

Abstract
Growing evidence suggests that maltreatment is reproduced across generations as victims of maltreatment are at an increased risk for maltreatment perpetration. Unfortunately, little information about mediating pathways exists to provide an explanation for why maltreatment begets maltreatment. We use the number of types of maltreatment experienced to predict later maltreatment perpetration and then examine two developmental pathways that may serve as bridges between maltreatment victimization and perpetration: adolescent problem behaviors and precocious transitions to adulthood. With prospective, longitudinal data from the Rochester Youth Development Study, we assess the relevance of these pathways for the number of maltreatment experiences as well as the number of maltreatment victimization experiences by developmental period (i.e., childhood and adolescence). Our results demonstrate a significant relationship between maltreatment victimization and maltreatment perpetration. Adolescent delinquency and two precocious transitions, dropping out of school and independent living, as well as the accumulation of precocious transitions and problem behaviors, serve as mediators of this intergenerational relationship. Furthermore, the relationship between the number of types of maltreatment and subsequent perpetration is primarily driven by experiences of maltreatment during adolescence. We discuss the implications of these results and set an agenda for the development of programs and policies to interrupt the cycle of maltreatment.
The primary responsibility of parents and guardians is to provide a safe, stable, and nurturing environment for youth. Safety is the extent to which a child is free from fear and from physical or psychological harm; stability is the degree of predictability and consistency in the child’s social, emotional, and physical environment, and nurturing is the extent to which a person is available to sensitively respond to the needs of the child (Mercy & Saul, 2009). These essential ingredients for a child’s healthy growth and development help to ensure the successful socialization of the next generation and, as noted by the Institute of Medicine and National Research Council (2014, p. 1): “it is in the national interest to have healthy children. Healthy children are … more likely to become healthy adults who contribute … to the continued vitality of society.”
Most parents and guardians exhibit appropriate and effective skills that yield safe, stable, and nurturing environments for youth. Unfortunately though, not all parents and care-givers have the resources necessary to create safe, stable, and nurturing environments for children, which can negatively affect the next generation through inappropriate parenting and caregiving behaviors. At the end of the continuum of negative parenting and caregiving lies a set of behaviors that are so extreme and inappropriate as to be criminalized. Identified as child maltreatment, it is defined as “any recent act or set of acts or failure to act on the part of a parent or caretaker, which results in death, serious physical or emotional harm, sexual abuse or exploitation, or an act or failure to act, which presents an imminent risk of serious harm” (42 U.S.C. § 101 note). The most common type of maltreatment is neglect, followed by physical abuse, psychological abuse, and sexual abuse (Institute of Medicine and National Resource Council, 2014). Although representing somewhat distinct forms of maltreatment, these types of abuse often co-occur within the same family and even within the same incident (also referred to as multitype abuse; US Department of Health and Human Services, 2012).
Research indicates that maltreatment has particularly pernicious consequences for development (Cicchetti & Toth, 2005; Institute of Medicine and National Resource Council, 2014). Being a victim of maltreatment is associated with negative consequences ranging from compromised cognitive functioning and brain development (Shonkoff, Boyce, & McEwen, 2009) to short- and long-term behavioral problems (Gilbert et al., 2009). Moreover, some work suggests that the number of maltreatment types is a critically important factor with respect to a victim’s psychological and social functioning (e.g., internalizing and externalizing symptoms and trauma symptomology; Clemmons, Walsh, DiLillo, & Messman-Moore, 2007; English et al., 2005; Teicher, Samson, Polcari, & McGreenery, 2006). Overall, maltreatment victimization poses serious consequences for affected children and families, as well as for society at large. With the total lifetime economic costs of new maltreatment cases (both fatal and nonfatal) estimated to be as high as $124 billion per year in the United States (Fang, Brown, Florence, & Mercy, 2012), it is obviously in the interest of everyone (the child, the family, and society at large) to minimize its occurrence.
In order to effectively prevent the occurrence of maltreatment, however, we first need to understand its origins. Given that most manifestations of maladaptation, including child maltreatment perpetration, have origins in childhood and adolescence, the purpose of this paper is to explore the etiologic pathways from earlier stages of development to maltreatment perpetration (see Cicchetti, 2004; Hinshaw, 2013). In particular, we focus on a history of maltreatment victimization, in particular victimization specific to childhood and to adolescence, as starting points for atypical development that will increase the likelihood of later maltreatment perpetration. In doing so, we investigate the proximal consequences associated with child maltreatment, which indicate impairments in several life domains, and explore whether these consequences are also potential developmental processes that increase the likelihood that a parent, guardian, or caretaker will engage in maltreating behaviors.1
The Cycle of Maltreatment
It is often hypothesized that maltreatment is reproduced across the generations. This expectation is consistent with the life course concept of interdependent or linked lives: “Each generation is bound to fateful decisions and events in the other’s life course” (Elder, 1985, p. 40). In this case, generations become linked with respect to a maladaptive pattern of parent–child interactions. Experiencing maltreatment both models the behavior and generates negative consequences affecting the victim’s development, which may increase the likelihood that maltreatment will be reproduced in the next generation.
Several prospective, intergenerational studies provide compelling evidence that maltreatment does beget maltreatment. Widom, Czaja, and DuMont (2015), used multiple indicators of victimization and perpetration (e.g., Child Protective Services [CPS] records and self-report) and found the strongest evidence of continuity when both maltreatment victimization and perpetration were measured by CPS records. Participants with a history of officially recognized maltreatment were significantly more likely to have CPS reports of engaging in maltreating behaviors. Jaffee et al. (2013) found that mothers who retrospectively reported a history of childhood maltreatment were significantly more likely to have children who experienced physical maltreatment. Adding more nuance to the investigation of continuity, Kim (2009) demonstrated that a self-reported history of neglect significantly increased the likelihood of later involvement in both neglect and physical abuse whereas a self-reported history of physical abuse significantly increased the likelihood of involvement in physical abuse but was only marginally related to neglect.
In one of the most rigorous examinations of intergenerational continuity in maltreatment, Thornberry and Henry (2013) used propensity scores to control for selection effects and examined the impact of maltreatment victimization on the likelihood of engaging in maltreating behaviors using measures of substantiated cases of maltreatment incidents from CPS. As hypothesized, victimization significantly increased the odds of becoming a perpetrator of maltreatment, but when they accounted for the timing of victimization by dividing the sample into those who experienced childhood-limited maltreatment (at least one substantiated incident prior to the age of 12) and adolescent maltreatment (at least one substantiated incident between the ages of 12 and 17), Thornberry and Henry (2013) found that childhood-limited maltreatment did not significantly increase the odds of maltreatment perpetration. Only maltreatment that occurred in adolescence significantly increased the risk for engaging in perpetrating behaviors later in life.
Other prospective studies, using diverse samples and various measures of maltreatment, also reported significant levels of continuity between victimization and perpetration (e.g., Berlin, Appleyard, & Dodge, 2011; Conger, Schofield, Neppl, & Merrick, 2013; Dixon, Browne, & Hamilton-Giachritsis, 2005). While there are differences in how maltreatment is measured (self-reports and official data; Widom et al., 2015) and support for the cycle of maltreatment varies by the timing of maltreatment victimization (Thornberry & Henry, 2013), a history of maltreatment victimization, nonetheless, appears to be a significant risk for later involvement in maltreating behaviors.
Searching for the Developmental Processes That Promote the Cycle of Maltreatment
While evidence of a significant degree of intergenerational continuity in maltreatment grows, much less is known about mediating processes that explain why a history of maltreatment victimization increases the risk of engaging in maltreating behaviors. A recent overview concluded that “relatively little progress has been made in understanding the causes of child abuse and neglect” (Institute of Medicine and National Research Council, 2014, p. 69). Understanding mediating processes is important for several reasons. Theoretically, it provides at least a partial explanation for how the relationship between child maltreatment victimization and later maltreatment perpetration works. That is, it helps identify the developmental processes through which exposure to maltreatment during childhood is translated into involvement in maltreating behaviors during adulthood. Practically, understanding these developmental processes helps pinpoint specific targets that prevention and intervention programs can use to interrupt the cycle of maltreatment.
Obviously, there are multiple pathways that could account for this relationship, ranging from genetic endowments passed from parent to child (Stallings et al., 1997) to shared environments in which each generation is exposed to the same social influences (e.g., poverty and stress) that generate maltreatment anew (Stith et al., 2009). Previous investigations of mediators of the cycle of maltreatment have examined individual and family characteristics such as psychopathology (Belsky & Jaffee, 2006), cognitive development (Berlin et al., 2011), and the co-occurrence of intimate partner violence (Capaldi, Kim, & Pears, 2009). However, none adopted a life course perspective or took into account the developmental timing of maltreatment victimization.
We adopt a life course perspective and focus on the proximal behavioral consequences of maltreatment that are also known risk factors for perpetrating behaviors and, therefore, may provide bridges that perpetuate the cycle of maltreatment across the generations. In addition, we pay particular attention to the fact that the behavioral consequences of maltreatment may be dependent on the timing of the maltreatment victimization itself. In doing so, we investigate not only the general developmental processes that perpetuate the cycle of maltreatment but also how the timing of maltreatment may differentially invoke pathways to maltreatment. In particular, we examine two developmental pathways, experiencing precocious transitions from adolescence to adulthood and involvement in adolescent problem behaviors, that have the potential to serve as mediators of intergenerational continuity in maltreatment (see Augustyn, Thornberry, & Krohn, 2014). It is important to keep in mind that we do not view the life course pathways proposed as alternatives to the other processes previously identified that help account for the cycle of maltreatment (Belsky & Jaffee, 2006; Berlin et al., 2011). All these pathways likely play a role in accounting for intergenerational continuity in maltreatment.
Precocious Transitions
One form of maladaptation, grounded in the life course perspective and its focus on the appropriate timing of life events (Elder, 1998), is a precocious transition to adulthood (e.g., dropping out of high school, prematurely leaving the house-hold of origin, and/or becoming a parent during the teenage years). Individuals whose formative years are beset by adversity in the form of trauma and stress, including exposure to maltreating behaviors, are more likely than others to experience accelerated biological and social maturation and “rush to adulthood.” Not only are maltreatment experiences and other forms of adversity associated with earlier pubertal timing (Belsky, Ruttle, Boyce, Armstrong, & Essex, 2015; Ryan, Mendle, & Markowitz, 2015), but often maltreated youth seek out early transitions to adulthood in order to escape a stressful or traumatic environment. Prior research suggests that maltreatment victimization is associated with an increased likelihood of dropping out of high school (Allwood & Widom, 2013; Kendall-Tackett & Eckenrode, 1996; Perez & Widom, 1994; Thornberry, Ireland, & Smith, 2001), as well as teenage parenthood (Lansford et al., 2007; Putnam-Hornstein Cederbaum, King, & Needell, 2013; Thornberry et al., 2001) and prematurely leaving the family home to live on one’s own (Thrane, Hoyt, Whitbeck, & Yoder, 2006; Tyler & Bersani, 2008; Westat, 1997). Thus, we hypothesize that maltreatment victimization is significantly related to the likelihood of experiencing precocious transitions.
We also expect adolescent experiences of maltreatment to be particularly salient to the likelihood of experiencing precocious transitions as adolescent maltreatment may lead to multiple and more serious attempts to transition or escape from a stressful adolescence into the perceived independence in adulthood. To date, very few studies examined the impact of developmentally specific measures of maltreatment on the likelihood of experiencing precocious transitions. However, consistent with our expectation, Thornberry et al. (2001) reported that adolescent maltreatment, but not childhood maltreatment, significantly increased the chances of teen pregnancy, and Kaplow and Widom (2007) found that an older age of onset for maltreatment was significantly related to school dropout.
Precocious transitions, such as dropping out of school, early parenthood, and independent living during adolescence, limit the acquisition of human and social capital (Hagan & Foster, 2001) and increase the likelihood of negative consequences for individual and family well-being. Those transitions often create stressful life contexts that are maladaptive as adolescents are not equipped with the cognitive or emotional skills and competencies to handle these role changes (Foster, Hagan, & Brooks-Gunn, 2008; Oshri, Rogosch, Burnette, & Cicchetti, 2011; Wickrama, Conger, Lorenz, & Jung, 2008; Wickrama, O’Neal, & Oshri, 2014). Furthermore, those who experience precocious transitions often struggle with the emotional, social (e.g., familial), and financial demands of adulthood, which are atypical to adolescence (Hatch, 2005; Wickrama, Conger, Wallace, & Elder, 2003). As a result, individuals who “rush to adulthood” are, on average, less able to successfully discharge the major roles of adulthood, including providing a safe, stable, and nurturing environment for children. Thus, we hypothesize that precocious transitions will increase the chances of involvement in child maltreatment. Consistent with this hypothesis, dropping out of school is a significant predictor of later maltreatment (Brown, Cohen, Johnson, & Salzinger, 1998; Cox, Kotch, & Everson 2003; Stith et al., 2009; Thornberry et al., 2013), as is early independent living (Thornberry et al., 2014) and teenage parenthood (Brown et al., 1998; Chaffin, Kelleher, & Hollenberg, 1996; Cox et al., 2003, Thornberry et al., 2013).
As trajectories become interwoven over the course of development, precocious transitions often cluster together. For example, dropping out of high school and becoming a teen parent are interrelated (Brooks-Gunn & Chase-Lansdale, 1995; Kane, Morgan, Harris, & Guilkey, 2013), although the direction of the relationship is often ambiguous. We hypothesize, therefore, that maltreatment victimization, particularly maltreatment in adolescence, will increase the likelihood of experiencing multiple precocious transitions. In turn, experiencing multiple precocious transitions will increase the risk of maltreatment perpetration.
