

Abstract
Background
Botulism is an acute paralytic illness caused by a neurotoxin produced by Clostridium botulinum. Supportive care, including intensive care, is key, but the role of other medical treatments is unclear. This is an update of a review first published in 2011.
Objectives
To assess the effects of medical treatments on mortality, duration of hospitalization, mechanical ventilation, tube or parenteral feeding, and risk of adverse events in botulism.
Search methods
We searched the Cochrane Neuromuscular Specialised Register, CENTRAL, MEDLINE, and Embase on 23 January 2018. We reviewed bibliographies and contacted authors and experts. We searched two clinical trials registers, WHO ICTRP and clinicaltrials.gov, on 21 February 2019.
Selection criteria
Randomized controlled trials (RCTs) and quasi‐RCTs examining the medical treatment of any of the four major types of botulism (infant intestinal botulism, food‐borne botulism, wound botulism, and adult intestinal toxemia). Potential medical treatments included equine serum trivalent botulism antitoxin, human‐derived botulinum immune globulin intravenous (BIG‐IV), plasma exchange, 3,4‐diaminopyridine, and guanidine.
Data collection and analysis
We followed standard Cochrane methodology.
Our primary outcome was in‐hospital death from any cause occurring within four weeks from randomization or the beginning of treatment. Secondary outcomes were death from any cause occurring within 12 weeks, duration of hospitalization, duration of mechanical ventilation, duration of tube or parenteral feeding, and proportion of participants with adverse events or complications of treatment.
Main results
A single RCT met the inclusion criteria. Our 2018 search update identified no additional trials. The included trial evaluated BIG‐IV for the treatment of infant botulism and included 59 treatment participants and 63 control participants. The control group received a control immune globulin that did not have an effect on botulinum toxin. Participants were followed during the length of their hospitalization to measure the outcomes of interest. There was some violation of intention‐to‐treat principles, and possibly some between‐treatment group imbalances among participants admitted to the intensive care unit and mechanically ventilated, but otherwise the risk of bias was low. There were no deaths in either group, making any treatment effect on mortality inestimable. There was a benefit in the treatment group on mean duration of hospitalization (BIG‐IV: 2.60 weeks, 95% confidence interval (CI) 1.95 to 3.25; control: 5.70 weeks, 95% CI 4.40 to 7.00; mean difference (MD) ‐3.10 weeks, 95% CI ‐4.52 to ‐1.68; moderate‐certainty evidence); mechanical ventilation (BIG‐IV: 1.80 weeks, 95% CI 1.20 to 2.40; control: 4.40 weeks, 95% CI 3.00 to 5.80; MD ‐2.60 weeks, 95% CI ‐4.06 to ‐1.14; low‐certainty evidence); and tube or parenteral feeding (BIG‐IV: 3.60 weeks, 95% CI 1.70 to 5.50; control: 10.00 weeks, 95% CI 6.85 to 13.15; MD ‐6.40 weeks, 95% CI ‐10.00 to ‐2.80; moderate‐certainty evidence), but not on proportion of participants with adverse events or complications (BIG‐IV: 63.08%; control: 68.75%; risk ratio 0.92, 95% CI 0.72 to 1.18; absolute risk reduction 0.06, 95% CI 0.22 to ‐0.11; moderate‐certainty evidence).
Authors' conclusions
We found low‐ and moderate‐certainty evidence supporting the use of BIG‐IV in infant intestinal botulism. A single RCT demonstrated that BIG‐IV probably decreases the duration of hospitalization; may decrease the duration of mechanical ventilation; and probably decreases the duration of tube or parenteral feeding. Adverse events were probably no more frequent with immune globulin than with placebo. Our search did not reveal any evidence examining the use of other medical treatments including serum trivalent botulism antitoxin.
Keywords: Humans; Infant; Botulinum Toxins; Botulism; Botulism/therapy; Critical Care; Critical Care/methods; Hospitalization; Immunoglobulins; Immunoglobulins, Intravenous; Immunoglobulins, Intravenous/therapeutic use; Parenteral Nutrition; Randomized Controlled Trials as Topic; Respiration, Artificial
Medical treatment for botulism
Review question
We reviewed the evidence on the effect of medical treatment on human botulism.
Background
Botulism is a serious illness that starts suddenly and causes paralysis (an inability to use muscles). The cause of botulism is a germ called Clostridium botulinum. If the illness is left untreated, many people with botulism will die. There are four main types of botulism: adult and infant types where the intestine (gut) is infected; botulism from contaminated food; and wound botulism.
We searched for clinical trials of medical treatments for any of the four major types of botulism. We assessed the effects of treatment on the rate of deaths in hospital from any cause within four weeks of infection. We were also interested in deaths within 12 weeks, length of hospital stay, the need for a ventilator to help with breathing (mechanical ventilation), feeding by tube, and harmful events of treatment.
Study characteristics
Our searches of the medical literature revealed one relevant study, which was in infant botulism. The treatment was a single dose of a medicine made from human immune proteins (human‐derived botulinum immune globulin intravenous, or BIG‐IV). Fifty‐nine infants received BIG‐IV, and 63 infants received a placebo (inactive treatment). Each study participant was followed up for the duration of their hospitalization. This study was sponsored by the California Department of Health Services.
Key results and certainty of the evidence
There were no deaths in either group in the trial. Infants treated with BIG‐IV spent, on average, about three weeks less time in hospital (i.e. 3.1 weeks versus 5.7 weeks) than infants who received the inactive treatment, and spent about three weeks less on a ventilator (1.8 weeks versus 4.4 weeks). The average duration of tube feeding in the BIG‐IV group was more than six weeks less than in the placebo group (i.e. 3.6 versus 10 weeks). The risk of harmful effects of the treatment was probably no greater with BIG‐IV than with the inactive treatment. The evidence was mostly of moderate certainty (low certainty for time spent on a ventilator).
The review shows that BIG‐IV probably shortens hospitalization; may shorten time spent on a ventilator; and probably reduces the duration of tube feeding compared to placebo. On the other hand, we found no evidence for or against botulism antitoxin or other treatments for botulism.
The evidence is up‐to‐date to January 2018, when we updated the searches and found no new trials.
Summary of findings
Summary of findings for the main comparison.
Human‐derived botulinum immune globulin intravenous for infant botulism
| Human‐derived botulinum immune globulin intravenous for infant botulism | ||||||
| Patient or population: individuals with infant botulism Settings: hospital Intervention: human‐derived botulinum immune globulin intravenous Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No. of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Placebo | Human‐derived botulinum immune globulin intravenous | |||||
| In‐hospital death from any cause occurring within 4 weeks of randomization or the beginning of treatment | See comment | See comment | Not estimable | 122 (1 study) | ⊕⊕⊕⊝ moderatea | No deaths occurred in the included study. |
| Duration of hospitalization (in weeks) | The mean duration of hospitalization in the control groups was 5.7 weeks. | The mean duration of hospitalization in the intervention groups was 3.1 lower (4.52 to 1.68 lower). | ‐ | 122 (1 study) | ⊕⊕⊕⊝ moderatea | ‐ |
| Duration of mechanical ventilation (in weeks) | The mean duration of mechanical ventilation in the control groups was 4.4 weeks. | The mean duration of mechanical ventilation in the intervention groups was 2.6 lower (4.06 to 1.14 lower). | ‐ | 59 (1 study) | ⊕⊕⊝⊝ lowa,b | ‐ |
| Duration of tube or parenteral feeding (in weeks) | The mean duration of tube or parenteral feeding in the control groups was 10 weeks. | The mean duration of tube or parenteral feeding in the intervention groups was 6.4 lower (10 to 2.8 lower). | ‐ | 122 (1 study) | ⊕⊕⊕⊝ moderatea | ‐ |
| Risk of adverse events (until time of hospital discharge) | 688 per 1000 | 632 per 1000 (495 to 811) | RR 0.92 (0.72 to 1.18) | 129 (1 study) | ⊕⊕⊕⊝ moderatea | ‐ |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence High certainty: Further research is very unlikely to change our confidence in the estimate of effect. Moderate certainty: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low certainty: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low certainty: We are very uncertain about the estimate. | ||||||
aWe downgraded the evidence once for study limitations due to the baseline imbalance between the comparator groups, in particular, age, weight, and sex, and because intention‐to‐treat principles were violated when the efficacy analyses excluded seven participants who were initially enrolled in the trial but were later found not to have infant botulism. bWe downgraded the evidence a second time for study limitations. Sixty‐three participants who were never mechanically ventilated were excluded from this analysis, thereby compromising randomized treatment allocation and allowing for possible between‐treatment group imbalances and uncontrolled confounding.
Background
Description of the condition
Botulism is an acute paralytic illness caused by a neurotoxin produced by the bacterium Clostridium botulinum. C botulinum is a sporulating (spore‐forming), obligate anaerobic, gram‐positive bacillus, and is ubiquitous in soil and aquatic sediment. There are seven types of C botulinum, differentiated by the antigenicity of the neurotoxin produced. Types A, B, and E are most often implicated in human disease (Dowell 1984).
