

Abstract
Background
According to the latest revised National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer's Disease and Related Disorders Association (now known as the Alzheimer's Association) (NINCDS‐ADRDA) diagnostic criteria for Alzheimer's disease dementia of the National Institute on Aging and Alzheimer Association, the confidence in diagnosing mild cognitive impairment (MCI) due to Alzheimer's disease dementia is raised with the application of biomarkers based on measures in the cerebrospinal fluid (CSF) or imaging. These tests, added to core clinical criteria, might increase the sensitivity or specificity of a testing strategy. However, the accuracy of biomarkers in the diagnosis of Alzheimer’s disease dementia and other dementias has not yet been systematically evaluated. A formal systematic evaluation of sensitivity, specificity, and other properties of plasma and CSF amyloid beta (Aß) biomarkers was performed.
Objectives
To determine the accuracy of plasma and CSF Aß levels for detecting those patients with MCI who would convert to Alzheimer's disease dementia or other forms of dementia over time.
Search methods
The most recent search for this review was performed on 3 December 2012. We searched MEDLINE (OvidSP), EMBASE (OvidSP), BIOSIS Previews (ISI Web of Knowledge), Web of Science and Conference Proceedings (ISI Web of Knowledge), PsycINFO (OvidSP), and LILACS (BIREME). We also requested a search of the Cochrane Register of Diagnostic Test Accuracy Studies (managed by the Cochrane Renal Group).
No language or date restrictions were applied to the electronic searches and methodological filters were not used so as to maximise sensitivity.
Selection criteria
We selected those studies that had prospectively well defined cohorts with any accepted definition of cognitive decline, but no dementia, with baseline CSF or plasma Aß levels, or both, documented at or around the time the above diagnoses were made. We also included studies which looked at data from those cohorts retrospectively, and which contained sufficient data to construct two by two tables expressing plasma and CSF Aß biomarker results by disease status. Moreover, studies were only selected if they applied a reference standard for Alzheimer's dementia diagnosis, for example the NINCDS‐ADRDA or Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM‐IV) criteria.
Data collection and analysis
We screened all titles generated by the electronic database searches. Two review authors independently assessed the abstracts of all potentially relevant studies. We assessed the identified full papers for eligibility and extracted data to create standard two by two tables. Two independent assessors performed quality assessment using the QUADAS‐2 tool. Where data allowed, we derived estimates of sensitivity at fixed values of specificity from the model we fitted to produce the summary receiver operating characteristic (ROC) curve.
Main results
Alzheimer's disease dementia was evaluated in 14 studies using CSF Aß42. Of the 1349 participants included in the meta‐analysis, 436 developed Alzheimer’s dementia. Individual study estimates of sensitivity were between 36% and 100% while the specificities were between 29% and 91%. Because of the variation in assay thresholds, we did not estimate summary sensitivity and specificity. However, we derived estimates of sensitivity at fixed values of specificity from the model we fitted to produce the summary ROC curve. At the median specificity of 64%, the sensitivity was 81% (95% CI 72 to 87). This equated to a positive likelihood ratio (LR+) of 2.22 (95% CI 2.00 to 2.47) and a negative likelihood ratio (LR–) of 0.31 (95% CI 0.21 to 0.48).
The accuracy of CSF Aß42 for all forms of dementia was evaluated in four studies. Of the 464 participants examined, 188 developed a form of dementia (Alzheimer’s disease and other forms of dementia).The thresholds used were between 209 mg/ml and 512 ng/ml. The sensitivities were between 56% and 75% while the specificities were between 47% and 76%. At the median specificity of 75%, the sensitivity was estimated to be 63% (95% CI 22 to 91) from the meta‐analytic model. This equated to a LR+ of 2.51 (95% CI 1.30 to 4.86) and a LR– of 0.50 (95% CI 0.16 to 1.51).
The accuracy of CSF Aß42 for non‐Alzheimer's disease dementia was evaluated in three studies. Of the 385 participants examined, 61 developed non‐Alzheimer's disease dementia. Since there were very few studies and considerable variation between studies, the results were not meta‐analysed. The sensitivities were between 8% and 63% while the specificities were between 35% and 67%.
Only one study examined the accuracy of plasma Aß42 and the plasma Aß42/Aß40 ratio for Alzheimer's disease dementia. The sensitivity of 86% (95% CI 81 to 90) was the same for both tests while the specificities were 50% (95% CI 44 to 55) and 70% (95% CI 64 to 75) for plasma Aß42 and the plasma Aß42/Aß40 ratio respectively. Of the 565 participants examined, 245 developed Alzheimer’s dementia and 87 non‐Alzheimer's disease dementia.
There was substantial heterogeneity between studies. The accuracy of Aß42 for the diagnosis of Alzheimer's disease dementia did not differ significantly (P = 0.8) between studies that pre‐specified the threshold for determining test positivity (n = 6) and those that only determined the threshold at follow‐up (n = 8). One study excluded a sample of MCI non‐Alzheimer's disease dementia converters from their analysis. In sensitivity analyses, the exclusion of this study had no impact on our findings. The exclusion of eight studies (950 patients) that were considered at high (n = 3) or unclear (n = 5) risk of bias for the patient selection domain also made no difference to our findings.
Authors' conclusions
The proposed diagnostic criteria for prodromal dementia and MCI due to Alzheimer's disease, although still being debated, would be fulfilled where there is both core clinical and cognitive criteria and a single biomarker abnormality. From our review, the measure of abnormally low CSF Aß levels has very little diagnostic benefit with likelihood ratios suggesting only marginal clinical utility. The quality of reports was also poor, and thresholds and length of follow‐up were inconsistent. We conclude that when applied to a population of patients with MCI, CSF Aß levels cannot be recommended as an accurate test for Alzheimer's disease.
Keywords: Humans, Alzheimer Disease, Alzheimer Disease/diagnosis, Amyloid beta‐Peptides, Amyloid beta‐Peptides/blood, Amyloid beta‐Peptides/cerebrospinal fluid, Biomarkers, Biomarkers/blood, Biomarkers/cerebrospinal fluid, Cognitive Dysfunction, Cognitive Dysfunction/diagnosis, Dementia, Dementia/diagnosis, Disease Progression, Peptide Fragments, Peptide Fragments/blood, Peptide Fragments/cerebrospinal fluid, Sensitivity and Specificity
Plain language summary
Proteins in blood and cerebrospinal fluids for early prediction of developing Alzheimer’s disease or other dementia in people with cognitive problems
The numbers of people with dementia and other cognitive problems are increasing globally. A diagnosis of the pre‐dementia phase of disease is recommended but there is no agreement on the best approach. A range of tests have been developed which healthcare professionals can use to assess people with poor memory or cognitive impairment. In this review, however, we have found that measuring protein in cerebrospinal fluid (CSF amyloid beta (Aβ40) or CSF Aβ42), as a single test, lacks the accuracy to identify those patients with mild cognitive impairment who would develop Alzheimer's disease dementia or other forms of dementia.
Summary of findings
Summary of findings'. 'Performance of plasma and CSF amyloid biomarkers.
| What is the diagnostic accuracy of plasma and CSF amyloid biomarker levels for detecting Alzheimer's disease pathology in patients with mild cognitive impairment (MCI), and identifying those MCI participants who would convert to Alzheimers disease dementia or other forms of dementia over time | |||||||
| Patient population | Participants diagnosed with MCI at baseline using any of the Petersen criteria or CDR = 0.5 or any 16 definitions included by Matthews (Matthews 2008) | ||||||
| Prior testing | The only testing prior to performing the plasma and CSF biomarkers was the application of diagnostic criteria for identifying participants with MCI | ||||||
| Settings | Participants were recruited from i) secondary care – outpatient clinic (n = 12); ii) secondary care – inpatients (n = 2); iii) community care (n = 2) and mixed setting (n = 1) | ||||||
| Index tests | Plasma or CSF Aß 42, Aß 40, or Aß 42/Aß 40 ratio | ||||||
| Reference standard | NINCDS‐ADRDA or DSM or ICD criteria for Alzheimer's disease dementia; McKeith criteria for Lewy body dementia; Lund criteria for frontotemporal dementia; and NINDS AIREN criteria for vascular dementia | ||||||
| Target condition | Alzheimer’s disease dementia or any other form of dementia | ||||||
| Included studies | 17 studies (2228 participants) of prospectively well defined cohorts with any accepted definition of MCI were included | ||||||
| Quality concerns | Patient selection and conduct of the index and reference standard were poorly reported. Applicability concerns were generally low. Regarding the inclusion criteria set in the review, each included study did match the review question: 'Could Plasma and CSF Aßbiomarkers identify those MCI participant with Alzheimer’s disease pathology at baseline who would convert clinically to dementia at follow up?' However, due to limited number of included studies and levels of heterogeneity it is difficult to determine to what extent the findings from a meta‐analysis can be applied to clinical practice. | ||||||
| Limitations | Limited investigation of heterogeneity due to insufficient number of studies. There was a lack of common thresholds and poor reporting of thresholds. | ||||||
| Test | Studies | Cases/participants | Median specificity from included studies |
Sensitivity (95% CI)1 at median specificity |
Consequences in a cohort of 100 | ||
| Median percentage converting (range)2 | Missed cases3 |
Overdiagnosed 3 |
|||||
| Alzheimer's disease dementia | |||||||
| CSF Aß 42 | 14 | 436/1349 | 64 | 81 (72, 87) | 38 (9 to 56) | 7 | 22 |
| All forms of dementia | |||||||
| CSF Aß 42 | 4 | 188/464 | 75 | 63 (22, 91) | 45 (27 to 53) | 17 | 14 |
| Non‐Alzheimer's disease dementia | |||||||
| CSF Aß 42 | 3 | 61/385 | 65 | No meta‐analysis | 16 (15 to 19) | ||
| Investigation of heterogeneity: the planned investigations were not possible due to the limited number of studies available for each analysis. We were unable to investigate the effect of duration of follow up due to substantial variation in length and reporting. | |||||||
| Conclusions: from our review, abnormally low CSF Aß levels has very little diagnostic benefit with likelihood ratios suggesting only marginal clinical utility. The quality of reports was also poor, and thresholds and length of follow up were inconsistent. We conclude that when applied to a population of patients with MCI, CSF Aß levels cannot be recommended as an accurate test for Alzheimer's disease. | |||||||
1 Meta‐analytic estimate of sensitivity derived from the HSROC model at a the median value of specificity computed from the included studies. Summary estimates of sensitivity and specificity were not computed because the studies that contributed to the estimation of the summary ROC curve used various thresholds.
2 The median percentage converting and range were computed using all the studies included in the analysis for each target condition.
3 Missed and overdiagnosed numbers were computed using the median percentage converting for each target condition.
Background
Alzheimer’s disease is an incurable, progressive, neurodegenerative condition which accounts for over 50% of dementias, afflicting 5% of men and 6% of women over 60 years old worldwide (World Health Organization 2010). As age is the principal risk factor, the general ageing of the global population, despite some suggestions that dementia incidence is falling, means that the total number of people suffering from Alzheimer's dementia is likely to still be increasing. The prevalence increases exponentially with age as Alzheimer's dementia affects < 1% of people aged 60 to 64 years old and 24% to 33% of those aged over 85 years (Ferri 2005).
It is important to distinguish Alzheimer's disease (which is the underlying pathology) from Alzheimer's dementia, which is the final stage of a clinical syndrome that develops as a result of the pathology. The diagnosis of pre‐dementia Alzheimer's disease is currently being debated and the best nosology to define this stage of illness lacks consensus, especially with regards to the use of various terms (for example prodromal dementia) in clinical practice. It is also important to be able to distinguish between the various subtypes of dementia as early as possible in the course of illness to maximise the impact of treatment and risk modification.
The target condition being diagnosed by the testing of cerebrospinal fluid (CSF) and plasma for amyloid beta (Aß) 40 or 42 and the 40/42 ratio is Alzheimer's disease both as a distinct entity from normal ageing as well as from other subtypes of dementia (for example vascular dementia, Lewy body dementia and frontotemporal dementias). In this review we aimed to determine whether CSF or plasma Aß levels were diagnostic of Alzheimer's disease in people with cognitive impairment but no dementia. Subsequent reviews will explore the accuracy of this test to discriminate between subtypes of dementia (Kokkinou 2014).
The first complaints that people make (either to their general practitioner (GP) or to family) are often regarding subjective cognitive complaints such as memory lapses or getting lost. This may lead to a diagnosis of mild cognitive impairment (MCI) being made if formal testing reveals objective evidence of cognitive impairment. In some people, this will progress to Alzheimer's dementia, though currently we are unable to accurately predict those who will progress. This has led to the development of numerous research programmes seeking to define clinical, cognitive and biomarker tests that can identify those with MCI who will develop dementia. The presence of Alzheimer's disease, which may be indexed by low levels of CSF or plasma Aß, in patients with early cognitive complaints is thereby considered to be a very strong risk factor for developing Alzheimer's dementia in the future. Therefore, the presence of Alzheimer's disease within patients with MCI is proposed as being a diagnostic test for the delayed verification of Alzheimer's disease dementia (Davis 2013).
Alzheimer's pathology is associated with a central amyloidosis and for many years the amyloid cascade hypothesis (Hardy 1992) has been used to describe the disruption of a probably normal cerebral process which is associated with ageing and how this disruption can lead to Alzheimer's disease. The model describes a pathway by which Aß monomers are produced, aggregate into oligomers and then are sequestered and potentially inactivated into the characteristic extracellular amyloid plaques. This may explain why on neuroimaging some cognitively ‘normal’ individuals have amyloid plaques after the age of 65 years (Aizenstein 2008). In Alzheimer's disease, however, the equilibrium of this system is biased to pathological, away from a physiological function, and an increased conversion to the Aß oligomers from the ‘inert’ monomers results in a toxic pool of soluble amyloid species which are central to the neurotoxicity of Alzheimer's disease. The amount of oligomeric Aß is too great to be sequestered into plaque and thereby remains present in the extracellular space to exert its toxic effects. As a consequence of neuronal disruption from these oligomeric species, intracellular cascades may lead to the hyperphosphorylation of tau, compromising the cytoskeletal protein tubulin with the development of neuro‐fibrillary tangles (NFTs). Toxic oligomers may also compromise synaptic activity leading in part to the clinical symptoms of MCI and eventually Alzheimer's disease dementia. There is also an associated inflammatory response from glial cells causing oxidative stress, synaptotoxicity and (via excess glutamate release) neurotoxicity. At the latter stages of disease progression the senile plaques are believed to also be pro‐inflammatory and thereby stimulate a further neurotoxic inflammatory response.
The amyloid hypothesis has yet to be decisively proven however (Shankar 2008) and one conflicting argument states that the increased production of Aß in Alzheimer's disease is a protective mechanism, due to its potent antioxidant ability, to counter a primary upstream effect, with mitochondrial dysfunction being heavily implicated (Castellani 2004). Moreover, the amyloid hypothesis has been questioned in light of recent studies and drug trials which have indicated no impact on the clinical course of disease after significant reduction in post‐mortem cerebral amyloid following active immunisation (Holmes 2008).
There are two main pathological isoforms of Aß, defined by their amino acid length: 40 and 42. Aß42 has a greater capacity to form oligomers and thereafter fibrils (the main constituent of amyloid plaques) and therefore has a higher neurotoxicity than its shorter counterpart Aß40. Successive ß‐ and ƴ‐secretase cleavage of the ubiquitous amyloid precursor protein (APP) is responsible for Aß42 production. The ɑ‐secretase cleavage of APP does not form either of these amyloid proteins but produces a much more soluble shorter moiety, Aß17, and its action is relatively suppressed in Alzheimer's disease. Despite the increased production of Aß42 in Alzheimer's disease, the trafficking of Aß42 into plaques may in fact lead to an observable lowering of the CSF and plasma levels of Aß42 with maintenance of the smaller, more soluble species in Alzheimer's disease compared to age‐matched controls. Therefore studies have shown that consistently there is a lowering of CSF levels of Aß42 in Alzheimer's disease dementia compared with controls, which may be indicative of extant central Aß pathology. Hypothetically, as the Aß42 levels decrease to a greater degree than the Aß40 levels, it follows that the ratio of Aß42:Aß40 will decrease, which may prove to be a more accurate test for Alzheimer's disease pathology than the absolute values of each protein in plasma or CSF.
It is worth noting that the Aß found in plasma is likely to have emanated from the alpha granules of platelets, where APP is also found in abundance, and therefore may be less closely related to the Alzheimer's disease central pathology. Little concurrence has been found between plasma and CSF Aß levels (Mehta 2001), therefore CSF Aß assays may prove to be a more accurate reflection of central amyloid pathology associated with Alzheimer's disease. However, as plasma is a much more accessible bodily fluid than CSF the accuracy of plasma Aß in diagnosing Alzheimer's disease pathology merits review.
There have been numerous attempts to clinically define the pre‐dementia phase of neurodegenerative disease. MCI is a heterogeneous condition which has been defined, using clinical criteria, by several authors, for example Petersen 1999. There have been over a dozen different definitions used to describe cognitive impairment that exceeds in extent and is somehow qualitatively different from normal ageing. Whilst remaining attentive to the widely differing prognostic implications of the differing terms, in this review the term MCI will be used to collectively describe the 16 conditions included in the research by Matthews 2008 (Matthews 2008). This leads to the proposal that from within these populations additional tests may help support the notion that there is central pathology that will mediate (over time) progression to one of the dementia syndromes. Knowing that a person with MCI has Alzheimer's disease as the cause of their symptoms would allow for the targeting of (future) disease modifying therapies, risk modifying strategies as well as psychosocial management.
There is currently no pre‐mortem gold standard test for Alzheimer's disease pathology. The observation that a patient with MCI, when followed carefully over time, develops Alzheimer's disease dementia can be taken (for the purposes of this review) that they had Alzheimer's disease pathology at baseline (that is when diagnosed with MCI) and it was this Alzheimer's pathology that caused the symptoms observed in MCI. However, since vascular events and Lewy body pathology may not be independent of amyloid pathology, it is also important to examine whether the index test predicts all causes of dementia and whether the accuracy in predicting these outcomes is different from the accuracy of predicting Alzheimer's disease dementia.
Inevitably this means that studies exploring the diagnostic accuracy of a test in MCI for Alzheimer's disease pathology will have a long time interval between the diagnostic test and the reference standard being applied (that is conversion to Alzheimer's disease dementia). However, as the course of this illness cannot be interrupted or affected by any therapeutic intervention, this is not as problematic as it would be in other conditions where interventions have an effect on the course of disease. Accordingly, studies must be long enough to allow 'conversion' from MCI to Alzheimer's disease dementia to occur and must use standardised criteria both to define the baseline population (MCI) and the conversion to Alzheimer's disease dementia.
In essence this review aims to understand the diagnostic test accuracy of Aß40 or Aß42, or their ratio, in CSF or plasma in patients with any of the described forms of MCI to identify them as having Alzheimer's disease pathology.
Target condition being diagnosed
Alzheimer's disease dementia
Other forms of dementia
Index test(s)
Studies that assessed the accuracy of plasma or CSF measurements of:
Aß42, or
Aß40, or
Aß42 to Aß40 ratio.
Aß is measured in ng.l‐1 or pg.ml‐1, which generate the same values.
The assays most commonly used are the conventional Innogenetics INNOTEST® beta‐amyloid1‐42 kit or the multiplexing INNO‐BIA AlzBio3 for CSF, or INNO‐BIA plasma Aß forms for plasma.
Clinical pathway
Dementia develops over a trajectory of several years. There is a presumed period when people are asymptomatic, and when pathology is accumulating. Individuals or their relatives may notice subtle impairments of recent memory. Gradually more cognitive domains become involved and difficulty planning complex tasks becomes increasingly apparent. In the UK, people often present to their GP when they or a family member or friend note memory deficits. The GP will potentially refer them to a memory clinic after taking a history of the problem and conducting a brief assessment of cognitive function. However, many people with dementia do not present to their GP for several years after the first onset of symptoms and will follow a different pathway to diagnosis, for example being identified during an admission to a general hospital for a physical illness.
Access to diagnostic assessment pathways may vary in other healthcare settings and diagnoses may be made by a variety of specialists including neurologists and geriatricians, who may rely to a greater or lesser degree on tests to assist with the diagnosis. In recent years there have been attempts across the world to identify dementia at the earliest stage, with an emphasis on the GP being vigilant in observing their patients for cognitive decline and then making referrals to specialist services. Accordingly, there is a growing interest in the accuracy of cognitive tests to support a referral and then of biomarkers (such as in imaging and in plasma or CSF) applied in specialist centres.
Alternative test(s)
We did not include alternative tests in this review because there are currently no standard practice tests available for the diagnosis of dementia.
This review is one of a series of diagnostic test accuracy reviews of biomarkers and scales being conducted by the Cochrane Dementia and Cognitive Improvement Group (CDCIG):
CSF (cerebrospinal fluid analysis of tau and tau/Aß ratio);
sMRI (structural magnetic resonance imaging);
18F‐2‐fluoro‐2‐deoxy‐D‐glucose positron emission tomography (18F‐FDG‐PET);
positron emission tomography Pittsburg Compound‐C (11C‐PIB‐PET);
neuropsychological tests (Mini‐Mental State Examination (MMSE); Mini‐Cog; Montreal Cognitive Assessment (MoCA));
informant interviews (IQCODE; AD8);
apolipoprotein Ɛ4 (APOEƐ4);
regional cerebral blood flow single photon emission computerised tomography (rCBF SPECT).
Although we are conducting reviews on individual tests compared to a reference standard, we plan to compare the results from the reviews in an overview.
Rationale
The two recently proposed diagnostic criteria for Alzheimer’s disease referred to MCI due to Alzheimer’s disease pathology and the prodromal (pre‐dementia phase) of Alzheimer's disease pathology (Albert 2011; Dubois 2010) and incorporate biomarkers based on imaging or CSF measures within the diagnostic rubric. These tests are core to the criteria, assuming they will improve the specificity of the traditional solely clinical criteria. It is crucial that each of these biomarkers is assessed for their diagnostic accuracy before they are adopted as routine tests in clinical practice. It is worth noting that in each of these criteria a single abnormality in any of the proposed biomarker or imaging tests is considered sufficient to make a diagnosis of prodromal Alzheimer’s disease dementia.
Underpinning the new criteria is the assumption that if Alzheimer’s disease pathology can be diagnosed at an earlier, pre‐dementia stage, this could open critical windows for interventions that will have a greater likelihood of success in affecting disease pathways and thereby improving clinical symptoms. Earlier, accurate diagnosis will also help people with pre‐dementia cognitive impairment and their families and potential carers make timely plans for the future. Coupled with appropriate contingency planning, proper recognition of the disease may also help to prevent inappropriate and potentially harmful admissions to hospital or institutional care (Bourne 2007). In addition, the accurate early identification of a dementia syndrome may improve opportunities for the use of newly evolving interventions designed to delay or prevent progression to more debilitating stages of dementia.
Objectives
To determine the accuracy of plasma and CSF Aß levels in identifying those participants with MCI at baseline who will convert to Alzheimer’s disease dementia or other forms of dementia over time.
Secondary objectives
To determine the nature, extent and impact of heterogeneity on the diagnostic accuracy of plasma and CSF Aß levels.
Methods
Criteria for considering studies for this review
Types of studies
We included all studies that had prospectively well defined cohorts with any accepted definition of cognitive decline but no dementia with baseline CSF or plasma Aß levels, or both, documented at or around the time that the above diagnoses were made. We also included studies which looked at data from those cohorts retrospectively, and contained sufficient data to construct 2 × 2 tables expressing plasma and CSF Aß biomarker results by disease status. The results in those that progressed to clinical Alzheimer's dementia were compared to those who did not progress, improved or developed another dementia.
We excluded any studies which potentially overlapped patient data and recorded them as multiple publications. We also excluded review papers.
Participants
We included participants who were diagnosed with a cognitive decline but with no dementia condition at baseline.
The cognitive decline but no dementia group is defined as patients who have been diagnosed using any of the Petersen criteria, or Clinical Dementia Rating (CDR) = 0.5, or any of the 16 definitions included by Matthews (Matthews 2008).
We excluded those patients or populations with cognitive decline no dementia possibly caused by:
current or a history of alcohol or drug abuse;
central nervous system (CNS) trauma (e.g. subdural haematoma), tumour or infection;
other neurological conditions e.g. Parkinson’s or Huntingdon’s diseases;
any other dementia co‐morbidity e.g. frontotemporal or vascular dementias.
We excluded studies that included patients with psychiatric, neurological, metabolic, immunological, hormonal or cerebrovascular disorders, or patients likely to have a genetic cause for their dementia (for example familial autosomal dominant Alzheimer’s disease or frontotemporal dementia, cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy, or Huntington’s disease).
If participants were involved in disease modifying clinical trials we excluded them from the analysis.
Patients with a family history of Alzheimer's disease dementia may be more readily diagnosed with MCI and therefore there can be spectrum bias with these participants. On this basis we examined separately those studies which included those with a known genetic predisposition.
Similarly, early onset Alzheimer's disease dementia, defined as a diagnosis under the age of 50 years, is likely to indicate a different aetiopathogenesis from late onset Alzheimer's disease dementia (including autosomally inherited mutation in the presenilin 1 and 2 genes, or the amyloid precursor protein (Filley 2007)). We excluded studies which included patients below the age of 50 years.
