

Abstract
Introduction
This study aimed to compare the results from three Australian scuba diver surveys. As the surveys differed in recruitment methods, the expectation was that respondents would differ in some important characteristics.
Methodology
Anonymous, online, cross-sectional surveys of the demographics, health, diving practices and outcomes were distributed to: (1) Divers Alert Network Asia-Pacific (DAN AP) members; (2) Professional Association of Diving Instructors (PADI) Asia-Pacific members; and (3) divers who had received any PADI non-leadership certification within the previous four years. Only data from divers resident in Australia were analysed.
Results
A total of 2,275 responses were received from current Australian residents, comprising 1,119 of 4,235 (26.4%) DAN members; 350 of 2,600 (13.5%) PADI members; and 806 of 37,000 (2.2%) PADI divers. DAN and PADI members had similar diving careers (medians 14 and 15 years, respectively). PADI members had undertaken more dives (median 800) than DAN members (330) and PADI divers (28). A total of 692 respondents reported suffering from diabetes or a cardiovascular, respiratory, neurological or psychological condition and included 34% of the DAN members and 28% of each of the PADI cohorts. Eighty-four divers had been treated for decompression illness (approximately 5% of DAN and PADI member groups and 1% of the PADI divers). Eighty-seven of 1,156 (7.5%) PADI respondents reported a perceived life-threatening incident while diving.
Conclusions
Despite low response rates, this study indicates clear differences in the characteristics of the divers in the three cohorts. Therefore, a survey of a single cohort may represent that diving population alone and the findings may be misleading. This bias needs to be clearly understood and any survey findings interpreted accordingly.
Keywords: Survey, Fitness to dive, Health surveillance, Cardiovascular, Scuba divers, Recreational divers
Introduction
Historically, participants in recreational scuba diving in Australia were mainly young, fit males who were experienced breath-hold divers.[ 1] More recently, broader subsets of the population (age, gender and aquatic skills) have been attracted to the sport. In addition, some of the earlier divers who have remained active have aged with an associated risk of co-existing disease and subsequent morbidity and mortality during diving.[ 2 - 7] It is important to have an understanding of the demographics, activities and health of current divers to better cater for their needs. For example, if a substantial older diver demographic is identified, targeted diving health campaigns could be offered, better pre-dive screening tools created and implemented and potential justification provided for the increased availability of defibrillators on dive boats. In general, the availability of such data enables the appropriate planning for incident mitigation and management strategies as well as safety initiatives. It also can serve to inform parts of the diving community about the level and type of activity of certain diving cohorts. However, there are few useful and publicly available data on Australian scuba divers since most relevant data are captured and held internally by the diver certification agencies for commercial purposes.
The aim of this study was to compare demographic, health and diving activity data of respondents to three Australian scuba diver surveys. As the survey samples were recruited from different cohorts of divers (i.e., insured divers, certified dive professionals and other, generally more-recently certified divers) the expectation was that respondents would differ in important characteristics. Confirmation of such differences would highlight that a survey of a single diver group may not be representative of the general diving population. Therefore, diver surveys must ensure that respondents are drawn from divers from a variety of different affiliations covering a spectrum of age, experience and diving activity.
Methodology
Two similar anonymous, online, cross-sectional surveys for distribution to scuba divers were created using an online survey development system (Survey Monkey). Ethics approval was received from the Human Research Ethics Committee of Deakin University, Victoria, Australia (HEAG-H 100_2015). As there were no pre-existing questions on which validity and reliability had been tested, we developed our own questionnaire. The questionnaire was trialled for face validity on a small group of potential respondents and revised prior to its use.
DAN MEMBERS SURVEY
The Divers Alert Network Asia-Pacific (DAN AP) is a non-profit, membership-based association with a mission to improve recreational diving safety. Among other benefits, it provides its members with access to diving injury insurance. In December 2014, an invitation to participate in a DAN AP survey (DAN-S)[ 8] was emailed to all current DAN AP members over 18-years-old (9,927) with a recorded email address at that time (99% of members). A reminder was sent in March 2015 and the survey was closed in April 2015. No a priori sample size calculation was undertaken as all DAN AP members were invited to participate. The survey sought details about the respondents’ age, gender, height and weight (from which body mass index (BMI) was calculated), perceived fitness, any significant medical conditions and diving history and activity. Diving data included the years of diving, number of dives, dives per year, frequency of diving and the types of dives undertaken (deeper, technical, decompression and repetitive). Data were also collected on personal experiences with decompression illness (DCI).
