

Abstract
Background
Inguinal hernia repair is the most frequent operation in general surgery. There are several techniques: the Shouldice technique is sometimes considered the best method but different techniques are used as the "gold standard" for open hernia repair. Outcome measures, such as recurrence rates, complications and length of post operative stay, vary considerably among the various techniques.
Objectives
To evaluate the efficacy and safety of the Shouldice technique compared to other non‐laparoscopic techniques for hernia repair.
Search methods
We searched MEDLINE, EMBASE, and The Cochrane Central Register of Controlled Trials (CENTRAL), April 2008 and updated the searches September 2011, for relevant randomised controlled trials.
Selection criteria
Any randomised or quasi‐randomised controlled trials (RCT) on the treatment of primary inguinal hernia in adults were considered for inclusion.
Data collection and analysis
All abstracts identified by the search strategies were assessed by two independent researchers to exclude studies that did not meet the inclusion criteria. The full publications of all possibly relevant abstracts were obtained and formally assessed. Missing or updated informations was sought by contacting the authors.
Main results
Sixteen trials contributed to this review. A total of 2566 hernias were analysed in the Shouldice group with 1121 mesh and 1608 non‐mesh techniques. The recurrence rate with Shouldice techniques was higher than mesh techniques (OR 3.80, 95% CI 1.99 to 7.26) but lower than non‐mesh techniques (OR 0.62, 95% CI 0.45 to 0.85). There were no significant differences in chronic pain, complications and post‐operative stay. Female were nearly 3% of included patients.
Authors' conclusions
Shouldice herniorrhaphy is the best non‐mesh technique in terms of recurrence, though it is more time consuming and needs a slightly longer post‐operative hospital stay. The use of mesh is associated with a lower rate of recurrence. The quality of included studies, assessed with jaded scale, were low. Patients have similar characteristic in the treatment and control group but seems more healthy than in general population, this features may affect the dimension of effect in particularly recurrence rate could be higher in general population. Lost to follow‐up were similar in the treatment and control group but the reasons were often not reported. The length of follow‐up vary broadly among the studies from 1 year to 13.7 year.
Keywords: Adult; Female; Humans; Male; Fasciotomy; Suture Techniques; Hernia, Inguinal; Hernia, Inguinal/prevention & control; Hernia, Inguinal/surgery; Inguinal Canal; Inguinal Canal/surgery; Length of Stay; Postoperative Complications; Postoperative Complications/etiology; Randomized Controlled Trials as Topic; Secondary Prevention; Surgical Mesh
Plain language summary
Shouldice technique is better than other open techniques, not using mesh
Inguinal hernia is a very common disease that mainly affects men in young and middle age and it's reparation is the most frequent operation in general surgery. Hernias present as bulges in the groin area that can become more prominent when coughing, straining, standing up and in all situation where the abdominal pressure grow. If uncomplicated they are rarely painful, and the bulge commonly disappears on lying down. There are various surgical strategies which may be considered in the planning of inguinal hernia repair. These include the consideration of mesh use (mesh is a prosthesis made up by net of synthetic material that help to contrast a abdominal wall tension). A tension free repair method have been proposed to achieve better results in terms of pain and infections and to avoid the problem to present again (recurrence).
We found that the Shouldice technique is the best way to cure an inguinal hernia without using a prosthesis in terms of recurrence. The use of prosthesis reduces the recurrence even more. The persisting pain, post‐operative stay and complications after the intervention do not show significant differences between the techniques. Nevertheless the methodological quality of the most included studies is low, length of follow‐up is different among studies and findings lacks in patients oriented outcome so the unwelcome results, particularly in patients with chronic disease, for example diabetic or patients under steroidal therapy, should be considered with caution.
Background
Inguinal hernia repair is the most frequent operation in general surgery (Schumpelick 1994; Rutkow 2003; Mc Vay 1978). Since Bassini introduced his method for radical treatment of inguinal hernia (Bassini 1887), opening the modern era of herniorrhaphy, many other techniques have been developed using tension sutures between musculo‐aponeurotic tissues. These so‐called "non‐mesh" techniques have since been followed by many procedures that use synthetic fabrics made of various polymers to reinforce weak tissues ("mesh" techniques). Recurrence rates (reappearance of the hernia) vary considerably for the various techniques: reports vary from less than 5% to 25% (Grant 2002) and many of these recurrent hernias need repeated surgery (SHR 2002; Nilsson 1993). Improving the results would therefore have a useful medical and economic impact. The best results are achieved by surgeons reporting personal series using standard surgical procedures (Glassow 1986; Lichtenstein 1987; Wantz 1989). Some authors consider the Shoudice technique the best conventional method for open hernia repair (Bendavid 1997; Arvidsson 2005; Schippers 1996) while others prefer the Lichtenstein technique, achieving lower recurrence rates and shorter operating times (Nordin 2002). The main differences between the Shouldice technique and the other herniorrhaphies are the excision of the weakened fascia transversalis and the reconstruction of posterior wall of the inguinal canal with a running suture in three or four layers (Benard 1986; Devlin 1986). Recurrence rates for the Shouldice technique in specialist centres are as low as 0.6 ‐ 1.4% (Schumpelick 1994; Glassow 1986; Wantz 1989). However, under trial conditions in non‐specialised centres they range between 0 and 10% (Arlt 2002; Tons 1991; Kux 1994; Hoffmann 1991; Oosterhuis 1986; Tran 1992; Paul 1994; Panos 1992; Kingsnorth 1992; Fingerhut 1993; Kux 1994b). The superiority of this technique is therefore uncertain (Simons 1996). Moreover, chronic pain is common after repair, and it is not clear to what extent the different techniques influence its incidence (Koninger 2004). Some authors report a lower incidence of chronic pain after the Shouldice technique, while others found no difference after different operative techniques (Bay‐Nielsen 2004).
Even though the last search (2011) for additional included studies identified no new evidence, we decided to present this updated review, because Shouldice repair can be still the objective of new research (Higgins 2008).
Objectives
The primary objective of this review is to evaluate the efficacy of the Shouldice technique compared to other non‐laparoscopic techniques in reducing inguinal hernia recurrence rates in adults.
Methods
Criteria for considering studies for this review
Types of studies
Randomised or quasi‐randomised (allocating participants to a treatment on a not strictly random basis e.g. date of birth, hospital record number or alternation) controlled trials on the treatment of inguinal hernia were considered for inclusion. If the randomisation method was not specified the trial was included anyway. Trials in any language were included. We also considered studies including either primary and recurrent inguinal hernia when the report allowed the separate extraction of data on the primary repair.
Types of participants
Adults (age >18 years) of either sex presenting for treatment of primary inguinal hernia were included. The only specific definition of inguinal hernia was a groin protrusion. We excluded patients referred for femoral hernias.
Types of interventions
Treatment group: All forms of Shouldice technique, performed in the standard manner or slightly modified (e.g. differences in suture materials, number of layers).
Control group:
The surgical strategies were classified as:
1. "mesh" techniques (synthetic fabrics to reinforce weakened tissues):
Lichtenstein;
Plug and mesh;
Stoppa;
Trabucco.
2. "non‐mesh" techniques (tension sutures between musculo‐aponeurotic tissues):
Plication darn;
Bassini;
McVay.
There were three possible comparisons:
Shouldice versus "mesh" techniques;
Shouldice versus "non‐mesh" techniques;
Shouldice versus all techniques.
Types of outcome measures
Primary outcome
Recurrence of hernia defined as a clinically manifest bulge or protrusion exacerbated by a Valsalva manoeuvre in the operated groin. The assessor could be a surgeon, a physician or the patient himself. For the primary outcome we considered studies with at least one year follow‐up .
Secondary outcome:
Postoperative hospital stay (days).
Chronic pain, i.e. pain persisting for more than three months (only presence or absence)
Post‐operative satisfaction ( including general satisfaction and satisfaction with appearance. Numbers of participants dissatisfied, or the level of dissatisfaction on a visual analogue scale (0‐100) at the end of the trial were used).
Other complications, such as wound infection (SSI), hematoma and seroma
Conversion to the "opposite" technique after the procedure had started.
Duration of operation (minutes).
Search methods for identification of studies
The following databases were searched for relevant articles:
The Cochrane Library, EMBASE, MEDLINE.
Data collection and analysis
Eligibility
All abstracts identified by the above search strategies were assessed by two independent researchers to exclude studies that did not meet the inclusion criteria. The full publications of all possibly relevant abstracts were obtained and formally assessed for inclusion. Review authors were not blinded to the names of the authors, their institutions, the journal of publication, or the results.
Data extraction
A data extraction form was developed to record details of study design, participants, setting and timing, interventions, patients characteristics, follow‐up and outcomes. Data was extracted independently by two authors (CR and NR), seeking information on the patients: age, activities (i.e. job, sport, hobbies), health status (i.e. COPD, constipation, prostatism), hernia bilaterality, type of study, surgical techniques (standard or modified manner, kind of mesh, duration of intervention), outcomes, follow‐up, enter all data from the original articles onto specially designed, pre‐tested paper forms. Where a difference of opinion arose between reviewers, they were resolved through discussion with a third author (LM). Missing or updated informations were sought by contacting study authors.
Assessment of methodological quality
All studies that met meet the selection criteria were assessed for methodological quality, as recommended by the Cochrane Collaboration's Reviewers' Handbook (CC Handbook 2008; Deeks 2006). The internal validity of individual trials was assessed using the scale devised by Jadad et al. (Jadad 1996) and a single‐component approach exploring some important potential sources of bias:
The comparability of patients in the treatment and control groups (type of hernia, sex, age, abdominal pressure factors and bilaterality);
The randomizations method and concealed treatment allocation;
Exclusions after randomisation or losses to follow‐up without appropriate intention‐to‐treat analysis (particularly if related to one or other surgical approaches);
Ascertainment of outcome where knowledge of the allocation might have influenced the outcome measurement (we stress the importance of an independent assessor for diagnosis of recurrence (Schulz 1996; Smythe 1977),e.g. a surgeon unaware of the procedure performed).
Analysis of data from individual trials
Dichotomous outcomes Dichotomous outcomes (e.g., presence/absence of chronic pain) were reported as proportions (or response rates for each treatment) and compared directly (difference in proportions). We used these proportions to calculate odds ratios (OR), absolute risk reductions (risk differences), and numbers‐needed‐to‐treat (NNT), with 95% confidence intervals (CI). NNT were calculated as the reciprocal of the absolute risk reduction (Altman 1998). For unwanted effects (e.g., adverse events), the NNT becomes the number‐needed‐to‐harm (NNH), and was calculated in the same way.
