

Supplemental Digital Content is available in the text.
Abstract
Background:
Nerve injuries in the hand are common and often pose a challenge for the upper extremity surgeon. A range of reconstructive options exist for nerve repair, but proper matching of nerve diameter is important for many of these techniques. The purposes of this study were to (1) describe the nerve diameters of the hand and their relative differences and (2) investigate whether there is a relationship between nerve diameter and external hand dimensions or body mass index.
Methods:
We utilized 18 freshly frozen cadaveric hands from adult donors aged 20–86 of both sexes for this study. Two independent observers measured each nerve diameter to the nearest 0.1 mm using a digital caliper.
Results:
Using the flexor zones as boundaries, a total of 33 nerve measurements were performed for each cadaveric hand. Nerve diameter increased from the distal to the proximal flexor zones. The internal common digital nerves in flexor zone 3 were larger than the external digital nerves. The median nerve was found to be nearly 2 times larger than the ulnar nerve at 2 locations within the wrist. There was a positive correlation between body mass index, hand span, hand width, and nerve diameter at several measured locations.
Conclusions:
This study provides reference values for nerve diameters of the hand and wrist and describes their relative differences. It is important for surgeons to be aware of these differences and to consider this information as we advance our efforts to reconstruct the hand and develop technologies for nerve repair.
INTRODUCTION
Nerve injuries in the hand are common and continue to pose a challenge to the upper extremity surgeon.1,2 Depending on the mechanism of injury, elapsed time since nerve transection, and degree of soft-tissue edema, techniques of nerve coaptation include direct repair, hollow tube (conduit/connector) repair, and repair with autograft or allograft.3 Despite a progressively greater understanding of neural physiology and technical advances during nerve repair, not all outcomes are satisfactory.4
Although previous anatomic studies have investigated nerve branching patterns within the hand and the axonal count related to autograft harvest,5–9 to our knowledge, there have been no studies investigating nerve diameter throughout the hand and digits. Knowledge of nerve diameter could prove useful for future clinical and research efforts into treating nerve injuries of the hand.
This cadaveric study was conducted to investigate nerve diameter within the wrist and hand, compare the nerve diameter between flexor zones and between digits, and determine whether nerve diameter is related to other factors such as external hand dimension and body mass index (BMI).
MATERIALS AND METHODS
We utilized 18 freshly frozen cadaveric hands from adult donors of both sexes for this study. The median age of the cadavers was 72 years (range: 20–86), 8 (44%) were male, and the mean ± SD BMI was 22.5 ± 4.6 kg/m2 (Table 1). We measured the external hand dimensions across three axes: (1) span: tip of thumb to tip of small finger with digits passively abducted as widely as possible, (2) length: distance between distal wrist flexion crease and distal tip of the middle finger, and (3) width: distance from most radial aspect of the hand at the level of the second metacarpal to the most ulnar aspect of the hand near the fifth metacarpal (Fig. 1).
Table 1.
Demographics
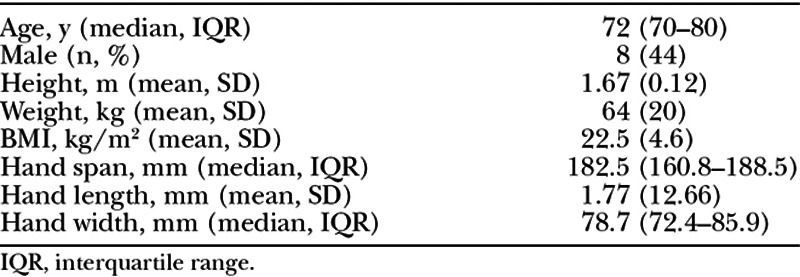
Fig. 1.