PADI SURVEY
The Professional Association of Diving Instructors (PADI) is the world’s largest diver certification agency and PADI Asia-Pacific is responsible for the vast majority of diver certifications in Australia. A survey was distributed by PADI Asia-Pacific in September 2015 and a reminder sent in December 2015 to two cohorts of its certified divers: (1) current PADI members (i.e., divers with a PADI divemaster or instructor qualification, or higher, PADI-M; 2,600 divers) recorded as living in Australia; and (2) divers with an Australian address who had received any non-leadership certification from PADI within the previous four years (PADI-D; 37,000 divers).
The survey distributed to the PADI cohorts included almost identical questions to the DAN-S. However, it also contained a screening question to identify those who had already responded to the DAN survey, as well as some questions about life-threatening diving incidents that had been experienced. The questions about life-threatening incidents were added in order to gather information for additional research, subsequent to the DAN-S. The authors were not provided with data on the proportion of each of the PADI groups for which email addresses were known. The PADI surveys were closed in February 2016. For all three surveys, only respondents with an Australian residential address were included in the analysis of the surveys.
STATISTICAL ANALYSIS
Statistical analysis was conducted using SPSS Version 22 (IBM, Armonk, NY; 2013). Estimates were presented as means or proportions with 95% confidence intervals. Chi-square tests were used to compare categorical variables such as health conditions, diving certifications and demographic characteristics of the participants in the three surveys. ANOVA was used to compare age and BMI across the three surveys.
The level of significance used throughout was 0.05. A priori sample size calculations were performed using the National Statistical Service online calculator.[ 9] The calculated sample sizes required were 335 (CL = 95, proportion = 0.5, CI = 0.05) for PADI-M, and 381 for PADI-D (CL = 95, proportion = 0.5, CI = 0.05). Prevalence rates were calculated based on an exact binomial test in the R statistical package.[ 10]
Results
DEMOGRAPHICS
A total of 9,927 DAN AP members were emailed and details of the full cohort of respondents are reported elsewhere.[ 8] Of the 4,235 of these invitees recorded as Australian residents, there were 1,119 (26.4%) respondents. Information was available on the age and gender of all DAN AP members so it was possible to determine the age and gender of non-respondents. Three-hundred-and-seventy-five of 2,600 (14.5%) and 868 of 37,000 (2.3%) of the PADI-M and PADI-D invitees responded, respectively. Demographic data on invitees and respondents are shown in Table 1.
Table 1. Age and gender of invitees, respondents and non-respondents to surveys of DAN AP members (DAN-S) and PADI certified divers (PADI-S) and members (PADI-M); age and gender not known in PADI-S non-respondents; NA = not available; *Australian residents only .
| Age (y) | Gender | |
| mean (SD) | % (male) | |
| DAN AP Members | ||
| Invitees (n = 4,235) | 53 (13) | 73 |
| Respondents (n = 1,119)* | 50 (12) | 71 |
| PADI Divers | ||
| Invitees (n = 37,000) | 31 (10) | 62 |
| Respondents (n = 806)* | 38 (10) | 58 |
| PADI Members | ||
| Respondents (n = 2,600) | 35 (11) | 76 |
| Respondents (n = 350)* | 44 (12) | 70 |
| Non-Respondents (n = 2,250) | NA | NA |
Of the 37,000 invited divers who had received a (non-leadership) PADI certification in the previous four years, approximately 14,000 opened the invitation email and 868 responded (2.3%) to the survey. Of the 2,600 PADI members who were invited to participate, 1,458 (56%) opened the invitation and of these 375 (25.7%) responded. Overall, 329 DAN-S, 25 PADI-M and 62 PADI-D respondents were excluded as they no longer lived in Australia. Twenty-nine PADI divers (two PADI-M and 27 PADI-D divers) had previously completed the DAN-S so were excluded from the PADI data. Thus, the following results are based on 1,119 DAN members (DM), 350 PADI members (PM) and 806 PADI divers (PD), a total of 2,275 Australian-based divers. Respondents to the DAN-S were on average significantly younger than non-respondents (mean ages 50 and 54 years respectively; P < 0.001).