Ordinal outcomes When outcome data were provided on an ordinal scale (e.g., for chronic pain: none, mild, moderate, severe, extremely severe), we selected a threshold based on the definition of clinically significant improvement and converted these data into dichotomous form. When it was not possible to split ordinal data into dichotomous outcomes meeting our a priori definition and no continuous data were reported, we assigned a numeric score to each category and analyse the results as continuous data.
Continuous outcomes For continuous data (e.g., duration of intervention), results are presented as weighted mean differences (WMD). However, when different scales were used to measure the same outcome, standardized mean differences (SMD) are used instead. We expected some studies to report treatment and control group means, without any data on the variance associated with these means. In such cases, we calculated or estimated variances based on primary data or test statistics, if these were reported. Combining results across studies For each broad comparison of surgical techniques (mesh/non‐mesh), we conducted a summary analysis of data on primary outcomes to provide an overall quantitative estimate of the relative Shouldice effect. The final summary analysis was conducted irrespective of the mesh comparator status (Shouldice vs. all techniques). We did not combine data from trials judged by consensus to be too clinically heterogeneous. When outcomes were reported at different time points greater than one year, data were pooled for each point and combined with data from other trials at similar time points. This allowed an estimate of the onset and persistence of treatment effect, at least over the time points available for combination of the data. A decision about which time points to be included in the final analysis was made by consensus after the data were collected with preference to outcomes measured at the end of the treatment period but also with the goal of comparing them if possible. outcomes at different points. We used the Cochrane Collaboration software Review Manager 5 (RevMan 5) for the figures and statistical analyses.
Heterogeneity Heterogeneity of effect sizes was assessed using the Z score and the Q (Chi‐square) and I‐squared statistic. The Q (Chi‐square) statistic was set at P < 0.10 because of the low statistical power of the test. I2 indicates the percent variability due to between or inter ‐ study variability as opposed to within or intra‐study variability. An I‐squared value greater than 50% was considered large (Higgins 2002). If statistical evidence was obtained for homogeneity of effect sizes, the analysis was to use a fixed‐effect model (Deeks 2001). Where there was significant statistically heterogeneity, a careful clinical review of the data was done to find the source (Thompson 2001). The reviewers than decided either: (1) to redo the analysis using the homogenous subgroup (only if there was a clear and compelling reason to exclude the heterogeneous data can be made); (2) to abandon statistical combining of the trials in favour of a narrative review of the literature; or (3) to redo the analysis using the random‐effects model. (DerSimonian 1986).
Sensitivity and subgroup analyses We planned a sensitivity analyses to explore how the following factors influenced the effect size: 1. Repeating the analysis taking account of study quality, as specified above; 2. Repeating the analysis excluding any very long or large studies to establish how much they dominate the results. Subgroup analyses were done to explore effect size differences, as follows: 1. Setting (specialised/non specialised surgery centre); 2. Trial country (Canada/other countries).
Evidence and clinical implications will be graded based on the quality single‐component approach in the following order of preference: detection bias, selection bias and attrition bias. Discordance between data sources was resolved using this grading system, with higher‐graded studies taking precedence over lower‐graded one.
Results
Description of studies
From the searches performed in April 2008, we identified 225 eligible studies; 111 were duplicates and were removed. According to the title or the abstract, 74 studies were excluded because they did not meet the inclusion criteria: 24 were not RCTs, 31 were about laparoscopic techniques and 19 papers were outside of the topic. Forty study reports were considered potentially relevant and the full text was sought.
The updated search (September 2011) revealed one study (Prieto‐Diaz‐Chavez 2009), potentially eligible for inclusion, but excluded because data about primary inguinal hernia were not extractable.
We could not find the full text of four papers (Pyka 2003; Stanislawek 2003; Strand 1998; Panos 1992) in either digital or in hard version and it was not possible to contact the authors; these articles were excluded. Sixteen articles were excluded because they did not meet the inclusion criteria (see 'Characteristics of excluded studies' table). The most common reason for exclusion was not being a RCT. Five studies are still awaiting classification because of translation (Koninger 1998; Kux 1994; Mittelstaedt 1999; Schmitz 1997; Porrero 2005). The characteristics of the 16 studies included are summarised in the "Characteristics of included studies" table, and assessment of the methodological quality of these 16 studies are presented in Table 1. All the authors of the included studies were contacted by mail to obtain further information. All additional data was considered unpublished data.
1. Assessment of methodological quality: Jadad Scale.
| Study | Randomization | Double‐blinding | Dropout/Withdrawls | TotalScore |
| Barth | 1 | 0 | 0 | 1 |
| Beets | 2 | 2 | 0 | 4 |
| Butters | 2 | 1 | 1 | 3 |
| Danielsson | 1 | 0 | 1 | 2 |
| Hay | 2 | 1 | 0 | 3 |
| Hetzer | 0 | 0 | 1 | 1 |
| Kingsnorth | 2 | 1 | 0 | 3 |
| Kovacs | 0 | 1 | 1 | 2 |
| Kux | 0 | 1 | 1 | 2 |
| McGillicuddy | 0 | 0 | 1 | 1 |
| Miedema | 2 | 1 | 1 | 4 |
| Nordin | 1 | 2 | 0 | 3 |
| Paul | 1 | 1 | 0 | 2 |
| Thapar | 1 | 0 | 1 | 2 |
| Tran | 1 | 0 | 0 | 1 |
| Zieren | 1 | 1 | 1 | 3 |
Sixteen trials were included in this review: the earliest were published in 1992 (Kingsnorth 1992; Tran 1992) and the most recent in 2004 (Miedema 2004; Koninger 2004). A total of 2566 hernias were analysed in the Shouldice group and compared with 1121 mesh techniques and 1608 non mesh techniques. Of the 16 studies included: seven compared the Shouldice technique versus mesh techniques (Barth 1998; Danielsson 1999; Hetzer 1999; Koninger 2004; McGillicuddy 1998; Nordin 2002; Zieren 1998), eight studies compared Shouldice and non mesh techniques (Beets 1997; Hay 1995; Kingsnorth 1992; Kovacs 1997; Kux 1994b; Paul 1994; Thapar 2000; Tran 1992), one study compared Shouldice with both mesh and non‐mesh techniques (Miedema 2004). All the sixteen studies considered a Shouldice hernioplasty using layers of unabsorbable continuous suture (Shouldice 1945; Glassow 1986); one study also considered a two‐layer Shouldice arm (Kux 1994b) and was excluded from the analysis. All the mesh hernioplasties were done according to the Lichtenstein technique (Lichtenstein 1989), except for one (Zieren 1998) that was a plug and mesh reconstruction (Rutkow 2003). Non‐mesh procedures were performed either according to the Bassini technique (Bassini 1887; Wantz 1989) in five studies (Beets 1997; Hay 1995; Kovacs 1997; Kux 1994b; Paul 1994); or according to the Mc Vay technique (Mc Vay 1978) in two studies (Hay 1995; Miedema 2004); and finally one study (Thapar 2000) used the Moloney's herniorrhaphy technique (Moloney 1972). The mean number of patients randomised in the included studies was 331 and ranged from 50 (Hetzer 1999) to 1647 (Hay 1995). Even though the Shouldice technique was developed in Canada most of the included trials were performed and conducted in Europe and USA. None of the included studies were from Canada. Only one trial (McGillicuddy 1998) was performed in a centre specialized in hernia repair; the others were in general surgery units.
CHARACTERISTICS OF OUTCOME MEASURES
Recurrence rate Thirteen of the included studies (Danielsson 1999; Hay 1995; Kingsnorth 1992; Kovacs 1997; Kux 1994b; McGillicuddy 1998; Miedema 2004; Nordin 2002; Paul 1994; Thapar 2000; Tran 1992; Zieren 1998) reported the recurrence rate, which was one of the most commonly recorded outcomes. Given that the timing of follow‐up to recurrence varied widely, recurrence rates were analysed at the longest follow‐up. Follow‐up varied between one year (Danielsson 1999; Kovacs 1997) and 13.7 years (Beets 1997) with a mean of 3.6 years. Seven studies considered recurrence as a lump in the groin not necessarily repaired; one considered a bulge at the operated groin and operated again, and four did not specify what they considered as a recurrence.
Lenght of post‐operative stay Eight studies reported the post‐operative stay, as the mean, in days +/‐ SD. Data expressed in hours were converted to days. When variability was reported as range or SEM, those data were converted to SD.
Chronic pain Seven studies reported data for pain persisting for more than eight weeks. If different times of follow‐up were available, only the longest was considered.
Other complications 13 studies reported data about surgical site infection. Only four reported the incidence of seroma; testicular atrophy was reported in five studies and haematoma was reported as an outcome in ten papers.
Duration of the operation Seven studies reported the duration of the operation, expressed as minutes in the operating room.
Risk of bias in included studies
‐ Randomization methods (allocation concealment and generation sequence) Most trials did not describe the generation of the random sequence or an adequate method to conceal allocation. Only one (Miedema 2004) reported a good method of allocation concealment (randomizations list held by a person not associated with the study) and proper sequence generation (random digit table). Of the remaining trials three (Nordin 2002; Paul 1994; Zieren 1998) reported the use of random number tables or computer randomisation but did not give any information about the allocation concealment; five trials (Beets 1997; Butters 2007; Hay 1995; Kingsnorth 1992; Thapar 2000) reported only allocation concealment and four (Barth 1998; Danielsson 1999; Kux 1994b; Tran 1992) did not give any information about randomizations or allocation concealment. Three trials (Hetzer 1999; Kovacs 1997; McGillicuddy 1998) used an inadequate method of randomizations (tossing a coin) or did not use any method and the method of allocation concealment was also considered inadequate for these trials.
‐ Dropouts and withdrawals
Reporting of drop‐outs and withdrawals was unsatisfactory in most trials and intention‐to‐treat analysis was very rare. Twelve trials reported data about exclusions after randomizations (four also specified the reasons). Dropout rate and length of follow‐up differed significantly between trials from 0% (Thapar 2000; Zieren 1998) to 51.8% (Kovacs 1997); 614 patients were lost to follow‐up (15.5%). Four studies had 20% or more losses to the longest follow‐up (Koninger 2004; Kovacs 1997; McGillicuddy 1998; Miedema 2004). Losses to follow‐up did not vary between treatment and control groups in any study. Mean follow‐up was 3.6 years (from 7 days (Barth 1998) to 13.7 years (Beets 1997)).
‐ Blinding Outcome assessors were unaware of the techniques used in six cases. The outcome assessor differed significantly in the trials: an independent surgeon was the assessor in three, the operating surgeon himself in three and a physician in three other studies.