Adolescent Problem Behaviors
Exposure to maltreatment is also related to other behavioral indicators of maladaptation, including heightened involvement in adolescent problem behaviors such as delinquency, substance use, and aggression (e.g., Fagan, 2005; Mersky, Topitzes, & Reynolds, 2012; Stewart, Livingston, & Dennison, 2008; Widom, 1989). Exposure to maltreatment, particularly if it is violent and severe, creates an environment in which problem behaviors, including delinquency and aggression, are modeled, reinforced, and subsequently internalized as acceptable and appropriate responses to many of life’s challenges (Capaldi et al., 2009; Pears & Capaldi, 2001). Even neglect, the most prevalent form of child maltreatment, affects involvement in subsequent problem behaviors (Eckenrode et al., 2001; Ryan, Williams, & Courtney, 2013) as it reduces the likelihood of a safe, stable, and nurturing environment affecting the formation of self-control, responsibility (Gottfredson & Hirschi, 1990), and prosocial attachments to caregivers (Conger et al., 2013). Cicchetti and colleagues (Lynch & Cicchetti, 1998; Shields & Cicchetti, 1998) found that childhood experiences of maltreatment were related to aggression and other conduct problems, and Kim (2009) found that maltreatment was related to increased levels of delinquency during adolescence.
Individuals who engage in more chronic forms of delinquency and aggression during adolescence are often characterized as impulsive and irritable, and those who exhibit these characteristics are more likely to engage in maltreating behaviors (Simons, Whitbeck, Conger, & Wu, 1991; Thornberry, 2005). Empirically, delinquency, especially if it is serious and prolonged, is associated with an increased likelihood of maltreatment perpetration (Brown et al., 1998; Moffitt, Caspi, Harrington, & Milne, 2002; Thornberry et al., 2013; Verlaan & Schwartzman, 2002). Thus, we hypothesize that maltreatment victimization increases involvement in delinquency and aggression, and high levels of involvement in these behaviors during adolescence increases the likelihood of subsequent maltreatment perpetration.
Maltreatment victimization also increases the likelihood of alcohol and drug use (Gilbert et al., 2009; Jonson-Reid, Kohl, & Drake, 2012), including prolonged use during adolescence, perhaps as a means of escape or self-medication (Lansford, Dodge, Pettit, & Bates, 2010). It is possible, though, that this relationship may be driven primarily by adolescent experiences of maltreatment given that Widom, Ireland, and Glynn (1995) and Thornberry et al. (2001) found childhood experiences of maltreatment were unrelated to alcohol use.
Adolescent substance use is related to continued substance use during adulthood (Odgers et al., 2008; Ohannessian, Finan, Schulz, & Hesselbrock, 2015), and substance use significantly reduces the quality of parenting behaviors (Dishion, Capaldi, & Yoerger, 1999; Fals-Stewart, Kelley, Fincham, Golden, & Logsdon, 2004). Several reasons are proposed to account for this effect. For example, substance use deflects resources, including material resources and social support, away from the child. In addition, the reactions of substance using parents to child behavior is often erratic, driven more by the emotional and drug-dependent needs of the adult rather than the behaviors and needs of the child (Patterson, Reid, & Dishion, 1992). Both factors serve to increase the chances of inappropriate parenting behaviors, including maltreatment. Empirically, alcohol use and marijuana use during adolescence are significant risk factors for involvement in maltreatment during adulthood (Cash & Wilkie, 2003; Thornberry et al., 2014; Widom & Hiller-Sturmhofel, 2001). Thus, we hypothesize that maltreatment victimization will increase adolescent substance use and this, in turn, will increase the likelihood of maltreatment perpetration.
Furthermore, we expect the impact of adolescent substance use, delinquency, and aggression on subsequent maltreatment perpetration to be particularly salient among those who experienced maltreatment victimization during adolescence. The recency of the maltreatment may serve to promote problem behaviors as a coping mechanism, learned responses to difficult situations such as aggression (i.e., physical abuse) or withdrawal (i.e., neglect), or manifestations of low self-control. Several studies have shown that adolescent maltreatment has a stronger impact than childhood maltreatment on delinquency, aggression, and substance use (Eckenrode et al., 2001; Jonson-Reid & Barth, 2000; Stewart et al., 2008; Thornberry et al., 2001), although other studies showed that both childhood and adolescent maltreatment have significant effects on these outcomes (Keiley, Howe, Dodge, Bates, & Pettit, 2001; Mersky et al., 2012).
Finally, as with precocious transitions, the co-occurrence of different types of problem behaviors often exists. We therefore hypothesize that maltreatment victimization will be associated with involvement in multiple types of problem behavior, a relationship that will be especially relevant for victims of adolescent maltreatment (Thornberry et al., 2001). In turn, the accumulation of problem behaviors will increase the risk of later involvement in maltreatment perpetration.
Hypotheses
Prior research tests various pieces of these developmental processes that potentially help explain the link from maltreatment victimization to later perpetration, but there is no examination of a formal mediation model that empirically assesses the entire process as outlined in Figure 1. As a result, we do not know which, if any, of the proposed precocious transitions and problem behaviors act as intermediate variables and explain the cycle of maltreatment. Accordingly, we use prospective, longitudinal data to confirm the previously out-lined hypotheses regarding Path a and Path b in Figure 1 before explicitly testing the following hypotheses derived from our proposed mediation model.
Figure 1.
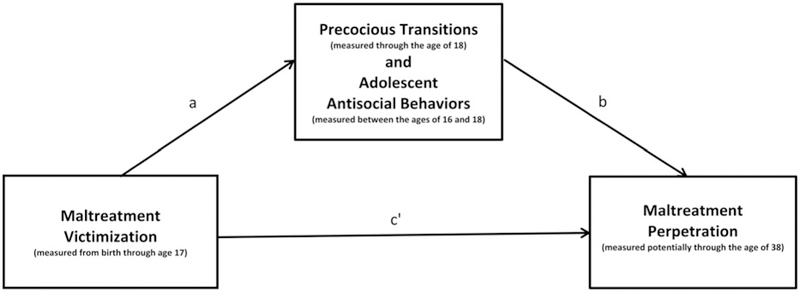
Mediation model of the cycle of maltreatment.
Each precocious transition (e.g., dropping out of high school) and problem behavior (e.g., alcohol use) mediates, in part, the relationship between maltreatment victimization and maltreatment perpetration.
The accumulation of multiple precocious transitions and involvement in multiple forms of problem behavior will mediate the relationship between maltreatment victimization and perpetration, accounting for a greater proportion of the relationship between victimization and perpetration that any one precocious transition or problem behavior on its own.
We also investigate whether these processes operate differentially based on the timing of maltreatment in the life course (childhood-limited vs. adolescent maltreatment victimization). Recall, studies that incorporate developmentally specific measures of maltreatment suggest that the proposed relationships are more consistently observed for victimization that occurs during adolescence as compared to childhood. Therefore, we first test the mediation model for the full sample and then examine whether the timing of maltreatment informs these developmental pathways by assessing the mediation model for childhood-limited maltreatment and adolescent maltreatment, respectively.
Data and Method
Data come from the Rochester Youth Development Study, a multiwave panel study of the development of antisocial behavior that, starting in 1988, interviewed a sample of 1,000 adolescents 14 times (Waves 1–14) from age 14 to age 31. A parent of the focal participant was also interviewed (up to 11 times; Waves 1–8, 10–12) until the focal participant was age 23 and official data were collected from the police, schools, and social services, in some cases to as late as age 38.
Sample
The target population was limited to seventh- and eighthgrade students in the public schools of Rochester, New York, a city that has a diverse population and a high crime rate. The sample was then stratified on two dimensions. The Rochester Youth Development Study oversampled youth at a high risk for serious delinquency and drug use because the base rates for these behaviors are relatively low (Elliott, Huizinga, & Menard, 1989). First, males were oversampled, 75% versus 25%, because they are more likely to engage in serious antisocial behaviors (Blumstein, Cohen, Roth, & Visher, 1986). Second, adolescents from areas of the city where high proportions of adult offenders lived were over-sampled on the premise that youth residing in these areas are at a greater risk for offending. Each census tract was assigned a resident arrest rate reflecting the proportion of the population living in that tract arrested by the Rochester police in 1986. Adolescents were sampled proportionate to the rate of offenders living in their tract of residence.
The initial cooperation rate was 80%, and if a family did not want to participate, it was replaced by another family, selected at random, from the same or similar stratum. Data collection was done via face-to-face interviews and was conducted separately for the adolescent and the parent. Attrition is acceptable for a longitudinal study of this duration. When the adolescent participants reached age 23, the last point at which parents were interviewed, 85% of the adolescents and 83% of their parents were retained; at age 31, 79% of the initial adolescents were retained. Comparing the gender, race/ethnicity, resident arrest rate, baseline levels of delinquency and drug use, and family structure of those who were retained at age 31 to those who left the study demonstrates that attrition did not bias the sample (Bushway, Krohn, Lizotte, Phillips, & Schmidt, 2013; Thornberry, Henry, Krohn, Lizotte, & Nadel, 2018). All aspects of the study were reviewed and approved by the institutional review board at the University at Albany.
The participants are predominantly African American (68%) with about equal proportions of Hispanics (17%) and Whites (15%). Study participants come from relatively disadvantaged family backgrounds. For example, at the start of the study, over half of participants’ parents received public assistance, completed on average 11 years of education, and had their first child as a teenager. At the start of the study, only one-quarter of the youth lived with both biological parents, and a substantial number lived in impoverished neighborhoods. Although the study oversampled at-risk families, the full range of the Rochester city socioeconomic spectrum is represented (Farnworth, Thornberry, Krohn, & Lizotte, 1994).
Analytic sample
Our sample consists of the 816 participants who were still active in the study in 2010 and for whom there was informed consent for a search of CPS records at the New York State Office of Children and Family Services (OCFS), the statewide repository for maltreatment records. We include all participants, not just those who were biological parents (n = 611), as nonparents can and, in our data set, are implicated in incidents of child maltreatment. Over the course of the study, most of the participants (>90%) had a biological child or lived in a household with children at one point or another, for example, as a live-in boyfriend or a stepparent, and had the opportunity to maltreat. We conducted several additional analyses to assess the consequences of parent status, and limiting the sample to only parents (biological or stepparents) did not lead to substantively different results. As the analytic method selected precludes the use of multiple imputed data sets to retain all participants in this analysis, we use listwise deletion and have a final sample of 732 participants. It is worth noting that the final 732 subjects did not significantly ( p<.05) vary from the initial 816 available participants across an array of demographic characteristics including gender, race/ethnicity, community arrest rate, age at baseline, poverty status at baseline, parental education, and maternal age at first birth.
Maltreatment measures
Our indicators of maltreatment victimization and maltreatment perpetration are based on official records of maltreatment taken from different agencies in New York State. We recognize that official maltreatment records have limitations; for example, not all instances of maltreatment are reported and not all reported cases are substantiated (Eckenrode, Powers, Doris, Munsch, & Bolger, 1988; Straus, Gelles, & Smith, 1995; Widom, 1988). In addition, investigation bias may lead to the overestimation or underestimation of maltreatment by certain groups within the overall population (Widom et al., 2015). Despite these limitations, prospective measures based on substantiated CPS records have several advantages. They have strong psychometric properties, especially for capturing incidents of maltreatment at the more severe end of the continuum (Institute of Medicine and National Research Council, 2014; Widom, Raphael, & DuMont, 2004). They also allow for temporal ordering of variables, which is central to mediation analysis. Moreover, results from studies examining the consequences of maltreatment victimization using official measures suggest strong construct validity (Gilbert et al., 2009).
Maltreatment victimization.
Maltreatment victimization is based on data from CPS records of the Monroe County Department of Social Services, the county of residence for participants at the start of the study. Information was collected on all substantiated incidents, from birth through age 17, in which a study participant was listed as a victim of maltreatment. This includes neglect, physical abuse, emotional abuse, and sexual abuse. A substantial number of these incidents (43.75%) involved multiple types of maltreatment. Overall, 19% of those in our sample were victims of at least one incident of maltreatment.
The independent variable in this study is the number of different types of maltreatment to which the participant was exposed. The different types could occur in one incident or across multiple incidents. This measurement strategy was selected given that the severity of abuse is highly correlated with the number of different forms of abuse incurred, and severity is often linked to later negative outcomes (Clausen & Crittendon, 1991; Clemmons et al., 2007). Due to the small number of individuals who experienced three or more types of maltreatment (<3%), the number of maltreatment types was collapsed into an ordinal count variable: 0, 1, and 2 or more types of maltreatment. In our analytic sample, 81% of subjects never experienced maltreatment, 8% experienced only 1 type of maltreatment, and 11% experienced 2 or more types of maltreatment.2
We also calculated the number of types of maltreatment experienced for subjects who experienced childhood-limited maltreatment (substantiated incident(s) through age 11 and no substantiated incidents at age 12 or older) and then among subjects who experienced maltreatment in adolescence (a substantiated incident(s) at or after age 12; see Thornberry & Henry, 2013). Once again, respondents were coded as having experienced 0, 1, or 2 or more types of maltreatment (e.g., physical, sexual, neglect, etc.). Among the childhood-limited sample, 12% were victims of maltreatment, with 6% experiencing only 1 type of maltreatment and 6% experiencing 2 or more types of maltreatment. Among the adolescent maltreatment sample, 8% were victims of maltreatment. Of those, 3% experienced only 1 type of maltreatment and 5% experienced 2 or more types of maltreatment.
Maltreatment perpetration.
Information on whether or not the participant was named a perpetrator of any type of child maltreatment (i.e., neglect, physical, emotional, or sexual abuse) was collected from OCFS through the year 2010. Due to the limited nature of the data available in this statewide repository, the dependent variable is whether or not the participant had a record of at least one substantiated case of maltreatment perpetration. Overall, these records indicate that 12.5% (n = 102) of the individuals included in this analysis had at least one incident of maltreatment perpetration.