Botulinum neurotoxin (BoNT), a 150 kDa protein, is among the most potent known toxins. Some authors have estimated that as little as 1 g of aerosolized BoNT could lead to the death of over 1.5 million people (McNally 1994). Botulinum neurotoxin binds to receptors in the presynaptic cell membrane of the neuromuscular junction. Endocytosis allows the 50 kDa light chain of the neurotoxin to cross the neuronal cell membrane. Within the axon terminal, BoNT acts as a protease, interrupting exocytosis through the cleavage of three different components of the synaptic fusion complex including SNAP‐25, syntaxin, and synaptobrevin (Dembek 2007). Through this proteolytic activity, BoNT prevents the release of neurotransmitter vesicles into the synaptic cleft, in particular those responsible for the release of acetylcholine. Failure of neuromuscular transmission ensues, resulting in muscle weakness or paralysis.
There are four major forms of human botulism: infant botulism, food‐borne botulism, wound botulism, and adult intestinal toxemia botulism. There are also case reports of inhalational botulism as well as iatrogenic botulism, following cosmetic or therapeutic injection of BoNT, but these remain exceedingly rare (Sobel 2005).
A median of 71 reported cases of infant botulism occur annually in the USA (Shapiro 1998), although it is estimated that the true number of cases may be as high as 250 (Cox 2002). Between 1976 and 2006, 524 cases were reported in 25 countries in Asia, Australia, Europe, and the Americas, although this is also presumed to be a gross underestimate due to under‐reporting (Koepke 2008). Food‐borne botulism is less common, with roughly 24 cases reported annually in the USA and 62 cases reported in the UK between 1922 and 2005 (McLauchlin 2006; Shapiro 1998). Wound and adult intestinal toxemia botulism are the least common, with only a few cases reported annually (Shapiro 1998).
Both infant and adult enteric toxemia botulism occur after the ingestion of C botulinum spores, typically found in honey or soil, which germinate in the host’s gastrointestinal tract and subsequently produce BoNT (Cox 2002). Wound botulism occurs after the direct introduction of spores into devitalized flesh, classically after crush injuries to an extremity, but increasingly among injection drug users as well (Brett 2005; Sieradzan 2005). Food‐borne botulism differs from other types of botulism in that it occurs after the ingestion of preformed BoNT. It occurs with the ingestion of foods such as home‐canned comestibles and salted, smoked, or fermented meats, where C botulinum spores have suitable environments to germinate (Sobel 2005).
The clinical course of botulism may be heralded by the onset of nausea and vomiting, the exact mechanism of which is unclear. These features are conspicuously absent in wound botulism (Sobel 2005). Cranial nerve symptoms and signs are consistently the initial neurological manifestation, presenting as blurred vision and photophobia, diplopia, ptosis, dysarthria, dysphonia, and dysphagia (Dembek 2007). Varying degrees of descending and symmetrical muscle paralysis, beginning with the neck muscles and progressing to respiratory and limb muscles, often follow the initial deficits. In an outbreak of food‐borne botulism in the Nan province of Thailand involving 163 individuals, 9.3% of hospitalized patients had weakness of the extremities, while 29.8% required mechanical ventilation (CDC 2006). Autonomic dysfunction may also be present, characterized by orthostatic hypotension, dilated and fixed pupils, xerostomia, intestinal ileus, and urinary retention (Dembek 2007).
The rapidity of disease onset and rate of progression depend on the dose of the neurotoxin, with a range of hours to several days. Death from botulism typically occurs due to airway obstruction secondary to pharyngeal muscle paralysis, and respiratory arrest in the context of respiratory muscle and diaphragmatic failure (Sobel 2005).
Description of the intervention
If left untreated, botulism has a mortality rate of 40% to 50% (Dembek 2007). Modern intensive care therapy, particularly mechanical ventilation, has had a large impact on the outcome of the disease. Over the past 40 years several different medical therapies have also been introduced. In the 1960s, trivalent equine‐derived antitoxin became available and is now widely used (Dembek 2007). In October 2003, the US Food and Drug Administration approved human botulinum immune globulin intravenous (BIG‐IV) for the treatment of infant botulism. This blood product is derived from the pooled plasma of human adults immunized with pentavalent botulinum toxoid. It has been presented as having a far lower risk of anaphylaxis when compared to trivalent equine antitoxin (Robinson 2003). Other suggested medical therapies include guanidine hydrochloride, a derivative of the nucleic acid guanine, and 3,4‐diaminopyridine, a presynaptic potassium channel blocker, both of which promote presynaptic release of acetylcholine at the neuromuscular junction (Davis 1992; Kaplan 1979). Finally, there have been an increasing number of advocates of plasma exchange for botulism (Sato 2000).
How the intervention might work
Trivalent equine‐derived antitoxin and human‐derived botulism immune globulin intravenous are assumed to directly block or inhibit the effect of BoNT at the presynaptic membrane, or nerve terminal. Guanidine and 3,4‐diaminopyridine enhance nerve terminal release of acetylcholine by blocking voltage‐gated potassium channels involved in nerve terminal membrane repolarization. The putative mechanism of plasma exchange in botulism is unclear.
Why it is important to do this review
Despite the potentially devastating impact of botulism, the effectiveness of these medical therapies remains unclear. Several factors have contributed to this: the relative rarity of botulism, making participant recruitment a challenge; the perception that certain therapies are standard practice and, therefore, a placebo‐controlled trial may be ethically untenable; and limited government or industry interest in funding clinical trials in botulism. The aim of this systematic review was to assess whether there is sufficient evidence to support the use of any medical therapy in the treatment of human botulism. This is the second update of a review first published in 2011.
Objectives
To assess the effects of medical treatments on mortality, duration of hospitalization, mechanical ventilation, tube or parenteral feeding, and risk of adverse events in botulism.
Methods
Criteria for considering studies for this review
Types of studies
We included randomized controlled trials (RCTs) or quasi‐RCTs, regardless of publication status, language, or period of participant inclusion. Placebo control or blinding were not required for inclusion of a trial in the review. Cross‐over trials were eligible for inclusion.
Types of participants
We included male or female participants, without age restriction. The reports had to state clearly the criteria for the diagnosis of botulism. Ideally laboratory data, such as identification of C botulinum toxin or the organism in the serum or the feces, or electrodiagnostic studies supported the diagnosis.
Types of interventions
We included equine serum trivalent botulinum antitoxin, human‐derived botulinum immune globulin intravenous, plasma exchange, 3,4‐diaminopyridine, and guanidine, and aimed to compare these with standard supportive treatment. The standard supportive treatment may or may not have included a placebo.
Types of outcome measures
Primary outcomes
In‐hospital death from any cause occurring within four weeks from randomization or the beginning of treatment.
We assessed this measure as a dichotomous variable. This measure is unambiguous and quantitative, and we anticipated that it would have been included in most or all studies. We considered it to be most meaningful clinically in botulism to treat mortality as a dichotomous rather than a continuous variable (i.e. death or not within a defined time, rather than time to death), where the overall mortality is low, and the goal of treatment is to decrease mortality rather than prolong survival. A particular difficulty with choosing a primary outcome measure in botulism is the large proportion of infants in the patient population, which limits the use of measures such as time to independent ambulation or scales grading motor function. Likewise, only a fraction of patients require mechanical ventilation or tube feeding, making time requiring those measures poorly representative of the impact of treatment. An important disadvantage of mortality is that it is likely to be determined to an extent by the quality of available supportive care. However, successful randomized treatment allocation would be expected to control for these sources of within‐study variability.
Secondary outcomes
Death from any cause occurring within 12 weeks from randomization or the beginning of treatment
Duration of hospitalization
Duration of mechanical ventilation
Duration of tube or parenteral feeding
Proportion of participants with adverse events or complications of treatment
Search methods for identification of studies
Electronic searches
We searched the following databases on 23 January 2018:
the Cochrane Neuromuscular Specialised Register via the Cochrane Register of Studies (CRS‐Web; Appendix 1);
the Cochrane Central Register of Controlled Trials (CENTRAL) via the CRS‐Web (Appendix 2);
MEDLINE (1946 to January 2018; Appendix 3);
Embase (1980 to January 2018; Appendix 4).
We searched the following clinical trial registries on 21 February 2019:
World Health Organization International Clinical Trials Registry Platform (WHO ICTRP: apps.who.int/trialsearch; Appendix 5);
US National Institutes of Health Ongoing Clinical Trials Register ClinicalTrials.gov (www.clinicaltrials.gov; Appendix 6).
We cross‐referenced the results of these register searches through MEDLINE and EBSCO to find available publications.
Searching other resources
We reviewed the bibliographies of identified randomized trials and contacted the author of one large study (Arnon 2006).