Many data about methodological quality and results were reported in unclear terms and incompletely. These shortcomings on quality aspects and reporting are not surprising considering that the majority of trials were published before the arrival of initiatives and tools to improve the standards of trial reporting, such as the CONSORT Statement.
Table 1 reports the quality score according to Jadad 1996.
Effects of interventions
In our protocol we planned to present the final summary analysis irrespective of mesh comparator status. However, in view on the wide heterogeneity among the majority of analyses for broad comparisons of surgical techniques (mesh / non‐mesh) we decided to report the subgroup separately in a single Forest plot, without showing the final pooled estimate, but only the subgroup pooled estimates.
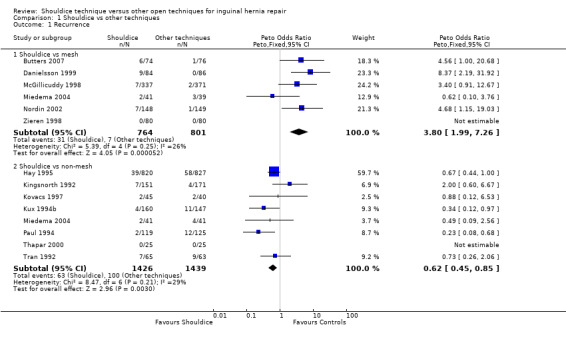
Shouldice vs. other techniques for recurrence rates (primary outcome) A Peto odds ratio was used to calculate the effect estimate because of the low event rate, with a high frequency of zero events in series. Sub‐category: Shouldice vs. mesh Five studies reported this outcome, comparing Shouldice with mesh (all) techniques. Five studies with 1415 patients reported lower recurrence rates in the control group (Peto OR 3.65, 95% CI 1.79 to 7.47, NNH 36). One of these five reported no events so it was excluded from the meta‐analysis. Three reported an OR in favour of control techniques; only one (Miedema 2004) showed an OR for recurrence in favour of Shouldice, but it was not significant. There were 31 recurrences in this sub‐group (25 in the Shouldice group and six in the control group). Heterogeneity was wide (I2 =43.6%).
Sub‐category: Shouldice vs. non‐mesh Eight trials comprising 2865 patients compared rates of recurrence after Shouldice and non‐mesh techniques. There was a significant difference in favour of the Shouldice technique (Peto OR 0.62, 95% CI 0.45 to 0.85, NNH 40). Heterogeneity was low (I2=29.2%). A total of 163 recurrences developed in this subgroup (63 Shouldice and 100 controls). One study reported no events so it was excluded from the meta‐analysis. Only one reported an OR (2.0, 95% CI 0.60 to 6.67) in favour of the control technique (modified Bassini technique); six studies reported an OR in favour of the Shouldice technique with OR ranging from 0.23 to 0.88 (Paul 1994; Kovacs 1997). Hay 1995 reported the most of data and its weight in the analysis was 59.56%.
PATIENT‐ORIENTED OUTCOMES
Shouldice vs. other techniques for length of post‐operative stay Trials were pooled using a weighted mean difference with a random effect model due to the expected wide heterogeneity.
Sub‐category: Shouldice vs. mesh Four trials assessed length of post‐operative stay, using data from 1045 patients. Three reported a WMD slightly in favour of Shouldice (Danielsson 1999; Hetzer 1999; Nordin 2002); one trial reported a significantly shorter post‐operative stay after a mesh technique (Zieren 1998). Pooling the data showed a WMD of 0.38 days (95% CI ‐0.41 to 1.18) in favour of mesh techniques, indicating that the post‐operative stay did not differed in the two groups.
Sub‐category: Shouldice vs. non‐mesh Patients undergoing Shouldice herniorrhaphy had a longer post‐operative stay (WMD 0.25, 95% CI 0.01 to 0.49). None of the four studies (565 patients) reported a shorter post‐operative stay for the Shouldice group; WMD varied from 0 (Kovacs 1997; Tran 1992) to 0.70 (Paul 1994).
Shouldice vs. other techniques for chronic pain A Peto OR was used to calculate the effect estimate because of the low event rate, with a high frequency of zero events in series.
Sub‐category: Shouldice vs. mesh Five trials reporting data about chronic pain in 1371 patients were pooled; 94 patients experienced chronic pain (44 in the Shouldice group, 50 in the mesh group). Peto OR was in favour of Shouldice (Peto OR 0.87, 95% CI 0.55 to 1.39), but not significantly. Heterogeneity was wide (I2 = 59.6%). Two studies reported a Peto OR in favour of the Shouldice technique (McGillicuddy 1998; Miedema 2004) but only the second one was significant. The other three reported a higher rate of chronic pain in the Shouldice group (Koninger 2004; Nordin 2002; Zieren 1998) none of these was significant.
Sub‐category: Shouldice vs. non‐mesh Only three trials involving 1968 patients compared the Shouldice and non‐mesh techniques. Peto OR was 0.30 (95% CI 0.40 to 1.22) in favour of Shouldice. One trial (Hay 1995), with 1647 patients had a substantial weight in the pooled data (81.83%).
Shouldice vs. other techniques for patient satisfaction level We were unable to develop a Forest plot because we found only one study (Miedema 2004) that considered this.
OTHER COMPLICATIONS
Shouldice vs. other techniques for complications A Peto OR was used to calculate the effect estimate because of the low event rate with a high frequency of zero events in series.
Sub‐category: Shouldice vs. mesh Seven trials assessed wound infection rates. One (Barth 1998) reported no events so it was excluded from the meta‐analysis. Patients who underwent Shouldice herniorrhaphy had fewer wound infections (Peto OR 0.74, 95% CI 0.37 to 1.49). Seroma and testicular did not differed in the two groups (Peto OR 0.96 and 1.05). The haematoma rate was slightly in favour of the Shouldice group (Peto OR 0.63, 95% CI 0.24 to 1.66).
Sub‐category: Shouldice vs. non‐mesh Seven trials pooling 1635 patients showed a slightly higher infection rate in the Shouldice group (Peto OR 1.34, 95% CI 0.70 to 2.54). Thapar 2000 reported no events in both groups. Only one trial (Tran 1992) reported seroma rates (Peto OR 2.86, 95% CI 0.39 to 20.74). Three studies considered testicular atrophy; one (Kovacs 1997) reported no events. Pooling the other two (Hay 1995; Beets 1997) resulted in a Peto OR 1.09 (95% CI 0.21 to 5.50). Seven reported a lower haematoma rate in the Shouldice group (Peto OR 0.84, 95% CI 0.63 to 1.13).
TECHNICAL OUTCOMES
Shouldice vs. other techniques for conversion to another technique No trials reported on this outcome.
Shouldice vs. other techniques for duration of operation Trials were pooled using a WMD with a random effect model on account of expected wide heterogeneity.
Sub‐category: Shouldice vs. mesh Five trials involving 1251 patients reported the duration of the operation. The mesh techniques took less time (WMD 9.64 minutes, 95% CI 6.96 to 12.32). Four studies (Barth 1998; Danielsson 1999; Hetzer 1999; Zieren 1998) reported a shorter operating time for the mesh group (WMD between 2 and 15 minutes). Only Miedema 2004 reported a longer time in the mesh group (WMD ‐ 2 minutes, 95% CI ‐15.86 to 11.86). Heterogeneity was wide (I2 = 63.9%).
Sub‐category: Shouldice vs. non‐mesh Three trials involving 372 patients assessed operating time as an outcome. Shouldice was a longer procedure than non‐mesh techniques (WMD 10.10, 95% CI 6.78 to 13.42). Miedema 2004 reported no differences in the duration of the operation (WMD 0 minutes, 95% CI ‐13.86 to 13.86). Test for heterogeneity was significant (I2 = 83.4%).
We planned a series of sensitivity and sub‐group analyses but were not able to do the planned subgroup analysis because of the small number of studies found or the lack of variability among them.
Discussion
Our results showed that Shouldice herniorrhaphy is a good technique for inguinal hernia repair compared to other non‐mesh techniques, giving better results in terms of recurrence (4.4% vs. 6.9%; Peto OR 0.62, 95% CI 0.45 to 0.85, NNH 40). Comparing Shouldice to mesh techniques, the recurrence rate was lower in the control group (3.6% vs, 0.8%; Peto OR 3.65, 95% CI 1.79 to 7.47, NNH 36). The review by Scott (Scott 2001) also found Shouldice to be the best non‐mesh technique in terms of recurrence. These results mainly reflect differences in the control procedures and different degrees of familiarity of the surgeons with the techniques, making it impossible to eliminate the "handcraft" variable from surgical trials. Data about recurrences were recorded at different times of follow‐up; however, this source of heterogeneity does not affect the overall direction or strength of our results. None of the trials reported a shorter duration of operation for the Shouldice group and in fact all the control techniques took less time to perform regardless of whether they used mesh or not (WMD 9.64 and 10.10 minutes vs. mesh and non‐mesh respectively). However, this outcome showed wide heterogeneity (time to perform a Shouldice techniques from 47 to 121 minutes) for various reasons (e.g. different ways of collecting data about the duration of the operation (skin‐to‐skin, time in the operating room) and different levels of skill). There were no significant differences about chronic pain, complications and post‐operative stay for the various techniques. The lack of differences between Shouldice and other techniques for chronic pain might reflect the small number of trials. Complications rates did not differ either, between Shouldice and other techniques indicating that these are mainly due to the dissection time of the procedure rather than to the reconstruction technique. The Shouldice technique seemed to require a longer post‐operative stay but these data were not significant and highly heterogeneous. Only one trial (Miedema 2004) considered satisfaction as an outcome and found no difference between Shouldice and other techniques.
Thease conclusion from this systematic review of RCT is flawed by some problems:
1) The quality of included studies, assessed by using the Jadad scale (Jadad 1996), were low.
2) the outcome assessor wasn't blind in a relevant number of trials often the outcome evaluator was the same surgeon that performed the intervention.
3) Patients have similar characteristic in the treatment and control group but seems more healthy than in general population, this features may affect the dimension of effect in particularly recurrence rate in general population could be higher, for example patients with chronic disease, that could affect tissue reparation, were often excluded. We do not find data on patients employment that we considered relevant in terms of recurrence rate causal condition (heavy workers vs office workers). Female were nearly 3% of included patients.
4) Lost to follow‐up were similar in the treatment and control group but the reasons were often not reported and the length of follow‐up vary broadly among the studies (from 1 year to 13.7 year)
5) The data on perioperative treatment are missing or not comparable, especially the duration of intervention.