At the time of the search in 2010, 82% of the participants still resided in New York State, so coverage from the statewide OCFS records is rather complete. Nevertheless, there is some right-hand censoring as there were not record searchers for all participants through the end of the follow-up period. We know either the age at which each participant engaged in his or her first substantiated case of perpetration or, if none, the age at the last available year of data collection from OCFS (i.e., the age at right censoring). For 59% of the sample, the age at censoring is the participant’s age in 2010 when the CPS records from OCFS were last collected, but for some individuals it is the age when he or she left the study and informed consent expired or when the individual moved out of New York State. The average age of CPS record coverage is 33.2; 85% of the sample were at least 30, and the oldest participants were 38. We therefore have data for a considerable portion of the early adulthood, from age 18 to the average age of 33, or 15 years of exposure. Nevertheless, given the right-hand censoring, we model the outcome as a survival process (see below).
Precocious transitions
We examine whether dropping out of high school, teenage parenthood, and independent living that occurs prior to the 19th birthday (i.e., through the age of 18) help to explain the cycle of maltreatment. High school dropout is a binary variable indicating whether or not the adolescent self-reported permanently dropping out of high school before graduation, thus failing to earn his or her high school diploma. If the adolescent subsequently earned a General Education Development high school certificate (GED), he or she is still counted as a high school dropout given the significant differences between earning a diploma and obtaining a GED on various life outcomes (Heckman, Humphries, & Kautz, 2015). Forty-six percent of the analytic sample failed to graduate from high school. Teenage parenthood is a binary variable that indicates whether or not the adolescent self-reported having a biological child through the age of 18. A little over one-quarter (26%) of the participants met this definition. Independent living is a binary variable that indicates whether or not an adolescent self-reported living without a guardian (i.e., parent, stepparent, grandparent, aunt/uncle, etc.) at any point prior to his or her 19th birthday.3 Nine percent of the sample lived independently of adult supervision at some point through the age of 18.
Problem behaviors
Problem behavior (alcohol use, drug use, delinquency, and aggression) was measured when participants were, on average, between the ages of 16 and 18 (Waves 6–9).4 In Waves 6 through 9, participants were asked whether or not they drank beer, wine, wine coolers, or hard liquor without their parent’s permission since the last interview and, if so, how many times. The number of times reported at each interview was summed to create an overall incidence measure of alcohol use. Participants were also asked how many times they used any of the following drugs since the last interview: marijuana, inhalants, hallucinogens, cocaine, crack, heroin, PCP, tranquilizers, uppers, and downers. The number of times that they reported using any of these illicit drugs from Waves 6 through 9 was summed to create an overall incidence measure of drug use. Adolescents were also asked whether or not they engaged in 28 different criminal behaviors ranging from vandalism and minor property crimes to serious violent and property crimes such as robbery since their last interview, and, if so, how many times. Our measure of delinquency is the sum of the individual frequencies for each of the 28 criminal behaviors reported from Waves 6 through 9. The final indicator of adolescent problem behavior is based on parent reports, using the aggression subscale of the Child Behavior Checklist (Achenbach, 1991) asked in Waves 6 and 7 (but not at Waves 8 and 9). Each parent or guardian was queried how often (always, sometimes, or never) the adolescent engaged in 12 behaviors such as being hyperactive and getting into fights. The average score from Waves 6 and 7 forms the measure of aggression.
We dichotomized each problem behavior at the riskiest quartile of the distribution in order to identify more serious, chronic offenders (Farrington & Loeber, 2000) given that prior research suggests that greater involvement in these behaviors predicts subsequent maltreatment. Dichotomizing these measures also provides a consistent metric for all potential mediators, allows for the comparison of the magnitude of each proposed mediator, and permits the creation of cumulative measures.
Cumulative indicators
As previously noted, consequences of child maltreatment (precocious transitions and problem behaviors) often cluster together, potentially intensifying their impact. Previous research indicates that as the number of risk factors for maltreatment increases, the likelihood of involvement in maltreatment perpetration increases dramatically (Brown et al., 1998; MacMillan, 2000; Thornberry et al., 2013). Therefore, we created three separate count measures of the mediators: the number of precocious transitions, the number of problem behaviors, and the total number of problem behaviors and precocious transitions engaged in by each participant. The total number of precocious transitions ranges from 0 to 3 (high school dropout, independent living, and teenage parenthood), with 43.5% experiencing 0 transitions, 35.6% experiencing 1, 15.2% experiencing 2, and 4.6% experiencing 3. The total number of problem behaviors ranges from 0 to 4 (alcohol use, drug use, delinquency, and aggression), with 48.65% reporting 0 problem behaviors, 25.27% reporting 1, 11.35% reporting 2, 9.59% reporting 3, and 5.14% reporting 4. Finally, we created a summed score of precocious transitions and problem behaviors, 29.67% had a score of 0, 23.63% had 1, 19.09% had 2, 12.36% had 3, 6.87% had 4, 6.46% had 5, 1.65% had 6, and 0.27% had 7.
Control variables
While prior research examining the effect of maltreatment victimization on subsequent perpetration with the same data set used propensity score methodology to address issues of selection related to maltreatment victimization, current propensity score methodology does not lend itself to mediation analysis with an ordinal independent variable, binary/count mediators, and a survival process as the outcome. Therefore, we control for the same confounding factors used by Thornberry and Henry (2013) to examine if the effect of maltreatment victimization on maltreatment perpetration through the proposed developmental pathways is spurious. We include a control variable for neighborhood, resident arrest rate described above. Parent education refers to the highest grade completed by the participant’s principal family wage earner. We also include a continuous measure of the primaryguardian’s ageat first birth. Finally, we control for demographic variables, including the participant’s gender (male), race/ethnicity (African American and Hispanic), and age at Wave 1. We refrain from including additional covariates given that they violate temporal ordering. Table 1 includes descriptive statistics for the full analytic sample, the childhood-limited maltreatment sample, and the adolescent maltreatment sample. A correlation matrix for all covariates in this analysis is provided in Appendix A.
Table 1.
Descriptive statistics
| Full sample (n = 732) |
Childhood-limited maltreatment sample (n = 681) |
Adolescent maltreatment sample (n = 659) |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Range | Value at 75th percentile | Mean/ proportion | SD | Mean/ proportion | SD | Mean/ proportion | SD | |||
| Maltreatment | ||||||||||
| Perpetrationa | 0, 1 | 0.13 | 0.11 | 0.12 | ||||||
| Victimization | 0, 2 | 0.91 | ||||||||
| No victimization (0) | 0.81 | 0.88 | 0.03 | |||||||
| One type of victimization (1) | 0.08 | 0.06 | 0.06 | |||||||
| Two or more types of victimization (2) | 0.11 | 0.06 | ||||||||
| Antisocial behaviors | ||||||||||
| Alcohol use | 0–740 | 20.00 | 31.17 | 75.97 | 29.22 | 72.76 | 30.88 | 77.56 | ||
| Drug use | 0–577 | 4.00 | 19.74 | 62.32 | 18.36 | 60.64 | 19.60 | 62.29 | ||
| Delinquency | 0–873 | 27.00 | 47.50 | 108.56 | 44.70 | 106.4 | 46.25 | 107.37 | ||
| Aggression | 0–1.75 | 0.58 | 0.37 | 0.32 | 0.36 | 0.32 | 0.36 | 0.33 | ||
| Sum of antisocial behaviors | 0–4 | 0.99 | 1.22 | 0.96 | 1.20 | 0.96 | 1.20 | |||
| Precocious transitions | ||||||||||
| High school dropouta | 0, 1 | 0.46 | 1.63 | 0.44 | ||||||
| Teenage parenthooda | 0, 1 | 0.26 | 1.63 | 0.26 | ||||||
| Independent livinga | 0, 1 | 0.09 | 0.08 | 0.09 | ||||||
| Sum of precocious transitions | 0–3 | 0.80 | 0.86 | 0.76 | 0.84 | 0.78 | 0.86 | |||
| Sum of problem behaviors and transitions | 0–7 | 0.80 | 1.63 | 1.65 | 1.61 | 1.66 | 1.63 | |||
| Control variables | ||||||||||
| Malea | 0, 1 | 0.71 | 0.68 | 0.71 | ||||||
| African Americana | 0, 1 | 0.69 | 0.68 | 0.68 | ||||||
| Hispanica | 0, 1 | 0.16 | 0.17 | 0.18 | ||||||
| Age at Wave 1 | 11.1–15.0 | 13.52 | 0.76 | 11.44 | 0.76 | 13.51 | 0.77 | |||
| Parent education | 6−18 | 11.40 | 2.16 | 11.44 | 2.18 | 11.42 | 2.18 | |||
| Mother’s age at first birth | 0, 1 | 19.04 | 3.68 | 19.10 | 3.76 | 19.10 | 3.61 | |||
| Resident neighborhood arrest rate | 0.12−7.87 | 4.22 | 2.08 | 4.18 | 2.06 | 4.19 | 2.09 | |||
Note: Binary variable. SD, standard deviation (not reported for proportion).
Analytic plan
The identification of the mediators of a process is critical for the understanding of how or why a certain treatment (e.g., maltreatment victimization) influences an outcome (e.g., maltreatment perpetration). When mediator and outcome are normally distributed, continuous variables and there is not a nonlinear or treatment by mediator interaction effect present, mediation is examined via the estimation of two effects: (a) the effect of the treatment on the mediator (Path a in Figure 1) and (b) the effect of the mediator on the outcome, holding constant the treatment (Path b in Figure 1). The product of these two coefficients (a*b) is the indirect effect (Baron & Kenny, 1986). In the current analysis, none of the mediators, nor the outcome variable, are normally distributed, continuous variables. Rather, our mediators are binary and categorical and our outcome is a survival process. Therefore, the product of coefficients approach is not appropriate (VanderWeele, 2011).
Recent advances in mediation analysis using the counterfactual framework (Pearl, 2009; VanderWeele & Vansteelandt, 2009, 2010) allow for definitions of direct and indirect effects and the decomposition of a total effect into direct and indirect effects for models with nonlinearities. Valeri and VanderWeele (2013) outline a formal approach to the assessment of mediation grounded in the counterfactual framework that allows for dichotomous and count mediators. It was subsequently expanded upon by Valeri and VanderWeele (2015) for mediation analysis when the outcome is a survival process.
Under this framework we let A denote the treatment, T denote the value of the time-to-event outcome, M denote the mediator, and C denote additional covariates. We can model T as a failure time variable using a Cox-proportional hazard model and define the following mediator regression:
If no unmeasured confounding assumptions hold and the Cox-proportional hazard regression is employed, then under the counterfactual framework (see Lange & Hanson, 2011; Valeri & VanderWeele, 2013), the total effect of an exposure on a survival time ratio scale can be decomposed into the following components (Valeri & VanderWeele, 2015): the controlled direct effect, which compares the effect of treatment A to A*fixing the mediator to level M,
and the natural indirect effect, which compares the effect of the mediator at levels MA and MA*
All analyses were conducted in SAS, version 9.3. Logistic (for each binary mediator) and Poisson (for cumulative indicators) regression models are first used to assess the effect of maltreatment on the mediators (Path a in Figure 1). Then, Cox-proportional hazard models were used to assess the effects of each mediator on the onset of maltreatment perpetration (Path b in Figure 1). Finally, Cox-proportional hazard models were used to assess the controlled direct and natural indirect effects of the treatment on the onset of maltreatment perpetration via each precocious transition and problem behavior mediator using the method outlined by Valeri and VanderWeele (2015), setting the appropriate estimation procedure for each specific mediator (either a logistic regression model or a Poisson regression model) and assigning a treatment and mediator level. We present the results of the decomposed causal effects for a change in treatment from no maltreatment to one type of maltreatment with the mediator level set to one and from no maltreatment to two or more types of maltreatment with the mediator level set to one, respectively, in order to demonstrate that the general pattern of causal pathways between maltreatment types and perpetrating behaviors is not linear in nature.
Finally, mediation models assume proper temporal order from the treatment variable to the mediator and then to the outcome. For Path a, proper temporal order is ensured for all individuals. In other words, for each victim of maltreatment, the age at one’s first incident of maltreatment victimization was prior to the age when one experienced a precocious transition and when the problem behaviors were assessed (Wave 6, average age 16.5 years old). For Path b, there are a handful of cases in which it is difficult to determine the exact temporal order as there is a range of occurrence for the mediator (at some point during the time period between two adjacent interviews) rather than a specific date of occurrence. Specifically, there are five cases where the (first/only) act of maltreatment perpetration may have occurred prior to one of the precocious transitions, but for four of these participants, there is clear evidence that at least one of the precocious transitions occurred before the (first/only) act of maltreatment perpetration. As such, we decided to include these four cases so as to maximize the sample size. Supplemental analyses removed these participants, and the results did not change in direction or significance.
Results
We begin with an examination of the total effect of the number of types of maltreatment victimization on perpetration, irrespective of mediators, controlling for gender, race/ethnicity, age, parent education, primary guardian age at first birth, and community arrest rate.5 The hazard ratio (HR) for this relationship is 1.63 (95% confidence interval; CI [1.26, 2.11]).