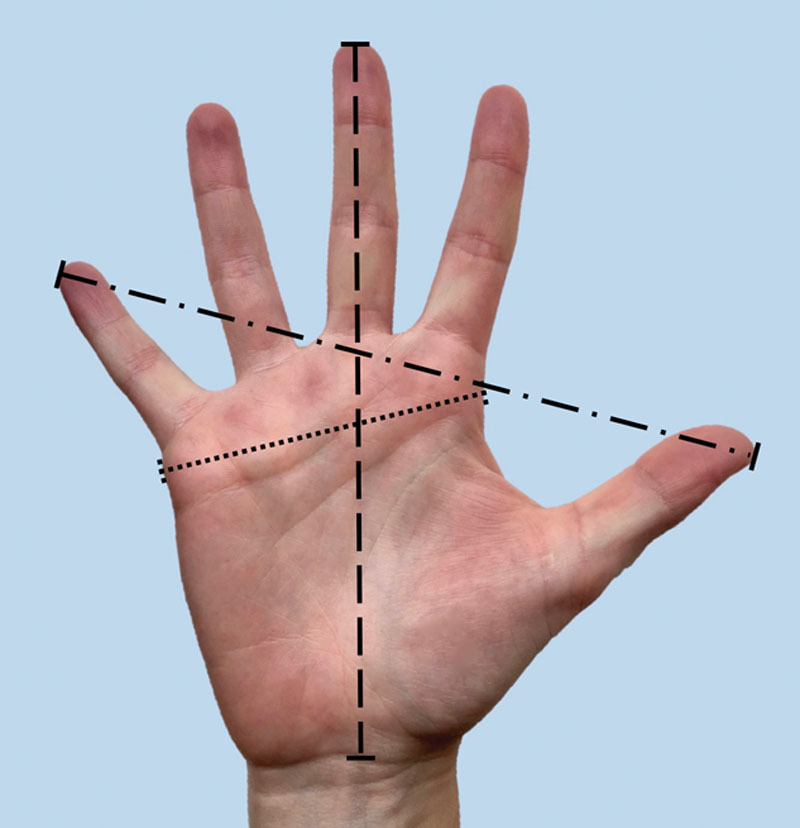
The dimensions of the hand. Description: The 3 axes we used as external dimensions of the hand.
The same two independent observers measured the nerves of each cadaver. We used the mean measurement of both observers as the measurement for the nerve. The nerve diameter was measured using a digital caliper, and measurements were taken to the nearest 0.1 mm. Before data collection, both observers practiced measuring on the same cadaver to establish a standardized measuring technique, which focused on measuring nerve diameter without compressing the nerve.
Using the flexor zones as boundaries, we measured nerves at a total of 33 locations for each cadaveric hand (Fig. 2). These included the ulnar and radial branch of the digital nerves at the middle of the middle phalanx in flexor zone 1 and at the neck of the proximal phalanges in flexor zone 2, the common digital nerves 1 cm from their origin in flexor zone 3, the median nerve proximal and distal to the transverse carpal ligament (TCL) in flexor zone 4, the ulnar nerve proximal to Guyon’s canal in flexor zone 4, the median and ulnar nerves at the wrist crease in flexor zone 5, and the recurrent motor branch of the median nerve in flexor zone 4. We marked the precise location of each measurement for each specimen using a purple skin marker so that both observers measured the same location along the nerve. Two data points were not possible to measure because of poor preservation and thus poor visualization of the nerves (the small finger of hand 7 and the ulnar nerve of hand 15), and we excluded these from statistical analyses.
Fig. 2.
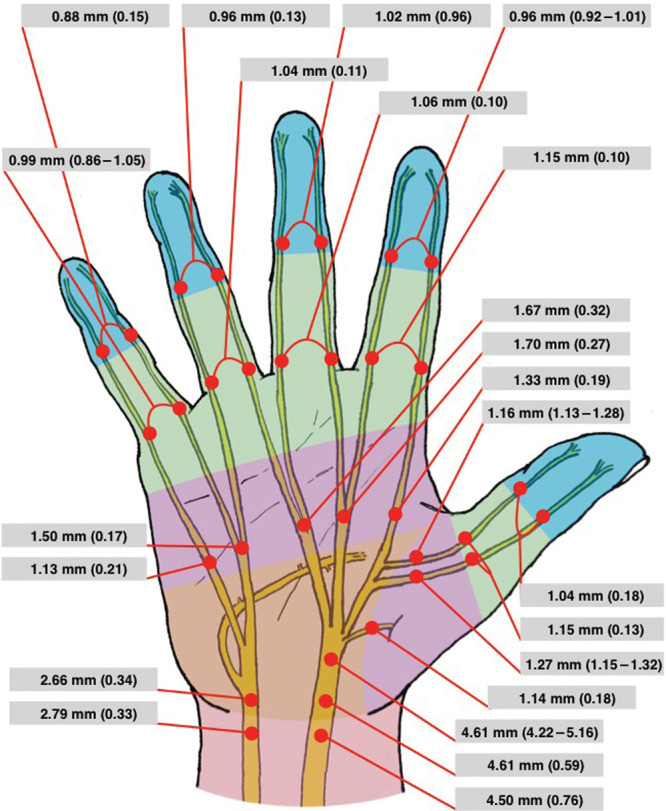
The measurement locations and their nerve diameters. Description: The 33 locations within the hand and wrist where we measured the diameter of each nerve.