Data collection and analysis
Selection of studies
Two review authors independently reviewed the title and abstract of all studies identified by the search strategy. We did not identify any unpublished studies. The two review authors independently used an initial inclusion or exclusion form to determine whether the studies met the initial review criteria based on title and abstract. We obtained the full texts of all studies deemed potentially eligible for a more detailed assessment, and two review authors independently reviewed the full texts to determine whether or not to include the studies in the review. Any discrepancies were resolved by discussion between the two review authors; where the two review authors were unable to reach agreement, three review authors reached a consensus. We have reported the reasons for exclusion of those studies that met the initial review criteria and were prospective in design but that were excluded following full‐text review.
Data extraction and management
Two review authors independently extracted data onto data collection forms specifically designed for this review. The data extraction form included details of the study design, risk of bias (as noted below), inclusion and exclusion criteria for participants including form of botulism (i.e. infant botulism, food‐borne botulism, wound botulism, or adult intestinal toxemia botulism), numbers of participants, numbers of withdrawals, age of participants, intervention used, timing of the intervention, baseline participant parameters, outcome measures, and adverse effects. We were unable to obtain individual patient data from published studies. Any discrepancies were resolved by discussion between the two review authors; where the two review authors were unable to reach agreement, three review authors reached a consensus. One review author entered data, and a second review author confirmed its accuracy.
We collected and presented the available data on the cost‐effectiveness of medical treatment in the Discussion.
Assessment of risk of bias in included studies
Two review authors completed a 'Risk of bias' assessment on included studies as described by the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011a). We assessed random sequence generation, allocation concealment, blinding of participants and personnel and of outcome assessors, incomplete outcome data, and selective outcome reporting. We judged each of these criteria as high, low, or unclear risk of bias. Any discrepancies were resolved by discussion between the two review authors; where the two review authors were unable to reach agreement, three review authors reached a consensus.
Measures of treatment effect
We planned to analyze each medical therapy separately.
We measured the primary outcome, in‐hospital death within four weeks, and the secondary outcome measures of death within 12 weeks, duration of hospitalization, duration of mechanical ventilation, duration of tube or parenteral feeding, and adverse events or complications as either continuous (number of days) or dichotomous variables. For continuous data, we calculated the mean differences (MD) with 95% confidence intervals (CIs). All continuous outcomes are duration, the units for which we have converted to weeks. Standardised mean differences were not required given the easily achieved homogeneity of the continuous outcomes.
For dichotomous variables, we calculated the risk ratio (RR) and absolute risk reduction (ARR) with 95% CIs.
Unit of analysis issues
We did not encounter any unit of analysis issues. Our outcome measures were fixed endpoints, not repeated observations for the same outcome. We included any outcome reported as an adverse effect at any time during the trial, irrespective of whether that adverse effect eventually resolved.
Dealing with missing data
We did not encounter studies with missing data. We contacted the trial authors of the included study for individual participant data, however these data were not available.
We have described the methods used for dealing with missing data in Appendix 7.
Assessment of heterogeneity
We had planned to test for heterogeneity using Chi2 tests, but this was unnecessary with only one included study. See Appendix 7 for further details on the planned methods.
Assessment of reporting biases
We planned to perform an analysis of study size to measure the effect of reporting bias in the meta‐analysis (Egger 1997). This proved to be unnecessary with only one included study.
Data synthesis
We have reported the methods we planned to use to meta‐analyze data in Appendix 7.
'Summary of findings' table
We have included a 'Summary of findings' table with the following outcomes:
In‐hospital death from any cause within four weeks from randomization or the beginning of treatment;
duration of hospitalization;
duration of mechanical ventilation;
duration of tube or parenteral feeding;
time to regain independent ambulation (if applicable); and
proportion of participants with adverse events or complications of treatment.
We used the five GRADE considerations (study limitations, consistency of effect, imprecision, indirectness, and publication bias) to assess the certainty of a body of evidence (studies that contributed data for the prespecified outcomes). We used the methods and recommendations described in Section 8.5 and Chapter 12 of the Cochrane Handbook for Systematic Reviews of Interventions (Schünemann 2013a; Schünemann 2013b), employing GRADEpro software (GRADEpro 2008). We justified decisions to downgrade or upgrade the certainty of the evidence using footnotes.
Subgroup analysis and investigation of heterogeneity
We did not perform any subgroup analyses given that there was only a single included study with a homogeneous population. Furthermore, we were not able to analyze the timing of the initiation of treatment after disease onset due to a lack of available data. See Appendix 7 for planned subgroup analyses.
Sensitivity analysis
Sensitivity analyses (see Appendix 7) were unnecessary with only one included study.
This review has a published protocol (Chalk 2009). We have documented any differences between the methods of the review and the protocol in Differences between protocol and review.
Results
Description of studies
Results of the search
One study was included from the previous version of the review (Arnon 2006). The updated search retrieved the following citations from each database: MEDLINE = 313 (57 new), Embase = 68 (22 new), the Cochrane Neuromuscular Specialised Register = 3 (0 new), and CENTRAL = 4 (0 new). Our search of the WHO ICTRP and ClinicalTrials.gov identified two ongoing studies that may be of future interest, but none that are completed or not already identified by our search of electronic databases. We therefore identified a total of 81 new records from these searches. After removal of duplicates, there were a total of 73 citations. Sixty‐nine of the excluded studies were literature reviews, case reports, small retrospective case series, or pharmacokinetic studies on healthy individuals. We assessed four full‐text articles, but they were not randomised or not conducted in humans (Bradford 2018; Friggeri 2013; Khouri 2018; Mottate 2016).
A PRISMA flow chart illustrating the study selection process is shown in Figure 1.
Figure 1.
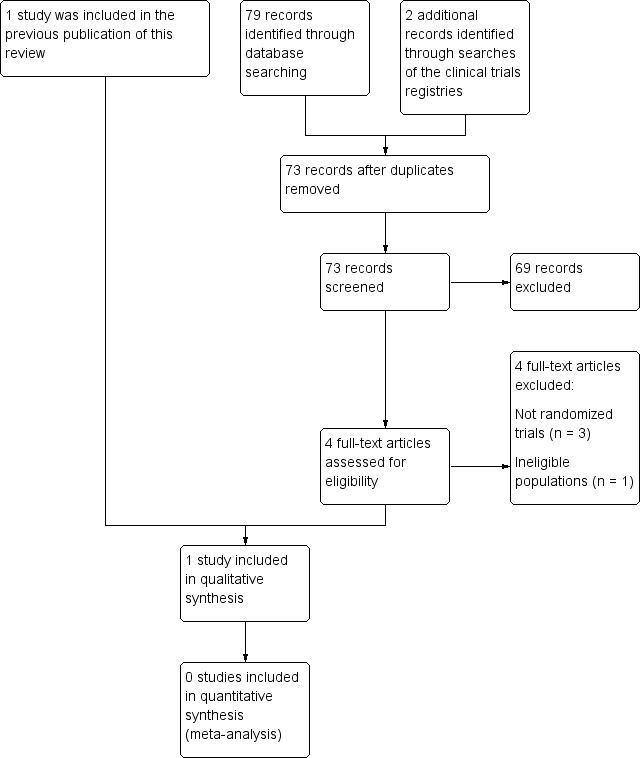
Study flow diagram.
Included studies
The included study was a parallel‐group, randomized, placebo‐controlled, participant‐, interviewer‐, and outcome assessor‐blinded trial that compared human‐derived botulism immune globulin intravenous (BIG‐IV) with a placebo control in the treatment of infant botulism (see Characteristics of included studies). The study was carried out in California from 1992 to 1997. Patients were eligible if they had a diagnosis of suspected infant botulism based on initial history, physical examination, and laboratory studies, and if they had been hospitalized for less than three days. Botulism was confirmed in all participants with the identification of C botulinum toxin or organisms in the participant’s feces. In the majority of cases this confirmation occurred after the administration of the BIG‐IV or the control treatment. The treatment group received a single intravenous infusion of BIG‐IV (50 mg/kg of body weight). The control group received intravenous immune globulin (Gammagard or Gammagard S/D) that was shown not to neutralize botulinum toxin in a mouse assay.
The included study involved 65 treatment and 64 control participants. However, one control and six treatment participants had negative laboratory examinations for C botulinum toxin or organisms and were excluded from the efficacy analyses, thereby violating intention‐to‐treat principles. Similar violations occurred in the analysis of the secondary outcomes of length of intensive care unit stay and duration of mechanical ventilation when these were limited to those participants who were admitted to the intensive care unit or mechanically ventilated, potentially resulting in further uncontrolled confounding. The safety analyses included all treatment participants. There was a significant difference in age at symptom onset, with a mean of 131 days in the treatment group and 105 days in the control group (two‐sided t‐test; P = 0.02). There was also a significant difference in weight, with a mean of 6.7 kg in the treatment group and 5.9 kg in the control group (two‐sided t‐test; P = 0.01). Otherwise, the study participants in the primary analysis were comparable for all other variables measured at baseline including mean time from symptom onset to treatment infusion (4.2 days in the treatment group and 4.3 days in the control group; two‐sided t‐test; P = 0.97). Approximately 60% of participants had type A botulinum toxin, while the remaining 40% had type B. There was no significant difference in the distribution of toxin types between the treatment and control groups (Fisher’s exact test; P = 0.79).