Path a in the mediation model (Figure 1) hypothesizes that maltreatment victimization increases the risk of involvement in problem behaviors and precocious transitions. Our analyses revealed that maltreatment victimization significantly increased the likelihood of involvement in all problem behaviors; as the number of types of maltreatment victimization increased, youths self-reported more alcohol use (odds ratio; OR = 1.33, 95% CI [1.02, 1.72]), more drug use (OR = 1.35, 95% CI [1.05, 1.73]), more delinquent behavior (OR = 1.41, 95% CI [1.07, 1.81]), and were perceived by their parents as more aggressive (OR = 1.39, 95% CI [1.07, 1.81]). Each additional type of maltreatment was also associated with increased involvement in multiple problem behaviors (relative risk reduction; RRR = 1.21, 95% CI [1.09, 1.35]). Turning to the precocious transitions, there were significant effects of maltreatment victimization on the likelihood of dropping out of high school (OR = 1.85, 95% CI [1.43, 2.38]), living independently from one’s parents (OR = 1.50, 95% CI [1.06, 2.13]), and experiencing multiple precocious transitions (RRR = 1.24, 95% CI [1.11, 1.39]). The number of maltreatment types, however, was not significantly related to teenage parenthood (OR = 1.22, 95% CI [0.94, 1.59]), after adjusting for the control variables. The impact of the number of types of maltreatment victimization on the summed score of all mediators ( precocious transitions plus problem behaviors), was also positive and significant (RRR = 1.22, 95% [CI 1.12, 1.32]).
Next, we investigated whether adolescent problem behaviors and precocious transitions were significant precursors to later involvement in maltreating behaviors (Path b) in the mediation model. Youth who were involved in alcohol use (HR = 2.38, 95% CI [1.55, 3.66]), drug use (HR = 2.26, 95% CI [1.48, 3.45]), delinquency (HR = 2.24, 95% CI [1.47, 3.36]), and parent-reported aggression (HR = 1.71, 95% CI [1.04, 2.80]) were significantly more likely than their counterparts to have a substantiated record of maltreatment perpetration. In addition, as the number of antisocial behaviors in which they were involved increased, so did the odds of involvement in maltreating behaviors (HR = 1.38, 95% CI [1.18, 1.62]). Each of the precocious transitions was significantly related to the likelihood of later involvement in maltreating behaviors. Youth who dropped out of school (HR = 3.34, 95% CI [2.02, 5.51]), became a teen parent (HR = 3.06, 95% CI [1.96, 4.77]), or who lived independently before age 19 (HR = 3.64, 95% CI [2.13, 6.21]) were significantly more likely to maltreat children. The total number of precocious transitions also increased the odds of being involved in maltreatment (HR = 2.33, 95% CI [1.84, 2.94]). Likewise, as the total number of precocious transitions plus problem behaviors increased, the odds of maltreating a child increased as well (HR = 1.46, 95% CI [1.30, 1.64]).
We directly assessed our mediation hypotheses by partitioning the total effect of child maltreatment on maltreatment perpetration into three parts: the controlled direct effect, the natural indirect effect via each mediator, and the total effect. Table 2 presents the results, with each row representing a separate equation, including all control variables. In each model estimated, there is a significant direct effect of maltreatment victimization on the likelihood of maltreatment perpetration. Even when each mediator was included, maltreatment increased the risk of perpetration. There is also evidence of mediation. Delinquency partially mediated the effect of the number of types of maltreatment victimization on later perpetration, accounting for approximately 12% of the total effect of one type of maltreatment victimization on maltreatment perpetration and 15% of two or more types of maltreatment victimization on perpetrating behaviors. The summed problem behavior score also served as a mediator, accounting for 65% of the total effect of one type of maltreatment victimization on subsequent perpetration and 75% of the total effect of two or more types of maltreatment victimization on perpetration. For the precocious transitions, dropping out of high school was a significant mediator, and it accounted for 35% of the total effect of one type of maltreatment victimization on subsequent perpetration and 38% of two or more types of maltreatment victimization on perpetration. The summated variable for precocious transitions also significantly mediated the effect of one type of maltreatment victimization on maltreatment perpetration, accounting for 70% of the total effect of victimization on perpetration. Moreover, the summed score of precocious transitions accounts for 79% of the total effect of two or more types of maltreatment victimization on subsequent perpetrating behaviors. In addition, the total summed score across all problem behaviors and precocious transitions served as a mediator of the cycle of maltreatment, also accounting for nearly 70% of the effect of one type of victimization on perpetration and nearly 80% of the total effect of two types or more of maltreatment victimization on perpetration.
Table 2.
Cox proportional hazards models results of direct and indirect effects of maltreatment victimization on perpetration
| Controlled direct effect |
Natural indirect effect |
Total effect |
Proportion mediated estimate | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mediator | HR | 95% CI | HR | 95% CI | HR | 95% CI | |||
| Antisocial behaviors | |||||||||
| Alcohol use at 1 maltreatment type | 1.61** | [1.25, 2.07] | 1.05† | [0.99, 1.11] | 1.70** | [1.31, 2.19] | 0.12 | ||
| Alcohol use at 2+ maltreatment types | 2.59** | [2.01, 3.33] | 1.12† | [0.99, 1.26] | 2.89** | [1.31, 2.19] | 0.16 | ||
| Drug use at 1 maltreatment type | 1.58** | [1.23, 2.03] | 1.05† | [1.00, 1.11] | 1.66** | [1.29, 2.15] | 0.12 | ||
| Drug use at 2+ maltreatment types | 2.50** | [1.95, 3.22] | 1.11† | [0.99, 1.24] | 2.78** | [1.67, 4.63] | 0.15 | ||
| Delinquency at 1 maltreatment type | 1.56** | [1.21, 2.01] | 1.12* | [1.00, 1.11] | 1.65** | [1.28, 2.13] | 0.13 | ||
| Delinquency at 2+ maltreatment types | 2.44** | [1.89, 3.15] | 1.12* | [1.00, 1.25] | 2.73** | [1.64, 4.56] | 0.17 | ||
| Aggression at 1 maltreatment type | 1.58** | [1.20, 2.09] | 1.03 | [0.99, 1.08] | 1.64** | [1.24, 2.16] | 0.09 | ||
| Aggression at 2+ maltreatment types | 2.51** | [1.91, 3.30] | 1.07 | [0.98, 1.18] | 2.69** | [1.55, 4.68] | 0.11 | ||
| Sum of antisocial at 1 maltreatment type | 1.56** | [1.18, 2.06] | 1.07* | [1.01, 1.13] | 1.66** | [1.25, 2.21] | 0.65 | ||
| Sum of antisocial at 2+ maltreatment types | 2.43** | [1.38, 4.25] | 1.14* | [1.02, 1.27] | 2.76** | [1.57, 4.86] | 0.78 | ||
| Precocious transitions | |||||||||
| High school dropout at 1 maltreatment type | 1.43** | [1.11, 1.85] | 1.16** | [1.07, 1.26] | 1.67** | [1.62, 4.51] | 0.35 | ||
| High school dropout at 2+ maltreatment types | 2.06** | [1.50, 2.66] | 1.31** | [1.15, 1.50] | 2.70** | [1.62, 4.51] | 0.38 | ||
| Teenage parenthood at 1 maltreatment type | 1.67** | [1.30, 2.15] | 1.05 | [0.98, 1.13] | 1.75** | [1.35, 2.28] | 0.11 | ||
| Teenage parenthood at 2+ maltreatment types | 2.78** | [2.16, 3.58] | 1.11 | [0.96, 1.28] | 3.08** | [1.27, 2.12] | 0.14 | ||
| Independent living at 1 maltreatment type | 1.56** | [1.21, 2.01] | 1.05† | [0.99, 1.12] | 1.64** | [1.27, 2.12] | 0.13 | ||
| Independent living at 2+ maltreatment types | 2.43** | [1.89, 3.13] | 1.13 | [0.98, 1.31] | 2.75** | [1.64, 4.61] | 0.18 | ||
| Sum of precocious at 1 maltreatment type | 1.44** | [1.11, 1.86] | 1.18** | [1.08, 1.29] | 1.70** | [1.31, 2.22] | 0.70 | ||
| Sum of precocious at 2+ maltreatment types | 2.08** | [1.24, 3.48] | 1.39** | [1.17, 1.66] | 1.70** | [1.71, 4.93] | 0.79 | ||
| Sum of problem behaviors at 1 maltreatment type | 1.50** | [1.13, 2.00] | 1.15** | [1.06, 1.26] | 1.74** | [1.67, 5.42] | 0.69 | ||
| Sum of problem behaviors at 2+ maltreatment types | 2.66** | [1.28, 4.01] | 1.33** | [1.12, 1.58] | 3.01** | [1.67, 5.42] | 0.78 | ||
Note: All models estimate separate equations with causal effects estimated for a change in the treatment from 0 to 1 with the mediator set at 1 and at the mean level of covariates or for a change in the treatment from 0 to 2 with the mediator set at 1 and at the mean level of covariates. All models control for focal participant’s gender, race/ethnicity, age at baseline; highest education level of a parent, primary guardian’s age at first birth, and residential arrest rate at baseline. Sample sizes for each estimated equation are a result of listwise deletion: alcohol use (n = 732), drug use (n = 732), delinquency (n = 732), aggression (n = 670), sum of antisocial behaviors (n = 670), high school dropout (n = 731), teenage parenthood (n = 724), independent living (n = 724), sum of precocious transitions (n = 718), sum of antisocial behaviors and precocious transitions (n = 658). HR, hazard ratio. CI, confidence interval.
p<.10.
p<.05.
p<.01 (two-tailed tests).
Analyses by timing of maltreatment
Among the childhood-limited sample, maltreatment victimization did not significantly affect the likelihood of maltreatment perpetration with a hazard ratio of 1.41 (95% CI [0.96, 2.07]), after adjusting for our control variables.6 Among the adolescent maltreatment sample, maltreatment victimization significantly increased the likelihood of maltreatment perpetration and each additional type of maltreatment experienced increased this risk with a hazard ratio of 1.89 (95% CI [1.39, 2.57]).
Next, we examined Path a in the mediation model for childhood-limited maltreatment and adolescent maltreatment samples separately. Among the childhood-limited sample, the number of types of maltreatment was related to increased parent-reported aggression (OR = 1.39, 95% CI [1.01, 1.92]) and dropping out of high school (OR = 1.49, 95% CI [1.08, 2.04]). It was also related to the total number of precocious transitions (RRR = 1.17, 95% CI [1.01, 1.36]) and the total number of problem behaviors plus precocious transitions (RRR = 1.16, 95% CI [1.04, 1.29]). Among the adolescent maltreatment sample, the number of types of maltreatment was significantly related to self-reported alcohol use (OR 1.5, 95% CI [1.05, 2.30]), drug use (OR = 1.56, 95% CI [1.08, 2.25]), delinquency (OR = 1.78, 95% CI [1.25, 2.25]), and the summated score of adolescent problem behaviors (RRR = 1.34, 95% CI [1.14, 1.58]). The number of maltreatment types during adolescence was also significantly related to dropping out of high school (OR = 2.49, 95% CI [1.62, 3.85]), independent living (OR = 1.77, 95% CI [1.11, 2.82]), the total number of precocious transitions (RRR = 1.30, 95% CI [1.12, 1.51]), and the total number of precocious transitions plus problem behaviors (RRR = 1.31, 95% CI [1.16, 1.48]).
Examining the Path b in the mediation model, self-reported alcohol use (HR = 2.15, 95% CI [1.33, 3.49]), drug use (HR = 2.09, 95% CI [1.29, 3.38]), delinquency (HR = 2.07, 95% CI [1.31, 3.29]) and the total number of problem behaviors (HR = 1.35, 95% CI [1.13, 1.61]) increased the likelihood of engaging in maltreating behaviors among the childhood-limited sample. Moreover, each precocious transition (high school dropout HR = 3.73, 95% CI [2.12, 6.55]; teenage parenthood HR = 2.55, 95% CI [1.54, 4.202]; independent living HR = 3.09, 95% CI [1.67, 5.70]), the total number of precocious transitions (HR 2.19, 95% CI [1.70, 2.83]), and the total number of problem behaviors plus precocious transitions (HR 1.42, 95% CI [1.25, 1.62]) increased the likelihood of maltreatment perpetration among the childhood-limited sample. Of note, the same pattern of results emerged for the adolescent maltreatment sample, with the exception of teenage parenthood, which was not related to the likelihood of maltreatment perpetration.
After establishing the significant paths among the childhood-limited and adolescent maltreatment samples, we assessed the mediation hypotheses (Table 3 and 4). Once again, we note that each row represents a separate equation, including all control variables. Among the childhood-limited maltreatment sample, one type of maltreatment victimization did not exert a significant ( p<.05) controlled direct effect total effect on maltreatment perpetration in any model estimated. In addition, no significant mediating pathways were identified. With respect to two types of maltreatment victimization, there is evidence of a controlled direct effect between two or more types of maltreatment victimization and subsequent perpetrating behaviors. There is also evidence that dropping out of high school, the total number of precocious transitions, and the total number of problem behaviors partially mediate the relationship between two or more types of maltreatment victimization and subsequent perpetration among childhood victims of maltreatment but the total effect was not significant ( p<.05).3
Table 3.