With regard to duration of follow‐up, Bruscoli 2004 indicated that an annual average of 10% of MCI patients become demented and therefore cohort studies would ideally have a minimum follow‐up time of 24 months. This provides a conversion rate to Alzheimer's disease dementia of approximately 19% and gives sufficient time for clinicians to diagnose a cause of MCI. Shorter durations of follow‐up may yield low conversion rates.
Index tests
Studies that assessed the accuracy of plasma or CSF measurements of:
Aß42, or Aß40, or the ratio Aß42/Aß40 were included.
There are currently no generally accepted standards for the plasma or CSF Aß test threshold, and therefore it was not possible to pre‐specify what constituted a positive or negative result. The thresholds that we used in this review were those generated and presented within each included study. It should be noted that where Aß42 and Aß40 data were presented separately, rather than as a ratio, then both tests would be analysed separately.
Measure of index test: Aß level in plasma or CSF, or both (ng.l‐1 or pg.ml‐1).
The assays most commonly used are conventional Innogenetics INNOTEST beta‐amyloid1‐42 kit or the multiplexing INNO‐BIA AlzBio3 for CSF, or INNO‐BIA plasma Aß forms for plasma.
We did not include a comparator test because there are currently no standard practice tests available for the diagnosis of dementia.
Target conditions
There were two target conditions in this review:
Alzheimer’s disease dementia (conversion from cognitive decline no dementia to Alzheimer’s disease dementia);
any other forms of dementia (conversion from cognitive decline no dementia to other (non‐Alzheimer's) forms of dementia);
any dementia (conversion from cognitive decline no dementia to any form of dementia).
Reference standards
The gold standard for Alzheimer's disease dementia is a post‐mortem. There is no ‘gold‐standard’ ante‐mortem diagnostic test for Alzheimer's disease dementia. Therefore, the reference standard in this review was conversion from MCI to Alzheimer's disease dementia based on the National Institute for National Institute of Neurological and Communicative Diseases and Stroke/Alzheimer's Disease and Related Disorders Association (NINCDS‐ADRDA) criteria (McKhann 1984) to define ‘probable’ Alzheimer's disease.
The NINCDS‐ADRDA criteria define three ante‐mortem groups: probable, possible and unlikely Alzheimer's disease dementia, based on evaluation of eight cognitive domains including memory and language.
The post‐consensus (on those cases in which there is a disagreement) specificity of the NINCDS‐ADRDA criteria is 0.84 and its sensitivity is 0.83 (Blacker 1994) against post‐mortem diagnosis. Exploring the impact of using different post‐mortem definitions of Alzheimer's disease, Nagy 1998 showed that the sensitivity of ‘possible’ and ‘probable’ dementia of the Alzheimer’s type according to NINCDS‐ADRDA criteria is 91% to 98% compared to the post‐mortem Khachaturian criteria, Tierney A3 criteria and the CERAD protocol at autopsy. Studies using Diagnostic and Statistical Manual of Mental Disorders criteria (DSM) (DSMIII 1987; DSMIV 1994) or International Statistical Classification of Diseases and Related Health Problems (ICD) criteria (World Health Organization 2010) exclusively to diagnose Alzheimer's disease dementia were also considered though the criteria would be entered as a covariate to assess their impact on results.
For Lewy body dementia as an outcome the reference standard is the McKeith criteria (McKeith 1996); for frontotemporal dementia, the Lund Criteria (Lund 1994); and for vascular dementia the NINDS AIREN criteria (Roman 1993).
Search methods for identification of studies
Electronic searches
The most recent search for this review was performed on 3 December 2012. We searched MEDLINE (OvidSP), EMBASE (OvidSP), BIOSIS Previews (ISI Web of Knowledge), Web of Science and Conference Proceedings (ISI Web of Knowledge), PsycINFO (OvidSP), and LILACS (BIREME). See Appendix 1 for details of the sources searched, the search strategies used, and the number of hits that were retrieved.
We also requested a search of the Cochrane Register of Diagnostic Test Accuracy Studies (managed by the Cochrane Renal Group).
We did not apply any language or date restrictions to the electronic searches; methodological filters were not used so as to maximise sensitivity.
Searching other resources
We checked the reference lists of all relevant studies for additional studies.
We also conducted searches in the MEDION database (Meta‐analyses van Diagnostisch Onderzoek) at www.mediondatabase.nl, Database of Abstracts of Reviews of Effects (DARE) at www.york.ac.uk/inst/crd/crddatabases.htm#DARE, Health Technology Assessments Database (HTA Database) at www.york.ac.uk/inst/crd/crddatabases.htm#HTA, and Aggressive Research Intelligence Facility (ARIF) database at www.arif.bham.ac.uk for other related systematic diagnostic accuracy reviews; we searched for systematic reviews of diagnostic studies from the International Federation of Clinical Chemistry and Laboratory Medicine Committee for Evidence‐based Laboratory Medicine database (C‐EBLM). We checked reference lists of any relevant systematic reviews for additional studies.
Data collection and analysis
Selection of studies
We selected studies initially from title and abstract screening by the review authors. We excluded articles on animal studies at this stage. We then obtained the full text for each potentially eligible study. We independently assessed these papers against the inclusion criteria for inclusion or exclusion. We resolved disagreements by discussion with a third author.
Data extraction and management
We extracted data to a study specific proforma which included the following.
Author, year of publication and journal.
The index test and assay type used (thresholds used to define positive and negative tests).
The criteria used for clinical definition for the baseline population.
Baseline demographics of the study population (age, gender, apolipoprotein E (ApoE) status, MMSE and clinical setting).
The duration of follow‐up (mean, minimum, maximum and median).
The proportion of patients developing the outcome of interest (Alzheimer's dementia using NINCDS‐ADRDA criteria) as well as other dementias where standard criteria were used.
The sensitivity and specificity of the index test in defining Alzheimer's dementia was used to back‐translate into a 2 x 2 table.
Other data relevant for creating 2 x 2 tables (TP = true test positive; FP = false test positive; FN = false test negative; TN = true test negative) e.g. a number of 'abnormal' and 'normal' tests and at baseline; a number of disease 'presence' and disease 'absence' at follow‐up, as well as through scrutiny of scatter plots.
We piloted the proforma against two primary diagnostic studies (Bjerke 2009; Hampel 2004) and amended it as necessary. We extracted data independently with disagreements then resolved by a third author.
Assessment of methodological quality
One review author and an independent assessor performed methodological quality assessments of each study using the QUADAS‐2 tool (Whiting 2011) as recommended by the Cochrane Collaboration. The tool is made up of four domains: patient selection, index test, reference standard and patient flow. Each domain is assessed in terms of risk of bias, with the first three domains also considered in terms of applicability concerns (http://www.bris.ac.uk/quadas/quadas‐2 Appendix 2). The components of each of these domains and a rubric which details how judgments concerning risk of bias are made are detailed in Appendix 3. Certain key areas important for this review regarding quality assessment were participant selection, blinding and missing data.
Statistical analysis and data synthesis
We performed separate analyses for each test and for each form of dementia (Alzheimer's disease dementia, non‐Alzheimer's disease dementia, and all forms of dementia). The disease negatives in each of these analyses were formed by all participants who did not develop the disease of interest. For example, where Alzheimer's disease dementia was the outcome, a participant developing another form of dementia would be in the disease negative group. We conducted exploratory analyses by plotting estimates of sensitivity and specificity from each study on forest plots and in receiver operating characteristic (ROC) space. To summarise test accuracy data across studies, we fitted hierarchical summary receiver operating characteristic (HSROC) models using the NLMIXED procedure in the SAS software package (version 9.2; SAS Institute, Cary, NC). The HSROC model accounts for between study variability through the inclusion of random effects that allow for heterogeneity in threshold and accuracy. Studies with different thresholds can be included (one threshold per study) in the HSROC model for the estimation of a summary ROC curve. A summary point can be identified on the summary ROC curve but summary estimates of sensitivity and specificity only have a clinically meaningful interpretation at a specific threshold. Therefore, in analyses where inclusion of studies was unrestricted by threshold, we used HSROC model parameters to derive sensitivities, with 95% confidence intervals, at median, lower and upper quartile values of the specificities from the included studies. When there were few studies and it was not possible to fit the complete HSROC model, we simplified the model by assuming a symmetrical summary ROC curve or fixed‐effect estimates, or both. In additional analyses, we planned to restrict analyses to only those studies that reported data at a common threshold if there were a sufficient number of studies.
Investigations of heterogeneity
The main sources of heterogeneity considered a priori were:
differences in test thresholds;
which proprietary laboratory tests were used to undertake the CSF and plasma analyses;
duration of follow‐up: we planned to perform a subgroup analysis of short (< 2 years) and longer (2 or more years) duration of follow‐up;
criteria used for definition of cognitive impairment and dementia;
age of participants.
The HSROC model can be extended to include covariates to assess whether threshold, accuracy, or the shape of the summary ROC curve varies with patient or study characteristics. Where possible, we investigated the effect of each potential source of heterogeneity by using covariates to estimate differences in both the accuracy and threshold parameters, but the underlying shape of the summary ROC curve was assumed to be constant. This assumption was necessary due to the limited number of studies.
Sensitivity analyses
We undertook sensitivity analyses to investigate the impact of bias in the selection of participants, and bias in the conduct and interpretation of the index test, on test performance.
Results
Results of the search
Our search resulted in 37,555 citations, of which 527 full‐text papers were assessed for eligibility. Of the 527, we discarded 437 (82.9%). Of the remaining 90 papers, 17 were included, one paper was identified as an ongoing study, 33 were multiple publications of the included papers, and 39 papers were excluded for various reasons outlined in the PRISMA flow diagram (Figure 1). No extra studies were found through reference checking though usable data for four studies (Galluzzi 2010; Hertze 2010; Vos 2013; Zetterberg 2003) were identified through contacting authors of studies.
1.
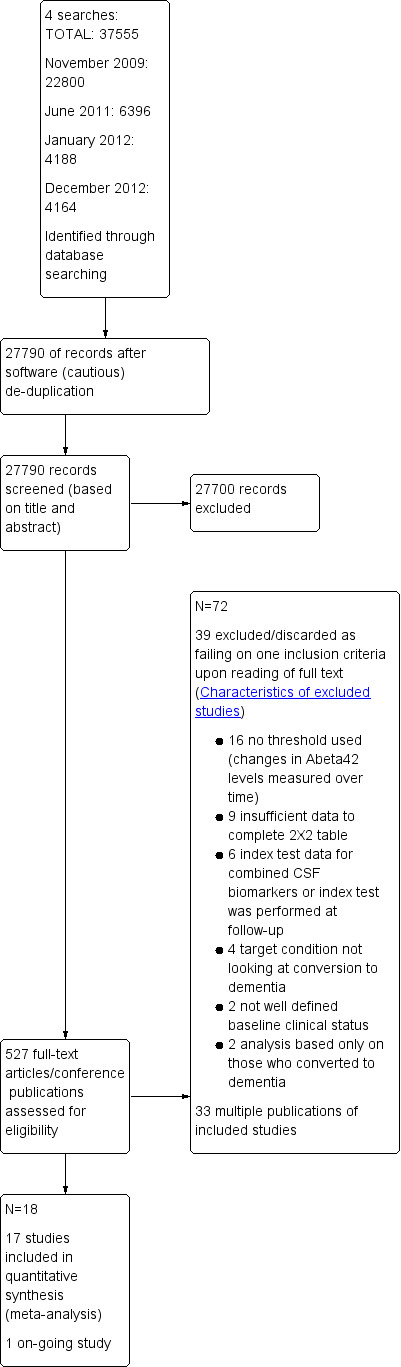
Flow of studies through the screening process.
Included studies
The Characteristics of included studies table lists the characteristics of the 17 included studies involving a total of 2228 participants with cognitive decline but no dementia at baseline, of whom 2058 had analysable data. All but two of the included studies used one version or another of the Petersen criteria for MCI; the other two used a CDR score of 0.5 to define cognitive decline but no dementia. The Alzheimer's Disease Neuroimaging Initiative (ADNI) study (Shaw 2009) referenced the full ADNI protocol where it was clear the Petersen criteria were used though this was not clear from the actual manuscript. Of those 2057 participants, 703 developed Alzheimer’s dementia and 206 non‐Alzheimer's dementia. In addition, in one study (Herukka 2007) 33 participants were described as converting to dementia and though the subtypes were described it was not possible (despite contact with author) to generate the required 2 x 2 table for Alzheimer's disease dementia.
The median sample size of the included studies was 79 (range 37 to 588). All the studies were recent publications (2003 to 2013). Most of the studies (14/17) were conducted in Europe (six in Sweden, three in Italy, one in Finland, one in the Netherlands, one in Spain, and one in Greece). There was one study conducted in both Sweden and the Netherlands, two took place in the USA, and one in China. The participants were mainly recruited from secondary care (12 studies from outpatient clinics and two studies from inpatient departments), two studies recruited the participants from the community (Brys 2009; Fei 2011), and one from a mixed setting (Shaw 2009).
Excluded studies
Several hundred studies were discarded because they failed to satisfy two or more inclusion criteria. The proportion of studies excluded because they failed to meet one of the four key inclusion criteria for the review was 39 out of 56 (69.6%) (Figure 1). The main reasons for exclusion were incorrect study design (cross‐sectional rather than longitudinal) and target population (not MCI participants at baseline) (see Figure 1). Two studies used a definition which was unclear for 'cognitive decline no dementia' in their baseline population; two studies did not investigate conversion to Alzheimer’s dementia or other dementias in the MCI sample included, rather they investigated different stages of cognitive decline. Ten studies did not use thresholds for the Aß test instead reporting changes in plasma or CSF Aß42 levels over time. Two studies used combined CSF Aß42 and tau index tests, and one study performed the index test at follow‐up. Seventeen papers were excluded as the data were not presented in a manner that allowed extraction to construct the necessary 2 x 2 table to generate sensitivities and specificities of the test, despite attempts made to contact authors.
Methodological quality of included studies
We assessed methodological quality using the QUADAS‐2 tool (Whiting 2011).
Review authors’ judgments about each methodological quality item for each included study are presented in the Characteristics of included studies table and Figure 2. The overall methodological quality of the included study cohorts is summarised in Figure 3.
2.
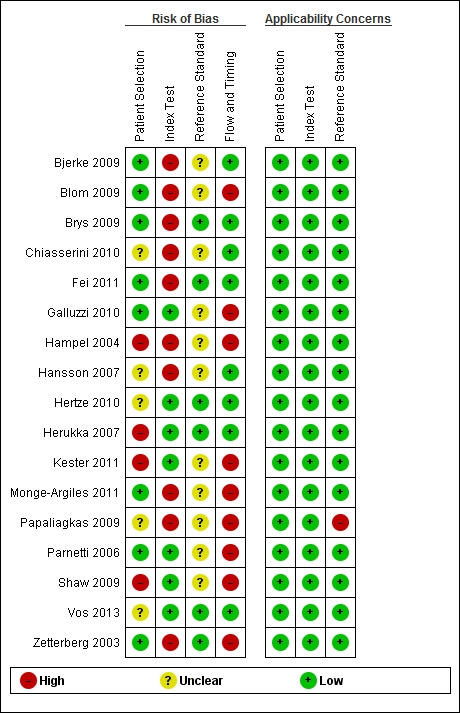
Risk of bias and applicability concerns summary: review authors' judgements about each domain for each included study.
3.
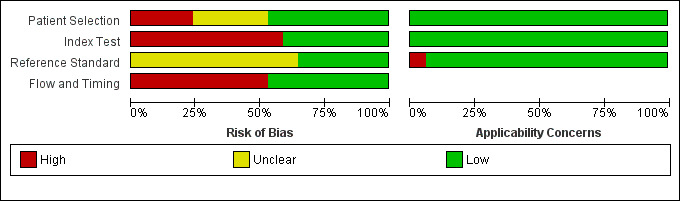
Risk of bias and applicability concerns graph: review authors' judgements about each domain presented as percentages across included studies.
In the patient selection domain, we considered eight studies (47%) to be at low risk of bias because participants were enrolled consecutively and inappropriate exclusions were avoided. In the review, we only included data on performance of the index test to discriminate between patients with MCI who converted to dementia and those who remained stable; therefore, we stated that a case‐control design was avoided in all included studies. We considered four (24%) studies to be at high risk of bias mainly because the participants were not consecutively or randomly enrolled. Five studies (29%) scored unclear risk of bias due to poor reporting.
In the index test domain, we considered 10 studies (60%) to be at high risk of bias because the threshold used was not pre‐specified and the optimal cut‐off level was determined from ROC analyses; therefore, the accuracy of the plasma and CSF Aß biomarkers reported in these studies appeared to be overestimated. We considered seven remaining studies (40%) to be at low risk of bias because the threshold used was pre‐specified and the index test results were interpreted without knowledge of the results of the reference standard.
In the reference standard domain, we judged six studies (35%) to be at low risk of bias because the reference standard used was likely to correctly classify the target condition and clinicians conducting follow‐up were not aware of the initial CSF analysis results. We considered eleven remaining studies (65%) to be at unclear risk of bias due to poor reporting.
In the flow and timing domain, we considered nine studies (53%) to be of high concern for risk of bias because not all patients were accounted for in the analysis or the time interval between the index test and reference standard was not appropriate (duration of follow‐up was shorter than one year). We considered eight remaining studies (47%) to be at low risk of bias.
According to the QUADAS‐2 assessment of applicability, we found few concerns that the included patients and setting, index test, its conduct or interpretation, and the target condition (as defined by the reference standard) in each of the included studies did not match the review question: could plasma and CSF Aß biomarkers identify those MCI participant with Alzheimer’s disease pathology at baseline who would convert clinically to dementia at follow‐up? However, due to the limited number of included studies and levels of heterogeneity with respect to the three domains mentioned above, it was difficult to determine to what extent the findings from a meta‐analysis could be applied to clinical practice.
Findings
There were three target conditions for this review: [1] Alzheimer's disease dementia, [2] all forms of dementia, and [3] non‐Alzheimer's disease dementia, and our ability to present data for each was determined by what was undertaken within each of the primary studies. There were also six possible index tests: [1] CSF Aß42, [2] CSF Aß40, [3] CSF Aβ42/Aβ40, [4] plasma Aß42, [5] plasma Aß40, and [6] plasma Aβ42/Aβ40. However primary research for review was not available for most of the possible combinations of target conditions and index tests.
All papers using NINCDS‐ADRDA criteria presented data where probable Alzheimer's disease dementia (8) was the outcome, or it was not stated (8).
The control group in each of the analyses below was formed by all participants who did not develop the outcome of interest, therefore where Alzheimer's disease dementia was the outcome participants developing another form of dementia or MCI non‐converters were in the control group.
CSF Aß42 for detecting Alzheimer's disease dementia
The accuracy of Aß42 for Alzheimer's disease dementia was evaluated in 14 studies. The individual study estimates of sensitivity and specificity from these 14 studies (1349 patients) are shown in Figure 4. The sensitivities were between 36% and 100% while the specificities were between 29% and 91%. The summary ROC curve summarising the accuracy of Aß42 across all 14 studies, irrespective of the threshold used, is shown in Figure 5. Because of the variation in thresholds we did not estimate a summary sensitivity and specificity. However, we derived estimates of sensitivity at fixed values of specificity (see Table 2) from the model we fitted to produce the summary ROC curve. At the median specificity of 64%, the estimated sensitivity was 81% (95% CI 72 to 87). This equated to a positive likelihood ratio (LR+) of 2.22 (95% CI 2.00 to 2.47) and a negative likelihood ratio (LR–) of 0.31 (95% CI 0.21 to 0.48).
4.
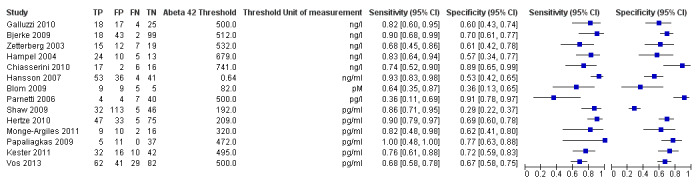
Forest plot of study results of cerebrospinal amyloid beta 42 for detection of Alzheimer's disease dementia.
5.
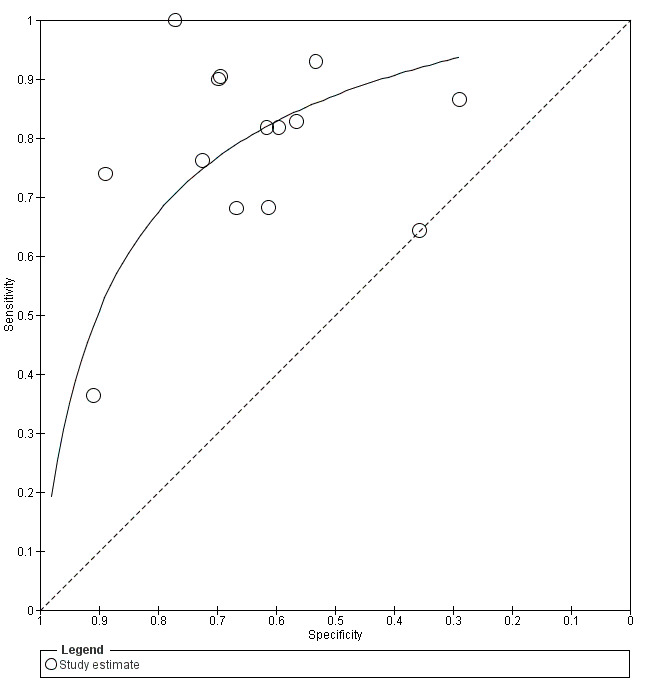
Summary ROC plot for cerebrospinal amyloid beta 42 for detection of Alzheimer's disease dementia. Study estimates of sensitivity and specificity are shown with the summary ROC curve.
1. Sensitivity of CSF Aß42 at fixed values of specificity for conversion to Alzheimer's dementia and all forms of dementia.
| Statistic | Fixed value of specificity % | Estimated sensitivity % (95% CI) |
| Conversion to Alzheimer's dementia (n = 14; cases = 436 ; non‐cases = 913) | ||
| Lower quartile | 57 | 84 (76, 90) |
| Median | 64 | 81 (72, 87) |
| Upper quartile | 72 | 75 (64, 83) |
| Conversion to Alzheimer's dementia sensitivity analyses excluding Kester 2011* (n = 13; cases = 394 ; non‐cases = 855) | ||
| Median | 62 | 82 (73, 88) |
| Conversion to Alzheimer's dementia sensitivity analyses excluding studies at high or unclear risk of bias for patient selection domain (n = 6; cases = 100 ; non‐cases = 299) | ||
| Median | 61 | 78 (55, 91) |
| Conversion to Alzheimer's dementia sensitivity analyses excluding studies at high risk of bias for index test domain (n = 6; cases = 255 ; non‐cases = 534) | ||
| Median | 68 | 76 (60, 87) |
| Conversion to Alzheimer's dementia sensitivity analyses excluding 3 outliers (n = 11; cases = 374 ; non‐cases = 696) | ||
| Median | 67 | 82 (69, 90) |
| All forms of dementia (n = 4; cases = 188; non‐cases = 276) | ||
| Median | 75 | 63 (22, 91) |
* The study did not consider a sample of MCI non‐AD converters in their analysis but excluded them.
The middle 50% of specificities from the included studies were between the lower and upper quartile, i.e. the interquartile range.
CSF Aß42 for detecting all forms of dementia
The accuracy of Aß42 for all forms of dementia was evaluated in four studies (464 patients) (Figure 6). The thresholds used were between 209 mg/ml and 512 ng/ml. The sensitivities were between 56% and 75% while the specificities were between 47% and 76%. The summary ROC curve summarising the accuracy of Aß42 across all four studies, irrespective of the threshold used, is shown in Figure 7. At the median specificity of 75%, the sensitivity was estimated to be 63% (22% to 91%) from the meta‐analytic model. This equated to a LR+ of 2.51 (95% CI 1.30 to 4.86) and a LR– of 0.50 (95% CI 0.16 to 1.51).
6.

Forest plot of study results of cerebrospinal amyloid beta 42 for detection of all forms of dementia.
7.
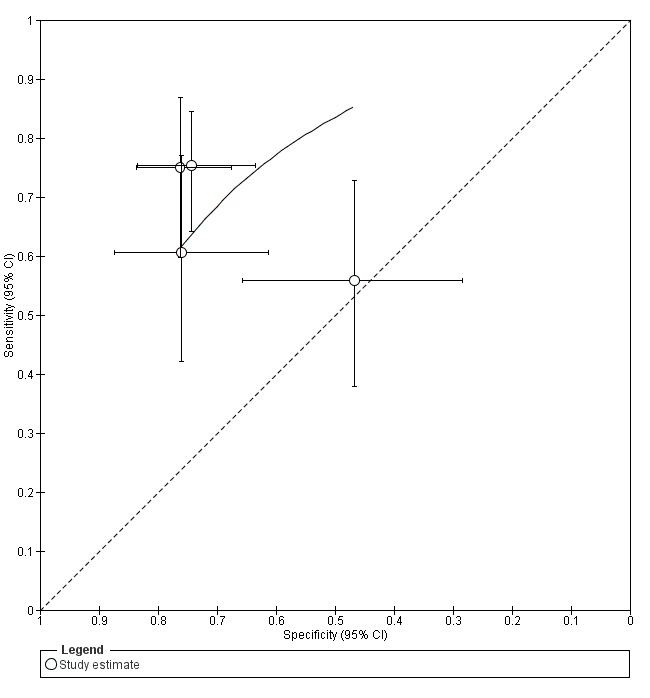
Summary ROC plot for cerebrospinal amyloid beta 42 for detection of all forms of dementia. Study estimates of sensitivity and specificity (with 95% confidence intervals) are shown with the summary ROC curve.