6) None of the included trials report if the authors have some conflict of interest or the source of founding to develop the study
7) Patient‐oriented outcomes (satisfaction and post‐operative discomfort) were rare and should be investigated as primary outcomes
The absence of some relevant information on blinding, generation of allocation sequence, type of randomizations, allocation concealment, reasons of withdrawals and lost to follow‐up or declaration of conflict of interest are mainly ascribable to poor reporting, this is imputable to the date of publication of the studies (most of them have been published before CONSORT Statement development). Nevertheless the large amount of patients included in the review makes our results consistent and reliable.
Authors' conclusions
Implications for practice.
Shouldice herniorrhaphy is the best non‐mesh techniques in terms of recurrence even though longer to perform and needs a slightly longer post‐operative hospital stay. However the use of mesh markedly reduces recurrences (3.6% vs. 0.8%). When mesh is not available, is too costly or is refused by the patient, the Shouldice technique is the best alternative.
Implications for research.
Further investigations in hernia surgery are still needed. Patient‐oriented outcomes (satisfaction and post‐operative discomfort) should be investigated as primary outcomes, like recurrence rates. The low methodological quality and poor data reporting of most of the trials call for improvement in surgical RCTs, in accordance with CONSORT requirements.
What's new
| Date | Event | Description |
|---|---|---|
| 7 August 2012 | Review declared as stable | It is unlikely that their will be new studies to add to this systematic review |
History
Protocol first published: Issue 2, 2006 Review first published: Issue 4, 2009
| Date | Event | Description |
|---|---|---|
| 14 March 2012 | New citation required but conclusions have not changed | Review updated ‐ no new trials included |
| 14 March 2012 | New search has been performed | xxx |
| 27 February 2012 | New search has been performed | Searches updated |
| 7 March 2009 | New search has been performed | major update |
| 22 July 2008 | Amended | Converted to new review format. |
Acknowledgements
None
Appendices
Appendix 1. EMBASE search strategy
1. exp inguinal hernia 2. inguinal hernia.mp. 3. 1 or 2 4. shouldice technique.mp. 5. shouldice.mp. 6. 4 or 5 7. 3 and 6 8. randomized controlled trial 9. randomization 10. controlled study 11. multicenter study 12. phase 3 clinical trial 13. phase 4 clinical trial 14. double blind procedure 15. single blind procedure 16. ((singl* or doubl* or trebl* or tripl*) adj (blind* or mask*)).ti,ab. 17. (random* or cross* over* or factorial* or placebo* or volunteer*).ti,ab. 18. 13 or 10 or 14 or 16 or 9 or 15 or 11 or 8 or 17 or 12 19. "human*".ti,ab. 20. (animal* or nonhuman*).ti,ab. 21. 20 and 19 22. 20 not 21 23. 18 not 22 24. 7 and 23
Appendix 2. MEDLINE search strategy
1. exp Hernia, Inguinal 2. inguinal hernia.mp. 3. 1 or 2 4. shouldice technique.mp 5. shouldice.mp. 6. 4 or 5 7. 3 and 6 8. randomized controlled trial.pt. 9. controlled clinical trial.pt. 10. randomized.ab. 11. placebo.ab. 12. clinical trial.sh. 13. randomly.ab. 14. trial.ti. 15. 8 or 9 or 10 or 11 or 12 or 13 or 14 16. humans.sh. 17. 15 and 16 18. 7 and 17
Appendix 3. COCHRANE LIBRARY search strategy
1. MeSH descriptor Hernia, Inguinal, this term only in MeSH products 2. inguinal‐hernia in All Fields in all products 3. (#1 OR #2) 4. (shouldice technique) in All Fields in all products 5. shouldice in All Fields in all products 6. (#4 OR #5) 7. (#3 AND #6)
Data and analyses
Comparison 1. Shouldice vs other techniques.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Recurrence | 13 | Peto Odds Ratio (Peto, Fixed, 95% CI) | Subtotals only | |
| 1.1 Shouldice vs mesh | 6 | 1565 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 3.80 [1.99, 7.26] |
| 1.2 Shouldice vs non‐mesh | 8 | 2865 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.62 [0.45, 0.85] |
| 2 Lenght of postoperative stay (days) | 8 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 Shouldice vs mesh | 4 | 1045 | Mean Difference (IV, Random, 95% CI) | 0.38 [‐0.41, 1.18] |
| 2.2 Shouldice vs non mesh | 4 | 565 | Mean Difference (IV, Random, 95% CI) | 0.25 [0.01, 0.49] |
| 3 Chronic pain | 7 | Peto Odds Ratio (Peto, Fixed, 95% CI) | Subtotals only | |
| 3.1 Shouldice vs mesh | 5 | 1371 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.87 [0.55, 1.39] |
| 3.2 Shouldice vs non mesh | 3 | 1968 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.70 [0.40, 1.22] |
| 4 Wound Infection | 13 | Peto Odds Ratio (Peto, Fixed, 95% CI) | Subtotals only | |
| 4.1 Shouldice vs mesh | 7 | 1938 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.74 [0.37, 1.49] |
| 4.2 Shouldice vs non mesh | 7 | 2635 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 1.34 [0.70, 2.54] |
| 5 Seroma | 4 | Peto Odds Ratio (Peto, Fixed, 95% CI) | Subtotals only | |
| 5.1 Shouldice vs mesh | 3 | 1165 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.96 [0.37, 2.50] |
| 5.2 Shouldice vs non mesh | 1 | 142 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 2.86 [0.39, 20.74] |
| 6 Testicular atrophy | 6 | Odds Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 6.1 Shouldice vs mesh | 3 | 1155 | Odds Ratio (M‐H, Random, 95% CI) | 1.05 [0.04, 27.38] |
| 6.2 Shouldice vs non mesh | 3 | 1995 | Odds Ratio (M‐H, Random, 95% CI) | 1.09 [0.21, 5.50] |
| 7 Haematoma | 10 | Peto Odds Ratio (Peto, Fixed, 95% CI) | Subtotals only | |
| 7.1 Shouldice vs mesh | 3 | 562 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.64 [0.25, 1.64] |
| 7.2 Shouldice vs non mesh | 7 | 2797 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.84 [0.63, 1.13] |
| 8 Duration of the operation (Minutes) | 7 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 8.1 Shouldice vs Mesh | 5 | 954 | Mean Difference (IV, Fixed, 95% CI) | 9.64 [6.96, 12.32] |
| 8.2 Shouldice vs non mesh | 3 | 372 | Mean Difference (IV, Fixed, 95% CI) | 10.10 [6.78, 13.42] |
1.1. Analysis.
Comparison 1 Shouldice vs other techniques, Outcome 1 Recurrence.
1.2. Analysis.

Comparison 1 Shouldice vs other techniques, Outcome 2 Lenght of postoperative stay (days).
1.3. Analysis.

Comparison 1 Shouldice vs other techniques, Outcome 3 Chronic pain.
1.4. Analysis.

Comparison 1 Shouldice vs other techniques, Outcome 4 Wound Infection.
1.5. Analysis.

Comparison 1 Shouldice vs other techniques, Outcome 5 Seroma.
1.6. Analysis.

Comparison 1 Shouldice vs other techniques, Outcome 6 Testicular atrophy.
1.7. Analysis.

Comparison 1 Shouldice vs other techniques, Outcome 7 Haematoma.
1.8. Analysis.

Comparison 1 Shouldice vs other techniques, Outcome 8 Duration of the operation (Minutes).
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Barth 1998.
| Methods | Multicenter, two arms RCT of Shouldice vs Lichtenstein. Randomization: methods not stated. Maximum follow up: 7 days. Exclusions after randomizations: not reported. Protocol violations: 2 patients randomised to Shouldice received Lichtenstein(analysed in Shouldice group). Analyses by protocol. Jadad quality score: 1. | |
| Participants | Country: USA. Setting: 2 centres not specialized in hernia repair. Total enrolled patients: 105 (105 hernias) 51 Shouldice vs 54 Lichtenstein. Mean age (SEM): Shouldice 51 (2,4); Lichtenstein 53 (2,2). Gender: 104 M; 1 F. Inclusion criteria: age> 18, inguinal primary hernia, only elective repair. Exclusion criteria: not reported. Demographic and baseline data reported: comparable for hernia duration (months), age, hernia type and diameter, employment. | |
| Interventions | Shouldice standard (n=51) performing 4 layers. Polypropylene 2/0. Lichtenstein standard (n=54). Polypropylene Mesh. Polypropylene 2/0. | |
| Outcomes | Lenght of postoperative stay. Wound infection. Haematoma. Duration of operation. | |
| Notes | Conflict of interest: not reported. Sources of funding: not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Beets 1997.
| Methods | Single centre, four arms RCT ‐ comparisons: Shouldice vs Bassini (considered in this review); Bassini vs Ring Narrowing (the two arms are not considered in this review). Randomization: generation of sequence not stated; allocation concealment using sealed envelopes. Maximum follow up: 13.7 years. Exclusions after randomizations: 6 hernias (reasons not specified). Protocol violations: 49 Shouldice repairs converted to Bassini (reasons: surgeon not familiar with Shouldice technique or not aware about patient's enrolled in the trial). Analyses by protocol. Losses to follow up (data collapsed for all arms): 30 patients (11,4%). Jadad quality score: 4. | |
| Participants | Country: Netherlands. Setting: centre not specialized in hernia repair. Total enrolled patients (four arms): 375 (hernias 425). Two interest arms: 263 hernias, 103 Shouldice and 160 Bassini. Mean age (SD): Shouldice 57 (13); Bassini 57 (14). Gender: 375 M. Inclusion criteria: age>18, primary inguinal hernia, elective repair. Exclusion criteria: life expectancy <2 year, major concomitant operation. Demographic and baseline data reported: comparability for activities, COPD, prostatism, constipation, bilaterality, experience of operating surgeon; unbalance between arms for previous repair of inguinal hernia (Shouldice 11% vs Bassini 22%). | |
| Interventions | Bassini modified by Stetten (n=160). Non Mesh. Nylon 2/0. Shouldice modified (n=103) performing 3 layers. Nylon 2/0. | |
| Outcomes | Recurrence (lump in groin not necessarily re‐operated). Chronic pain. Wound infection Testicular atrophy. Haematoma. | |
| Notes | Recurrence at 13.7 follow up years assessed by an independent surgeon in 179/194 hernias (four arms); 15/194 by telephone interview. 89 patients (100 hernias) died during the study. Conflict of interest: not reported. Sources of funding: not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
Butters 2007.