Cox proportional hazard model results of direct and indirect effects of childhood-limited maltreatment victimization on perpetration
| Controlled direct effect |
Natural indirect effect |
Total effect |
Proportion mediated estimate | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mediator | HR | 95% CI | HR | 95% CI | HR | 95% CI | |||
| Antisocial behaviors | |||||||||
| Alcohol use at 1 maltreatment type | 1.40+ | [0.97, 2.04] | 1.03 | [0.97, 1.10] | 1.45+ | [0.99, 2.11] | 0.10 | ||
| Alcohol use at 2+ maltreatment types | 1.97** | [1.36, 2.86] | 1.07 | [0.94, 4.15] | 2.10+ | [0.99, 4.48] | 0.12 | ||
| Drug use at 1 maltreatment type | 1.39+ | [0.96, 2.02] | 1.03 | [0.97, 1.09] | 1.43+ | [0.99, 2.09] | 0.09 | ||
| Drug use at 2+ maltreatment types | 1.94** | [1.34, 2.81] | 1.06 | [0.94, 1.19] | 2.06+ | [0.97, 4.36] | 0.11 | ||
| Delinquency at 1 maltreatment type | 1.39+ | (0.96, 2.01] | 1.03 | [0.97, 1.09] | 1.42+ | [0.98, 2.07] | 0.09 | ||
| Delinquency at 2+ maltreatment types | 1.92** | [1.33, 2.79] | 1.06 | [0.94, 1.19] | 2.03+ | [0.96, 4.32] | 0.11 | ||
| Aggression at 1 maltreatment type | 1.38 | [0.93, 2.03] | 1.03 | [0.98, 1.07] | 1.41+ | [0.96, 2.08] | 0.08 | ||
| Aggression at 2+ maltreatment types | 1.89** | [1.28, 2.79] | 1.05 | [0.95, 1.16] | 1.99+ | [0.92, 4.33] | 0.10 | ||
| Sum of antisocial at 1 maltreatment type | 1.36 | [0.92, 2.02] | 1.04 | [0.98, 1.11] | 1.42+ | [0.95, 2.12] | 0.61 | ||
| Sum of antisocial at 2+ maltreatment types | 1.85 | [0.84, 4.09] | 1.09 | [0.97, 1.23] | 2.02+ | [0.91, 4.48] | 0.69 | ||
| Precocious transitions | |||||||||
| High school dropout at 1 maltreatment type | 1.31 | [0.90, 1.90] | 1.12* | [1.02, 1.24] | 1.47+ | [1.00, 2.15] | 0.34 | ||
| High school dropout at 2+ maltreatment types | 1.71** | [1.17, 2.48] | 1.24* | [1.05, 1.47] | 2.12+ | [0.99, 4.53] | 0.37 | ||
| Teenage parenthood at 1 maltreatment type | 1.39+ | [0.96, 2.01] | 1.03 | [0.96, 1.11] | 1.44+ | [0.99, 2.07] | 0.11 | ||
| Teenage parenthood at 2+ maltreatment types | 1.93** | [1.34, 2.79] | 1.07 | [0.92, 1.25] | 2.07+ | [0.98, 4.37] | 0.13 | ||
| Independent living at 1 maltreatment type | 1.32 | [0.91, 1.90] | 1.02 | [0.97, 1.09] | 1.35 | [0.93, 1.95] | 0.09 | ||
| Independent living at 2+ maltreatment types | 1.73** | [1.20, 2.50] | 1.05 | [0.92, 1.20] | 1.82 | [0.87, 3.81] | 0.11 | ||
| Sum of precocious at 1 maltreatment type | 1.25 | [0.86, 1.81] | 1.11* | [1.00, 1.22] | 1.38+ | [0.94, 2.02] | 0.66 | ||
| Sum of precocious at 2+ maltreatment types | 1.55 | [0.74, 3.26] | 1.23* | [1.01, 1.49] | 1.90+ | [0.89, 4.07] | 0.72 | ||
| Sum of problem behaviors at 1 maltreatment type | 1.29 | [0.86, 1.94] | 1.10* | [1.00, 1.20] | 1.42† | [0.94, 2.14] | 0.65 | ||
| Sum of problem behaviors at 2+ maltreatment types | 1.67 | [0.74, 3.75] | 1.21* | [1.01, 1.45] | 2.01† | [0.87, 4.58] | 0.72 | ||
Note: All models estimate separate equations with causal effects estimated for a change in the treatment from 0 to 1 with the mediator set at 1 and the mean level of all other covariates and for a change in the treatment from 0 to 2 types of maltreatment with the mediator set at 1 and at the mean level of all other covariates. All models control for focal participant’s gender, race/ethnicity, age at baseline; highest education level of a parent, primary guardian’s age at first birth, and residential arrest rate at baseline. Sample sizes for each estimated equation in the childhood-limited maltreatment analysis are as follows: alcohol use (n = 676), drug use (n = 676), delinquency (n = 676), aggression (n = 625), sum of antisocial behaviors (n = 625), high school dropout (n = 675), teenage parenthood (n = 669), independent living (n = 669), sum of precocious transitions (n = 663), sum of antisocial behaviors and precocious transitions (n = 614). Sample sizes for each estimated equation in the adolescent maltreatment analysis are as follows: alcohol use (n = 655), drug use (n = 655), delinquency (n = 655), aggression (n = 597), sum of antisocial behaviors (n = 597), high school dropout (n = 653), teenage parenthood (n = 648), independent living (n = 648), sum of precocious transitions (n = 642), sum of antisocial behaviors and precocious transitions (n = 586). All models control for focal participant’s gender, race/ethnicity, age at baseline; highest education level of a parent, primary guardian’s age at first birth, and residential arrest rate at baseline. HR, hazard ratio. CI, confidence interval.
†p<.10.
p<.05.
p<.01 (two-tailed tests).
Table 4.
Cox proportional hazard model results of direct and indirect effects of adolescent maltreatment victimization on perpetration
| Controlled direct effect |
Natural indirect effect |
Total effect |
Proportion mediated estimate | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mediator | HR | 95% CI | HR | 95% CI | HR | 95% CI | |||
| Antisocial behaviors | |||||||||
| Alcohol use at 1 maltreatment type | 1.86** | [1.32, 2.52] | 1.10† | [0.99, 1.22] | 2.01** | [2.07, 7.97] | .18 | ||
| Alcohol use at 2+ maltreatment types | 3.33** | [2.41, 4.61] | 1.22† | [0.98, 1.51] | 4.06** | [2.07, 7.97] | .24 | ||
| Drug use at 1 maltreatment type | 1.77** | [1.27, 2.45] | 1.10† | [1.00, 1.22] | 1.95** | [1.94, 7.49] | .19 | ||
| Drug use at 2+ maltreatment types | 3.12** | [2.24, 4.33] | 1.22* | [1.00, 1.49] | 3.81** | [1.94, 7.49] | .25 | ||
| Delinquency at 1 maltreatment type | 1.74** | [1.25, 2.43] | 1.11† | [1.01, 1.22] | 1.94** | [1.39, 2.73] | .21 | ||
| Delinquency at 2+ maltreatment types | 3.04** | [2.18, 4.24] | 1.25* | [1.02, 1.51] | 3.80** | [1.94, 7.43] | .27 | ||
| Aggression at 1 maltreatment type | 1.84** | [1.25, 2.43] | 1.05 | [0.97, 1.12] | 1.92** | [1.31, 2.82] | .09 | ||
| Aggression at 2+ maltreatment types | 3.37** | [2.30, 4.93] | 1.10 | [0.95, 1.26] | 3.70** | [1.71, 8.00] | .69 | ||
| Sum of antisocial at 1 maltreatment type | 1.71** | [1.16, 2.52] | 1.14** | [1.02, 1.26] | 1.95** | [1.31, 2.89] | .69 | ||
| Sum of antisocial at 2+ maltreatment types | 2.93** | [1.35, 6.37] | 1.29* | [1.04, 1.59] | 3.78** | [1.72, 8.32] | .81 | ||
| Precocious transitions | |||||||||
| High school dropout at 1 maltreatment type | 1.58* | [0.90, 1.90] | 1.26** | [1.11, 1.43] | 1.99** | [1.42, 2.81] | .41 | ||
| High school dropout at 2+ maltreatment types | 2.50** | [1.17, 2.48] | 1.46* | [1.23, 1.73] | 3.66** | [1.88, 7.13] | .44 | ||
| Teenage parenthood at 1 maltreatment type | 2.08** | [0.96, 2.01] | 1.08 | [0.96, 1.21] | 2.24** | [1.57, 3.20] | .13 | ||
| Teenage parenthood at 2+ maltreatment types | 4.34** | [1.34, 2.79] | 1.16 | [0.91, 1.47] | 5.06** | [2.47, 10.33] | .18 | ||
| Independent living at 1 maltreatment type | 1.91** | [0.91, 1.90] | 1.12† | [0.99, 1.26] | 2.14** | [1.49, 3.06] | .20 | ||
| Independent living at 2+ maltreatment types | 3.66** | [1.20, 2.50] | 1.30† | [0.96, 1.76] | 4.76** | [2.27, 9.99] | .29 | ||
| Sum of precocious at 1 maltreatment type | 1.68** | [0.86, 1.81] | 1.32** | [1.14, 1.54] | 2.22** | [1.54, 3.20] | .75 | ||
| Sum of precocious at 2+ maltreatment types | 2.81** | [0.74, 3.26] | 1.75** | [1.29, 2.36] | 4.92** | [2.37, 10.21] | .86 | ||
| Sum of problem behaviors at 1 maltreatment type | 2.81** | [0.86, 1.94] | 1.31** | [1.12, 1.54] | 2.16** | [1.42, 3.29] | .75 | ||
| Sum of problem behaviors at 2+ maltreatment types | 2.71* | [1.22, 6.01] | 1.72** | [1.25, 2.38] | 4.67** | [2.01, 10.81] | .85 | ||
Note: All models estimate separate equations with causal effects estimated for a change in the treatment from 0 to 1 with the mediator set at 1 and the mean level of all other covariates and for a change in the treatment from 0 to 2 types of maltreatment with the mediator set at 1 and at the mean level of all other covariates. All models control for focal participant’s gender, race/ethnicity, age at baseline; highest education level of a parent, primary guardian’s age at first birth, and residential arrest rate at baseline. Sample sizes for each estimated equation in the childhood-limited maltreatment analysis are as follows: alcohol use (n = 676), drug use (n = 676), delinquency (n = 676), aggression (n = 625), sum of antisocial behaviors (n = 625), high school dropout (n = 675), teenage parenthood (n = 669), independent living (n = 669), sum of precocious transitions (n = 663), sum of antisocial behaviors and precocious transitions (n = 614). Sample sizes for each estimated equation in the adolescent maltreatment analysis are as follows: alcohol use (n = 655), drug use (n = 655), delinquency (n = 655), aggression (n = 597), sum of antisocial behaviors (n = 597), high school dropout (n = 653), teenage parenthood (n = 648), independent living (n = 648), sum of precocious transitions (n = 642), sum of antisocial behaviors and precocious transitions (n = 586). All models control for focal participant’s gender, race/ethnicity, age at baseline; highest education level of a parent, primary guardian’s age at first birth, and residential arrest rate at baseline. HR, hazard ratio. CI, confidence interval.
p<.10.
p<.05.
p<.01 (two-tailed tests).
Among the adolescent maltreatment sample, there was a significant direct effect of both one and two or more types of maltreatment victimization on the likelihood of maltreatment perpetration in each model estimated. Moreover, there was evidence of mediation as adolescent drug use and delinquency partially mediated the effect of two or more types of maltreatment victimization on subsequent perpetration, accounting for 25% and 27% of the total effect, respectively. The total number of adolescent problem behaviors mediated 69% of the total effect of one type of maltreatment victimization on maltreatment perpetration and 81% of the total effect of two or more types of maltreatment victimization on subsequent perpetration. Dropping out of high school mediated part of the cycle of maltreatment, accounting for 41% of the effect of one type of maltreatment type on maltreatment perpetration and 44% of two or more types of maltreatment victimization on perpetration. The total number of precocious transitions and the total number of adolescent problem behaviors plus precocious transitions also served as mediators of the cycle of maltreatment, accounting for over three-quarters of the relationship between one type of maltreatment victimization on subsequent perpetrating behaviors and two or more types of maltreatment victimization on subsequent perpetration.
Discussion
Child abuse and neglect are serious and pervasive societal problems in America (Institute of Medicine and National Research Council, 2014), and it is imperative that we fully understand the developmental processes that lead some adults, primarily parents, to become involved in maltreating behaviors. Doing so is essential to developing firm theoretical models of the origins of maltreatment and to developing effective prevention programs to reduce maltreatment and increase the likelihood that all youth will experience safe, stable, and nurturing environments.
One important developmental path to maltreatment perpetration is experiencing maltreatment victimization as a youth. As shown here, maltreatment is, to some extent, reproduced across the generations, a finding consistent with other intergenerational studies (e.g., Jaffee et al., 2013; Schofield, Lee, & Merrick, 2013; Widom et al., 2015). Yet identifying this main effect is just the beginning of the scientific task before us. We are still left with the challenge of identifying the mechanisms that translate a history of maltreatment into an increased likelihood of subsequently engaging in maltreating behaviors. Why should someone maltreated as a child or adolescent be significantly more likely to engage in the same type of inappropriate, maladaptive behavior when he or she becomes a parent or guardian? To this end, we found that experiencing maltreatment increased the risk for engaging in subsequent maladaptive behaviors, and this risk increased with multiple forms of maltreatment. Moreover, we identified two unique, yet overlapping developmental pathways that indicate disrupted development, and partially explain why one’s history of maltreatment victimization increases the chances of involvement in later maltreatment perpetration.
One pathway identified was involvement in adolescent problem behaviors. Maltreatment victimization increased alcohol use, drug use, delinquency, aggression, and involvement in multiple forms of problem behavior. In turn, each of these increased the likelihood of engaging in maltreating behaviors as an adult. Moreover, high levels of delinquency served as a significant mediator of the cycle of maltreatment, as did the total number of problem behaviors; the latter accounted for a greater proportion of the effect of maltreatment victimization on maltreatment perpetration (65% for the summed problem behaviors vs. 13% for delinquency alone for one type of maltreatment and 75% for the summed problem behaviors vs. 17% for delinquency alone for two or more types of maltreatment). Overall parents and caretakers who display elevated levels of these problem behaviors are at an increased risk of responding to children with a set of behaviors that cross the threshold into the realm of maltreatment.