CSF Aß42 for detecting non‐Alzheimer's disease dementia
The accuracy of Aß42 for non‐Alzheimer's disease dementia was evaluated in three studies (385 patients). Since there were very few studies and considerable variation in test performance, the results were not meta‐analysed. Study specific estimates of sensitivity and specificity are summarised in Figure 8 and Figure 9. The sensitivities were between 8% and 63% while the specificities were between 35% and 67%. The study that did report the lowest threshold had a low sensitivity and the lowest specificity.
8.

Forest plot of study results of cerebrospinal amyloid beta 42 for detection of non‐Alzheimer's disease dementia.
9.
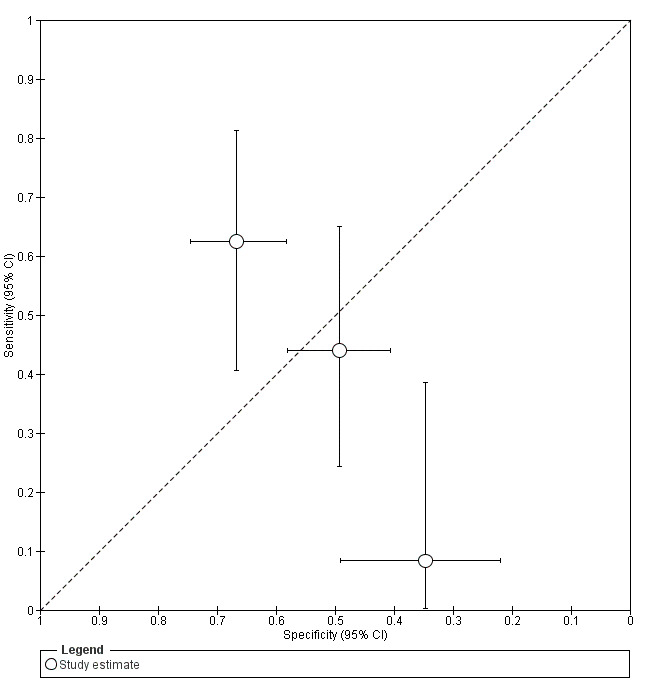
Study estimates of sensitivity and specificity with 95% confidence intervals plotted in ROC space for cerebrospinal amyloid beta 42 for the detection of non‐Alzheimer's disease dementia.
CSF ratio Aβ42/Aβ40 for detecting Alzheimer's disease dementia
The accuracy of the CSF Aβ42/Aβ40 for Alzheimer's disease dementia was evaluated in two studies (199 patients). The sensitivities were between 64% and 88% while the specificities were between 70% and 78%.
Plasma Aß42 and plasma Aβ42/Aβ40 ratio for detecting Alzheimer’s disease dementia
The accuracy of these plasma Aβ biomarkers for Alzheimer's disease dementia was evaluated only in one study (565 and 562 patients respectively). The sensitivity was 86% while the specificities were 50% and 70% respectively.
Investigations of heterogeneity
Investigations of heterogeneity were performed to assess the effect of pre‐specifying the threshold on the accuracy of Aß42 for Alzheimer's disease dementia. Test performance did not differ significantly (P = 0.8) between studies that pre‐specified the threshold (n = 6) and those that only determined the threshold at follow‐up (n = 8). The summary ROC curves for the two groups of studies are shown on the summary ROC plot in Figure 10. There is a paucity of knowledge around thresholds for Aß42 for Alzheimer's disease dementia. Despite best efforts a reliable and valid threshold remains elusive for clinical practice and research. Our findings also raise issues around risk of bias and the appropriateness of artificially determining cut‐offs.
10.
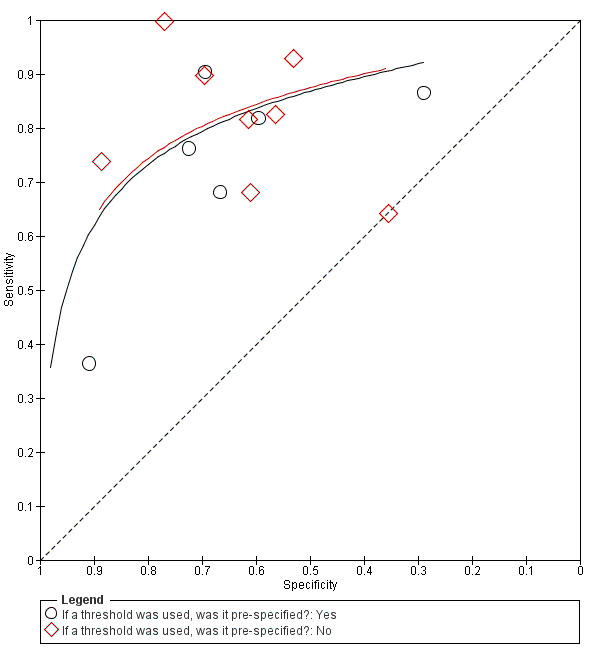
Summary ROC plot for cerebrospinal amyloid beta 42 for detection of Alzheimer's disease dementia. Study estimates of sensitivity and specificity (with 95% confidence intervals) and summary ROC curves are shown according to whether or not studies pre‐specified the threshold for determining test positivity.
We were unable to investigate the effect of duration of follow‐up due to substantial variation in study length and reporting. For instance, some studies measured mean and standard deviation, or the range of duration of follow‐up, while others measured only the median or mean and standard deviation for conversion period. Poor reporting of patient demographic information also contributed to unknown sources of heterogeneity. Due to variation and missing variables, and insufficient number of studies we could not adequately compare patient characteristics between studies. Finally, as the Peterson criteria were used in the majority of studies to diagnose MCI there were not enough studies to investigate different MCI criteria for sources of heterogeneity.
Sensitivity analyses
We undertook sensitivity analysis by excluding one study (Kester 2011) from the analysis of CSF Aß42 for predicting conversion to Alzheimer's disease dementia, because the authors excluded a sample of MCI non‐Alzheimer's disease converters from their analysis. Exclusion of this study made no difference to our results (Table 2). A second sensitivity analysis was undertaken to assess the effect of risk of bias in the patient selection domain on our findings. Eight studies (n = 950 patients) were considered at high (n = 3) or unclear (n = 5) risk of bias. The exclusion of these studies made no difference to our findings. A third sensitivity analysis involved the index test domain; 8 studies (n = 560 patients) were considered to have a high risk of bias. Exclusion of these studies had no impact on our findings.
Discussion
Summary of main results
We included 17 studies in the review. Although we did not specify inclusion based on the use of the term 'mild cognitive impairment (MCI)' to describe 'cognitive impairment but no dementia', all of the included studies defined their baseline population using the MCI criteria. We will therefore use the term MCI in the remainder of this discussion.
The meta‐analysis of the accuracy of CSF Aβ42 for conversion from MCI to Alzheimer's dementia is based on the results from 14 studies. Three studies were included in the meta‐analysis of the accuracy of CSF Aβ42 for conversion from MCI to non‐Alzheimer's disease dementias and four studies for conversion from MCI to all forms of dementia. Only one study reported the use of plasma Aβ42 levels or the plasma ratio Aβ42/Aβ40 for the delayed verification of Alzheimer's disease dementia, which yielded the same sensitivity of 86% (95% CI 81 to 90) and specificities of 50% (95% CI 44 to 55) and 70% (95% CI 64 to 75) for plasma Aβ42 and plasma Aβ42/Aβ40 ratio respectively.
The total number of MCI participants at baseline was 2228. The accuracy of plasma and CSF Aβ biomarkers was evaluated in 2058 participants, of whom 703 developed Alzheimer's disease dementia and 186 non‐Alzheimer's disease dementia. Fourteen studies used one of the Petersen diagnostic criteria of MCI (Petersen 1999; Petersen 2004; Petersen 2006), highlighting the dominance of this description of the individual with objective cognitive impairment but no dementia. Two papers used the CDR value of 0.5 as their definition of cognitive impairment but no dementia. Studies were variable in duration of follow‐up, with a range from six months to eight years (Appendix 4). In general, studies with a longer length of follow‐up tended to show higher sensitivities as a consequence of the greater number converting to dementia in their cohorts as a function of time. The accuracy of low levels of CSF Aß42 in the 17 included studies ranged from specificities of 29% (Shaw 2009) to 91% (Parnetti 2006) and sensitivities from 8% (Galluzzi 2010) to 100% (Papaliagkas 2009). The main utility of CSF Aß42 in the proposed new criteria is the specificity of lowered CSF Aβ42 to identify Alzheimer's disease in people with cognitive impairment but no dementia. We evaluated 14 studies and obtained a summary sensitivity of 81% (95% CI 72 to 87) from the summary ROC curve at the median specificity of 64% (the range of specificity from the included studies was 29% to 91%). This test appears to have low specificity and only modest sensitivity rather than having the desired specificity for Alzheimer's disease proposed in the new criteria.
Strengths and weaknesses of the review
This review took place after extensive discussion within The Cochrane Collaboration regarding the optimal methodology to determine the test accuracy of wet lab biomarkers, imaging modalities and neuropsychological tests for neurodegenerative disease present before the development of dementia. There is a major impetus in this area, driven by both clinical need and the limitations of existing diagnostic criteria, to support discovery of more effective treatments for dementia. Newly proposed criteria have emphasised the integration of biomarker criteria with cognitive criteria with the aim of improving the specificity of diagnosis prior to dementia onset. This review used specific criteria to answer the question, which yielded a reasonably large dataset given the challenges of conducting the primary research in what remains a relatively undeveloped research area. The oldest publication in our data set was from 2003 and 13 of the included studies were published within the last five years. In its own right this would raise concerns about the validity of the proposed criteria, which were published in 2010 and 2011 and therefore relied on a small dataset to form conclusions with no published meta‐analysis of those studies available at the time. This review is the first such systematic review of this emerging literature base. Although there were 17 studies in the review that contributed to the conclusions, the review is limited by the large number of studies that have taken place and which probably had data that could have been used in the review but, despite contact with authors, did not present the results in a manner that could be extracted and used. It is hoped that future revisions of this review will have access to these datasets or data yet to be published from ongoing studies that will be presented in the appropriate format. In these papers, data were presented as mean difference between groups of patients with stable MCI and those who converted to Alzheimer’s dementia, in effect exploratory studies determining statistical associations between disease progression and the biomarker rather than the clinical utility of these markers in diagnostic terms. This observation reflects the predominantly exploratory nature of the use of these biomarkers for identifying disease process rather than as diagnostic tests with clinical utility, in effect representing phase 2 proof of concept studies as opposed to later stage phase 3 clinically useful studies.
Despite this, the findings from our review are entirely consistent with the JAMA paper (Mattsson 2009) that had access to full data sets from seven studies (Bjerke 2009; Brys 2009; Chiasserini 2010; Hansson 2007; Herukka 2007; Kester 2011; Parnetti 2006) of the 17 studies included in our review. Their optimal sensitivity and specificity were virtually identical to the ones we generate from our summary ROC curve, giving our findings external validity (Table 2). It is considered unlikely, therefore, that the inclusion of other studies in our review would have had much impact on our summary of the accuracy of lowered CSF Aβ42 for diagnosing Alzheimer’s disease in a population with cognitive decline but no dementia.
Although the quality of the papers reported in our analysis was generally good, overall the methodological and reporting quality of all considered papers was poor. An international consensus initiative (the STARDdem Initiative) was conducted recently, co‐ordinated by the Cochrane Dementia and Cognitive Improvement Group. This initiative aimed to review the current standard of reporting in diagnostic test accuracy studies and cognitive impairment and to generate enhanced guidance to the existing reporting guideline for diagnostic test accuracy studies (Noel‐Storr 2013; the STARDdem Initiative website). This developing research field would be supported by acceptance of consistent methodologies and reporting which would assist future reviews of the diagnostic accuracy of tests and their synthesis in meta‐analysis.
The small number of studies included in our review precluded formal statistical analysis of the effect of potential sources of heterogeneity. We observed that longer duration studies tended to yield greater sensitivity. As age is the key risk factor for Alzheimer’s disease dementia, it stands to reason that as the cohort ages the incidence of dementia will increase, improving the sensitivity of the test in question. In effect the number of false positives diminishes as a function of time. However, formal analysis of the influence of these factors on the accuracy of CSF Aβ was not possible as age, ApoE status, duration of MCI prior to cohort entry, gender and cognitive function at baseline were not consistently reported.
Most of the studies (14) were conducted in western Europe, two in the USA and one in China. Overall, the ethnic distribution of the population being studied was unclear from the reports. It is also noteworthy that individual studies in the most part generated their own optimal cut points for what constituted a positive or negative test. Such inconsistency is being addressed currently, though the genesis of uniform analysis techniques and thresholds will not alter the diagnostic accuracy of the test but will allow for easier integration of results across studies.
Applicability of findings to the review question
Although there were differences between studies, including test threshold, we suggest that low CSF Aβ42 should not be used as a diagnostic test for Alzheimer’s disease in patients with cognitive decline but no dementia. The test is invasive, costly, suffers from a lack of consensus on sampling and analysis, and is non‐specific. It does not have the necessary accuracy to aid the clinician in making decisions as to which of their patients with cognitive decline but no dementia are likely to develop Alzheimer's dementia.
Recently proposed diagnostic criteria for prodromal AD emphasise low CSF Aβ42 in isolation from any other biomarker test as indicating ‘likely’ Alzheimer’s disease in a patient population with objective cognitive impairment. This proposal is not supported by our findings and the evidence points in the opposite direction where a normal test may have some modest utility in suggesting that normal CSF Aβ42 may rule out Alzheimer’s disease; even in this regard the risks and cost of testing may outweigh the potential benefit.
Authors' conclusions
Implications for practice.
In 2009, Petersen wrote that the use of CSF biomarkers was of value in clinical research, specifically stratification for clinical trials, but lacked the necessary accuracy for clinical practice. This meta‐analysis endorses that view. The proposed criteria for prodromal dementia would allow a diagnosis of prodromal Alzheimer's dementia to be made in the presence of low CSF Aβ in a person with significant amnestic symptoms. This review does not support this. It is possibly the case that in concert with other biomarker tests, be they imaging or other CSF markers, a reasonable accuracy can be obtained. The proposed criteria should be adapted at this stage in light of our findings that as a single test CSF Aß lacks the accuracy to diagnose Alzheimer's disease in patients with cognitive impairment but no dementia. That said, sequential testing with different tests is limited by the important assumption that each of the tests is conditionally independent of each other; this would not be the case for example with PET‐PiB and CSF Aβ, which are highly correlated measures of the same pathological process. To illustrate the lack of value of this test, if over a three‐year period 20% of people with MCI will go on to develop Alzheimer’s dementia, the pre‐test probability is 20% on the basis of the clinical diagnosis alone (Mitchell 2009). In these patients, a low level of CSF Aβ42 and a LR of 2.22 would yield a post‐test probability of 36% or an increment in risk of developing Alzheimer's dementia of 16%. Conversely, given a negative test result and a negative LR of 0.31, the post‐test probability of that person developing Alzheimer’s dementia is 7.2%; a decrement in risk of developing Alzheimer's dementia of 12.8%. There have been recent initiatives to screen primary care populations for cognitive impairment and refer those who screen positive to specialist care for further evaluation. In effect this may identify large populations with cognitive impairment but no dementia who are not seeking health care themselves. It is known that when applying the Petersen criteria in population and primary care settings the conversion rate to Alzheimer's dementia is lower than in secondary care services (Mitchell 2009). The effect therefore of identification of an at risk population in primary care would be to in effect reduce the pre‐test probability. As likelihood ratios are a function of the test, the effect of reducing the pre‐test probability on the incremental benefit of abnormal CSF Aβ42 is shown in Figure 11. This shows that the incremental benefit of an abnormal CSF Aß level in a patient identified through screening of primary care populations is substantially less than the already low figures achieved in a secondary care population. This is a theoretical conclusion as no studies in our sample were conducted in an explicitly defined primary care population, however in primary care it is likely that the pre‐test probability for Alzheimer's dementia is lower than it would be in a secondary care 'memory clinic' population. The optimal pre‐test probability for incremental benefit of a positive test is 40%, and 64% for a negative test, but even at this optimum level the benefits are modest. The results of this review are that abnormal CSF Aß levels are of little value in patients referred to specialists services and of even less value in those in whom cognitive impairment but no dementia is identified through primary care screening.
11.
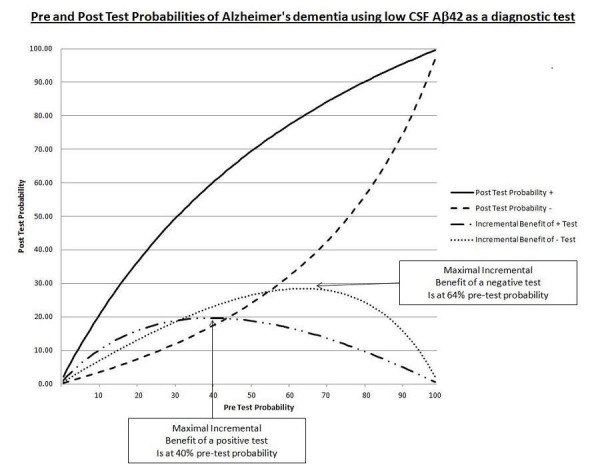
Pre‐ and post‐ tests probabilities of Alzheimer's dementia using low CSF amyloid beta 42 as a diagnostic test.
Implications for research.
The observations we have made regarding the utility of CSF Aß in identifying Alzheimer's disease prior to the onset of dementia suggest that at least at the MCI phase of illness there is little utility in its use. However, future research may identify that at even earlier stages (younger individuals) an accumulation of Aß in the brain as manifested through low CSF Aß will have greater specificity for indicating pathology rather than being a consequence of normal ageing in the elderly. Moreover, more uniform approaches to thresholds, analysis and study conduct, in particular uniformity of length of follow‐up, may provide a more homogenous estimate than was available here. The exploration for better, more accessible and more accurate biomarkers with, in particular, better specificity are urgently required. This research effort should be stimulated by the observation that CSF Aß does not appear to have the accuracy to draw to a conclusion the search for more accurate biomarkers for Alzheimer's disease. However, where clinical trials using specific anti‐amyloid therapies would benefit from small incremental changes towards improved post‐test probabilities, then CSF Aß may be useful in enriching the population. Our work, summarised in Figure 11, perhaps illustrates best the additional accuracy that can be achieved by using this test and the trial sponsors can apply this empirical evidence in their selection criteria for studies.
Acknowledgements
We wish to acknowledge Anne Eisinga for her assistance with developing the search strategy; Susanna Wisniewski for helping to perform a first assessment of the search results from the first search for this review; Paweł Kanturski for help with translation of a study subsequently excluded.