We described continuous variables with normal distribution with means and SDs and analyzed them using paired t tests, whereas we described continuous variables with a nonnormal distribution with medians and interquartile ranges and analyzed them using signed rank tests. We analyzed the correlation between normally distributed continuous data with Pearson’s correlation coefficient and nonnormally distributed continuous data with Spearman’s rank correlation. We calculated interobserver agreement using intraclass correlation coefficients with an absolute agreement, 2-way mixed effect model. We interpreted intraclass correlation coefficient values 0.5 or less as indicating “poor agreement”; 0.5 to 0.75, “moderate agreement”; 0.75 to 0.9, “good agreement”; and 0.9 and greater, “excellent agreement.10
Our institution does not require review of cadaveric studies.
RESULTS
There was an increase in diameter from flexor zone 1 (0.97 mm) to flexor zone 2 (1.07 mm) and from flexor zone 2 to flexor zone 3 (1.46 mm) (Fig. 3). When separating these measurements by digit, there were statistically significant differences between flexor zone 1 and flexor zone 2 of the thumb, index, and ring finger. When comparing flexor zone 2 with flexor zone 3 (common digital nerves), there were differences across all nonthumb digits (see appendix, Supplemental Digital Content 1, which displays the mean nerve diameter of each measurement location, http://links.lww.com/PRSGO/B6).
Fig. 3.
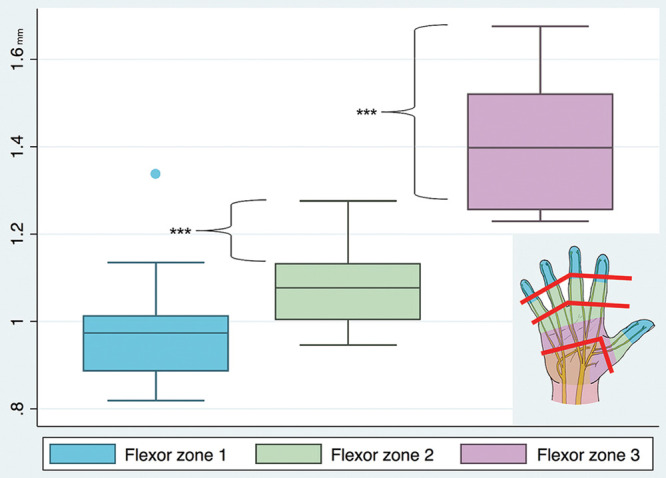
The mean nerve diameter for flexor zones 1–3. Description: A boxplot presenting the average nerve diameter in each flexor zone. ***P < 0.001. Excluding the measurements of case 18 in flexor zone 1. Excluding the measurements of the thumb from cases 2, 17, and 18 in flexor zone 3. Excluding the measurements of the common digital nerve from case 7 in flexor zone 3.
In comparing the nerve diameters between digits within the same flexor zones, there was a difference within flexor zone 1 between the small finger (0.88 mm) and all other digits. In addition, there was a difference between the diameter of the middle finger digital nerves and the ring finger digital nerves within flexor zone 1. Within flexor zone 2, the nerve diameters of each digit were all different from each other, except the index finger versus thumb and middle versus ring finger. Within flexor zone 3, the external common digital nerves innervating one digit (external digital nerves) were each smaller than each of the internal common digital nerves innervating two digits (internal digital nerves) (Fig. 4).
Fig. 4.