There were no deaths in either the treatment or control group, so we could not make estimates for our primary outcome, in‐hospital death from any cause within four weeks, and the first of our secondary outcomes, death from any cause within 12 weeks. Among our secondary outcomes, the trial report included data on duration of hospitalization, mechanical ventilation, and tube or parenteral feeding as well as the risk of adverse events or complications. Cost‐effectiveness was also estimated in this single study.
Excluded studies
We excluded two studies that, although prospective, did not adhere to a proper randomization protocol; one involved a single participant, and the other was a cross‐over trial that did not randomize participants to placebo or experimental intervention (see Characteristics of excluded studies) (Davis 1992; Kaplan 1979).
Risk of bias in included studies
The 'Risk of bias' assessment of the included study is summarized in the 'Risk of bias' table within Characteristics of included studies and Figure 2. We judged the risk of bias as low for all domains other than incomplete outcome data. Although all enrolled participants were included in the primary analysis (length of hospital stay), with the exception of those found after randomization not to have laboratory‐confirmed infant botulism, the trial authors excluded participants never admitted to the intensive care unit or never mechanically ventilated from the "Length of intensive care unit stay" and "Duration of mechanical ventilation" analyses, which compromised randomized treatment allocation and allowed for possible between‐treatment group imbalances and uncontrolled confounding for these outcomes.
Figure 2.
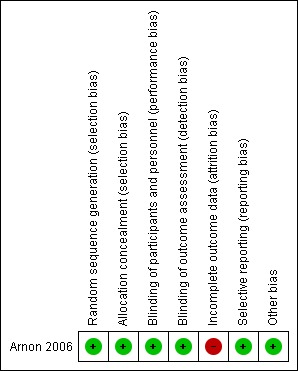
'Risk of bias' summary: review authors' judgements about each 'Risk of bias' item for each included study. Red = high risk of bias; yellow = unclear risk of bias (not shown); green = low risk of bias.
Effects of interventions
See: Table 1
The included study presented numerical outcome data in tables. We were unable to obtain individual participant data from the study authors.
We performed no subgroup analyses investigating any effect of mechanism of botulism, children versus adults, risk of bias, year of the trial, and location of the study due to the fact that our search of the literature resulted in the inclusion of only a single study. We could not perform a subgroup analysis of timing of the initiation of treatment due to the limits of the data reported in the original paper.
Primary outcome measure
In‐hospital death from any cause occurring within four weeks from randomization or the beginning of treatment
There were no in‐hospital deaths within four weeks in either the treatment or the control group of the single study examining the use of BIG‐IV in infant botulism. As a result, it was not possible to estimate the risk ratio (RR), while the absolute risk reduction (ARR) was 0.00 (95% confidence interval (CI) ‐0.03 to 0.03) (see Analysis 1.1, Analysis 1.2).
Analysis 1.1.
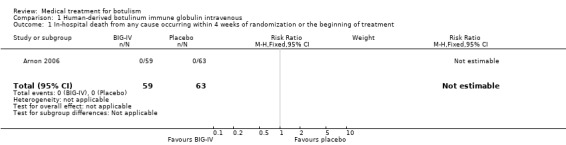
Comparison 1 Human‐derived botulinum immune globulin intravenous, Outcome 1 In‐hospital death from any cause occurring within 4 weeks of randomization or the beginning of treatment.
Analysis 1.2.

Comparison 1 Human‐derived botulinum immune globulin intravenous, Outcome 2 In‐hospital death from any cause occurring within 4 weeks of randomization or the beginning of treatment.
Secondary outcome measures
Death from any cause occurring within 12 weeks from randomization or the beginning of treatment
There were no deaths within 12 weeks in either the treatment or the control group of the single study examining the use of BIG‐IV in infant botulism. As a result, it was not possible to estimate the RR, while the ARR was 0.00 (95% CI ‐0.03 to 0.03) (see Analysis 1.3, Analysis 1.4). One death occurred five months after symptom onset in a participant who received the control treatment and was eventually diagnosed with spinal muscular atrophy.
Analysis 1.3.
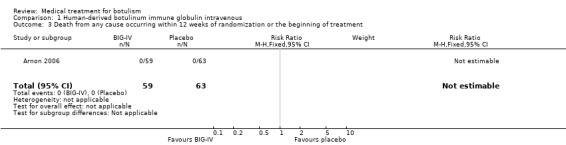
Comparison 1 Human‐derived botulinum immune globulin intravenous, Outcome 3 Death from any cause occurring within 12 weeks of randomization or the beginning of treatment.
Analysis 1.4.

Comparison 1 Human‐derived botulinum immune globulin intravenous, Outcome 4 Death from any cause occurring within 12 weeks of randomization or the beginning of treatment.
Duration of hospitalization
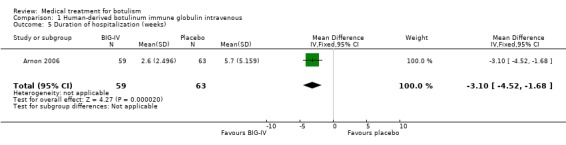
Reported in Arnon 2006 (59 participants treated with BIG‐IV and 63 participants who received the control treatment)
There was a significant beneficial effect of treating infant botulism with BIG‐IV: mean hospital stay 2.60 weeks (95% CI 1.95 to 3.25) compared to control: 5.70 weeks (95% CI 4.40 to 7.00), which resulted in a mean difference (MD) of ‐3.10 weeks (95% CI ‐4.52 to ‐1.68) (see Analysis 1.5, Figure 3).
Analysis 1.5.
Comparison 1 Human‐derived botulinum immune globulin intravenous, Outcome 5 Duration of hospitalization (weeks).
Figure 3.

Forest plot of comparison: 1 Human‐derived botulinum immune globulin intravenous, outcome: 1.5 Duration of hospitalization (weeks).
Duration of mechanical ventilation
Reported in Arnon 2006 (24 participants treated with BIG‐IV and 35 participants who received the control treatment)
The substantially fewer participants involved in this analysis was due entirely to the fact that only a proportion of participants required intubation. There was a significant beneficial effect of treating infant botulism with BIG‐IV: mean duration 1.80 weeks (95% CI 1.20 to 2.40) compared to control: 4.40 weeks (95% CI 3.00 to 5.80), which resulted in an MD of ‐2.60 weeks (95% CI ‐4.06 to ‐1.14) (see Analysis 1.6, Figure 4).
Analysis 1.6.

Comparison 1 Human‐derived botulinum immune globulin intravenous, Outcome 6 Duration of mechanical ventilation (weeks).
Figure 4.

Forest plot of comparison: 1 Human‐derived botulinum immune globulin intravenous, outcome: 1.6 Duration of mechanical ventilation (weeks).
Duration of tube or parenteral feeding
Reported in Arnon 2006 (59 participants treated with BIG‐IV and 63 participants who received control treatment)
There was a significant beneficial effect of treating infant botulism with BIG‐IV: mean duration 3.60 weeks (95% CI 1.70 to 5.50) compared to control: 10.00 weeks (95% CI 6.85 to 13.15), which resulted in an MD of ‐6.40 weeks (95% CI ‐10.00 to ‐2.80) (see Analysis 1.7, Figure 5).
Analysis 1.7.

Comparison 1 Human‐derived botulinum immune globulin intravenous, Outcome 7 Duration of tube or parenteral feeding (weeks).
Figure 5.

Forest plot of comparison: 1 Human‐derived botulinum immune globulin intravenous, outcome: 1.7 Duration of tube or parenteral feeding (weeks).
Risk of adverse events or complications of treatments
Reported in Arnon 2006 (65 participants treated with BIG‐IV and 64 participants who received the control treatment)
There were 41 participants with adverse events in the treatment group and 44 participants with adverse events in the control group. There was no significant difference in the risk of adverse events between groups (RR 0.92, 95% CI 0.72 to 1.18; ARR 0.06, 95% CI 0.22 to ‐0.11). Of the 129 randomized participants, seven proved not to have botulism. Unfortunately, we were not able to calculate the RR for this subgroup because the article provided insufficient data (see Analysis 1.8, Analysis 1.9).
Analysis 1.8.

Comparison 1 Human‐derived botulinum immune globulin intravenous, Outcome 8 Adverse events.
Analysis 1.9.

Comparison 1 Human‐derived botulinum immune globulin intravenous, Outcome 9 Adverse events.
