

Abstract
Corrosive ingestion is a common form of poisoning. Corrosive agents cause severe damage to the gastrointestinal (GI) tract. The most severe forms of injury can lead to mortality; however, the major concern with this type of injury is life-long morbidity. Upper GI endoscopy is the test of choice for assessing severity in the acute phase of the disease. The long-term management is based on the site, length, number, location, and tightness of the stricture. This information is best provided by the barium contrast studies. In this pictorial review, a spectrum of findings in patients with corrosive injuries of the esophagus and stomach is illustrated. The role of various imaging modalities including barium studies, endoscopic ultrasound, computed tomography, and magnetic resonance imaging is discussed.
Keywords: Barium, corrosive, stricture
Introduction
Corrosives can damage any segment of the gastrointestinal (GI) tract. However, it most commonly affects the upper GI tract comprising oropharynx, larynx, esophagus, and stomach.[1] Corrosive injuries of the GI tract are seen in accidental or suicidal intake of acids or alkalis. Accidental intake is more commonly seen in children, whereas the suicidal intent is the usual cause in adults.[2,3,4] Overall, the corrosive injuries of the upper GI tract are more often seen in the developing countries.[5,6] For a long time, it was believed that the acids cause more damage to the gastric mucosa, whereas alkalis have a tendency for greater damage to the esophageal mucosa.[7] However, it is now known that these agents cause mucosal injuries in both the organs with no selective preference.[8,9,10] Acidic agents, frequently responsible, are the ones that are commonly available such as cleaning agents (hydrochloric acid) and a gold solvent, which is a mixture of hydrochloric and nitric acid (aqua regia).[11] Alkalis commonly used are hydroxides of sodium and potassium. The mechanism of acidic and alkaline injury is coagulation necrosis and liquefactive necrosis, respectively. Injuries due to corrosives can be restricted to the esophagus or stomach. Coexistent esophageal and gastric injuries are seen in 20%–62.5% cases.[9,12,13]
Pathology
The acute phase of the disease (an initial couple of days) shows necrosis, small vessel thrombosis, and sloughing of the mucosa. This is followed by bacterial invasion and migration of fibroblasts (4–7 days). Collagen deposits are seen beyond 2 weeks. Scar retraction begins by the third week, which eventually leads to strictures.[13] The esophageal layer involved in fibrosis is determined by the depth of injury caused by the caustic substance. These patients may have repeated small ulcers due to minor traumas caused by food, which subsequently heal by re-epithelialization leading to further narrowing of the lumen. Such episodes may cause recurrence of symptoms after dilatation.[14]
Clinical Features
The acute phase of corrosive injuries involves perforation of the esophagus, stomach, or duodenum. Chronic phase of corrosive injuries may result in several complications, most common among them is a stricture. Esophageal strictures cause dysphagia.[13] However, the patients are usually not symptomatic when the lumen of the esophagus remains >10 mm.[15] In a study by Mamede et al., it was observed that 89.3% of patients developed esophagitis following corrosive intake and about 1% died during the acute phase. About 72.6% of patients progressed to strictures causing luminal stenosis.[14] Gastric involvement can lead to achlorhydria, outlet obstructions, and rarely carcinomas. Gastric outlet obstructions are much less common than esophageal strictures, constituting about 5% of all corrosive injuries.[13]
Imaging Features
Plain radiograph
A plain chest radiograph may demonstrate pneumomediastinum suggesting esophageal perforation. There may be free air under the diaphragm suggesting gastric perforation. In these situations, a water-soluble contrast agent is preferred for an esophagogram. More subtle signs of upper GI injury may include mucosal thickening, nodularity. In more severe cases, intramural air may be seen.