Appendices
Appendix 1. Search strategies and sources searched
| Source | Search strategy | Hits retrieved |
| 1. MEDLINE In‐process and other non‐indexed citations and MEDLINE 1950‐present [Searched most recently on 3 December 2012 (OvidSP)] | 1. exp Dementia/ 2. Cognition Disorders/ 3. exp Neurofibrils/ 4. Neurofilament Proteins/ 5. Senile Plaques/ 6. Neuropil Threads/ 7. (alzheimer$ or dement$).ti,ab. 8. ((cognit$ or memory or cerebr$ or mental$) adj3 (declin$ or impair$ or los$ or deteriorat$ or degenerat$ or complain$ or disturb$ or disorder$)).ti,ab. 9. (forgetful$ or confused or confusion).ti,ab. 10. MCI.ti,ab. 11. ACMI.ti,ab. 12. ARCD.ti,ab. 13. SMC.ti,ab. 14. CIND.ti,ab. 15. BSF.ti,ab. 16. AAMI.ti,ab. 17. MD.ti,ab. 18. LCD.ti,ab. 19. QD.ti,ab. 20. AACD.ti,ab. 21. MNCD.ti,ab. 22. MCD.ti,ab. 23. (neurofibril$ adj3 tangle$).ti,ab. 24. (neurofilament adj3 protein$).ti,ab. 25. ((senile or amyloid or neuritic) adj3 plaque$).ti,ab. 26. (neuropil adj3 thread$).ti,ab. 27. or/1‐26 28. exp Amyloid Beta‐Protein/ 29. Peptide Fragments/ 30. ABPP.ti,ab. 31. APP.ti,ab. 32. beta?A4.ti,ab. 33. (beta adj3 A4).ti,ab. 34. Abeta$.ti,ab. 35. amyloid.ti,ab. 36. (amyloidogenic adj3 (peptide$ or protein$)).ti,ab. 37. (Innotest or Inno‐bia or Alzbio3).ti,ab. 38. or/28‐37 39. (cerebrospinal fluid$ or csf or spinal fluid$).ti,ab. 40. (blood or plasma).ti,ab. 41. Cerebrospinal Fluid/ 42. Blood‐Brain Barrier/ 43. or/39‐42 44. (cf or bl or di or du).fs. 45. 27 and 38 and (43 or 44) 46. exp Dementia/bl, cf [Blood, Cerebrospinal Fluid] 47. exp Dementia/di [Diagnosis] 48. 47 and 43 49. Cerebrospinal Fluid Proteins/ 50. Biological Markers/cf, bl [Cerebrospinal Fluid, Blood] 51. or/49‐50 52. 27 and 51 53. or/45‐46,48,52 54. exp Animals/ not Humans.sh. 55. 53 not 54 |
Nov 2009: 8424 Jun 2011: 1479 Jan 2012: 601 Dec 2012: 1051 TOTAL: 11555 |
| 2. EMBASE [Searched most recently: December 2012 search: 197406‐November week 4 2012 (OvidSP)] |
1. exp dementia/ 2. exp cognitive defect/ or exp mild cognitive impairment/ 3. exp neurofilament/ 4. exp neurofilament protein/ 5. senile plaque/ 6. neuropil thread/ 7. (alzheimer$ or dement$).ti,ab. 8. ((cognit$ or memory or cerebr$ or mental$) adj3 (declin$ or impair$ or los$ or deteriorat$ or degenerat$ or complain$ or disturb$ or disorder$)).ti,ab. 9. (forgetful$ or confused or confusion).ti,ab. 10. MCI.ti,ab. 11. ACMI.ti,ab. 12. ARCD.ti,ab. 13. SMC.ti,ab. 14. CIND.ti,ab. 15. BSF.ti,ab. 16. AAMI.ti,ab. 17. MD.ti,ab. 18. LCD.ti,ab. 19. QD.ti,ab. 20. AACD.ti,ab. 21. MNCD.ti,ab. 22. MCD.ti,ab. 23. ("N‐MCI" or "A‐MCI" or "M‐MCI").ti,ab. 24. (neurofibril$ adj3 tangle$).ti,ab. 25. (neurofilament adj3 protein$).ti,ab. 26. ((senile or amyloid or neuritic) adj3 plaque$).ti,ab. 27. (neuropil adj3 thread$).ti,ab. 28. or/1‐27 29. exp amyloid beta protein/ 30. peptide fragment/ 31. ABPP.ti,ab. 32. APP.ti,ab. 33. beta?A4.ti,ab. 34. Abeta$.ti,ab. 35. amyloid.ti,ab. 36. (beta adj3 A4).ti,ab. 37. (amyloidogenic adj3 (peptide$ or protein$)).ti,ab. 38. (Innotest or Inno‐bia or Alzbio3).ti,ab. 39. or/29‐38 40. 28 and 39 41. (cerebrospinal fluid$ or csf or spinal fluid$).ti,ab. 42. (blood or plasma).ti,ab. 43. cerebrospinal fluid/ 44. blood brain barrier/ 45. or/41‐44 46. 28 and 39 and 45 47. (cf or bl or di or du).fs. 48. or/45,47 49. 28 and 39 and 48 50. exp Dementia/di [Diagnosis] 51. 50 and 39 52. (bl or cf).fs. 53. 50 and (46 or 52) 54. protein cerebrospinal fluid level/ 55. biological marker/ and (blood or plasma or CSF or "cerebrospinal fluid").ti,ab. 56. 54 or 55 57. 28 and 56 58. or/49,51,53,57 59. animal/ 60. human/ 61. 59 and 60 62. 59 not 61 63. 58 not 62 |
Nov 2009: 5594 Jun 2011: 1739 Jan 2012: 1805 Dec 2012: 1629 TOTAL: 10767 |
| 3. PsycINFO [Searched most recently: December 2012 search: 1806‐November week 4 2012 (OvidSP)] |
1. exp Dementia/ 2. exp Cognitive Impairment/ 3. Neurofibril*.mp. 4. exp Neurofibrillary Tangles/ 5. Senile Plaques/ 6. "neuropil threads".mp. 7. (alzheimer$ or dement$).ti,ab. 8. ((cognit$ or memory or cerebr$ or mental$) adj3 (declin$ or impair$ or los$ or deteriorat$ or degenerat$ or complain$ or disturb$ or disorder$)).ti,ab. 9. (forgetful$ or confused or confusion).ti,ab. 10. MCI.ti,ab. 11. ACMI.ti,ab. 12. SMC.ti,ab. 13. CIND.ti,ab. 14. BSF.ti,ab. 15. AAMI.ti,ab. 16. MD.ti,ab. 17. LCD.ti,ab. 18. QD.ti,ab. 19. AACD.ti,ab. 20. MNCD.ti,ab. 21. MCD.ti,ab. 22. ("N‐MCI" or "A‐MCI" or "M‐MCI").ti,ab. 23. (neurofibril$ adj3 tangle$).ti,ab. 24. ARCD.ti,ab. 25. (neurofilament adj3 protein$).ti,ab. 26. ((senile or amyloid or neuritic) adj3 plaque$).ti,ab. 27. (neuropil adj3 thread$).ti,ab. 28. or/1‐27 29. exp Beta Amyloid/ 30. exp Peptides/ 31. ABPP.ti,ab. 32. APP.ti,ab. 33. beta?A4.ti,ab. 34. (beta adj3 A4).ti,ab. 35. Abeta$.ti,ab. 36. amyloid.ti,ab. 37. (amyloidogenic adj3 (peptide$ or protein$)).ti,ab. 38. (Innotest or Inno‐bia or Alzbio3).ti,ab. 39. or/29‐38 40. 28 and 39 41. (cerebrospinal fluid$ or csf or spinal fluid$).ti,ab. 42. (blood or plasma).ti,ab. 43. Cerebrospinal Fluid/ 44. Blood Brain Barrier/ 45. or/41‐44 46. 28 and 39 and 45 47. Cerebrospinal Fluid/ 48. exp Biological Markers/ 49. 47 or 48 50. 28 and 49 51. 46 or 50 52. limit 51 to human |
Nov 2009: 1848 Jun 2011: 620 Jan 2012: 446 Dec 2012: 382 TOTAL: 3296 |
| 4. BIOSIS Previews (ISI Web of Knowledge) [searched most recently on 3 December 2012] | Topic=(dementia OR neurofibrils OR neurofilament OR "senile plaques" OR neuropil OR alzheimer* OR cognit* OR memory OR MCI OR ACMI OR SMC OR CIND OR BSF OR AAMI OR AACD OR MNCD OR MCD OR nMCI OR aMCI OR mMCI) AND Topic=("amyloid beta" OR "a beta" OR abeta OR amyloidogenic OR innotest OR "inno‐bia" OR alzbio3) AND Topic=("cerebrospinal fluid" OR "cerebro spinal fluid" OR CSF OR blood OR plasma OR "blood‐brain barrier") | Nov 2009: 1936 Jun 2011: 1321 Jan 2012: 743 Dec 2012: 551 TOTAL: 4551 |
| 5. Web of Science and conference proceedings (1945‐present) [searched most recently on 3 December 2012] | Topic=(dementia OR neurofibrils OR neurofilament OR "senile plaques" OR neuropil OR alzheimer* OR cognit* OR memory OR MCI OR ACMI OR SMC OR CIND OR BSF OR AAMI OR AACD OR MNCD OR MCD OR nMCI OR aMCI OR mMCI) AND Topic=("amyloid beta" OR "a beta" OR abeta OR amyloidogenic OR innotest OR "inno‐bia" OR alzbio3) AND Topic=("cerebrospinal fluid" OR "cerebro spinal fluid" OR CSF OR blood OR plasma OR "blood‐brain barrier") AND Year Published=(2011‐2012) Timespan=All Years. Databases=SCI‐EXPANDED, SSCI, A&HCI, CPCI‐S, CPCI‐SSH. Lemmatization=On |
Nov 2009: 4998 Jun 2011: 1237 Jan 2012: 587 Dec 2012: 551 TOTAL: 7373 |
| 6. LILACS (BIREME) [searched most recently on 3 December 2012] | “peptídeo beta‐amilóide” OR “placas neuríticas” OR “emaranhados neurofibrilares” OR “senile plaques” OR “β‐amyloid” OR “beta‐amiloide” OR “b‐Amiloid” OR “ovillos neurofibrilares” OR amilóide OR innotest OR “inno‐bia” OR alzbio3 [Words] and CSF OR LCR OR cefalorraquidiano OR “biological marker” OR “biological markers” OR plasma OR plasmáticos OR plasmocitos [Words] and “comprometimento cognitivo leve” OR “cognitive impairment” OR MCI OR Alzheimer OR Alzheimer’s OR AD OR memory OR Memória OR memórias OR demências OR demência OR dementia [Words] | Nov 2009: 0 Jun 2011: 0 Jan 2012: 6 Dec 2012: (13‐6)= 7 new TOTAL: 13 |
| Additional sources: Additional other review sources: MEDION database (searched 31 Jan for all dates); Database of Abstracts of Reviews of Effects (searched Issue 1 of The Cochrane Library 2013); Health Technology Assessments Database (searched Issue 1 of the Cochrane Library 2013); ARIF Aggressive Research Intelligence Facility www.arif.bham.ac.uk [searched 3 Dec for all dates] | Dec 2012: 14 TOTAL: 14 |
|
| TOTAL before de‐duplication | Nov 2009: 22800 Jun 2011: 6396 Jan 2012: 4188 Dec 2012: 4171 TOTAL: 37555 |
|
Appendix 2. Assessment of methodological quality table QUADAS‐2 tool
| DOMAIN | PATIENT SELECTION | INDEX TEST | REFERENCE STANDARD | FLOW AND TIMING |
| Description | Describe methods of patient selection: Describe included patients (prior testing, presentation, intended use of index test and setting): | Describe the index test and how it was conducted and interpreted | Describe the reference standard and how it was conducted and interpreted | Describe any patients who did not receive the index test(s) and/or reference standard or who were excluded from the 2x2 table (refer to flow diagram): Describe the time interval and any interventions between index test(s) and reference standard |
| Signalling questions (yes/no/unclear) |
Was a consecutive or random sample of patients enrolled? | Were the index test results interpreted without knowledge of the results of the reference standard? | Is the reference standard likely to correctly classify the target condition? | Was there an appropriate interval between index test(s) and reference standard? |
| Was a case‐control design avoided? | If a threshold was used, was it pre‐specified? | Were the reference standard results interpreted without knowledge of the results of the index test? | Did all patients receive a reference standard? | |
| Did the study avoid inappropriate exclusions? | Did all patients receive the same reference standard? | |||
| Were all patients included in the analysis? | ||||
| Risk of bias: High/low/ unclear | Could the selection of patients have introduced bias? | Could the conduct or interpretation of the index test have introduced bias? | Could the reference standard, its conduct, or its interpretation have introduced bias? | Could the patient flow have introduced bias? |
| Concerns regarding applicability: High/low/ unclear | Are there concerns that the included patients do not match the review question? | Are there concerns that the index test, its conduct, or interpretation differ from the review question? | Are there concerns that the target condition as defined by the reference standard does not match the review question? |
Appendix 3. Anchoring statements for quality assessment of plasma and CSF Abeta biomarkers diagnostic studies
We provide some core anchoring statements for quality assessment of diagnostic test accuracy review of plasma and CSF Aß levels in dementia. These statements are designed for use with the QUADAS‐2 tool and are based on the guidance for quality assessment of diagnostic test accuracy reviews of IQCODE in dementia (Quinn 2012).
During a two day, multidisciplinary focus group and the piloting / validation of the guidance, it was clear that certain issues were key to assessing quality, while other issues were important to record but less important for assessing overall quality. To assist, we describe a 'weighting' system. Where an item is weighted “high risk” then that section of the QUADAS‐2 results table is likely to be scored as high risk of bias. For example in dementia diagnostic test accuracy studies, ensuring that clinicians performing dementia assessment are blinded to results of index test is fundamental. If this blinding was not present then the item on reference standard should be scored 'high risk of bias', regardless of the other contributory elements.
In assessing individual items, the score of unclear should only be given if there is genuine uncertainty. In these situations review authors will contact the relevant study teams for additional information.
Anchoring statements to assist with assessment for risk of bias
| Question | Response and weighting | Explanation |
| Patient selection | ||
| Was the sampling method appropriate? | No = high risk of bias Yes = low risk of bias Unclear = unclear risk of bias |
Where sampling is used, the designs least likely to cause bias are consecutive sampling or random sampling. Sampling that is based on volunteers or selecting subjects from a clinic or research resource is prone to bias. |
| Was a case‐control or similar design avoided? | No = high risk of bias Yes = low risk of bias Unclear = unclear risk of bias |
Designs similar to case control that may introduce bias are those designs where the study team deliberately increase or decrease the proportion of subjects with the target condition, which may not be representative. Some case control methods may already be excluded if they mix subjects from various settings. |
| Are exclusion criteria described and appropriate? | No = high risk of bias Yes = low risk of bias Unclear = unclear risk of bias |
Study will be automatically graded unclear if exclusions are not detailed (pending contact with study authors). Where exclusions are detailed, the study will be graded as “low risk” if exclusions are felt to be appropriate by the review authors. Certain exclusions common to many studies of dementia are: medical instability; terminal disease; alcohol/substance misuse; concomitant psychiatric diagnosis; other neurodegenerative condition. Exclusions are not felt to be appropriate if ‘difficult to diagnose’ patients are excluded. Post hoc and inappropriate exclusions will be labelled “high risk” of bias. |
| Index test | ||
| Was plasma and CSF Abeta biomarker assessment/interpretation performed without knowledge of clinical dementia diagnosis? | No = high risk of bias Yes = low risk of bias Unclear = unclear risk of bias |
Terms such as “blinded” or “independently and without knowledge of” are sufficient and full details of the blinding procedure are not required. Interpretation of the results of the index test may be influenced by knowledge of the results of reference standard. If the index test is always interpreted prior to the reference standard then the person interpreting the index test cannot be aware of the results of the reference standard and so this item could be rated as ‘yes’. For certain index tests the result is objective and knowledge of reference standard should not influence result, for example level of protein in cerebrospinal fluid, in this instance the quality assessment may be “low risk” even if blinding was not achieved. |
| Were plasma and CSF Abeta biomarker thresholds pre‐specified? | No = high risk of bias Yes = low risk of bias Unclear = unclear risk of bias |
For scales and biomarkers there is often a reference point (in units or categories) above which subjects are classified as “test positive”; this may be referred to as threshold; clinical cut‐off or dichotomisation point. A study is classified high risk of bias if the authors define the optimal cut‐off post‐hoc based on their own study data because selecting the threshold to maximise sensitivity and / specificity may lead to overoptimistic measures of test performance. Certain papers may use an alternative methodology for analysis that does not use thresholds and these papers should be classified as not applicable. |
| Reference standard | ||
| Is the assessment used for clinical diagnosis of dementia acceptable? | No = high risk of bias Yes = low risk of bias Unclear = unclear risk of bias |
Commonly used international criteria to assist with clinical diagnosis of dementia include those detailed in DSM‐IV and ICD‐10. Criteria specific to dementia subtypes include but are not limited to NINCDS‐ADRDA criteria for Alzheimer’s dementia; McKeith criteria for Lewy Body dementia; Lund criteria for frontotemporal dementia; and the NINDS‐AIREN criteria for vascular dementia. Where the criteria used for assessment is not familiar to the review authors or the Cochrane Dementia and Cognitive Improvement group (‘unclear’) this item should be classified as “high risk of bias”. |
| Was clinical assessment for dementia performed without knowledge of the plasma and CSF Abeta biomarker biomarker? | No = high risk of bias Yes = low risk of bias Unclear = unclear risk of bias |
Terms such as “blinded” or “independently and without knowledge of” are sufficient and full details of the blinding procedure are not required. Interpretation of the results of the reference standard may be influenced by knowledge of the results of index test. |
| Patient flow | ||
| Was there an appropriate interval between plasma and CSF Abeta biomarker and clinical dementia assessment? | No = high risk of bias Yes = low risk of bias Unclear = unclear risk of bias |
As we test the accuracy of the plasma and CSF Abeta biomarker for MCI conversion to dementia, there will always be a delay between the index test and the reference standard assessments. The time between reference standard and index test will influence the accuracy (Geslani 2005;Bourne 2007;Visser 2006), and therefore we will note time as a separate variable (both within and between studies) and will test its influence on the diagnostic accuracy. We have set a minimum mean time to follow‐up assessment of 1 year. If more than 16% of subjects of subjects have assessment for MCI conversion before nine months this item will score ‘no’. |
| Did all subjects get the same assessment for dementia regardless of plasma and CSF Abeta biomarker? | No = high risk of bias Yes = low risk of bias Unclear = unclear risk of bias |
There may be scenarios where subjects who score “test positive” on index test have a more detailed assessment. Where dementia assessment differs between subjects this should be classified as high risk of bias. |
| Were all patients who received plasma and CSF Abeta biomarker assessment included in the final analysis? | No = high risk of bias Yes = low risk of bias Unclear = unclear risk of bias |
If the number of patients enrolled differs from the number of patients included in the 2x2table then there is the potential for bias. If patients lost to drop‐outs differ systematically from those who remain, then estimates of test performance may differ. If drop outs these should be accounted for; a maximum proportion of drop outs to remain low risk of bias has been specified as 20% |
| Were missing plasma and CSF Abeta biomarker results or uninterpretable plasma and CSF Abeta biomarker results reported? | No = high risk of bias Yes = low risk of bias Unclear = unclear risk of bias |
Where missing or uninterpretable results are reported, and if there is substantial attrition (we have set an arbitrary value of 50% missing data), this should be scored as ‘no’. If those results are not reported, this should be scored as ‘unclear’ and authors will be contacted |
| Anchoring statements to assist with assessment for applicability | ||
| Question | Explanation | |
| Were included patients representative of the general population of interest? |
The included patients should match the intended population as described in the review question. The review authors should consider population in terms of symptoms; pre‐testing; potential disease prevalence; setting If there is a clear ground for suspecting an unrepresentative spectrum the item should be rated poor applicability. |
|
| Index test | ||
| Were sufficient data on plasma and CSF Abeta biomarker application given for the test to be repeated in an independent study? | Variation in technology, test execution, and test interpretation may affect estimate of accuracy. In addition, the background, and training/expertise of the assessor should be reported and taken in consideration. If plasma and CSF Abeta biomarker was not performed consistently this item should be rated poor applicability. | |
| Reference standard | ||
| Was clinical diagnosis of dementia made in a manner similar to current clinical practice? | For many reviews, inclusion criteria and assessment for risk of bias will already have assessed the dementia diagnosis. For certain reviews an applicability statement relating to reference standard may not be applicable. There is the possibility that a form of dementia assessment, although valid, may diagnose a far larger proportion of subjects with disease than usual clinical practice. In this instance the item should be rated poor applicability. | |
Appendix 4. Duration of conversion from MCI to Alzheimer's disease dementia
| Study | Duration of follow‐up | |
| < 2 years | 2 years or more | |
| Bjerke 2009 | 4 years (conversion within 4 years) | |
| Bloom 2009 | range: 3‐12 years (mean ± SD 5.6 ± 2.7 years) for MCI‐MCI (stable); 1‐8 years (mean ± SD 3.4 ± 2.1 years) for MCI‐AD (converters) | |
| Chiasserini 2010 | 4 years (annual follow‐up; mean follow‐up not reported) | |
| Galluzzi 2010 | mean 24.0 ± 9.7 months | |
| Hampel 2004 | mean 8.4±5.1 months (range 2‐24 months); follow‐up interval for converters was 9.6±5.4, | |
| Hansson 2007 | mean: 5.2 years (range 4‐6.8 years) | |
| Hertze 2010 | mean 4.7 years (range 3.0‐7.2) | |
| Kester 2011 | median 18 months (IQR 13‐24); for MCI‐converters the median was 17 months (IQR 13‐24); for MCI‐stable the median was 18 months (IQR 12‐25) | |
| Monge‐Argiles 2011 | 6 months (conversion within 6 months) | |
| Papaialgkas 2009 | 11 months (conversion within 11 months) | |
| Parnetti | 12 months (conversion within 12 months) | |
| Shaw 2009 | 12 months (conversion within 12 months) | |
| Vos 2013 | mean 2.5 years (max duration 5 years) | |
| Zetterberg 2003 | mean 20±10 months | |
Data
Presented below are all the data for all of the tests entered into the review.
Tests. Data tables by test.
| Test | No. of studies | No. of participants |
|---|---|---|
| 1 CSF Abeta42 AD | 14 | 1349 |
| 2 CSF Abeta 42 All dementia | 4 | 464 |
| 3 CSF Abeta 42 non‐AD | 3 | 385 |
| 4 CSF Abeta42/Abeta40 AD | 2 | 199 |
| 5 Plasma Abeta 42 AD | 1 | 565 |
| 6 Plasma Abeta42/Abeta40 AD | 1 | 562 |
1. Test.
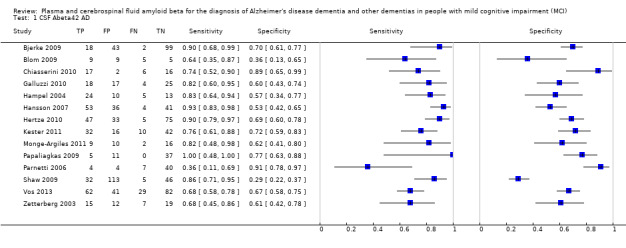
CSF Abeta42 AD.
2. Test.
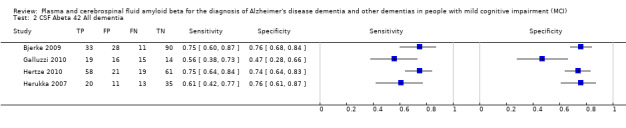
CSF Abeta 42 All dementia.
3. Test.

CSF Abeta 42 non‐AD.
4. Test.

CSF Abeta42/Abeta40 AD.
5. Test.

Plasma Abeta 42 AD.
6. Test.

Plasma Abeta42/Abeta40 AD.
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Bjerke 2009.
| Study characteristics | |||
| Patient sampling | 174 consecutive participants with mild cognitive impairment and 52 healthy elderly controls. We only included data on performance of the index test to discriminate between patients with MCI who convert to dementia and those who remained stable. Exclusion criteria: acute/unstable somatic disease; severe psychiatric disorder (e.g. major depression, psychotic disorder, bipolar disorder); substance abuse; confusion caused by medication |
||
| Patient characteristics and setting | 174 MCI participants from the Goteborg study diagnosed by the Petersen 1999 and Winbald 2004 criteria at baseline. Baseline demographic data reported for 162 participants Gender: 68 men; 94 women. MCI‐MCI: 53 M; 65 F; MCI‐SVD: 5 M; 4F; MCI‐MD: 2 M; 13 F; MCI‐AD: 8 M; 12 F Age: mean 66.75 years; MCI‐MCI 62 (57‐68) years; MCI‐SVD 68 (66‐74) years; MCI‐MD 69 (65‐74) years; MCI‐AD 68 (58‐72) years APOE ϵ4 carrier: 86; MCI‐MCI 54/118 (46%); MCI‐SVD 6/9 (67%); MCI‐MD 12/15 (80%); MCI‐AD 14/20 (70%) MMSE: MCI‐MCI: 29 (28, 30); MCI‐SVD: 28 (26, 28); MCI‐MD: 28 (26, 29); MCI‐AD 28 (27. 29) Setting: secondary care, outpatients ‐ memory clinic, Goteborg, Sweden |
||
| Index tests | CSF: Abeta42 LP through L3/L4 or L4/L5 interspace; CSF, collected in polypropylene tubes, was submitted to centrifugation at 2,000 g at +4°C for 10min. The CSF analysis on A 42 levels were performed on a single occasion by the standardised Luminex xMAP technology. Raw data from the Luminex assay were normalized to ELISA concentrations of abeta42 by running the same samples with both methods. A stable batch of ELISA reagents was used for all comparisons.The limit of detection for Abeta 42 was 61 ng/L Threshold: 512 ng/l determined at follow‐up (the case‐control derived threshold was applied) (Fig.1c, p351) At baseline 162 MCI:101 with 'normal CSF abeta42 level'; 61 with 'abnormal CSF abeta42 level' Index test was conducted before follow‐up |
||
| Target condition and reference standard(s) | Target condition: Alzheimer's disease dementia or other forms of dementia Reference standards: NINCDS‐ADRDA and ICD‐10 criteria for Alzheimer's disease dementia; DSM‐III‐R and ICD‐10 criteria for other dementia Unclear whether clinicians conducting follow‐up were aware of initial CSF analysis results |
||
| Flow and timing |
Duration of follow‐up: 4 years At baseline=174 MCI: 44 MCI‐converters (20 MCI‐AD; 15 MCI‐MD; 9 MCI‐SVD); 8 with normal cognition; 3 converted to dementia with unknown cause; 1 converted to primary progressive aphasia 36 patients converted to dementia within 2 years and 8 patients within 4 years Number included in analyses=162 TP=18; FP=43; FN=2; TN=99 for conversion to Alzheimer's disease dementia (Fig 1, p351) TP=33; FP=28; FN=11; TN=90 for conversion to all dementias (Fig 1, p351) TP=15; FP=46; FN=9; TN=92 for conversion to non‐AD dementia (Fig 1, p351) Loss to follow‐up: 12 patients were excluded from further analysis (8 patients had improved their condition at follow‐up; 3 patients converted to a dementia disorder where no etiology could be clinically established; 1 patient converted to primary progressive aphasia) (p350) |
||
| Comparative | |||
| Notes | |||
| Methodological quality | |||
| Item | Authors' judgement | Risk of bias | Applicability concerns |
| DOMAIN 1: Patient Selection | |||
| Was a consecutive or random sample of patients enrolled? | Yes | ||
| Was a case‐control design avoided? | Yes | ||
| Did the study avoid inappropriate exclusions? | Yes | ||
| Low | Low | ||
| DOMAIN 2: Index Test All tests | |||
| Were the index test results interpreted without knowledge of the results of the reference standard? | Yes | ||
| If a threshold was used, was it pre‐specified? | No | ||
| High | Low | ||
| DOMAIN 3: Reference Standard | |||
| Is the reference standards likely to correctly classify the target condition? | Yes | ||
| Were the reference standard results interpreted without knowledge of the results of the index tests? | Unclear | ||
| Unclear | Low | ||
| DOMAIN 4: Flow and Timing | |||
| Was there an appropriate interval between index test and reference standard? | Yes | ||
| Did all patients receive the same reference standard? | Yes | ||
| Were all patients included in the analysis? | No | ||
| Low | |||
Blom 2009.
| Study characteristics | |||
| Patient sampling | 58 patients with MCI, 47 with AD and 35 healthy elderly controls. Patients with AD and MCI were recruited consecutively from patients at a university hospital who underwent lumbar puncture as part of their dementia investigation between 1993 and 2001; control subjects were mainly spouses of participants. We only included data on performance of the index test to discriminate between patients with MCI who convert to dementia and those who remained stable. No exclusion criteria were reported |
||
| Patient characteristics and setting | 58 participants diagnosed by the Petersen 1999 criteria at baseline; 28 MCI patients revisited the clinic. Gender: 28 men; 30 women Age: mean 62.9 years; MCI‐MCI 61.3 years; MCI‐AD 71.7 years; MCI‐Progressors 66.0 years APOE ϵ4 carrier: 20 MMSE: not reported Setting: Secondary care, outpatients ‐ Department of Geriatrics, Huddinge, Sweden |
||
| Index tests | CSF: Abeta42 Following standard lumbar puncture, the CSF sample was aliquoted and stored at –80°C until quantification. Levels of A 42 and A 40 were analysed using a well‐characterized ELISA with BNT77 (mouse IgA anti‐A 11–28; Takeda, Osaka, Japan) and horseradish peroxidase‐conjugated detector antibodies (BA27 IgG2 mouse anti‐A 40 and BC05 IgG1 mouse anti‐A 42). Threshold: 82 pM for Abeta 42 determined at follow‐up (the case‐control derived threshold was applied) (p 460 and Fig.2c, p 462) At baseline 28 MCI who had a follow‐up assessment: 10 with 'normal CSF abeta42 level'; 18 with 'abnormal CSF abeta42 level' Index test was conducted before follow‐up |
||
| Target condition and reference standard(s) | Target condition: Alzheimer's disease dementia Reference standard: NINCDS‐ADRDA criteria Unclear whether clinicians conducting follow‐up were aware of CSF biomarker results |
||
| Flow and timing |
Duration of follow‐up: Range: 3‐12 years (mean ± SD 5.6 ± 2.7 years) for MCI‐MCI (stable); 1‐8 years (mean ± SD 3.4 ± 2.1 years) for MCI‐AD (converters) 28 MCI: 14 MCI‐MCI; 14 MCI‐AD Number included in analyses=28: 10 with 'normal CSF abeta amyloid level': 5 MCI‐MCI; 5 MCI‐AD; 18 with 'abnormal CSF abeta amyloid level': 9 MCI‐MCI; 9 MCI‐AD (Fig 2, p462) TP=9; FP=9; FN=5; TN=5 (Fig 2, p462) Loss to follow‐up: 30 MCI participants; no reasons were reported |
||
| Comparative | |||
| Notes | There is no overlap between Bloom 2009 and Zetterberg 2003 studies regarding the participants (Dr Zetterberg's email on 04/10/13) | ||
| Methodological quality | |||
| Item | Authors' judgement | Risk of bias | Applicability concerns |
| DOMAIN 1: Patient Selection | |||
| Was a consecutive or random sample of patients enrolled? | Yes | ||
| Was a case‐control design avoided? | Yes | ||
| Did the study avoid inappropriate exclusions? | Unclear | ||
| Low | Low | ||
| DOMAIN 2: Index Test All tests | |||
| Were the index test results interpreted without knowledge of the results of the reference standard? | Yes | ||
| If a threshold was used, was it pre‐specified? | No | ||
| High | Low | ||
| DOMAIN 3: Reference Standard | |||
| Is the reference standards likely to correctly classify the target condition? | Yes | ||
| Were the reference standard results interpreted without knowledge of the results of the index tests? | Unclear | ||
| Unclear | Low | ||
| DOMAIN 4: Flow and Timing | |||
| Was there an appropriate interval between index test and reference standard? | Yes | ||
| Did all patients receive the same reference standard? | Yes | ||
| Were all patients included in the analysis? | No | ||
| High | |||
Brys 2009.