Discussion
Summary of main results
A single RCT at low risk of bias provided evidence of low or moderate certainty for the use of human‐derived botulinum immune globulin intravenous (BIG‐IV) in infant botulism (Arnon 2006). The study demonstrated based on moderate‐certainty evidence that the use of BIG‐IV resulted in significant decreases in the duration of hospitalization and tube or parenteral feeding, and with low‐certainty evidence that it reduced the duration of mechanical ventilation (see Table 1). Moderate‐certainty evidence indicated that there was no significant increase in the risk of adverse events. The absence of any deaths attributable to botulism is likely to be a reflection of the importance of modern intensive care supportive therapy, in particular mechanical ventilation. This single study provided some evidence of the cost‐effectiveness of BIG‐IV in infant botulism. The authors reported a significant decrease of almost USD 90,000 (2004 USD) in the mean total hospital charges between participants who received BIG‐IV versus those who received the control treatment (from USD 163,400 to USD 74,800; two‐sided t‐test; P < 0.001). However, the hospital charges considered in these calculations did not include the cost of BIG‐IV, the fees of the attending physicians unless billed through the hospital, and the cost of any hospital transfers.
Other evidence
An open‐label extension of the aforementioned RCT included 382 participants. This study demonstrated that treatment of infant botulism with BIG‐IV resulted in a decrease in the mean duration of hospitalization of 3.5 weeks relative to historical controls. In addition, the results suggested that treatment within three days as compared to seven days of hospitalization resulted in statistically different results, with a mean length of hospital stay of 2.0 weeks as compared to 2.9 weeks, respectively (Arnon 2006). Finally, three retrospective studies examining 150 participants, 46 of whom received BIG‐IV, demonstrated similar decreases in the duration of hospitalization, mechanical ventilation, and parenteral or tube feeding (Thompson 2005; Tseng‐Ong 2007; Underwood 2007).
A recent retrospective cohort study of 49 patients with infant botulism seen in Mendoza, Argentina between 1993 and 2007 was the first to investigate the efficacy of equine‐derived botulism antitoxin in this form of botulism (Vanella de Cuetos 2011). Thirty‐one patients treated with equine‐derived botulinum antitoxin within five days of the onset of signs were compared to 18 patients who were not treated. Infants treated with the antitoxin had a mean length of hospital stay of 28.7 days (95% CI 24.6 to 32.8) versus 52.6 (95% CI 39.3 to 65.9) for those not treated with antitoxin; mean length of intensive care unit stay of 17.1 days (95% CI 15.3 to 18.9) versus 28.3 days (95% CI 19.9 to 36.7); mean duration of mechanical ventilation of 14.3 days (95% CI 12.5 to 16.1) versus 25.4 days (95% CI 16.6 to 34.2); and mean duration of tube or intravenous feeding of 24.8 days (95% CI 21.3 to 28.3) versus 49.2 days (95% CI 37.2 to 61.2). The only adverse reaction attributed to the use of the antitoxin was in one infant who developed a transient erythematous exanthem. The authors chose to limit participant inclusion to those who underwent some period of mechanical ventilation, thereby limiting the generalizability of their results. In addition, there was no attempt to control for potentially confounding factors such as age, serum concentration of botulinum toxin, incubation period, and timing of antitoxin administration.
Equine‐derived antitoxin is not widely used in infant botulism, but it is considered 'standard of care' by many clinicians in the treatment of food‐borne botulism. Although there is no RCT‐level evidence to support its use, there is one retrospective cohort study of 132 cases of laboratory‐confirmed type A food‐borne botulism reported to the Centers for Disease Control and Prevention between 1973 and 1980, 115 (87%) of whom received trivalent (types A, B, and E) equine‐derived botulinum antitoxin (Tacket 1984). The authors’ observations suggest that the antitoxin produced a 36% decrease in mortality when given within 24 hours of symptom onset and a 31% decrease in mortality when given after 24 hours of symptom onset compared to those not receiving antitoxin. Causes of death and when deaths occurred were not clearly defined. In survivors, a shorter median number of days of hospitalization was associated with antitoxin use (56 days if no antitoxin; 41 days if antitoxin infused > 24 hours after symptom onset; 10 days if antitoxin infused < 24 hours after symptom onset). This association was also found in survivors for median number of days of mechanical ventilation (28 days if no antitoxin; 21 days if antitoxin infused > 24 hours after symptom onset; 0 days if antitoxin infused < 24 hours after symptom onset). In this study, there was only a modest attempt to control for confounders (stratification based on age and incubation period), and adverse effects, or lack thereof, were not reported. In addition, by failing to report any inferential statistics (that is 95% CI, P values, etc.), the authors limited the generalizability of their results, making it difficult to extrapolate their estimates to other countries besides the USA or time periods after 1980.
A smaller case series of 18 participants, all of whom received trivalent equine‐derived botulinum antitoxin for food‐borne botulism after an outbreak of botulism in Thailand due to contaminated bamboo shoots, also suggests that the antitoxin was effective in increasing the rate of recovery, and that earlier administration of the antitoxin was more effective (Kongsaengdao 2006). In this study, the investigators reported that infusion of the antitoxin on day four versus day six after exposure to the botulinum toxin resulted in a significant decrease in the number of days of mechanical ventilation and in the number of days from botulinum toxin exposure to extubation, as demonstrated by Kaplan‐Meier survival analyses (P = 0.028 and P = 0.022, respectively).
The use of equine‐derived botulinum antitoxin has been described in wound botulism as well. A retrospective case series reported that among seven participants with laboratory‐confirmed wound botulism from the subcutaneous injection of heroin, there was more rapid recovery among the two who received the antitoxin within four days after symptom onset compared to the four who received the antitoxin after eight days and the one participant who never received antitoxin (Chang 2003).
The most important reported complications of equine‐derived antitoxin are hypersensitivity reactions. In a review of all cases of antitoxin treatment reported to the Centers for Disease Control and Prevention between 1967 and 1977, of 268 participants, 24 (9%) suffered a hypersensitivity reaction, 5 (1.9%) of which were anaphylaxis and 10 (3.7%) of which were serum sickness (Black 1980). A more recent study evaluated the safety and efficacy of Japanese‐manufactured monovalent (serotype E) and tetravalent (serotypes A, B, E, and F) equine‐derived botulinum antitoxin therapy. Among 134 individuals with food‐borne botulism reported in the literature over a 52‐year period in Japan, adverse effects were reported in only 2 people (1.5%): a non‐fatal immediate allergic reaction in one, and serum‐sickness‐like rash and arthralgia in the other. The completeness of reporting of adverse effects in the cohort studied is unclear (Mottate 2016). There were no reports of anaphylaxis or serum sickness during the trial of BIG‐IV (Arnon 2006).
An investigational recombinant botulinum vaccine for BoNT serotypes A and B was assessed in an open‐label, uncontrolled study in 45 healthy volunteers who had previously been immunized with pentavalent botulinum toxoid. A single dose of the vaccine produced an appropriate antibody response in most participants, and was free of serious adverse effects (Khouri 2018). Such a vaccine is potentially useful to provide occupational protection for botulism laboratory workers (Khouri 2018).
There are a number of case reports and small retrospective case series examining the use of guanidine in food‐borne botulism, some of which suggest that guanidine may provide some improvement in symptoms and electrophysiologic parameters (Cherington 1968; Cherington 1970; Cherington 1974; Faich 1971; Oh 1975; Puggiari 1978). However, the only prospective study, a double‐blind, cross‐over study of six volunteers with moderate to severe food‐borne botulism that was without randomization and with the use of placebo in only three participants, demonstrated no change in the rate of improvement while the participants were receiving guanidine compared to the weeks when they received placebo (Kaplan 1979).
There are two case reports describing the use of 3,4‐diaminopyridine (3,4 DAP) in food‐borne botulism, the results of which are conflicting (Davis 1992; Dock 2002). A more recent animal study and a case series (involving three participants) suggest that 3,4 DAP therapy may be an effective symptomatic treatment and may delay the advancement of paralysis to respiratory failure, although the overall mechanisms for reversing paralysis in BoNT‐poisoned nerve terminals are not yet fully understood (Bradford 2018; Friggeri 2013). There are three case reports describing the use of plasmapheresis in food‐borne botulism that suggest it may be of some benefit (Atabek 2002; Paterson 1992; Sato 2000).
Overall completeness and applicability of evidence
There is no RCT evidence for or against the use of BIG‐IV in other forms of botulism such as food‐borne, wound, or adult intestinal toxemia botulism. In fact, our search of the literature failed to produce even non‐RCT evidence for the use of BIG‐IV in non‐infant botulism.
Quality of the evidence
The single included study was well designed and reasonably well executed, although intention‐to‐treat principles were violated when the efficacy analyses excluded participants initially enrolled in the trial but later found not to have infant botulism. In addition, there were possible between‐treatment group imbalances among those participants admitted to the intensive care unit as well as those who were mechanically ventilated.
Potential biases in the review process
The possibility of publication bias is impossible to exclude, although the small number of studies revealed by our search is likely to be a reflection of the rarity of the disease. Our search of trials registries did not identify any completed and unpublished studies.
Agreements and disagreements with other studies or reviews
We are not aware of any other systematic reviews examining the medical treatment of botulism.