Upper GI endoscopy
Upper GI endoscopy (UGIE) is usually carried out during the first 2 days of the injury. However, it can be safely carried out up to 4 days from the time of injury, usually under general anesthesia, with minimal insufflation of air. Risk of perforation is higher in endoscopies performed later on, between 5 and 15 days, due to friable healing mucosa[15,16] Mucosal injuries can be better evaluated using endoscopy than with computed tomography (CT).[17] In cases where perforation is suspected or in patients with supraglottic airway edema or third-degree hypopharyngeal burns, UGIE is avoided as it may worsen the airway obstruction.[2] Endoscopic grading of corrosive injuries holds prognostic significance and also guides management. Chronic complications are not usually seen in cases of grade 0 and 1 injuries.[2] There is ninefold increase in morbidity and mortality with each increase in grade.[15] Endoscopic grades 1, 2, and 2A are considered as “low-grade”injuries, whereas injuries falling into grades 2B, 3, and 4 are categorized as “high-grade” injuries.[15] High-grade injuries are more likely to develop chronic complications, such as esophageal strictures and gastric outlet obstruction. Further, the complications are likely to be higher in Grade 3 injuries as compared with grade 2B.[18] About 80% patients with Grade 3 injuries are likely to develop strictures.[19]
Barium Study
UGIE is a very useful tool in acute stage to assess the severity. Radiographs and water-soluble oral contrast studies may be helpful in detecting the perforations.[8] Barium swallow and barium meal are reliable tests to assess the length, number, and extent of the upper GI stricture in subacute and chronic stages.[8,9] Usually, barium studies are carried out after 3 weeks of corrosive intake.[7]
Esophageal strictures
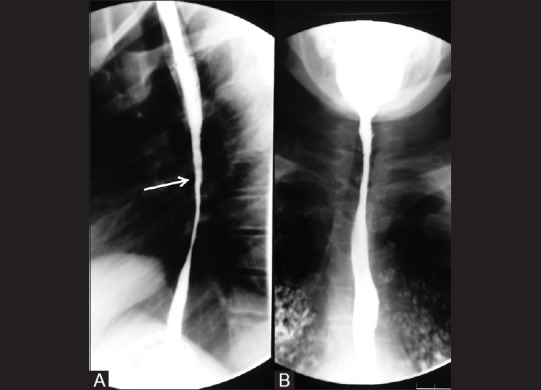
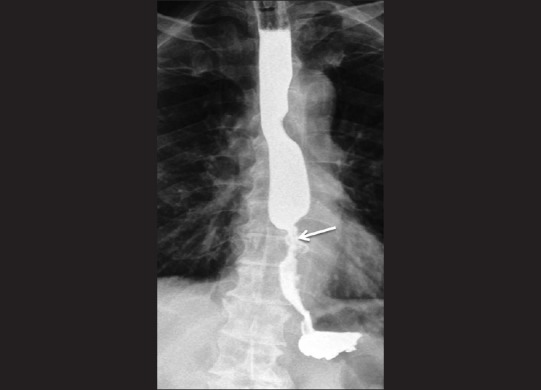
Esophageal strictures due to corrosives usually cause smooth concentric narrowing of the lumen in the affected segments, with tapered proximal and distal margins [Figure 1]. In comparison to this, malignant strictures usually cause irregularly narrowed lumen with an abrupt shelf at the proximal and distal margins.[8,20,21] Strictures which show typical benign appearance with the previous history of corrosive intake do not need to be evaluated further with endoscopic biopsy.[21] Corrosive strictures may affect a short segment of the esophagus (~1cm) [Figure 2] or may involve long segments [Figure 3], affecting almost the entire esophagus with or without gastric involvement.[8] Strictures can be single or multiple [Figure 4].[22] Very short segment strictures in the cervical esophagus may resemble webs [Figure 5] and the ones at the gastroesophageal junction may mimic primary achalasia[Figure 6]. In a study by Gundogdu et al., 40.6% of esophageal strictures were seen in the upper third, 23.8% involved the mid-third, and 23.3% affected the lower third. In 12.4%cases, the entire esophagus was affected. Esophageal narrowing is seen more commonly in the upper third among the children, whereas it is seen more often in the mid and distal third in the adults.[14,23]
Figure 1.

Typical esophageal corrosive stricture: there is a smooth symmetrical mid-esophageal stricture (arrow)
Figure 2.

Short-segment stricture: there is a short segment stricture involving the cervical esophagus (arrow)
Figure 3 (A and B).
Long-segment stricture: two different patients with long-segment involvement. (A) shows the involvement of thoracic esophagus and (B) shows the involvement of cervical esophagus
Figure 4.

Multiple strictures: there are multiple strictures involving the cervical and upper thoracic esophagus (arrows)
Figure 5.

Web-like stenosis: there is a web-like narrowing of the cervical esophagus (arrow)
Figure 6.