Table 2 describes the demographic characteristics of respondents from the three cohorts. These differed significantly in mean age and gender mix. There was a small, albeit statistically significant difference between the mean BMIs of the cohorts, although these differences were not clinically significant. There was also a significant difference in the proportions of obese respondents in the different gender subgroups with higher rates of obesity in male PM divers (P = 0.012). However, all comparisons need to be interpreted cautiously due to the low response rates to the surveys.
Table 2. Demographic information of 2,275 Australian-resident divers; BMI – body mass index; * 25 < BMI < 30 kg·m⁻²; ** BMI ≥ 30 kg·m⁻²; † comparison made of relative fitness levels reported between groups, n.s. – not significant .
| DAN Members | PADI Members | PADI Divers | P-value | |
| Age (y) mean (SD) | ||||
| All | 50 (12) | 44 (12) | 38 (13) | <0.001 |
| Males | 51 (11) | 45 (12) | 40 (13) | <0.001 |
| Females | 46 (9) | 41 (11) | 35 (12) | <0.001 |
| Gender n (%) | ||||
| Male | 79 (71) | 244 (70) | 470 (58) | <0.001 |
| BMI (kg·m-2) mean (SD) | ||||
| All | 26.9 (4.9) | 26.5 (4.0) | 25.5 (4.3) | <0.001 |
| Males | 27.5 (4.8) | 27.5 (4.9) | 26.5 (4.1) | 0.001 |
| Females | 25.2 (4.8) | 24.4 (3.5) | 24.0 (4.2) | 0.004 |
| Overweight * n (%) | ||||
| All | 490 (44) | 131 (43) | 247 (36) | n.s. |
| Males | 391 (49) | 77 (39) | 181 (44) | n.s. |
| Females | 97 (30) | 32 (36) | 66 (24) | n.s. |
| Obese **n (%) | ||||
| All | 220 (20) | 55 (18) | 94 (14) | n.s. |
| Males | 179 (23) | 57 (29) | 72 (18) | 0.012 |
| Females | 41 (13) | 5 (6) | 22 (8) | n.s. |
| Fitness n (%) | ||||
| very fit | 220 (20) | 55 (18) | 94 (14) | n.s. |
| fit | 73 (7) | 24 (8) | 49 (7) | 0.002† |
| moderately fit | 568 (51) | 124 (39) | 332 (46) | |
| unfit | 69 (6) | 17 (5) | 61 (8) |
DIVING HISTORY AND CHARACTERISTICS
DAN members reported having conducted a total of 812,685 dives, PM reported 603,564 dives and the PD had conducted a total of 84,899 dives. With medians of 14 and 15 years respectively, DAN and PM divers had been diving far longer than the PD group, who had dived for a median of four years (P < 0.01). On average, PM divers reported many more dives (median 800) than the DM (330) and PD cohorts (28), and the proportions of each cohort who reported having done more than 200 dives were 72% (DAN), 83% (PM) and 7.5% (PD). PM divers had also done more dives in the previous year (median 50) than DM (30) and PD divers (10). Sixty-two per cent of the DM and 60% of the PM had dived in the month prior to the survey, compared to only 24% of the PD cohort (Table 3). The numbers of divers undertaking decompression dives or technical diving were too small for useful analysis. However, 80% of the divers in each group reported commonly doing repetitive diving (Table 3).