| Methods | Single centre, three arms RCT ‐ Conparisons: Shouldice vs Lichtenstein vs TAPP (not considered). Randomization: generation of sequence not stated, Allocation concealment using sealed envelopes. Maximum follow up: 52 months. Exclusion after randomizations: no. Losses to follow up: Shouldice 19, Lichtenstein 17 (9 deaths, 5 moved to other places and 22 refused to continue). Analyses by protocol | |
| Participants | Country: Germany. Setting: centre specialized in hernia repair. Total enrolled patients: 186 (93 Shouldice vs 93 Lichtenstein). Mean age: Shouldice: 53; Lichtenstein 56. Gender: 186 M. Inclusion criteria: age >18, primary inguinal hernia, elective repair. Exclusion criteria: no known. Demographic and baseline data reported: comparability for age, type of hernia. | |
| Interventions | Shouldice (n=93). Technical notes not specified. Lictenstein standard (n=93). | |
| Outcomes | Recurrence (definition of recurrence not reported). Chronic pain (data from Koninger 2004). Postoperative satisfaction level Testicular atrophy |
|
| Notes | 52 months follow up assessed by a resident surgeon by physical examination in 150 patients (80.6%) Conflict of interest: not reported. Sources of funding: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
Danielsson 1999.
| Methods | Single centre, two arms RCT of Shouldice vs Lichtenstein. Randomization: methods not reported. Maximum follow up: 1 year. Exclusions after randomizations: 22 (reasons not specified). Analyses by protocol Losses to follow up: 8 patients. Jadad quality score: 2. | |
| Participants | Country: Sweden. Setting: centre not specialized in hernia repair. Total enrolled patients: 200; 178 hernias (89 Shouldice vs 89 Lichtenstein). Mean age (SD): Shouldice 56 (16); Lichtenstein 58 (14). Gender: 200 M. Inclusion criteria: age> 18, inguinal primary hernia, only elective repair. Exclusion criteria: incarcerated hernias and emergency operations. Demographic and baseline data reported: comparable for activities (data not provided) and age. | |
| Interventions | Shouldice standard (n=89) performing 4 layers. Non‐absorbable monofilament. Lichtenstein standard (n=89). Polypropylene Mesh. | |
| Outcomes | Recurrence (symptomatic lump in groin and re operated). Lenght of postoperative stay. Wound infection. Duration of operation. | |
| Notes | Recurrence at 1 year follow up assessed by surgeon or patient himself in 170 patients (84 Shouldice; 86 Lichtenstein). Conflict of interest: not reported. Sources of funding: not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Hay 1995.
| Methods | Multicenter, four arms RCT ‐ comparisons: Shouldice steel and Shouldice polypropylene (pooled together) vs Bassini vs Mc Vay. Randomization: generation of sequence not reported; allocation concealment by un stapling corner of the questionnaire. Maximum follow up: 8,5 years. Exclusions after randomizations: 57 patients (most were foreigners who returned their countries). Intention to treat analyses. Losses to follow up: 86 patients (5,6%). Jadad quality score: 3. | |
| Participants | Country: France. Setting: centres not specialized in hernia repair. Total enrolled patients: 1578(1706 hernias); 1521patients (1647 hernias) (829 Shouldice, 420 Bassini, 407 Mc Vay). Mean age (SD): Shouldice 52,5 (15,6); Bassini 55 (15,2); Mc Vay 54,2 (14,8). Gender: 1578 M. Inclusion criteria: age> 15, inguinal primary hernia, elective or emergency repair. Exclusion criteria: Females, foreigners, femoral ipsilateral hernia associated. Demographic and baseline data reported: comparable for sex, age, activities, COPD, constipation and dysuria, healing influencing factors (all data reported). | |
| Interventions | Shouldice steel (n=401). 4 layers. Steel wire and polypropylene. Shouldice polypropylene (n=419). 4 layers. Polypropylene. Bassini modified (n=420). Polypropylene. Mc Vay modified (n=407). Polypropylene. | |
| Outcomes | Recurrences (lump in groin not necessarily re operated) ‐ data not extractable Lenght of postoperative stay Chronic pain Wound infection Testicular atrophy Haematoma | |
| Notes | Recurrence at 8,5 years follow up assessed by an independent surgeon or patient himself or physician. Conflict of interest: not reported. Sources of funding: not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
Hetzer 1999.
| Methods | Multicenter, two arms RCT of Shouldice vs Lichtenstein. Randomization: Day of intervention. Allocation concealment inadequate. Maximum follow up: 3 months. Exclusions after randomizations: 562 hernias (randomizations performed before evaluation of inclusion criteria). Analyses by protocol. Losses to follow up: none. Jadad quality score: 1. | |
| Participants | Country: Switzerland. Setting: centres not specialized in hernia repair. Total enrolled patients (two arms): 385 patients; number of hernias: 410 (171 Shouldice vs 239 Lichtenstein). Mean age (SD): Shouldice 53 (16,77); Lichtenstein 58 (17,36). Gender: 385 M. Inclusion criteria: age>18, primary inguinal hernia, elective repair. Exclusion criteria: incarcerated hernia, previous operation in the inguinal region, coagulopathy, diabetes, prostatic hyperplasia, wish for general anaesthesia. Demographic and baseline data reported: comparability for age, type of hernia(all data reported). | |
| Interventions | Shouldice Standard (n=171). 4 layers. PDS 2/0. Lichtenstein (n=239). Polypropylene meshes. Polypropylene 2/0. | |
| Outcomes | Lenght of postoperative stay. Wound Infection. Duration of operation. | |
| Notes | Conflict of interest: not reported. Sources of funding: not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | High risk | C ‐ Inadequate |
Kingsnorth 1992.
| Methods | Single centre, two arms RCT of Shouldice vs Plication Darn (Bassini modified). Randomization: generation of sequence not stated, allocation concealment: randomizations just before skin incision. Maximum follow up: 2 years. Exclusions after randomizations: no. Intention to treat analyses. Losses to follow up: 98 (reasons not specified). Jadad quality score: 3. | |
| Participants | Country: UK. Setting: centre not specialized in hernia repair. Total enrolled patients: 322; 322 hernias (151 Shouldice vs 171 Plication Darn). Mean age: Shouldice 58,3; Plication Darn 57. Gender: 304 M; 18 F Inclusion criteria: age>18, primary inguinal hernia, elective repair. Exclusion criteria: no known. Demographic and baseline data reported: comparability for age, type of hernia, sex (all data reported). | |
| Interventions | Shouldice (n=151). Technical notes not specified. Plication Darn (Bassini modified) (n=171). | |
| Outcomes | Recurrence (definition of recurrence not reported). Lenght of postoperative stay. Wound infection. Haematoma. | |
| Notes | Recurrence at 2 years follow up assessed by a consultant or a surgical registrar or pro forma in 224 patients. Recurrence at 4 years follow up only in 61 (18,9%) patients so data from this follow up will not be considered. Conflict of interest: not reported. Sources of funding: not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
Kovacs 1997.
| Methods | Single centre, two arms RCT of Shouldice vs Bassini‐Kirschner. Randomization: date of birth, allocation concealment not specified. Maximum follow up: 1 year. Exclusions after randomizations: no. Losses to follow up: Shouldice 18, Bassini‐Kirschner 26 (reasons not specified). Jadad quality score: 2. | |
| Participants | Country: Hungary. Setting: centre not specialized in hernia repair. Total enrolled patients: 129 (63 Shouldice vs 66 Bassini‐Kirschner). Mean age: Shouldice 52; Bassini‐Kirschner 54. Gender: 129 M. Inclusion criteria: age>18, primary inguinal hernia. Exclusion criteria: no known. Demographic and baseline data reported: comparability for age, bilaterality and sex. | |
| Interventions | Shouldice standard (n=63) performing 4 layers. Non‐absorbable monofilament. Bassini‐Kirschner (n=66). Suture in Mersilene 0. | |
| Outcomes | Recurrence (lump in groin and re operated). Lenght of postoperative stay. Wound infection. Testicular atrophy Haematoma. Duration of the operation. | |
| Notes | Recurrence at 1 year follow up assessed by a hospital staff surgeon in 85 patients (66%). Conflict of interest: not reported. Sources of funding: not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | High risk | C ‐ Inadequate |
Kux 1994b.
| Methods | Single centre, four arms RCT ‐ comparison: Shouldice vs Bassini (Bassini with absorbable sutures and two‐layers Shouldice not considered). Randomization: methods not stated. Maximum follow up: 2 years. Exclusions after randomizations: not reported. Analyses by protocol. losses to follow up: 50 (reasons not specified) Jadad quality score: 2. | |
| Participants | Country: Austria. Setting: centre not specialized in hernia repair. Total enrolled patients: 400. 307 primary hernia repair. (Shouldice 4 rows 160; Bassini unabsorbable 147). Mean age (SD): not reported. Gender: data not clear. Inclusion criteria: Inguinal hernia (also recurrent hernias). Exclusion criteria: not reported. Demographic and baseline data reported: comparability for sex, type of hernia, recurrence, obesity, bronchitis, hernia sac >8 cm (all data reported). | |
| Interventions | Shouldice standard (n=160). 4 layers. Polypropylene. Bassini modified (n=147). Polyester. | |
| Outcomes | Recurrence (lump in groin not necessarily re operated). | |
| Notes | Recurrence at 2 years follow up assessed by a hospital staff surgeon in 683 patients(93,6%). Conflict of interest: not reported. Sources of funding: not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
McGillicuddy 1998.
| Methods | Single centre, two arms RCT of Shouldice vs Lichtenstein. Randomization: coin toss, allocation concealment inadequate. Maximum follow up: 5 years. Exclusion after randomizations: 31 (patients decided to undergo a laparoscopic repair). Intention to treat analyses. Losses to follow up: 251(35,5%) Jadad quality score: 1. | |
| Participants | Country: USA Setting: private centre specialized in hernia repair. Total enrolled patients: 672. 717 hernias. Mean age (SD): data not reported Gender: 672 M. Inclusion criteria: inguinal hernia. Demographic and baseline data reported: comparability for sex, age, activity (data not reported). | |
| Interventions | Shouldice standard (n=337) performing 4 layers. Non‐absorbable monofilament. Lichtenstein standard (n=371). Polypropylene Mesh. | |
| Outcomes | Recurrence Chronic pain Wound infection Testicular atrophy | |
| Notes | Recurrence at 5 years follow up assessed by the operating surgeon in 99% of patients. Conflict of interest: not reported. Sources of funding: not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | High risk | C ‐ Inadequate |
Miedema 2004.