Stricture mimicking achalasia: there is a short-segment stricture involving the gastroesophageal junction (arrow) with marked dilatation of the proximal esophagus resembling achalasia
Gastric strictures
Gastric strictures can be classified into five types as follows:[11]
Short ring stricture within 1–2cm of the pylorus.
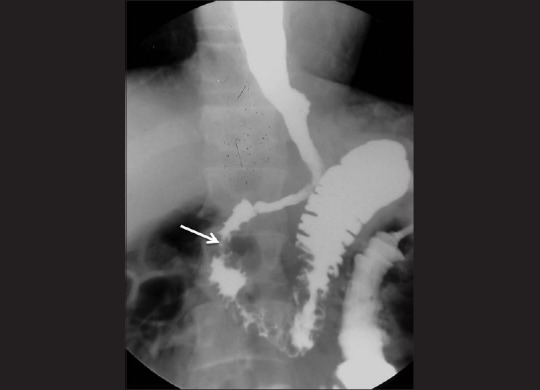
Strictures extending upto the antrum [Figure 7].
Strictures involving the body of the stomach (mid-part)[Figure 8].
Linitis plastica due to diffuse gastric involvement [Figure 9].
Strictures involving the stomach and the first part of the duodenum [Figure 10].
Figure 7.

Stenosis of antropyloric region: there is stenosis involving antropyloric region (arrow)
Figure 8.

Involvement of the body of stomach: there is a narrowing of the body of the stomach (arrow). Also, note the involvement of the duodenum with multiple pseudodiverticula (short arrows)
Figure 9.
Gastric contraction: there is a marked reduction in the entire gastric volume (arrows) with linitis-plastica-like appearance
Figure 10.

Stricture of the antropyloric region and duodenum: there is a long-segment narrowing of the antropyloric region and the first part of the duodenum (arrow)
Acids usually accumulate in the prepyloric segment of the stomach. They induce an intense pylorospasm, resulting in the stasis of the agent at the level of antrum. This may result in stricture due to prolonged contact.[8,24] Antropyloric narrowing is the most frequent site of gastric narrowing following corrosive intake. This may result in gastric outlet obstruction. However, gastric outlet obstruction is much less common as compared with corrosive esophageal strictures. In a few cases, they may become obvious after dilatation of the esophageal strictures, as a result of improved food intake.[7] Acids can result in strictures of any part of the stomach depending upon the quantity of intake. In patients who have consumed large volumes of acid, there can be involvement of body and fundus too. This can cause a marked reduction in the gastric volume with cicatrization, giving an appearance of linitis plastica.[2,5] Irregularities and shortening of the lesser curvature and hourglass deformities can also be seen following corrosive intake.[7]
Uncommon imaging features
Intramural diverticulae of the esophagus and stomach, tracheoesophageal fistula, gastro-colic fistula, aorto-enteric fistula, and esophageal carcinoma are the other well known, though rare complications following corrosive esophageal injury.[3,22,23] Intramural esophageal diverticulae are multiple tiny flask-shaped outpouchings in the wall of the esophagus which show pooling of contrast within [Figure 11].[25,26,27] Sometimes, there may be large sacculations or diverticulae in the esophagus or stomach [Figure 12]. Localized perforation (with a tract in the wall or adjoining mediastinum) without communication with adjacent hollow viscus is another manifestation [Figure 13]. Esophageal cancer is more frequent in the patients with caustic GI injuries than in the general population. The average duration between caustic damage and cancer is about 40 years.[3,14] Carcinoma developing in the background of a corrosive stricture leads to irregular narrowing of lumen resembling carcinomas occurring in the general population[Figure 14].[8] Status of malignant-appearing strictures and radiologically equivocal strictures needs to be confirmed by endoscopic biopsies.[20] A few reports of gastric carcinoma have also been reported in individuals with a past history of corrosive gastric strictures. However, unlike esophageal cancer, the etiological relationship between gastric cancer and corrosive gastric injury has not been well established.[8]
Figure 11.