Table 3. Diving history and characteristics of combined survey participants; OW − open water; OW+ − post-basic certification other than others listed; Tech − technical diver; DM − divemaster; Inst − instructor; Comm − commercial diver; * hold commercial qualifications but still dive recreationally .
| Group | DAN Members | PADI Members | PADI Divers | P-value |
| Years diving, med (range) | 14 (1−60) | 15 (1−47) | 4 (1−45) | < 0.01 |
| OW only | 34 (4) | NA | 299 (37) | < 0.01 |
| OW+ | 357 (39) | NA | 483 (60) | |
| Tech | 126 (14) | NA | 17 (2) | |
| DM | 203 (22) | 143 (41) | NA | |
| Inst | 160 (17) | 178 (51) | NA | |
| Comm* | 35 (4) | 28 (8) | 6 (<1) | |
| Total dives, med (range) | 330 (4−16,000) | 800 (15−20,000) | 28 (4−10000) | <0.001 |
| Dives past year, med (range) | 30 (0−500) | 50 (2−1000) | 10 (0−200) | <0.001 |
| Time since last dive, months (%) | ||||
| <0.001 | 673 (62) | 208 (60) | 194 (24) | <0.001 |
| 1 to < 6 | 322 (30) | 82 (24) | 267 (33) | |
| 6 to < 12 | 72 (7) | 37 (11) | 270 (34) | |
| ≥ 12 | 19 (2) | 19 (5) | 71 (9) | |
| Dives > 30 m deep (%; med (IQR)) | 10 (3−25) | 10 (5−25) | 1 (0−10) | |
| Repetitive dives (%; med (IQR)) | 80 (40−95) | 80 (50−95) | 80 (38−100) |
MEDICAL CONDITIONS
A total of 692 respondents reported suffering from diabetes, or a cardiovascular, respiratory, neurological or psychological condition. These included 376 (34%), 97 (28%) and 222 (28%) of the DM, PM and PD cohorts, respectively. Three respondents reported multiple conditions. With the exception of cardiac conditions (P = 0.099), the cohorts differed significantly in the proportions with the other medical conditions (P < 0.001 for all except neurological conditions P = 0.033). The most obvious difference was the higher incidence of hypertension in the older cohorts. The numbers reporting inner ear injuries (39 DM, 15 PM and 25 PD respectively) are unexpectedly high. Figure 1 compares the proportions in the Australian adult population with particular medical conditions, as reported in Australian Bureau of Statistics National Health Survey 2014–2015,11 to those in our survey respondents.
Figure 1.
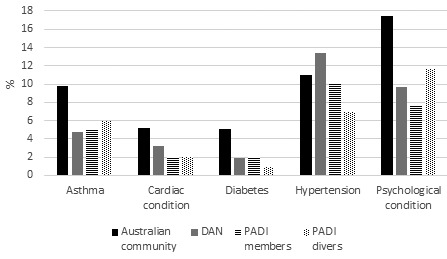
Comparative proportions of medical conditions in the general community[ 11] and the diving survey cohorts
DECOMPRESSION ILLNESS
Eighty-four respondents, 58 (5%) DM, 18 (5%) PM and 8 (1%) PD, reported being treated for DCI (seven on more than one occasion). This yields an approximate DCI prevalence in the respondent cohorts of 7.1 per 100,000 dives (95% CI 5.4−9.2) for DM; 3.0 per 100,000 dives (95% CI 1.8−4.7) for PM and 9.4 per 100,000 dives (95% CI 4.1−18.6) for the PD group (P < 0.001).
LIFE-THREATENING INCIDENTS
A total of 81 of the 1,156 PADI-S respondents reported what they perceived to have been a life-threatening incident while diving. Fifty of these individuals were PM and 31 PD divers. These included 92 incidents and identified 137 precipitating problems, 87 of which involved PM and 50 PD divers (Table 4). Numbers were too small for useful statistical analysis. Based on denominators of 603,564 and 84,899 reported total dives for the PM and PD cohorts respectively, the prevalence of a life-threatening event in the respondents was 8.3 per 100,000 dives (95% CI: 6.1−10.9) for the PM and 36.5 per 100,000 dives (95% CI: 24.8−51.8) for the PD cohort.