| Methods | Single centre, three arms RCT of Shouldice vs Lichtenstein vs Mc Vay. Randomization: generation of sequence by random digit table; allocation list maintained by a person unassociated with the study. Follow up: 7 years. Exclusions after randomizations: not reported. Losses to follow up: 29 (could not be contacted). Analyses by protocol. Jadad quality score: 4. | |
| Participants | Country: USA. Setting: centre not specialized in hernia repair. Total enrolled patients: 146. Three arms: 150 hernias (52 Shouldice, 49 Lichtenstein and 49 Mc Vay). Mean age: 62 Shouldice, 63 Lichtenstein, 65 Mc Vay. Gender: 146 M. Inclusion criteria: Primary inguinal hernia. Exclusion criteria: age <18 years, use of systemic steroids, incarcerated hernia, recurrent hernia, collagen or vascular disease, ASA 4 or 5, allergy to acetaminophen or codeine. Demographic and baseline data reported: comparability for sex, COPD, prostatism and constipation. | |
| Interventions | Shouldice modified (n=41). 4 layers. Polypropylene. Lichtenstein standard (n=39). McVay standard (n=41). | |
| Outcomes | Recurrence (lump in groin not necessarily re‐operated). Lenght of postoperative stay. Postoperative satisfaction level. Wound infection. Haematoma. Duration of the operation. | |
| Notes | Recurrence at 6‐9 years follow up assessed by clinical examination in 121 patients(29 lost at follow up). Conflict of interest: not reported. Sources of funding: not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
Nordin 2002.
| Methods | Single centre, two arms RCT of Shouldice vs Lichtenstein. Randomization: generation sequence by computer generated in blocks of ten patients, allocation concealment not specified. Maximum follow up: 6 years. Exclusions after randomizations: 2 patients refused to continue, 1 hernia not found. Losses to follow up: 9 (reasons not specified). Intention to treat analyses Jadad quality score: 3. | |
| Participants | Country: Sweden. Setting: centre not specialized in hernia repair. Total enrolled patients: 300. 297 hernias (148 Shouldice 149 Lichtenstein). Age range: 25‐75. Gender: 300 M. Inclusion criteria: age >18, primary inguinal hernia. Exclusion criteria: irreducibility of hernia, coagulation abnormalities or anticoagulant treatment. Demographic and baseline data: comparability for age, type of hernia, activities, testicular preoperative size (data not reported). | |
| Interventions | Shouldice Standard (n=148). 4 layers. Polypropylene 2/0. Lichtenstein (n=149). Marlex meshes. Polypropylene 2/0. | |
| Outcomes | Recurrence (lump in groin not necessarily re operated). Lenght of postoperative stay. Chronic pain. Wound infection. Seroma. Testicular atrophy. Haematoma. Duration of operation. | |
| Notes | Recurrence at 3‐6 years follow up assessed by an independent surgeon in 284 patients. Conflict of interest: not reported. Sources of funding: not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Paul 1994.
| Methods | Single centre, two arms RCT of Shouldice vs Bassini. Randomization: balanced blocks, allocation concealment not specified. Maximum follow up: 5 years. Exclusions after randomizations: no. Losses to maximum follow up: 21 (reasons not specified). Analyses by protocol Jadad quality score: 2. | |
| Participants | Country: Germany. Setting: centre not specialized in hernia repair. Total enrolled patients: 265. (119 Shouldice vs 125 Bassini) Mean age (SD): data not reported Gender: 265 M. Inclusion criteria: Primary inguinal hernia. Exclusion criteria: Bilaterality, femoral hernias, incarcerated hernias, renal and liver failure. Demographic and baseline data reported: comparability for constipation, obesity, bronchitis(data not reported). | |
| Interventions | Shouldice modified (n=119). 4 layers. unabsorbable suture. Bassini modified (n=125). 2 layers. interrupted stitches of unabsorbable suture. | |
| Outcomes | Recurrence (symptomatic lump in groin and re operated). Lenght of postoperative stay. Duration of operation. | |
| Notes | Recurrence at 3 years follow up assessed by clinical examination in 91,5%of Shouldice group and 92,6% of Bassini group. Conflict of interest: not reported. Sources of funding: not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Thapar 2000.
| Methods | Single centre, two arms RCT of Shouldice vs Moloney's Darn. Randomization: generation sequence: Unclear; allocation concealment: randomizations just before skin incision. Maximum follow up: 2 years. Exclusions after randomizations: no. Losses to follow up: none. Jadad quality score: 2. | |
| Participants | Country: India. Setting: centre not specialized in hernia repair. Total enrolled patients: 50 (25 Shouldice vs 25 Moloney's darn). Age range: 18‐40. Gender: 50 M. Inclusion criteria: age >18. Exclusion criteria: bilaterality, recurrent hernias and inguinoscrotal pathologies Demographic and baseline data: comparability for side and type of hernia (data reported). | |
| Interventions | Shouldice standard (n=25). 4 layers. unabsorbable suture. Moloney's darn (n=25). 2 layers. unabsorbable suture. | |
| Outcomes | Recurrence (lump in groin not necessarily re operated). Lenght of postoperative stay. Wound infection. Haematoma. | |
| Notes | Conflict of interest: not reported. Sources of funding: not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
Tran 1992.
| Methods | Single centre, two arms RCT of Shouldice vs Bassini‐Kirschner. Randomization: method not specified, allocation concealment not specified. Maximum follow up: 2 years. Exclusions after randomizations: 5 (2 recurrent hernias, 1 femoral hernia, 1 refused the randomizations and in 1 for technical matters). Analyses by protocol. Losses to follow up: 8 patients (reasons not specified). Jadad quality score: 1. | |
| Participants | Country: Germany. Setting: centre not specialized in hernia repair. Total enrolled patients: 138. 142 hernias (70 Shouldice vs 72 Bassini‐Kirschner). Mean age: Shouldice: males 55, females 62; Bassini‐Kirschner: males 54, females 47. Gender: 114 M, 24 F. Inclusion criteria: age >14, primary inguinal hernia. Exclusion criteria: not specified. Demographic and baseline data reported: comparability for age, sex, weight, height, type of hernia, qualification of operating surgeon (data reported). | |
| Interventions | Shouldice unclear (n=70). Bassini‐Kirschner unclear (n=72). Vicryl metric 1. | |
| Outcomes | Recurrence (lump in groin not necessarily re operated). Lenght of postoperative stay. Wound infection. Seroma. Haematoma. Duration of operation. | |
| Notes | Recurrence at 24 months follow up assessed by a general physician or one of the author in 128 patients. Conflict of interest: not reported. Sources of funding: not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Zieren 1998.
| Methods | Single centre, three arms RCT ‐ comparisons: Shouldice vs Plug and patch vs TAPP (not considered for the analyses). Randomization: computer generated. Allocation concealment not specified. Maximum follow up: 25 months. Exclusions after randomizations: not reported. Analyses by protocol Losses to follow up: none. Jadad quality score: 3. | |
| Participants | Country: Germany. Setting: centre not specialized in hernia repair. Total enrolled patients: 160 (80 for each group) Mean age (SD): Shouldice 46 (15); Plug and Patch 47 (14). Gender:147 M, 13 F. Inclusion criteria: Primary inguinal hernia repair, age >18. Exclusion criteria: incarcerated hernias, coagulation disorders, contraindication for general anaesthesia, cardiac insufficiency (NYHA 3‐4). Demographic and baseline data: comparability for age, sex, type of hernia (Nyhus), occupation, BMI (all data reported). | |
| Interventions | Shouldice modified (n=80). 4 layers. Unabsorbable monofilament. Plug and Patch (n=80). Polypropylene meshes and plugs. | |
| Outcomes | Recurrence (method not stated). Lenght of postoperative stay. Chronic pain. Wound Infection. Seroma. Haematoma. Duration of operation. | |
| Notes | Recurrence at 25 months assessed for 96% of Shouldice group and 94% of Plug and Patch. Conflict of interest: not reported. Sources of funding: not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Aust 1993 | Comment to Kingsnorth 1992 |
| Bay‐Nielsen 2004 | Review |
| Bergin 1998 | Comparison about different suture materials |
| Carter 1993 | Comment to Kingsnorth 1992 |
| Cunningham 1996 | No comparisons between surgical techniques |
| Deysine 2006 | CCT |
| Kawji 1999 | CCT |
| Kingsnorth 1995 | Comment on Kingsnorth 1992 |
| Koninger 2004 | Data considered in Butters 2007 |
| Manson 1993 | Comment to Kingsnorth 1992 |
| Negro 1997 | Comment to Schrenk 1996 |
| Panos 1992 | Full text not available |
| Paul 1993 | Data reprised in Paul 1994 |
| Prieto‐Diaz‐Chavez 2009 | Data on primary inguinal hernia not extractable |
| Pyka 2003 | Full text not available |
| Stanislawek 2003 | Full text not available |
| Strand 1998 | Full text not available |
| Wayman 1996 | Out of topic |
| Woodward 1995 | Letter to Paul 1994 |
| Wyatt 1995 | Comment to Kingsnorth 1992 |
Characteristics of studies awaiting assessment [ordered by study ID]
Koninger 1998.
| Methods | RCT |
| Participants | 280 patients |
| Interventions | Shouldice, Lichtenstein, TAPP |
| Outcomes | Recurrence, Duration of Operation, Wound infection, Complications |
| Notes |
Kux 1994.
| Methods | RCT |
| Participants | 209 patients |
| Interventions | Shouldice, Lichtenstein |
| Outcomes | Recurrence, Postoperative pain |
| Notes |
Mittelstaedt 1999.
| Methods | RCT |
| Participants | 119 patients |
| Interventions | Shouldice, Bassini, Mc Vay |
| Outcomes | Recurrence |
| Notes |
Porrero 2005.
| Methods | RCT |
| Participants | 54 patients |
| Interventions | Shouldice, Lichtenstein |
| Outcomes | Duration of operation, Lenght of postoperative stay, Costs |
| Notes |
Schmitz 1997.
| Methods | RCT |
| Participants | 64 patients |
| Interventions | Shouldice, Tension‐free |
| Outcomes | Postoperative pain, Complications |
| Notes |
Contributions of authors
Bruno Amato worked on the whole project and coordinated the reviewers.
Corrado Rispoli and Nicola Rocco were involved in the review design and in writing the protocol, results, discussion, collection and interpreting the data.
Giovanni Persico and Salvatore Panico were involved with interpreting the data and commenting on the studies included.
Lorenzo Moja designed and wrote the review draft and was the supervisor for data collection and interpretation; he was also involved in data analyses.
Ivan Moschetti provided general advice on the review and contributed to the interpretation of data, commented on successive drafts of the manuscript and coordinated the review process.
Sources of support
Internal sources
No source of support received, Not specified.
External sources
No sources of support supplied
Declarations of interest
Corrado Rispoli, Nicola Rocco, Bruno Amato and Giovanni Persico are general surgeons; in their hospital they usually employ Trabucco or Lichtenstein techniques. Ivan Moschetti, Lorenzo Moja and Salvatore Panico are clinicians/researchers. None of them received grants from any pharmaceutical industry involved in mesh or other device production.