However, this pathway was only relevant for the full sample and the adolescent maltreatment sample. With the exception of parent-reported aggression, childhood maltreatment victimization was unrelated to the other problem behavior or the total number of problem behaviors. As such, it may be that the long-term negative consequences of childhood maltreatment are likely to manifest in other forms of maladaptation, related to brain development and cognitive functioning, which may provide other pathways to maltreatment perpetration (Institute of Medicine and National Research Council, 2014; Teicher et al., 2003).
The second developmental pathway concerns the timing of transitions as one moves from adolescence to adulthood. The present results suggest that these, too, are important to why maltreatment begets maltreatment. Dropping out of high school, living independent of adult supervision, and experiencing multiple precocious transitions all mediate part of the cycle of maltreatment. Precocious transitions, individually and collectively, have been shown to reduce successful adaptation to major adult roles such as partner, parent, and worker (Elder, 1998), and our results indicate that another explanation for the reproduction of maltreating behaviors flows through precocious transitions to adulthood. Once again, this pattern was stronger and more consistent for adolescent victims of maltreatment, but it was also observed, to some extent, for childhood-limited victims.
While our results contribute to a fuller understanding of the cycle of maltreatment, they are driven primarily by those who experience maltreatment during adolescence. We found weak evidence supporting the cycle of maltreatment among childhood-limited maltreatment victims. Only failing to earn a high school diploma and the total number of antisocial behaviors linked childhood experiences of victimization to perpetration, but the total effect was not significant. These findings are similar in some respects with Thornberry and Henry (2013), who used a binary indicator of maltreatment victimization in childhood. It appears the cycle of maltreatment is largely a function of adolescent maltreatment experiences, which tends to be more severe in nature (e.g., a greater number of substantiated incidents, and incidents are more likely to be related to physical and sexual abuse; Thornberry & Henry, 2013), or marked by maltreatment experiences that extend from childhood to adolescence, which are known to have stronger, more consistent negative consequences through the life course due to their persistence over time (Eckenrode et al., 2001; Stewart et al. 2008; Thornberry et al., 2001). It may also be that the causal pathways explored in this research are temporally closer to adolescent experiences of maltreatment compared to childhood-limited experiences of maltreatment and, therefore, more relevant among adolescent victims. In any case, it is imperative for maltreatment prevention programs to target those who experienced instances of maltreatment during adolescence in order to break the cycle of maltreatment.
Overall, our findings suggest several avenues for future research. In our analysis, the count measures of precocious transitions and problem behaviors accounted for at least 70% of the cycle of maltreatment among the adolescent maltreatment victimization sample. The model that combined all of the mediator variables accounted for at least 75% of the cycle of maltreatment. Thus, an unmediated direct effect of adolescent victimization on perpetration still remains. Clearly, other important influences are at play and pertinent to the understanding of how maltreatment is reproduced across the generations. Expanding the investigation to additional arenas, including genetic risk and protective factors (Stallings et al., 1997), brain development and neurophysiological risk (Shackman & Pollack, 2014; Teicher, Samson, Anderson, & Ohashi, 2016), the broader family environment (Belsky & Jaffee 2006), and economic well-being (Conger, Conger, & Martin, 2010), is another important task for research.
Moreover, adolescent problem behaviors and precocious transitions are themselves interrelated. Involvement in problem behaviors such as high levels of delinquency and substance use increases the likelihood of precocious transitions, and they, in turn, increase the likelihood of continued involvement in problem behaviors (Conger et al., 2010; Krohn, Lizotte, & Perez, 1997). We were not able to examine a more precise mediational model that establishes temporal order among the mediating variables or how these mediators may condition the effect of one another on subsequent perpetration. Examining these more complex developmental pathways is an important next step in order to expand the understanding of the cycle of maltreatment. We also were not able to examine the role of social influences that are more contemporaneous with the perpetration of maltreatment. For example, experiencing precocious transitions and involvement in adolescent problem behaviors promote stressful environments (e.g., unemployment) and negative affective states (e.g., depression) that are related to maltreatment (Belsky & Jaffee, 2006). Therefore, our research is limited as it does not identify the full set of pathways that operate through precocious transitions and problem behaviors. Examining these and other concurrent influences in research will provide a fuller, more comprehensive understanding of the cycle of maltreatment.
The findings reported here contain important information for prevention programming. The significant direct effect of maltreatment victimization on the likelihood of perpetration suggests that programs and services to reduce the chances of maltreatment perpetration should include appropriate screening to identify individuals with a history of victimization, particularly in adolescence, as these victims are at increased risk of engaging in maltreating behaviors (Berlin et al., 2011). In addition, many services for maltreatment victims focus on immediate consequences, but the present findings indicate that maltreatment also has long-term consequences, rippling across to the next generation. Maltreatment programs should be cognizant of long-term consequences and when possible provide services to reduce their likelihood by focusing on potential intervening mechanisms.
Our identification of significant mediating pathways suggests appropriate settings and content for these services. One mediating pathway identified is through increased involvement of maltreated youth in problem behaviors, particularly higher levels of delinquency and involvement in multiple problem behaviors. Youth exhibiting this pattern of behavior (and their families) are often caught up in multiple service systems such as the juvenile justice, child welfare, school, and mental health systems, and we should extend interventions in these settings to incorporate the prevention of later maltreatment perpetration. Moreover, multiproblem youth are likely to become parents and guardians at relatively young ages (Krohn et al., 1997). Youth enmeshed in the juvenile justice and related service systems are potentially important targets for programs with demonstrated effectiveness for preventing adolescent experiences of maltreatment such as the Triple P Positive Parenting Program (Printz, Sanders, Shapiro, Whitaker, & Lutzker, 2009) and parent–child interaction therapy (Chaffin et al., 2004).
Another pathway to maltreatment is through early life course transitions. The strong impact of dropping out of high school deserves special attention. It is possible that this transition is driven, at least in part, by an inability to cope with daily life stressors and responsibilities that befall a high school student. This is likely an early sign that these same individuals will struggle when given the responsibilities of childcare. As such, programs that promote positive parenting strategies and coping mechanisms in time of stress may be beneficial (Chaffin et al., 2004; Printz et al., 2009). These individuals may also struggle in parent or guardianship roles as a result of diminished economic capital, which precludes financial security and stability. For example, the median income for a high school dropout falls below the 2012 poverty standard of $23,050 (US Department of Health and Human Services, 2012). Thus, programs targeting the prevention of precocious transitions such as those designed to prevent youth from dropping out of school or promote educational and economic opportunities for high school dropouts, such as National Guard Work ChalleNGe and Job Corps (see Bloom, 2010, for a review), may have not only short-term benefits (e.g., improving graduation rates and employment) but also long-term benefits such as reducing future maltreatment.
Finally, cumulative risk, as indicated by involvement in multiple problem behaviors and experiencing multiple precocious transitions, significantly increases maltreatment perpetration and mediates a substantial part of the cycle of maltreatment. Theoretically, it is hardly surprising that youth displaying these various behaviors are the most likely to engage in maltreating behaviors, and they are surely the ones most in need of services. Several programs developed for multiple problem youth, including Functional Family Therapy (Alexander & Robbins, 2011), Multisystemic Therapy (Henggeler, Schoenwald, Borduin, Rowland, & Leeb, 2009), and Multidimensional Treatment Foster Care (Chamberlain, 2003), are effective in reducing problem behaviors and precocious transitions and they are cost-effective. It may be wise to extend these and similar programs to specifically target the prevention of future maltreatment.
Although the present investigation emphasized intergenerational continuity in maltreatment, we should not lose sight of the fact that there is also a substantial degree of discontinuity from one generation to the next. Abused children becoming abusers is not a given! Most people who have a history of maltreatment do not go on to become involved in maltreating behaviors. In this study, 84% of the childhood-limited maltreatment victims and 66% of the adolescent maltreatment victims did not subsequently engage in maltreating behaviors, through their middle 30s. This discontinuity represents a substantial degree of resilience. Another important (and understudied) topic is to identify protective factors that may mitigate the risk created by a history of maltreatment victimization (Schofield et al., 2013). Studies of resilience will provide additional information on the cycle of maltreatment and how prevention programs should be structured.
Finally, we acknowledge several limitations to this work. From a statistical perspective, maltreatment is a relatively rare event, and it was not possible to conduct more refined subgroup analyses, for example, for separate types of maltreatment. Relatedly, the Rochester study oversampled males by a ratio of 3 to 1, and given the relatively small number of female participants, we were not able to conduct separate analyses by gender, an important issue because females are somewhat more involved in maltreatment than males, particularly neglect (Institute of Medicine and National Research Council, 2014). In addition, we relied entirely on official measures of substantiated maltreatment, which likely underestimate the level of maltreatment and incorporate unknown biases that may exist in official reporting and recording procedures. Our results are also specific to a particular cohort drawn from a single city, and replicating these mediational pathways in other settings would certainly strengthen their generalizability.
As noted earlier, there are also other pathways that can serve as mediators of the impact of victimization on perpetration; thus, the present analysis does not offer a complete explanation for intergenerational continuity in maltreatment. It investigated two pathways that appear to offer important insights into the cycle of maltreatment but recognizes that future research will have to investigate more comprehensive models. The investigation of these larger models, in general and for various subgroups, will require larger sample sizes than is available in the present study, and in most intergenerational studies (Thornberry, 2016).
Despite these limitations, the current investigation makes significant contributions to our understanding of the processes by which child maltreatment is reproduced across successive generations. Specifically, it identified two important pathways, adolescent problem behaviors and precocious transitions, that link a history of maltreatment victimization to an increased likelihood of involvement in maltreatment perpetration. The maltreatment of youth, particularly adolescents, creates cascading negative consequences in the victim’s development, and in turn, those consequences increase the chances that maltreating behaviors will be repeated against future generations. Fortunately, identifying these processes increases our understanding of how the cycle of maltreatment works and, therefore, how we can intervene to break that cycle. Clearly, it will not be an easy or straightforward task to prevent maltreatment, but we hope that this investigation contributes to that objective. Only by persistently addressing this problem will we be able to make progress in our efforts to keep our youth safe from harm.
Acknowledgments
Support for the Rochester Youth Development Study has been provided by National Institute on Drug Abuse Grant R01DA020195 and Centers for Disease Control and Prevention Grant R01CE001572. Work on this project was also aided by grants to the Center for Social and Demographic Analysis at the University at Albany (NICHD Grant P30HD32041 and NSF Grant SBR-9512290). Points of view or opinions in this document are those of the authors and do not necessarily represent the official position or policies of the funding agencies.
We would like to thank the New York State Office of Children and Family Services for their assistance in collecting the Child Protective Services data.
Appendix A. Correlation Matrix
| 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. | 9. | 10. | 11. | 12. | 13. | 14. | 15. | 16. | 17. | 18. | 19. | 20. | 21. | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. | 1 | ||||||||||||||||||||
| 2. | .14** | 1 | |||||||||||||||||||
| 3. | .06 | — | 1 | ||||||||||||||||||
| 4. | .18** | — | — | 1 | |||||||||||||||||
| 5. | .16** | .07* | .05 | .06 | 1 | ||||||||||||||||
| 6. | .16** | .09** | .04 | .09* | .62** | 1 | |||||||||||||||
| 7. | .17** | .09** | .04 | .12** | .44** | .43** | 1 | ||||||||||||||
| 8. | .12** | .15** | .11** | .12** | .21** | .28** | .17** | 1 | |||||||||||||
| 9. | .16** | .10** | .06 | .10* | .79** | .79** | .70** | .52** | 1 | ||||||||||||
| 10. | .22** | .15** | .08* | .16** | .25** | .32** | .21** | .22** | .32** | 1 | |||||||||||
| 11. | .23** | .07* | .01 | .11** | .10** | .09** | .13** | .02 | .09* | .22** | 1 | ||||||||||
| 12 | .23.** | .09** | .02 | .14** | .16** | .17** | .09** | .08* | .15** | .21** | .28** | 1 | |||||||||
| 13. | .32** | .15** | .06 | .19** | .25** | .29** | .21** | .17** | .29** | .76** | .72** | .59** | 1 | ||||||||
| 14. | .26** | .14** | .08* | .16** | .68** | .71** | .60** | .46** | .87** | .61** | .43** | .38** | .71** | 1 | |||||||
| 15. | .07 | .07 | .02 | .09* | 2.00 | 2.01 | .10** | 2.02 | .03 | .04 | .14** | .03 | .11** | .08* | 1 | ||||||
| 16. | .12** | 2.05 | 2.02 | 2.06 | 2.05 | 2.02 | 2.09** | .00 | 2.03 | 2.19** | 2.20** | 2.16** | 2.26** | 2.15** | 2.24** | 1 | |||||
| 17. | −.08* | −.06 | 2.03 | 2.06 | 2.01 | 2.00 | 2.03 | 2.06 | 2.04 | 2.13** | 2.14** | 2.09* | 2.17** | 2.13** | 2.11** | .28** | 1 | ||||
| 18. | .07* | −.12** | 2.00 | 2.20** | .15** | ** | .05 | 2.00 | .11** | .03 | 2.22 | 2.08* | 2.14** | .02 | .15** | .07 | .09* | 1 | |||
| 19. | .10** | .04 | .01 | .06 | 2.07* | 2.01 | .02 | 2.03 | 2.03 | 2.06 | 2.09 | 2.06 | 2.01 | 2.02 | .25** | .06 | 2.17** | 2.18** | 1 | ||
| 20. | −.04 | −.09* | 2.08* | 2.05 | .06 | .00 | .03 | 2.07 | .01 | .09** | .08* | .11** | .13** | .05 | .03 | 2.28** | 2.04 | .06 | 2.65** | 1 | |
| 21. | .10** | .03 | .02 | .02 | .23** | .19** | .14** | 2.01 | .19** | .27** | .03 | .16** | .22** | .24** | .05 | 2.16** | 2.09* | .05 | .08* | 1 | |
| 1. Maltreatment perpetration | |||||||||||||||||||||
| 2. Number of maltreatment types | 12. Independent living | ||||||||||||||||||||
| 3. Number of maltreatment types—Childhood only | 14. Sum of antisocial behaviors and precocious transitions | ||||||||||||||||||||
| 4. Number of maltreatment types—Adolescence | 13. Sum of precocious transitions | ||||||||||||||||||||
| 5. Alcohol use | 15. Community arrest rate | ||||||||||||||||||||
| 6. Drug use | 16. Parent education | ||||||||||||||||||||
| 7. Delinquency | 17. Parent age at first birth | ||||||||||||||||||||
| 8. Aggression | 18. Male | ||||||||||||||||||||
| 9. Sum of antisocial behaviors | 19. Black | ||||||||||||||||||||
| 10. High school dropout | 20. Hispanic | ||||||||||||||||||||
| 11. Teenage parenthood | 21. Age at baseline | ||||||||||||||||||||
p<.05.
p<.01.