| Study characteristics | |||
| Patient sampling | 65 consecutive participants with MCI and 21 healthy elderly controls. Healthy controls were not included in the analysis of CSF markers for the prediction of conversion of MCI to AD. Exclusion criteria: medical conditions or a history of significant conditions that may affect brain structure or function (e.g. stroke, fronto‐temporal and Lewy body dementia, depression, uncontrolled hypertension or type II diabetes); MRI‐based evidence of lacunar or cortical infarctions |
||
| Patient characteristics and setting | 65 community‐dwelling participants with MCI at baseline; the diagnosis of MCI was based on: progressive memory complaints corroborated by an informant, a CDR=0.5, GDS score = 3 and clinically recognisable memory impairment without fulfilling either the DSM‐IV or NINCDS‐ADRDA criteria for Alzheimer's disease dementia. Gender: 34 men; 31 women Age: 72.1 years MCI‐MCI; 71.3 years MCI‐AD APOE ϵ4 carrier: 33 MMSE: MCI‐MCI: 28.1±1.7; MCI‐AD: 27.3±2.1 Setting: community care, New York, USA There were no significant differences in baseline demographic characteristics between healthy controls and MCI participants who did or did not progress to AD |
||
| Index tests | CSF: Abeta42/Abeta40 ratio All subjects underwent lumbar puncture within 3 months of their longitudinal clinical assessment periods. CSF was stored at ‐80°C. The CSF amyloid β levels (Aβ40, Aβ42) were measured using a monoclonal antibody 6E10 (specific to an epitope present on Aβ‐16) and to rabbit antisera to Aβ40 and Aβ42 respectively, in a double antibody sandwich ELISA Threshold(s): the detection limit for both Aβ40 and Aβ42 was 10 pg/ ml (p 3) Optimal cut‐off level was determined from ROC analysis, with consideration to the recommendation (AD diagnostic tests Consensus Working Group) that sensitivity should be >80%; the value of the threshold was not reported At baseline 65 MCI: 29 with 'normal CSF abeta42/abeta40 ratio level'; 36 with 'abnormal CSF abeta42/abeta40 ratio level' Index tests were conducted before clinical follow‐up |
||
| Target condition and reference standard(s) | Target condition: Alzheimer's disease dementia References standard: NINCDS‐ADRDA criteria; DSM‐IV criteria "The creation of study groups was solely based on the clinical diagnosis and was blinded to all CSF results" (p2) |
||
| Flow and timing |
Duration of follow‐up: 2±0.7 years for MCI‐MCI and 2.1±0.5 years for MCI‐AD At follow‐up: 65 MCI: 43MCI‐MCI; 22 MCI‐AD (Abstract) Sensitivity 63%; Specificity: 69% for conversion to AD (p5) Number included in analyses=65 MCI: 29 with 'normal CSF abeta42/40 amyloid level': 26 MCI‐MCI; 3 MCI‐converters; 36 with 'abnormal CSF abeta amyloid level': 17 MCI‐MCI; 19 MCI‐converters TP=14; FP=13; FN=8; TN=30 Loss to follow up: data were reported for all 65 MCI participants |
||
| Comparative | |||
| Notes | |||
| Methodological quality | |||
| Item | Authors' judgement | Risk of bias | Applicability concerns |
| DOMAIN 1: Patient Selection | |||
| Was a consecutive or random sample of patients enrolled? | Yes | ||
| Was a case‐control design avoided? | Yes | ||
| Did the study avoid inappropriate exclusions? | Yes | ||
| Low | Low | ||
| DOMAIN 2: Index Test All tests | |||
| Were the index test results interpreted without knowledge of the results of the reference standard? | Yes | ||
| If a threshold was used, was it pre‐specified? | No | ||
| High | Low | ||
| DOMAIN 3: Reference Standard | |||
| Is the reference standards likely to correctly classify the target condition? | Yes | ||
| Were the reference standard results interpreted without knowledge of the results of the index tests? | Yes | ||
| Low | Low | ||
| DOMAIN 4: Flow and Timing | |||
| Was there an appropriate interval between index test and reference standard? | Yes | ||
| Did all patients receive the same reference standard? | Yes | ||
| Were all patients included in the analysis? | Yes | ||
| Low | |||
Chiasserini 2010.
| Study characteristics | |||
| Patient sampling | 98 participants attending a centre for memory disturbances in the period 2003‐2008. No further details of recruitment procedure reported. 32 participants had probable AD, 41 participants had MCI; 25 age‐matched participants, without signs of cognitive impairment, who underwent CSF analysis for other reasons (headache, suspected myopathy, etc) were also included. We only included data on performance of the index test to discriminate between patients with MCI who convert to dementia and those who remained stable. No exclusion criteria were reported |
||
| Patient characteristics and setting | 41 participants diagnosed by the Petersen 1999 criteria at baseline Gender: 20 men; 21 women; MCI‐MCI: 8 M; 10 F; MCI‐AD: 12 M; 11 F Age: 65.39 years; MCI‐MCI: 64.61±8.10; MCI‐AD: 67.17±7.71 APOE ϵ4 carrier: not reported MMSE: MCI‐MCI: 27.61±1.46; MCI‐AD: 26.91±1.57 Setting: secondary care, outpatients ‐ Center for Memory Disturbance, Perugia, Italy |
||
| Index tests | CSF: Abeta42 LP was performed in the morning, after overnight fasting, following a standardised procedure. CSF was collected in polypropylene tubes, gently mixed to avoid possible gradient effects, centrifugated at 1200 x g for 10 min, aliquoted and stored at ‐80ºC. Abeta1‐41 was measured using commercially available ELISA (no details reported). Threshold(s): 741pg/ml; determined at follow‐up from ROC analysis (Fig.1, B, p1284) At baseline 41 MCI: 22 with 'normal CSF abeta1‐42 level'; 19 with 'abnormal CSF abeta1‐42 level' Index test was conducted before clinical follow‐up |
||
| Target condition and reference standard(s) | Target condition: Alzheimer's disease dementia Reference standard: NINCDS‐ADRDA criteria Unclear whether clinicians conducting follow‐up were aware of CSF biomarker results |
||
| Flow and timing |
Duration of follow‐up: 4 years (annual follow‐up; mean follow‐up not reported) At follow‐up: 41 MCI: 23 MCI‐AD; 18 MCI‐MCI (p1282) Number included in analyses=41: 22 with 'normal CSF abeta amyloid level': 16 MCI‐MCI; 6 MCI‐AD; 19 with 'abnormal CSF abeta amyloid level': 2 MCI‐MCI; 17 MCI‐AD (Fig 1B) TP=17; FP=2; FN=6; TN=16 (Fig 1B) Loss to follow‐up: follow‐up data appear to have been available for all MCI participants |
||
| Comparative | |||
| Notes | |||
| Methodological quality | |||
| Item | Authors' judgement | Risk of bias | Applicability concerns |
| DOMAIN 1: Patient Selection | |||
| Was a consecutive or random sample of patients enrolled? | Unclear | ||
| Was a case‐control design avoided? | Yes | ||
| Did the study avoid inappropriate exclusions? | Unclear | ||
| Unclear | Low | ||
| DOMAIN 2: Index Test All tests | |||
| Were the index test results interpreted without knowledge of the results of the reference standard? | Yes | ||
| If a threshold was used, was it pre‐specified? | No | ||
| High | Low | ||
| DOMAIN 3: Reference Standard | |||
| Is the reference standards likely to correctly classify the target condition? | Yes | ||
| Were the reference standard results interpreted without knowledge of the results of the index tests? | Unclear | ||
| Unclear | Low | ||
| DOMAIN 4: Flow and Timing | |||
| Was there an appropriate interval between index test and reference standard? | Yes | ||
| Did all patients receive the same reference standard? | Yes | ||
| Were all patients included in the analysis? | Yes | ||
| Low | |||
Fei 2011.
| Study characteristics | |||
| Patient sampling | Participants were selected by random sampling of community‐dwelling elders (>65 years) from eight communities. Participants had to be native Chinese speakers, physically able to participate in study home visits, have no clinical diagnosis of dementia, consent to annual assessment, and have sufficient vision and hearing to complete neuropsychological tests. Participants meeting these criteria were assessed for eligibility based on presence of MCI (588 participants). Exclusion criteria: major depressive disorder; schizophrenia; substance abuse; mental retardation according to DSM‐IIIR; cerebrovascular disorders, hydrocephalus, intra‐cranial mass; abnormalities in serum folate and vitamin B12; syphilis serology; abnormalities in thyroid hormones; history of traumatic brain injury or other neurological disease; significant medical problems (e.g. poorly controlled diabetes or hypertension, cancer within the last 5 years, clinically significant hepatic, renal, cardiac or pulmonary disorders); use of psychotropic agents, nontropic drugs, cholinergic or anticholinergic agents , antiplatelet agents, anticoagulants, steroids, or serotoninergic drugs, unless a 14 day wash‐out had been observed |
||
| Patient characteristics and setting | 588 participants diagnosed with MCI by the Petersen 2001 criteria at baseline Demographic characteristics reported on 572 participants Gender: 209 men; 363 women. MCI‐MCI: 113 M; 127 F; MCI‐AD: 67 M; 178F; MCI‐other dementias: 29 M; 58 F Age: MCI‐MCI: 66±4.3 years; MCI‐AD:74±3.6; MCI‐other dementias: 75±3.9 APOE ϵ4 carrier: 290; MCI‐MCI: 74/240 (31%); MCI‐AD: 171/245 (66%); MCI‐other dementias: 45/87 (52%) MMSE: MCI‐MCI: 27.4±1.7; MCI‐AD:26.3±1.5; MCI‐other dementias: 26.9±1.4 Setting: community setting; index test assessed in the tertiary care ‐ research centre, Taiyuan city, China |
||
| Index tests | Plasma: Abeta42; Plasma Abeta42/Abeta 40 ratio Fasting morning plasma, drawn into ethylendiaminetetraacetic acid tubes. Samples spun immediately (10 min, 3000 rpm, 4ºC) and separated samples stored in polypropylene tubes at ‐80ºC. The plasma Abeta40 and Abeta42 peptide assay was performed using a sandwich enzyme‐linked immunosorbent assay constructed to specifically measure abeta amyloid. Plasma samples were assayed in triplicate on two 96‐well microtiter EUSA plates coated with R162 or R165. This method allowed the quantification of both lengths of Abeta and the ratio of the more aggregable form of the protein. Abeta40 and Abeta42 were simultaneously analysed. All peptide level measurements were performed in duplicate. Threshold(s): the optimal cut‐off values: 0.64 ng/ml for Abeta42; 0.95 ng/ml for Abeta42/40 ratio; determined at follow‐up from ROC analysis (p 94) Index test was conducted before clinical follow‐up |
||
| Target condition and reference standard(s) | Target condition: Alzheimer's disease dementia or other forms of dementia Reference standard: DSM‐III‐R criteria; NINCDS‐ADRDA criteria; NINDS‐AIREN Internatinal criteria; McKeith et al criteria Clinicians conducting follow‐up were blinded to the initial CSF analysis results |
||
| Flow and timing |
Duration of follow‐up: mean 5.2 years (range 4‐6.8 years) At follow‐up: 565: 332 MCI‐converters (245 MCI‐AD; 87 MCI‐other dementias); 233 MCI‐MCI for plasma Abeta42; 562: 332 MCI‐converters (245 MCI‐AD; 87 MCI‐other dementias); 230 MCI‐MCI (p94) For plasma Abeta42 a number included in analyses =565; sensitivity=85.7% and specificity=49.6% for conversion to AD dementia (p 94); TP=210; FP=161; FN=35; TN=159 For plasma Abeta42/Abeta 40 a number included in analyses=562; sensitivity=85.7% and specificity=69.7% for conversion to AD dementia (p94);TP=210; FP=96; FN=35; TN=221 Loss to follow‐up: 23 for plasma Abeta 42 (13 died before the last follow‐up ended; 7 dropped out because of adverse effects; 3 uninterpretable data); 26 for plasma Abeta42/Abeta 40 ratio (13 died before the last follow‐up ended; 7 dropped out because of adverse effects; 6 uninterpretable data) Withdrawals explained? Yes N=588; 13 participants died before the last follow‐up; 7 participants dropped out because of adverse effects |
||
| Comparative | |||
| Notes | |||
| Methodological quality | |||
| Item | Authors' judgement | Risk of bias | Applicability concerns |
| DOMAIN 1: Patient Selection | |||
| Was a consecutive or random sample of patients enrolled? | Unclear | ||
| Was a case‐control design avoided? | Yes | ||
| Did the study avoid inappropriate exclusions? | Yes | ||
| Low | Low | ||
| DOMAIN 2: Index Test All tests | |||
| Were the index test results interpreted without knowledge of the results of the reference standard? | Yes | ||
| If a threshold was used, was it pre‐specified? | No | ||
| High | Low | ||
| DOMAIN 3: Reference Standard | |||
| Is the reference standards likely to correctly classify the target condition? | Yes | ||
| Were the reference standard results interpreted without knowledge of the results of the index tests? | Yes | ||
| Low | Low | ||
| DOMAIN 4: Flow and Timing | |||
| Was there an appropriate interval between index test and reference standard? | Yes | ||
| Did all patients receive the same reference standard? | Yes | ||
| Were all patients included in the analysis? | No | ||
| Low | |||
Galluzzi 2010.
| Study characteristics | |||
| Patient sampling | 108 consecutive participants with MCI, referred to an outpatient memory clinic over 24 months Participants were excluded if they had a history or presence of neurological signs of major stroke |
||
| Patient characteristics and setting | 90 participants, who had diagnosed by the Petersen 1999 criteria at baseline and had follow‐up assessment, were included in the study; CSF was obtained from 64 participants. Demographic data are reported on 90 participants. Gender: 37 men; 53 women Age: mean 72.05 years; MCI‐MCI: 70.09±7.1; MCI‐AD: 72.2±7.1; MCI‐nAD: 25.5±1.9 APOE ϵ4 carrier: 35; MCI‐MCI: 19; MCI‐AD: 14; MCI‐nAD: 2 MMSE: MCI‐MCI: 26.3±1.9; MCI‐AD: 26.4±1.6; MCI‐other dementia: 73.0±7.1 Setting: secondary care, outpatients ‐ Translational Outpatient Memory Clinic (TOMC), Brescia, Italy |
||
| Index tests | CSF: Abeta42 CSF was obtained by lumbar tap between L4 and L5 or L3 and L4 and processed as detailed elsewhere (Frisoni 2009). Levels of Abeta42 protein was determined by commercially available enzyme linked immunosorbent assay (Innogenetics, Belgium). Threshold(s): <500 pg/ml; determined at baseline and based on published criteria (p 2006) At baseline 64 MCI: 29 with 'normal CSF Abeta42 level'; 35 with 'abnormal CSF Abeta42 level' Index test was conducted before clinical follow‐up |
||
| Target condition and reference standard(s) |
Target condition: Alzheimer's disease dementia or other forms of dementia Reference standard: NINCDS‐ADRDA criteria Unclear whether clinicians conducting follow‐up a were aware of initial CSF analysis results |
||
| Flow and timing |
Duration of follow‐up: 24.0 ± 9.7 months At follow‐up: 39/90 participants converted to dementia (Abstract) Number included in analyses=64: 29 with 'normal CSF Abeta42 amyloid level':15 MCI‐converters (4 MCI‐AD probable; 11 MCI‐non‐AD); 14 MCI‐MCI; 35 with 'abnormal CSF Abeta42 amyloid level': 19 MCI‐converters (16 MCI‐AD probable; 2 MCI‐AD possible; 1 MCI‐non‐AD); 16 MCI‐MCI (from Dr Galluzzi's emails) TP=18; FP=17; FN=4; TN=25 (conversion to AD dementia) TP=19; FP=16; FN=15; TN=14 (conversion to all dementia) TP=1; FP=34; FN=11; TN=18 (conversion to non‐AD dementia) Loss to follow‐up: 44 (16 refused follow‐up assessment; 2 did not follow‐up due to logistic problems; 24 refused LP; 2 failure to reach the arachnoid space due to osteoarthrosis) Withdrawals explained? No 18 participants from the consecutive sample (N=108) were excluded from the study because they did not have a follow‐up assessment. CSF was not available from 26/90 participants: 24 participants refuse the LP procedure; 2 LPs were not performed due to osteoarthrosis |
||
| Comparative | |||
| Notes | The trial investigators contacted; they provided data tor the 2x2 table to be completed; emails from Dr Galluzi on 30/3/12 and 5/1/13 | ||
| Methodological quality | |||
| Item | Authors' judgement | Risk of bias | Applicability concerns |
| DOMAIN 1: Patient Selection | |||
| Was a consecutive or random sample of patients enrolled? | Yes | ||
| Was a case‐control design avoided? | Yes | ||
| Did the study avoid inappropriate exclusions? | Yes | ||
| Low | Low | ||
| DOMAIN 2: Index Test All tests | |||
| Were the index test results interpreted without knowledge of the results of the reference standard? | Yes | ||
| If a threshold was used, was it pre‐specified? | Yes | ||
| Low | Low | ||
| DOMAIN 3: Reference Standard | |||
| Is the reference standards likely to correctly classify the target condition? | Yes | ||
| Were the reference standard results interpreted without knowledge of the results of the index tests? | Unclear | ||
| Unclear | Low | ||
| DOMAIN 4: Flow and Timing | |||
| Was there an appropriate interval between index test and reference standard? | Yes | ||
| Did all patients receive the same reference standard? | Yes | ||
| Were all patients included in the analysis? | No | ||
| High | |||
Hampel 2004.
| Study characteristics | |||
| Patient sampling | 93 participants with probable AD, 52 with MCI, and 10 healthy, age‐matched controls were recruited from a hospital rehabilitation department. We only included data on performance of the index test to discriminate between patients with MCI who convert to dementia and those who remained stable.The MCI group was not a consecutive sample and was selected at follow‐up. No exclusion criteria were specified |
||
| Patient characteristics and setting | 52 MCI participants diagnosed by the Petersen 1999 criteria at baseline Gender: 24 men; 28 women Age: mean age 72.6 years (range 54–87) APOE ϵ4 carrier: not reported MMSE (all MCI): 28.9±1 (range 26‐30) Setting: secondary care, inpatients ‐ Department of Rehabilitation, Pitea, Sweden |
||
| Index tests | CSF: Abeta42 CSF Abeta 1‐42 to predict conversion from MCI to AD CSF samples were taken by lumbar puncture, collected in polypropylene tubes, and stored at ‐80ºC. Abeta1–42 was measured in duplicate using a commercial ELISA (Innotest beta‐amyloid 1‐42, Innogenetics, Belgium) Threshold(s): <679 ng/l, established in the MCI‐MCI versus MCI‐AD at follow‐up (p707) At follow‐up: 18 with 'normal CSF Abeta42 amyloid level': 13 MCI‐MCI; 5 MCI‐AD; 34 with 'abnormal CSF Abeta42 amyloid level': 10 MCI‐MCI; 24 MCI‐AD Index test was conducted before clinical follow‐up |
||
| Target condition and reference standard(s) | Target condition: Alzheimer's disease dementia Reference standard: NINCDS‐ADRDA criteria; DSM‐IV criteria Unclear whether clinicians conducting follow‐up a were aware of initial CSF analysis results |
||
| Flow and timing |
Duration of follow‐up: mean 8.4±5.1 months (range 2‐24 months); follow‐up interval for converters was 9.6±5.4, and for non‐converters 7.0±4.3 months At follow‐up: 52 MCI: 29 MCI‐AD; 23 MCI‐MCI (p94) Number included in analysis=52; Sensitivity 83%; Specificity 57% (p707); D+ 29: D‐ 23 TP=24; FP=10; FN=5; TN=13 Loss to follow‐up: data for all 52 MCI participants were reported |
||
| Comparative | |||
| Notes | |||
| Methodological quality | |||
| Item | Authors' judgement | Risk of bias | Applicability concerns |
| DOMAIN 1: Patient Selection | |||
| Was a consecutive or random sample of patients enrolled? | No | ||
| Was a case‐control design avoided? | Yes | ||
| Did the study avoid inappropriate exclusions? | Unclear | ||
| High | Low | ||
| DOMAIN 2: Index Test All tests | |||
| Were the index test results interpreted without knowledge of the results of the reference standard? | Yes | ||
| If a threshold was used, was it pre‐specified? | No | ||
| High | Low | ||
| DOMAIN 3: Reference Standard | |||
| Is the reference standards likely to correctly classify the target condition? | Yes | ||
| Were the reference standard results interpreted without knowledge of the results of the index tests? | Unclear | ||
| Unclear | Low | ||
| DOMAIN 4: Flow and Timing | |||
| Was there an appropriate interval between index test and reference standard? | No | ||
| Did all patients receive the same reference standard? | Yes | ||
| Were all patients included in the analysis? | Yes | ||
| High | |||
Hansson 2007.
| Study characteristics | |||
| Patient sampling | 137 patients with MCI, who had sought medical advice for subjective memory difficulties and from whom CSF was obtained at baseline, recruited at a University hospital. 36 healthy controls were also included, but appear to have been used for comparison purposes only and not included in the ROC analysis. No exclusion criteria were specified |
||
| Patient characteristics and setting | 137 participants diagnosed by the Petersen 1999 criteria. Baseline demographic data reported for 131 participants GENDER: 58 men; 73 women AGE (median): MCI‐MCI (stable) 65 years; MCI‐AD 75 years; MCI‐other dementia 76 years; range 50‐85 years APOE ϵ4 carrier: not reported MMSE: MCI‐MCI 27.3±1.8; MCI‐AD 26.9±1.4; MCI‐other dementia 27.0±1.5 Setting: secondary care, outpatients ‐ memory disorder clinic, University hospital, Malmo, Sweden |
||
| Index tests | CSF: Abeta42; Abeta42/Abeta40 ratio Abeta42 and Abeta40 concentrations were determined by commercially available ELISA kits (The Genetics Company) using the capture antibody W02 (epitope Abeta5–8) and the detection antibodies G2–10 for A 40 and G2–13 for A 42 Threshold (s) : determined at follow‐up (p 318); ROC analyses were used to identify optimal cut‐offs: 0.64 ng/ml for Abeta42 and 0.95 ng/l for Abeta42/Abeta40 ratio Index test was conducted before clinical follow‐up |
||
| Target condition and reference standard(s) | Target condition: Alzheimer's disease dementia or other forms of dementia Reference standards: NINCDS‐ADRDA and DSM‐III‐R for Alzheimer's disease dementia; DSM‐III‐R for vascular dementia; McKeith for Lewy bodies dementia and Brun for frontotemporal dementia Unclear whether clinicians conducting follow‐up were aware of CSF biomarker results |
||
| Flow and timing |
Duration of follow‐up: range: mean: 5.2 years (4‐6.8 years) At follow‐up:134 MCI: 57 MCI‐AD; 21 MCI‐other dementias (15 SVD; 3LBD; 1 FTD; 1 semantic dementia; 1 traumatic brain injury‐induced dementia); 56 MCI‐MCI (stable); (p317) Number included in analysis: 134 Conversion to AD dementia for CSF Abeta42: Sensitivity 93%; Specificity 53% (p318) TP=53; FP=36; FN=4; TN=41 Conversion to AD dementia for CSF Abeta42/Abeta40 ratio; Sensitivity 87%; Specificity 78% (p318) TP=50; FP=17; FN=7; TN=60 Loss to follow‐up: 3 participants died before completion of 4 years follow‐up and were excluded from the analyses because their cognitive ability was uncertain |
||
| Comparative | |||
| Notes | |||
| Methodological quality | |||
| Item | Authors' judgement | Risk of bias | Applicability concerns |
| DOMAIN 1: Patient Selection | |||
| Was a consecutive or random sample of patients enrolled? | Unclear | ||
| Was a case‐control design avoided? | Yes | ||
| Did the study avoid inappropriate exclusions? | Unclear | ||
| Unclear | Low | ||
| DOMAIN 2: Index Test All tests | |||
| Were the index test results interpreted without knowledge of the results of the reference standard? | Yes | ||
| If a threshold was used, was it pre‐specified? | No | ||
| High | Low | ||
| DOMAIN 3: Reference Standard | |||
| Is the reference standards likely to correctly classify the target condition? | Yes | ||
| Were the reference standard results interpreted without knowledge of the results of the index tests? | Unclear | ||
| Unclear | Low | ||
| DOMAIN 4: Flow and Timing | |||
| Was there an appropriate interval between index test and reference standard? | Yes | ||
| Did all patients receive the same reference standard? | Yes | ||
| Were all patients included in the analysis? | No | ||
| Low | |||
Hertze 2010.