Table 4. Prevalence of perceived life-threatening incidents in the PADI surveys; no statistically significant differences between the groups; CI – confidence interval .
| Life-threatening incidents (n) | PADI members | PADI divers |
| Gas supply | 16 | 6 |
| Sea/weather | 12 | 8 |
| Overhead environment | 6 | 4 |
| Marine animal | 5 | 0 |
| Equipment fault | 12 | 8 |
| Equipment misuse | 1 | 2 |
| Medical condition | 0 | 1 |
| Anxiety/panic | 5 | 6 |
| Lack skills/experience | 9 | 4 |
| Own error | 16 | 6 |
| Own error | 16 | 6 |
| Other's error | 16 | 5 |
| Total incidents | 87 | 50 |
| Total dives | 603,564 | 84,899 |
| Incidents/100,000 dives | 8.3 | 36.5 |
| (95% CI) | (6.1−10.9) | (24.8−51.8) |
Discussion
The varying demographics and diving characteristics of the three cohorts indicate that a survey of a single diver cohort may not be representative of the Australian diving population. These data represented two cohorts of relatively or highly experienced, often long-term active divers (DM and PM). The other cohort (PD) comprised predominantly inexperienced divers who had been diving for four years or less. However, this latter cohort also included some more experienced divers who had upgraded their certification (to one other than a leadership certification) during the previous four years.
DEMOGRAPHICS
A review of Australian sporting surveys from 2001 to 2010 inclusive indicated that 76% of Australian divers were male.[ 12] This gender distribution is reflected in both the DM and PM cohorts of mainly longer-term divers. However, there was a higher proportion of females among the more recently-certified divers and those undergoing further training in the PD cohort. These surveys also indicated that 30% of Australian divers were aged 45 years or older, this proportion being identical to that of the PD cohort but considerably lower than the proportions in the DM (65%) and PM (47%) divers. This suggests that older divers in these cohorts (or at least the survey respondents) are over-represented or that highly qualified divers continue the sport for longer and that older divers are more likely to take out diving insurance.
The proportion of DM and PM divers who were either overweight or obese was similar to that found in the general Australian adult population,[ 11] whereas the corresponding proportion in the PD cohort was substantially lower, likely reflective of the younger age of this respondent cohort.[ 11] However, the obesity rate in the general population (27%)[ 13] is higher than in our respondent cohorts, which may reflect a greater level of physical activity in the diving cohort, 93% of whom perceived themselves to be at least moderately fit. However, this perception needs to be interpreted cautiously as there are no directly comparable data from the general population, and self-reported fitness, especially without further questions about specific activities, does not always correlate well with that measured objectively.[ 14 , 15]
DIVING HISTORY AND PRACTICES
The DM and PM cohorts were predominantly experienced and moderately to highly active divers. This is unsurprising given that much of this cohort had current dive insurance and/or were dive masters or instructors. On the other hand, most of the PD cohort were relatively new divers and dived less frequently; their median of 10 dives over the previous year being consistent with an unpublished survey from the Australian Sports Commission for 2001–2010 also reporting a median of 10 dives per year. (Rauber G, personal communication, 2014).
The large proportion of post-basic certifications in all cohorts is encouraging from the dive safety perspective, as further education and training should enhance knowledge and skills and offers the opportunity to increase experience in a more controlled manner. The high proportion of PM who dived near home is likely reflective of the fact that many of these are working dive professionals. On the other hand, the DM and PD cohorts did around one third of their diving overseas. The reported high rate of repetitive diving is typical of modern-day, computer-guided recreational diving whilst technical and decompression diving made up a very small proportion of the diving of all respondent cohorts.
MEDICAL CONDITIONS
The age-specific Australian asthma prevalence for 2014−2015 is estimated to have been a minimum rate of 10.5% (95% CI: 9.2, 11.8) for the age range from 15 to 74 years.[ 16] This suggests that the reported proportion of respiratory conditions (almost all asthma) in each of our diving cohorts was lower than in the general adult Australian population. This may be a result of the historical discouragement of people with asthma from partaking in scuba diving.[ 17] In addition, the lower rate of diabetes and cardiac conditions in the diving group likely reflects a similarly cautious approach to diving with these conditions. The slightly higher proportion of DAN respondents with cardiac conditions is consistent with the greater average age of this cohort.[ 18] The presence of co-existing cardiac conditions is well-represented in dive fatality reports,[ 6 , 7 , 19] although divers with known and well-managed cardiac conditions are known to dive with relative safely.[ 20 , 21]
It is interesting to note that 8−12% of respondents continued to dive despite a psychological disorder. This deserves further research, especially relating to medications taken to control the disorders and any impact these may have on diving safety.[ 22] The reported incidence of inner ear problems seems disproportionally high, and the authors suspect is the result of confusion amongst some responders between inner ear and middle ear problems, the latter being much commoner in diving.