Footnotes
For simplicity, we will typically use the term “parent” instead of “parent, guardian, caretaker, and so on” throughout this paper. This reflects the fact that approximately 80% of the perpetrators of maltreatment are either biological or stepparents (Institute of Medicine and National Research Council, 2014). In our empirical analyses, we include all adult sample members to be comprehensive and to reflect the fact that although maltreatment is primarily a parental behavior, it is not limited to parents but includes other adult guardians as well.
Among the sample, 65 participants without a maltreatment record had five or fewer years of residence in New York State during the childhood developmental period (i.e., birth through age 11) or 3 or fewer years of residence in New York State during the adolescent developmental period (i.e., age 12 to age 18). Because these individuals spent a shorter period of time in New York State, we could not be confident about their status regarding the number of types of maltreatment experienced. Additional analyses were performed removing these individuals from the analytic sample, and the results remained the same.
If the participant indicated that he or she lived in an educational dormitory setting through the age of 18, then he or she was not classified as experiencing this precocious transition.
We measure involvement in problem behaviors between the ages of 16 and 18 for consistency in measurement as this is after the vast majority of first experiences of maltreatment victimization, and it is when the majority of precocious transitions were also experienced.
The analyses presented use an ordinal indicator of the number of types of maltreatment. Additional analyses were performed using a binary indicator of maltreatment victimization (i.e., any substantiated incident of maltreatment victimization based on OCFS records) and the results were the same in direction and significance.
For the models presented, participants who only experienced maltreatment in adolescence were coded as missing for the childhood-limited maltreatment analysis and participants who experienced childhood-limited maltreatment were coded missing for the adolescent maltreatment analysis. Additional analyses were performed where adolescent maltreatment participants were coded as 0 for the childhood-limited maltreatment analysis and participants who experienced childhood-limited maltreatment were coded as 0 for the adolescent maltreatment analysis. The results were substantively similar in direction and significance.
References
- Achenbach TM (1991). Manual for the Child Behavior Checklist/4–18 and 1991 Profile Burlington, VT: University of Vermont, Department of Psychology. [Google Scholar]
- Alexander JF, & Robbins MS (2011). Functional family therapy New York: Springer. [Google Scholar]
- Allwood MA, & Widom CS (2013). Child abuse and neglect, developmental role attainment, and adult arrests. Journal of Research in Crime and Delinquency, 50, 551–578. [Google Scholar]
- Augustyn MB, Thornberry TP, & Krohn MD (2014). Gang membership and pathways to maladaptive parenting. Journal of Research on Adolescence, 24, 252–267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baron RM, & Kenny DA (1986). The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51, 1173. [DOI] [PubMed] [Google Scholar]
- Belsky J, & Jaffee SR (2006). The multiple determinants of parenting. In Cicchetti D & Cohen DJ (Eds.), Developmental psychopathology: Risk, disorder and adaptation (pp. 38–75). New York: Wiley. [Google Scholar]
- Belsky J, Ruttle PL, Boyce WT, Armstrong JM, & Essex MJ (2015). Early adversity, elevated stress physiology, accelerated sexual maturation, and poor health in females. Developmental Psychology, 51, 816. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berlin LJ, Appleyard K, & Dodge KA (2011). Intergenerational continuity in child maltreatment: Mediating mechanisms and implications for prevention. Child Development, 82, 162–176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bloom D (2010). Transitional jobs: Background, program models, and evaluation evidence New York: Manpower Demonstration Research Corporation; Retrieved from http://files.eric.ed.gov/fulltext/ED509317.pdf [Google Scholar]
- Blumstein A, Cohen J, Roth JA, &, Visher CA (1986). Criminal careers and “career criminals” (Vol. 2). Washington, DC: National Academies Press. [Google Scholar]
- Brooks-Gunn J, & Chase-Lansdale L (1995). Adolescent parenthood. In Bornstein MH (Ed.), Handbook of parenting: Vol. 3. Status and social conditions of parenting Hillsdale, NJ: Erlbaum. [Google Scholar]
- Brown J, Cohen P, Johnson JG, & Salzinger S (1998). A longitudinal analysis of risk factors for child maltreatment: Findings of a 17-year prospective study of officially recorded and self-reported child abuse and neglect. Child Abuse & Neglect, 22, 1065–1078. [DOI] [PubMed] [Google Scholar]
- Bushway SD, Krohn MD, Lizotte AJ, Phillips MD, & Schmidt NM (2013). Are risky youth less protectable as they age? The dynamics of protection during adolescence and young adulthood. Justice Quarterly, 30, 84–116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Capaldi DM, Kim HK, & Pears KC (2009). The association between partner violence and child maltreatment: A common conceptual framework. In Whitaker DJ & Lutzker JR (Eds.), Preventing partner violence (pp. 93–111). Washington, DC: American Psychological Association. [Google Scholar]
- Cash SJ, & Wilke DJ (2003). An ecological model of maternal substance abuse and child neglect: Issues, analyses, and recommendations. American Journal of Orthopsychiatry, 73, 392–404. [DOI] [PubMed] [Google Scholar]
- Chaffin M, Kelleher K, & Hollenberg J (1996). Onset of physical abuse and neglect: Psychiatric, substance abuse, and social risk factors from prospective community data. Child Abuse & Neglect, 20, 191–203. [DOI] [PubMed] [Google Scholar]
- Chaffin M, Silovsky JF, Funderburk B, Valle LA, Brestan EV, Balachova T, … Bonner BL (2004). Parent-child interaction therapy with physically abusive parents: Efficacy for reducing future abuse reports. Journal of Consulting and Clinical Psychology, 72, 500. [DOI] [PubMed] [Google Scholar]
- Chamberlain P (2003). Treating chronic juvenile offenders: Advances made through the Oregon multidimensional treatment foster care model Washington DC: American Psychological Association. [Google Scholar]
- Cicchetti D (2004). An odyssey of discovery: lessons learned through three decades of research on child maltreatment. American Psychologist, 59(8), 731. [DOI] [PubMed] [Google Scholar]
- Cicchetti D, & Toth SL (2005). Child maltreatment. Annual Review Clinical Psychology, 1, 409–438. [DOI] [PubMed] [Google Scholar]
- Claussen AH, & Crittenden PM (1991). Physical and psychological maltreatment: Relations among types of maltreatment. Child Abuse & Neglect, 15, 5–18. [DOI] [PubMed] [Google Scholar]
- Clemmons JC, Walsh K, DiLillo D, & Messman-Moore TL (2007). Unique and combined contributions of multiple child abuse types and abuse severity to adult trauma symptomatology. Child Maltreatment, 12, 172–181. [DOI] [PubMed] [Google Scholar]
- Conger RD, Conger KJ, & Martin MJ (2010). Socioeconomic status, family processes, and individual development. Journal of Marriage and Family, 72, 685–704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conger RD, Schofield TJ, Neppl TK, & Merrick MT (2013). Disrupting intergenerational continuity in harsh and abusive parenting: The importance of a nurturing relationship with a romantic partner. Journal of Adolescent Health, 53, S11–S17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cox CE, Kotch JB, & Everson MD (2003). A longitudinal study of modifying influences in the relationship between domestic violence and child maltreatment. Journal of Family Violence, 18, 5–17. [Google Scholar]
- Dishion TJ, Capaldi DM, & Yoerger K (1999). Middle childhood antecedents to progressions in male aadolescent substance use: An ecological analysis of risk and protection. Journal of Adolescent Research, 14, 175–205. [Google Scholar]
- Dixon L, Browne K, & Hamilton-Giachritsis C (2005). Risk factors of parents abused as children: A mediational analysis of the intergenerational continuity of child maltreatment (Part I). Journal of Child Psychology and Psychiatry, 46, 47–57. [DOI] [PubMed] [Google Scholar]
- Eckenrode J, Powers J, Doris J, Munsch J, & Bolger N (1988). Substantiation of child abuse and neglect reports. Journal of Consulting and Clinical Psychology, 56, 9–16. [DOI] [PubMed] [Google Scholar]
- Eckenrode J, Sielinski D, Smith E, Marcynyszyn LA, Henderson CR Jr., Kitzman H, … Olds DL (2001). Child maltreatment and the early onset of problem behaviors: Can a program of nurse home visitation break the link? Development and Psychopathology, 13, 873–890. [PubMed] [Google Scholar]
- Elder GH Jr. (1985). Perspectives on the life course. In Elder GH Jr. (Ed.), Life course dynamics New York: Cornell University Press. [Google Scholar]
- Elder GH Jr. (1998). The life course as developmental theory. Child Development, 69, 1–12. [PubMed] [Google Scholar]
- Elliott DS, Huizinga D, & Menard S (1989). Research in criminology. Multiple problem youth: Delinquency, substance use, and mental health problems New York: Wiley. [Google Scholar]
- English DJ, Upadhyaya MP, Litrownik AJ, Marshall JM, Runyan DK, Graham JC, & Dubowitz H (2005). Maltreatment’s wake: The relationship of maltreatment dimensions to child outcomes. Child Abuse & Neglect, 29, 597–619. [DOI] [PubMed] [Google Scholar]
- Fagan AA (2005). The relationship between adolescent physical abuse and criminal offending: Support for an enduring and generalized cycle of violence. Journal of Family Violence, 20, 279–290. [Google Scholar]
- Fals-Stewart W, Kelley ML, Fincham FD, Golden J, & Logsdon T (2004). Emotional and behavioral problems of children living with drug-abusing fathers: Comparisons with children living with alcohol-abusing and non-substance-abusing fathers. Journal of Family Psychology, 18, 319–330. [DOI] [PubMed] [Google Scholar]
- Fang X, Brown DS, Florence CS, & Mercy JA (2012). The economic burden of child maltreatment in the United States and implications for prevention. Child Abuse & Neglect, 36, 156–165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Farnworth M, Thornberry TP, Krohn MD, & Lizotte AJ (1994). Measurement in the study of class and delinquency: Integrating theory and research. Journal of Research in Crime and Delinquency, 31, 32–61. [Google Scholar]
- Farrington DP, & Loeber R (2000). Some benefits of dichotomization in psychiatric and criminological research. Criminal Behavior and Mental Health, 10, 100–122. [Google Scholar]
- Foster H, Hagan J, & Brooks-Gunn J (2008). Growing up fast: Stress exposure and subjective “weathering” in emerging adulthood. Journal of Health and Social Behavior, 49, 162–177. [DOI] [PubMed] [Google Scholar]
- Gilbert R, Widom CS, Browne K, Fergusson D, Webb E, & Janson S (2009). Burden and consequences of child maltreatment in high-income countries. Lancet, 373, 68–81. [DOI] [PubMed] [Google Scholar]
- Gottfredson MR, & Hirschi T (1990). A general theory of crime Stanford, CA: Stanford University Press. [Google Scholar]
- Hagan J, & Foster H (2001). Youth violence and the end of adolescence. American Sociological Review, 66, 874–899. [Google Scholar]
- Hatch SL (2005). Conceptualizing and identifying cumulative adversity and protective resources: Implications for understanding health inequalities. Journal of Gerontology Series B: Psychological Sciences and Social Sciences, 60, S130–S134. [DOI] [PubMed] [Google Scholar]
- Heckman JJ, Humphries JE, & Kautz T (Eds.) (2015). The myth of achievement tests: The GED and the role of character in American life Chicago, IL: University of Chicago Press. [Google Scholar]
- Henggeler SW, Schoenwald SK, Borduin CM, Rowland MD, & Cunningham PB (2009). Multisystemic therapy for antisocial behavior in children and adolescents (2nd ed.). New York: Guilford Press. [Google Scholar]
- Hinshaw SP (2013). Developmental psychopathology as a scientific discipline. In Beauchaine TP & HInshaw SP (Eds.), Child and Adolescent psychopathology (pp. 3–28). Hoboken, NJ: Wiley. [Google Scholar]
- Institute of Medicine and National Research Council. (2004). Children’s health, the nation’s wealth: Assessing and improving child health Washington, DC: National Academies Press. [Google Scholar]
- Institute of Medicine and National Research Council. (2014). New directions in child abuse and neglect research Washington, DC: National Academies Press. [PubMed] [Google Scholar]
- Jaffee SR, Bowes L, Ouellet-Morin I, Fisher HL, Moffitt TE, & Merrick MT (2013). Safe, stable, nurturing relationships break the intergenerational cycle of abuse: A prospective nationally representative cohort of children in the United Kingdom. Journal of Adolescent Health, 53, S4–S10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jonson-Reid M, & Barth R (2000). From maltreatment report to juvenile incarceration: The role of child welfare services. Child Abuse & Neglect, 24, 505–520. [DOI] [PubMed] [Google Scholar]
- Jonson-Reid M, Kohl PL, & Drake B (2012). Child and adult outcomes of chronic child maltreatment. Pediatrics, 129, 839–845. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kane JB, Morgan SP, Harris KM, & Guilkey DK (2013). The educational consequences of teen childbearing. Demography, 50, 2129–2150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaplow JB, & Widom KS (2007). Age of onset of child maltreatment predicts long-term mental health outcomes. Journal of Abnormal Psychology, 116, 176–187. [DOI] [PubMed] [Google Scholar]