| Study characteristics | |||
| Patient sampling | 94 patients with AD, 166 patients with MCI and 29 patients with depressive disorder recruited from a university hospital memory clinic and 38 healthy controls. We only included data on performance of the index test to discriminate between patients with MCI who convert to dementia and those who remained stable. Patients with other causes of cognitive impairment (subdural haematoma, brain tumour, CNS infection,schizophrenia, major depressive episode, or current alcohol abuse) were excluded. MCI participants with signs of white matter changes or silent brain infarctions were not excluded, because these changes are common in the elderly. MCI participants with moderate depression and low plasma concentrations of vitamin B12 or folate were also not excluded. |
||
| Patient characteristics and setting | 166 MCI participants diagnosed by the Petersen 2004 criteria at baseline. Baseline demographic data reported for 159 participants. Gender: 65 men; 91women. MCI‐MCI: 36 M; 46 F; MCI‐AD: 18 M; 34 F; MCI‐other: 14 M; 11 F Age: mean 72 (7.3) years; MCI‐MCI 69 (7.5) years; MCI‐AD 76 (7.8) years; MCI‐other 72 (6.7) years APOE ϵ4 carrier: 63; MCI‐MCI 37/82 (45%); MCI‐AD 40/52 (77%); MCI‐other 12/25 (48%) MMSE: MCI‐MCI: 28.3 (1.3); MCI‐MD: 26.1 (1.6); MCI‐AD 26.9 (2.0) Setting: secondary care, outpatients ‐ memory clinic, Malmo University hospital, Sweden |
||
| Index tests | CSF: Abeta42 CSF was collected in polypropylene tubes, stored at −80C and analysed after the clinical follow‐up of the study was completed. The procedure followed The Alzheimer’s Association Flow Chart for LP and CSF sample processing (Blennow 2010). Abeta 42 and Abeta 40 levels were analysed using an electrochemiluminescence method, using the MS6000 Human Abeta 3‐Plex Ultra‐sensitive kit (Meso Scale Discovery, USA). Threshold(s): 209 pg/ml determined at baseline and based on previously established cut‐off levels in AD, control and depression (Fig.3B, p1125) At baseline MCI:101 with 'normal CSF abeta42 level'; with 'abnormal CSF abeta42 level' It was unclear whether those interpreting the index test results were aware of the outcome of clinical follow‐up |
||
| Target condition and reference standard(s) | Target condition: Alzheimer's disease dementia or other forms of dementia Reference standards: NINCDS‐ADRDA and DSM‐III‐R criteria for Alzheimer's disease dementia; NINDS‐AREN ICD and DSM‐III‐R criteria for vascular dementia; McKeith criteria for LB dementia The index test was conducted using stored samples, after clinical follow‐up |
||
| Flow and timing |
Duration of follow‐up: 4.7 years (range 3.0‐7.2) At follow‐up: 166 MCI: 81 MCI‐converters (55 MCI‐AD; 26 MCI‐other); 85 MCI‐MCI (p1125) Number included in analyses=159: 77 MCI‐converters (52 MCI‐AD; 25 MCI‐other); 82 MCI‐MC TP=47; FP=32; FN=5; TN=75 for conversion to Alzheimer's disease dementia (Fig 1B, p1125) TP=11; FP=68; FN=14; TN=66 for conversion to non‐Alzheimer's disease dementia (Fig 1B, p1125) TP=58; FP=21; FN=19; TN=61 for conversion to all dementias (Fig 1B, p1125) Loss to follow‐up: In 7 MCI participants xMAP analysis resulted in technical errors and this sample was excluded from the study (p1121) |
||
| Comparative | |||
| Notes | The trial investigators contacted; they confirmed that their study is not a multiple publication to Hansson 2007; email from Dr Hertze on 7/1/13 | ||
| Methodological quality | |||
| Item | Authors' judgement | Risk of bias | Applicability concerns |
| DOMAIN 1: Patient Selection | |||
| Was a consecutive or random sample of patients enrolled? | Unclear | ||
| Was a case‐control design avoided? | Yes | ||
| Did the study avoid inappropriate exclusions? | Yes | ||
| Unclear | Low | ||
| DOMAIN 2: Index Test All tests | |||
| Were the index test results interpreted without knowledge of the results of the reference standard? | Unclear | ||
| If a threshold was used, was it pre‐specified? | Yes | ||
| Low | Low | ||
| DOMAIN 3: Reference Standard | |||
| Is the reference standards likely to correctly classify the target condition? | Yes | ||
| Were the reference standard results interpreted without knowledge of the results of the index tests? | Yes | ||
| Low | Low | ||
| DOMAIN 4: Flow and Timing | |||
| Was there an appropriate interval between index test and reference standard? | Yes | ||
| Did all patients receive the same reference standard? | Yes | ||
| Were all patients included in the analysis? | No | ||
| Low | |||
Herukka 2007.
| Study characteristics | |||
| Patient sampling | Participants examined in a university hospital neurological department,or from an ongoing population‐based study were included if they agreed to a lumbar puncture for research purposes and had a baseline diagnosis of MCI; 79 participants met these criteria. 60 controls (who were referred to the neurological department for different symptoms, or who were included in the population‐based study and had depression with normal performance inneuropsychological tests) were also included. We only included data on performance of the index test to discriminate between patients with MCI who convert to dementia and those who remained stable. No exclusion criteria were specified |
||
| Patient characteristics and setting | 79 MCI participants diagnosed by the CDR=0.5 criteria at baseline. Gender: 33 men; 46 women Age:70.56 years; MCI‐MCI: 69.46֨±8.14; MCI‐progressive: 71.76±6.71 APOE ϵ4 carrier: 41; MCI‐MCI: 15/45 (33.3%); MCI‐progressive: 26/33 (78.8%) MMSE: MCI‐MCI: 24.09±2.49; MCI‐progressive: 23.91±2.69 Setting: Secondary care, inpatients ‐ Neurological department, Kuopio University Hospital, Finland |
||
| Index tests | CSF Abeta42 The CSF samples were collected by LP during the baseline visit. The samples were stored in polypropylene tubes at ‐70°C until analysis. CSF Abeta 42 analysed using a commercial ELISA (Innogenetics, Belgium) Threshold(s): 450 pg/ml; determined at baseline using previously published cut off values from the ROC analysis (Herruka 2005) At baseline 79 MCI: 48 with 'normal CSF Abeta42 level'; 31 with 'abnormal CSF Abeta42 level' Index test was conducted before clinical follow‐up |
||
| Target condition and reference standard(s) | Target condition: Alzheimer's disease dementia or other forms of dementia Reference standard: NINCDS‐ADRDA for Alzheimer's disease dementia; DSM‐IV‐R criteria for other dementia Diagnosis of dementia was done independently and blinded to CSF biomarker results |
||
| Flow and timing |
Duration of follow‐up: mean 3.52±1.95 years in MCI‐converters; mean 4.56±3.09 years in MCI‐stable At follow‐up:79 MCI: 33 MCI‐converters (27 MCI‐AD; 1 MCI‐SVD; 5 MCI‐MD); 46 MCI‐MCI (p509) Number included in analyses=79: 48 with 'normal CSF Abeta amyloid level': 35 MCI‐MCI; 13 MCI‐converters; 31 with 'abnormal CSF Abeta42 amyloid level': 11 MCI‐MCI; 20 MCI‐converters (Fig 1, p510) TP=20, FP=11, FN=13, TN=35 (Fig 1, p510) (for all dementias) Loss to follow‐up: CSF marker and follow‐up data appeared to have been available for all participants |
||
| Comparative | |||
| Notes | |||
| Methodological quality | |||
| Item | Authors' judgement | Risk of bias | Applicability concerns |
| DOMAIN 1: Patient Selection | |||
| Was a consecutive or random sample of patients enrolled? | No | ||
| Was a case‐control design avoided? | Yes | ||
| Did the study avoid inappropriate exclusions? | Unclear | ||
| High | Low | ||
| DOMAIN 2: Index Test All tests | |||
| Were the index test results interpreted without knowledge of the results of the reference standard? | Yes | ||
| If a threshold was used, was it pre‐specified? | Yes | ||
| Low | Low | ||
| DOMAIN 3: Reference Standard | |||
| Is the reference standards likely to correctly classify the target condition? | Yes | ||
| Were the reference standard results interpreted without knowledge of the results of the index tests? | Yes | ||
| Low | Low | ||
| DOMAIN 4: Flow and Timing | |||
| Was there an appropriate interval between index test and reference standard? | Yes | ||
| Did all patients receive the same reference standard? | Yes | ||
| Were all patients included in the analysis? | Yes | ||
| Low | |||
Kester 2011.
| Study characteristics | |||
| Patient sampling | 153 MCI participants with available CSF results and APOE ϵ4 genotyping were recruited from the memory clinic in the period between January 2001 and May 2008. 107 of those 153 patients had follow‐up data available. No exclusion criteria were reported |
||
| Patient characteristics and setting | 153 MCI participants diagnosed by the Petersen 1999 criteria at baseline. Baseline demographic data reported for 100 participants, who were included in the analysis. Gender: 59 men; 41 women. MCI‐MCI: 38 M; 20 F; MCI‐AD: 21 M; 21 F Age: 67±9 years MCI‐MCI; 69±7 years MCI‐AD APOE ϵ4 carrier: 27/58 MCI‐MCI; 30/42 MCI‐AD MMSE: 27±2 MCI‐MCI; 26±3 MCI‐AD Setting: secondary care, outpatients ‐ memory clinic, Amsterdam, Netherlands |
||
| Index tests | CSF: Abeta42 CSF was obtained by lumbar puncture between the L3/L4 and L4/L5 intervertebral space and collected in 10ml polypropylene tubes. CSF samples were processed within 2 hours (centrifuged at 1800 g for 10 min at 4°C and stored at ‐80°C in polypropylene tubes until analysis). Abeta42 was measured using a commercial sandwich ELISA (Innotest). Threshold(s): <495 pg/ml abnormal level; determined at baseline and based on published data (Table 1, p1374) Index test was conducted before clinical follow‐up |
||
| Target condition and reference standard(s) | Target condition: Alzheimer's disease dementia or other forms of dementia Reference standard: NINCDS‐ADRDA criteria Alzheimer's disease dementia; Neary 1998 criteria; Roman 1993 criteria; McKeith 2005 criteria Unclear whether clinicians conducting follow‐up were aware of CSF biomarker results |
||
| Flow and timing |
Duration of follow‐up: median 18 months (IQR 13‐24); for MCI‐converters the median was 17 months (IQR 13‐24); for MCI‐stable the median was 18 months (IQR 12‐25) At follow‐up: 107 MCI: 49 MCI‐converters (42 MCI‐AD; 3 MCI‐FTD, 2 MCI‐VD; 1 MCI‐LBD; 1 MCI‐dementia due to hydrocephalus); 58 MCI‐MCI (p1373) Number included in analyses=100: 52 with 'normal' CSF Abeta42 level: 42 MCI‐MCI, 10 MCI‐AD; 48 'abnormal' CSF Abeta42 level: 16 MCI‐MCI, 32 MCI‐AD (Table 1, p1374) TP=32; FP=16; FN=10; TN=42 Loss to follow‐up: 53: 7 'MCI participants who converted to other dementias were excluded from the analysis; 46 participants did not have follow‐up data; no further information |
||
| Comparative | |||
| Notes | |||
| Methodological quality | |||
| Item | Authors' judgement | Risk of bias | Applicability concerns |
| DOMAIN 1: Patient Selection | |||
| Was a consecutive or random sample of patients enrolled? | No | ||
| Was a case‐control design avoided? | Yes | ||
| Did the study avoid inappropriate exclusions? | Unclear | ||
| High | Low | ||
| DOMAIN 2: Index Test All tests | |||
| Were the index test results interpreted without knowledge of the results of the reference standard? | Yes | ||
| If a threshold was used, was it pre‐specified? | Yes | ||
| Low | Low | ||
| DOMAIN 3: Reference Standard | |||
| Is the reference standards likely to correctly classify the target condition? | Yes | ||
| Were the reference standard results interpreted without knowledge of the results of the index tests? | Unclear | ||
| Unclear | Low | ||
| DOMAIN 4: Flow and Timing | |||
| Was there an appropriate interval between index test and reference standard? | No | ||
| Did all patients receive the same reference standard? | Yes | ||
| Were all patients included in the analysis? | No | ||
| High | |||
Monge‐Argiles 2011.
| Study characteristics | |||
| Patient sampling | 37 patients with MCI, attending the cognitive deterioration out‐patients clinic of a general hospital and 24 control subjects without subjective memory loss or known cognitive deterioration. We only included data on performance of the index test to discriminate between patients with MCI who convert to dementia and those who remained stable. Participants with dementia or other neurological, psychiatric or medical disease which could provoke cognitive deterioration, anti‐coagulant therapy, failure to obtain informed consent, or a Yesavage depression scale score >5 were excluded |
||
| Patient characteristics and setting | 37 participants diagnosed by the Petersen 2006 criteria at baseline Gender: 13 men; 24 women; MCI‐MCI: 11M, 15F; MCI‐AD: 2M, 9F Age: mean 73.43±6.63 years APOE ϵ4 carrier: not reported MMSE: mean 25±2.4; MCI‐AD: mean 23±1.2 Time between MCI diagnosis and study entry (months): 1‐12 (n=5); 13‐24 (n=9); 25‐36 (n=1); 37‐48 (n=3); 49‐60 (n=6); >61: 2 Setting: secondary care, outpatients ‐ General Hospital, Spain |
||
| Index tests | CSF: Abeta42 The LP was performed by their own neurologist with a 20X3.5 gauge needle. CSF was collected in standard tubes and centrifuged if little sanguinolent, before being frozen. CSF samples with obvious blood were discarded. Abeta 1–42 was analysed using xMAP Luminex technology and INNO‐BIA Alzbio3 reagents (Innogenetics, Belgium). Threshold(s): 320 pg/ml; determined at follow‐up and derived from ROC analysis of controls and the whole MCI population (Table 6, p 990) At baseline 37 MCI: 18 with 'normal CSF Abeta amyloid level'; 19 with 'abnormal CSF Abeta amyloid level' Index test was conducted before clinical follow‐up |
||
| Target condition and reference standard(s) | Target condition: Alzheimer's disease dementia Reference standard: NINCDS‐ADRDA criteria Unclear whether clinicians conducting follow‐up were aware of CSF biomarker results |
||
| Flow and timing |
Duration of follow‐up: 6 months At follow‐up: 37MCI: 11 MCI‐AD; 26 MCI‐MCI (Table 1, p989); Sensitivity 82%; Specificity 62% (Table 6, p990) Number included in analyses=37 MCI: 18 with 'normal CSF Abeta amyloid level': 16 MCI‐MCI; 2 MCI‐converters; 19 with 'abnormal CSF Abeta amyloid level': 10 MCI‐MCI; 9 MCI‐converters TP=9, FP=10, FN=2, TN=16 Loss to follow‐up: CSF marker and follow‐up data appeared to have been available for all participants |
||
| Comparative | |||
| Notes | |||
| Methodological quality | |||
| Item | Authors' judgement | Risk of bias | Applicability concerns |
| DOMAIN 1: Patient Selection | |||
| Was a consecutive or random sample of patients enrolled? | Unclear | ||
| Was a case‐control design avoided? | Yes | ||
| Did the study avoid inappropriate exclusions? | Yes | ||
| Low | Low | ||
| DOMAIN 2: Index Test All tests | |||
| Were the index test results interpreted without knowledge of the results of the reference standard? | Yes | ||
| If a threshold was used, was it pre‐specified? | No | ||
| High | Low | ||
| DOMAIN 3: Reference Standard | |||
| Is the reference standards likely to correctly classify the target condition? | Yes | ||
| Were the reference standard results interpreted without knowledge of the results of the index tests? | Unclear | ||
| Unclear | Low | ||
| DOMAIN 4: Flow and Timing | |||
| Was there an appropriate interval between index test and reference standard? | No | ||
| Did all patients receive the same reference standard? | Yes | ||
| Were all patients included in the analysis? | Yes | ||
| High | |||
Papaliagkas 2009.
| Study characteristics | |||
| Patient sampling | 53 patients with MCI, selected from a hospital memory and dementia clinic No exclusion criteria were reported |
||
| Patient characteristics and setting | 53 MCI participants diagnosed by the Petersen 1999 criteria at baseline Gender: 22 men; 31 women Age: 67.2 years MCI‐MCI; 73.0 years MCI‐AD APOE ϵ4 carrier: not reported MMSE: 28 (27‐29) MCI‐MCI; 26 (24‐28) MCI‐AD Setting: secondary care, outpatients ‐ Memory and Dementia clinic, 'G. Papanikolaou' Hospital, Thessaloniki, Greece |
||
| Index tests | CSF: Abeta42 LP through L3/L4 or L4/L5 interspace. All CSF samples were stored at –80 ° C until analysis. Abeta 1‐42 analysis used a commercial sandwich ELISA (Innotest‐amyloid (1–42), Innogenetics, Belgium). Threshold(s): 472 pg/ml; determined at follow‐up nd derived from ROC analysis (p32) At baseline 53 MCI: 37 with 'normal Abeta42 level'; 16 with 'abnormal CSF Abeta1‐42 level' Index test was conducted before clinical follow‐up |
||
| Target condition and reference standard(s) | Target condition: Alzheimer's disease dementia Reference standard: the criteria used to define progression to Alzheimer's disease dementia were not clearly defined Unclear whether clinicians conducting follow‐up were aware of CSF biomarker results |
||
| Flow and timing |
Duration of follow‐up: 11 months At follow‐up: 53 MCI: 5 MCI‐AD; 48 MCI‐MCI (Table 1, p32; Fig 2, p33) Number included in analyses=53; Sensitivity 100%; Specificity 77.1% (p32) TP=5, FP=11, FN=0, TN=37 Loss to follow‐up: CSF marker and follow‐up data appeared to have been available for all participants |
||
| Comparative | |||
| Notes | Relevant clinical information? Unclear from text | ||
| Methodological quality | |||
| Item | Authors' judgement | Risk of bias | Applicability concerns |
| DOMAIN 1: Patient Selection | |||
| Was a consecutive or random sample of patients enrolled? | Unclear | ||
| Was a case‐control design avoided? | Yes | ||
| Did the study avoid inappropriate exclusions? | Unclear | ||
| Unclear | Low | ||
| DOMAIN 2: Index Test All tests | |||
| Were the index test results interpreted without knowledge of the results of the reference standard? | Yes | ||
| If a threshold was used, was it pre‐specified? | No | ||
| High | Low | ||
| DOMAIN 3: Reference Standard | |||
| Is the reference standards likely to correctly classify the target condition? | Unclear | ||
| Were the reference standard results interpreted without knowledge of the results of the index tests? | Unclear | ||
| Unclear | High | ||
| DOMAIN 4: Flow and Timing | |||
| Was there an appropriate interval between index test and reference standard? | No | ||
| Did all patients receive the same reference standard? | Yes | ||
| Were all patients included in the analysis? | Yes | ||
| High | |||
Parnetti 2006.
| Study characteristics | |||
| Patient sampling | 273 consecutive patients with a suspected cognitive impairment were referred by GPs or other specialists to an out‐patient memory clinic during the period January 2001 to June 2003. Exclusion criteria: patients fulfilling clinical and neuroradiological criteria for subcortical ischaemic vascular dementia were excluded; patients with secondary cases of cognitive impairment were also excluded. No further exclusion criteria were defined |
||
| Patient characteristics and setting | 55 MCI participants were diagnosed by the Petersen 1999 criteria at baseline Gender: not reported Age: not reported APOE ϵ4 carrier: not reported MMSE: not reported Setting: secondary care, memory clinic, Perugia, Italy |
||
| Index tests | CSF: Abeta42 CSF was centrifuged for 10 min at 4000 g, then stored at ‐80ºC until analysis. Abeta 42 was assessed using a commercial ELISA (Innotest b‐amyloid 1–42, Innogenetics). Threshold(s): 500 pg/l; determined at baseline and based on published criteria (p130) At baseline 55 participants: 47 with 'normal CSF Abeta1‐42 level'; 8 with 'abnormal CSF Abeta1‐42 level' Index test was conducted before clinical follow‐up |
||
| Target condition and reference standard(s) | Target condition: Alzheimer's disease dementia Reference standard: NINCDS‐ADRDA criteria Unclear whether clinicians conducting follow‐up were aware of CSF biomarker results |
||
| Flow and timing |
Duration of follow‐up: 12 months At follow‐up: 55 MCI: 11 MCI‐AD; 33 MCI‐MCI (stable); 11 participants showed a further progression of cognitive impairment, still not fulfilling the diagnostic criteria for dementia (p130) Number included in analyses=55: 11 MCI‐ADD; 44 MCI‐non‐converters; Sensitivity 36%; Specificity 91% (p131) TP=4, FP=4; FN=7; TN=40 Loss to follow‐up: CSF marker and follow‐up data appeared to have been available for all participants |
||
| Comparative | |||
| Notes | |||
| Methodological quality | |||
| Item | Authors' judgement | Risk of bias | Applicability concerns |
| DOMAIN 1: Patient Selection | |||
| Was a consecutive or random sample of patients enrolled? | Yes | ||
| Was a case‐control design avoided? | Yes | ||
| Did the study avoid inappropriate exclusions? | Unclear | ||
| Low | Low | ||
| DOMAIN 2: Index Test All tests | |||
| Were the index test results interpreted without knowledge of the results of the reference standard? | Yes | ||
| If a threshold was used, was it pre‐specified? | Yes | ||
| Low | Low | ||
| DOMAIN 3: Reference Standard | |||
| Is the reference standards likely to correctly classify the target condition? | Yes | ||
| Were the reference standard results interpreted without knowledge of the results of the index tests? | Unclear | ||
| Unclear | Low | ||
| DOMAIN 4: Flow and Timing | |||
| Was there an appropriate interval between index test and reference standard? | No | ||
| Did all patients receive the same reference standard? | Yes | ||
| Were all patients included in the analysis? | Yes | ||
| High | |||
Shaw 2009.
| Study characteristics | |||
| Patient sampling | 819 Participants from the ADNI longitudinal neuroimaging study who met the criteria for initial diagnosis of amnestic MCI (397), probable AD (193), or normal cognition (229). The ADNI is a large multicenter, longitudinal neuroimaging study; participants have been recruited from over 50 sites across the United States and Canada. Baseline CSF samples were available for 416 participants (200 with amnestic MCI, 102 with probable AD and 114 with normal cognition). We only included data on performance of the index test to discriminate between patients with MCI who convert to dementia and those who remained stable. Data from normal controls were used, along with data from samples from ADNI‐independent, autopsy‐confirmed AD cases, to derive cut‐off values for biomarkers. Exclusion criteria: any serious neurological disease other than possible AD, history of brain lesions of head trauma, use of psychoactive medication (antidepressants, neuroleptics, chronic anxiolytics, or sedative hypnotics) |
||
| Patient characteristics and setting | 200 participants with baseline CSF sample, diagnosed with MCI condition if: i) a Mini‐Mental State Examination score was 24 to 30; ii) a Memory Box score was at least 0.5. Baseline demographic data reported for 196 participants. Manuscript cited the full ADNI protocol available on line and this confirmed use of Petersen Criteria components as inclusion for their amnestic MCI group. Gender: 131men / 65 women Age: 75 years MCI‐MCI; 76 years MCI‐ADD APOE ϵ4 carrier: 106 MMSE: 26.9±1.8 Participants fulfilling the criteria for the clinical diagnosis of MCI Setting: mixed setting; multicentre study ‐ USA |
||
| Index tests | CSF: Abeta42 CSF samples were obtained in the morning, following overnight fast. Samples were transferred into polypropylene transfer tubes and frozen on dry ice within 1 hour of collection, and shipped overnight to the ADNI Biomarker Core laboratory at the University of Pennsylvania Medical Center. Samples were then stored in polypropylene vials at ‐80°C. Abeta 1‐42 was analysed using the multiplex xMAP Luminex platform (Luminex, Texas) with immunoassay kit‐based reagents (Innogenetics, Belgium). Threshold: 192 pg/ml determined at baseline and derived from ROC analysis of the ADNI normal cognition subjects and the ADNI‐independent autopsy‐confirmed AD samples (fig 1, p407) At baseline196 MCI: 51 with 'normal CSF Abeta1‐42 level'; 145 with 'abnormal CSF Abeta1‐42 level Index test was conducted before clinical follow‐up |
||
| Target condition and reference standard(s) | Target condition: Alzheimer's disease dementia Reference standard: NINCDS‐ADRDA (all MCI‐ADD participants met criteria for probable AD: MMSE score was between 20 and 26, a global Clinical Dementia Rating was 0.5 or 1, a sum‐of‐boxes Clinical Dementia Rating was 1.0 to 9.0) Unclear whether clinicians conducting follow‐up were aware of CSF biomarker results |
||
| Flow and timing |
Duration of follow‐up: 12 months At follow‐up: 196 MCI: 37 MCI‐AD; 156 MCI‐MCI; 3 MCI‐normal (Table 2, p408) Number included in analyses=196: 37 MCI‐AD; 159 MCI‐non‐converters TP=32, FP=113, FN=5, TN=46 (Fig 1B; Fig 3) Loss to follow‐up: 4 participants; no reasons were reported |
||
| Comparative | |||
| Notes | |||
| Methodological quality | |||
| Item | Authors' judgement | Risk of bias | Applicability concerns |
| DOMAIN 1: Patient Selection | |||
| Was a consecutive or random sample of patients enrolled? | No | ||
| Was a case‐control design avoided? | Yes | ||
| Did the study avoid inappropriate exclusions? | Yes | ||
| High | Low | ||
| DOMAIN 2: Index Test All tests | |||
| Were the index test results interpreted without knowledge of the results of the reference standard? | Yes | ||
| If a threshold was used, was it pre‐specified? | Yes | ||
| Low | Low | ||
| DOMAIN 3: Reference Standard | |||
| Is the reference standards likely to correctly classify the target condition? | Yes | ||
| Were the reference standard results interpreted without knowledge of the results of the index tests? | Unclear | ||
| Unclear | Low | ||
| DOMAIN 4: Flow and Timing | |||
| Was there an appropriate interval between index test and reference standard? | No | ||
| Did all patients receive the same reference standard? | Yes | ||
| Were all patients included in the analysis? | No | ||
| High | |||
Vos 2013.