Stable (no update expected for reasons given in 'What's new')
References
References to studies included in this review
Barth 1998 {published data only}
- Barth RJ Jr, Burchard KW, Tosteson A, Sutton JE Jr, Colacchio TA, Henriques HF, et al. Short‐term outcome after mesh or Shoudice herniorrhaphy: a randomized, prospective study. Surgery 1998;123(2):121‐6. [PubMed] [Google Scholar]
Beets 1997 {published data only}
- Beets GL, Oosterhuis KJ, Go PMNYH, Baeten CGMI, Kootstra G. Longterm follow up (12‐15 years) of a randomized controlled trial comparing Bassini‐Stetten, Shouldice, and high ligation with narrowing of the internal ring for primary inguinal hernia repair. J Am Coll Surg 1997;185(4):352‐7. [PubMed] [Google Scholar]
Butters 2007 {published data only}
- Butters M, Redecke J, Koninger J. Long‐term results of a randomized clinical trial of Shouldice, Lichtenstein and transabdominal preperitoneal hernia repairs Br J Surg 2007;94(5):562‐5.. Br J Surg 2007;94(5):562‐5. [DOI] [PubMed] [Google Scholar]
Danielsson 1999 {published data only}
- Danielsson P, Isacson S, Hansen MV. Randomised study of Lichtenstein compared with Shouldice inguinal hernia repair by surgeons in training. Eur J Surg 1999;165(1):49‐53. [DOI] [PubMed] [Google Scholar]
Hay 1995 {published data only}
- Hay JM, Boudet MJ, Fingerhut A, Pourcher J, Hennet H, Habib E, et al. Shouldice inguinal hernia repair in the male adult: the gold standard? A multicenter controlled trial in 1578 patients. Ann Surg 1995;222(6):719‐27. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hetzer 1999 {published data only}
- Hetzer FH, Hotz T, Steinke W, Schlumpf R, Decurtins M, Largiader F. Gold standard for inguinal hernia repair: Shouldice or Lichtenstein?. Hernia 1999;3:117‐20. [Google Scholar]
Kingsnorth 1992 {published data only}
- Kingsnorth AN, Gray MR, Nott DM. Prospecitive randomized trial comparing the Shouldice and plication darn for inguinal hernia. Br J Surg 1992;79:1068‐70. [DOI] [PubMed] [Google Scholar]
Kovacs 1997 {published data only}
- Kovacs JB, Gorog D, Szabo J, Fehervari I, Jaray J, Perner F. Prospective randomized trial comparing Shouldice and Bassini‐Kirschner operation technique in primary inguinal hernia repair. Acta Chir Hung 1997;36(1‐4):179‐81. [PubMed] [Google Scholar]
Kux 1994b {published data only}
- Kux M, Fuchsjager N, Schemper M. Shouldice is superior to Bassini inguinal herniorrhaphy. Am J Surg 1994;168:15‐8. [DOI] [PubMed] [Google Scholar]
McGillicuddy 1998 {published data only}
- Gillicuddy JE, Nyhus LM. Prospective randomized comparison of the Shouldice and Lichenstein hernia repair procedures. Arch Surg 1998;133(9):974‐8. [DOI] [PubMed] [Google Scholar]
Miedema 2004 {published data only}
- Miedema BW, Ibrahim SM, Davis BD, Koivunen DG. A prospective trial of primary inguinal hernia repair by surgical trainees. Hernia 2004;8(1):28‐32. [DOI] [PubMed] [Google Scholar]
Nordin 2002 {published data only}
- Nordin P, Bartelmess P, Jansson C, Svensson C, Edlund G. Randomized trial of Lichtenstein versus Shouldice hernia repair in general surgical practice. Br J Surg 2002;89:45‐9. [DOI] [PubMed] [Google Scholar]
Paul 1994 {published data only}
- Paul A, Troidl H, Williams JI, Rixen D, Langen R, Cologne Hernia Study Group. Randomized trial of modified Bassini versus Shouldice inguinal hernia repair. Br J Surg 1994;81:1531‐4. [DOI] [PubMed] [Google Scholar]
Thapar 2000 {published data only}
- Thapar V, Rao P, Deshpande A, Sanghavi B, Supe AN. Shouldice herniorrhaphy versus Moloney's darn herniorrhaphy in young patients (a prospective randomised study). J Postgrad Med 2000;46(1):9‐12. [PubMed] [Google Scholar]
Tran 1992 {published data only}
- Tran VK, Putz T, Rohde H. A randomized controlled trial for inguinal hernia repair to compare the Shouldice and the Bassini‐Kirschner operation. Int Surg 1992;77:235‐7. [PubMed] [Google Scholar]
Zieren 1998 {published data only}
- Zieren J, Zieren HU, Jacobi CA, Wenger FA, Muller JM. Prospective randomized study comparing laparoscopic and open tension‐free inguinal hernia repair with Shouldice's operation. Am J Surg 1998;175:330‐3. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Aust 1993 {published data only}
- Aust JB. Prospective randomized trial comparing the Shouldice technique and plication darn for inguinal hernia. Br J Surg 1993;80(6):807. [DOI] [PubMed] [Google Scholar]
Bay‐Nielsen 2004 {published data only}
- Bay‐Nielsen M, Nilsson E, Nordin P, Kehlet H. Chronic pain after open mesh and sutured repair of indirect inguinal hernia in young males. Br J Surg 2004;91(10):1372‐6. [DOI] [PubMed] [Google Scholar]
Bergin 1998 {published data only}
- Bergin FG, Devlin HB, Gilliland EL. Shouldice inguinal hernia repair revisited: a prospective, randomized trial of non‐absorbable versus absorbable suture. Br J Surg 1998;85(Suppl 1):35. [Google Scholar]
Carter 1993 {published data only}
- Carter P. Prospective randomized trial comparing the Shouldice technique and plication darn for inguinal hernia. Br J Surg 1993;80(4):536. [PubMed] [Google Scholar]
Cunningham 1996 {published data only}
- Cunningham J, Temple WJ, Mitchell P, Nixon JA, Preshaw RM, Hagen NA. Cooperative hernia study. Pain in the post repair patient. Ann Surg 1996;224(5):598‐602. [DOI] [PMC free article] [PubMed] [Google Scholar]
Deysine 2006 {published data only}
- Deysine M. Inguinal herniorrhaphy: 25‐year results of technical improvements leading to reduced morbidity in 4,029 patients. Hernia 2006;10(3):207‐12. [DOI] [PubMed] [Google Scholar]
Kawji 1999 {published data only}
- Kawji R, Feichter A, Fuchsjager N, Kux M. Postoperative pain and return to activity after five different types of inguinal herniorrhaphy. Hernia 1999;3(1):31‐5. [Google Scholar]
Kingsnorth 1995 {published data only}
- Kingsnorth AN. Randomized trial of modified Bassini versus Shouldice inguinal hernia repair. Further comment. Br J Surg 1995;82(3):420‐1. [DOI] [PubMed] [Google Scholar]
Koninger 2004 {published data only}
- Koninger J, Redecke J, Butters M. Chronic pain after hernia repair: a randomized trial comparing Shouldice, Lichtenstein and TAPP. Langenbecks Arch Surg 2004 Oct;389(5):361‐5. [DOI] [PubMed] [Google Scholar]
Manson 1993 {published data only}
- Manson WG, Reed MW. Prospective randomized trial comparing the Shouldice technique and plication darn for inguinal hernia. Br J Surg 1993;80(4):536. [PubMed] [Google Scholar]
Negro 1997 {published data only}
- Negro P, Gossetti F, Catarci M. Prospective randomized trial comparing postoperative pain and return to physical activity after transabdominal preperitoneal, total preperitoneal or Shouldice technique for inguinal hernia repair. Br J Surg 1997;84(5):728‐9. [DOI] [PubMed] [Google Scholar]
Panos 1992 {published data only}
- Panos RG, Beck DE, Maresh JE, Harford FJ. Preliminary results of a prospective randomized study of Cooper's ligament versus Shouldice herniorrhaphy technique. Surg Gynecol Obstet 1992;175:315‐19. [PubMed] [Google Scholar]
Paul 1993 {published data only}
- Paul A, Troidl H, Rixen D, Williams J. Inguinal hernia surgery after Shouldice or Bassini: results of a controlled randomized trial. Langenbecks Archiv fur chirurgie 1993;suppl kongessbericht:302‐4. [Google Scholar]
Prieto‐Diaz‐Chavez 2009 {published data only}
- Prieto‐Diaz‐Chavez E, Medina‐Chavez JL, Anaya‐Prado R. A cost‐effectiveness analysis of tension‐free versus Shouldice inguinal hernia repair: a randomized double‐blind clinical trial. Hernia 2009;13:233‐8. [DOI] [PubMed] [Google Scholar]
Pyka 2003 {published data only}
- Pyka P, Grabowski K, Biernacki A, Dassbrowiecki S. Three‐ layer modification of Shouldice's method in the surgical treatment of inguinal hernias ‐ Its usefulness. Polski Przeglad Chirurgiczny 2003;75(9):858‐70. [Google Scholar]
Stanislawek 2003 {published data only}
- Stanislawek J, Gluszek S, Wysocki A, Dabrowiecki S. Comparison of the efficacy of inguinal hernia surgical treatment using Shouldice's and Prolene Hernia System methods. Polski Przeglad Chirurgiczny 2003;75(8):741‐57. [Google Scholar]
Strand 1998 {published data only}
- Strand L. Randomized trial of three types of repair used in 324 consecutive operation of hernia. A study of the frequency of recurrence. Ugeskrift for læger 1998;160(7):1010‐3. [PubMed] [Google Scholar]
Wayman 1996 {published data only}
- Wayman J, Ahmed SM, Stock SE. A study of postoperative pain in patients undergoing repair of inguinal hernia by the Lichtenstein and Shouldice techniques. Br J Surg 1996;83(Suppl 1):36. [Google Scholar]
Woodward 1995 {published data only}
- Woodward A, Carr ND, Beynon J. Randomized trial of modified Bassini versus Shouldice hernia repair. Br J Surg 1995; Vol. 82, issue 3:419‐20. [PubMed]
Wyatt 1995 {published data only}
- Wyatt JP, Kingsnorth AN, Gray MR, Nott D. Prospective randomized trial comparing the Shouldice technique and plication darn for inguinal hernia. Br J Surg 1993;80(3):403. [DOI] [PubMed] [Google Scholar]