The mean nerve diameter for each finger in flexor zones 1–3. Description: A boxplot presenting the average nerve diameter for each finger in flexor zones 1–3. *P < 0.05, ***P < 0.001. Excluding the measurements of case 18 in flexor zone 1. Excluding the measurements of the thumb from cases 2, 17, and 18 in flexor zone 3. Excluding the measurements of the common digital nerve from case 7 in flexor zone 3.
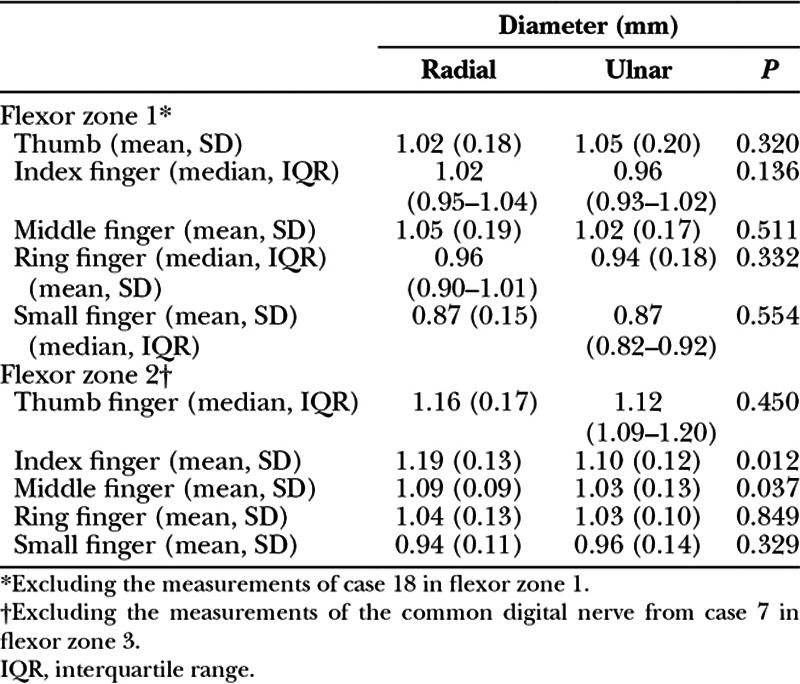
In evaluating diameter of the radial digital versus ulnar digital nerves, the radial digital nerves were larger in diameter than the ulnar digital nerves in zone 2 of the index and middle fingers and in the common digital nerves (zone 3) of the thumb (Table 2).
Table 2.
Ulnar Branch Versus the Radial Branch of the Digital Nerve
There were variations in the branching of the digital nerves of the thumb, such that 15/18 hands (83.3%) of cadavers did not have a common digital nerve and instead had separate radial and ulnar digital nerves branching directly from the median nerve. The other 3/18 (16.7%) of cadavers had a common digital nerve of the thumb, which distally splits into a radial and ulnar branch.
The median nerve was found to be about 1.6 times larger than the ulnar nerve at two different locations. These were at a location proximal to the TCL (4.61 versus 2.66 mm) and at the distal wrist crease (4.50 versus 2.79 mm) (Fig. 5). The mean ± SD size of the recurrent motor nerve was 1.14 ± 0.18 mm.
Fig. 5.
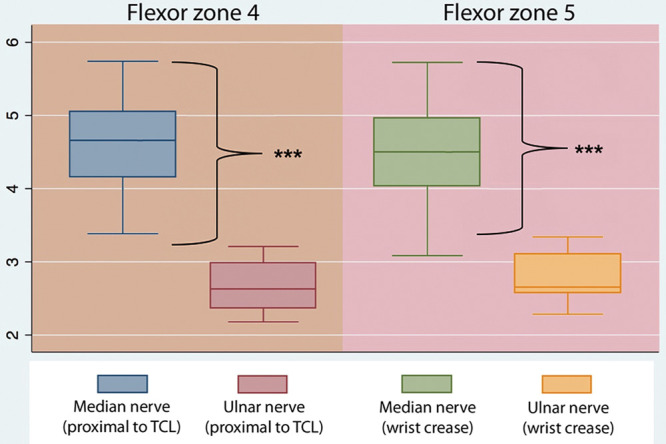
The mean nerve diameter of the median and ulnar nerves at flexor zones 4 and 5. Description: A boxplot presenting the average nerve diameter of the median and ulnar nerve in flexor zones 4 and 5. ***P < 0.001. Excluding the measurement of the ulnar nerve at the wrist crease of case 15.