DECOMPRESSION ILLNESS
The rates of DCI in different diving cohorts are dependent on a variety of factors, including diving conditions and practices, differences in diver characteristics, data reliability and calculation methodology and, therefore, vary widely between reports. It has been reported that the incidence of decompression sickness in recreational divers is 0.01–0.02% (10–19 cases per 100,000 dives).[ 23] The comparatively low rate of DCI in respondents to these surveys suggest that these cohorts dive relatively safely, although, for the reasons outlined earlier, this should be interpreted cautiously.
LIFE-THREATENING INCIDENTS
The rates for perceived life-threatening incidents are sobering. When compared to the estimated annual fatality rate for Australian divers (0.46 per 100,000 dives),[ 12] the prevalence rates for perceived ‘near-misses’ were many times higher in the PADI surveys. This needs to be interpreted cautiously as it is based on low response rates but implies that, for each fatality, there may be a considerable number of near-misses. Longer-term divers are more likely to have experienced such an incident, but the likelihood of occurrence probably reduces with experience. It is also possible that some less-experienced divers over-report these incidents, perceiving something to be life-threatening that may not be so.
As with most activities, whether recreational or occupational, there are many more non-fatal incidents than deaths. For example, a 12-year analysis of recreational dive-related incidents in the United Kingdom (UK) recorded a total of 4,799 incidents, of which 197 (4.1%) were fatal.[ 19] Non-fatal incidents are potentially a far richer source of information, not only due to the greater volume, but also because the victim can often provide valuable information, unlike in a fatality. The British Sub-Aqua Club, DAN America and DAN AP collect data on non-fatal diving incidents in their regions and divers are encouraged to report these.
In these surveys, despite the low response rates, the major categories of equipment, gas supply and conditions-related incident triggers appeared strikingly similar to the suspected incident triggers that result in Australian diving fatalities.[ 6] Equipment and anxiety-related incidents were more common in less experienced divers, likely a result of less familiarity with the equipment and diving environment. The higher incidence of dangerous marine animal encounters in the more experienced divers likely reflects greater exposure. The smaller proportion of gas supply-related problems in the newer divers may be a result of lower exposure and/or less complacency or, in some cases, closer supervision.
Equipment-related problems remain common and contribute to deaths (and near deaths) at a comparable rate in Australia to those in the USA (15%)[ 7] and UK (20%).[ 19] They are often preventable with appropriate familiarisation and maintenance. This need for adequate familiarisation and maintenance is especially true for closed circuit rebreathers (CCRs) which were associated with about a quarter of all the reported equipment-related incidents in the PADI cohorts. This rate seems disproportionately high given the small number of respondents using CCRs. These data, combined with fatality data from the UK and elsewhere, support the assertion that, because of their greater complexity, there is a higher risk of mechanical failure and indeed death with CCRs compared to open-circuit scuba.[ 24]
Despite the ubiquitousness of generally accurate pressure gauges, breathing gas supply problems persist, contributing to 12–18% of the near misses in this series and being a suspected trigger in an alarming 41% of US diving deaths.[ 7] Although the unpredictable can occur and catch a diver unawares, good dive preparation, including gas consumption planning and monitoring, can prevent many 'out of air' emergencies. In addition, the high incidence of problems related to currents, surge and rough seas demonstrate that even experienced divers must take care with dive site selection and monitoring.
LIMITATIONS
There are a variety of limitations to this study, the major one being the low and differing response rates. This non-response creates the potential for the data not to accurately reflect each group. However, large numbers within the groups and the substantial differences between them suggest that, while selection bias may have affected the results, it is unlikely that it was so large that it was responsible for all the observed group differences.