References to studies awaiting assessment
Koninger 1998 {published data only}
- Koninger JS, Oster M, Butters M. Managemet of inguinal hernia ‐‐ a comparison of current methods. Der Chirurg 1998;69(12):1340‐4. [DOI] [PubMed] [Google Scholar]
Kux 1994 {published data only}
- Kux M, Fuchsjaeger N, Feichter A. Lichtenstein patch versus Shouldice technique in primary inguinal hernia with a high risk of recurrence. Chirurg 1994;65:59‐62. [PubMed] [Google Scholar]
Mittelstaedt 1999 {published data only}
- Mittelstaedt WE, Rodrigues Junior AJ, Duprat J, Bevilaqua RG, Birolini D. Treatment of inguinal hernias. Is the Bassani's technique current yet? A prospective, randomized trial comparing three operative techniques: Bassini, Shouldice and Mc Vay. Rev Ass Med Bras 1999;45(2):105‐14. [DOI] [PubMed] [Google Scholar]
Porrero 2005 {published data only}
- Porrero JL, Bonachia O, Lopez Buenadicha A, Sanjuanbenito A, Sanchez, Cabezudo C. Repair of primary inguinal hernia: Lichtenstein versus Shouldice techniques. Prospective randomized study of pain and hospital cost [Reparacion de la hernia inguinal primaria: Lichtenstein frente a Shouldice. Estudio prospectivo y aleatorizado sobre el dolor y los costes hospitalarios]. Cir Esp 2005;77(2):75‐8. [DOI] [PubMed] [Google Scholar]
Schmitz 1997 {published data only}
- Schmitz R, Treckmann J, Shah S, Schneidr K. "Tension‐free technique" in open inguinal hernia repair. A prospective, randomized study of postoperative pain perception ("tension‐free reconstruction" vs. Shouldice technique). Der Chirurg 1997;68(3):259‐63. [DOI] [PubMed] [Google Scholar]
Additional references
Altman 1998
- Altman DJ. Confidence intervals for the number needed to treat. BMJ 1998;317:1309‐12. [DOI] [PMC free article] [PubMed] [Google Scholar]
Arlt 2002
- Arlt G, Schumpelick V. The Shouldice repair for inguinal hernia‐technique and results. Zentralbl Chir 2002 Jul;127(7):565‐9. [DOI] [PubMed] [Google Scholar]
Arvidsson 2005
- Arvidsson D, Berndsen FH, Larsson LG, Leijonmarck CE, Rimback G, Rudberg C, Smedberg S, Spangen L, Montgomery A. Randomized clinical trial comparing 5‐year recurrence rate after laparoscopic versus Shouldice repair of primary inguinal hernia. Br J Surg 2005 Sep;92(9):1085‐91. [DOI] [PubMed] [Google Scholar]
Bassini 1887
- Bassini E. New method about radical treatment of inguinal hernia [Nuovo metodo sulla cura radicale dell'ernia inguinale.]. Arch Soc Ital Chir 1887;4:380. [Google Scholar]
Benard 1986
- Benard F, Chiotasso P, Legrand G, Lezorthes F. Inguinal hernia. The Shouldice parietal repair. Presse Med 1986 Jul 5‐12;15(27):1276‐80. [PubMed] [Google Scholar]
Bendavid 1997
- Bendavid R. Shouldice Herniotomy. Chirurg 1997 Oct;68(10):965‐9. [DOI] [PubMed] [Google Scholar]
CC Handbook 2008
- Higgins JPT, Green S (editors). Assessment of study quality. Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.1 [updated September 2008]; Part 2. The Cochrane Collaboration, 2008. Available from www.cochrane‐handbook.org. Sept 2008.
Deeks 2001
- Deeks JJ, Altman DG, Bradburn MJ. Statistical methods for examining heterogeneity and combining results from several studies in meta‐analysis. In: Egger M, Davey Smith G, Altman DG editor(s). Systematic reviews in health care: meta‐analysis in context. Second Edition. London: BMJ Books, 2001:285‐312. [Google Scholar]
Deeks 2006
- Deeks JJ, Higgins JPT, Altman DG, editors. Assessment of study quality. Cochrane Reviewers' Handbook 4.2.5 [updated May 2005]; Section 6. In: The Cochrane Library, Issue 1, 2006. Chichester, UK: John Wiley & Sons, Ltd..
DerSimonian 1986
- DerSimonian R, Laird N. Meta‐analysis in clinical trials. Controlled Clinical Trials 1986;7(3):177‐88. [DOI] [PubMed] [Google Scholar]
Devlin 1986
- Devlin HB, Gillen PH, Waxman BP, MacNay RA. Short stay surgery for inguinal hernia: experience of the Shouldice operation. Br J Surg 1986 Feb;73(2):123‐4. [DOI] [PubMed] [Google Scholar]
Fingerhut 1993
- Fingerhut A, Hay JM, Hennet H, Boudet MJ. Shouldice or not Shouldice? Late results of a controlled trial in 1593 patients. 7th annual meeting of the French Association for Surgical Research (ARC) and 1st French‐German joint meeting with the permanent working party on clinical studies (CAS ) of the German Surgical Society, March 1993, Paris France. Theor Surg. 1993; Vol. 8:163‐7.
Glassow 1986
- Glassow F. The Shouldice Hospital technique. Int Surg 1986;71:148‐53. [PubMed] [Google Scholar]
Grant 2002
- Grant AM, EU Hernia Trialists Collaboration. Open mesh versus non‐mesh repair of groin hernia: meta‐analysis of randomised trials based on individual patient data [corrected]. Hernia 2002;6(3):130‐6. [DOI] [PubMed] [Google Scholar]
Higgins 2002
- Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta‐analysis. Statistics in Medicine 2002;21:1539‐58. [DOI] [PubMed] [Google Scholar]
Higgins 2008
- Higgins JPT, Green S, Scholten RJPM. Chapter 3: Maintaining reviews: updates, amendments and feedback. In: Higgins JPT, Green S editor(s). Cochrane Handbook for Systematic Reviews of Interventions. The Cochrane Collaboration, September 2008. [Google Scholar]
Hoffmann 1991
- Hoffmann R, Frick T, Attinger B, Platz A, Largiader F. Bassini or Shouldice operation?. Helv Chir Acta 1991;58:207‐12. [PubMed] [Google Scholar]
Jadad 1996
- Jadad A, Moore R, Carroll D, Jenkinson C, Reynolds J, Gavaghan D, et al. Assessing the quality of reports of randomised clinical trials: is blinding necessary?. Controlled Clinical Trials 1996;17(1):1‐12. [DOI] [PubMed] [Google Scholar]
Lichtenstein 1987
- Lichtenstein IL. Herniorrhaphy. A personal experience with 6321 cases. Am J Surg 1987;153:553‐9. [DOI] [PubMed] [Google Scholar]
Lichtenstein 1989
- Lichtenstein IL, Schulman AG, Amid PK, Montllor MM. The tension‐free hernioplasty. Am J Surg 1989;157:188‐93. [DOI] [PubMed] [Google Scholar]
Mc Vay 1978
- Vay C. Hernia. 2nd Edition. JB Lippincott, 1978. [Google Scholar]
Moloney 1972
- Moloney GE. Darning inguinal hernias. Arch surg 1972;104(2):129‐130. [DOI] [PubMed] [Google Scholar]
Nilsson 1993
- Nilsson E, Anderberg B, Bragmark M, Erikson T, Fordell R, Haapaniemi S. Hernia surgery in a de.ned population. Improvements possible in outcome and cost effectiveness. Ambulatory Surg 1993;1:150‐3. [Google Scholar]
Oosterhuis 1986
- Oosterhuis KJ, Greep JM. Bassini or Shouldice, a comparative study on inguinal hernia repair. Tagung Vereinigung Niederrheinisch‐Westfaelischer Chirurgen Congres von Chirurgischer Lehrstuhl der Universitaet zu Koeln. 1986.
Rutkow 2003
- Rutkow IM. Demographic and socioeconomic aspects of hernia repair in the United States in 2003. Surg Clin North Am 2003 Oct;83(5):1045‐51. [DOI] [PubMed] [Google Scholar]
Schippers 1996
- Schippers E, Peiper C, Schumpelick V. Pro‐Shouldice: primary tension‐free hernia repair‐‐conditio sine qua non?. Swiss Surg 1996;Suppl 4:33‐6. [PubMed] [Google Scholar]
Schulz 1996
- Schulz KF, Grimes DA, Altman DG, Hayes RJ. Blinding and exclusions after allocation in randomised controlled trials: survey of published parallel group trials in obstetrics and gynaecology. BMJ 1996;312:742‐744. [DOI] [PMC free article] [PubMed] [Google Scholar]
Schumpelick 1994
- Schumpelick V, Treutner KH, Arlt G. Inguinal hernia repair in adults. Lancet 1994;344:375‐9. [DOI] [PubMed] [Google Scholar]
Scott 2001
- Scott N, Go PMNYH, Graham P, McCormack K, Ross SJ, Grant AM. OpenMesh versus non‐Mesh for groin hernia repair. Cochrane Database of Systematic Reviews 2001, Issue 3. [DOI: 10.1002/14651858.CD002197] [DOI] [Google Scholar]
Shouldice 1945
- Shouldice EE. Surgical treatment of hernia. Ont Med Rev 1945;4:43. [Google Scholar]
SHR 2002
- Swedish Hernia Register. Swedish Hernia Register (Svenska Brackregistret). 2002 May. [http://www.sos.se/mars/kva002/kva002.htm/ [3 March 2003]]
Simons 1996
- Simons MP, Kleijnen J, Geldere D, Hoitsma HFW, Obertop H. Role of the Shouldice technique in inguinal hernia repair: a systematic review of controlled trials and a meta‐analysis. British Journal of Surgery 1996;83:734‐738. [DOI] [PubMed] [Google Scholar]
Smythe 1977
- Smythe HA, Helewa A, Goldsmith CH. "Independent assessor" and "pooled index" as techniques for measuring treatment effects in rheumatoid arthritis. J Rheumatol 1977;4(2):144‐52. [PubMed] [Google Scholar]
Thompson 2001
- Thompson SG. Why and how sources of heterogeneity should be investigated. In: Egger M, Davey Smith G, Altman DG editor(s). Systematic reviews in health care: meta‐analysis in context. Second Edition. London: BMJ Books, 2001:157‐75. [Google Scholar]
Tons 1991
- Tons C, Klinge U, Kupczyk‐Joeris D, Rotzscher VM, Schumpelick V. Controlled study of cremaster resection in Shouldice repair of primary inguinal hernia. Zentralblatt für Chirurgie 1991;116:737‐43. [PubMed] [Google Scholar]
Wantz 1989
- Wantz GE. The Canadian repair: personal observations. World J Surg 1989;13:516‐21. [DOI] [PubMed] [Google Scholar]