The mean length of each hand was 177 mm; median width, 78.7 mm; and median span, 182.5 mm (Table 1: demographics). In assessing for a correlation between hand dimensions and nerve diameter, we generally found a positive correlation between BMI, hand span, hand width, and the diameter of the nerve. Seven measurements had a statistically significant positive correlation. For BMI, these were the radial branch of the digital nerve of the thumb in flexor zone 2 (r = 0.49, P = 0.0382), the common digital nerve of the index finger (r = 0.49, P = 0.0369), and the common digital nerve of the ring and small finger (r = 0.62, P = 0.0066). For hand width, these were the radial branch of the digital nerve of the thumb in flexor zone 3 (rs = 0.62, P = 0.0123), the ulnar branch of the digital nerve of the thumb in flexor zone 3 (rs = 0.60, P =0.0176), and the common digital nerve of the ring and small finger (rs = 0.61, P =0.0074). For hand span, only the ulnar nerve distal to the TCL was statistically significant (rs = 0.53, P = 0.0222). One measurement was negatively correlated with length of the hand and the diameter of the ulnar branch of the index finger in flexor zone 1 (rs = −0.49, P = 0.0467) (see appendix, Supplemental Digital Content 2, which displays correlation between hand width, hand span, hand length and BMI with the nerve diameter, http://links.lww.com/PRSGO/B7). Spearman’s rank correlation coefficient showed that BMI and hand width (rs = 0.77, P < 0.001), BMI and hand span (rs = 0.72, P < 0.001), and hand span and hand width (rs = 0.73, P < 0.001) positively correlate with each other.
Intraclass correlation showed interobserver agreement ranging from poor to excellent agreement. The measurements of the common digital nerve at the index finger and the common digital nerves at the thumb had a mean coefficient that was negative (−0.10, CI: −2.03 to 0.59; −0.47, CI: −1.95 to 0.42; −0.055, CI: −2.8 to 0.44, respectively). The measurements of the median nerve proximal to the TCL and the radial branch of the digital nerve of the middle finger at flexor zone 2 had a good interobserver agreement: moderate to excellent agreement (0.81, CI: 0.50–0.93) and poor to excellent agreement (0.81, CI: 0.43–0.93), respectively. The measurements of 10 locations had a moderate interobserver agreement, ranging from poor to excellent agreement. The measurements of the 17 other locations had a poor interobserver agreement ranging from poor to good agreement (see appendix, Supplemental Digital Content 3, which displays interobserver reliability, http://links.lww.com/PRSGO/B8).
DISCUSSION
This study reports the diameter of nerves in the distal upper extremity, which can help inform surgeons caring for patients with these injuries. This study provides reference values for diameter of the nerves in the hand and demonstrates that (1) nerve diameter decreases from proximal to distal flexor zones, (2) nerve diameter differs between digits within flexor zone 2 and between the common digital nerves of flexor zone 3, (3) the median nerve is 1.6 times larger than the ulnar nerve at the wrist, and (4) there is a correlation between nerve size and baseline patient factors such as hand dimensions and BMI.
This study must be interpreted in light of its limitations. Nerve diameter, in general, is difficult to precisely measure because nerves are pliable and easily compressed during measurement. Variability in technique can consequently lead to inaccurate measurement. Therefore, we utilized a standardized method and used the mean outcome of two observers for each nerve diameter to mitigate this problem. Because this was a cadaveric study, the mean age of these cadavers was not representative of the mean age of patients with acute nerve injuries in the hand.11 Previous studies have suggested that nerve cross-sectional area may increase with age and that it is important to take this into account when evaluating nerve size.12,13 However, these studies did not include digital nerves or those distal to the wrist. Our samples did not allow for a proper analysis of the effect of age on nerve diameter, and further studies are needed to elucidate this. Lastly, our sample size consisted of 18 cadaveric hands and two observers, which was limited by the number of cadavers, the availability of surgeons to dissect the specimens, and the need to complete the study expeditiously to prevent desiccation from affecting the measurements.