| Study characteristics | |||
| Patient sampling | 399 participants with aMCI and 226 participants with naMCI from the DESCRIPA cohort and Alzheimer Center of the VU University medical center (VUmc). DESCRIPA is a European multicentre study performed in a memory‐clinic setting and enrolled subjects between 2003 and 2005.11 For this study, 431 eligible subjects were selected from 16 participating centers in which CSF was collected, MRI was performed, or APOE genotype was determined. The VUmc center was one of the DESCRIPA centers and contributed an additional sample of 194 subjects that were seen outside the DESCRIPA inclusion period with data on CSF, MRI, or APOE measures. No differences in biomarkers were found between subjects from the VUmc center in the DESCRIPA study and those from the additional VUmc sample. Exclusion criteria were diagnosis of dementia at baseline or any other somatic, psychiatric or neurological disorder that might have caused the cognitive impairment |
||
| Patient characteristics and setting | 625 MCI participants diagnosed by Petersen 2004 criteria at baseline. 231 of those participants had CSF Abeta1‐42 assessment. 214 subjects with CSF data had a least one follow‐up assessment. Baseline demographic data reported on all 625 participants. Gender: 270 men; 335 women Age: 70.7±7.6 years naMCI; 70.7±7.8 aMCI MMSE: 27.5±2.1 naMCI; 26.5±2.5 aMCI Setting: secondary care ‐ European multicentre memory clinics |
||
| Index tests | CSF Abeta1‐42 CSF was collected by lumbar puncture, centrifuged, and stored at ‐80°C in polypropylene tubes. Three samples were thawed twice but analyses without these samples revealed similar results. CSF Abeta1‐42 and total tau (t‐tau) were measured by experienced technicians using commercially available sandwich ELISAs (Innotest Abeta‐amyloid 1‐42; Innotest hTAU‐Ag; Innogenetics, Ghent, Belgium), specially constructed to measure Abeta‐amyloid 1‐42 and t‐tau, at the lab in Gothenburg for the DESCRIPA cohort and in Amsterdam for the additional subjects of the VUmc cohort. We corrected for interlaboratory ELISA differences by analyzing 33 samples at both labs and we adjusted VUmc values to those of DESCRIPA using the following formula: Gothenborg=(SD Gothenborg/SD VUmc)*VUmc+average Gothenborg– ((SD Gothenborg /SD VUmc)*average VUmc). Threshold: <500 pg/ml determined at baseline and based on published criteria (Hulstaert 1999; Wolz 2010) At baseline 214 MCI: 111 with 'normal CSF Abeta42 level'; 103 with 'abnormal CSF Abeta42 level' Index test was conducted before follow‐up |
||
| Target condition and reference standard(s) | Target condition: Alzheimer's disease dementia Reference standard: DSM‐IV criteria; NINCDS‐ADRDA criteria Diagnosis of dementia was conducted blinded to results of CSF biomarker analysis (p8) |
||
| Flow and timing |
Duration of follow‐up: mean 2.5 years (max duration 5 years); follow‐up was performed annually At baseline: 214 At follow‐up: 214 MCI: 91 MCI‐AD; 123 MCI‐MCI Number included in analysis: 214 (with CSF data who had a least one follow‐up assessment) TP=62; FP=41; FN=29; TN=82 (from Dr Vos's email) Loss to follow‐up: 17 (some participants refused to participate or were untraceable or died before follow‐up) |
||
| Comparative | |||
| Notes | In press. The trial investigators contacted; they provided requested data tor the 2x2 table to be completed; email from Dr Vos on 8/2/13 | ||
| Methodological quality | |||
| Item | Authors' judgement | Risk of bias | Applicability concerns |
| DOMAIN 1: Patient Selection | |||
| Was a consecutive or random sample of patients enrolled? | Unclear | ||
| Was a case‐control design avoided? | Yes | ||
| Did the study avoid inappropriate exclusions? | Yes | ||
| Unclear | Low | ||
| DOMAIN 2: Index Test All tests | |||
| Were the index test results interpreted without knowledge of the results of the reference standard? | Yes | ||
| If a threshold was used, was it pre‐specified? | Yes | ||
| Low | Low | ||
| DOMAIN 3: Reference Standard | |||
| Is the reference standards likely to correctly classify the target condition? | Yes | ||
| Were the reference standard results interpreted without knowledge of the results of the index tests? | Yes | ||
| Low | Low | ||
| DOMAIN 4: Flow and Timing | |||
| Was there an appropriate interval between index test and reference standard? | Yes | ||
| Did all patients receive the same reference standard? | Yes | ||
| Were all patients included in the analysis? | No | ||
| Low | |||
Zetterberg 2003.
| Study characteristics | |||
| Patient sampling | 53 Consecutive patients from a speciality referral university hospital memory clinic No exclusion criteria were reported The study aimed to evaluate a combination of biomarkers for identifying incipient AD in MCI patients |
||
| Patient characteristics and setting | 53 participants diagnosed by the Petersen 1999 criteria at baseline Gender: not reported Age: range = 50‐83 years APOE ϵ4 carrier: not reported MMSE: mean 27±1.7 participants fulfilling the criteria for the clinical diagnosis of MCI Setting: secondary care, outpatients ‐ memory clinic, Huddinge, Sweden |
||
| Index tests | CSF Abeta42 CSF analysis methods were not described, but other publications were cited (Hulsteart 1999; Vanmechelen 2000)) Threshold(s): 'the optimal cut‐point for Abeta42 alone was 532 ng/L, defined using the Youden index' (email from Dr Zetterberg on 6/12/10) CSF analysis methods were not described, but other publications were cited (refs 13 and 19) The optimal cut‐off for Abeta 42 was reported as < 400 pg/mL, derived from ROC analysis Index test was conducted before clinical follow‐up |
||
| Target condition and reference standard(s) | Target condition: Alzheimer's disease dementia or other forms of dementia Reference standard: DSM‐IV criteria 'Diagnoses were made independently of CSF markers' (p67) |
||
| Flow and timing |
Duration: 20±10 months At follow‐up: 53 MCI; 22 MCI‐AD; 10 MCI‐other dementias (3 VD, 2 LBD, 1 FTD, 1 normal pressure hydrocephalus,1 corticobasal degeneration, 1 PD with dementia and 1 depressive pseudodementia); 21 MCI‐MCI (p67‐68) Sensitivity 68; Specificity 61% Number included in analyses=53; Sensitivity=68; Specificity=61% (from Dr Zetterberg's email) TP=15; FP=12; FN=7; TN=19 (from Dr Zetterberg's email) Loss to follow‐up: follow‐up data were reported for all participants; biomarker data were only reported as mean and SD |
||
| Comparative | |||
| Notes | The trial investigators contacted; they provided requested data tor the 2x2 table to be completed (email from Dr Zetterberg on 2/12/10). There is no overlap between Zetterberg 2003 and Bloom 2009 studies regarding the participants (email from Dr Zetterberg on 4/10/13) | ||
| Methodological quality | |||
| Item | Authors' judgement | Risk of bias | Applicability concerns |
| DOMAIN 1: Patient Selection | |||
| Was a consecutive or random sample of patients enrolled? | Yes | ||
| Was a case‐control design avoided? | Yes | ||
| Did the study avoid inappropriate exclusions? | Unclear | ||
| Low | Low | ||
| DOMAIN 2: Index Test All tests | |||
| Were the index test results interpreted without knowledge of the results of the reference standard? | Yes | ||
| If a threshold was used, was it pre‐specified? | No | ||
| High | Low | ||
| DOMAIN 3: Reference Standard | |||
| Is the reference standards likely to correctly classify the target condition? | Yes | ||
| Were the reference standard results interpreted without knowledge of the results of the index tests? | Yes | ||
| Low | Low | ||
| DOMAIN 4: Flow and Timing | |||
| Was there an appropriate interval between index test and reference standard? | No | ||
| Did all patients receive the same reference standard? | Yes | ||
| Were all patients included in the analysis? | Yes | ||
| High | |||
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Andersson 2007 | Study design: no threshold used. The trial investigators contacted. No reply |
| Andersson 2008 | Study design: no threshold used. The trial investigators contacted. No reply |
| Andreasen 2001 | Study design: threshold based on combined biomarkers: Abeta and tau |
| Andreasen 2003 | Study design: only AD progressors used in analysis |
| Bertens 2012 | Target condition: not looking at MCI conversion to dementia (changes in Abeta42 levels measured over time) |
| Blasko 2008 | Study design: no threshold used. The trial investigators contacted. No reply |
| Bouwman 2007 | Insufficient data to complete 2x2 table. Additional data were requested from the trial investigators but no further information was available at the time this review was prepared |
| de Leon 2002 | Study design: no threshold used |
| de Leon 2006 | Insufficient data to complete 2x2 table. Additional data were requested from the trial investigators but no further information was available at the time this review was prepared |
| Ellis 2012 | Study design: no threshold used |
| Fagan 2007 | Target condition: not looking at MCI conversion to dementia |
| Forlenza 2010 | Insufficient data to complete 2x2 table. Additional data were requested from the trial investigators but no further information was available at the time this review was prepared |
| Gustafson 2007 | Population: unclear MCI diagnostic criteria used at baseline |
| Hansson 2010 | Insufficient data to complete 2x2 table. Additional data were requested from the trial investigators but no further information was available at the time this review was prepared |
| Ivanoiu 2005 | Insufficient data to complete 2x2 table. Additional data were requested from the trial investigators but no further information was available at the time this review was prepared |
| Johansson 2011 | Index test: CSF was performed at follow‐up. The trial investigators contacted |
| Li 2007 | Target condition: not looking at conversion to dementia in the MCI sample included |
| Lopez 2008 | Study design: no threshold used. The trial investigators contacted |
| Maruyama 2001 | Study design: analysis based on those who converted and distinguishing healthy controls from MCI |
| Mayeux 2003 | Target condition: not looking at conversion to dementia in the MCI sample included |
| Parnetti 2012 | Insufficient data to complete 2x2 table. Additional data were requested from the trial investigators but no further information was available at the time this review was prepared |
| Perneczky 2011 | Study design: no threshold used. The trial investigators contacted |
| Pesaresi 2006 | Population: unclear MCI diagnostic criteria used at baseline |
| Ramakers 2012 | Target condition: not looking at MCI conversion to dementia; the focus of the study is the association between abnormal CSF biomarkers' concentration and neuropsychological decline (e.g. in memory performances, excecutive functioning, etc.) |
| Riemenschneider 2002 | Index test: combined CSF Abeta42 and tau proteins |
| Seppala 2010 | Study design: no threshold used |
| Skoog 2003 | Study design: no threshold used |
| Snider 2009 | Study design: no threshold used |
| Sobow 2007 | Study design: no threshold used. The trial investigators contacted. No reply |
| Storace 2010 | Insufficient data to complete 2x2 table. Additional data were requested from the trial investigators but no further information was available at the time this review was prepared |
| Uspenskaya 2010 | Insufficient data to complete 2x2 table. Additional data were requested from the trial investigators but no further information was available at the time this review was prepared |
| Vanderstichele 2005a | Study design: no threshold used |
| Visser 2009 | Index test: looking at the tau/Abeta ratio |
| Vos 2011 | Index test: looking at the tau/Abeta ratio |
| Vos 2012 | Index test: looking at the tau/Abeta ratio |
| Vos 2012a | Index test: looking at the tau/Abeta ratio |
| Wahlund 2003 | Study design: no threshold used |
| Zetterberg 2007 | Study design: no threshold used and looking at intra‐individual variations in biomarkers over time |
Characteristics of ongoing studies [ordered by study ID]
Rainero 2012.
| Trial name or title | Predictive value of CSF biomarkers for Alzheimer's disease in cohort of patients with mild cognitive impairment |
| Target condition and reference standard(s) | Alzheimer's disease dementia |
| Index and comparator tests | CSF Aß 42 |
| Starting date | Not stated in the conference abstract |
| Contact information | irainero@molinette.piemonte.it |
| Notes | An update at the 2013 AAN meeting in San Diego" (email from Prof Rainero on 5/1/13) |
Differences between protocol and review
In the protocol we stated that we will consider MCI participants who have been diagnosed using any of the 16 definitions of MCI (Matthews 2008). In our review we also included participants whose clinical diagnosis of MCI was based on the CDR = 0.5 criteria.
Contributions of authors
CR: designed and drafted protocol; overall responsibility of study selection and data extraction; advised about data and analyses; finalised manuscript
LF: contributed to design, study selection and data extraction
RMS: conception, funding, design, and reviewing draft protocol
ANS: searches; study selection and data extraction; contacted study authors; characteristics of excluded studies; data entry check; set up data and analysis tables
YT: statistical analyses and reviewed the draft manuscript
NS: study selection and data extraction; characteristics of included and excluded studies tables; entered data and data entry check; QUADAS‐2 assessment; set up data and analysis tables; drafted manuscript; managed the review process and produced progress reports, attended progress meetings and worked with all review authors to ensure that the review met publication deadlines.
Declarations of interest
None
New
References
References to studies included in this review
Bjerke 2009 {published data only}
- Bjerke M, Andreasson U, Rolstad S, Nordlund A, Lind K, Zetterberg H, et al. Subcortical vascular dementia biomarker pattern in mild cognitive impairment. Dementia and Geriatric Cognitive Disorders 2009;28(4):348‐56. [DOI] [PubMed] [Google Scholar]
- Hanson O, Zetteberg H, Vanmechelen E, Vanderstichele H, Andreason U, Londos E, et al. Evaluation of plasma Aß40 and Aß42 as predictors of conversion to Alzheimer's disease in patients with mild cognitive impairment. Neurobiology of Aging 2010;31:357‐67. [DOI] [PubMed] [Google Scholar]
- Mattsson N, Portelius E, Rolstad S, Gustavsson M, Andreasson U, Stridsberg M, et al. Longitudinal cerebrospinal fluid biomarkers over four years in mild cognitive impairment. Journal of Alzheimer's Disease 2012;30(4):767‐78. [DOI] [PubMed] [Google Scholar]
- Mattsson N, Zetterberg H, Hansson O, Andreasen N, Parnetti L, Jonsson M, et al. CSF biomarkers and incipient Alzheimer disease in patients with mild cognitive impairment. JAMA 2009;302(4):385‐93. [DOI] [PubMed] [Google Scholar]
- Nordlund A, Rolstad S, Hellstrom P, Sjogren M, Hansen S, Wallin A. The Goteborg MCI study: mild cognitive impairment is a heterogeneous condition. Journal of Neurology, Neurosurgery, and Psychiatry 2005;76:1485‐90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nordlund A, Rolstad S, Klang S, Edman A, Hansen S, Wallin A. Two‐year outcome of MCI subtypes and aetiologies in the Goteborg MCI study. Journal of Neurology, Neurosurgery, and Psychiatry 2010;81:541‐6. [DOI] [PubMed] [Google Scholar]
- Rolstad S, Nordlund A, Eckerstrom C, Gustavsson MH, Zetterberg H, Wallin A. Cognitive reserve in relation to abeta42 in patients converting from MCI to dementia ‐ a follow‐up report. Dementia and Geriatric Cognitive Disorders 2009;28(2):110‐5. [DOI] [PubMed] [Google Scholar]
- Rolstad S, Nordlund A, Eckerstrom C, Gustavsson MH, Zetterberg H, Wallin A. Biomarkers in relation to cognitive reserve in patients with mild cognitive impairment ‐ proof of concept. Dementia and Geriatric Cognitive Disorders 2009;27:194‐200. [DOI] [PubMed] [Google Scholar]
- Wallin A, Gothlin M, Gustavsson M, Zetterberg H, Eckerstrom C, Blennow K, et al. Progression from mild to pronounced MCI is not associated with cerebrospinal fluid biomarker deviations. Dementia and Geriatric Cognitive Disorders 2011;32(3):193‐7. [DOI] [PubMed] [Google Scholar]
Blom 2009 {published data only}
- Blom ES, Giedraitis V, Zetterberg H, Fukumoto H, Blennow K, Hyman BT, et al. Rapid progression from mild cognitive impairment to Alzheimer's disease in subjects with elevated levels of tau in cerebrospinal fluid and the APOE ϵ4/ϵ4 genotype. Dementia and Geriatric Cognitive Disorders 2009;27(5):458‐64. [DOI] [PMC free article] [PubMed] [Google Scholar]
Brys 2009 {published data only}
- Brys M, Pirraglia E, Rich K, Rolstad S, Mosconi L, Switalski R, et al. Prediction and longitudinal study of CSF biomarkers in mild cognitive impairment. Neurobiology of Aging 2009; Vol. 30, issue 5:682‐90. [DOI] [PMC free article] [PubMed]
Chiasserini 2010 {published data only}
- Chiasserini D, Parnetti L, Andreasson U, Zetterberg H, Giannandrea D, Calabresi P, Blennow K. CSF levels of heart fatty acid binding protein are altered during early phases of Alzheimer's disease. Journal of Alzheimer's Disease 2010;22:1281‐8. [DOI] [PubMed] [Google Scholar]
Fei 2011 {published data only}
- Fei M, Jianghua W, Rujuan M, Wei Z, Quian W. The relationship of plasma Aß levels to dementia in aging individuals with mild cognitive impairment. Journal of the Neurological Sciences 2011;305:92‐6. [DOI] [PubMed] [Google Scholar]
Galluzzi 2010 {published data only}
- Galluzzi S, Geroldi C, Amicucci G, Chiavetto LB, Bonetti M, Bonvicini C, et al. Supporting evidence of the Alzheimer's disease biomarker dynamic model in patients with mild cognitive impairment. Conference Publication: Alzheimer's Association International Conference 2012 Vancouver, BC Canada. Conference Start: 20120714 Conference End: 20120719. Conference Publication:(var.pagings). 2012. [Google Scholar]
- Galluzzi S, Geroldi C, Ghidoni R, Paghera B, Amicucci G, Bonetti M, et al. The new Alzheimer's criteria in a naturalistic series of patients with mild cognitive impairment. Journal of Neurology 2010;257:2004‐14. [DOI] [PubMed] [Google Scholar]
- Prestia A, Caroli A, Herholz K, Reiman E, Jagust W, Chen K, et al. Accuracy of different biomarkers to predict progression from mild cognitive impairment to probable Alzheimer's dementia in two independent clinical series. Accuracy of different biomarkers to predict progression from mild cognitive impairment to probable Alzheimer's dementia in two independent clinical series. Conference Publication: Alzheimer's Association International Conference 2012 Vancouver, BC Canada. Conference Start: 20120714 Conference End: 20120719. Conference Publication:(var.pagings) 2012. [Google Scholar]
Hampel 2004 {published data only}
- Hampel H, Teipel SJ, Fuchsberger T, Andreasen N, Wiltfang J, Otto M, at al. Value of CSF ß‐amyloid1‐42 and tau as predictors of Alzheimer's disease in patients with mild cognitive impairment. Molecular Psychiatry 2004;9:705‐10. [DOI] [PubMed] [Google Scholar]
Hansson 2007 {published data only}
- Buchhave P, Minthon L, Zetterberg H, Wallin AK, Blennow K, Hansson O. Cerebrospinal fluid levels of beta‐amyloid 1‐42, but not of tau, are fully changed already 5 to 10 years before the onset of Alzheimer dementia. Archives of General Psychiatry 2012;69(1):98‐106. [DOI] [PubMed] [Google Scholar]
- Buchhave P, Stomrud E, Warkentin S, Blennow K, Minthon L, Hansson O. Cube copying test in combination with rCBF or CSF A beta 42 predicts development of Alzheimer's disease. Dementia and Geriatric Cognitive Disorders 2008;25(6):544‐52. [DOI] [PubMed] [Google Scholar]
- Hansson O, Zetteberg H, Buchhave P, Londos E, Blennow K, Minthon L. Association between CSF biomarkers and incipientt Alzheimer's disease in patients with mild cognitive impairment: a follow‐up. Lancet Neurol 2006;5:228‐34. [DOI] [PubMed] [Google Scholar]
- Hansson O, Zetteberg H, Vanmechelen E, Vanderstichele H, Andreason U, Londos E, et al. Evaluation of plasma Aß40 and Aß42 as predictors of conversion to Alzheimer's disease in patients with mild cognitive impairment. Neurobiology of Aging 2010;31:357‐67. [DOI] [PubMed] [Google Scholar]
- Hansson O, Zetterberg H, Buchhave P, Andreasson U, Londos E, Minthon L, et al. Prediction of Alzheimer's disease using the CSF Aß42/Aß40 ratio in patients with mild cognitive impairment. Dementia and Geriatric Cognitive Disorders 2007;23(5):316‐20. [DOI] [PubMed] [Google Scholar]
- Mattsson N, Rosen E, Hansson O, Andreasen N, Parnetti L, Jonsson M, et al. Age and diagnostic performance of Alzheimer disease CSF biomarkers. Neurology 2012;78(7):468‐76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mattsson N, Zetterberg H, Hansson O, Andreasen N, Parnetti L, Jonsson M, et al. CSF biomarkers and incipient Alzheimer disease in patients with mild cognitive impairment. JAMA 2009;302(4):385‐93. [DOI] [PubMed] [Google Scholar]
Hertze 2010 {published data only}
- Hertze J, Minthon L, Zetterberg H, Vanmechelen E, Blennow K, Hansson O. Evaluation of CSF biomarkers as predictors of Alzheimer's disease: a clinical follow‐up study of 4.7 years. Journal of Alzheimer's Disease 2010; Vol. 21, issue 4:1119‐28. [DOI] [PubMed]
- Palmqvist S, Hertze J, Minthon L, Wattmo C, Blennow K, Zetterberg H, et al. Comparison of brief cognitive tests and csf analysis in predicting Alzheimer's disease in mild cognitive impairment: Six‐year follow‐up study. Alzheimer's and Dementia 2012. Conference Publication: Alzheimer's Association International Conference 2012 Vancouver, BC Canada. Conference Start: 20120714 Conference End: 20120719. Conference Publication:(var.pagings). 2012. [Google Scholar]
Herukka 2007 {published data only}
- Herukka SK, Hallikainen M, et al. CSF Abeta42 and tau or phosphorylated tau and prediction of progressive mild cognitive impairment. Neurology 2005;64:1294‐7. [DOI] [PubMed] [Google Scholar]
- Herukka SK, Helisalmi S, Hallikainen M, Tervo S, Soinien H, Pirtilla T. CSF Aß42, tau and phosphorylated tau, APOE ϵ4 allele and MCI type in progressive MCI. Neurobiology of Aging 2007;28:507‐14. [DOI] [PubMed] [Google Scholar]
- Herukka SK, Pennanen C, Soininen H, Pirttila T. CSF Aß42, tau and phosphorylated tau correlate with medial temporal lobe. Journal of Alzheimer's Disease 2008;14:51‐7. [DOI] [PubMed] [Google Scholar]
- Seppala TT, Koivisto AM, Hartikainen P, Helisalmi S, Soininen H, Herukka S‐K. Longitudinal changes of CSF biomarkers in Alzheimer's disease. Journal of Alzheimer's Disease 2011;25(4):583‐94. [DOI] [PubMed] [Google Scholar]
Kester 2011 {published data only}
- Kester MI, Verwey NA, Elk EJ, Blankenstein MA, Scheltens P, Flier WM. Progression from MCI to AD: Predictive value of CSF Aß42 is modified by APOE genotype. Neurobiology of Aging 2011;32(8):1372‐8. [DOI] [PubMed] [Google Scholar]
- Rossum IA, Visser PJ, Knol DL, Flier WM, Teunissen CE, Barkhof F, et al. Injury markers but not amyloid markers are associated with rapid progression from mild cognitive impairment to dementia in Alzheimer's disease. Journal of Alzhemer's Disease 2012;29(2):319‐27. [DOI] [PubMed] [Google Scholar]
Monge‐Argiles 2011 {published data only}
- Monge‐Argiles JA, Munoz‐Ruiz C, Pampliega‐Perez A, Gomez‐Lopez MJ, Sanchez‐Paya J, Rodriguez‐Borja E, et al. Biomarkers of Alzheimer's disease in the cerebrospinal fluid of Spanish patients with mild cognitive impairment. Neurochemical Research 2011;36:986‐93. [DOI] [PubMed] [Google Scholar]
- Monge‐Argiles JA, Munoz‐Ruiz C, Sanchez‐Paya J, Marti‐Martinez S, Blanco‐Canto M, Leiva‐Santana C. Rapid progression from mild cognitive impairment to Alzheimer's disease related with CSF biomarker abnormalities. European Journal of Neurology 2012;19 Suppl 1(Special Issue SI):463. [Google Scholar]
Papaliagkas 2009 {published data only}
- Papaliagkas VT, Anogianakis G, Tsolaki MN, Koliakos G, Kimiskidis VK. Progression of mild cognitive impairment to Alzheimer's disease: improved diagnostic value of the combined use of N200 latency and ß‐amyloid(1‐42) levels. Dementia and Geriatric Cognitive Disorders 2009;28:30‐5. [DOI] [PubMed] [Google Scholar]
- Papalliagkas VT, Anogianakis G, Tsolaki MN, Kimiskidis VK. Combination of P300 and CSF Aßamyloid1‐42 assays may provide a potential tool in the early diagnosis of Alzheimer's disease. Current Alzheimer Research 2010;7:295‐9. [DOI] [PubMed] [Google Scholar]
Parnetti 2006 {published data only}
- Parnetti L, Lanari A, Silvestrelli G, Saggese E, Reboldi P. Diagnosing prodromal Alzheimer's disease: Role of CSF biochemical markers. Mechanisms of Ageing and Development 2006;127:129‐32. [DOI] [PubMed] [Google Scholar]
Shaw 2009 {published data only}
- Chou YY, Lepore N, Avedissian C, Madsen SK, Parikshak N, Hua X, et al. Mapping correlations between ventricular expansion and CSF amyloid and tau biomarkers in 240 subjects with Alzheimer's disease, mild cognitive impairment and elderly controls. Neuroimage 2009;46(2):394‐410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davatzikos C, Bhatt P, Shaw LM, Batmanghelich KN, Trojanowski JQ. Prediction of MCI to AD conversion, via MRI, CSF biomarkers, and pattern classification. Neurobiology of Aging 2011;32(12):2322.e19‐27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meyer G, Shapiro F, Vanderstichele H, Vanmechelen E, Engelborghs S, Deyn P, et al. Diagnosis‐independent Alzheimer disease biomarker signature in cognitively normal elderly people. Archives of Neurology 2010;67(8):949‐56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ewers M, Walsh C, Trojanowski JQ, Shaw LM, Petersen RC, Jack CR, et al. Prediction of conversion from mild cognitive impairment to Alzheimer's disease dementia based upon biomarkers and neuropsychological test performance. Neurobiology of Aging 2012;33(7):1203‐14.e2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heister D, Brewer JB, Magda S, Blennow K, McEvoy LK. Predicting MCI outcome with clinically available MRI and CSF biomarkers. Neurology 2011;77(17):1619‐28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jack CR, Wiste HJ, Vemuri P, Weigand SD, Senjem ML, Zeng G, et al. Brain beta‐amyloid measures and magnetic resonance imaging atrophy both predict time‐to‐progression from mild cognitive impairment to Alzheimer's disease. Brain 2010;133:3336‐48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lo RY, Hubbard AE, Shaw LM, Trojanowski J, Petersen RC, Aisen PS, et al. Longitudinal change of biomarkers in cognitive decline. Archives of Neurology 2011;68(10):1257‐66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Novak G, Einstein S, Guthrie S, Margolin R, Yu HJ, Bracoud L, et al. Discordance for hippocampal atrophy and amyloid burden in amnestic mild cognitive impairment may identify distinct subgroups of patients. Alzheimer's Association International Conference 2012 Vancouver, BC Canada. Conference Start: 20120714 Conference End: 20120719. Conference Publication:(var.pagings) 2012. [Google Scholar]
- Okonkwo OC, Mielke MM, Griffith HR, Moghekar AR, O'Brien RJ, Shaw LM, et al. Cerebrospinal fluid profiles and prospective course and outcome in patients with amnestic mild cognitive impairment. Archives of Neurology 2011;68(1):113‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schmand B, Eikelenboom P, Gool WA. Value of diagnostic tests to predict conversion to Alzheimer's disease in young and old patients with amnestic mild cognitive impairment. Journal of Alzheimer's Disease 2012 2012;29(3):641‐8. [DOI] [PubMed] [Google Scholar]
- Shaw LM, Vanderstichele H, Knapik‐Czajka M, Clark CM, Aisen PS, Petersen RC, et al. Cerebrospinal fluid biomarker signature in Alzheimer's disease neuroimaging initiative subjects. Annals of Neurology 2009;65:403‐13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vemuri P, Wiste HJ, Weigand SD, Knopman DS, Trojanowski MD, Shaw LM, at al. Serial MRI and CSF biomarkers in normal aging, MCI and AD. Neurology 2010;75:143‐51. [DOI] [PMC free article] [PubMed] [Google Scholar]
Vos 2013 {published data only}
- Vos SJB, Rossum IA, Verhey F, Knol DL, Soinien H, Wahlund LO, et al. Prediction of Alzheimer's disease in subjects with amnestic and non‐amnestic MCI. Neurology 2013;In press:1‐28. [DOI] [PubMed] [Google Scholar]
Zetterberg 2003 {published data only}
- Zetterberg H, Wahlund LO, Blennow K. Cerebrospinal fluid markers for prediction of Alzheimer's disease. Neuroscience Letters 2003;352:67‐9. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Andersson 2007 {published data only}
- Andersson C, Blennow K, Johansson SE, Almkvist O, Engfeldt P, Lindau M, et al. Differential CSF biomarker levels in APOE‐4‐positive and‐negative patients memory impairment. Dementia and Geriatric Cognitive Disorders 2007;23:87‐95. [DOI] [PubMed] [Google Scholar]
Andersson 2008 {published data only}
Andreasen 2001 {published data only}
- Andreasen N, Gottfries J, Vanmechelen E, Vanderstichele H, Davidson P, Blennow K, et al. Evaluation of CSF biomarkers for axonal and neuronal degeneration, gliosis, and beta‐amyloid metabolism in Alzheimer's disease. Journal of Neurology, Neurosurgery, and Psychiatry 2001; Vol. 71, issue 4:557‐8. [DOI] [PMC free article] [PubMed]
Andreasen 2003 {published data only}
- Andreasen N, Vanmechelen E, Vanderstichele H, Davidsson P, Blennow K. Cerebrospinal fluid levels of total‐tau, phospho‐tau and A beta 42 predicts development of Alzheimer's disease in patients with mild cognitive impairment. Acta Neurologica Scandinavica. Supplementum 2003; Vol. 179:47‐51. [DOI] [PubMed]
Bertens 2012 {published data only}
- Bertens D, Scheltens P, Visser PJ. Use of biomarkers as endpoint in trials with subjects with preclinical and prodromal Alzheimer's disease: an ADNI study. Alzheimer's and Dementia 2012; Vol. Conference: Alzheimer's Association International Conference 2012 Vancouver, BC Canada. Conference Start: 20120714 Conference End: 20120719. Conference Publication:, issue var.pagings.