Authors' conclusions
We found low‐ and moderate‐certainty evidence that human‐derived botulinum immune globulin intravenous is of benefit in facilitating earlier recovery from infant botulism than no treatment, although this is based upon a single randomized controlled trial. Human‐derived botulinum immune globulin intravenous probably decreases the duration of hospitalization; may decrease the duration of mechanical ventilation; and probably decreases the duration of tube or parenteral feeding.
Further clinical trials are required to investigate the use of human‐derived botulinum immune globulin intravenous, equine‐derived antitoxin, and other potential therapies including plasmapheresis in all forms of botulism. Although botulism is a relatively rare disease and the mortality is now quite low, early recovery can have significant implications on medical costs as well as patient morbidity (Arnon 2006). In addition, although generally rare, the risk of botulism remains important as evidenced by the recent large outbreak in Thailand that involved 209 people (Kongsaengdao 2006).
Acknowledgements
The Information Specialist of Cochrane Neuromuscular conducted the searches for the review.
This project was supported by the National Institute for Health Research (NIHR), via Cochrane Infrastructure funding to the Cochrane Neuromuscular Disease Group. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, National Health Service (NHS), or the Department of Health. Cochrane Neuromuscular is also supported by the MRC Centre for Neuromuscular Disease.
Appendices
Appendix 1. Cochrane Neuromuscular Specialised Register via the Cochrane Register of Studies (CRS‐Web) search strategy
#1 MESH DESCRIPTOR Botulism EXPLODE ALL WITH QUALIFIER DT PC TH AND INREGISTER #2 MESH DESCRIPTOR Clostridium botulinum EXPLODE ALL AND INREGISTER #3 clostridium ADJ2 botulinum AND INREGISTER #4 #2 OR #3 AND INREGISTER #5 MESH DESCRIPTOR Botulinum Antitoxin EXPLODE ALL AND INREGISTER #6 botulinum ADJ2 antitoxin AND INREGISTER #7 #5 OR #6 AND INREGISTER #8 #4 AND #7 AND INREGISTER #9 #1 OR #8 AND INREGISTER
Appendix 2. Cochrane Central Register of Controlled Trials (CENTRAL) via the Cochrane Register of Studies (CRS‐Web) search strategy
#1 MESH DESCRIPTOR Botulism EXPLODE ALL WITH QUALIFIER DT PC TH AND CENTRAL:TARGET #2 MESH DESCRIPTOR Clostridium botulinum EXPLODE ALL AND CENTRAL:TARGET #3 clostridium ADJ2 botulinum AND CENTRAL:TARGET #4 #2 OR #3 AND CENTRAL:TARGET #5 MESH DESCRIPTOR Botulinum Antitoxin EXPLODE ALL AND CENTRAL:TARGET #6 botulinum ADJ2 antitoxin AND CENTRAL:TARGET #7 #5 OR #6 AND CENTRAL:TARGET #8 #4 AND #7 AND CENTRAL:TARGET #9 #1 OR #8 AND CENTRAL:TARGET
Appendix 3. MEDLINE (OvidSP) search strategy
Database: Ovid MEDLINE(R) Epub Ahead of Print, In‐Process & Other Non‐Indexed Citations, Ovid MEDLINE(R) Daily and Ovid MEDLINE(R) <1946 to Present> Search Strategy: ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐ 1 randomized controlled trial.pt. (451600) 2 controlled clinical trial.pt. (92093) 3 randomized.ab. (400436) 4 placebo.ab. (185728) 5 drug therapy.fs. (1986134) 6 randomly.ab. (283540) 7 trial.ab. (415540) 8 groups.ab. (1754833) 9 or/1‐8 (4122481) 10 exp animals/ not humans.sh. (4416296) 11 9 not 10 (3560815) 12 Botulism/dt, th [Drug Therapy, Therapy] (608) 13 exp Clostridium botulinum/ (2820) 14 Botulinum Antitoxin/ (304) 15 (botulinum adj5 antitoxin$).mp. (474) 16 or/12‐15 (3465) 17 11 and 16 (314) 18 remove duplicates from 17 (313)
Appendix 4. Embase (OvidSP) search strategy
Database: Embase <1980 to 2018 Week 04> Search Strategy: ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐ 1 crossover‐procedure.sh. (53781) 2 double‐blind procedure.sh. (142439) 3 single‐blind procedure.sh. (30087) 4 randomized controlled trial.sh. (480356) 5 (random$ or crossover$ or cross over$ or placebo$ or (doubl$ adj blind$) or allocat$).tw,ot. (1443866) 6 trial.ti. (234007) 7 or/1‐6 (1607044) 8 (animal/ or nonhuman/ or animal experiment/) and human/ (1683457) 9 animal/ or nonanimal/ or animal experiment/ (3815641) 10 9 not 8 (3164930) 11 7 not 10 (1477492) 12 limit 11 to (conference abstracts or embase) (1244313) 13 Botulism/dt, th [Drug Therapy, Therapy] (884) 14 exp Clostridium botulinum/ (4026) 15 Botulinum Antiserum/ (586) 16 (botulinum adj5 antitoxin$).ti,ab. (129) 17 or/13‐16 (4821) 18 12 and 17 (69) 19 remove duplicates from 18 (68)
Appendix 5. World Health Organization International Clinical Trials Registry Platform
Condition: Botulism
Intervention: antitoxin OR antiserum
Appendix 6. ClinicalTrials.gov
Condition or Disease: Botulism
Appendix 7. Protocol for use if meta‐analysis becomes possible (from standard protocol)
Unit of analysis issues
Where multiple trial arms are reported in a single trial, we will include only the treatment arms relevant to the review topic. If two comparisons (e.g. drug A versus placebo and drug B versus placebo) are combined in the same meta‐analysis, we will follow guidance in Section 16.5.4 of the Cochrane Handbook for Systematic Reviews of Interventions to avoid double‐counting (Higgins 2011b). Our preferred approach will be to combine groups to create a single pairwise comparison, as recommended. For cross‐over or other trials where the summary data for each intervention group may not be reported, we will use the generic inverse‐variance meta‐analysis, as described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011c).
Dealing with missing data
We will contact investigators or study sponsors in order to verify key study characteristics and to obtain missing numerical outcome data where possible (e.g. when a study is available as an abstract only). Where this is not possible, and the missing data are thought to introduce serious bias, we will explore the impact of including such studies in the overall assessment of results by a sensitivity analysis.
We will replace data that cannot be obtained with replacement values representing a poor outcome for dichotomous outcomes, and the mean value for continuous outcomes. We will assess the effect of our assumptions in a sensitivity analysis. We will address the impact of missing data in our Discussion section.
Assessment of heterogeneity
We will use the I2 statistic to measure heterogeneity among the trials in each analysis. If we identify substantial unexplained heterogeneity, we will report it and explore possible causes by prespecified subgroup analysis. We will use the rough guide to interpretation as outlined in the Cochrane Handbook for Systematic Reviews of Interventions, as follows:
0% to 40%: might not be important;
30% to 60%: may represent moderate heterogeneity;
50% to 90%: may represent substantial heterogeneity;
75% to 100%: considerable heterogeneity.
We will avoid the use of absolute cut‐off values, but interpret the I2 statistic in relation to the size and direction of effects and strength of evidence for heterogeneity (e.g. P value from the Chi2 test, or the confidence interval for I2) (Deeks 2011).
Assessment of reporting biases
If we are able to pool more than 10 trials, we will create and examine a funnel plot to explore possible small‐study biases.
Data synthesis
We will use a random‐effects model in Review Manager 5 (RevMan 2014), as this is usually a more conservative approach. Where analyses include both small and large studies, we will perform a sensitivity analysis to determine whether their results are systematically different, since under such circumstances, use of a random‐effects meta‐analysis will exacerbate the effects of the bias. If the results are systematically different, we will perform a sensitivity analysis in which small studies are excluded.
If the review includes more than one comparison that cannot be included in the same analysis, we will report the results for each comparison separately.
If regression methods have been used for the censored data, we will pool the estimated hazard ratios or treatment effect differences with their standard errors for the different studies using the generic inverse‐variance function in Review Manager 5 (RevMan 2014).
Subgroup analysis and investigation of heterogeneity
We will perform subgroup analyses (limited to our primary outcomes) to investigate the influence of the mechanism of botulism (infant botulism, food‐borne botulism, wound botulism, and adult intestinal toxemia botulism), children versus adults (adults defined as 18 years of age or older), and hyperacute (less than 24 hours) versus acute (greater than 24 hours but less than seven days) versus subacute (greater than or equal to seven days) initiation of treatment after disease onset, as well as risk of bias, year of the trial, and location of the study.
We will use the formal test for subgroup interactions in Review Manager 5 (RevMan 2014).
Sensitivity analysis
We will perform sensitivity analyses including:
fixed‐effect versus random‐effects models;
publication status (published versus unpublished);
after removal of studies assessed at high risk of bias in any 'Risk of bias' domain;
study size (fewer than 20 study participants in each intervention group)
Data and analyses
Comparison 1.