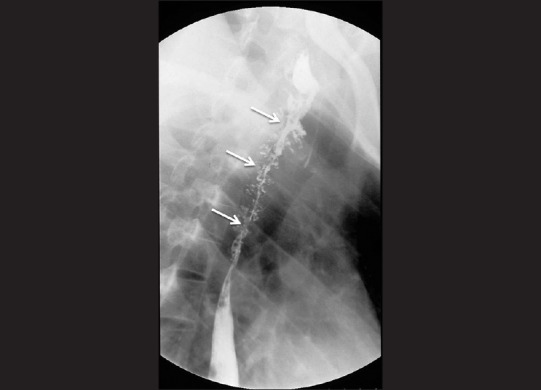
Intramural esophageal diverticula: there is a long-segment narrowing of the mid-thoracic esophagus with intramural diverticula along the entire length (arrow)
Figure 12.

Sacculation: there are multiple sacculations along the mid-thoracic esophagus (arrows)
Figure 13.

Intramural contrast leak: there is a long contrast filled tract extending along the posterior aspect of the cervical and upper thoracic esophagus
Figure 14.
Corrosive ingestion associated esophageal cancer: there is an asymmetrical stricture with ulceration involving the lower thoracic esophagus (arrow)
Computed Tomography
CT scan has several advantages in cases of corrosive injuries. CT is available in most centers. It is cost effective, noninvasive, and helps in assessing the length of involvement of the strictured segment of esophagus and stomach.[17] In cases of threatened perforation or existing perforation, CT is the investigation of choice.[5] It can also be useful to evaluate the extra GI involvement in corrosive injuries.[17] Preoperatively CT angiography is used for evaluation of vascular anatomy. CT scan can be used in the early stages of corrosive injuries to assess the degree of injury[Figures 15 and 16]. In the study by Motlagh et al., the sensitivity and specificity of CT in detection of esophageal damage were 96.29% and 57.14%, respectively.[17] Another study by Lurie et al. showed that CT had a high specificity (>90%) and low sensitivity (~30% to 40%) in predicting the need for surgical intervention as well as eventual mortality.[28] Hence, it cannot replace endoscopy in the early stage of disease.[17,28] However, in the study by Ryu et al., it was demonstrated that CT scan in the early stage can accurately predict the development of esophageal stricture with a larger area under the receiver operating characteristic curve.[29]
Figure 15.

Corrosive injury of the esophagus: computed tomography (CT): axial and coronal reformatted CT images show smooth circumferential wall thickening of the mid and distal esophagus (arrows)
Figure 16.
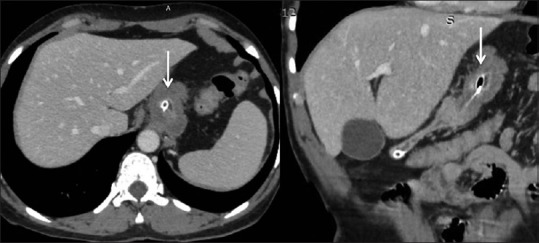
Corrosive injury of the stomach: computed tomography (CT): axial and coronal reformatted CT images show diffuse circumferential wall thickening of the stomach with marked volume loss
CT grading of corrosive esophageal injury is as follows:[29]
Grade I: No definite thickening of esophagus wall (maximum thickness of 3 mm-normal range).
Grade II: Edematous thickening of the wall (>3mm) without periesophageal soft tissue infiltration.
Grade III: Edematous thickening of the wall (>3mm) with periesophageal soft tissue infiltration and well-demarcated tissue interface.
Grade IV: Edematous thickening of the wall with periesophageal soft tissue infiltration and blurring of tissue interfaces/localized adjacent fluid collections.
Endoscopy and Endoscopic Ultrasound
A few studies have evaluated the role of endoscopic ultrasound (EUS) in corrosive injuries. No significant advantage of EUS over conventional endoscopy has been noted in predicting acute complications.[30] However, EUS may be useful in predicting stricture formation. Patients with involvement of the muscularis propria are more likely to develop strictures and are likely to require more sessions of dilatation [Figure 17].[2,31]
Figure 17.