Blasko 2008 {published data only}
- Blasko I, Jellinger K, Kemmler G, Krampla W, Jungwirth S, Wichart I, et al. Conversion from cognitive health to mild cognitive impairment and Alzheimer's disease: prediction by plasma amyloid beta 42, medial temporal lobe atrophy and homocysteine. Neurobiology of Aging 2008; Vol. 29, issue 1:1‐11. [DOI] [PubMed]
Bouwman 2007 {published data only}
de Leon 2002 {published data only}
de Leon 2006 {published data only}
Ellis 2012 {published data only}
- Ellis K, Maruff P, Martins R, Masters C, McBride S, Macaulay L, et al. Rates of conversion to MCI and Alzheimer's in the australian imaging biomarkers and lifestyle (AIBL) cohort over 36 months. Alzheimer's and Dementia 2012; Vol. Conference: Alzheimer's Association International Conference 2012 Vancouver, BC Canada. Conference Start: 20120714 Conference End: 20120719. Conference Publication:, issue var.pagings.
Fagan 2007 {published data only}
Forlenza 2010 {published data only}
- Diniz BS, Nunes PV, Yassuda MS, Periera FS, Flaks MK, Viola LF, et al. Mild cognitive impairment: cognitive screening or neuropsychological assessment?. Revista Brasileira de Psiquiatria 2008;30(4):316‐21. [DOI] [PubMed] [Google Scholar]
- Forlenza OV, Diniz BS, Talib LL, Radanovic M, Yassuda MS, Ojopi EB, et al. Clinical and biological predictors of Alzheimer's disease in patients with amnestic mild cognitive impairment. Revista Brasileira de Pisquiatria 2010;32(3):216‐22. [DOI] [PubMed] [Google Scholar]
Gustafson 2007 {published data only}
- Gustafson DR, Skoog I, Rosengren L, Zetterberg H, Blennow K. Cerebrospinal fluid beta‐amyloid 1‐42 concentration may predict cognitive decline in older women. Journal of Neurology, Neurosurgery, and Psychiatry 2007; Vol. 78, issue 5:461‐4. [DOI] [PMC free article] [PubMed]
Hansson 2010 {published data only}
- Hansson O, Zetteberg H, Vanmechelen E, Vanderstichele H, Andreason U, Londos E, et al. Evaluation of plasma Aß40 and Aß42 as predictors of conversion to Alzheimer's disease in patients with mild cognitive impairment. Neurobiology of Aging 2010;31:357‐67. [DOI] [PubMed] [Google Scholar]
- Nordlund A, Rolstad S, Klang S, Edman A, Hansen S, Wallin A. Two‐year outcome of MCI subtypes and aetiologies in the Goteborg MCI study. Journal of Neurology, Neurosurgery, and Psychiatry 2010;81:541‐6. [DOI] [PubMed] [Google Scholar]
Ivanoiu 2005 {published data only}
Johansson 2011 {published data only}
- Johansson P, Mattson N, Hansson O, Wallin A, Johansson JO, Andreasson U. Cerebrospinal fluid biomarkers for alzheimer's disease: diagnostic performance in a homogenous mono‐center population. Journal of Alzheimer's Disease 2011;24:537‐46. [DOI] [PubMed] [Google Scholar]
Li 2007 {published data only}
Lopez 2008 {published data only}
- Lopez OL, Kuller LH, Mehta PD, Becker JT, Gach HM, Sweet RA, et al. Plasma amyloid levels and the risk of AD in normal subjects in the Cardiovascular Health Study. Neurology 2008;70(19):1664–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
Maruyama 2001 {published data only}
Mayeux 2003 {published data only}
Parnetti 2012 {published data only}
- Parnetti L, Chiasserini D, Eusebi P, Giannandrea D, Bellomo G, Carlo C, et al. Performance of Abeta1‐40, Abeta1‐42, total tau, and phosphorylated tau as predictors of dementia in a cohort of patients with mild cognitive impairment. Journal of Alzheimer's Disease 2012; Vol. 29, issue 1:229‐38. [DOI] [PubMed]
Perneczky 2011 {published data only}
- Perneczky R, Tsolakidou A, Arnold A, Diehl‐Schmid J, Grimmer T, Förstl H, Kurz A, Alexopoulos P. CSF soluble amyloid precursor proteins in the diagnosis of incipient Alzheimer disease. Neurology 2011;77:35‐38. [DOI] [PubMed] [Google Scholar]
Pesaresi 2006 {published data only}
Ramakers 2012 {published data only}
- Ramakers I, Verhey FRJ, Vos S, Koehler S, Praag L, Scheltens P, et al. Cerebrospinal fluid biomarkers for Alzheimer's disease and specific cognitive decline in subjects with mild cognitive impairment. Alzheimer's and Dementia 2012; Vol. Conference: Alzheimer's Association International Conference 2012 Vancouver, BC Canada. Conference Start: 20120714 Conference End: 20120719. Conference Publication:, issue var.pagings.
Riemenschneider 2002 {published data only}
- Riemenschneider M, Lautenschlager N, Wagenpfeil S, Diehl J, Drzezga A, Kurz A. Cerebrospinal fluid tau and beta‐amyloid 42 proteins identify Alzheimer's disease in subjects with mild cognitive impairment. Archives of Neurology 2002;59:1729‐34. [DOI] [PubMed] [Google Scholar]
Seppala 2010 {published data only}
- Seppala T, Herukka S‐K, Hanninen T, Tervo S, Hallikainen M, Soininen H, Pirttila T. Plasma Aß42 and Aß40 as markers of cognitive change in follow‐up: a prospective, longitudinal, population‐based cohort study. Journal of Neurology, Neurosurgery, and Psychiatry 2010;81:1123‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Skoog 2003 {published data only}
Snider 2009 {published data only}
- Snider BJ, Fagan AM, Roe C, Shah AR, Grant EA, Xiong C, et al. Cerebrospinal fluid biomarkers and rate of cognitive decline in very mild dementia of the Alzheimer type. Archives of Neurology 2009; Vol. 66, issue 5:638‐45. [DOI] [PMC free article] [PubMed]
Sobow 2007 {published data only}
- Sobow T, Kloszewska I. Predictors of amnesic mild cognitive impairment to dementia progression: a two‐year prospective study [Czynniki prognostyczne progresji amnestycznych lagodnych zaburzen poznawczych w dwuletnieji obserwacji podluznej]. Postepy Psychiatrii i Neurologii 2007;16(2):133‐8. [Google Scholar]
Storace 2010 {published data only}
- Cammarata S, Borghi R, Giliberto L, Pardini M, Pollero V, Novello C, et al. Amyloid‐ß42 plasma levels are elevated in amnestic mild cognitive impairment. Journal of Alzheimer's Disease 2009;18:267‐71. [DOI] [PubMed] [Google Scholar]
- Storace D, Cammarata S, Borghi R, Sanguineti R, Giliberto L, Piccini A, at al. Elevation of ß‐amyloid1‐42 autoantibodies in the blood of amnestic patients with mild cognitive impairments. Archives of Neurology 2010;67(7):867‐72. [DOI] [PubMed] [Google Scholar]
Uspenskaya 2010 {published data only}
- Uspenskaya. Neurochemical markers of neurodegeneration in the early diagnosis of Alzheimer’s disease, vascular and mixed dementia. 2010. [PubMed]
Vanderstichele 2005a {published data only}
Visser 2009 {published data only}
- Visser PJ, Verhey F, Knol DL, Scheltens P, Wahlund LO, Freund‐Levi Y, et al. Prevalence and prognostic value of CSF markers of Alzheimer's disease pathology in patients with subjective cognitive impairment or mild cognitive impairment in the DESCRIPA study: a prospective cohort study. Lancet Neurology 2009; Vol. 8, issue 7:619‐27. [DOI] [PubMed]
Vos 2011 {published data only}
- Vos SJB, Visser PJ, Verhey FRJ. The role of CSF markers in the early diagnosis of Alzheimer's disease [De rol van liquormarkers bij de vroege diagnostiek van de ziekte van Alzheimer]. Tijdschrift voor Psychiatrie 2011;53(9):647‐653. [PubMed] [Google Scholar]
Vos 2012 {published data only}
- Vos S, Rossum I, Verhey F, Soininen H, Wahlund L‐O, Hampel H, et al. Cerebrospinal fluid markers for predicting Alzheimer's‐type dementia in subjects with amnestic versus nonamnestic mild cognitive impairment. Alzheimer's and Dementia 2012; Vol. Conference: Alzheimer's Association International Conference 2012 Vancouver, BC Canada. Conference Start: 20120714 Conference End: 20120719. Conference Publication:, issue var.pagings.
Vos 2012a {published data only}
Wahlund 2003 {published data only}
Zetterberg 2007 {published data only}
References to ongoing studies
Rainero 2012 {published and unpublished data}
- Rainero I, Vacca A, Rubino E, Martino P, Govone F, Giobbe L, Pinessi L. Predicitve value of CSF biomarkers for Alzheimer's disease in a cohort of patients with mild cognitive impairment. Conference abstracts. Proceedings 2012;VII Congresso Sindem, Italian Association for the study of dementia linked to the Italian Neuropsychological Society (SIN). [Google Scholar]
Additional references
Aizenstein 2008
- Aizenstein HJ, Nebes RD, Saxton JA, Price JC, Mathis CA, Tsopelas ND, et al. Frequent amyloid deposition without significant cognitive Impairment among the elderly. Archives of Neurology 2008;65(11):1509‐17. [DOI] [PMC free article] [PubMed] [Google Scholar]
Albert 2011
- Albert MS, DeKosky ST, Dickson D, Dubois B, Feldman HH, Fox NC, et al. The diagnosis of mild cognitive impairment due to Alzheimer's disease: recommendations from the National Institute on Aging‐Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimer’s & Dementia 2011;7(3):270‐9. [10.1016/j.jalz.2011.03.008]. [DOI] [PMC free article] [PubMed] [Google Scholar]
Blacker 1994
- Blacker D, Albert MS, Bassett SS, Go RC, Harrell LE, Folstein MF. Reliability and validity of NINCDS‐ADRDA criteria for Alzheimer's disease. The National Institute of Mental Health Genetics Initiative. Archives of Neurology 1994;51(12):1198‐204. [DOI] [PubMed] [Google Scholar]
Bourne 2007
- Bourne J. Improving services and support for people with dementia. National Audit Office 2007. [Google Scholar]
Bruscoli 2004
- Bruscoli M, Lovestone S. Is MCI really just early dementia? A systematic review of conversion studies. International Psychogeriatrics 2004;16:129‐40. [DOI] [PubMed] [Google Scholar]
Castellani 2004
- Castellani RJ, Honda K, Zhu X, Cash AD, Nunomura A, Perry G, et al. Contribution of redox‐active iron and copper to oxidative damage in Alzheimer disease. Ageing Research Reviews 2004;3:319‐26. [DOI] [PubMed] [Google Scholar]
Davis 2013
- Davis DHJ, Creavin ST, Noel‐Storr A, Quinn TJ, Smailagic N, Hyde C, et al. Neuropsychological tests for the diagnosis of Alzheimer’s disease dementia and other dementias: a generic protocol for cross‐sectional and delayed‐verification studies. Cochrane Database of Systematic Reviews 2013, Issue 3:Art. No.: CD010460 DOI: 10.1002/14651858.CD010460. [DOI] [PMC free article] [PubMed] [Google Scholar]
DSMIII 1987
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 3rd revised edition. Washington. DC: American Psychiatric Association 1987. [Google Scholar]
DSMIV 1994
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th edition. Washington. DC: American Psychiatric Association 1994. [Google Scholar]
Dubois 2010
- Dubois B, Feldman HH, Jacova C, Cummings JL, Dekosky ST, Barberger‐Gateau P, et al. Revising the definition of Alzheimer's disease: a new lexicon. Lancet Neurology 2010;9(11):118‐27. [DOI] [PubMed] [Google Scholar]
Ferri 2005
- Ferri CP, Prince M, Brayne C, Brodaty H, Fratiglioni L, Ganguli M, et al. Global prevalence of dementia: a Delphi consensus study. Lancet 2005;366:2112‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Filley 2007
- Filley CM, Rollins YD, Anderson CA, Arciniegas DB, Howard KL, Murrell JR, et al. The genetics of very early onset Alzheimer disease. Cognitive and Behavioural Neurology 2007;20(3):149‐56. [DOI] [PubMed] [Google Scholar]
Geslani 2005
- Geslani DM, Tierney MC, Herrmann N, Szalai JP. Mild cognitive impairment: an operational definition and its conversion rate to Alzheimer's disease. Dementia and Geriatric Cognitive Disorders 2005;19(5‐6):383‐9. [DOI] [PubMed] [Google Scholar]
Hardy 1992
- Hardy JA, Higgins GA. Alzheimer's disease: the amyloid cascade hypothesis. Science 1992;256(5054):184‐5. [DOI] [PubMed] [Google Scholar]
Holmes 2008
- Holmes C, Boche D, Wilkinson D, Yadegarfar G, Hopkins V, Bayer A, et al. Long‐term effects of Aß42 immunisation in Alzheimer’s disease: follow‐up of a randomised, placebo‐controlled phase I trial. Lancet 2008;372:216‐23. [DOI] [PubMed] [Google Scholar]
Kokkinou 2014
- Kokkinou M, Smailagic N, Noel‐Storr AH, Hyde C, Ukoumunne O, Worrall RE, et al. Plasma and Cerebrospinal fluid (CSF) Abeta42 for the differential diagnosis of Alzheimer's disease dementia in participants diagnosed with any dementia subtype in a specialist care setting. Cochrane Database of Systematic Reviews 2014;1:CD010945. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lund 1994
- The Lund and Manchester Groups. Clinical and neuropathological criteria for frontotemporal dementia [Consensus statement]. Journal of Neurology, Neurosurgery, and Psychiatry 1994;57(4):416‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Matthews 2008
- Matthews FE, Stephan BC, McKeith IG, Bond J, Brayne C, Medical Research Council Cognitive Function and Ageing Study. Two‐year progression from mild cognitive impairment to dementia: to what extent do different definitions agree?. Journal of the American Geriatrics Society 2008;56(8):1424‐33. [DOI] [PubMed] [Google Scholar]
Mattsson 2009
- Mattsson N, Zetterberg H, Hansson O, Andreasen N, Parnetti L, Jonsson M, et al. CSF biomarkers and incipient Alzheimer disease in patients with mild cognitive impairment. JAMA 2009;302(4):385‐93. [DOI] [PubMed] [Google Scholar]
McKeith 1996
- McKeith IG, Galasko D, Kosaka K, Perry EK, Dickson DW, Hansen LA, et al. Consensus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the consortium on DLB international workshop. Neurology 1996;47(5):1113‐24. [DOI] [PubMed] [Google Scholar]
McKhann 1984
- McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM. Clinical diagnosis of Alzheimer's disease: report of the NINCDS‐ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer's Disease. Neurology 1984;34(7):939‐44. [DOI] [PubMed] [Google Scholar]
Mehta 2001
- Mehta PD, Pirttila T, Patrick BA, Barshatzky M, Mehta SP. Amyloid b protein 1‐40 and 1‐42 levels in matched cerebrospinal fluid and plasma from patients with Alzheimer disease. Neuroscience Letters 2001;304:102‐6. [DOI] [PubMed] [Google Scholar]
Mitchell 2009
- Mitchell AJ, Shiri‐Feshki M. Rate of progression of mild cognitive impairment to dementia ‐ meta‐analysis of 41 robust inception cohort studies. Acta Psychiatrica Scandinavica 2009;119:252‐65. [DOI] [PubMed] [Google Scholar]
Nagy 1998
- Nagy Z, Esiri MM, Hindley NJ, Joachim C, Morris JH, King EM, et al. Accuracy of clinical operational diagnostic criteria for Alzheimer's disease in relation to different pathological diagnostic protocols. Dementia and Geriatric Cognitive Disorders 1998;9(4):219‐26. [DOI] [PubMed] [Google Scholar]
Noel‐Storr 2013
- Noel‐Storr AH, Flicker L, Ritchie CW, et al. Systematic review of the body of evidence for use of biomarkers in the diagnosis of dementia. Alzheimer’s & Dementia 2013;9(3):e96‐e105. [DOI] [PubMed] [Google Scholar]
Petersen 1999
- Petersen RC, Smith GE, Waring SC, Ivnik RJ, Tangalos EG, Kokmen E. Mild cognitive impairment: clinical characterization and outcome. Archives of Neurology 1999;56:303‐8. [DOI] [PubMed] [Google Scholar]
Petersen 2004
- Petersen RC. Mild cognitive impairment as a diagnostic entity. Journal of Internal Medicine 2004 2004;256:183‐94. [DOI] [PubMed] [Google Scholar]
Petersen 2006
- Petersen RC, Parisi JE, Dickson DW, Johnson KA, Knopman DS, Boeve BF, et al. Neuropathologic features of amnestic mild cognitive impairment. Archives of Neurology 2006;63(5):665‐72. [DOI] [PubMed] [Google Scholar]
Quinn 2012
- Quinn TJ, McShane R, Fearon P, Young C, Noel‐Storr A, Stott DJ. IQCODE for the diagnosis of Alzheimer's disease dementia and other dementias within a community setting. Cochrane Database of Systematic Reviews 2012, Issue 9. Art. No.: CD010079 DOI: 10.1002/14651858.CD010079 2012. [Google Scholar]
Roman 1993
- Roman GC, Tatemichi TK, Erkinjuntti T, Cummings JL, Masdeu JC, Garcia JH, et al. Vascular dementia: diagnostic criteria for research studies. Report of the NINDS‐AIREN International Workshop. Neurology 1993;43(2):250‐60. [DOI] [PubMed] [Google Scholar]
Shankar 2008
- Shankar GM, Li S, Mehta TH, Garcia‐Munoz A, Shepardson NE, Smith I, et al. Amyloid‐b protein dimers isolated directly from Alzheimer’s brains impair synaptic plasticity and memory. Nature Medicine 2008;14:6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Visser 2006
- Visser PJ, Kester, Jolles J, Verhey F. Ten‐year risk of dementia in subjects with mild cognitive impairment. Neurology 2006;67(7):1201‐7. [DOI] [PubMed] [Google Scholar]
Whiting 2011
- Whiting PF, Rutjes AWS, Westwood ME, Mallet S, Deeks JJ, Reitsma JB. QUADAS‐2: a revised tool for the quality assessment of diagnostic accuracy studies. Annals of Internal Medicine 2011;155:529‐36. [DOI] [PubMed] [Google Scholar]
World Health Organization 2010
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems (ICD‐10 Version: 2010). http://apps.who.int/classifications/icd10/browse/2010/en (accessed 9 January 2013). [Google Scholar]