Human‐derived botulinum immune globulin intravenous
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 In‐hospital death from any cause occurring within 4 weeks of randomization or the beginning of treatment | 1 | 122 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 2 In‐hospital death from any cause occurring within 4 weeks of randomization or the beginning of treatment | 1 | 122 | Risk Difference (M‐H, Fixed, 95% CI) | 0.0 [‐0.03, 0.03] |
| 3 Death from any cause occurring within 12 weeks of randomization or the beginning of treatment | 1 | 122 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 4 Death from any cause occurring within 12 weeks of randomization or the beginning of treatment | 1 | 122 | Risk Difference (M‐H, Fixed, 95% CI) | 0.0 [‐0.03, 0.03] |
| 5 Duration of hospitalization (weeks) | 1 | 122 | Mean Difference (IV, Fixed, 95% CI) | ‐3.1 [‐4.52, ‐1.68] |
| 6 Duration of mechanical ventilation (weeks) | 1 | 59 | Mean Difference (IV, Fixed, 95% CI) | ‐2.60 [‐4.06, ‐1.14] |
| 7 Duration of tube or parenteral feeding (weeks) | 1 | 122 | Mean Difference (IV, Fixed, 95% CI) | ‐6.4 [‐10.00, ‐2.80] |
| 8 Adverse events | 1 | 129 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.92 [0.72, 1.18] |
| 9 Adverse events | 1 | 129 | Risk Difference (M‐H, Fixed, 95% CI) | ‐0.06 [‐0.22, 0.11] |
What's new
| Date | Event | Description |
|---|---|---|
| 20 August 2018 | New citation required but conclusions have not changed | Discussion updated. We documented methods for use in the event of meta‐analysis in more detail to conform to current reporting standards. We reviewed and downgraded the evidence an additional level compared to the previous update, with most evidence now of moderate certainty, and evidence for the effects on the duration of mechanical ventilation of low certainty (Table 1). We updated the Discussion. |
| 27 July 2018 | New search has been performed | Update based on a search on 23 January 2018. We found no new included studies. |
History
Protocol first published: Issue 4, 2009 Review first published: Issue 3, 2011
| Date | Event | Description |
|---|---|---|
| 12 November 2013 | New citation required but conclusions have not changed | We identified no additional trials from the updated searches. |
| 9 September 2013 | New search has been performed | Update based on a search on 30 March 2013. 'Summary of findings' table included. |
Differences between protocol and review
There were no significant differences between the design of the protocol and the method by which the review was carried out. However, we described the methods for use in meta‐analysis using text from the current standard Cochrane Neuromuscular protocol at this update and moved these to Appendix 7.
We included a 'Summary of findings' table in the first update of the review.
We did not contact pharmaceutical companies as stated in the protocol, however we added searches of clinical trials registers to identify ongoing and unpublished studies.
Characteristics of studies
Characteristics of included studies [ordered by study ID]
| Methods | Randomized, placebo‐controlled, participant‐, study investigator‐, and outcome assessor‐blinded trial | |
| Participants | 129 participants with initial clinical findings consistent with infant botulism, which was later confirmed with Clostridium botulinum toxin or organisms isolated in stool or enema, who had been admitted to hospital for less than 3 days by the time of study inclusion. Mean age of the intervention group was 131 days, 47% of whom were male, while the mean age of the placebo group was 105 days, 32% of whom were male (the remainder were female). | |
| Interventions | Intervention: human‐derived botulism immune globulin intravenous 50 mg/kg, single dose (n = 65) Placebo: "Identical‐appearing" intravenous immune globulin (Gammagard or Gammagard S/D) that did not neutralize botulinum toxin in the mouse bioassay (n = 64) |
|
| Outcomes | Length of hospital stay required (measured in weeks, defined as the time required until the fulfillment of certain criteria for discharge including no further need for inpatient care for infant botulism or its complications, no need for mechanical ventilation or supplemental oxygenation for at least 3 days, no worsening of paralysis in the previous 3 days and a demonstrated improvement in motor and bulbar function, 3 days of intake by tube feeding of 25% or less of maintenance volume and calories)
|
|
| Conflicts of interest | No major conflicts of interest | |
| Funding | A co‐operative agreement between the US Food and Drug Administration Office of Orphan Products Development and the Calfiornia Department of Public Health | |
| Notes | Length of follow‐up limited to duration of hospitalization. Intervention group was older (mean 131 versus 105 days old), heavier (mean weight 6.7 kg versus 5.9 kg), and more likely to be male (47% versus 32%), demonstrating that randomized treatment allocation was not entirely successful. The review authors were unable to obtain individual patient data and therefore had to reconstruct standard deviations using the 95% confidence interval provided in the original article. Due to the rounding of values in the original article, this led to small discrepancies between our calculated 95% confidence interval and those reported in the original article. Conducted from 1992 to 1997 in the USA |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Trialists used a printed random‐number table to generate a number that was associated with 1 of 8 letter codes stamped on the drug vials through the use of a master sequential list. |
| Allocation concealment (selection bias) | Low risk | The study statistician performed allocation using a printed random‐number table to assign a letter code‐associated drug vial to each participant. The study statistician kept the master sequential list, and it was unavailable to the study investigators. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Participants and study investigators appeared to have been blinded to allocation status, although it would have been preferable if there had been an attempt to measure the success of this blinding in survey participants and study investigators to see whether they were able to successfully guess allocation status. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Although the published manuscript was not clear, we contacted the authors who confirmed that the outcome assessors were blinded to allocation status. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | All participants enrolled into the trial were included in the primary analysis (length of hospital stay), with the exception of those participants found after randomization not to have laboratory‐confirmed infant botulism (6 treatment participants, 1 control participant). On the other hand, the authors excluded participants never admitted to the intensive care unit or never mechanically ventilated from the "Length of intensive care unit stay" and "Duration of mechanical ventilation" analyses, compromising randomized treatment allocation and allowing for possible between‐treatment group imbalances and uncontrolled confounding. The safety analysis included all enrolled participants. |
| Selective reporting (reporting bias) | Low risk | The report fully describes the results for all outcomes. |
| Other bias | Low risk | No apparent other bias |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Davis 1992 | This was a double‐blinded, placebo‐controlled, cross‐over trial that was done on a single participant, with the outcomes measured while the participant was alternating on or off 3,4‐diaminopyridine versus placebo, with no evident attempt to randomize when the participant received the intervention. |
| Kaplan 1979 | This was a double‐blinded, placebo‐controlled, cross‐over trial where 50% of the participants (3 of 6 participants) withdrew from the study before receiving placebo, and there was no attempt to randomly assign participants to intervention versus placebo. |
Contributions of authors
In 2011, the first draft of the Background was written by MK; the study selection criteria and outcomes by CC; and the data analysis by TB. All authors contributed to editing and revising the final version of the protocol. CC, TB, and MK shared assessment of search strategy citations, 'Risk of bias' assessment, and data extraction. MK performed the analyses. MK wrote the first draft of the text of the full review. All authors contributed to editing and revising the final version of the review text.
For the 2013 update, CC, TB, and MK shared assessment of search strategy citations; MK wrote the first draft of the text of the update; and all authors contributed to editing and revising the final version of the update.
For the 2018 update, CC and JP shared assessment of search strategy citations; JP wrote the first draft of the text of the update; and all authors contributed to editing and revising the final version of the update.
Sources of support
Internal sources
None, Other.
External sources
None, Other.
Declarations of interest
CC: none known.
TB: none known.
JP: none known.
MK: I report speaker and advisory fees for Eisai, Elsevier, Sunovion, Novartis, Sage Therapeutics, and UCB; unrestricted educational grants from UCB; and research grants from UCB and Eisai.