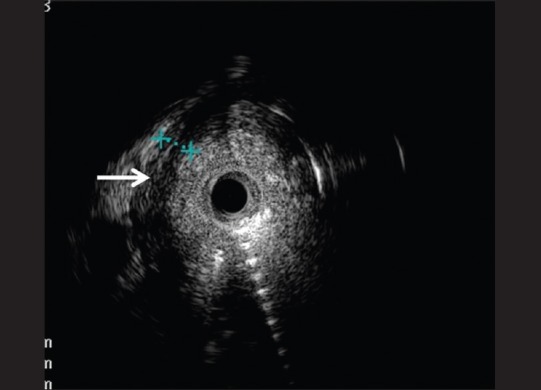
Corrosive injury of the esophagus: endoscopic ultrasound (EUS):radial EUS image shows asymmetric mural thickening of the esophagus. Note significantly thickened and hypoechoic muscularis propria (cursors and arrow)
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) does not have significant benefits over CT in cases of corrosive injuries. Obvious advantage of MRI is the lack of radiation. However, disadvantages are its limited availability, cost, poor evaluation of mucosal involvement, and long duration of the study, which may not be practical in sick and uncooperative patients.[31] No studies have evaluated the role of MRI in evaluation of corrosive esophageal injuries. However, it may be hypothesized that it can show the degree of submucosal involvement, hence predicting response to endoscopic dilatation [Figure 18].
Figure 18.
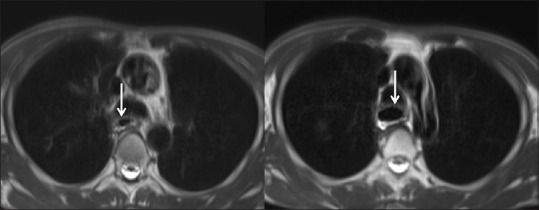
Corrosive injury of the esophagus: magnetic resonance imaging: axial T2-weighted images show mild narrowing in the mid-thoracic esophagus (left arrow) with upstream dilatation (right arrow)
Differential diagnosis of corrosive esophageal strictures
Mediastinal irradiation: Most radiation strictures occur in the upper or midesophagus. These appear as smooth, relatively long segments of concentric, tapered narrowing.[32]
Drug ingestion: Tetracycline and doxycycline are the two agents most commonly responsible for drug-induced esophagitis; however, as the ulceration is superficial, stricture formation is rare. On the other hand, drugs including quinidine, alendronate, potassium chloride, aspirin, and nonsteroidal anti-inflammatory agents may result in larger areas of ulceration and the development of strictures. These strictures are usually located in the upper or mid esophagus. The barium examination reveals these strictures as segmental areas of concentric narrowing.[33]
Skin diseases: Skin disorders such as epidermolysis bullosa dystrophica, benign mucous membrane pemphigoid, and erythema multiforme major may rarely be associated with upper or mid-esophageal stricture. These strictures appear as one or more segments of concentric or asymmetric narrowing.[34]
Esophageal intramural pseudodiverticula: Some patients with this condition may develop strictures in the upper or midesophagus. These strictures may have a variable length. These strictures are associated with pseudodiverticula that usually extend a considerable distance above and below the level of the strictures.[35]
Other unusual causes of strictures that may mimic corrosive strictures include tubercular esophagitis, Crohn disease, candida esophagitis, graft-versus-host disease, and eosinophilic esophagitis.[20]
An accurate diagnosis may be achieved by a detailed history and evaluation of barium signs.
Imaging features predicting response to endoscopic dilatation
Barium study: Length of stricture, tightness of stricture, and number of strictures have been shown to predict the response to endoscopic dilatation. The greater the length, tightness, and number of strictures, poorer is the response.[7]
CT: maximum esophageal wall thickness (EWT) has been reported in one study to predict the response to endoscopic dilatation.[7] A greater degree of EWT is predictive of poor response.