In addition, DAN members are likely older than the general diving population and respondents to the DAN-S were younger than non-respondents, possibly introducing some selection bias. Although there were no details of non-respondents to the PADI surveys, it appears that they were likely older than non-respondents and there was a higher response rate from females, potential sources of selection bias. The very low response rate from the PADI divers would likely introduce further bias towards more experienced divers or enthusiastic divers who engage with the sport.
Whilst many Australian divers will fall into one of these population groups, they will not be representative of the entire Australian diving population. Although it would have been useful to examine age-specific combined data, this was not possible as the ages of the PADI populations were not available. The nature of some of the more historical questions, such as the number and characteristics of dives undertaken, may have introduced a recall bias and this may be more likely in the longer-term divers. Finally, self-reporting on medical conditions, diving activities and events may have been another source of reporting bias.
Conclusions
Although limited by low and differing response rates and potential response bias, this study indicates that there are differences in the health-related conditions and diving experiences of the respondents in the three survey groups. Therefore, a survey of any single diver group may not be representative of the general recreational diving population and the findings from such surveys may be misleading. This bias needs to be clearly understood and any survey findings interpreted accordingly. Despite their limitations, these data provide an insight into the varying demographics, diving practices and outcomes of these groups of active Australian divers and can provide a background for further research in accident mitigation, other safety initiatives and industry planning.
Footnotes
Acknowledgements
The authors wish to acknowledge the assistance of PADI Asia-Pacific enabling access to members and divers, and to Adam Lippmann and Scott Jamieson for assisting with data collection.
Conflicts of interest and funding
John Lippmann is Chairman of DAN Asia-Pacific which sells dive injury insurance.
Contributor Information
J Lippmann, Divers Alert Network Asia-Pacific, Ashburton, Victoria, Australia; School of Health and Social Development, Deakin University, Melbourne.
D McD Taylor, Department of Emergency Medical Research, Austin Hospital, Melbourne, Victoria; Department of Medicine, Melbourne University, Victoria.
C Stevenson, School of Health and Social Development, Deakin University, Melbourne.
JW Williams, School of Health and Social Development, Deakin University, Melbourne.
References
- Byron T. History of spearfishing and scuba diving in Australia – the first 80 years 1917 to 1997 Sydney: Tom Byron Publications; 1998. [Google Scholar]
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, et al. Heart disease and stroke statistics-2015 update: a report from the American Heart Association . [cited 2015 December 21];Circulation. 2015 131:e29–e322. doi: 10.1161/CIR.0000000000000152. Available from: http://circ.ahajournals.org/content/131/4/e29 . [DOI] [PubMed] [Google Scholar]
- Berenji Ardestani S, Buzzacott P, Eftedal I. The aging diver: endothelial biochemistry and its potential implications for cardiovascular health . Diving Hyperb Med. 2015;45:235–239. [PubMed] [Google Scholar]
- Pougnet R, Constanzo L, Lodde B, Henckers A, Dherbecourt L, Lucas D, et al. Cardiovascular risk factors and cardiovascular assessment in professional divers . Int Marit Health. 2012;63:164–169. [PubMed] [Google Scholar]
- Jousilahti P, Vartiainen E, Tuomilehto J, Uuska P. Sex, age, cardiovascular risk factors and coronary heart disease: a prospective follow-up study of 14,786 middle-aged men and women in Finland . Circulation. 1999;99:1165–1172. doi: 10.1161/01.cir.99.9.1165. [DOI] [PubMed] [Google Scholar]
- Lippmann J, Baddeley A, Vann R, Walker D. An analysis of the causes of compressed gas diving fatalities in Australia from 1972–2005 . Undersea Hyperb Med. 2013;40:49–61. [PubMed] [Google Scholar]
- Denoble PJ, Caruso JL, Dear Gde L, Pieper CF, Vann RD. Common causes of open-circuit recreational diving fatalities . Undersea Hyperb Med. 2008;35:393–406. [PubMed] [Google Scholar]
- Lippmann J, McD Taylor D, Stevenson C, Mitchell S. The demographics and diving behaviour of DAN Asia-Pacific members with and without pre-existing medical conditions . Diving Hyperb Med. 2016;46:200–6. [PubMed] [Google Scholar]
- National Statistical Service . [cited 2015 August 16]. Sample size calculator. Available from: http://www.nss.gov.au/nss/home.NSF/pages/Sample+size+calculator .