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
- Arnon SS, Schechter R, Maslanka SE, Jewell NP, Hatheway CL. Human botulism immune globulin for the treatment of infant botulism. New England Journal of Medicine 2006;354(5):462‐71. [PUBMED: 16452558] [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
- Davis LE, Johnson JK, Bicknell JM, Levy H, McEvoy KM. Human type A botulism and treatment with 3,4‐diaminopyridine. Electromyography and Clinical Neurophysiology 1992;32(7‐8):379‐83. [PubMed] [Google Scholar]
- Kaplan JE, Davis LE, Narayan V, Koster J, Katzenstein D. Botulism, type A, and treatment with guanidine. Annals of Neurology 1979;6(1):69‐71. [DOI] [PubMed] [Google Scholar]
Additional references
- Atabek ME, Yavuz H, Oran B, Karaaslan S, Erkul I. Plasmapheresis as an adjunct treatment in severe botulism. Intensive Care Medicine 2002;28(6):814. [DOI] [PubMed] [Google Scholar]
- Black RE, Gunn RA. Hypersensitivity reactions associated with botulinal antitoxin. American Journal of Medicine 1980;69(4):567‐70. [DOI] [PubMed] [Google Scholar]
- Bradford AB, Machamer JB, Russo TM, McNutt PM. 3,4‐diaminopyridine reverses paralysis in botulinum neurotoxin‐intoxicated diaphragms through two functionally distinct mechanisms. Toxicology and Applied Pharmacology 2018;341:77‐86. [DOI] [PubMed] [Google Scholar]
- Brett M, Hood J, Brazier J, Duerden B, Hahné S. Soft tissue infections caused by spore‐forming bacteria in injecting drug users in the United Kingdom. Epidemiology and Infection 2005;133(4):575‐82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. Botulism from home‐canned bamboo shoots ‐ Nan Province, Thailand. Morbidity and Mortality Weekly Report 2006;55(14):389‐92. [PubMed] [Google Scholar]
- Chang GY, Ganguly G. Early antitoxin treatment in wound botulism results in better outcome. European Journal of Neurology 2003;49(3):151‐3. [DOI] [PubMed] [Google Scholar]
- Cherington M, Ryan DW. Botulism and guanidine. New England Journal of Medicine 1968;278(17):931‐3. [DOI] [PubMed] [Google Scholar]
- Cherington M, Ryan DW. Treatment of botulism with guanidine. Early neurophysiologic studies. New England Journal of Medicine 1970;282(4):195‐7. [DOI] [PubMed] [Google Scholar]
- Cherington M. Botulism: ten year experience. Archives of Neurology 1974;30(6):432‐7. [DOI] [PubMed] [Google Scholar]
- Cox N, Hinkle R. Infant botulism. American Family Physician 2002;65(7):1388‐92. [PubMed] [Google Scholar]
- Deeks JJ, Higgins JPT, Altman DG, editor(s). Chapter 9: Analysing data and undertaking meta‐analyses. In: Higgins JPT, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
- Dembek ZF, Smith LA, Rusnak JM. Botulism: cause, effects, diagnosis, clinical and laboratory identification, and treatment modalities. Disaster Medicine and Public Health Preparedness 2007;1(2):122‐34. [DOI] [PubMed] [Google Scholar]
- Dock M, Ali B, Karras A, Misset B, Garrouste‐Orgeas M, Deletie E, et al. Treatment of severe botulism with 3,4 diaminopyridine [Traitement d'un botulisme grave par la 3,4‐diaminopyridine]. Presse Medicale 2002;31(13):601‐2. [PubMed] [Google Scholar]
- Dowell VR Jr. Botulism and tetanus: selected epidemiologic and microbiologic aspects. Reviews of Infectious Diseases 1984;6 Suppl 1:S202‐7. [DOI] [PubMed] [Google Scholar]
- Egger M, Smith GD, Phillips AN. Meta‐analysis: principles and procedures. BMJ 1997;315(7121):1533‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Faich GA, Graebner RW, Sato S. Failure of guanidine therapy in botulism A. New England Journal of Medicine 1971;283(14):773‐6. [DOI] [PubMed] [Google Scholar]
- Friggeri A, Marçon F, Marciniak, S, Lemaire‐Hurtel AS, Seydi AA, Ammenouche N, et al. 3,4‐diaminopyridine may improve neuromuscular block during botulism. Critical Care 2013;17(5):449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brozek J, Oxman A, Schünemann H. GRADEpro. Version 3.2 for Windows. Brozek J, Oxman A, Schünemann H, 2008.
- Higgins JPT, Altman DG, Sterne JAC, editor(s). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
- Higgins JPT, Deeks JJ, Altman DG, editor(s). Chapter 16: Special topics in statistics. In: Higgins JPT, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
- Higgins JPT, Deeks JJ, editor(s). Chapter 7: Selecting studies and collecting data. In: Higgins JPT, Green S, editor(s), Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
- Khouri JM, Motter RN, Arnon SS. Safety and immunogenicity of investigational recombinant botulinum vaccine, rBV A/B, in volunteers with pre‐existing botulinum toxoid immunity. Vaccine 2018;36(15):2041‐8. [DOI] [PubMed] [Google Scholar]
- Koepke R, Sobe J, Arnon SS. Global occurrence of infant botulism, 1976‐2006. Pediatrics 2008;122:e73‐82. [DOI] [PubMed] [Google Scholar]
- Kongsaengdao S, Samintarapanya K, Rusmeechan S, Wongsa A, Pothirat C, Permpikul C, et al. An outbreak of botulism in Thailand: clinical manifestations and management of severe respiratory failure. Clinical Infectious Diseases 2006;43(10):1247–56. [DOI] [PubMed] [Google Scholar]
- McLauchlin J, Grant KA, Little CL. Food‐borne botulism in the United Kingdom. Journal of Public Health 2006;28(4):337‐42. [DOI] [PubMed] [Google Scholar]
- McNally RE, Morrison MB, Bernt JE, Stark M, Fisher J, Bo'Berry J. Effectiveness of Medical Defense Interventions Against Predicted Battlefield Level of Botulinum Toxin A. Joppa, MD: Science Applications International Corporation, 1994. [Google Scholar]
- Mottate K, Yokote H, Mori S, Horita A, Miyatsu Y, Torii Y, et al. Retrospective survey to evaluate the safety and efficacy of Japanese botulinum antitoxin therapy in Japan. Toxicon 2016;110:12‐8. [DOI] [PubMed] [Google Scholar]
- Oh SJ, Halsey JH. Guanidine in type B botulism. Archives of Internal Medicine 1975;135(5):726‐8. [DOI] [PubMed] [Google Scholar]
- Paterson DL, King MA, Boyle RS, Pond SM, Whitby M, Wright M, et al. Severe botulism after eating home‐preserved asparagus. Medical Journal of Australia 1992;157(4):269‐70. [DOI] [PubMed] [Google Scholar]
- Puggiari M, Cherington M. Botulism and guanidine. Ten years later. JAMA 1978;240(21):2276‐7. [PubMed] [Google Scholar]
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
- Robinson RF, Nahata MC. Management of botulism. Annals of Pharmacotherapy 2003;37(1):127‐31. [DOI] [PubMed] [Google Scholar]
- Sato Y, Kimata N, Miyahara S, Nihel H, Agishi T, Takahashi M. Extracorporeal adsorption as a new approach to treatment of botulism. ASAIO Journal 2000;46(6):783‐5. [DOI] [PubMed] [Google Scholar]
- Schünemann HJ, Oxman AD, Higgins JPT, Vist GE, Glasziou P, Guyatt GH. Chapter 11: Presenting results and ‘Summary of findings' tables. In: Higgins JPT, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
- Schünemann HJ, Oxman AD, Vist GE, Higgins JPT, Deeks JJ, Glasziou P, et al. Chapter 12: Interpreting results and drawing conclusions. In: Higgins JPT, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
- Shapiro RL, Hatheway C, Swerdlow DL. Botulism in the United States: a clinical and epidemiologic review. Annals of Internal Medicine 1998;129(3):221‐8. [DOI] [PubMed] [Google Scholar]
- Sieradzan KA. Wound botulism. Practical Neurology 2005;5(1):46‐51. [Google Scholar]
- Sobel J. Botulism. Clinical Infectious Diseases 2005;41(8):1167‐73. [DOI] [PubMed] [Google Scholar]
- Tacket CO, Shandera WX, Mann JM, Hargrett NT, Blake PA. Equine antitoxin use and other factors that predict outcome in type A foodborne botulism. American Journal of Medicine 1984;76(5):794‐8. [DOI] [PubMed] [Google Scholar]
- Thompson JA, Filloux FM, Orman CB, Swoboda K, Peterson P, Firth SD, et al. Infant botulism in the age of botulism immune globulin. Neurology 2005;64(12):2029‐32. [DOI] [PubMed] [Google Scholar]
- Tseng‐Ong L, Mitchell WG. Infant botulism: 20 years' experience at a single institution. Journal of Child Neurology 2007;22(12):1333‐7. [DOI] [PubMed] [Google Scholar]
- Underwood K, Rubin S, Deakers T, Newth C. Infant botulism: a 30‐year experience spanning the introduction of botulism immune globulin intravenous in the intensive care unit at Children's Hospital Los Angeles. Pediatrics 2007;120(6):1380‐5. [DOI] [PubMed] [Google Scholar]
- Vanella de Cuetos EEV, Fernandez RA, Bianco MI, Sartori OJ, Piovano ML, Lúquez C, et al. Equine botulinum antitoxin for the treatment of infant botulism. Clinical and Vaccine Immunology 2011;18(11):1845‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to other published versions of this review
- Chalk C, Benstead TJ, Keezer M. Medical treatment for botulism. Cochrane Database of Systematic Reviews 2009, Issue 4. [DOI: 10.1002/14651858.CD008123] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chalk C, Benstead TJ, Keezer M. Medical treatment for botulism. Cochrane Database of Systematic Reviews 2011, Issue 3. [DOI: 10.1002/14651858.CD008123.pub2] [DOI] [PubMed] [Google Scholar]