EUS: Involvement of muscularis propria predicts poor response and greater number of session of endoscopic dilatation.[31]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Kluger Y, Ishay OB, Sartelli M, Katz A, Ansaloni A, Gomez CA, et al. Caustic ingestion management: World society of emergency surgery preliminary survey of expert opinion. World J Emerg Surg. 2015;10:48. doi: 10.1186/s13017-015-0043-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Contini S, Scarpignato C. Caustic injury of the upper gastrointestinal tract: A comprehensive review. World J Gastroenterol. 2013;19:3918–30. doi: 10.3748/wjg.v19.i25.3918. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Gumaste VV, Dave PB. Ingestion of corrosive substances by adults. Am J Gastroenterol. 1992;87:1–5. [PubMed] [Google Scholar]
- 4.Lakshmi CP, Vijayahari R, Kate V, Ananthakrishnan N. A hospital-based epidemiological study of corrosive alimentary injuries with particular reference to the Indian experience. Natl Med J India. 2013;26:31–6. [PubMed] [Google Scholar]
- 5.Ananthakrishnan N, Parthasarathy G, Kate V. Acute corrosive injuries of the stomach: A single unit experience of thirty years. ISNR Gastroenterol. 2011;2011:914013. doi: 10.5402/2011/914013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ramasamy K, Gumaste VV. Corrosive ingestion in adults. J Clin Gastroenterol. 2003;37:119–24. doi: 10.1097/00004836-200308000-00005. [DOI] [PubMed] [Google Scholar]
- 7.Lahoti D, Broor SL. Corrosive injury to the upper gastrointestinal tract. Indian J Gastroenterol. 1993;12:135–41. [PubMed] [Google Scholar]
- 8.Nagi B, Kochhar R, Thapa BR, Singh K. Radiological spectrum of late sequelae of corrosive injury to upper gastrointestinal tract. A pictorial review. Acta Radiol. 2004;45:7–12. doi: 10.1080/02841850410003329. [DOI] [PubMed] [Google Scholar]
- 9.Zargar SA, Kochhar R, Nagi B, Mehta S, Mehta SK. Ingestion of corrosive acids: Spectrum of injury to upper gastrointestinal tract and natural history. Gastroenterology. 1989;97:702–7. [PubMed] [Google Scholar]
- 10.Zargar SA, Kochhar R, Nagi B, Mehta S, Mehta SK. Ingestion of strong corrosive alkalis: Spectrum of injury to upper gastrointestinal tract and natural history. Am J Gastroenterol. 1992;87:337–41. [PubMed] [Google Scholar]
- 11.Ananthakrishnan N, Parthasarathy G, Kate V. Chronic corrosive injuries of the stomach-a single unit experience of 109 patients over thirty years. World J Surg. 2010;34:758–64. doi: 10.1007/s00268-010-0393-8. [DOI] [PubMed] [Google Scholar]
- 12.Postlethwait RW. Chemical burns of the esophagus. Surg Clin North Am. 1983;63:915–24. doi: 10.1016/s0039-6109(16)43092-6. [DOI] [PubMed] [Google Scholar]
- 13.Meena BL, Narayan KS, Goyal G, Sultania S, Nijhawan S. Corrosive injuries of the upper gastrointestinal tract. J Dig Endosc. 2017;8:165–9. [Google Scholar]
- 14.Mamede RC, de Mello Filho FV. Ingestion of caustic substances and its complications. Sao Paulo Med J. 2001;119:10–5. doi: 10.1590/S1516-31802001000100004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Zargar SA, Kochhar R, Mehta S, Mehta SK. The role of fiberoptic endoscopy in the management of corrosive ingestion and modified endoscopic classification of burns. Gastrointest Endosc. 1991;37:165–9. doi: 10.1016/s0016-5107(91)70678-0. [DOI] [PubMed] [Google Scholar]
- 16.Chiu HM, Lin JT, Huang SP, Chen CH, Yang CS, Wang HP. Prediction of bleeding and stricture formation after corrosive ingestion by EUS concurrent with upper endoscopy. Gastrointest Endosc. 2004;60:827–33. doi: 10.1016/s0016-5107(04)02031-0. [DOI] [PubMed] [Google Scholar]
- 17.Bahrami-Motlagh H, Hadizadeh-Neisanghalb M, Peyvandi H. Diagnostic accuracy of computed tomography scan in detection of upper gastrointestinal tract injuries following caustic ingestion. Emerg (Tehran) 2017;5:e61. [PMC free article] [PubMed] [Google Scholar]