We chose to use the different flexor tendon zones as locations for measurement. These territories of the hand are well established and were originally classified by Verdan and Kleinert for the discussion and treatment of tendon injuries.14,15 For the purposes of this study, we used flexor zones as measurement locations for practical utility: so that surgeons would have a common frame of reference for these measurements. This nomenclature is familiar to hand surgeons, and we thought it superior to other, purely “anatomic” location for measurements as these would have less applicability to the operating surgeon.
Proper matching of nerve length and diameter is important for many techniques used in nerve repair. When using conduits, undersizing the device can constrict the regenerating nerve, whereas oversizing can lead to tube collapse or mobility that fails to support axons and poorer functional recovery.16,17 For nerve autografts, a mismatch in nerve diameter can lead to either inadequate axonal counts or fascicular redundancy, which may lead to axonal escape.18 Knowledge of nerve diameter may help the surgeon considering the use of nerve allograft, to accurately size match the graft to the proximal and distal nerve stumps. Furthermore, increasing the accuracy with which we can estimate nerve diameter may minimize the risk of obtaining an unsuitable conduit or allograft for use in the operating room. Lastly, knowledge about nerve diameter may also prove helpful in other clinical situations, such as in the use of perineural injections and the development of nerve repair technologies.
This study found that the median nerve diameter (4.50 mm) at the wrist was significantly and nearly two times larger than the ulnar nerve diameter (2.79 mm). This finding supports previous reports using ultrasound to measure nerves of the forearm13,19 but is not necessarily intuitively understood by all hand surgeons. The difference in size likely stems from the fact that the median nerve is responsible for the motor and sensory innervation of a larger area of the hand as compared to the ulnar nerve and may be flatter and more elliptical, leading to a wider nerve when measured.
Anecdotal evidence in the operating room led us to hypothesize that the radial digital nerves are larger than the ulnar digital nerves, particularly in the radial digits. Although we found statistical significance supporting this theory within flexor zone 2 of the index and middle fingers, we did not find this to be true in other digits. A larger sample size might reveal additional differences between the radial and ulnar digital nerves in other digits.
Previous studies showed a positive correlation between nerve size and age, weight, and BMI.12,13,20 Our study supports these findings with a positive correlation between nerve size and BMI, hand span, and hand width at seven measurement locations. Further analysis showed that hand width, hand span, and BMI positively correlate with each other. It is therefore likely that these variables are not independently associated with nerve diameter. A larger sample size is required to see whether these variables significantly correlate with nerve diameter at other measurement locations.
We identified three variations of median nerve branching to the thumb and index finger, similar to previous studies and originally illustrated by Jolley et al. in 1997.6,7,21 Our data support their findings that the most common branching pattern is a common digital nerve from the median nerve that supplies the index finger and the ulnar side of the thumb and a separate branch from the median nerve that supplies the radial thumb. This is in contrast to many anatomic illustrations, which show the least common branching pattern, a common digital nerve to the thumb that subsequently branches into radial and ulnar digital nerves.
This study provides reference values for nerve diameters of the hand and wrist and describes their relative differences. It is important for surgeons to be aware of these differences and to consider this information as we advance our efforts for nerve repair in the hand and develop technologies for nerve repair.
ACKNOWLEDGMENTS
We would like to acknowledge Mr. Orlando Merced-O'Neil and Dr. Anne Engemann for their contributions toward this study.
Supplementary Material
Footnotes
Published online 13 March 2019.
Mr. Amador and Dr. Westenberg should be considered co–first authors; they have contributed equally to this manuscript.
Disclosure: Materials for this study, including cadavers, were provided by the AxoGen Corporation. Dr. Eberlin is a consultant for AxoGen and Integra. Dr. Chen is a consultant for Miami Device Solutions. None of the other authors has any financial disclosures.
Supplemental digital content is available for this article. Clickable URL citations appear in the text.
This article was originally published with Ricardo O. Amador as Ricardo Ortiz.