- Keiley MK, Howe TR, Dodge KA, Bates JE, & Pettit GS (2001). The timing of child physical maltreatment: A cross-domain growth analysis of impact on adolescent externalizing and internalizing problems. Development and Psychopathology, 13, 891–912. [PMC free article] [PubMed] [Google Scholar]
- Kendall-Tackett KA, & Eckenrode J (1996). The effects of neglect on academic achievement and disciplinary problems: A developmental perspective. Child Abuse & Neglect, 20, 161–169. [DOI] [PubMed] [Google Scholar]
- Kim J (2009). Type-specific intergenerational transmission of neglectful and physically abusive parenting behaviors among young parents. Children and Youth Services Review, 31, 761–767. [Google Scholar]
- Krohn MD, Lizotte AJ, & Perez CM (1997). The interrelationship between substance use and precocious transitions to adult statuses. Journal of Health and Social Behavior, 38, 87–103. [PubMed] [Google Scholar]
- Lange T, & Hansen JV (2011). Direct and indirect effects in a survival context. Epidemiology, 22, 575–581. [DOI] [PubMed] [Google Scholar]
- Lansford JE, Dodge KA, Pettit GS, & Bates JE (2010). Does physical abuse in early childhood predict substance use in adolescence and early adulthood. Child Maltreatment, 15, 190–194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lansford JE, Miller-Johnson S, Berlin LJ, Dodge KA, Bates JE, & Pettit GS (2007). Early physical abuse and later violent delinquency: A prospective longitudinal study. Child Maltreatment, 12, 233–245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lynch M, & Cicchetti D (1998). An ecological-transactional analysis of children and contexts: The longitudinal interplay among child maltreatment, community violence, and children’s symptomatology. Development and Psychopathology, 10, 235–257. [DOI] [PubMed] [Google Scholar]
- MacMillan HL (2000). Child maltreatment: What we know in the year 2000. Canadian Journal of Psychiatry, 45, 702–709. [DOI] [PubMed] [Google Scholar]
- MacMillan HL, Jamieson E, & Walsh CA (2003). Reported contact with child protection services among those reporting child physical and sexual abuse: Results from a community survey. Child Abuse & Neglect, 27, 1397–1408. [DOI] [PubMed] [Google Scholar]
- Mercy JA, & Saul J (2009). Creating a healthier future through early interventions for children. Journal of the American Medical Association, 301, 2262–2264. [DOI] [PubMed] [Google Scholar]
- Mersky JP, Topitzes J, & Reynolds AJ (2012). Unsafe at any age: Linking childhood and adolescent maltreatment to delinquency and crime. Journal of Research in Crime and Delinquency, 49, 295–318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moffitt TE, Caspi A, Harrington H, & Milne BJ (2002). Males on the life-course-persistent and adolescence-limited antisocial pathways: Follow-up at age 26 years. Development and Psychopathology, 14, 179–207. [DOI] [PubMed] [Google Scholar]
- Odgers CL, Caspi A, Nagin DS, Piquero AR, Slutske WS, Milne BJ, & Moffitt TE (2008). Is it important to prevent early exposure to drugs and alcohol among adolescents? Psychological Science, 19, 1037–1044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ohannessian CM, Finan LJ, Schulz JS, & Hesselbrock V (2015). A long-term longitudinal examination of the effect of early onset of alcohol and drug use on later alcohol abuse. Substance Abuse, 36, 440–444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oshri A, Rogosch FA, Burnette ML, & Cicchetti D (2011). Developmental pathways to adolescent cannabis abuse and dependence: Child maltreatment, emerging personality, and internalizing versus externalizing psychopathology. Psychology of Addictive Behaviors, 25, 634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patterson GR, Reid JB, & Dishion TJ (1992). Antisocial Boys Eugene, OR: Castalia. [Google Scholar]
- Pearl J (2009). Causality: Models, reasoning and inference Cambridge: Cambridge University Press. [Google Scholar]
- Pears KC, & Capaldi DM (2001). Intergenerational transmission of abuse: A two generational prospective study of an at-risk sample. Child Abuse & Neglect, 25, 1439–1461. [DOI] [PubMed] [Google Scholar]
- Perez CM, & Widom CS (1994). Childhood victimization and long-term intellectual and academic outcomes. Child Abuse & Neglect, 18, 617–633. [DOI] [PubMed] [Google Scholar]
- Prinz RJ, Sanders MR, Shapiro CJ, Whitaker DJ, & Lutzker JR (2009). Population-based prevention of child maltreatment: The US Triple P System population trial. Prevention Science, 10, 1–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Putnam-Hornstein E, Cederbaum JA, King B, & Needell B (2013). California’s most vulnerable parents: When maltreated children have children: A data linkage and analysis project Conrad N. Hilton Foundation; Retrieved from http://www.cssp.org/reform/child-welfare/pregnant-and-parentingyouth/Vulnerable_Parents_Full_Report_11-11-13.pdf [Google Scholar]
- Ryan RM, Mendle J, & Markowitz AJ (2015). Early childhood maltreatment and girls’ sexual behavior: The mediating role of pubertal timing. Journal of Adolescent Health, 57, 342–347. [DOI] [PubMed] [Google Scholar]
- Ryan JP, Williams AB, & Courtney ME (2013). Adolescent neglect, juvenile delinquency and the risk of recidivism. Journal of Youth and Adolescence, 42, 454–465. [DOI] [PubMed] [Google Scholar]
- Schofield TJ, Lee RD, & Merrick MT (2013). Safe, stable, nurturing relationships as a moderator of intergenerational continuity of child maltreatment: A meta-analysis. Journal of Adolescent Health, 53, S32–S38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shackman JE, & Pollak SD (2014). Impact of physical maltreatment on the regulation of negative affect and aggression. Development and Psychopathology, 26(4, Pt. 1), 1021–1033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shields A, & Cicchetti D (1998). Reactive aggression among maltreated children: The contributions of attention and emotion dysregulation. Journal of Clinical Child Psychology, 27, 381–395. [DOI] [PubMed] [Google Scholar]
- Shonkoff JP, Boyce WT, & McEwen BS (2009). Neuroscience, molecular biology, and the childhood roots of health disparities: Building a new framework for health promotion and disease prevention. Journal of the American Medical Association, 301, 2252–2259. [DOI] [PubMed] [Google Scholar]
- Simons RL, Whitbeck LB, Conger RD, & Wu CI (1991). Intergenerational transmission of harsh parenting. Developmental Psychology, 27, 159–171. [Google Scholar]
- Stallings MC, Cherny SS, Young SE, Miles DR, Hewitt JK, & Fulker DW (1997). The familial aggregation of depressive symptoms, antisocial behavior, and alcohol abuse. American Journal of Medical Genetics, 74, 183–191. [DOI] [PubMed] [Google Scholar]
- Stewart A, Livingston M, & Dennison S (2008). Transitions and turning points: Examining the links between child maltreatment and juvenile offending. Child Abuse & Neglect, 32, 51–66. [DOI] [PubMed] [Google Scholar]
- Stith SM, Liu T, Davies LC, Boykin EL, Alder MC, Harris JM, … Dees JEMEG (2009). Risk factors in child maltreatment: A meta-analytic review of the literature. Aggression and Violent Behavior, 14, 13–29. [Google Scholar]
- Straus MA, Gelles RJ, & Smith C (1995). Physical violence in American families: Risk factors and adaptations to violence in 8,145 families New Brunswick, NJ: Transaction. [Google Scholar]
- Teicher MH, Andersen SL, Polcari A, Anderson CM, Navalta CP, & Kim DM (2003). The neurobiological consequences of early stress and childhood maltreatment. Neuroscience and Biobehavioral Reviews, 27, 33–44. [DOI] [PubMed] [Google Scholar]
- Teicher MH, Samson JA, Anderson CM, & Ohashi K (2016). The effects of childhood maltreatment on brain structure, function and connectivity. Nature Reviews Neuroscience, 17, 652–666. [DOI] [PubMed] [Google Scholar]
- Teicher MH, Samson JA, Polcari A, & McGreenery CE (2006). Sticks, stones, and hurtful words: Relative effects of various forms of childhood maltreatment. American Journal of Psychiatry, 163, 993–1000. [DOI] [PubMed] [Google Scholar]
- Thornberry TP (2005). Explaining multiple patterns of offending across the life course and across generations. Annals of the American Academy of Political and Social Science, 602, 156–195. [Google Scholar]
- Thornberry TP (2016). Three generation studies: Methodological challenges and promise. In Shanahan MJ, Mortimer JT, & Kirkpatrick Johnson M (Eds.), Handbook of the life course (pp. 571–596). New York: Springer International. [Google Scholar]
- Thornberry TP, & Henry KL (2013). Intergenerational continuity in maltreatment. Journal of Abnormal Child Psychology, 41, 555–569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thornberry TP, Henry KL, Krohn MD, Lizotte AJ, & Nadel EL (2018). Key findings from the Rochester intergenerational study. In Intergenerational Continuity of Criminal and Antisocial Behavior: An International Overview of Current Studies London: Routledge. [Google Scholar]
- Thornberry TP, Henry KL, Smith CA, Ireland TO, Greenman SJ, & Lee RD (2013). Breaking the cycle of maltreatment: The role of safe, stable, and nurturing relationships. Journal of Adolescent Health, 53, S25–S31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thornberry TP, Ireland TO, & Smith CA (2001). The importance of timing: The varying impact of childhood and adolescent maltreatment on multiple problem outcomes. Development and Psychopathology, 13, 957–979. [PubMed] [Google Scholar]
- Thornberry TP, Matsuda M, Greenman SJ, Augustyn MB, Henry KL, Smith CA, & Ireland TO (2014). Adolescent risk factors for child maltreatment. Child Abuse & Neglect, 38, 706–722. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thrane LE, Hoyt DR, Whitbeck LB, & Yoder KA (2006). Impact of family abuse on running away, deviance, and street victimization among homeless rural and urban youth. Child Abuse & Neglect, 30, 1117–1128. [DOI] [PubMed] [Google Scholar]
- Tyler KA, & Bersani BE (2008). A longitudinal study of early adolescent precursors to running away. Journal of Early Adolescence, 28, 230–251. [Google Scholar]
- US Department of Health and Human Services. (2012). Child Maltreatment 2011 Washington, DC: Author. [Google Scholar]
- Valeri L, & VanderWeele TJ (2013). Mediation analysis allowing for exposure–mediator interactions and causal interpretation: Theoretical assumptions and implementation with SAS and SPSS macros. Psychological Methods, 18, 137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Valeri L, & VanderWeele TJ (2015). SAS macro for causal mediation analysis with survival data. Epidemiology, 26, e23–e24. [DOI] [PubMed] [Google Scholar]
- VanderWeele TJ (2011). Causal mediation analysis with survival data. Epidemiology, 22, 582–585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- VanderWeele TJ, & Vansteelandt S (2009). Conceptual issues concerning mediation, interventions and composition. Statistics and Its Interface, 2, 457–468. [Google Scholar]
- VanderWeele TJ, & Vansteelandt S (2010). Odds ratios for mediation analysis for a dichotomous outcome. American Journal of Epidemiology, 172, 1339–1348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Verlaan P, & Schwartzman AE (2002). Mother’s and father’s parental adjustment: Links to externalising behaviour problems in sons and daughters. International Journal of Behavioral Development, 26, 214–224. [Google Scholar]
- Westat. (1997). National evaluation of runaway and homeless youth Washington, DC: US Department of Health and Human Services, Administration on Children, Youth and Families. [Google Scholar]
- Wickrama KAS, Conger RD, Lorenz FO, & Jung T (2008). Family antecedents and consequences of trajectories of depressive symptoms from adolescence to young adulthood: A life course investigation. Journal of Health and Social Behavior, 49, 468–483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wickrama KAS, Conger RD, Wallace LE, & Elder GH Jr. (2003). Linking early social risks to impaired physical health during the transition to adulthood. Journal of Health and Social Behavior, 44, 61–74. [PubMed] [Google Scholar]
- Wickrama KK, O’Neal CW, & Oshri A (2014). Are stressful developmental processes of youths leading to health problems amplified by genetic polymorphisms? The case of body mass index. Journal of Youth and Adolescence, 43, 1096–1109. [DOI] [PubMed] [Google Scholar]
- Widom CS (1988). Sampling biases and implications for child abuse research. American Journal of Orthopsychiatry, 58, 260–270. [DOI] [PubMed] [Google Scholar]
- Widom CS (1989). The cycle of violence. Science, 244, 160–166. [DOI] [PubMed] [Google Scholar]
- Widom CS, Czaja SJ, & DuMont KA (2015). Intergenerational transmission of child abuse and neglect: Real or detection bias? Science, 347, 1480–1485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Widom CS, & Hiller-Sturmhofel S (2001). Alcohol abuse as a risk factor for and consequence of child abuse. Alcohol Research & Health, 25, 52. [PMC free article] [PubMed] [Google Scholar]
- Widom CS, Ireland T, & Glynn PJ (1995). Alcohol abuse in abused and neglected children followed-up: Are they at increased risk? Journal of Studies on Alcohol, 56, 207–217. [DOI] [PubMed] [Google Scholar]
- Widom CS, Raphael KG, & DuMont KA (2004). The case for prospective longitudinal studies in child maltreatment research: Commentary on Dube, Williamson, Thompson, Felitti, and Anda (2004). Child Abuse & Neglect, 28, 715–722. [DOI] [PubMed] [Google Scholar]