- Ihaka R, Gentleman R. R: A language for data analysis and graphics . J Comp Graph Stat. 1996;5:299–314. [Google Scholar]
- Australian Bureau of Statistics . 4364.0.55.001 - National Health Survey: First results 2014–15. 2015. [cited 2017 February 04]. Available from: http://www.abs.gov.au/ausstats/abs@.nsf/Lookup/by%20Subject/4364.0.55.001~2014-15~Main%20Features~About%20the%20National%20Health%20Survey~3 .
- Lippmann J, Stevenson C, McD Taylor D, Williams J. Estimating the risk of a scuba diving fatality in Australia . Diving Hyperb Med. 2016;46:241–7. [PubMed] [Google Scholar]
- Australian Institute of Health and Welfare (AIHW) 2015 . Cardiovascular disease, diabetes and chronic kidney disease - Australian facts: risk factors. Cardiovascular, diabetes and chronic kidney disease series no. 4. Cat. no. CDK 004. AIHW: [cited 2017 January 25]. Available from: "http://www.aihw.gov.au/publication-detail/?id=60129550538 . [Google Scholar]
- Obling KH, Hansen A-LS, Overgaard K, Normann K, Sandbaek A, Maindal HT, et al. Association between self-reported and objectively measured physical fitness level in a middle-aged population in primary care . Prev Med Rep. 2015;2:462–6. doi: 10.1016/j.pmedr.2015.05.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knapik JJ, Jones BH, Reynolds KL, Staab JS. Validity of self-assessed physical fitness . Am J Prev Med. 1992;8:367–72. [PubMed] [Google Scholar]
- Australian Institute of Health and Welfare (AIHW) . Asthma and other chronic respiratory conditions. [cited 2017 November 20]. Available from: https://www.aihw.gov.au/reports/asthma-other-chronic-respiratory-conditions/asthma/data .
- Victorian Asthma Foundation . Policy of the Victorian Asthma Foundation Exercise challenge test: is a 15% fall in FEV1 sufficient for diagnosis . SPUMS J. 1987;17:133–4. [Google Scholar]
- Australian Institute of Health and Welfare (AIHW) . [2017 December 13]; How many Australian have cardiovascular disease. 2011–2012 . Available from: http://www.aihw.gov.au/cardiovascular-disease/prevalence .
- Cumming B, Peddie C, Watson . A review of the nature of diving in the United Kingdom and of diving fatalities (1998-2009) In: Vann RD, Lang MA, editors. Recreational diving fatalities. Proceedings of the Divers Alert Network 2010 April 8–10 Workshop. Durham, NC: Divers Alert Network; 2011. pp. 99–117. [Google Scholar]
- Lippmann J, McD Taylor D, Stevenson C, Williams J, Mitchell S. Diving with pre-existing health conditions . Diving Hyperb Med. 2017;47:180–90. doi: 10.28920/dhm47.3.180-190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- St Leger Dowse M, Waterman MK, Penny CE, Smerdon GR. Does self-certification reflect the cardiac health of UK sport divers? . Diving Hyperb Med. 2015;45:184–9. [PubMed] [Google Scholar]
- Querido AL. Diving and antidepressants . Diving Hyperb Med. 2017;47:253–6. doi: 10.28920/dhm47.4.253-256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vann RD, Butler FK, Mitchell SJ, Moon RE. Decompression illness . Lancet. 2010;377:153–64. doi: 10.1016/S0140-6736(10)61085-9. [DOI] [PubMed] [Google Scholar]
- Fock AW. Analysis of recreational closed-circuit rebreather deaths 1998–2010 . Diving Hyperb Med. 2013;43:78–85. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Citations
- National Statistical Service . [cited 2015 August 16]. Sample size calculator. Available from: http://www.nss.gov.au/nss/home.NSF/pages/Sample+size+calculator .