REFERENCES
- 1.Noble J, Munro CA, Prasad VS, et al. Analysis of upper and lower extremity peripheral nerve injuries in a population of patients with multiple injuries. J Trauma. 1998;45:116–122. [DOI] [PubMed] [Google Scholar]
- 2.Dahlin LB. Nerve injuries. Curr Orthop. 2008;22:9–16. [Google Scholar]
- 3.Isaacs J, Safa B, Evans PJ, et al. Technical assessment of connector-assisted nerve repair. J Hand Surg Am. 2016;41:760–766. [DOI] [PubMed] [Google Scholar]
- 4.Rbia N, Shin AY. The role of nerve graft substitutes in motor and mixed motor/sensory peripheral nerve injuries. J Hand Surg Am. 2017;42:367–377. [DOI] [PubMed] [Google Scholar]
- 5.Bas H, Kleinert JM. Anatomic variations in sensory innervation of the hand and digits. J Hand Surg Am. 1999;24:1171–1184. [DOI] [PubMed] [Google Scholar]
- 6.Loukas M, Louis RG, Jr, Stewart L, et al. The surgical anatomy of ulnar and median nerve communications in the palmar surface of the hand. J Neurosurg. 2007;106:887–893. [DOI] [PubMed] [Google Scholar]
- 7.Filfilan R, Kinsella A, Yong L, et al. A cadaveric study of the distribution pattern of the cutaneous sensory fibres of the distal palm of the hand. J Hand Surg Eur Vol. 2016;41:848–851. [DOI] [PubMed] [Google Scholar]
- 8.Higgins JP, Fisher S, Serletti JM, et al. Assessment of nerve graft donor sites used for reconstruction of traumatic digital nerve defects. J Hand Surg Am. 2002;27:286–292. [DOI] [PubMed] [Google Scholar]
- 9.Kim J, Lee YH, Kim MB, et al. Anatomy of the direct small branches of the proper digital nerve of the fingers: a cadaveric study. J Plast Reconstr Aesthet Surg. 2014;67:1129–1135. [DOI] [PubMed] [Google Scholar]
- 10.Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15:155–163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Thorsén F, Rosberg HE, Steen Carlsson K, et al. Digital nerve injuries: epidemiology, results, costs, and impact on daily life. J Plast Surg Hand Surg. 2012;46:184–190. [DOI] [PubMed] [Google Scholar]
- 12.Cartwright MS, Mayans DR, Gillson NA, et al. Nerve cross-sectional area in extremes of age. Muscle Nerve. 2013;47:890–893. [DOI] [PubMed] [Google Scholar]
- 13.Bedewi MA, Abodonya A, Kotb M, et al. Estimation of ultrasound reference values for the upper limb peripheral nerves in adults: a cross-sectional study. Medicine (Baltimore). 2017;96:e9306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kleinert HE, Kutz JE, Ashbell TS, Martinez E. Primary repair of lacerated flexor tendons in “No Man’s Land” (abstr). J Bone Joint Surg 1967;49A:577. [Google Scholar]
- 15.Verdan CE. Half a century of flexor-tendon surgery. Current status and changing philosophies. J Bone Joint Surg Am. 1972;54:472–491. [PubMed] [Google Scholar]
- 16.Isaacs J, Mallu S, Yan W, et al. Consequences of oversizing: nerve-to-nerve tube diameter mismatch. J Bone Joint Surg Am. 2014;96:1461–1467. [DOI] [PubMed] [Google Scholar]
- 17.Giusti G, Shin RH, Lee JY, et al. The influence of nerve conduits diameter in motor nerve recovery after segmental nerve repair. Microsurgery. 2014;34:646–652. [DOI] [PubMed] [Google Scholar]
- 18.Tang P, Kilic A, Konopka G, et al. Histologic and functional outcomes of nerve defects treated with acellular allograft versus cabled autograft in a rat model. Microsurgery. 2013;33:460–467. [DOI] [PubMed] [Google Scholar]
- 19.Brill NA, Tyler DJ. Quantification of human upper extremity nerves and fascicular anatomy. Muscle Nerve. 2017;56:463–471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Werner RA, Jacobson JA, Jamadar DA. Influence of body mass index on median nerve function, carpal canal pressure, and cross-sectional area of the median nerve. Muscle Nerve. 2004;30:481–485. [DOI] [PubMed] [Google Scholar]
- 21.Jolley BJ, Stern PJ, Starling T. Patterns of median nerve sensory innervation to the thumb and index finger: an anatomic study. J Hand Surg Am. 1997;22:228–231. [DOI] [PubMed] [Google Scholar]