- 18.Lu L-S, Tai W-C, Hu M-L, Wu K-L, Chiu Y-C. Predicting the progress of caustic injury to complicated gastric outlet obstruction and esophageal stricture, using modified endoscopic mucosal injury grading scale. Biomed Res Int. 2014;2014:919870. doi: 10.1155/2014/919870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Cheng H-T, Cheng C-L, Lin C-H, Tang J-H, Chu Y-Y, Liu N-J, et al. Caustic ingestion in adults: The role of endoscopic classification in predicting outcome. BMC Gastroenterol. 2008;8:31. doi: 10.1186/1471-230X-8-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Luedtke P, Levine MS, Rubesin SE, Weinstein DS, Laufer I. Radiologic diagnosis of benign esophageal strictures: A pattern approach. RadioGraphics. 2003;23:897–909. doi: 10.1148/rg.234025717. [DOI] [PubMed] [Google Scholar]
- 21.Gupta S, Levine MS, Rubesin SE, Katzka DA, Laufer I. Usefulness of barium studies for differentiating benign and malignant strictures of the esophagus. Am J Roentgenol. 2003;180:737–44. doi: 10.2214/ajr.180.3.1800737. [DOI] [PubMed] [Google Scholar]
- 22.Franken EA. Caustic damage of the gastrointestinal tract: Roentgen features. Am J Roentgenol Radium Ther Nucl Med. 1973;118:77–85. doi: 10.2214/ajr.118.1.77. [DOI] [PubMed] [Google Scholar]
- 23.Gündoǧdu HZ, Tanyel FC, Büyükpamukçu N, Hiçsönmez A. Colonic replacement for the treatment of caustic esophageal strictures in children. J Pediatr Surg. 1992;27:771–4. doi: 10.1016/s0022-3468(05)80114-9. [DOI] [PubMed] [Google Scholar]
- 24.Chaudhary A, Puri AS, Dhar P, Reddy P, Sachdev A, Lahoti D, et al. Elective Surgery for Corrosive-Induced Gastric Injury. World J Surg. 1996;20:703–6. doi: 10.1007/s002689900107. [DOI] [PubMed] [Google Scholar]
- 25.Kochhar R, Mehta SK, Nagi B, Goenka MK. Corrosive acid-induced esophageal intramural pseudodiverticulosis a study of 14 patients. J Clin Gastroenterol. 1991;13:371–5. doi: 10.1097/00004836-199108000-00002. [DOI] [PubMed] [Google Scholar]
- 26.Keh SM, Onyekwelu N, McManus K, McGuigan J. Corrosive injury to upper gastrointestinal tract: Still a major surgical dilemma. World J Gastroenterol. 2006;12:5223–8. doi: 10.3748/wjg.v12.i32.5223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Levine M, Moolten D, Herlinger H, Laufer I. Esophageal intramural pseudodiverticulosis: A re-evaluation. Am J Roentgenol. 1986;147:1165–70. doi: 10.2214/ajr.147.6.1165. [DOI] [PubMed] [Google Scholar]
- 28.Lurie Y, Slotky M, Fischer D, Shreter R, Bentur Y. The role of chest and abdominal computed tomography in assessing the severity of acute corrosive ingestion. Clin Toxicol (Phila) 2013;51:834–7. doi: 10.3109/15563650.2013.837171. [DOI] [PubMed] [Google Scholar]
- 29.Ryu HH, Jeung KW, Lee BK, Uhm JH, Park YH, Shin MH, et al. Caustic injury: Can CT grading system enable prediction of esophageal stricture? Clin Toxicol (Phila) 2010;48:137–42. doi: 10.3109/15563650903585929. [DOI] [PubMed] [Google Scholar]
- 30.De Lusong MAA, Timbol ABG, Tuazon DJS. Management of esophageal caustic injury. World J Gastrointest Pharmacol Ther. 2017;8:90–8. doi: 10.4292/wjgpt.v8.i2.90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Rana SS, Bhasin DK, Singh K. Role of endoscopic ultrasonography (EUS) in management of benign esophageal strictures. Ann Gastroenterol. 2011;24:280–4. [PMC free article] [PubMed] [Google Scholar]
- 32.Lepke RA, Libshitz HI. Radiation-induced injury of the esophagus. Radiology. 1983;148:375–8. doi: 10.1148/radiology.148.2.6867327. [DOI] [PubMed] [Google Scholar]
- 33.Bonavina L, DeMeester TR, McChesney L, Schwizer W, Albertucci M, Bailey RT. Drug-induced esophageal strictures. Ann Surg. 1987;206:173–83. doi: 10.1097/00000658-198708000-00010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Tishler JM, Han SY, Helman CA. Esophageal involvement in epidermolysis bullosa dystrophica. AJR Am J Roentgenol. 1983;141:1283–6. doi: 10.2214/ajr.141.6.1283. [DOI] [PubMed] [Google Scholar]
- 35.Cho SR, Sanders MM, Turner MA, Liu CI, Kipreos BE. Esophageal intramural pseudodiverticulosis. Gastrointest Radiol. 1981;6:9–16. doi: 10.1007/BF01890214. [DOI] [PubMed] [Google Scholar]