOI] [PubMed] [Google Scholar]
Roberts 1996
- Roberts J, Woolley D. A second look at the second stage of labor. Journal of Obstetric, Gynecologic, and Neonatal Nursing 1996;25:415‐23. [DOI] [PubMed] [Google Scholar]
Roberts 2002
- Roberts JE. The “push” for evidence: management of the second stage. Journal of Midwifery and Womens Health 2002;47:2‐15. [DOI] [PubMed] [Google Scholar]
Roberts 2007
- Roberts J, Hanson L. Best practices in second stage labour care: maternal bearing down and positioning. Journal of Midwifery & Women's Health 2007;52(3):238‐45. [DOI: 10.1016/j.jmwh.2006.12.011] [DOI] [PubMed] [Google Scholar]
Schaffer 2005b
- Schaffer JI, Bloom SL, Casey BM, McIntire DD, Nihira MA, Leveno KJ. A randomized trial of the effects of coached vs uncoached maternal pushing during the second stage of labor on postpartum pelvic floor structure and function. American Journal of Obstetrics and Gynecology 2005;192:1692‐6. [DOI] [PubMed] [Google Scholar]
Thompson 1995
- Thompson AM. Pushing techniques in the second stage of labour. Journal of Advanced Nursing 1995;22:1027‐34. [DOI] [PubMed] [Google Scholar]
Thorp 1996
- Thorp JA, Breedlove G. Epidural analgesia in labour: an evaluation on risks and benefits. Birth 1996;23:63‐83. [DOI] [PubMed] [Google Scholar]
Tuuli 2012
- Tuuli MG, Frey HA, Odibo AO, Macones GA, Cahill AG. Immediate compared with delayed pushing in the second stage of labor. Obstetrics & Gynecology 2012;120(3):660‐8. [DOI] [PubMed] [Google Scholar]
Wai 2011
- Wai CY, McIntire DD, Atnip SD, Schaffer JI, Bloom SL, Leveno KJ. Urodynamic indices and pelvic organ prolapse quantification 3 months after vaginal delivery in primiparous women. International Urogynecology Journal 2011;22:1293‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to other published versions of this review
Lemos 2011
- Lemos A, Amorim MMR, Dornelas de Andrade A, Souza AI, Cabral Filho JE, Correia JB. Pushing/bearing down methods for the second stage of labour.. Cochrane Database of Systematic Reviews 2011, Issue 5. [DOI: 10.1002/14651858.CD009124] [DOI] [Google Scholar]
Lemos 2015
- Lemos A, Amorim MMR, Dornelas de Andrade A, Souza AI, Cabral Filho JE, Correia JB. Pushing/bearing down methods for the second stage of labour. Cochrane Database of Systematic Reviews 2015, Issue 10. [DOI: 10.1002/14651858.CD009124.pub2] [DOI] [PubMed] [Google Scholar]